absorption, distribution & excretion of toxicants
TRANSCRIPT

ABSORPTION, DISTRIBUTION
& EXCRETION OF TOXICANTS
D TA

2
D TA

3
D TA

I TOXICANT – RECEPTOR INTERACTIONS (T
+ R TR RESPONSE)
A. Examples of some cell receptors and targets:
1. Cellular enzymes (activate or inhibit activity)
2. Receptor present in cellular membranes (plasma
membrane, etc.)
3. Cellular macromolecules (DNA, RNA, tubulin, etc.)
D TA

B. Examples of Toxicant – Target Bonds [bond
strength (kcal/mole)]
1. Covalent (100) – sharing of electrons [irreversible
– uncommon]
2. Van der Waals (0.5) – weak electrostatic
attraction [common]- REV
3. Hydrogen (2-5) – stronger electrostatic attraction
[common]- REV
4. Ionic (5) – bond between oppositely charged
groups [common]- REV
D TA

C. Structure Activity Relationship (lock and key
interaction)
Cell Surface Receptor
1. Affinity
2. Efficacy
3. Agonist effect
4. Antagonist effect
5. Competitive versus Noncompetitive effects
D TA
• A. ADME are interrelated and toxic effect depends upon
ADME cycles – In most cases a toxicant’s effect is
proportional to the level of toxicant in blood since free
toxicant at the site of action (tissues) is in equilibrium with
free toxicant in the plasma. Therefore, a toxicant’s effect is
influenced by toxicokinetics or how this toxicant gets into
(absorption), around (distribution) and out of the body
(metabolism and excretion).
• It is important to understand that patient characteristics
such as age, tissue function (liver, kidney, etc.), living
habits (smoking, drinking, etc.) and nutrition can markedly
influence the pharmacokinetics of toxicants.
II ABSORPTION—DISTRIBUTION—METABOLISM—EXCRETION
D TA

1. The onset of a toxicant’s action occurs when thattoxicant’s level of concentration at the site of action(receptors) is adequate to initiate and maintain T-Rinteraction. (consider absorption and distribution)
2. Toxicant levels at receptor site are determined bythe amount of exposure to toxicant (dose) and itscapacity to reach the most relevant site of action(bioavailability)
(i) Route of administration regulates the toxicantdelivery rate – The intravascular and intramuscularroutes of administration are fastest while oralabsorption is considered slow
B. Overview of toxicokinetics
D TA
(ii) In general, metabolism of a toxicant
(liver) will decrease toxicant bioavailability.
The metabolism of biomolecules by liver
cells can activate or inactivate toxicity
(iii) Distribution of the toxicant regulates the
movement of the toxicant from the blood
to receptors. Toxicants can bind to tissue
sites after circulating in plasma (perhaps,
bound to plasma proteins)D TAD TA
(iv) Termination of toxic action occurs
when toxicant levels at the action site
fall below a minimum effective
concentration. Toxicants are excreted
by various tissues
D TA

