acute flaccid paralysis ” - · pdf file• acute flaccid paralysis (afp) occurs when...
TRANSCRIPT
Neuro Dr. Nibal
“ Acute Flaccid Paralysis ”
Total Lec: 45

Acute flaccid paralysis
Dr Nebal Waill
Definition
• AcuteFlaccidParalysis(AFP)occurswhenthereisrapidevolutionofmotorweakness(<than4days),withalossoftoneintheparalysedlimb.Thisexcludesweaknessduetotraumaandspasticparalysis.
• AFPisamedicalemergencyasunnecessarydelayscanresultindeathanddisability

• ThelistofunderlyingcausesofAFPisbroad,andthereissubstantialvariationbyage,ethnicity,andgeographicarea.
• Intheabsenceofwildvirus-inducedpoliomyelitis,theacutedemyelinatingformofGuillain-Barresyndrome(AIDP)accountsforatleast50percentofAFPcasesgloballyfollowedinfrequencybyparalyticnon-polioenterovirusinfection,themotoraxonalformofGuillain-Barresyndrome(AMAN),traumaticneuritis,andacutetransversemyelitis.
Background
•1916-Guillian,BarreandStrohldescribed2Frenchsoldierswithmotorweakness,areflexia,and“albuniocytologicaldissociation”inthecerebrospinalfluid.Theyrecognizedtheperipheralnatureoftheillness.
Epidemiology
