a protocol to facilitate evar for ruptured aaa - ucsf … · 4/8/2011 1 a protocol to facilitate...
TRANSCRIPT

4/8/2011
1
A Protocol to Facilitate EVAR for Ruptured AAA
Manish Mehta MD MPHThe Vascular Group, Albany Medical Center
UCSF Vascular Symposium 2011
Research Grants/ Advisory Board/ Speaker/ honorarium:
WL Gore
Medtronic Ave
Cook Inc
Aptus
Trivascular
Cordis
Disclosures
UCSF Vascular Symposium 2011 UCSF Vascular Symposium 2011

4/8/2011
2
• Rupture AAA repair has evolved significantly
• EVAR for ruptured AAA
– Well documented and beyond feasibility
– Associated with significant reduction in morbidity & mortality
– Evolving to become the new ‘Gold Standard’
EVAR for Ruptured AAA EVAR for Ruptured AAA
• Limitations
– Availability of trained staff at all times
– Availability of equipment at all times
– The need for preoperative CT, particularly in hemodynamically unstable patients
– Surgeon bias and comfort level with EVAR under emergent circumstances
EVAR for Ruptured AAA
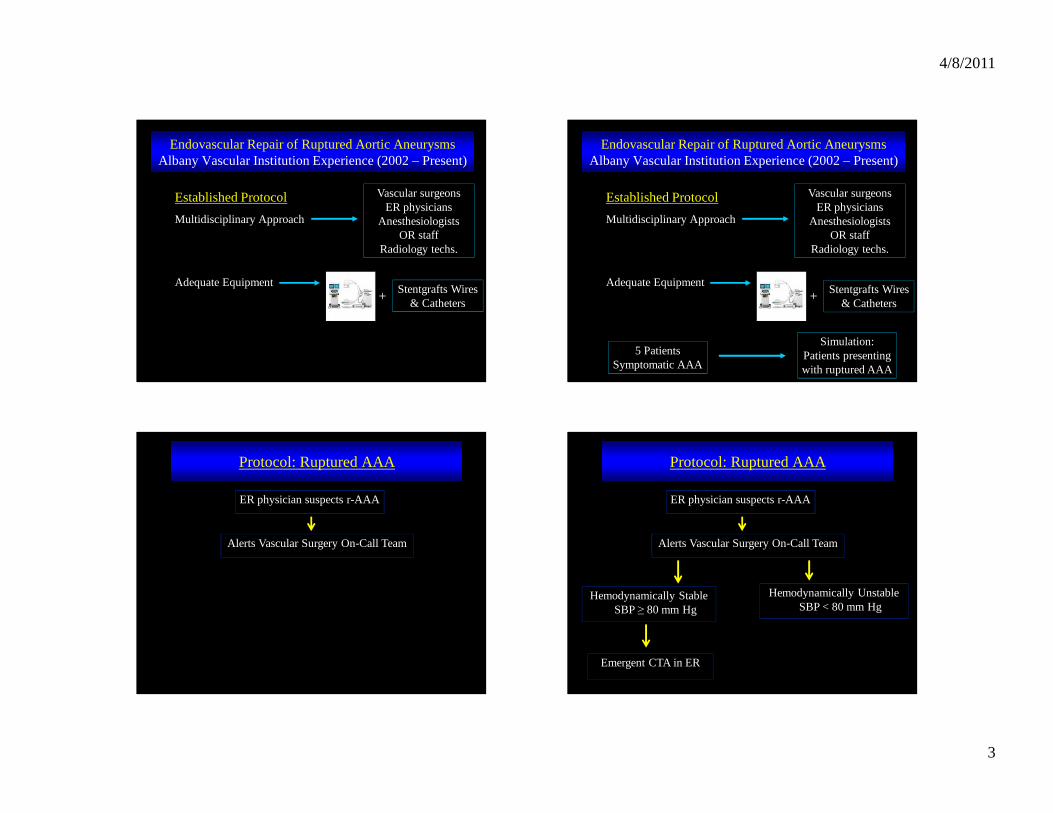
“Our first case”………2002Established Protocol
Multidisciplinary Approach
Endovascular Repair of Ruptured Aortic Aneurysms Albany Vascular Institution Experience (2002 – Present)
Vascular surgeons ER physicians
Anesthesiologists OR staff
Radiology techs.
4/8/2011
3
Established Protocol
Multidisciplinary Approach
Adequate Equipment
Endovascular Repair of Ruptured Aortic Aneurysms Albany Vascular Institution Experience (2002 – Present)
Vascular surgeons ER physicians
Anesthesiologists OR staff
Radiology techs.
+Stentgrafts Wires
& Catheters
Established Protocol
Multidisciplinary Approach
Adequate Equipment
Endovascular Repair of Ruptured Aortic Aneurysms Albany Vascular Institution Experience (2002 – Present)
5 Patients Symptomatic AAA
Simulation: Patients presenting with ruptured AAA
Vascular surgeons ER physicians
Anesthesiologists OR staff
Radiology techs.
+ Stentgrafts Wires & Catheters
ER physician suspects r-AAA
Protocol: Ruptured AAA
Alerts Vascular Surgery On-Call Team
ER physician suspects r-AAA
Protocol: Ruptured AAA
Alerts Vascular Surgery On-Call Team
Hemodynamically Stable SBP ≥ 80 mm Hg
Hemodynamically Unstable SBP < 80 mm Hg
Emergent CTA in ER

