1074 itu bajo riesgo de bacteriemia en infantes
TRANSCRIPT
8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 1/12
DOI: 10.1542/peds.2010-04792010;126;1074-1083; originally published online Nov 22, 2010;Pediatrics
CommitteeAcademy of Pediatrics Pediatric Emergency Medicine Collaborative Research
M. Plymale, Patrick Solari, Deborah J. Mann, Peter S. Dayan and for the AmericanJenniferBlackstone, Amit Sarnaik, Julie McManemy, Alison Brent, Jonathan Bennett,
Blake Bulloch, Dewesh Agrawal, Mary Saunders, Donna M. Sutherland, Mercedes M.Marc N. Baskin, Paul Ishimine, Camille Scribner, Pamela Okada, Heather Beach,
David Schnadower, Nathan Kuppermann, Charles G. Macias, Stephen B. Freedman, Events and Bacteremia
Febrile Infants With Urinary Tract Infections at Very Low Risk for Adverse
http://www.pediatrics.org/cgi/content/full/126/6/1074located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. Alland trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk publication, it has been published continuously since 1948. PEDIATRICS is owned, published,PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from

8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 2/12
Febrile Infants With Urinary Tract Infections at VeryLow Risk for Adverse Events and Bacteremia
WHAT’S KNOWN ON THIS SUBJECT:Febrile infants aged 29 to 60days who have urinary tract infections are typically hospitalizedfor 48 hours. Previous study results have indicated that mostpatients have benign clinical courses, but small sample sizeshave limited the ability to identify those at near-zero risk of adverse events.
WHAT THIS STUDY ADDS:We derived prediction models in alarge sample of patients that identify infants at very low risk foradverse events and at low risk for bacteremia. Shorterhospitalization or outpatient treatment with close follow-up maybe feasible for selected patients.
abstractBACKGROUND:There is limited evidence from which to derive guide-lines for the management of febrile infants aged 29 to 60 days withurinary tract infections (UTIs). Most such infants are hospitalized for
48 hours. Our objective was to derive clinical prediction models toidentify febrile infants with UTIs at very low risk of adverse events andbacteremia in a large sample of patients.
METHODS:This study was a 20-center retrospective review of infantsaged 29 to 60 days with temperatures of 38°C and culture-provenUTIs. We dened UTI by growth of 50 000 colony-forming units(CFU)/mL of a single pathogen or 10 000 CFU/mL in association withpositive urinalyses. We dened adverse events as death, shock, bacte-rial meningitis, ICU admission need for ventilator support, or othersubstantial complications. We performed binary recursive partitioninganalyses to derive prediction models.
RESULTS: We analyzed 1895 patients. Adverse events occurred in 51 of 1842 (2.8% [95% condence interval (CI): 2.1%–3.6%)] and bacteremiain 123 of 1877 (6.5% [95% CI:5.5%–7.7%]). Patients were at very lowriskfor adverse events if not clinically ill on emergency department (ED)examination and did not have a high-risk past medical history (predic-tion model sensitivity: 98.0% [95% CI: 88.2%–99.9%]). Patients were atlower risk for bacteremia if they were not clinically ill on ED examina-tion, did not have a high-risk past medical history, had a peripheralband count of 1250 cells per L, and had a peripheral absoluteneutrophil count of 1500 cells per L (sensitivity 77.2% [95% CI:68.6%–84.1%]).
CONCLUSION:Brief hospitalization or outpatient management withclose follow-up may be considered for infants with UTIs at very low riskof adverse events. Pediatrics 2010;126:1074–1083
AUTHORS:David Schnadower, MD, MPH, a NathanKuppermann, MD, MPH,b Charles G. Macias, MD, MPH,c
Stephen B. Freedman, MD, d Marc N. Baskin, MD,e PaulIshimine, MD,f Camille Scribner, MD, g Pamela Okada, MD, h
Heather Beach, MD, i Blake Bulloch, MD,j Dewesh Agrawal,MD,k Mary Saunders, MD, l Donna M. Sutherland, MD, m
Mercedes M. Blackstone, MD, n Amit Sarnaik, MD,o JulieMcManemy, MD,p Alison Brent, MD,q Jonathan Bennett,MD,r Jennifer M. Plymale, MD b Patrick Solari, MD, s
Deborah J. Mann, MD, t and Peter S. Dayan, MD, MSc a forthe American Academy of Pediatrics Pediatric EmergencyMedicine Collaborative Research Committeea Pediatric Emergency Medicine, Morgan Stanley Children’sHospital of New York, Columbia University College of Physiciansand Surgeons, New York, New York; b Emergency Medicine and Pediatrics, University of California, Davis School of Medicine,Sacramento, California; c Pediatric Emergency Medicine, TexasChildren’s Hospital, Baylor College of Medicine, Houston, Texas; d Paediatric Emergency Medicine and Gastroenterology,Hepatology and Nutrition, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada; e Pediatrics, Children’sHospital Boston and Harvard Medical School, Boston,Massachusetts; f Department of Medicine, Rady Children’sHospital, University of California, San Diego, California; g Pediatric Emergency Medicine, Children’s Hospital Oakland,Oakland, California; h Pediatric Emergency Medicine, Children’sMedical Center, University of Texas Southwestern Medical Center, Dallas, Texas; i Pediatric Emergency Medicine, Miami
Children’s Hospital, Miami, Florida; j Pediatric Emergency
Medicine, Phoenix Children’s Hospital, University of Arizona College of Medicine, Phoenix, Arizona; k Pediatric Emergency Medicine, Children’s National Medical Center, George Washington School of Medicine, Washington, District of Columbia; l Pediatric Emergency Medicine, Children’s Hospital of Wisconsin, Medical College of Wisconsin, Milwaukee, Wisconsin; m Pediatric Emergency Medicine, Wake Med Health, Raleigh,North Carolina; n Pediatric Emergency Medicine, Children’sHospital of Philadelphia, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania; o Pediatric Emergency Medicine, Children’s Hospital of Michigan, Wayne State University, Detroit, Michigan; p Pediatric Emergency Medicine, St Louis Children’s Hospital, Washington University School of Medicine, St Louis, Missouri; q Pediatric Emergency Medicine,Children’s Hospital, University of Colorado School of Medicine,Denver, Colorado; r Pediatric Emergency Medicine, A. I. duPont Hospital for Children, Thomas Jefferson University, JeffersonMedical College, Wilmington, Delaware; s Pediatric Emergency Medicine, Children’s Hospital and Regional Medical Center,University of Washington School of Medicine, Seattle,Washington; and t Emergency Medicine, State University of New York, Upstate, Syracuse, New York
(Continued on last page)
1074 SCHNADOWER et al. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from

8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 3/12
Urinary tract infection(UTI) is themostcommonserious bacterial illness in fe-brile infants younger than 60 days of age, occurring in 4% to 10% of theseinfants. 1– 6 In 1999, an American Acad-emy of Pediatrics guideline recom-
mended outpatient management withoral or parenteral antibiotics for chil-dren older than 2 months who haveUTIs unless thechild seemed “toxic, de-hydrated, or unable to take oral in-take,” in which case hospitalizationwas recommended. 7 There is little in-formation however, to guide the man-agement of infants aged 29 to 60days. 8,9 Although a recent clinical trialfound it feasible to treat febrile infants
with UTIs as outpatients with paren-teral antibiotics administered in an in-fusion center, 8 most clinicians hospi-talize these infants for 48 hours of parenteral therapy. 10–12
There are several reasons why clini-cians hospitalize infants aged 29 to 60days of age who have UTIs, includingthe unclear risk of long-term renal in-jury, and concern regarding follow-up.The most important reasons, however,
are the concerns of acute adverseevents and for missing concomitantbacteremia. Several small studieshave assessed the course of febrile in-fants with UTIs and suggest that other-wise well-appearing infants with orwithout concomitant bacteremia havebenign clinical courses when treatedwith appropriate antibiotics. 9–13 Be-cause of small sample sizes, investiga-tors have neither been able to provide
a precise estimate of the risk of ad-verse events or bacteremia nor derivepotential multivariable models to iden-tify risk factors for adverse events orbacteremia in young, febrile infantswith UTIs.
