2020 symposia series 1 - practicing clinicians
TRANSCRIPT

2020 Symposia Series 1

Managing the Spectrum of Psoriatic Disease in Primary Care

3
• Implement screening for CV disease, metabolic syndrome, and psoriatic
arthritis (PsA) in patients with psoriasis
• Identify side effects of drug classes used in the treatment of psoriatic
disease
• Apply long-term management strategies for patients with psoriasis in
coordination with a specialist
Learning Objectives
CV = cardiovascular.

4
Clinical Burden of Psoriatic Disease in the United States
• Chronic, multisystem inflammatory disorder
• Affects >8 million individuals
– 10% to 30% develop PsA
• Symptoms usually develop by 15 to 25 years of age but can occur at any time
• ~25% of patients have moderate to severe disease
– Extensive involvement on hands, feet, scalp, or genitals
• Negatively affects QoL, productivity, daily function
• Risk factors include smoking, obesity, stress, genetics
QoL = quality of life.
Mayo Clinic. www.mayoclinic.org/diseases-conditions/psoriasis/symptoms-causes/syc-20355840?p=1. Accessed April 21, 2020; Menter A, et al.
J Am Acad Dermatol. 2019;80:1029-1072; National Psoriasis Foundation. www.psoriasis.org/content/statistics. Accessed April 21, 2020.

5
Plaque Psoriasis: Disease Characteristics
Differential Diagnosis
• Eczema
• Combined
eczema/psoriasis
• Mycosis fungoides
• Plaque-stage cutaneous
T-cell lymphoma
• Tinea corporis
• Bowen disease
• Subacute cutaneous lupus
erythematosus
• 80% to 90% of patients with psoriasis have
plaque psoriasis
‒ Irregularly shaped, dry, thin plaques with
silvery-white scaling
‒ Tend to appear symmetrically
‒ Often found on scalp, trunk, buttocks,
or limbs
• Epidermal hyperproliferation
‒ Clinically evident as raised, inflamed,
scaly red skin lesions; cracking, itching
‒ Typically affects elbows, knees, scalp,
but can appear anywhere
Crow JM. Nature. 2012;492:S50-S51; Menter A, et al. J Am Acad Dermatol. 2008;58:826-850.

6
Plaque Psoriasis: Clinical Photos
Photos courtesy of Kristina Callis Duffin, MD.

7
Plaque Psoriasis: Clinical Photos (cont’d)
Photos courtesy of Veronica Richardson, MSN, ANP-BC, DCNP.

8
Guttate Psoriasis
Photo used with permission from Visual Dx (2005).
• Primarily affects young adults and children
• Usually triggered by a bacterial infection such as strep
throat
• Small, waterdrop-shaped, scaling lesions on trunk, arms,
legs, and scalp
• Lesions covered by a fine scale (not as thick as typical
plaques)
• Often misdiagnosed as a reaction to penicillin drugs just
given for strep infection
• Often resolves after strep infection resolves
• May portend future development of plaque psoriasis
Mayo Clinic. www.mayoclinic.org/diseases-conditions/psoriasis/symptoms-causes/syc-20355840?p=1. Accessed April 21, 2020.

9
AMP = antimicrobial peptide; DC = dendritic cell; IFN = interferon; KC = keratinocyte.
Arakawa A, et al. J Exp Med. 2015;212:2203-2212; Lande R, et al. Nat Commun. 2014;5:5621; Lowes MA, et al. Annu Rev Immunol. 2014;32:227-255.
Psoriatic Disease: Immunopathogenesis
Triggers
21Chronic diseaseEarly disease
KCs
+RNA
TLR7/9
Psoriasis 4
Amplification
feedback
Chemokines
AMPsT17
Th1, Tc1
Th22, Tc22
Neutrophils
IL-17A
IL-17F
IL-21
TNF
IFN-
TNF
IL-22
TNF
IL-23
IL-12
IFN-
LL37 (keratinocyte-derived)
ADAMTSL5 (melanocyte-derived)
+DNA/RNA
TLR7/8
IFN-/β
IL-12 IL-23
Myeloid DCs
T cells
a β/
CD4/CD8
3
TNF
Inflammatory
myeloid DCs
Mature dermal
DCs
Psoriasis

10
Physical and Mental Rankings of Psoriasis and Other Diseases
1
2
3
4
5
6
7
8
9
10
11
1
8
6
11
2
7
4
10
3
9
5
0 5 10 15 20
Healthy
Dermatitis
Cancer
Depression
Hypertension
Arthritis
Myocardial infarction
Chronic lung disease
Type 2 diabetes mellitus
Psoriasis
Heart failure
Physical rank Mental rank
Best Functioning (1) to Worst Functioning (11)
Van Voorhees AS, et al. www.psoriasis.org/sites/default/files/npf_pocketguide_2018_0010.pdf. Accessed April 28, 2020.
11
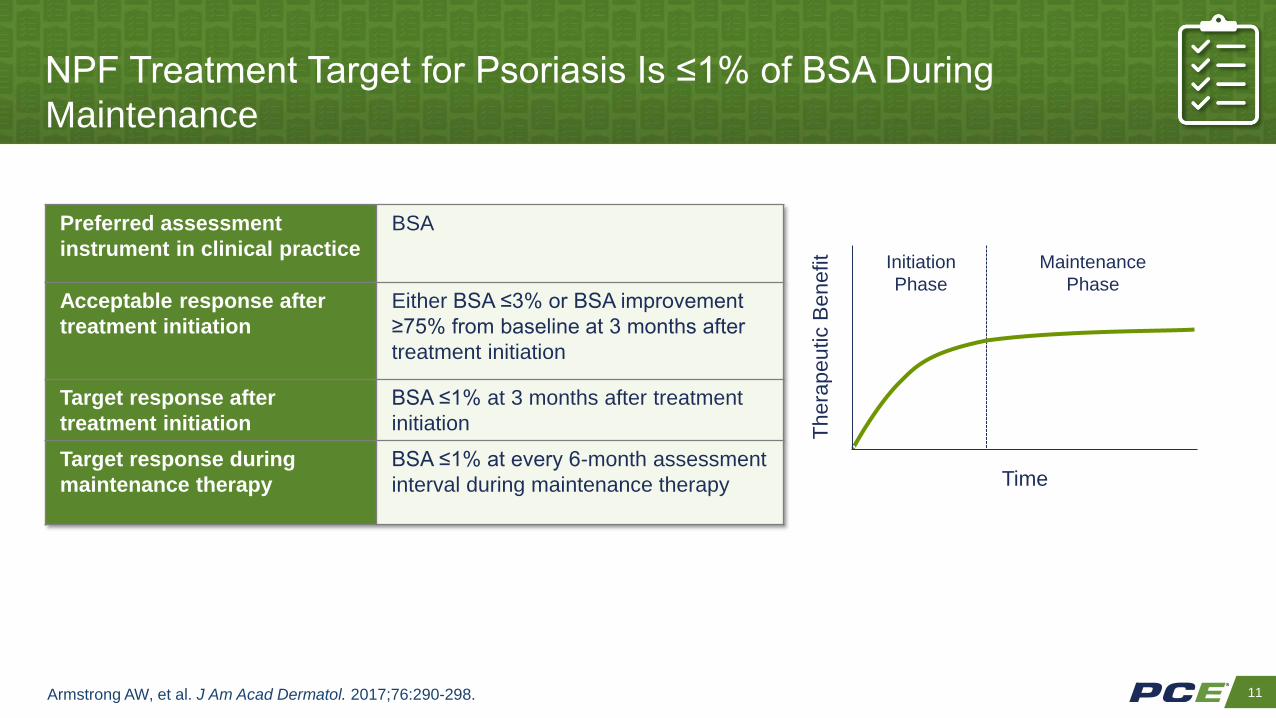
NPF Treatment Target for Psoriasis Is ≤1% of BSA During
Maintenance
Armstrong AW, et al. J Am Acad Dermatol. 2017;76:290-298.
The
rap
eu
tic B
en
efit
Time
Initiation
Phase
Maintenance
Phase
Preferred assessment
instrument in clinical practice
BSA
Acceptable response after
treatment initiation
Either BSA ≤3% or BSA improvement
≥75% from baseline at 3 months after
treatment initiation
Target response after
treatment initiation
BSA ≤1% at 3 months after treatment
initiation
Target response during
maintenance therapy
BSA ≤1% at every 6-month assessment
interval during maintenance therapy