• AnnualincidenceofGBS=1-3/100000personsannually.• Rareininfants.• Male&femalehavesimilarrisk• Anyagebutmostfrequentat4-9years

GBS subtypes
1. Sporadic AIDP (Acute Inflammatory Demyelinating Polyradiculoneuropathy)
2. AMSAN (Acute Motor and Sensory Axonal Neuropathy) 3. AMAN (Acute Motor Axonal Neuropathy ) 4. MFS ( Miller Fisher Syndrome )
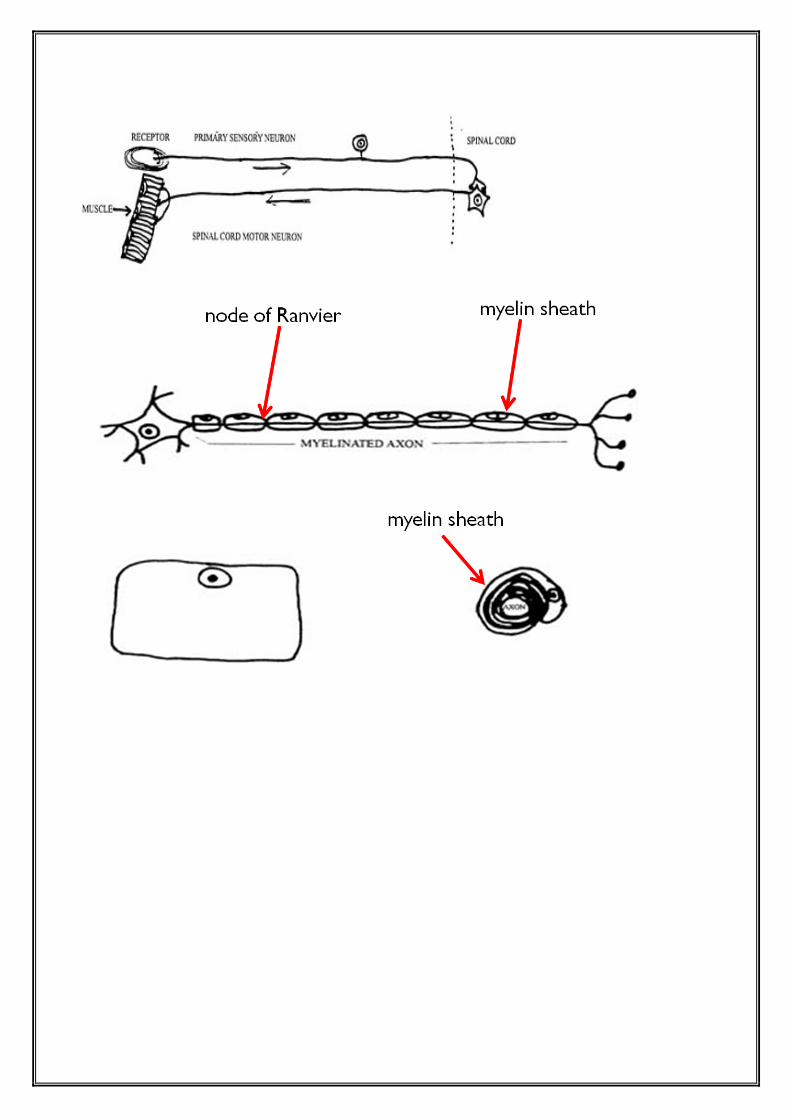
Pathology
• Bothmotorandsensoryfibersareaffected
• AIDP→segmentaldemyelination
↘axonaldegeneration(lessextensive)
• Segmentaldemyelinationoccursatalllevelsofperipheralnervoussystem
↘Anterior+posteriorroots
Sympatheticchainandganglia
Peripheralnerves
• CNSalterationsaresecondarytoaxonaldegenerationandaffect
↘Anteriorhorncellsinspinalgreymatter
Neuronsofmotorcranialnervesnucleiinbrainstem
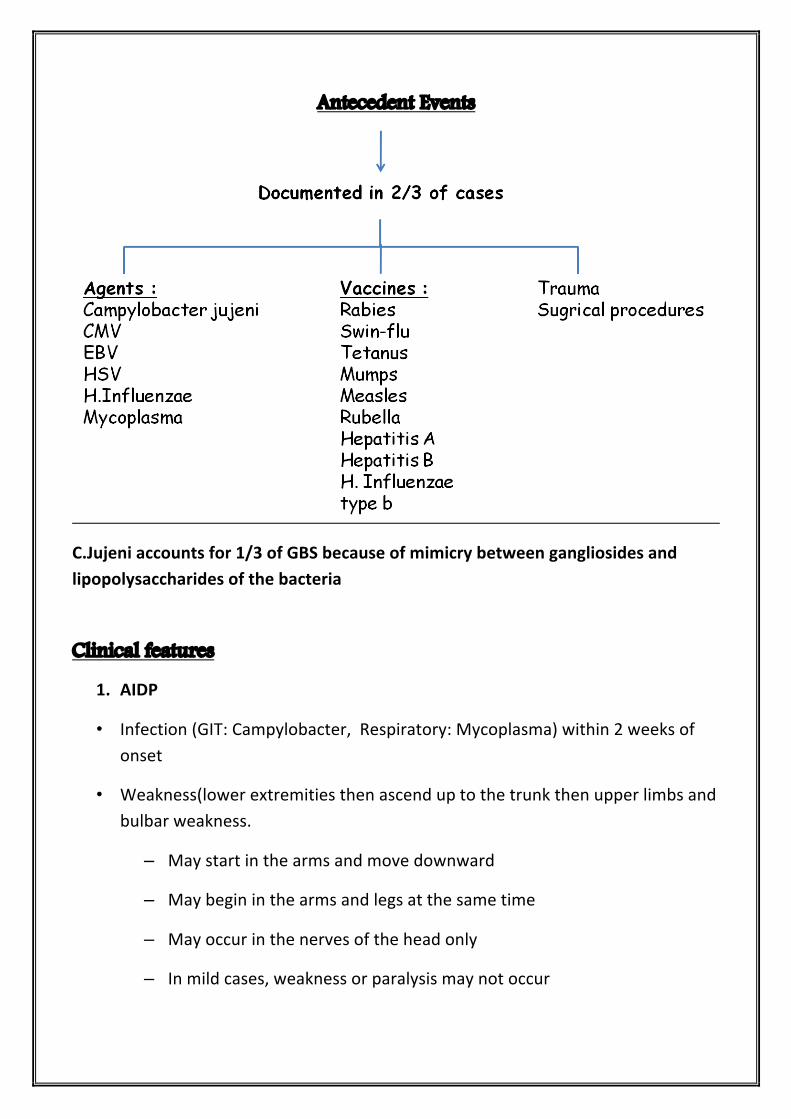
Antecedent Events
C.Jujeniaccountsfor1/3ofGBSbecauseofmimicrybetweengangliosidesandlipopolysaccharidesofthebacteria
Clinical features
1. AIDP
• Infection(GIT:Campylobacter,Respiratory:Mycoplasma)within2weeksofonset
• Weakness(lowerextremitiesthenascenduptothetrunkthenupperlimbsandbulbarweakness.