The aims of this study were to deter-mine the risk of adverse events andbacteremia in a large sample of febrileinfants aged 29 to 60 days with UTIswho present to the emergency depart-
ment (ED), and to derive clinical pre-diction models for infants at very lowrisk of adverse eventsand bacteremia.These data may help clinicians makemore informed decisions regardingthe need for, or length of hospitaliza-
tion of these infants.
METHODS
Study Design and Setting
We performed a retrospective chartreview at 20 medical centers that par-ticipated in the Pediatric EmergencyMedicine Collaborative Research Com-mittee of the American Academy of Pe-diatrics. The participating centers in-cluded 16 tertiary care pediatric EDsand 3 general EDs in the United Statesand 1 Canadian tertiary care ED. Ap-proval for the study with waiver of in-formed consent and for data sharingwith the coordinating institution andwith the centralized data center wasgranted by the institutional reviewboard at each participating institution.
Patient Identication
We performed case ascertainment byquerying laboratory databases for allurine cultures with bacterial growth inpatients aged 29 to 60 days that wereobtained in the ED between January1995 and May 2006. Lactobacillus , Mi- crococcus , diptheroids, Bacillus spe-cies and Staphylococcus epidermidiswere considered contaminants.
Inclusion Criteria
Children were classied as having aUTI if urine cultures grew a singlepathogen and colony counts met atleast 1 of 3 criteria:
1. 1000 colony-forming units (CFU)/mLfor urine cultures obtained by su-prapubic aspiration;
2. 50 000 CFU/mL from a catheter-ized specimen; or
3. 10 000 and 50 000 CFU/mL froma catheterized specimen in asso-
ciation with positive urinalysisresults. 14
We dened positive urinalysis resultsas those that met any of the following:(a ) any organisms visualized on Gram-stain; ( b) trace or greater result for
leukocyte esterase or nitrite on ED dip-stick or laboratory-based urinalysis;or ( c ) 5 white blood cells (WBCs) perhigh-power eld (standard micros-copy) or per L (hemocytometer) on acentrifuged or uncentrifuged urinespecimen. 15–17
Exclusion Criteria
We excluded patients for any of the fol-lowing: (a ) transfer from other hospi-
tals with previously obtained labora-tory results; ( b) urine specimensobtained by techniques other than su-prapubic aspiration or transurethralcatheterization; ( c ) urine cultures thatgrew multiple organisms; or ( d ) nomeasured temperature of 38.0°C inthe EDor athome within24 hours ofEDpresentation. We excluded patientswithout a measured fever because wewere interested in patients with a high
likelihood of true UTIs, not those withasymptomatic bacteriuria.
Data Collection and Potential Risk Factors
All coinvestigators were trained by thestudy’s principal investigator in per-sonor during conference calls.Each of the coinvestigators reviewed the med-ical charts for all study patients attheir site. Study data were entered
onto computerized PDF documents(“teleforms”) (Adobe Acrobat 8 Profes-sional, San Jose, CA) that were pro-grammed to improve data accuracyand completeness. The teleforms werethen uploaded electronically or by faxinto a central database to avoid sec-ondary transcription errors.
We collected data on patient demo-graphics, past medical history, pre-senting symptoms in the ED (including
ARTICLES
PEDIATRICSVolume 126, Number 6 , December 2010 1075. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from

8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 4/12
upper-respiratory infection symp-toms, vomiting, diarrhea, difcultyfeeding, and presence of seizures), vi-tal signs at triage, ED physical exami-nation ndings (general appearance,dehydration, and respiratory dis-
tress), and ED disposition.We obtaineddata regarding ED and inpatient man-agement and the patient’s clinicalcourse, radiologic study results, aswell as urine, blood,andcerebrospinaluid (CSF) laboratory and microbiol-ogy results.
We also assessed for the presence of acute concomitant diseases dened asan acute, focal infectious process dis-tinct from the UTI, such as pneumonia,
bronchiolitis, cellulitis, osteomyelitis, orseptic arthritis. We did not consideracute gastroenteritis or acute otitis me-dia as an acute concomitant disease.
A priori, we created the variable “clin-ically ill in the ED,” dened as an infantwho was judged as ill-appearing, dehy-drated, or in respiratory distress orwhohad an acute concomitant diseasediagnosed in the ED. We also createdthe variable “high risk past medical
history,” which included a history of genitourinary abnormalities, previousUTIs, bacteremia, meningitis, previouslaboratory evaluation for fever, prema-turity ( 37 weeks’ gestation), or his-tory of a severe systemic disease(complex heart, chronic lung, meta-bolic, or neurologic diseases). Otherpast medical history such as minorneonatal complications, jaundice, gas-troesophageal reux or a history of a
minor resolved acute illness was notconsidered to represent a high-riskpast medical history (coded “not highrisk”).
Outcome Measures
We had 2 study outcomes: adverseevents and bacteremia. Although theoccurrence of an adverse event wasconsidered the most clinically impor-tant outcome, we also included bacte-
remia because it is clinically relevanteven in the absence of an adverseevent.
An adverse event was consideredpresent if any of the following oc-curred: death, shock, bacterial menin-gitis, ICU or step-down ICU admissionor transfer (for ICU or step-down ICUlevel of care and monitoring), need forventilatory support (intubation,contin-uous, or bilevel positive airway pres-sure), need for surgical intervention,or other substantial clinical complica-tion. Patients did not meet this deni-tion if the adverse event was solely re-lated to an iatrogenic complication(eg, anaphylaxis because of a medica-tion, nosocomial infection).
We dened shock as ( a ) “shock”clearly stated in a faculty or fellowphy-siciannote, ( b) useof vasopressors, or(c ) the combination of low blood pres-sure ( 70 mm Hg systolic) or “hypo-tension” or “sepsis” clearly stated inmedical chart (“rule out sepsis” didnot qualify as sepsis) and the patientwas treated with intravenous uid bo-luses of 40 mL/kg.
To provide a conservative risk esti-mate, 18–20 we dened bacterial menin-gitis as denite or probable and in-cluded all cases in the analysis:
1. We deneddenite bacterialmenin-gitis as the growth of a knownpathogen in the CSF. Bacillus spe-cies, Propionibacterium acnes ,non– Staphylococcus aureus , andStreptococcus viridans were con-
sidered contaminants.2. For patients with no bacterial
growth in the CSF cultures, we de-ned probable bacterial meningitisas any of the following:● the combination of ( a ) CSF pleo-
cytosis ( 10 cells per L) and(b) positive blood culture and ( c )treatment consistent with bacte-rial meningitis (dened as 14days of parenteral antibiotics not
clearly administered for otherreasons on review of inpatientrecords); or
● the combination of ( a ) positiveCSF Gram-stain or positive latexagglutination tests and ( b) treat-
ment consistent with bacterialmeningitis; or
● the combination of ( a ) pretreat-ment with antibiotics before lum-bar puncture, ( b) CSF pleocytosis( 10 cells per L), and (c ) treat-ment consistent with bacterialmeningitis.