12
Case Study: Lori, a 31-Year-Old Music Teacher With
Scalp Psoriasis
• 6-year history of psoriasis, primarily on the scalp, for which
she has been applying an OTC anti-dandruff shampoo
• Family history of multiple sclerosis
• Mild depression treated with SSRI
• Currently taking an oral contraceptive
• New concerns
‒ Worsening itching and flaking of scalp behind her ears
• Strategically covers these areas with her hairstyle
• Visits a friend for haircuts; too embarrassed to go to
salon
SSRI = selective serotonin reuptake inhibitor.

13
Calculating Extent of Psoriasis
Menter A, et al. J Am Acad Dermatol. 2019;80:1029-1072; Van Voorhees AS, et al. www.psoriasis.org/sites/default/files/npf_pocketguide_2018_0010.pdf.
Accessed May 23, 2019.
• May also be considered severe if it:
– Involves the hands, feet, scalp, face,
or genitals
– Causes intractable pruritus
– Has significant impact on QoL
• Such an impact may justify use of
systemic therapy

14
• Create a partnership based on trust to foster open dialogue about impact
of psoriasis and treatment goals
• Treatment selection should reflect patient’s answers to questions such as:
‒ How does psoriasis affect your daily living, including function, sleep,
socializing, productivity, intimacy?
‒ What are your symptoms (eg, pain, itching, burning, dry skin), and what
are all the areas of your body affected?
‒ What has been your experience with previous treatments?
‒ What do you hope treatment will accomplish?
Assess the Patient’s Experience With Psoriatic Disease
Aldredge LM, Higham RC. J Dermatol Nurses Assoc. 2018;10:189-197; American Academy of Dermatology. www.aad.org/education/basic-derm-
curriculum/suggested-order-of-modules/psoriasis. Accessed May 23, 2019; Van Voorhees AS, et al.
www.psoriasis.org/sites/default/files/npf_pocketguide_2018_0010.pdf. Accessed April 28, 2020.

15Armstrong AW, et al. Dermatol Ther (Heidelb). 2017;7:97-109.
42%
3%
32%
22%
Types of Treatment in Year Prior to September 2012
Topical
Phototherapy
Traditional oral systemic
Biologic
Most Patients With Moderate to Severe Psoriasis
Are Undertreated or Untreated
• Data from US National Health and
Wellness Survey and insurance
claims, 2007 to 2012
− 1.7 million insured US patients
with moderate to severe
psoriasis
• 59% had not been treated in
past year
• Of those treated in past year,
50% were no longer being
treated
17% of patients taking a
biologic were also taking a
traditional oral systemic

16
Patients With Psoriatic Disease Are Dissatisfied With
Their Current Treatment: MAPP Survey
AEs/abnormal laboratory tests
Injection anxiety/fear
43.750
40
30
20
10
0
Pa
tie
nts
(%
)
16.4
7.0 6.33.9
17.8
25.6
13.310.0
13.3
Conventional Oral Therapy (n = 128) Biologic Therapy (n = 90)
Injection physical preparation
Pain/discomfort
Inconvenience
AEs/abnormal laboratory tests
Laboratory monitoring
Lifestyle modification
Lack/loss of effectiveness
Inconvenience
AE = adverse event; MAPP = Multinational Assessment of Psoriasis and Psoriatic Arthritis.
Lebwohl MG, et al. Am J Clin Dermatol. 2016;17:87-97.
50
40
30
20
10
0
Pa
tie
nts
(%
)

17
Case Study (cont’d): Lori’s Physical Exam and Lab Findings
A1C = glycated hemoglobin; FPG = fasting plasma glucose; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein
cholesterol; TC = total cholesterol; TG = triglycerides.
• Physical examination
– Height: 5 ft 4 in
– Weight: 179 lb
– BMI: 30.7 kg/m2
– Waist circumference: 35.5 in
– Blood pressure: 141/91 mm Hg
• Laboratory findings
– FPG: 121 mg/dL
– A1C: 6.3%
– Lipids:
• TC: 215 mg/dL
• LDL-C: 128 mg/dL
• HDL-C: 47 mg/dL
• TG: 260 mg/dL

18
Psoriatic Disease: Comprehensive, Collaborative,
Patient-Centered Care
Patient
Dermatologist
Topicals, systemic therapy,
biologics, refractory disease
Primary Care
Overall evaluation and
management; comorbidities,
vaccines, monitoring, education
Behavioral HealthCounseling
Pharmacist
Medication management
Rheumatologist
PsA, imaging

19
TNF-α
IFN-
IFN-α
IL-1
IL-6
IL-7
Psoriatic Disease and Atherosclerosis: Shared
Inflammatory Mediators
CRP = C-reactive protein; IFN = interferon; MCP-1 = monocyte chemotactic protein-1.
Adapted from: Gisondi P, Girolomoni G. Semin Thromb Hemostat. 2009;35:313-324.
Hugh J, et al. J Am Acad Dermatol. 2014;70:168-177.
CRP
Fibrinogen
LDL-C
TG
Leptin
Resistin
MCP-1
Insulin resistance
From endothelial dysfunction
to atherosclerosis
Psoriatic disease inflammation
Common link
Increased activity
of inflammatory
mediators
Future researchTherapies for psoriasis associated with fewer CV events
among patients with psoriasis; further long-term study needed
Liver
Skeletal
muscle
Adipose
tissue
Skin keratinocytes
+
Inflammatory cells