– Maystartinthearmsandmovedownward
– Maybegininthearmsandlegsatthesametime
– Mayoccurinthenervesoftheheadonly
– Inmildcases,weaknessorparalysismaynotoccur
• Thisweaknessissymmytrical(minorsidesdifferencesmayoccure),proximalanddistal
• 9%isasymmetrical
• progressslowlyoverdaysorweeksOrabruptandrapid
• Childbecomesirritable.
• Parasthesiamayoccur,89%painaccompanyweakness
• 50%bulbarinvolvement.
• Facialnerveinvolved.alsoVI,III,XII,IX,X
• Someshowviralmeningitisormeningoencephalitis.
• Papillodema(unexplainedpathogenesis)
• Respiratorymuscules:reducedvitalcapacityCO2retentioneveninabsenceofrespiratorysymptoms
Featuresrequiredfordiagnosis
1. Progressivemotorweaknessofmorethanonelimb.
2. Areflexiaorhyporeflexia(lossofanklejerksanddiminishedkneeandbicepsreflexeswillsufficeifotherfeaturesareconsistentwiththediagnosis.
� Featruessupportiveofdiagnosis
1. Progression:weaknessmaydeveloprapidlybutceasetoprogressafter4wk.Roughly50%willplateauwithin2wks,80%by3wks,and90%by4wks.
2. Relativesymmetry.
3. Mildsensorysymptomsandsigns.
4. Cranialnerveinvolvementslikefacialweaknessdevelopsinabout50%ofpatients.
5. Autonomicdysfunction.
6. Absenceoffeverattheonsetofneurologicalsymptoms.
7. Recoverywithoutspecifictherapy,begins2-4wksafterprogressionceases,occasionallydelayedformonths.
� Featurescastingdoubtonthediagnosis
1. Markedpersistentasymmetryinmotorfunction.
2. persistentbowelorbladderdysfunctionatonsetofsymptoms.
3. Discretesensorylevel.
4. Progressivephaselongerthan4wks.
5. CSFpleocytosis(>50wcc/mm3).
6. Completeophthalmoplegia(internalorexternal).
Clinical Phases
Guillian-barrecanbedividedintofivedistinctclinicalphases:
• Phase1-first24hrfrompresentation
• Phase2-diseaseprogression
• Phase3-plateauphase
• Phase4-initialrecovery
• Phase5-rehabilitation
Dx
1. Clinical
2. CSF
3. Electrophysiologic
4. MRI
Investigation
MRIofthebrainandspinalcord
Shouldbeconsideredinallpatients,usuallydoneif:
1. Thepresentationisacuteorrapidlyprogressive
2. Therearepredominantlysensorysymptoms(includingbackpain)
3. Thereispredominantsphincterdisturbanceofpresentation
4. Thereisaclearsensoryormarkedmotorlevel
Lumberpuncture
• ElevatedCSFproteinwithoutpleocytosisisasupportivediagnosticfinding,howevertheCSFmaybenormalwithinsevendaysofonsetofsymptoms
• Proteinlevel:elevated(>45mg/dl)afterthefirstweekofsymptoms,peak4-5wks
• WCC<10/mm3,occasionallyupto50mm3
• Glucoselevelnormal
Neurophysiology
• NormalnerveconductionstudiesinthefirstweekdoesnotexcludethediagnosisofGBS
• InAIDPnerveconductionimpairment=conductionblock,decreasecompoundactionpotentialamplitude
• SincethemediandurationofexcretionofCampylobacterinstoolsofinfectedpersonsisonly16daysandbecauseofthe1-to3-weeklagtimebetweeninfectionandtheonsetofGBS,manyGBSpatientswithprecedingCampylobacterinfectionmighthavefalselynegativestoolcultures.
• multiplestoolsamples(orrectalswabs)shouldbeobtainedfromGBSpatients
immediatelyuponadmissiontothehospital,preferably3overa3-dayperiod.
Otherinvestigations
• Fullbloodcount,bloodculture(ifpyrexial)
• Ureaandelectrolytes(hypokalemia)
• Creatinekinase(myositis)
• Chestx-ray,ECG
• Abdominalx-ray(palpablebladder,constipation)
Treatment
1. Admission
2. IVIG
3. Plasmaexchange
4. Supportivetreatment
5. Rehabilitation
• SymptomatictreatmentisanessentialpartofthemanagementofGBS.• Childrenshouldadmittedtothepediatricintensivecareunitiftheyhaveone
ormoreofthefollowing:
1. Flaccidtetraparesis
2. Severerapidlyprogressivecourse
3. Reducedvitalcapacityatorbelow20ml/kg
4. Bulbarpalsywithsymptoms
5. Autonomiccardiovascularinstabilitythatispersistenthypertensionorlabilebloodpressureorarrhythmias.
Plasmaexchange
• PlasmapheresishasremainedthegoldstandardtreatmentforGBSoverthelast20years.