Bacteremia wasdenedas thegrowthof a pathogen in the blood culture. We con-sidered blood cultures that grew Bacil- lus species, Propionibacterium acnes ,or non– S aureus as contaminated.
Data Validity and Reliability
Subjective Physical ExaminationVariables
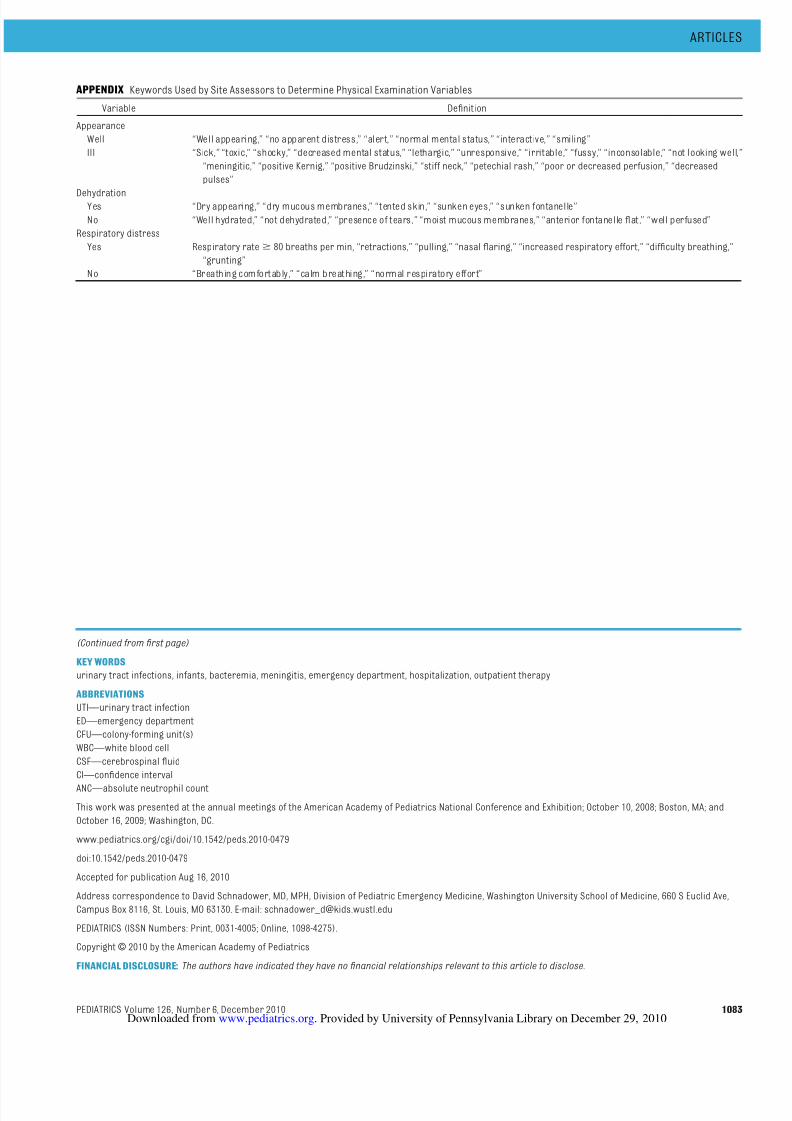
To minimize the potential bias associ-ated with abstracting physical exami-nation ndingsfromthe medical chart,we used specic, restrictive key wordsto determine and assign whether theinfant was ill-appearing, dehydrated,or in respiratory distress (see Appen-dix). To determine inter-rater reliabil-ity, a second assessor at each institu-tion performed an independentassessment of the documented physi-cal examination for a random sampleof 10% of patients as well as all pa-tients whohadbacteremia or evidenceof adverse events.
Determination of Adverse EventsTo achieve agreement on the presenceand timing of adverse events, a secondinvestigator at each institution inde-pendently reviewed the medical chartsof all patients who potentially had ad-verse events. For these patients, bothsite investigators assessed ( a ) the na-ture of the adverse events and ( b) thetime points at which the adverseevents were identied.
1076 SCHNADOWER et al. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from

8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 5/12
Missing Data
We labeled unavailable data as miss-ing except for particular presentingsymptoms (upper-respiratory infec-tion symptoms, vomiting, difcultyfeeding, diarrhea, and seizures), for
which the absence of a specic de-scription in the chart was interpretedas “not present.”
Patients Discharged Home From the ED
For these patients, investigators com-pleted a detailed chart review of allsubsequent visits to the hospitalwithin1 year ofthe EDvisit atwhich theUTI was diagnosed. If there were sub-
sequent visitsbutno documentation of adverse events that occurred duringthe UTI illness, we categorized the out-come as uncomplicated. If there wereno subsequent visits documentedwithin the year, we categorized theoutcome as unknown.
Statistical Analysis
We described the risk of adverseevents and bacteremia as proportionswith 95% condence intervals (CIs).The unweighted Cohen’s value wasused to determine the interrater reli-ability for the assessor review of sub-jective physical examination ndings.
Prediction Models for AdverseEvents and Bacteremia
We performed 2 separate binary re-cursive partitioning analyses to iden-tify a group of infants at very low riskfor adverse events and a group of in-fants at very lowrisk forbacteremia. Inthese analyses, we included all the fol-lowing potential predictor variableswith biological plausibility for associa-tion with the outcome variables: age;past medical history; history of feedingdifculty; vomiting; seizures; clinicalappearance in the ED; presence of acute concomitant disease; vital signsat triage; peripheral WBC count; pe-ripheral blood absolute neutrophil
count (ANC); peripheral blood band
count; peripheral blood immature/to-tal neutrophil ratio; and CSF WBCcount. Continuous variables were di-chotomized and rounded by analyzingfrequencydistributions, receiver oper-ating curves, and single-variable re-cursive partitioning analyses to iden-tify the best predictive and clinicallysensible cutoff points for associationwith each of the 2 outcomes.
Because our aim was to identify whichpatients were at very low risk of the 2outcomes, we assigned a high relativecost to misclassication of patientswith adverse events or bacteremia. Weassigned a relative cost of 100 to 1 forfailure to identify a patient with an ad-verse event versus incorrect classi-cation of a patient without an adverseevent,anda costof 20 to1 for failure toidentify a patient with bacteremia ver-sus incorrect classication of a patient
without bacteremia. We used “Gini”
splitting rules and pruned the result-ing trees to improve simplicity andgeneralizability. Finally, we used 10-fold cross-validation to develop robustand generalizable prediction models.We reporttest characteristics foreachoutcome and 95% CIs, calculated withexact methods. We used Classicationand Regression Tree software (CART 6[Salford Systems, San Diego, CA]) toconduct the recursive partitioning
analyses. Finally, we performed bivari-ate and multivariate regression analy-ses (using SPSS 16 [SPSS Inc, Chicago,IL]) for variables included in the pre-diction models to assess the strengthof association of these variables withthe 2 outcomes.