20
Clinical significance
• Increased risk of MI, stroke, CV death, T2DM, CKD
• 5 years of life lost
• 10-year risk of major CV event attributable to
psoriasis is 6%
• 30x more likely to experience MACE (attributable
to psoriasis) than to develop a melanoma
• ACC/AHA now considers psoriasis to be an
ASCVD risk enhancer
Risk of Cardiometabolic Disease in Patients With Severe Psoriasis
CKD = chronic kidney disease; MACE = major adverse cardiovascular events;
MI = myocardial infarction; NS = not significant; PsO = psoriasis; RR = relative risk.
Gelfand JM et al. JAMA. 2006;296:1735-1741. Gelfand JM et al. J Invest Dermatol.
2009;129:2411-2418. Mehta NN et al. Eur Heart J. 2010;31:1000-1006. Mehta NN et al.
Am J Med. 2011;124:775.e1-6. Azfar RS et al. Arch Dermatol. 2012;148:995-1000.
Wan J et al. BMJ. 2013;347:f5961; Arnett DK, et al. Circulation. 2019;140:e596-e646.
Slide courtesy of Joel M. Gelfand, MD
Outcome Mild PsO Severe PsO
MI 1.05 1.5
Stroke 1.06 1.4
CV Death Not done 1.6
MACE Not done 1.5
Diabetes 1.11 1.5
CKD 0.99 (NS) 1.9
Mortality Curve
Pe
rcen
t o
f S
ub
jects
Age
020
1
2
3
4
40 60 80 100
Psoriasis
Controls
Adjusted RR

21
Even Young Adults With Psoriatic Disease Are at
Increased Risk for CV Events
*Hypertension, diabetes, history of myocardial infarction, hyperlipidemia, age, sex, smoking, BMI.
Gelfand JM, et al. JAMA. 2006;296:1735-1741; National Psoriasis Foundation. www.psoriasis.org/about-psoriasis/living-well/reducing-your-risk-for-
comorbidities. Accessed April 28, 2020; Osto E, et al. Atherosclerosis. 2012;221:113-117; Pearson TA, et al. Circulation. 2002;106:388-391.
Age (Years) Mild Psoriasis Severe Psoriasis
30 1.29 3.10
60 1.08 1.36
• Young adults with psoriasis have early microvascular impairments
– Coronary flow reserve lower in young patients with psoriasis than in controls
– The lower the coronary flow reserve, the higher the PASI
• Risk factor screening recommended as early as age 20 years
Relative Risk of MI Among Patients With Psoriasis, Adjusted for Major CV Risk Factors*

22
Joint AAD-NPF Guidelines 2019: Psoriasis and CV Disease
Comorbidity Screening Recommendations
Recommendation SOR
2.1 CV risk assessment (screening for hypertension, diabetes, and
hyperlipidemia) with national guidelines is recommended for all patients
with psoriasis
B
2.2 Clinicians should consider early and more frequent screening for
hypertension, diabetes, and hyperlipidemia in psoriasis patients who are
candidates for systemic or phototherapy or who have psoriasis involving
>10% of BSA
B
Recommendation key: A = based on consistent and good quality patient-oriented evidence; B = based on inconsistent or limited-quality patient-
oriented evidence; based on consensus, opinion, case studies, or disease-oriented evidence.
SOR = strength of recommendation
Elmets CA, et al. J Am Acad Dermatol. 2019;80:1073-1113.

23
Additional Comorbidities of Psoriatic Disease
• In addition to CVD, psoriatic
disease associated with
increased risk of a wide array of
other comorbidities
• Most recent joint AAD/NPF
guidelines comprise 2 sections:
– Treatment with biologics
– Management of comorbidities
Depression/anxiety
Autoimmune ophthalmic
disease
Obstructive sleep apnea
COPD
Hypertension
Kidney disease
Fatty liver disease
IBD
Diabetes/metabolic syndrome
Osteoporosis
IBD = inflammatory bowel disease.
Andersson AM, et al. Curr Derm Rep. 2017;6:129-136; Elmets CA, et al. J Am Acad Dermatol. 2019;80:1073-1113; Menter A, et al.
J Am Acad Dermatol. 2019;80:1029-1072; Shah K, et al. J Am Acad Dermatol. 2017;77:287-292.

24
Case Study: (cont’d): Next Steps in Lori’s Treatment
• You prescribe a nutritious diet, regular exercise, a statin, and HCTZ for
Lori’s cardiometabolic risk profile
• She believes that her depression is largely related to her worsening scalp
psoriasis and the discomfort and embarrassment it causes
• You recommend she continue her current SSRI and recommend cognitive
behavioral therapy with a psychologist
• You refer Lori to a dermatologist to discuss therapies to help improve her
psoriasis
‒ At her dermatology appointment, Lori says she would rather not take a
systemic agent because the potential side effects are concerning to her

25
Psoriasis Is Independently Associated With Risk of Depression
Max 20-Year
Follow-up
36,299 without psoriasis
developed depression
~250,000 matched
individuals without
psoriasis
247,755 patients with psoriasis >18 years old from Danish registries
220,721 with mild
disease (topicals)24,771 with moderate
disease (systemic
nonbiologics)
2,263 with severe
disease (biologics)
HR 1.19
(95% CI
1.17-1.20)
HR 1.19
(95% CI
1.15-1.23)
45,641 patients with psoriasis developed depression
HR 1.50
(95% CI
1.23-1.84)
CI = confidence interval; HR = hazard ratio.
Egeberg A, et al. Br J Dermatol. 2019;180:116-121.

26
• Solutions, foams, and sprays are preferred vehicles for corticosteroids to treat
scalp psoriasis
• Keratolytic agents (eg, coal tar, salicylic acid) available as shampoos, gel- or
oil-based compounded formulas
• Significant burning and erythema can occur with topical calcineurin inhibitor use
‒ Often used in sensitive areas (genitals, skin folds, face)
‒ Warning patients in advance can reduce premature cessation of treatment
‒ Treat patients with topical steroids for 5 days to “cool down” region before
introducing the calcineurin inhibitor
Topical Therapy for Scalp Psoriasis
Chan CS, et al. J Am Acad Derm. 2009; 60:962-971; Veronica Richardson. Personal communication.

