a molecular signature in blood identifies early parkinson’s disease
TRANSCRIPT

BT-309 SEMINAR, TERM PAPER WRITING
PRESENTED BY
Archana S. Puranik
ROLL NO :- 21

A molecular signature in blood identifies early Parkinson’s disease
• Authors:- Leonid Molochnikov,Jose Rabey, EvgenyaDobronevsky, Ubaldo Bonuccelli,Roberto Ceravolo, Dniela Frosini ,Edna Grunblatt, Peter Riederer,Christian Jacob, Judith Aharon-Peretz, Yulia Bashenko, MoussaBH Youdim and Silvia A Mandel
• Journal:- Molecular Neurodegenration
• Volume :- 7
• Impact Factor :- 5.29
• Citation index :- 2892

Purpose of this paper
1. Parkinson’s disease is verycommon to old people acrossworld.
2. The gradual neuro degenerationresults in shivering of handswhich is also a key symptom ofdisease.
3. This makes hurdle in performingdaily activities which might hurtself respect of individual.
4. With this paper an earlydetection may improveindividual’s health andappearance .
3

AbstractThe aim of the experiment is toassess whether a gene from bloodcould support detection of early PD.The transcriptional expression ofseven genes were examined from62 early ages PD patients and 64healthy matched control. Stepwiseregression analysis found that fivegenes are optimal those areSKP1,HIP2,ALDH1A1,PSMC4 andHSP8. The performance of thesegene on de novo PD individualsresulted in similar ROC and AUC of0.95 indicating stability of model.
4

Methods
1) Study population.• 185 individuals were enrolled
for blood sample mRNAextraction:
• 62 early/mild PD patients.• Early 24 patients within 1st
year of medication.• 30 PD patients with advanced
disease.• 29 patients with AD are
examined along with 64healthy matched control.
• Patient data such as name,age, gender is maintained.
5

Methods
• Total white blood count as well asdifferential blood cell counts wereexamined for any bias in geneexpression changes.
6

Methods2) Isolation of total RNA and quality control.
• Venous blood samples werecollected using PAXgene BloodRNA System Tubs at differentcenters and sent for RNAextraction and real time PCRquantification except 10 ADsamples. The blood samples werefrozen at -80 degrees.
• Both control and cases sampleswere processed in parallel. TotalRNA was extracted from wholeblood with PAXgene blood RNA50 kit.
7

Methods
• RNA quality was determined bynano drop 1000spectrophotometer and by usingautomated electrophoresissystem. And RNA samples weretaken from it.
8

Methods
3) Quantitative real-time RT-PCR(QRT-PCR).
• RNA from each blood sample isconverted to cDNA employing theHigh-Capacity cDNA ReverseTranscription Kit.
• QRT-PCR was performed using SYBRGreen detection.
• Oligonucleotide primers areconstructed accordingly.
• Gene expression were analysed .
9

Methods4) Building a risk marker profile.
• The predictive probability toestablish a molecular marker wascalculated by using regressionanalysis.
• The predictive probability valueswere used to construct a ROCcurve depicting the relationshipbetween sensitivity andspecificity of early PD groupversus de novo PD group.
10

Methods
5) Statistical analysis .
• Comparison between experimentalgroups were carried out usingANOVA technique.
11

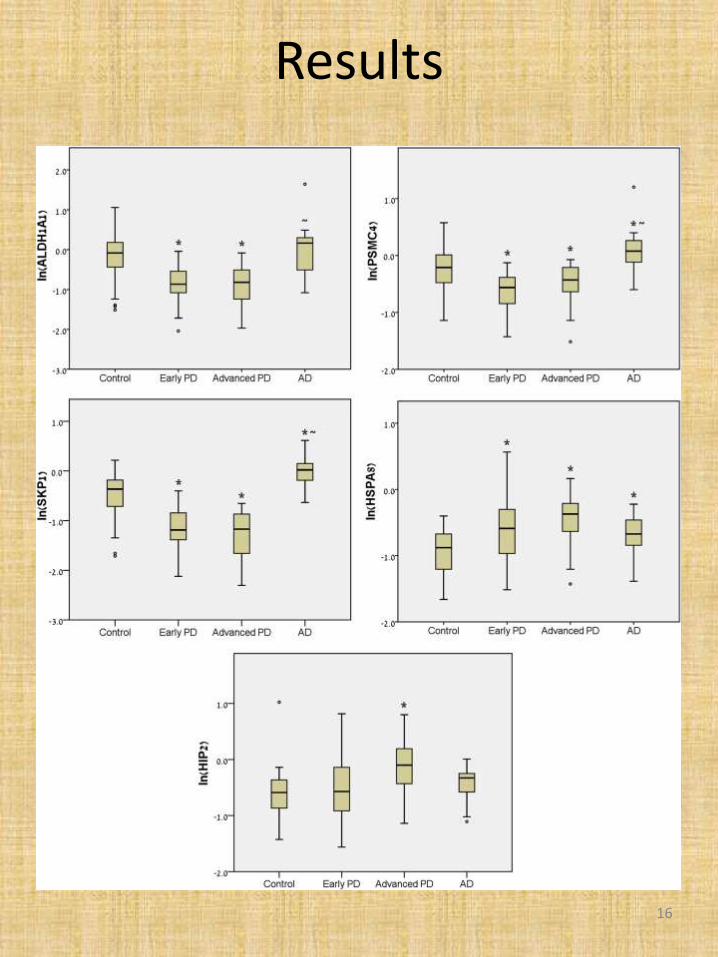
Results1) Identification of a PD risk genesignature.
Table 1 Variables in the predictedprobability equation
12
B Pvalue
OR 95%
LOW
C.I.ORUP
L_SKP1 -0.313 0.003 0.731 0.595 0.898
L_HIP2 0.274 0.008 1.315 1.076 1.608
L_ALDHA1
-0.148 0.030 0.862 0.754 0.986
L_PSMC4 -0.318 0.002 0.727 0.595 0.889
L_HSPA8 0.330 0.001 1.391 1.139 1.699