Sample Size
We based our sample size on the abilityto provide precise estimates of the
2477 patients aged 29–60 d withbacterial growth from urine cultures
obtained in ED
582 patients excluded⋅ 253 no measured temperature > 38.0° C
243 multiple organisms noted in urine culture58 transferred from another facility28 specimens not obtained bycatheterization or suprapubic aspiration
1895 febrile infants with UTIs analyzed
1719 hospitalized (90.7%)
General inpatient service: 1632 (94.9%)
ICU or step-down ICU: 37 (2.1%)Transferred to outside hospital: 50 (2.9%)
Adverse events: 0/146 a (0%)Bacteremia: 6/176 (3.4%)
Adverse events: 51/1696 a (3.0%)Bacteremia: 117/1701 a (6.9%)
176 discharged home from ED (9.3%)
⋅
⋅
⋅
⋅
FIGURE 1Study ow. a Of those with known outcomes.
ARTICLES
PEDIATRICSVolume 126, Number 6 , December 2010 1077. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from
8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 6/12
risk of adverse events, the risk of bac-teremia, and the sensitivities of theprediction models. In a sample of 1500infants aged 29 to 60 days with feverand UTIs, we expected the upper endsof the 95% CIs for an assumed 2% esti-
mated risk of adverse events and 5%estimated risk of bacteremia to be2.8% and 6%, respectively. Given theserisk assumptions, we required 50patients with adverse events and 100patients with bacteremia to result in a95% CI lower boundary of 94% for amodel to predict adverse events thatwas 100% sensitive, and a lower bound-ary of 89% for a model to predict bacte-remia that was 95% sensitive. Previous
literature suggested we were unlikely toderive a model that was 100% sensitiveto detect bacteremia. 12,13
RESULTS
The information from 1 of the 20 par-ticipating institutions was excludedbecause of systematically missingdata. The remaining institutions hadaccess to microbiology databases dat-ing 3 to 10 years. We identied 2477potentially eligible patients, of whom1895 were included in the analysis ( Fig 1).
Patient Characteristics
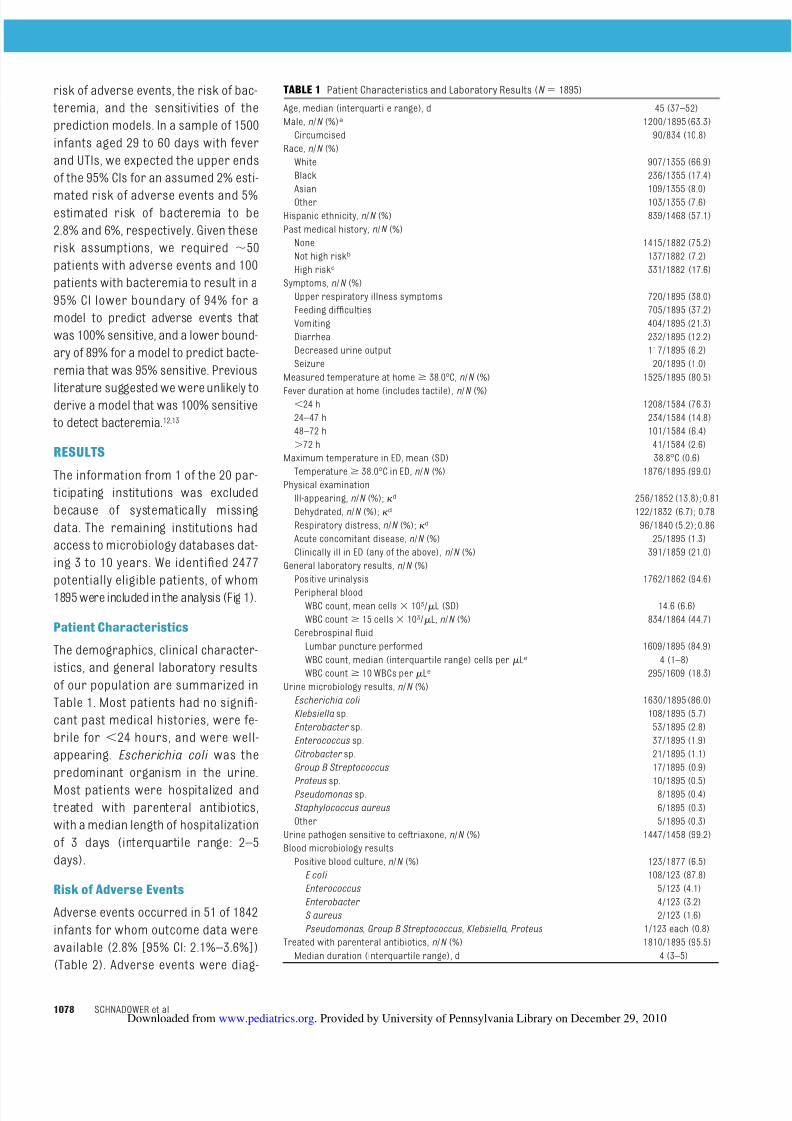
The demographics, clinical character-istics, and general laboratory resultsof our population are summarized inTable 1. Most patients had no signi-cant past medical histories, were fe-brile for 24 hours, and were well-appearing. Escherichia coli was thepredominant organism in the urine.Most patients were hospitalized andtreated with parenteral antibiotics,with a median length of hospitalizationof 3 days (interquartile range: 2–5days).
