1 psychiatric perspectives in children psychiatric perspectives in children with special educational...
TRANSCRIPT

1
Psychiatric Perspectives in Children Psychiatric Perspectives in Children
with Special Educational Needswith Special Educational Needs
Prof Maurice PlaceProf Maurice Place
Copy of Presentation @ Copy of Presentation @ www.tinyurl.com/www.tinyurl.com/yzp2axyyzp2axy
[email protected]@northumbria.ac.uk

2
James 14 yrs
Presentation - A good student until 18 months ago,
now poor work and frequently not handing in homework
violent outbursts at school for last few months
- excluded from school following an assault on teacher.

3
Becky 14 yrs
Presentation -Always a rather quiet girl, but not prompted concern until now
- recently more withdrawn – at break times either alone
or with “smoking group”
- says being bullied at school
- frequent arguments with mother about friends she’s out with,
time in etc.

4
What do you think is going on?
Do either of these cases require referral to a professional?
What would you expect the professional to achieve?

5
Issues of Diagnosis in Mental HealthIssues of Diagnosis in Mental Health

6
What Constitutes a Problem?
7
What Constitutes a Problem?
Who’s Problem is it?

8
What Constitutes a Problem?
Who’s Problem is it?
The Child
The Parent
The Teacher
“Society”
9
How to define it?

10
How to define it?
Unit 1 the child is frightened of going to school Unit 2 an unwritten contract between two people. The child is frightened to separate from mother Unit 3 triangular relationships - coalitions & alliances. The child is in close alliance with mother and her "problem" of school attendance takes precedence over marital difficulties

11
How to define it?
Unit 1 the child is frightened of going to school Unit 2 an unwritten contract between two people. The child is frightened to separate from mother Unit 3 triangular relationships - coalitions & alliances. The child is in close alliance with mother and her "problem" of school attendance takes precedence over marital difficulties
Probably two elements - school issues & family themes conspiring to produce non-attendance (Perugi et al 1988; Last & Strauss 1990)

12
What Constitutes a Problem?

13
• memory
• thought
• mood
• hallucinations - visual - tactile - auditory

14
• delusions
• behaviour
• vegetative

15
Let us consider:Let us consider:
A white english man who is referred because he is telling
his GP that he has had a message from God and been told to
give away all his possessions and preach on street corners.

16
Let us consider:Let us consider:
A white english man who is referred because he is telling
his GP that he has had a message from God and been told to
give away all his possessions and preach on street corners.
He is - a heavy drinker
- the managing director of an engineering firm.

17
Let us consider:Let us consider:
A white english man who is referred because he is telling
his GP that he has had a message from God and been told to
give away all his possessions and preach on street corners.
He is - an anglican vicar
- his wife has recently died

18
Disorder is characterised by:Disorder is characterised by:
atypical behaviour and/or distressatypical behaviour and/or distress
AND
dysfunction dysfunction
which is - persistent & severe
(Lask 2003)

19
How do these “adult concepts” apply to children?

20
Disorder is characterised by:Disorder is characterised by:
atypical behaviour and/or distressatypical behaviour and/or distress
AND
dysfunction dysfunction
which is - persistent & severe
(Lask 2003)

21
• Parenting Quality
• Family Dynamics
• Developmental Themes
• Friendships & Their Influences
• School Performance
Elements considered in assessment

22
So what of our two initial cases?
23
James 14 yrs
Presentation - A good student until 18 months ago, now poor work and frequently not handing in homework violent outbursts at school for last few months - excluded from school following an assault on teacher.
violent outbursts at home over same period. - frequent arguments with mother - “walking on egg-shells all the time”. 2 episodes where threatened to cut own throat with knife.

24
Presentation
Family & History - Only child. Parents separated 3 yrs ago. Marriage acrimonious & violent, sometimes towards James. Developmental milestones average. As junior - good peers, school attendance & performance. Weekend contact to dad - James tries to avoid going.
James 14 yrs

25
Presentation
Family & History.
Examination - Truculent, quick to angry responses. Never out with friends, only goes out with mother since exclusion. Spends most of day watching TV. Eating - not eating for 2 days then binges. Sleep - bed after midnight, to sleep in early hours, wakes at lunchtime. Says he is “sick of my life” & gets weepy when thinks of it.
James 14 yrs

26
Becky 14 yrs
Presentation -Always a rather quiet girl, but not prompted concern until now
- recently more withdrawn – at break times either alone
or with “smoking group”
- says being bullied at school
- frequent arguments with mother about friends she’s out with,
time in etc. - constant conflict with mother for 18 mths, most recent about hiding stolen mobile phone.
- mother feels losing control of daughter.