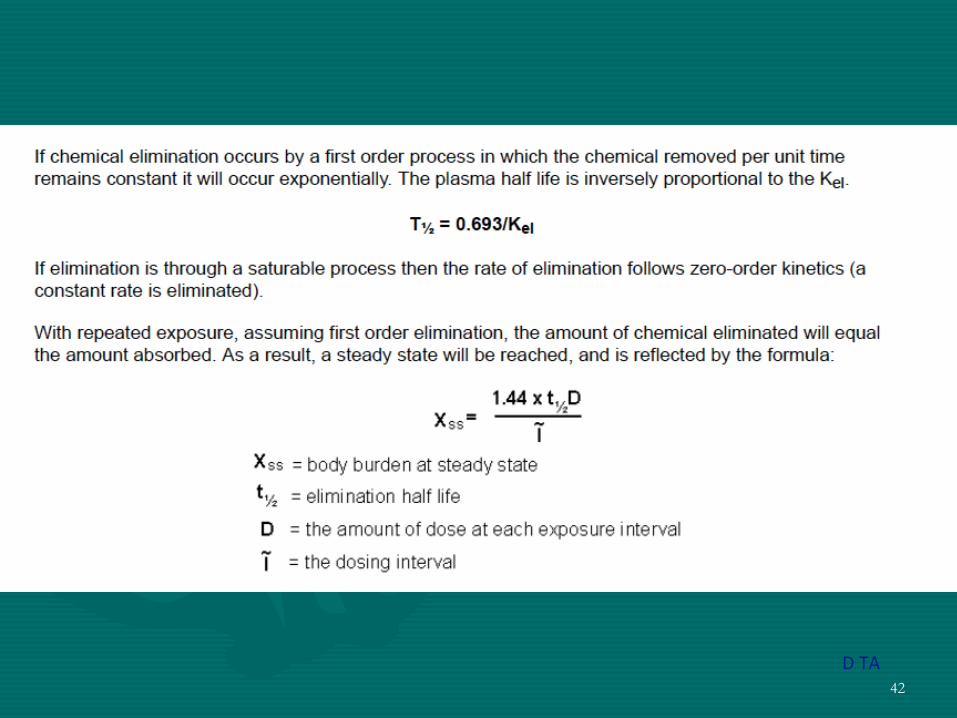
C. Expression of steady-state plasma level of repeatedly administered or repeat exposure toxicants
1. Css = F x D / CL x T
a. Css = steady-state plasma level (plateau)
b. F = bioavailability (% of drug absorbed)
c. D = dose
d. CL = clearance (elimination)
e. T = dose interval
D TA
D. A toxicant may pass through a membrane / barrier by:
1. Passive transport (diffusion according to Fick’s
Law) -no E req’d
a. Simple Diffusion – consider: hydrophobicity,
MW, ionization state
(i) Hendersen Hasselbalch
For acids: pKa – pH = log [nonionized]/[ionized]
For bases: pKa – pH = log [ionized]/[nonionized]
b. Filtration – relatively low MW (e.g., < 150- 300),
water soluble
D TA
2. Specialized transport – toxicant transported with E expenditure
a. active transport
(i) carrier mediates this
(ii) transport is dose dependent
(iii) competition for carrier is possible
b. protein binding may reduce toxicant transport
c. ionization remains a factor for toxicant transport
d. facilitated diffusion resembles active transport except that the toxicant moves with rather than against its conc. gradient
D TA
G. Absorption of Toxicants
1. Gastrointestinal Tract
a. mouth, esophagus, stomach, small intestines, large
intestines, rectum, common bile duct, portal blood
supply
b. absorption is a ‘dynamic’ process
(i) ionization state – note differing lumenal pH
through GI tract clinical management of poisoning;
pH change
(ii) anatomical factors – intestinal folds, villi,
microvilli can differ from individual to individual

(iii) GI carrier proteins – e.g., for iron, glucose,
purines or pyrimidines
(iv) lipid solubility and particle size
(v) modification by gut flora
(vi) liver enzyme transformations – P450 liver
enzymes differ from individual to individual;
P450 enzyme function can be induced or
inhibited
(vii) biliary addition / removal of molecules –
bile acid functions
D TA

2. Lungs – the uptake of inhaled toxicants dependsupon pulmonary perfusion and also onphysiochemical properties of the toxicant
a. nasopharyngeal and oral access routes to lungs,bronchi, broncheoli, alveoli, tissue differences perindividual, lung disease prior to toxicant exposure
b. absorption is a ‘dynamic’ process
(i) ionization state – although… less of an issue
(ii) anatomical factors
(iii) lung carrier proteins
(iv) plasma solubility and particle size – blood to gaspartition coefficient
(v) perfusion vs. ventilation rates as limiting factorsfor toxic effects
3. Skin – the rate limiting barrier in the dermal
absorption of chemicals is the epidermis.
Stratum corneum is most important layer.
a. absorption is a ‘dynamic’ process
(i) hydration of skin
(ii) anatomical factors
(iii) skin barrier proteins
(iv) plasma / lymph solubility and particle size
(v) ionization state of the toxicant

H. Distribution of Toxicant
1. Rate of distribution to organs or tissues is
determined by blood flow and the rate of
diffusion out of the capillary bed (key factors;
blood flow, affinity)
a. Volume of Distribution – three
compartments; plasma water, interstitial
water, and intracellular water
D TA

(i) Tissue binding
(ii) Lipid solubility
b. Tissue “Storage” of Toxicants – the depot release phenomena, the concept of primary distribution relative to redistribution
(i) Kidney / Liver
(ii) Bone
(iii) Fat
c. Barriers – blood / brain, blood / CSF, placental
I. Excretion of Toxicant – Urinary, Fecal, Expiratory
1. Urinary excretion: Renal glomerular filtration, Renal
tubule secretion and / or reabsorption processes
a. Glomerular filtration – considerations are rate
(GFR), bound or unbound toxicant particle size,
toxicant ionization state and lipid solubility,
presence or absence of renal disease
b. Renal tubular secretion / reabsorption – same
considerations as above with added consideration of
carrier proteins
D TA