Risk of Adverse Events
Adverse events occurred in 51 of 1842infants for whom outcome data wereavailable (2.8% [95% CI: 2.1%–3.6%])(Table 2) . Adverse events were diag-
TABLE 1 Patient Characteristics and Laboratory Results ( N 1895)
Age, median (interquartile range), d 45 (37–52)Male, n/N (%) a 1200/1895 (63.3)
Circumcised 90/834 (10.8)Race, n/N (%)
White 907/1355 (66.9)Black 236/1355 (17.4)Asian 109/1355 (8.0)Other 103/1355 (7.6)
Hispanic ethnicity, n/N (%) 839/1468 (57.1)Past medical history, n/N (%)
None 1415/1882 (75.2)Not high risk b 137/1882 (7.2)High risk c 331/1882 (17.6)
Symptoms, n/N (%)Upper respiratory illness symptoms 720/1895 (38.0)Feeding difculties 705/1895 (37.2)Vomiting 404/1895 (21.3)Diarrhea 232/1895 (12.2)Decreased urine output 117/1895 (6.2)Seizure 20/1895 (1.0)
Measured temperature at home 38.0°C, n/N (%) 1525/1895 (80.5)
Fever duration at home (includes tactile), n/N (%)24 h 1208/1584 (76.3)
24–47 h 234/1584 (14.8)48–72 h 101/1584 (6.4)
72 h 41/1584 (2.6)Maximum temperature in ED, mean (SD) 38.8°C (0.6)
Temperature 38.0°C in ED,n/N (%) 1876/1895 (99.0)Physical examination
Ill-appearing, n/N (%); d 256/1852 (13.8); 0.81Dehydrated, n/N (%); d 122/1832 (6.7); 0.78Respiratory distress, n/N (%); d 96/1840 (5.2); 0.86Acute concomitant disease, n/N (%) 25/1895 (1.3)Clinically ill in ED (any of the above), n/N (%) 391/1859 (21.0)
General laboratory results, n/N (%)Positive urinalysis 1762/1862 (94.6)Peripheral blood
WBC count, mean cells 103 / L (SD) 14.6 (6.6)WBC count 15 cells 103/ L,n/N (%) 834/1864 (44.7)
Cerebrospinal uidLumbar puncture performed 1609/1895 (84.9)WBC count, median (interquartile range) cells per Le 4 (1–8)WBC count 10 WBCs per Le 295/1609 (18.3)
Urine microbiology results, n/N (%)Escherichia coli 1630/1895 (86.0)Klebsiella sp. 108/1895 (5.7)Enterobacter sp. 53/1895 (2.8)Enterococcus sp. 37/1895 (1.9)Citrobacter sp. 21/1895 (1.1)Group B Streptococcus 17/1895 (0.9)
Proteus sp. 10/1895 (0.5)Pseudomonas sp. 8/1895 (0.4)Staphylococcus aureus 6/1895 (0.3)Other 5/1895 (0.3)
Urine pathogen sensitive to ceftriaxone, n/N (%) 1447/1458 (99.2)Blood microbiology results
Positive blood culture, n/N (%) 123/1877 (6.5)E coli 108/123 (87.8)Enterococcus 5/123 (4.1)Enterobacter 4/123 (3.2)S aureus 2/123 (1.6)Pseudomonas , Group B Streptococcus , Klebsiella , Proteus 1/123 each (0.8)
Treated with parenteral antibiotics, n/N (%) 1810/1895 (95.5)Median duration (interquartile range), d 4 (3–5)
1078 SCHNADOWER et al. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from
8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 7/12
nosed immediately in the ED in 26 of 51(51.0%) patients, within 4 hours of EDpresentation in 10 of 51 (19.6%), be-tween 4 and 23 hours in 11 of 51(21.6%), between 24 and 47 hours in 2of 51 (3.9%), and after 48 hours in 2of 51 (3.9%).
Risk of Bacteremia
Bacteremia was present in 123 of 1877infants from whom blood cultureswere obtained (6.5% [95% CI: 5.5% of 7.7%]) (Table 1) . The time from obtain-ing the blood culture to the time thatthe blood culture was noted to be pos-itive was available for 91 of 123 pa-tients (74%). The median time to posi-tivity was 16 hours (interquartilerange: 13–24 hours); 80 of 91 (88%)were positive within 24 hours. Ten of 123 patients with bacteremia hadadverse events (8.1% [95% CI: 4.2%–13.8%]), whereas 41 of 1754 patientswithout bacteremia had adverseevents (2.3% [95% CI: 1.7%–3.1%).
Prediction Models for AdverseEvents and Bacteremia
Adverse EventsRecursive partitioning analysis identi-ed a group of patients at very low riskof adverse events ( Fig 2). Patients be-longed tothe verylow riskgroup if theywere not clinically ill on ED examina-tion (well-appearing, not dehydrated,not in respiratory distress,andno con-comitant acute disease) and did nothave a high-risk past medical history.The prediction model sensitivity forad-
verse events was 98.0% (95% CI:88.2%–99.9%), and the negative pre-dictive value was 99.9% (95% CI:99.5%–100%). Of 1206 infants in thevery low risk group (65.5% of those an-alyzed), only 1 infant had an adverseevent (0.1% [95% CI: 0%–0.4%]): a 46-day-old boy who was well-appearingon physical examination in the ED butwhose initial CSF studies were lost. Asubsequent lumbar puncture 24 hours
after the initiation of intravenous anti-biotics revealed a negative Gram-stain,34 WBCs per L, 177 red blood cellsper L, 54 mg of glucose per dL, 85 mgof protein per dL, negative bacterialculture, and negative CSF bacterial an-
tigens. In accordance with subspecial-ist recommendations, the infant wastreated for 21 days with intravenousantibiotics for possible pretreatedbacterial meningitis. The patient didnot have bacteremia and had an other-wise uneventful hospital course.
Bacteremia
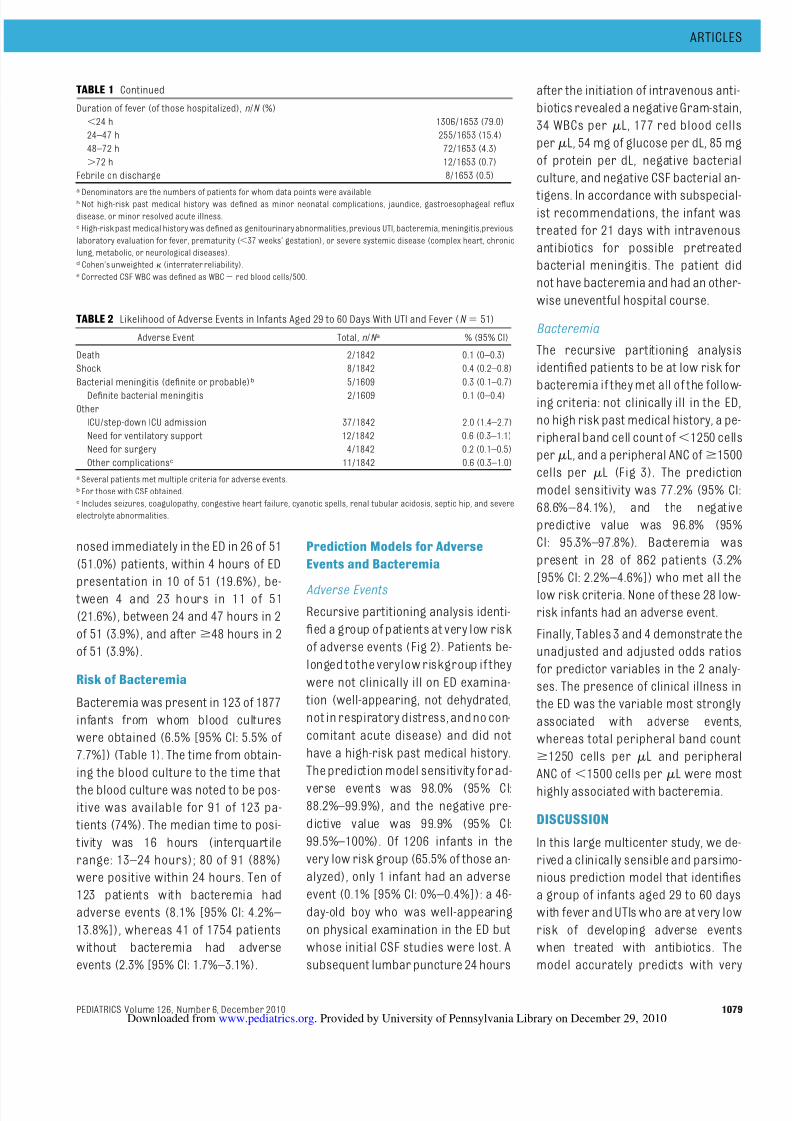
The recursive partitioning analysisidentied patients to be at low risk forbacteremia if they met all of the follow-ing criteria: not clinically ill in the ED,no high risk past medical history, a pe-ripheral band cell count of 1250 cellsper L, and a peripheral ANC of 1500cells per L (Fig 3). The predictionmodel sensitivity was 77.2% (95% CI:68.6%–84.1%), and the negativepredictive value was 96.8% (95%CI: 95.3%–97.8%). Bacteremia waspresent in 28 of 862 patients (3.2%[95% CI: 2.2%–4.6%]) who met all thelow risk criteria. None of these 28 low-risk infants had an adverse event.