• Shouldbeusedwithin4weeksofonsetofneuropaticsymptomsinnon-ambulatorypatients
• Shouldbeusedwithin2weeksofonsetofneuropathicsymptomsinambulatorypatients
• Plasmapheresisisgenerallysafeinchildrenwhoweigh10kgormore.Aseriesofexchangewithacumulativetotalofapproximately250ml/kgvolumeexchangeorroughlyatriplevolumeexchange.
• DisadvantagesofPlasmapheresisincludeitsrarecomplications,suchassepsis,riskofacquiringviralinfectionssuchashepatitisandHIV.
IVIGtreatmenthasadvantagesoverplasmapheresisbecause
• itiseasiertoadminister,• hassignificantlyfewercomplications,• andismorecomfortableforthepatient.
SideeffectsofIVIG
• expandstheplasmavolumesoitmustbeadministeredwithcautioninpatientswithcongestiveheartfailureandrenalinsufficiency
• fever,myalgia,headache,nausea,andvomiting,butthese"influenza-like"symptomsareself-limiting.
• asepticmeningitis,neutropenia,andhypertension
• Anaphylaxis
• Thromboembolicevents
• riskofserioushepatitisCinfectiontransmissionhasbeenreduced
• IVIGshouldbeusedwithin2weeks
• Corticosteroidnotrecommended
• SequentialtreatmentwithPEthenIVIGnotrecommended
• PE&IVIGrecommendedfortheseveredisease
Painmanagement
� Painofdiscomfortispresentin50-80%ofchildrenwithGBSatthetimeofpresentation.
Managingpainby:
• Opioids
• Nonsteroidalanti-inflammatorydrugs(ibuprofen)
• Anti-epilepticdrugs(carbamazepine,gabapentine)
• Tricyclicantiderpessants(amitryptine)
Preventionofpain:
• Airmatresses
• Turningpatientsandcarfulpositioningoflimbs
• Continuationofenteralfeeding,effectiveantacidsasomeprazole
• Preventingconstipation
• Preventandtreaturinaryretention.
Supportivetreatmentdirectedto:
1. Hypertension,hypotension
2. Cardiacarrhythmia
3. Pulmonaryembolism(Prophylaxisfordeepvenousthrombosisshouldbeprovidedbecausepatientsfrequentlyareimmobilizedformanyweeks).
4. Bladderandbowel
5. Psychologicalsupport
6. Nutrition,fluid,electrolytes
7. Pain
8. Skin
9. Cornea
10. Joints
11. Infection
12. communication
prognosis
� 40%→bedbound
� 15%→requireventilation
� 90-95%→completerecoverywithin6-12months
� Remainderambulatorywithminorresidualdeficit
� 4%→mortalityrate
• AntecedentsC.jujeniinfectioncorrelateswithpoorPx
Causesofdeath:
1. Autonomic(bradycardia,tachycardia,hypertension)
2. Respiratoryfailure
3. Pulmonaryembolism
4. Complicationofventilation
5. Cardiovascularcollapse
Chronicrelapsingorchronicunremitting(7%)
Featuressuggestiverelapsingare:
1. Severelyweak
2. Flaccidtetraplagia
3. Bulbarandrespiratorymuscleinvolvement
� Oneormorerelapsesover2mo.-years=CIDP
CongenitalGBS
� Weakness,areflexia,hypotonia.
� CSFandelectrophysicalstudiessuggestiveofGBS.
� Notreatment,gradualimprovement.