2. Fecal Excretion – Toxicants ingested but not
absorbed, Biliary excretions
a. Nonabsorbed
b. Biliary excretions –
(i) liver enzyme biotransformations
(ii) lipophilicity
(iii) hepatocellular transport into bile
(iv) bound or unbound toxicant particle size and
ionization state
(v) age and health of the exposed individual
c. Intestinal excretions

22
D TA

23
D TA

24
D TA

25
D TA

26

27

28
D TA

29
D TA

30
D TA

31
D TA
32
It is apparent from the material presented in this chapter and the
previous chapters related to metabolism that the metabolism of
xenobiotics is complex, involving many enzymes; that it is susceptible to
a large number of modifying factors, both physiological and exogenous;
and that the toxicological implications of metabolism are important.
Despite the complexity, summary statements of considerable
importance can be abstracted:
- Phase I metabolism generally introduces a functional group into a
xenobiotic, which enables conjugation to an endogenous metabolite to
occur during phase II metabolism.
- The conjugates produced by phase II metabolism are considerably
more water soluble than either the parent compound or the phase I
metabolite(s) and hence are more excretable.
- During the course of metabolism, and particularly during phase I
reactions, reactive intermediates that are much more toxic than the
parent compound may be produced. Thus xenobiotic metabolism may
be either a detoxication or an activation process.

33
As organisms evolved in complexity, several
consequences of increased complexity
compromised the efficiency of the passive
diffusion of toxic chemicals:
1. They increased in size.
2. Their surface area to body mass decreased.
3. Their bodies compartmentalized (i.e., cells,
tissues, organs).
4. They generally increased in lipid content.
5. They developed barriers to the external
environment. D TA
34
Three major routes of elimination culminate in the
specialized organs of elimination, the liver, kidneys,
and lungs.
The liver serves as a major organ at which lipophilic
materials are collected from the blood,
biotransformed to generally less toxic and more
polar derivatives, then eliminated into the bile.
The kidneys complement the liver in that these
organs collect wastes and other chemicals in the
blood through a filtration process and eliminate
these wastes in the urine. D TA

35
The respiratory membranes of the lungs are ideal for the
removal of volatile materials from the blood into expired
air. In addition to these major routes of elimination, several
quantitatively minor routes exist through which toxic
materials can be eliminated from the body. These include
the following:
1. Skin. Skin constitutes the largest organ in the human
body, and it spans the interface between the body and the
external environment. While the skin’s epidermis
constitutes a relatively impervious membrane across which
chemical elimination is difficult, the shear surface area
involved requires consideration of this organ as a route of
elimination. Volatile chemicals are particularly adept at
traversing the skin and exiting the body through this route.

36
2. Sweat. Humans lose an average of 0.7 L of water per day
due to sweating. This loss of fluid provides a route for the
elimination of water-soluble chemicals.
3. Milk. Mother’s milk is rich in lipids and lipoproteins. Milk
thus serves as an ideal route for the elimination of both water-
soluble and fat-soluble chemicals from the mother’s body. For
example, the DDT metabolite DDE, the flame retardant mirex,
and the polychlorinated biphenyls (PCBs) often have been
detected in mother’s milk. While lactation may provide a benefit
to the mother by the elimination of toxic chemicals, transfer of
these toxicants to the suckling infant can have dire
consequences.
4. Hair. Growing hair can serve as a limited route through
which chemicals can escape the body. Pollutants such as mercury
and drugs such as cocaine have been measured in human hair,
and hair analyses is often used as a marker of exposure to such
materials.D TA
37

38
- Because the number of enzymes involved in phase I and phase
II reactions is large and many different sites on organic
molecules are susceptible to metabolic attack, the number of
potential metabolites and intermediates that can be derived from a
single substrate is frequently very large.
- Because both qualitative and quantitative differences exist
among species, strains individual organs, and cell types, a
particular toxicant may have different effects in different
circumstances.
- Because exogenous chemicals can be inducers and/or inhibitors
of the xenobiotic metabolizing enzymes of which they are
substrates; such chemicals may interact to bring about toxic
sequelae different from those that might be expected from any of
them administered alone.
D TA

39
- Because endogenous factors also affect the enzymes of
xenobiotic metabolism, the toxic sequelae to be expected
from a particular toxicant will vary with developmental
stage, nutritional statue, health or physiological status, stress
or environment.
- Most enzymes involved in xenobiotic metabolism occur
as several isozymes, which coexist within the same
individual and, frequently, within the same subcellular
organelle.
An understanding of the biochemistry and molecular
genetics of these isozymes may lead to an understanding of
the variation among species, individuals, organs, sexes,
developmental stages.D TA

40
D TA

41
D TA
42
D TA

43
D TA