4/8/2011
4
ER physician suspects r-AAA
Protocol: Ruptured AAA
Alerts Vascular Surgery On-Call Team
Hemodynamically Stable SBP ≥ 80 mm Hg
Hemodynamically Unstable SBP < 80 mm Hg
Emergent CTA in EROR: Ready for EVAR and
Open Surgical Repair
‘Surgeon Bias’
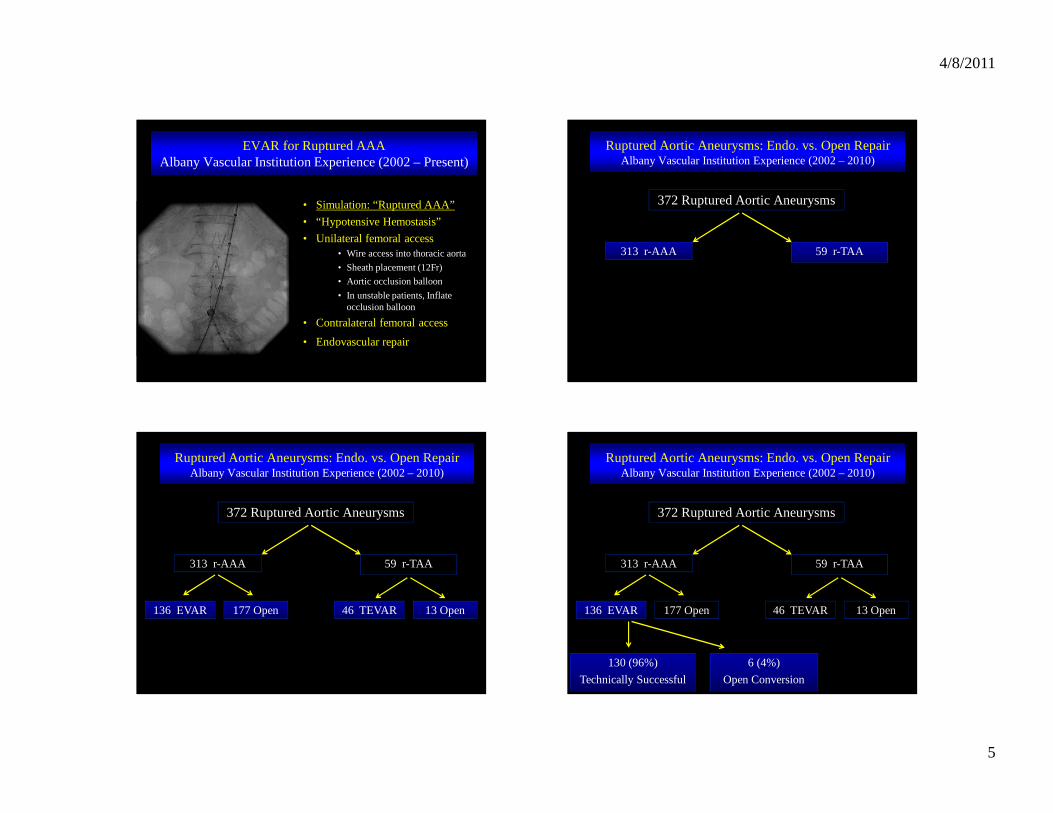
• Simulation: “Ruptured AAA”
• “Hypotensive Hemostasis”
• Unilateral femoral access• Wire access into thoracic aorta
• Sheath placement (12Fr)
• Aortic occlusion balloon
• In unstable patients, Inflate occlusion balloon
• Contralateral femoral access
• Endovascular repair
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – Present)
• Simulation: “Ruptured AAA”
• “Hypotensive Hemostasis”
• Unilateral femoral access• Wire access into thoracic aorta
• Sheath placement (12Fr)
• Aortic occlusion balloon
• In unstable patients, Inflate occlusion balloon
• Contralateral femoral access
• Endovascular repair
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – Present)
• Simulation: “Ruptured AAA”
• “Hypotensive Hemostasis”
• Unilateral femoral access• Wire access into thoracic aorta
• Sheath placement (12Fr)
• Aortic occlusion balloon
• In unstable patients, Inflate occlusion balloon
• Contralateral femoral access
• Endovascular repair
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – Present)
4/8/2011
5
• Simulation: “Ruptured AAA”
• “Hypotensive Hemostasis”
• Unilateral femoral access• Wire access into thoracic aorta
• Sheath placement (12Fr)
• Aortic occlusion balloon
• In unstable patients, Inflate occlusion balloon
• Contralateral femoral access
• Endovascular repair
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – Present)
Ruptured Aortic Aneurysms: Endo. vs. Open Repair Albany Vascular Institution Experience (2002 – 2010)
372 Ruptured Aortic Aneurysms
59 r-TAA313 r-AAA
Ruptured Aortic Aneurysms: Endo. vs. Open Repair Albany Vascular Institution Experience (2002 – 2010)
372 Ruptured Aortic Aneurysms
59 r-TAA313 r-AAA
46 TEVAR 13 Open136 EVAR 177 Open
Ruptured Aortic Aneurysms: Endo. vs. Open Repair Albany Vascular Institution Experience (2002 – 2010)
372 Ruptured Aortic Aneurysms
59 r-TAA313 r-AAA
46 TEVAR 13 Open136 EVAR 177 Open
130 (96%)
Technically Successful
6 (4%)
Open Conversion