27
Presentation
Family & History - Older sister allies with mother - fights with Becky. Father works away during week; mother works and seen by everyone as manager of family. Developmental milestones early. As junior - good peers, school attendance fine & seen as high flyer. Helpful round the house. Favourite aunt died in car accident 2 yrs ago.
Becky 14 yrs

28
Examination Quietly spoken, minimising issues, but is worried by loss of temper. Feels parents are constantly “on her back”. Sees dead aunt “covered in blood” who tells her life will get worse. Eating - episodes of over-eating - has sometimes been sick afterwards because of amount. Sleep - awake until 3 am, grumpy in mornings. Weeps quite frequently but she always ascribes to life events. School performance poor in recent months - “can’t be bothered… ...don’t see the point”. Interests - used to horse ride; friendships reduced to 2 – both frequently excluded from school for disruptive behaviour.
Becky 14 yrs

29
Differential Diagnoses
• depression
• conduct disorder/ opposition defiance
• adolescent challenge/ rebellion
• PTSD (James)
• abnormal bereavement reaction (Becky)

30

31
5 or more of:-5 or more of:-
1) Depressed mood Depressed mood as indicated by either subjective report (e.g. as indicated by either subjective report (e.g.
feels sad or empty) or observation made by others (e.g. tearful). feels sad or empty) or observation made by others (e.g. tearful).
In young people can be irritable mood.In young people can be irritable mood.
2) Markedly diminished Markedly diminished interest in activities.interest in activities.
3) Significant change in weight or appetite.Significant change in weight or appetite.
4) InsomniaInsomnia..
5) Psychomotor agitation or retardationPsychomotor agitation or retardation as observed by others. as observed by others.
6) Fatigue or loss of energyFatigue or loss of energy..
7) Feelings of worthlessness or guilt Feelings of worthlessness or guilt (which may be delusional).(which may be delusional).
8) Diminished ability to think or concentrate.Diminished ability to think or concentrate.
9) Recurrent thoughts of death.Recurrent thoughts of death.

32
James
1) Depressed mood/irritability Depressed mood/irritability x
2) Markedly diminished interest in activities.Markedly diminished interest in activities. x
3) Significant change in weight or appetite. Significant change in weight or appetite. x
4) InsomniaInsomnia. . x
5) Psychomotor agitation/retardation. Psychomotor agitation/retardation. -
6) Fatigue or loss of energyFatigue or loss of energy. . x
7) Feelings of worthlessness or guiltFeelings of worthlessness or guilt. . -
8) Diminished ability to think or concentrate. Diminished ability to think or concentrate. x
9) Recurrent thoughts of death. Recurrent thoughts of death. ?
33
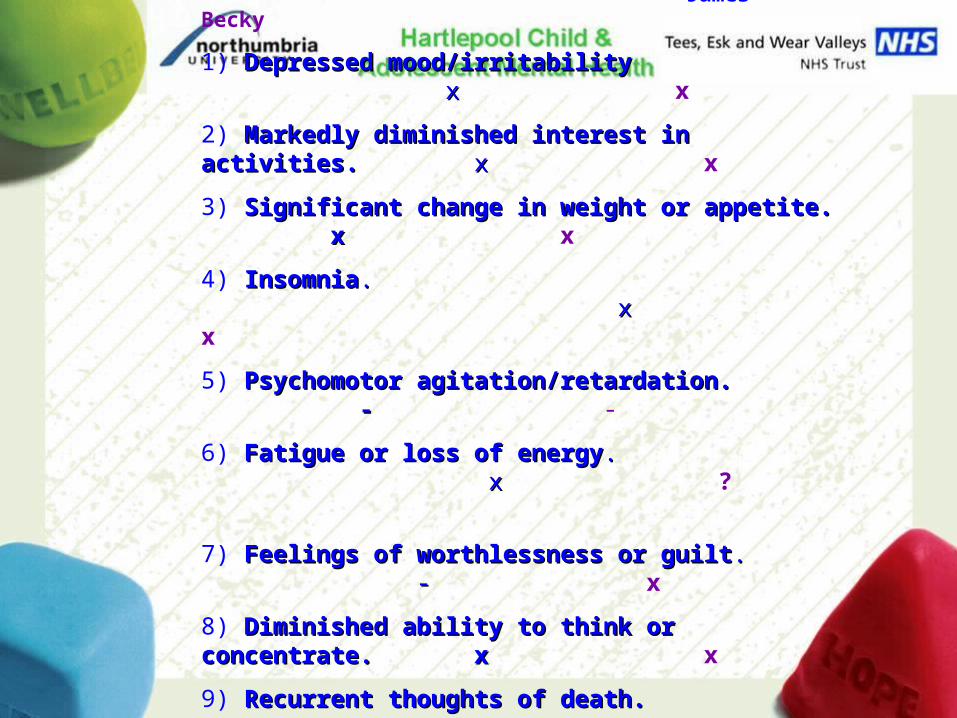
James Becky
1) Depressed mood/irritability Depressed mood/irritability x x x
2) Markedly diminished interest in activities.Markedly diminished interest in activities. x x x
3) Significant change in weight or appetite. x Significant change in weight or appetite. x x
4) InsomniaInsomnia. x . x x
5) Psychomotor agitation/retardation. - Psychomotor agitation/retardation. - -
6) Fatigue or loss of energyFatigue or loss of energy. x . x ?
7) Feelings of worthlessness or guiltFeelings of worthlessness or guilt. - . - x
8) Diminished ability to think or concentrate. x Diminished ability to think or concentrate. x x
9) Recurrent thoughts of death. ? Recurrent thoughts of death. ? x