Finally, Tables 3 and 4 demonstrate theunadjusted and adjusted odds ratiosfor predictor variables in the 2 analy-ses. The presence of clinical illness inthe ED was the variable most stronglyassociated with adverse events,whereas total peripheral band count
1250 cells per L and peripheralANC of 1500 cells per L were mosthighly associated with bacteremia.
DISCUSSION
In this large multicenter study, we de-rived a clinically sensible and parsimo-nious prediction model that identiesa group of infants aged 29 to 60 dayswith fever and UTIs who are at very lowrisk of developing adverse eventswhen treated with antibiotics. Themodel accurately predicts with very
TABLE 2 Likelihood of Adverse Events in Infants Aged 29 to 60 Days With UTI and Fever ( N 51)
Adverse Event Total, n/N a % (95% CI)
Death 2/1842 0.1 (0–0.3)Shock 8/1842 0.4 (0.2–0.8)Bacterial meningitis (denite or probable) b 5/1609 0.3 (0.1–0.7)
Denite bacterial meningitis 2/1609 0.1 (0–0.4)Other
ICU/step-down ICU admission 37/1842 2.0 (1.4–2.7)Need for ventilatory support 12/1842 0.6 (0.3–1.1)Need for surgery 4/1842 0.2 (0.1–0.5)Other complications c 11/1842 0.6 (0.3–1.0)
a Several patients met multiple criteria for adverse events.b For those with CSF obtained.c Includes seizures, coagulopathy, congestive heart failure, cyanotic spells, renal tubular acidosis, septic hip, and severeelectrolyte abnormalities.
TABLE 1 Continued
Duration of fever (of those hospitalized), n/N (%)24 h 1306/1653 (79.0)
24–47 h 255/1653 (15.4)48–72 h 72/1653 (4.3)
72 h 12/1653 (0.7)Febrile on discharge 8/1653 (0.5)a
Denominators are the numbers of patients for whom data points were available.b Not high-risk past medical history was dened as minor neonatal complications, jaundice, gastroesophageal reuxdisease, or minor resolved acute illness.c High-risk past medical history was dened as genitourinary abnormalities, previous UTI, bacteremia, meningitis,previouslaboratory evaluation for fever, prematurity ( 37 weeks’ gestation), or severe systemic disease (complex heart, chroniclung, metabolic, or neurological diseases).d Cohen’s unweighted (interrater reliability).e Corrected CSF WBC was dened as WBC red blood cells/500.
ARTICLES
PEDIATRICSVolume 126, Number 6 , December 2010 1079. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from

8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 8/12
high negative predictive value that in-fants who are not clinically ill in the EDandhave no high-risk past medical his-tory will have benign clinical courses.The model was highly sensitive, mis-classifying only 1 patient (0.1%) withan adverse event. This patient’s ad-verse event (bacterial meningitis)could be questioned because the CSFstudies obtained in the ED were lost,the subsequent CSF ndings were un-likely to represent bacterial illness,and his clinical course was uncompli-
cated. Although we are aware of nosimilar studies to derive models topredict adverse events in this popula-tion, the overall low risk of adverseevents that we found is similar to thatin small previous studies of infantswith UTIs.8,10,12,13
Our data suggest that infants with UTIsand fever who meet very low risk crite-ria for adverse events (ie, those whoare not clinically ill in the ED and haveno high-risk past medical history)
could be managed less conservativelythan commonly practiced. Possiblestrategies for managing these infantsinclude hospitalization for short peri-ods of time (eg, 24 hours) or perhapsdischarge with close follow-up to a re-
liable home environment after appro-priate antibiotic therapy is initiatedand the patient has a period of obser-vation in the ED. In the present study,approximately two-thirds of the in-fants met the low risk criteria for ad-verse events. Investigators recentlyshowed that outpatient intravenousantibiotic treatment in an infusioncen-ter was feasible and safe in low riskinfants with UTIs. That study, however,
included only 25 patients aged 29 to 60days. 8 In our series, 176 patients (9.3%of our study population) were dis-charged home from the ED after receiv-ing parenteral ceftriaxone without anyknown subsequent complications, in-cluding patients later found to have bac-teremia. A shorter hospitalization or out-patient therapy would decrease theexposureof these infants to thepotentialiatrogenic complications associated
with hospitalization. 21
We recognize that clinicians may beunwilling to discharge home from theED febrile infants with UTIs who poten-tially have bacteremia, even if they arelikely to haveotherwise uncomplicatedclinical courses. In our series, 6.5% of patientshad bacteremia, whereas pre-vious study estimates range from 0%to 21%.9,10,12,22–24 Similar to previous lit-erature, most patients in our study
who had positive blood cultures wereidentied within the rst 24 hours. 25
We attempted but were unsuccessfulin deriving a very low risk model toidentify infants with bacteremia. Thisreects the limitations in predictingbacteremia with standard clinical andlaboratory data. 12,13 The addition of aperipheral band count of 1250 cellsper L and peripheral ANC of 1500cells per L to those predictors that
latoT o AENAE Any predictor present 50 586 636No predictor present 1 1205 1206Total 51 1791 1842
Test characteristics of prediction modelSensitivity: 98.0% (95 CI: 88.2–99.9)Specificity: 67.3% (95% CI: 65.1–69.5)NPV: 99.9% (95% CI: 99.5–100)PPV: 7.9% (95% CI: 5.9–10.3)LR negative: 0.03 (95% CI: 0.00–0.20)
51/1842 AE (2.8%)1791/1842 no AE (97.2%)
40/382 AE (10.5%)342/382 no AE (89.5%)
11/ 1460 AE (0.8%)1449/1460 no AE (99.2%)
10/254 AE (3.9%)244/254 no AE (96.1%)
1/1206 AE (0.1%)1205/1206 no AE (99.9%)
Clinically ill in the ED? a
High-risk PMH? b
YesNo
YesNo
All infants with UTIs withknown outcomeN = 1842
FIGURE 2Prediction model to identify infants aged 29 to 60 days with febrile UTIs at very low risk of adverseevents. a Clinically ill in the ED, dened as ill-appearing, dehydrated, or in respiratory distress orpresence of an acute concomitant disease diagnosed in the ED; b high-risk past medical history,dened as genitourinary abnormalities, previous UTI, bacteremia, meningitis, previous laboratoryevaluation for fever, prematurity ( 37 weeks’ gestation), or severe systemic disease (complex heart,chronic lung, metabolic, or neurologic diseases). AE indicates adverse event; PMH, past medicalhistory; NPV, negative predictive value; PPV, positive predictive value; LR, likelihood ratio.
1080 SCHNADOWER et al. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from
8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 9/12
accurately identify infants at very lowrisk for adverse events did decreasethe likelihood of bacteremia to 3.2%.Previous research has noted an asso-ciation between high peripheral bandcounts or low peripheral ANC with
bacteremia caused by Gram-negativeorganisms. 12,23,26,27
Our study had several limitations typi-cal of medical chart reviews. These in-cluded potential biases in data ab-straction, particularly of subjectiveclinical ndings. We attempted to min-imize these biases by creating a de-tailed manual of operations that in-cluded specic key words to interpretsubjective ndings, by conducting in-
terrater reliability analyses of subjec-tive variables, and by using more ob-jective criteria to dene adverseevents. These efforts would not ac-count for clinician documentation bi-ased by previous knowledge of labora-tory results or clinical course.However, clinicians in the ED would beunlikely to know of future clinical dete-rioration before initial documentationin the medical chart.