27
Topical Nonsteroidal Agents for Psoriasis
Khosravi et.al. J Drugs Dermatol. 2017;16:760-766; Menter et. al. J Am Acad Dermatol.. 2009;60:643-59.
Calcineurin Inhibitors Vitamin D Analogs Keratolytics
• Tacrolimus 0.03%, 0.1% ointment
• Pimecrolimus 1% cream
• Calcipotriene 0.005%
• Calcitriol
• Salicylic acid
• Coal tar
• Retinoids
• Ammonium lactate
• Urea
Face/Genitals: burning and erythema
can occur. Consider pretreating for 3-5
days with topical steroids
Rotational
therapy/combine with
topical corticosteroids
Scalp: 10% Liquor Carbonis
Detergens with 2% salicylic acid in
oil, compounded for scalp
debridement therapy

28
Topical Corticosteroids for Psoriasis
Potency Examples Body Locations
• Class I super potent • Clobetasol/Halobetasol • Palms/soles, scalp,
elbows/knees
• Class II potent • Fluocinonide 0.05%
• Class III-V • Triamicinolone 0.1% • Extremities, torso
• Class VI-VII • Hydrocortisone 2.5%
• Desonide 0.05%
• Face, genitals, inverse
Considerations
• Body location
• Vehicle
Corticosteroids
Ference JD. Am Fam Physician. 2009;79:135.
• Cost/Coverage
• Quantity

29
Phototherapy for Psoriasis
• Decreased keratinocyte proliferation; anti-inflammatory
properties
• Narrowband UVB preferred over broadband UVB light
• Generally administered 3 times/week for ≥3 months; large
time commitment
• Side effect: With narrowband UVB, burns are more
severe, longer lasting than those with broadband UVB
• PUVA useful for palmoplantar psoriasis
PUVA = psoralen and ultraviolet A; UVB = ultraviolet B.
Kupetsky EA, Keller M. J Am Board Fam Med. 2013;26:787-801.
30
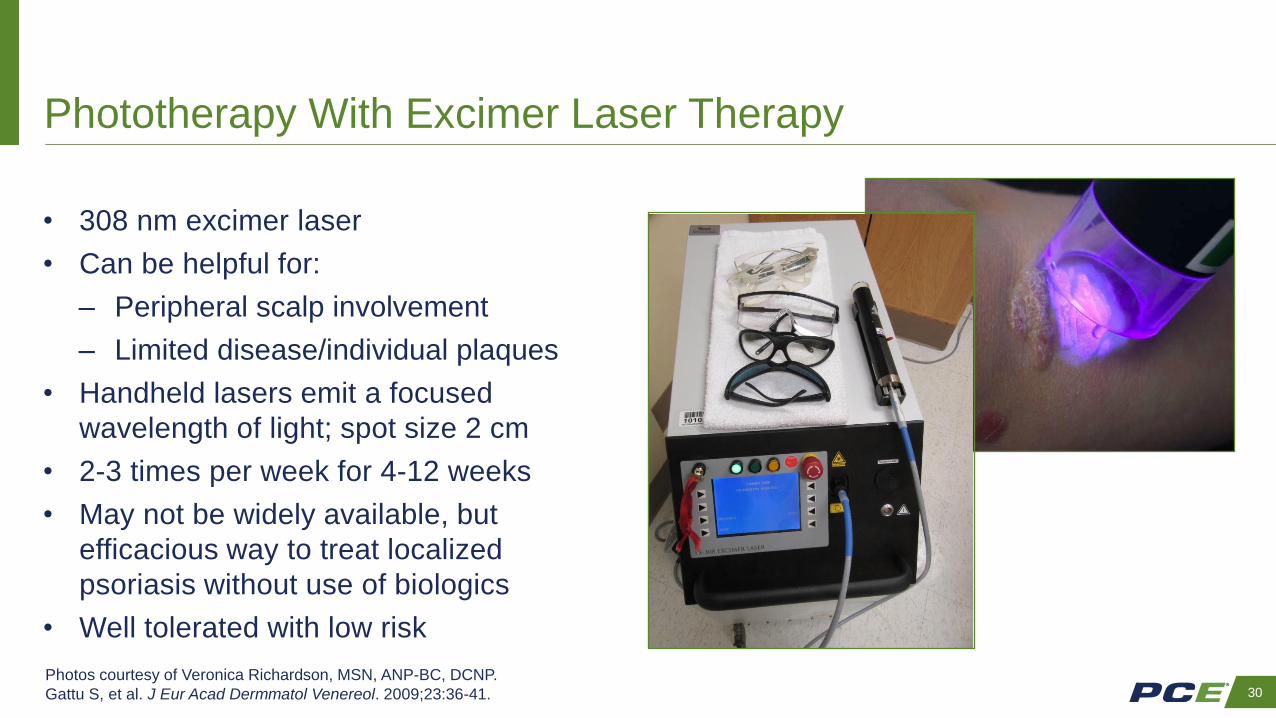
Phototherapy With Excimer Laser Therapy
• 308 nm excimer laser
• Can be helpful for:
‒ Peripheral scalp involvement
‒ Limited disease/individual plaques
• Handheld lasers emit a focused
wavelength of light; spot size 2 cm
• 2-3 times per week for 4-12 weeks
• May not be widely available, but
efficacious way to treat localized
psoriasis without use of biologics
• Well tolerated with low risk
Photos courtesy of Veronica Richardson, MSN, ANP-BC, DCNP.
Gattu S, et al. J Eur Acad Dermmatol Venereol. 2009;23:36-41.

31
Case Study (cont’d): Lori Returns to Her Dermatologist for
Follow-up 6 Months Later
• Even with aggressive scalp debridement, Lori’s scalp psoriasis is
recalcitrant and continues to cause her distress
• She reports her depression/anxiety is better controlled but notes:
‒ Recent plaque involvement of elbows and knees
‒ Hands a little stiff when she wakes up
• Lori considers phototherapy, but her schedule does not allow for the
frequent visits required, and her rural town has limited access to it
• She agrees to systemic therapy for her psoriasis
• She and her dermatologist select an IL-12/23 inhibitor because of its
efficacy, safety profile, and weight-based dosing