PoliomyelitisPolioviruses
• RNAviruses,Picornaviridaefamily,enterovirus
• 3geneticallydistinctserotypes
• SpreadfromintestinaltracttoCNS
• 90–95%inapperantinfections
• Transmission:humanistheonlyreservoir
• Fecal–oralroute
• Isolatedfromstoolfor2weeksbeforeparalysistoseveralweeksafteronsetofsymptoms
Pathogenesis
• Wildtypeandvaccinestrains
• GainhostentrythroughGIT
• Passtotheregionallymphnodes
• Goestothebloodcausingviremia
• WildtypeaccesstheCNSthroughperipheralnerves
• Incubationperiod8-12days
Clinical manifestions
Wildtypefollowoneofthefollowingcourses:
1. 90-95%inapparentinfection(nodisease&nosequelae
2. 5%inabortivedisease(influenza–likesyndrome1-2wkafterinfection,fever,malaise,anorexia,headache+/-vomiting)thenrecoverycomplete
3. Non-paralyticpoliomyelitis• 1%• Signsofabortivetype,fleetingparalysisofbladderandconstipation.• Thisisfirstphase(minor)thensymptoms-freeperiodthenmajorphase• O/E:nuchalrigidity,changesinthedeepandsuperficialreflexes
(impendingparalysis).Nosensorydefects4. Paralyticpoliomyelitis
• 0.1%• Spinaltype:majorphase,sensory(paresthesia,hypersthesia),motor(
fasiculationandspasms)progressto• Asymmetricparalysisofoneleg,then1arm• DTRinitiallyactivethendiminishedandabsent• Variablecourse:someprogress,somerecover
5. Bulbartype• +/-spinalcordinvolvement• Nasalvoiceorcry• Difficultyinswallowing• Accumulatedpharyngealsecretion• Absenceofeffectivecoughing• Nasalregurgitation• Deviationofpalate,uvula,tongue• Involvementofvitalcentersinthemedulla• Paralysisofvocalcords…hoarseness,aphonia• Sometimesculminateintoascendingparalysis(Landrytype)
6. polioencephalitis• Rare• Seizures,coma,spasticparalsysis,increasedreflexes• Respiratoryinsufficiency
7. Paralyticpoliowithrespiratoryinsufficiency• Anxiousexpression• Inabilitytospeakwithoutfrequentpauses• IncreasedRR• Movementofalanasi,accessorymuscles• Inabilitytocoughorsniff
• Paradoxicalabdominalmovement• Relativeimmobilityofintercostalspace
Diagnosis
• Shouldbeconsideredinanyunimmunizedorincompletelyimmunizedchildwithparalyticdisease
• Oranychildwithparalyticdiseaseoccurring7-14daysafterreceivingtheoralvaccine
• Stool:Isolatethevirusin2stoolspecimencollectedwith24–48hrapart
• Canisolatepoliovirusin80–90%inthefirstweekandlessthan20%within3-4wk
• CSF:normalinminordisease
• Cells20-200/mm3initiallythenreduced
• Protein:increasetoreach50-100mg/dlby2ndweek
• CSFserology:seroconversionor4foldsriseinantibodytiters
Treatment
• Nospecifictreatment
• Supportive:Limitprogression,preventskeletaldeformities,preparechildandfamilyforprolongedtreatment
Abortivepoliomyelitis
• Analgesics,sedatives
• Attractivediet
• Bedrestuntiltemperaturenormalize
• Avoidanceofexertionforensuing2wks
• Carefulneurologicandmusculoskeletalexamination
Nonparalyticpoliomyelitis
• Sameasabortive
• Reliefmuscletightness
• Analgesics
• Hotpacksfor15-30minevery2-4hr
• Hottubbaths
• Firmbed
• Footboardorsplinttokeepfeetatrightangletolegs
• Latergentlephysicaltherapy
Paralyticpoliomyelitis
• Hospitalization
• Physicalrest
• Suitablebodyalignmenttopreventdeformity
• Changepositionevery3-6hr
• Activeandpassivemovementindicatedaspaindisappear
• Moisthotpacks
• Opiatesandsedatives
• Treatconstipation
• Parasympatheticstimulantforbladderparalysis
• Adequatedietaryandfluidintake
• Orthopedist,physiatristshouldseethem
Bulbar
• Maintainairway
• Avoidriskofinhalation
• Gravitydrainageofaccumulatedsaliva
• Nursedinlateralorsemi-proneposition
• Aspiratorswithrigidtipsfororalpharyngealsecretionorflexiblecatheterfornasopharyngeal
• Fluidandelectrolytesequilibrium
• Bloodpressuretakenatleasttwice
• Impairedventilationsignsshouldbenoticedtodecidetracheostomy
Prognosis
• Inapparent,abortiveandasepticmeningitis=goodoutcome
• Paralytic=dependsontheextentandseverityofCNSinvolvement,recoveryphaselast6months
• Severebulbar=MR60%
• 30–40%ofpersonssurvivedparalyticpolio…mayexperiencemusclepainandexacerbationofexisitingweaknessafter30-40yr
Prevention
• Vaccination
• Hygienicmearures
Thank you