We were also challenged to dene bac-terial meningitis for patients with neg-ative CSF cultures. We used conserva-tive denitions for probable bacterialmeningitis to avoid missing patientswith this important outcome. It shouldalso be recognized that we queried mi-crobiology databases rather than at-tempting to identify patients who pre-sented to the ED with positiveurinalyses, which was not feasible.
Therefore, our results are applicableto those patients for whom urine cul-ture results are known and cannotnecessarily be extrapolated to thosefor whom only preliminary screeningtests for UTI are known.
CONCLUSIONS
We derived a highly accurate predic-tion model that identies a group of febrile infants aged 29 to 60 days with
Test characteristics of prediction modelSensitivity: 77.2% (95% CI: 68.6-84.1%)Specificity: 47.6% (95% CI: 45.2-50.0%)NPV: 96.8% (95% CI: 95.3-97.8%)PPV: 9.4% (95% Cl: 7.7-11.4%)LR negative:
Bacteremia No Bacteremia Total
Any predictorpresent 95 920 1015
No predictor present 28 834 862Total 123 1754 1877
123/1877 bacteremia (6.6%)1754/1877 no bacteremia (93.4%)
All infants with UTIs with ablood culture performedN = 1877
No Yes
22/251 bacteremia (8.8%)229/251 no bacteremia (91.2%)
87/1488 bacteremia (5.8%)1401/1488 no bacteremia (94.2%)
36/389 bacteremia (9.3%)353/389 no bacteremia (90.7%)
65/1237 bacteremia (5.3%)1172/1237 no bacteremia (94.7%)
34/337 bacteremia (10.1%)303/337 no bacteremia (89.9%)
31/900 bacteremia (3.4%)869/900 no bacteremia (96.6%)
3/38 bacteremia (7.9%)35/38 no bacteremia (92.1%)
28/862 bacteremia (3.2%)834/862 no bacteremia (96.8%)
Clinically ill in the ED?a
No
No
Yes
Yes
Yes
No
ANC <1500 cells per µ L?
Bands>
1250 cells per µ L?
High-risk PMH? b
0.48 (95% Cl: 0.34, 0.66)
FIGURE 3Prediction model to identify infants aged 29 to 60 days with febrile UTIs at low risk of bacteremia.a Clinically ill in the ED, dened as ill-appearing, dehydrated, or in respiratory distress or presence of an acute concomitant disease diagnosed in the ED; b high-risk past medical history, dened asgenitourinaryabnormalities, previous UTI,bacteremia, meningitis,previouslaboratory evaluation forfever, prematurity ( 37 weeks’ gestation), or severe systemic disease (complex heart, chronic lung,metabolic, or neurologic diseases). PMH indicates past medical history.
TABLE 3 Bivariate and Multivariate Adjusted Odds Ratios for Predictors of Adverse Events in theRecursive Partitioning Analysis
Variable Unadjusted OddsRatio (95% CI)
P Adjusted Odds Ratio(95% CI)
P
Clinical ly ill in ED 15 .5 (7 .8–30 .4) .001 15.6 (7.9–30.9) .001High-risk past medical
history4.0 (2.3–7.1) .001 4.3 (2.4–7.8) .001
ARTICLES
PEDIATRICSVolume 126, Number 6 , December 2010 1081. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from

8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 10/12
UTIs at very low risk for adverseevents. We attempted but were unsuc-cessful in deriving a very low riskmodel to identify infants who had bac-teremia. Initiating antimicrobial ther-
apy and brief hospitalization (eg, 24hours), within which time frame mostbacteremia will be identied, seemsappropriate management for thisgroup of infants. Outpatient manage-
ment with long-acting intramuscularantibiotics and close follow-up couldalso be considered after a period of observation. Future research shouldattempt to validate the predictionmodel for adverse eventsand continue
to assess the safety and feasibility of alternative management strategies forthese young febrile infants with UTIs.
ACKNOWLEDGMENTSThe authors would like to thank JohnKanegaye, MD, Ma Long and AchillesKalnoky, MD, for their participationand efforts in this study.
REFERENCES
1. Baker MD, Bell LM, Avner JR. The efcacy of routine outpatient management withoutantibioticsof fever in selected infants. Pedi- atrics . 1999;103(3):627– 631
2. Baker MD, Bell LM, Avner JR. Outpatientmanagement without antibiotics of fever inselected infants. N Engl J Med . 1993;329(20):1437–1441
3. BonadioWA, Smith DS,Sabnis S. Theclinicalcharacteristics and infectious outcomes of febrile infants aged 8 to 12 weeks. Clin Pe- diatr (Phila) . 1994;33(2):95–99
4. Hoberman A, Chao HP, Keller DM, Hickey R,
Davis HW, Ellis D.Prevalence ofurinarytractinfection in febrile infants. J Pediatr . 1993;123(1):17–23
5. Shaw KN, Gorelick M, McGowan KL, YakscoeNM, Schwartz JS. Prevalence of urinarytract infection in febrile young children inthe emergency department. Pediatrics .1998;102(2). Available at: www.pediatrics.org/cgi/content/full/102/2/e16
6. ZorcJJ,KiddooDA,ShawKN.Diagnosisandman-agement of pediatric urinary tract infections.ClinMicrobiol Rev . 2005;18(2):417–422
7. American Academy of Pediatrics, Commit-
tee on Quality Improvement and Subcom-mittee on Urinary Tract Infection. Practiceparameter: the diagnosis, treatment, andevaluation of the initial urinary tract infec-tion in febrile infants and young children.Pediatrics . 1999;103(4 pt 1):843– 852
8. Doré-Bergeron MJ, Gauthier M, Chevalier I,McManus B, Tapiero B, Lebrun S. Urinarytract infections in 1- to 3-month-old infants:ambulatory treatment with intravenous an-tibiotics. Pediatrics . 2009;124(1):16–22
9. Hoberman A, Wald ER, Hickey RW, et al. Oralversus initial intravenous therapy for uri-
nary tract infections in young febrile chil-dren. Pediatrics . 1999;104(1 pt 1):79–86
10. Dayan PS, Hanson E, Bennett JE, Langsam D,Miller SZ. Clinical course of urinary tractinfections in infants younger than 60daysof age. Pediatr Emerg Care . 2004;20(2):85–88
11. Bachur R. Nonresponders: prolonged feveramong infants with urinary tract infections.Pediatrics . 2000;105(5). Available at: www.pediatrics.org/cgi/content/full/105/6/e59
12. BachurR,CaputoGL. Bacteremiaandmeningitisamong infants with urinary tract infections. Pe- diatr EmergCare . 1995;11(5):280–284
13. Honkinen O, Jahnukainen T, Mertsola J, Es-kola J, Ruuskanen O. Bacteremic urinarytractinfection in children. Pediatr Infect DisJ . 2000;19(7):630–634
14. Zorc JJ,Levine DA,Platt SL,et al.Clinicalanddemographic factors associated with uri-nary tract infection in young febrile infants.Pediatrics . 2005;116(3):644–648
15. Gorelick MH, Shaw KN. Screening tests forurinary tract infection in children: a meta-analysis. Pediatrics . 1999;104(5). Availableat: www.pediatrics.org/cgi/content/full/104/5/e54