32
• UVB phototherapy (narrowband more effective
than broadband)
− UVB phototherapy alone
− UVB phototherapy + systemic retinoids
− UVB phototherapy + adjuvant topical agents
− UVB phototherapy + short-term isotretinoin, if
necessary
− Goeckerman therapy
If UVB phototherapy available, feasible, practical,
and suitable: FIRST LINE
If UVB phototherapy unavailable, contraindicated, or
ineffective or patient unable to comply: FIRST LINE
CsA = cyclosporine A; MTX = methotrexate.
Note: Risankizumab, a newer IL-23 inhibitor, was approved by the FDA after publication of this algorithm.
Skyrizi [prescribing information]. AbbVie; 2019; Van Voorhees AS, et al. www.psoriasis.org/sites/default/files/npf_pocketguide_2018_0010.pdf.
Accessed April 28, 2020.
• Adalimumab
• Apremilast
• Brodalumab
• Certolizumab pegol
• Cyclosporine
• Etanercept
• Guselkumab
• Infliximab
• Ixekizumab
• Methotrexate (MTX)
• PUVA
• Secukinumab
• Systemic retinoids
• Tildrakizumab
• Ustekinumab
SECOND LINE (Combination Therapies)
• MTX + CsA
• MTX + biologic
• Isotretinoin (short term, if necessary;
in conjunction with phototherapy)
• Systemic retinoid + biologic
• UVB + biologic
• Apremilast + UVB
NPF Algorithm for Women of Childbearing Potential Using Appropriate
Contraception With Chronic Plaque Psoriasis (>5% BSA), Without PsA

33
• UVB phototherapy (narrowband more effective
than broadband)
− UVB phototherapy alone
− UVB phototherapy + systemic retinoids
− UVB phototherapy + adjuvant topical agents
− UVB phototherapy + short-term isotretinoin, if
necessary
− Goeckerman therapy
If UVB phototherapy available, feasible, practical,
and suitable: FIRST LINE
If UVB phototherapy unavailable, contraindicated or
ineffective or patient unable to comply: FIRST LINE
CsA = cyclosporine A; MTX = methotrexate.
Note: Risankizumab, a newer IL-23 inhibitor, was approved by the FDA after publication of this algorithm.
Skyrizi [prescribing information]. AbbVie; 2019; Van Voorhees AS, et al. www.psoriasis.org/sites/default/files/npf_pocketguide_2018_0010.pdf.
Accessed April 28, 2020.
• Adalimumab
• Apremilast
• Brodalumab
• Certolizumab pegol
• Cyclosporine
• Etanercept
• Guselkumab
• Infliximab
• Ixekizumab
• Methotrexate (MTX)
• PUVA
• Secukinumab
• Systemic retinoids
• Tildrakizumab
• Ustekinumab
SECOND LINE (Combination Therapies)
• MTX + CsA
• MTX + biologic
• Isotretinoin (short term, if necessary;
in conjunction with phototherapy)
• Systemic retinoid + biologic
• UVB + biologic
• Apremilast + UVB
NPF Algorithm for Women of Childbearing Potential Using Appropriate
Contraception With Chronic Plaque Psoriasis (>5% BSA), Without PsA
WOMEN OF CHILDBEARING POTENTIAL SHOULD BE INFORMED ABOUT THE NEED TO ABSTAIN FROM
BECOMING PREGNANT AND REMAIN ON APPROPRIATE CONTRACEPTION FOR THE RECOMMENDED INTERVAL
AFTER THE DISCONTINUATION OF THESE MEDICATIONS.

34
Conventional Systemic Oral Therapies
for Moderate to Severe Psoriatic Disease
Kupetsky EA, Keller M. J Am Board Fam Med. 2013;26:787-801; Menter A, et al. J Am Acad Dermatol. 2009;61:451-485; Pang ML, et al. Expert
Opin Drug Metab Toxicol. 2008;4:953-964.
MTX Cyclosporine Acitretin
Widely prescribed for PsO; not FDA
approved for PsA but often used
Reserved for rescue therapy Often used with UV light; least effective as
monotherapy
PASI 75 achieved by 36% to 60% of
patients after 16 weeks
PASI 75 achieved by 50% to 70% of
patients after 8 to 16 weeks
Response takes 3 to 6 months; PASI 75 highly variable
For moderate or severe PsO; can be used
in combination with biologics
Use limited to 1 year; initial dosage:
3 mg/kg/day; usually divided in 2
doses
Dose-dependent efficacy; can be used with biologics
Single weekly dose: 15 mg; if needed,
titrate up to 25 mg; divided-dose schedule:
2.5 mg q12h x 3 doses
Retinoid; starting dosage 10-25 mg/d, increase q2wk
until xerosis appears
Key safety issues: hepatotoxicity, bone
marrow suppression, pneumonitis,
contraindicated in pregnancy (category X)
Key safety issues: renal
insufficiency, hypertension
Key safety issues: mucous membrane dryness,
↑ TG and liver function tests, contraindicated in
pregnancy (category X)

35
Newer Oral Therapies: Moderate to Severe Psoriatic Disease
PDE = phosphodiesterase.
Otezla [prescribing information]. Celgene; 2019; Xeljanz [prescribing information]. Pfizer; 2019.
*No boxed warning for apremilast, but warnings and precautions for diarrhea (especially in patients
≥65 years of age), nausea, vomiting, weight loss, and depression.
Indication(s) Recommended Dosage (adults) Boxed Warning
PDE-4 enzyme inhibitor
Apremilast PsO, PsA 5-day titration (10-30 mg), then 30 mg PO
twice/day
No*
Janus kinase (JAK) inhibitor
Tofacitinib PsA only 5 mg/day
Extended release: 11 mg/d
Serious infections, mortality,
malignancy, thrombosis

36
“Biologic agents, as monotherapy or
combined with other topical or
systemic medications, have a high
benefit-to-risk ratio, and because of
that, they are a welcome addition to
the armamentarium of psoriasis
management.”
– AAD/NPF Guidelines
Jabbar-Lopez ZK, et al. J Invest Dermatol. 2017;137:1646-1654; Menter A, et al. J Am Acad Dermatol. 2019;80:1029-1072; Sbidian E, et al.
Cochrane Database Syst Rev. 2017;12:Art. No. CD011535.
Biologic Therapies: Moderate to Severe Psoriasis
• Cochrane review
− 109 trials, N = 39,882
− Ranking of efficacy
• IL-17, IL-23, IL-12/23, TNF-ɑ inhibitors
• Small molecules
• Conventional systemic drugs
• Meta-analysis
− 41 trials, N = 20,561
− Biologics more effective than placebo or
MTX

37
*Risankizumab was not included in this review.
Sbidian E, et al. Cochrane Database Syst Rev. 2017;12:CD011535.
Cochrane Meta-analysis: Efficacy of Systemic Therapies
in Moderate to Severe Psoriasis
0
5
10
15
20
25
30
35
Rela
tive E
ffect vs P
lacebo
Risk Ratio for Achieving PASI 90*
PDE-4 JAK
TNF
IL 12/23
IL 17
IL 23
Conventional