4/8/2011
6
Ruptured AAA: Endovascular vs. Open Surgical Repair Albany Vascular Institution Experience (2002 – 2010)
Endo Open P-value
n 136 177
Male 71% 68% NS
Age (mean) 74 yrs. 73 yrs. NS
CAD 67% 44% <0.05
CRI 19% 8% <0.05
COPD 28% 12% <0.05
Ruptured AAA: Endovascular vs. Open Surgical Repair Albany Vascular Institution Experience (2002 – 2009)
Endo Open P-value
N 136 177
Preop. CT Available 80% 84% NS
Hemodynamically Unstable 25% 26% NS
Aortic Occlusion Balloon 20% N/A -
Aorto-uni-iliac & Fem-fem 16% N/A -
Blood Loss (mean) 464 cc 2791 cc <0.05
Operative Time (mean) 82 min 194 min <0.05
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)

4/8/2011
7
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
Wire-path along aortic neck:Gentle curve
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)

4/8/2011
8
Wire-path along aortic neck:Gentle curve
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
Wire-path along aortic neck:Gentle curve
Forward traction on stiff wire
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)

4/8/2011
9
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2010)
Ruptured AAA: Endovascular vs. Open Surgical Repair Albany Vascular Institution Experience (2002 – 2010)
Endo Open P-value
N 136 177
Myocardial Infarction 3% 16% <0.05
Ischemic Colitis (Grade 1-3) 6% 22% <0.05
ACS 16% 0 <0.05
Respiratory Failure 6% 9% NS
Renal Failure 5% 9% NS
Mean Hospital LOS (range) 11 (2-83) 17 (4-74) NS
• ACS: Abdominal Compartment Syndrome

4/8/2011
10
Ruptured AAA: Endovascular vs. Open Surgical Repair Albany Vascular Institution Experience (2002 –2009)
Endo Open P-value
N 136 177
Overall Mortality 16% 42% <0.01
EVAR for Ruptured AAA Albany Vascular Institution Experience (2002 – 2009)
N 136
Overall Mortality (EVAR r-AAA) 16% (22/136)
Mortality without ACS 9% (11/117)
Mortality with ACS 53% (10/19)P<0.05
ACS No ACS P-value
N 11 53
Operative Time (mean) 75 min 85 min NS
Aortic Occlusion Balloon 8 (73%) 3 (6%) < 0.01
Blood Transfusion 8 Units 2 Units < 0.01
aPTT 128 sec 52 sec < 0.01
Death 6 (55%) 4 (8%) < 0.05
EVAR for Ruptured AAAAbdominal Compartment Syndrome, Subset Analysis*
Mehta et al. JVS 2005
Endovascular Repair of Ruptured AAA
0
20
40
60
80
100
2002 2003 2004 2005 2006 2007 2008 2009 2010
%
13%
>75%

4/8/2011
11
0
20
40
60
80
100
2002 2003 2004 2005 2006 2007 2008 2009 2010
%
EVAR
Open Surgical
All Ruptured AAA52%
22%
EVAR and Open Repair of Ruptured AAA Operative Mortality
0
20
40
60
80
100
1 mo 1 yr 2 yr 3 yr 4 yr 5 yr
EVAR r-AAA Open r-AAA
Ruptured AAA: Endovascular vs. Open Surgical Repair Cumulative Survival
%
EVAR 102 64 43 22 12 7
Open 72 57 39 16 11 5@ Risk
P<0.05
• With standardized team approach, hemodynamically stable and unstable patients can be treated by endovascular means
• Preoperative CT scan is not an absolute necessity
• Single center experiences indicate EVAR for r-AAA has a significant midterm survival advantage when compared to open repair.
• With increasing experience, expanding the device IFU may increase the utility of EVAR in r-AAA patients
Take Home Message!
Movie