16. Shaw KN, McGowan KL, Gorelick MH,Schwartz JS. Screening for urinary tract in-fection in infants in the emergency depart-ment: which test is best? Pediatrics . 1998;101(6). Available at: www.pediatrics.org/cgi/content/full/101/6/e1
17. Herr SM, Wald ER, Pitetti RD, Choi SS. En-hanced urinalysis improves identicationof febrile infants ages 60 days and youngerat low risk for serious bacterial illness. Pe- diatrics . 2001;108(4):866–871
18. Nigrovic LE, Malley R, Macias CG, et al. Ef-fect of antibiotic pretreatment on cere-
brospinal uid proles of children withbacterial meningitis. Pediatrics . 2008;122(4):726–730
19. Nigrovic LE,KuppermannN, MaciasCG, et al.Clinical prediction rule for identifying chil-dren with cerebrospinal uid pleocytosis atvery low risk of bacterial meningitis. JAMA.2007;297(1):52–60
20. Shah SS,ZorcJJ, LevineDA, Platt SL,Kupper-mann N. Sterile cerebrospinal uid pleocy-tosis in young infants with urinary tract in-fections. J Pediatr . 2008;153(2):290–292
21. DeAngelis C, Joffe A, Wilson M, Willis E. Iatro-
genic risks and nancial costs of hospitaliz-ing febrile infants. Am J Dis Child . 1983;137(12):1146–1149
22. Crain EF, Gershel JC. Urinary tract infections infebrileinfants younger than 8 weeks of age. Pe- diatrics . 1990;86(3):363–367
23. Bonadio WA, Smith DS, Madagame E, MachiJ, Kini N. Escherichia coli bacteremia inchildren: a review of 91 cases in 10 years.Am J Dis Child . 1991;145(6):671–674
24. Ginsburg CM, McCracken GH Jr. Urinarytract infections in young infants. Pediatrics .1982;69(4):409– 412
25. Kaplan RL, Harper MB, Baskin MN, MaconeAB, Mandl KD. Time to detection of positivecultures in 28- to 90-day-old febrile infants.Pediatrics . 2000;106(6). Available at: www.pediatrics.org/cgi/content/full/106/6/e74
26. BonadioWA, SmithDS, Mathews S, RockA.Clini-calsignicanceofnewly documented neutrope-nia in febrileyounginfantsevaluatedforsepsis.PediatrInfectDisJ . 1991;10(5):407–408
27. PaulM,Gafter-GviliA,LeiboviciL,etal. The epide-miology of bacteremia withfebrileneutropenia:experience from a single center, 1988–2004. Isr Med Assoc J . 2007;9(6):424– 429
TABLE 4 Bivariate and Multivariate Adjusted Odds Ratios for Predictors of Bacteremia in theRecursive Partitioning Analysis
Variable Unadjusted OddsRatio (95% CI)
P Adjusted OddsRatio (95% CI)
P
Clinically ill in ED 1.6 (1.1–2.4) .02 1.5 (0.9–2.3) .117High-risk past medical
history1.7 (1.1–2.6) .016 1.5 (0.9–2.5) .105
Peripheral bands at1250 cells per L 2.7 (1.8–4.2) .001 3.8 (2.3–6.2) .001
Peripheral ANC of 1500 cells per L
3.0 (1.5–5.8) .002 9.0 (4.0–19.9) .001
1082 SCHNADOWER et al. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from
8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 11/12
APPENDIX Keywords Used by Site Assessors to Determine Physical Examination Variables
Variable Denition
AppearanceWell “Well appearing,” “no apparent distress,” “alert,” “normal mental status,” “interactive,” “smiling”Ill “Sick,” “toxic,” “shocky,” “decreased mental status,” “lethargic,” “unresponsive,” “irritable,” “fussy,” “inconsolable,” “not looking well,”
“meningitic,” “positive Kernig,” “positive Brudzinski,” “stiff neck,” “petechial rash,” “poor or decreased perfusion,” “decreasedpulses”
DehydrationYes “Dry appearing,” “dry mucous membranes,” “tented skin,” “sunken eyes,” “sunken fontanelle”No “Well hydrated,” “not dehydrated,” “presence of tears,” “moist mucous membranes,” “anterior fontanelle at,” “well perfused”
Respiratory distressYes Respiratory rate 80 breaths per min, “retractions,” “pulling,” “nasal aring,” “increased respiratory effort,” “difculty breathing,”
“grunting”No “Breathing comfortably,” “calm breathing,” “normal respiratory effort”
(Continued from rst page)
KEY WORDSurinary tract infections, infants, bacteremia, meningitis, emergency department, hospitalization, outpatient therapy
ABBREVIATIONSUTI urinary tract infectionED emergency departmentCFU colony-forming unit(s)WBC white blood cellCSF cerebrospinal uidCI condence interval
ANC absolute neutrophil count
This work was presented at the annual meetings of the American Academy of Pediatrics National Conference and Exhibition; October 10, 2008; Boston, MA; andOctober 16, 2009; Washington, DC.
www.pediatrics.org/cgi/doi/10.1542/peds.2010-0479
doi:10.1542/peds.2010-0479
Accepted for publication Aug 16, 2010
Address correspondence to David Schnadower, MD, MPH, Division of Pediatric Emergency Medicine, Washington University School of Medicine, 660 S Euclid Ave,Campus Box 8116, St. Louis, MO 63130. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no nancial relationships relevant to this article to disclose.
ARTICLES
PEDIATRICSVolume 126, Number 6 , December 2010 1083. Provided by University of Pennsylvania Library on December 29, 2010www.pediatrics.orgDownloaded from

8/7/2019 1074 ITU bajo riesgo de bacteriemia en infantes
http://slidepdf.com/reader/full/1074-itu-bajo-riesgo-de-bacteriemia-en-infantes 12/12
DOI: 10.1542/peds.2010-04792010;126;1074-1083; originally published online Nov 22, 2010;Pediatrics
CommitteeAcademy of Pediatrics Pediatric Emergency Medicine Collaborative Research
M. Plymale, Patrick Solari, Deborah J. Mann, Peter S. Dayan and for the American JenniferBlackstone, Amit Sarnaik, Julie McManemy, Alison Brent, Jonathan Bennett,
Blake Bulloch, Dewesh Agrawal, Mary Saunders, Donna M. Sutherland, Mercedes M.Marc N. Baskin, Paul Ishimine, Camille Scribner, Pamela Okada, Heather Beach,
David Schnadower, Nathan Kuppermann, Charles G. Macias, Stephen B. Freedman, Events and Bacteremia
Febrile Infants With Urinary Tract Infections at Very Low Risk for Adverse
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/126/6/1074including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/126/6/1074#BIBLat:This article cites 22 articles, 14 of which you can access for free
Subspecialty Collections
http://www.pediatrics.org/cgi/collection/infectious_disease Infectious Disease & Immunity
following collection(s):This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at:Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be fou nd online:
P id d b U i it f P l i Lib D b 29 2010di t iD l d d f