38
Biologic Therapies: Moderate to Severe Psoriatic Disease
Armstrong A, et al. Dermatol Ther (Heidelb); 2017;7:97-109; Cimzia [prescribing information]. UCB Inc; 2018; Enbrel [prescribing information]. Amgen;
2017; Humira [prescribing information]. AbbVie; 2018; Remicade [prescribing information]. Janssen; 2013; Simponi [prescribing information]. Janssen;
2018; Stelara [prescribing information]. Janssen; 2014.
ANA = antinuclear antibody; LFT = liver function tests
Agent/Indication(s) Common (>5%) AEs Boxed
Warning
Cautions/Considerations
TNF-α Inhibitors
Adalimumab PsO, PsA Injection site reaction + ANA; elevated
alkaline phosphatase, cholesterol
Serious
infections,
malignancy
Demyelinating disease
Congestive Heart Failure
Inflammatory Bowel Disease
(Adalimumab, Infliximab)
Pregnancy (Certolizumab)
Etanercept PsO, PsA Injection site reaction + ANA
Infliximab PsO, PsA Infusion reactions + ANA; elevated
LFT; neutralizing antibodies
Certolizumab PsO, PsA URIs, rash, UTIs
IL-12/23 Inhibitor
Ustekinumab PsO, PsA None No Inflammatory Bowel Disease
39
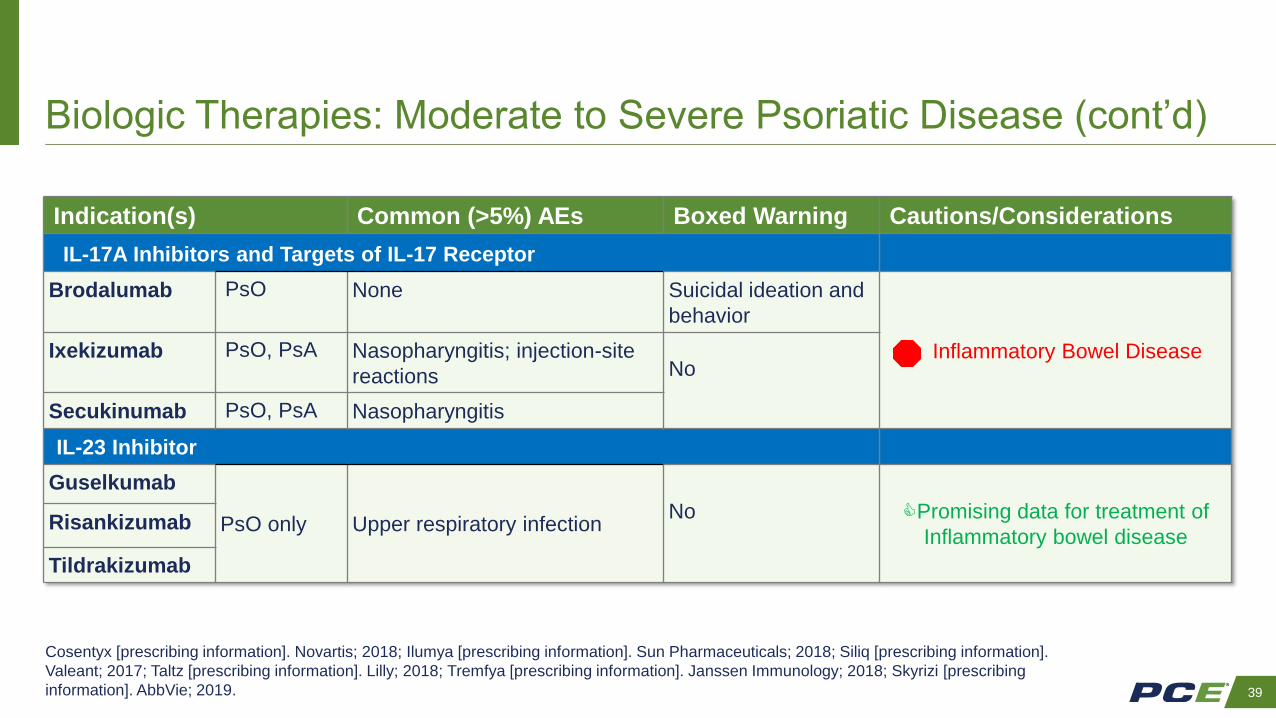
Biologic Therapies: Moderate to Severe Psoriatic Disease (cont’d)
Cosentyx [prescribing information]. Novartis; 2018; Ilumya [prescribing information]. Sun Pharmaceuticals; 2018; Siliq [prescribing information].
Valeant; 2017; Taltz [prescribing information]. Lilly; 2018; Tremfya [prescribing information]. Janssen Immunology; 2018; Skyrizi [prescribing
information]. AbbVie; 2019.
Indication(s) Common (>5%) AEs Boxed Warning Cautions/Considerations
IL-17A Inhibitors and Targets of IL-17 Receptor
Brodalumab PsO None Suicidal ideation and
behavior
Inflammatory Bowel DiseaseIxekizumab PsO, PsA Nasopharyngitis; injection-site
reactions No
Secukinumab PsO, PsA Nasopharyngitis
IL-23 Inhibitor
Guselkumab
PsO only Upper respiratory infectionNo Promising data for treatment of
Inflammatory bowel diseaseRisankizumab
Tildrakizumab

40
Long-term Efficacy of IL-17 and IL-12/23 Inhibitors: Patients With
Moderate to Severe Psoriasis Achieving PASI 90 at Week 52
76%
61%
0
20
40
60
80
Secukinumab Ustekinumab
Secukinumab vs Ustekinumab(N = 676)
76%
59%
0
20
40
60
80
Ixekizumab Ustekinumab
Ixekizumab vs Ustekinumab(N = 302)
P <0.0001P <0.01
Pa
tie
nts
(%
)
Pa
tie
nts
(%
)Blauvelt A, et al. J Am Acad Dermatol. 2017;76:60-69; Paul C, et al. J Am Acad Dermatol. 2019;80:70-79.

41
Impact of Biologics on QoL in Psoriasis
*12 studies; 12,240 participants; various QoL scales used; †Pooled analysis from 4 phase 3 trials; n = 309 secukinumab 300 mg, n = 282 placebo;
QoL measured with EuroQol 5-Dimensions (EQ-5D-3L) questionnaire.
Sbidian E, et al. Cochrane Database Systematic Rev. 2017;12. doi: 10.1002/14651858.CD011535.pub.2; Feldman SR, et al. Abstract presented at
Maui Derm for Dermatologists 2019; January 26-30, 2019, Maui, Hawaii.
Favors drug Favors placebo
Cochrane Database 2017 Meta-analysis* 2019 analysis: % patients reporting no problem with
domains below, secukinumab vs placebo, week 12†Drug
Ixekizumab
Guselkumab
Tildrakizumab
Ustekinumab
Etanercept
Tofacitinib
Adalimumab
Brodalumab
MTX
Apremilast
-2 -1 0 1
QoL
71%
87%83%
47% 43% 43%
0%
20%
40%
60%
80%
100%
Mobility Self care Usual Activities
Secukinumab Placebo
% P
atie
nts
Favors drug Favors placebo

42
Summary: Long-term Safety of Biologic Agents for Psoriatic Disease
• TNF inhibitors
‒ No long-term AEs noted beyond those identified in clinical trials
• IL-12/23 inhibitors
– No dose-related or cumulative toxicity with increasing duration of exposure
• IL-17A inhibitors
– No new safety signals with increasing duration of exposure
– IL-23 inhibitors (guselkumab, tildrakizumab-asmn, risankizumab-rzaa)
– Open-label extensions of phase 3 trials showed no new safety signals
Bilal J, et al. J Dermatolog Treat. 2018;29:569-578; Fagerli KM, et al. RMD Open. 2018;4:e000596; Griffiths CEM, et al. J Drugs Dermatol. 2018;17:826-
832; Reich K, et al. Lancet. 2017;390:276-288. Reich K, et al. Lancet. 2019;394:576-586.