Results
13

Results2)Validation of specificity andsensitivity of the gene risk panel.
• To validate the diagnostic value ofthe PD gene panel, a separate 30PD patients at advanced diseasestage and 29 patients withAlzheimer’s disease (AD) weretested with the logisticclassification model.
• The gene cluster positivelyclassified all 30 cases as PD (100%sensitivity) and discriminated PDfrom AD with 100% specificity (all29 cases were classified as non-PD), thus supporting thediagnostic value of the molecularsignature for detecting PD.
14

Results
15
Results
16
Conclusions
• Experimental studiesdemonstrated that the bloodgene model has strong predictivevalue for PD diagnosis andpossibly may help to identifyindividuals at early stages whoare good candidates forneuroprotective treatment.
17
Conclusions
• Large-scale, prospective,controlled studies, whichcombine our methodology withquantification of CSFtotal/oligomers of α-synucleinor/and DJ-1 and brain imagingmay be useful as a multi-modalbiomarker, not only for earlydiagnosis but for evaluation ofdisease progression.
18

References• 1. Hughes AJ, Daniel SE, Kilford L, Lees AJ: Accuracy of clinical diagnosis of
• idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases.
• J Neurol Neurosurg Psychiatry 1992, 55:181–184.
• 2. Fahn S, Elton R, UPDRS Development Committee: Unified Parkinson’s
• disease rating scale. In In Recent Developments in Parkinson’s Disease.
• Volume 2. Edited by Fahn S, Marsden CD, Goldstein M. New York: Macmillan;
• 1987:153–167.
• 3. Rabey JM, Bass H, Bonuccelli U, Brooks D, Klotz P, Korczyn AD, Kraus P,
• Martinez-Martin P, Morrish P, Van Sauten W, Van Hilten B: Evaluation of the
• Short Parkinson’s Evaluation Scale: a new friendly scale for the
• evaluation of Parkinson’s disease in clinical drug trials. Clin
• Neuropharmacol 1997, 20:322–337.
• 4. Marinus J, Visser M, Stiggelbout AM, Rabey JM, Martinez-Martin P, Bonuccelli
• U, Kraus PH, van Hilten JJ: A short scale for the assessment of motor
• impairments and disabilities in Parkinson’s disease: the SPES/SCOPA.
• J Neurol Neurosurg Psychiatry 2004, 75:388–395.
• 5. Hoehn MM, Yahr MD: Parkinsonism: onset, progression and mortality.
• Neurology 1967, 17:427–442.
• 6. Hughes AJ, Ben-Shlomo Y, Daniel SE, Lees AJ: What features improve the
• accuracy of clinical diagnosis in Parkinson’s disease: a clinicopathologic
• study. Neurology 1992, 42:1142–1146.
• 7. Yekhlef F, Ballan G, Macia F, Delmer O, Sourgen C, Tison F: Routine MRI for
• the differential diagnosis of Parkinson’s disease, MSA, PSP, and CBD.
• J Neural Transm 2003, 110:151–169.
• 8. Davie CA, Wenning GK, Barker GJ, Tofts PS, Kendall BE, Quinn N, McDonald
• WI, Marsden CD, Miller DH: Differentiation of multiple system atrophy
• from idiopathic Parkinson’s disease using proton magnetic resonance
• spectroscopy. Ann Neurol 1995, 37:204–210.
• 9. Barbiroli B, Martinelli P, Patuelli A, Lodi R, Iotti S, Cortelli P, Montagna P:
• Phosphorus magnetic resonance spectroscopy in multiple system
• atrophy and Parkinson’s disease. Mov Disord 1999, 14:430–435.
• 10. Jankovic J, Rajput AH, McDermott MP, Perl DP: The evolution of diagnosis in
• early Parkinson disease. Parkinson Study Group. Arch Neurol 2000, 57:369–372
19

20

THANK YOU
21