43
Screening Before Starting a Biologic
HBV = hepatitis B virus; HCV = hepatitis C virus.
Lebwohl M, et al. J Am Acad Dermatol. 2008;58:94-105; Stelara [prescribing information]. Janssen; 2018; Taltz [prescribing information]. Lilly; 2018;
Wine-Lee L, et al. J Am Acad Dermatol. 2013;69:1003-1013.
• Assess immunization status or disease
history
‒ Haemophilus influenzae
‒ HBV, HCV, HIV
‒ Human papillomavirus
‒ Pertussis
‒ Tetanus
‒ Streptococcus pneumoniae
‒ Varicella zoster
• TB test
– Baseline
– Periodically

44
Live Vaccines to Be Avoided When Using Biologics
*Shingrix is an inactivated recombinant, adjuvanted (non-live) vaccine for herpes zoster.
Centers for Disease Control and Prevention. www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/B/us-vaccines.pdf. Accessed April 28, 2020.
• Adenovirus
• Cholera
• Herpes zoster (shingles) – Zostavax only*
• Live attenuated viral/intranasal spray for
influenza
• Measles, mumps, rubella or measles,
mumps, rubella, varicella
• Rotavirus
• Typhoid (live attenuated
bacterial oral)
• Varicella
• Vaccinia (smallpox)
• Yellow fever

45
Vaccinations for Patients Taking Biologic Therapy
for Psoriatic Disease
• Assess vaccination status before starting any biologic agent
• Live attenuated vaccines should be avoided for patients who are receiving
biologics
• Inactivated influenza and pneumococcal vaccines are strongly
recommended and are safe, but therapeutic response may be reduced
• If live vaccine is indicated, administer 4 weeks before starting therapy for
psoriatic disease
• Routine immunizations should be up to date before travel
Wine-Lee L, et al. J Am Acad Dermatol. 2013;69:1003-1013.

46
Case Study (cont’d): Lori Is Diagnosed With PsA
• At a follow-up visit, Lori has noticed improvement in her skin, but the
stiffness in her joints continues to bother her, especially when she is giving
piano lessons to students
• She is referred to a rheumatologist for further evaluation
• At Lori’s visit to the rheumatologist, she is diagnosed with concomitant PsA

47
Psoriatic Arthritis
• Seronegative spondyloarthritis
• Present in 6% to 42% of patients with psoriasis
‒ Greater prevalence among those with more severe psoriasis
‒ ~50% of patients with PsA have progressive, disabling disease
• Missed diagnoses are common
‒ ~15% of psoriasis patients have undiagnosed PsA
‒ 21.5% of patients with moderate to severe PsA are not being treated
‒ Up to 20% of those with severe PsA receive only topical therapy
• Patients with PsA report worse QoL than do those with psoriasis only
Armstrong AW, et al. JAMA Dermatol. 2013;149:1180-1185; Gottlieb A, et al. J Am Acad Dermatol. 2008;58:851-864; Mease PJ, et al. Drugs.
2014;74:423-441; Mease PJ, et al. J Am Acad Dermatol. 2013;69:729-735; Menter A, et al. J Am Acad Dermatol. 2008;58:826-850.

48
PsA: Characteristics
• Enthesitis a predominant characteristic
• Asymmetric joint involvement in ~80% of
patients—usually involves 1 to 3 joints
• 80% to 90% of patients with PsA have nail lesions
• Fingers and toes may be enlarged (“sausage digits”)
• Can develop at any time, even before psoriasis
is evident, but usually between ages 30 and 50 years
• Other symptoms: stiffness, pain, swelling
• Severity of PsA may not correlate with severity of psoriasis
Gottlieb A, et al. J Am Acad Dermatol. 2008;58:851-864; Mease PJ, et al. J Rheumatol. 2014;41:1249-1251; National Psoriasis Foundation.
www.psoriasis.org/psoriatic-arthritis. Accessed April 28, 2020; Singh JA, et al. Arthritis Care Res (Hoboken). 2019;71:2-29.

49
PsA: Clinical Photos
49
Helliwell PS, et al. Ann Rheum Dis. 2007;66:113-117.
Dactylitis
Enthesitis(photo courtesy Alexis Ogdie, MD)
Nail Dystrophy
Associated with PSA

50
PsA: Differential Diagnosis
*Premenopausal women.
OA = osteoarthritis.
Gottlieb A, Merola J. J Dermatolog Treat. 2019; DOI: 10.1080/09546634.2019.1605142; Gottlieb A, et al. J Am Acad Dermatol. 2008;58:851-864;
Mease PJ, Armstrong AW. Drugs. 2014;74:423-441.
PsA RA OA Gout
Peripheral disease Asymmetric Symmetric Asymmetric —
Axial joint/spondylitis Yes — No Less often
Stiffness Morning/
immobility
Morning/
immobility
With activity Yes
Enthesitis Yes No No Yes
Nail lesions Yes No No No
Psoriasis Yes Uncommon Uncommon Uncommon
Female:male ratio 1:1 3:1 to 4:1 1:1 to 2:1 1:5 to 1:10*

51
Psoriasis Epidemiology Screening Tool (PEST)
5-item questionnaire (sensitivity = 92%; specificity = 78%; positive likelihood ratio 4:1)
1. Have you ever had a swollen joint (or joints)?
2. Has a clinician ever told you that you have arthritis?
3. Do your fingernails or toenails have holes or pits?
4. Have you had pain in your heel?
5. Have you had a finger or toe that was completely swollen
and painful for no apparent reason?
Ibrahim GH, et al. Clin Exp Rhematol. 2009;27:469-474.
Answering “yes” to ≥3 questions is suggestive of PsA.
52
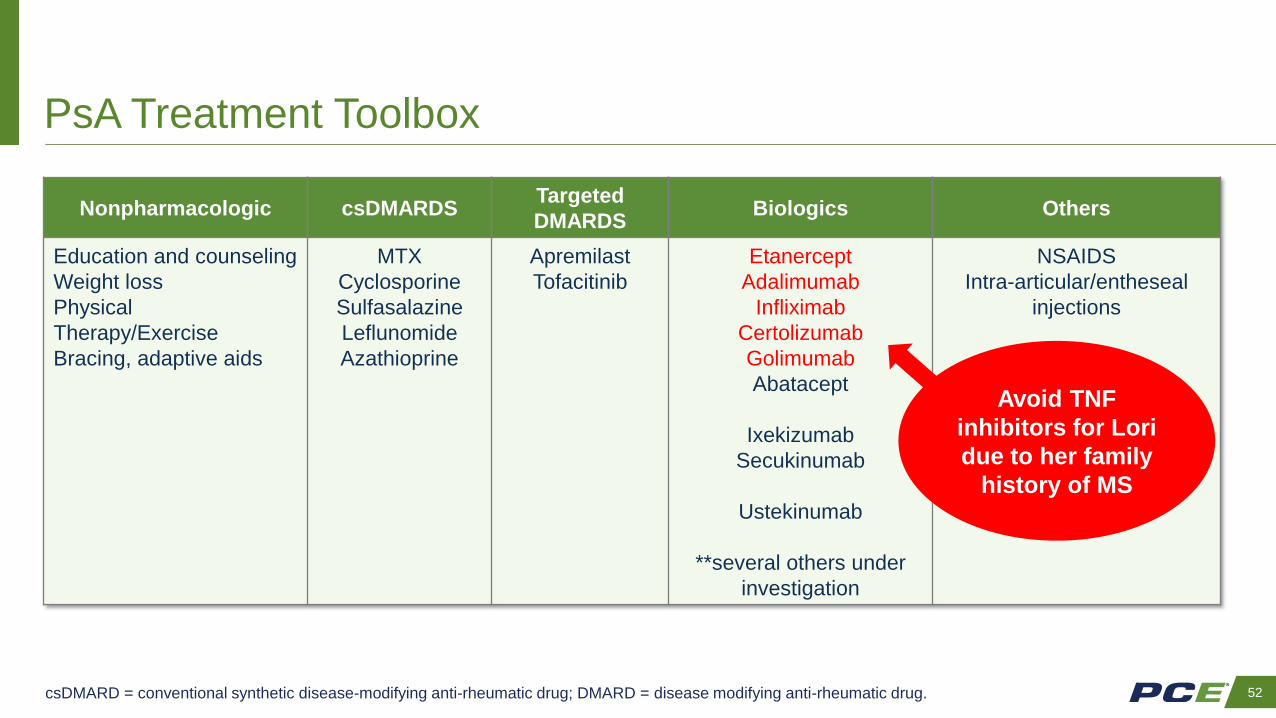
PsA Treatment Toolbox
Nonpharmacologic csDMARDSTargeted
DMARDSBiologics Others
Education and counseling
Weight loss
Physical
Therapy/Exercise
Bracing, adaptive aids
MTX
Cyclosporine
Sulfasalazine
Leflunomide
Azathioprine
Apremilast
Tofacitinib
Etanercept
Adalimumab
Infliximab
Certolizumab
Golimumab
Abatacept
Ixekizumab
Secukinumab
Ustekinumab
**several others under
investigation
NSAIDS
Intra-articular/entheseal
injections
Avoid TNF
inhibitors for Lori
due to her family
history of MS
csDMARD = conventional synthetic disease-modifying anti-rheumatic drug; DMARD = disease modifying anti-rheumatic drug.

53
PsA: Summary
• In patients with psoriasis, clinicians should look for signs and
symptoms of PsA at each visit
• However:
‒ PsA may appear before the diagnosis of psoriasis
‒ If PsA is suspected, refer patient to a rheumatologist
• Treatment goals
‒ Alleviate signs and symptoms of arthritis
‒ Inhibit structural damage
‒ Maximize QoL
.

54
Case Conclusion
• Lori has been taking an IL-17 inhibitor for 2 years
• Most of her lesions have resolved; maximum BSA involvement is 1%, and
she occasionally has complete clearance
• Stiffness in her fingers has diminished significantly
• She now visits the hair salon for cuts and styling
• Lori relies on your partnership to ensure her vaccinations remain current
and her cardiometabolic disease and depression are well managed
• You coordinate care with her dermatologist and rheumatologist
• You and Lori are vigilant for any AEs associated with her treatment

55
• AAD and NPF released statements on COVID-19 and immunosuppressive
therapies
‒ Stop therapy if patient tests positive or has symptoms consistent with
COVID-19; reinitiate once completely recovered
‒ Assess the risk vs benefits in lower-risk patients before initiating
immunosuppressive agents on a case-by-case basis
‒ High-risk individuals should have risk/benefit discussion with their
healthcare provider
‒ Initiation and cessation of systemic therapy should be discussed with
healthcare provider
What if Lori Was Infected With COVID-19?
55National Psoriasis Foundation. www.psoriasis.org/advance/coronavirus. Accessed April 30, 2020; American Academy of Dermatology.
www.aad.org/member/practice/coronavirus/clinical-guidance/biologics. Accessed April 30, 2020.

56
• Pregnancy and biologics
‒ No large scale trials
• Extrapolation from IBD and RA literature
• Weigh pros/cons
• Favor TNF use over other classes
‒ Certolizumab >entanercept >adalimumab >infliximab
• Generally deemed safe for first half of pregnancy
• Delayed live vaccination schedule for infant
What if Lori Wanted to Become Pregnant?
56IBD = inflammatory bowel disease.
Porter ML. Int J Womens Dermatol. 2017:3:21-25.

57
Biologics and surgery
• All biologics can be continued through low-risk surgery safely
• For moderate to high-risk surgery: case by case basis
‒ Most conservative approach is to discontinue biologic for a period of 3 to 4
half-lives (but this may not be feasible nor necessary in all cases)
• Informed risk/benefit discussion between patient, dermatology provider,
medical team, and surgery team
• Resume biologic therapy 1 to 2 weeks after surgery assuming no
complications
What if Lori Needed Surgery?
57
Choi YM, et al. J Am Acad Dermatol. 2016;75:798-805.

58
PCE Action Plan
✓ Set a target goal of complete/near-complete skin clearance for patients with moderate
to severe psoriasis
✓ Investigate all body areas that may be affected by psoriasis
✓ Consider patient’s perspective in selecting treatment
✓ Optimize care of patients with psoriatic disease by working as part of a collaborative
team
✓ Screen patients with psoriatic disease for CVD and other comorbidities
✓ Recommend appropriate vaccinations; HBV, HCV, and HIV screening; and TB testing
for patients taking biologic therapies
PCE Promotes Practice Change

2020 Symposia Series 1