34
Causes of Disturbance and Distress
Intrinsic - - e.g. birth trauma, epilepsy, ADHD, Pervasive
Developmental Disorder

35
Intrinsic
Parenting problems - failed system - - abusive, neglectful
- flawed system - - parental disagreement
- flawed delivery - - inconsistent
Causes of Disturbance and Distress

36
Intrinsic
Parenting problems
Aggressive maritals exaggerated emotions, poor self esteem,
aggressive with peers
Causes of Disturbance and Distress

37
Intrinsic
Parenting problems
Aggressive maritals
Alcohol / drug abuse in parents aggressive, poor emotional
control, moodiness, depression
Causes of Disturbance and Distress

38
Intrinsic
Parenting problems
Aggressive maritals
Alcohol / drug abuse in parents
Other adverse life events - bereavement
Causes of Disturbance and Distress

39
Intrinsic
Parenting problems
Aggressive maritals
Alcohol / drug abuse in parents
Other adverse life events – bereavement
divorce
Causes of Disturbance and Distress

40
Intrinsic
Parenting problems
Aggressive maritals
Alcohol / drug abuse in parents
Other adverse life events – bereavement
divorce
significant bullying
Causes of Disturbance and Distress

41
Intrinsic
Parenting problems
Aggressive maritals
Alcohol / drug abuse in parents
Other adverse life events – bereavement
divorce
significant bullying
abuse/trauma
Causes of Disturbance and Distress

42
Prevalence of Disorders
Overall prevalence
12% in the pre-adolescent age group (Kolvin et al., 1981)
25% in the adolescent population (Macmillan et al., 1980; Place et al., 1985)
Most not involved with mental health services (Offord et al., 1987; Rutter, Tizard, & Whitmore, 1970)
but a significant proportion do attend social services and primary care settings
(Kurtz, Thornes, & Wolkind, 1994).

43
Prevalence of Specific Disorders
Anxiety disorders - 12%
Disruptive conduct disorders-10%
Depression 6% (increasing in adolescence)
Attention deficit hyperactivity disorder (ADHD) - 3%
Pervasive developmental disorders 1%
Psychoses are rare, affecting less than 1 %
Prevalence of Disorders

44
Issues of Diagnosis in Our Issues of Diagnosis in Our Two CasesTwo Cases

45
Oppositional Defiance
• losing one's temper
• arguing with adults
• actively defying or refusing to comply with rules
• deliberately doing things that will annoy others
• blaming others for his misbehaviour
• being touchy or easily annoyed by others
• being angry and resentful
• being spiteful or vindictive

46
Oppositional Defiance
Child’s Temperament difficult, unadaptive (Bates et al. 1991).
Parents conflict destructive, rather than divorce per se (O'Leary and Emery 1982)
unemployment, divorce & poverty more prevalent (Webster–Stratton 1993)
fewer positive behaviours towards their children
more likely to threaten, criticise, and humiliate their children
less likely to monitor their children's behaviours
don't give enough time to comply with commands (Delfini et al. 1976; Forehand et al. 1975; Webster–Stratton and Spitzer 1991).

47
Conduct Disorder
Oppositional Defiance elements with -
aggression towards othersdestruction of property theft and deceit
If emerge in early years then a distinctly different group from those where emerges in adolescence.

48
Conduct Disorder
Severe conduct disorder associated with drug misuse, criminality, affective illness and youth suicide (Loeber et al., 2000)
If emerge in early years then a strong link with development of antisocial personality disorder (Frick, 1998). Rates of conduct disorder (adolescent emergence) are increasing quite dramatically (Loeber & Farrington, 1998; Smith, 1995).

49
conduct disorder should be viewed as the most
important area for mental health services to
concentrate their efforts in order to find effective
interventions (Werry 2000)

50
Child -focussed Treatments Task orientated - social skills, self esteem
Individual psychotherapy
Behaviour management
Drug therapy

51
Child -focussed Treatments Task orientated - social skills, self esteem
Individual psychotherapy
Behaviour management
Drug therapy
– do medicines have a role?

52
? When would meds be appropriate to
change classroom behaviour
and when would it not

53
Why treat these children?Why treat these children?• Presents a persistent and severe impairment of
psychological development
• The negative impact of a high level of inattentiveness, restless and impulsive behaviour upon functioning
• Increased risk (x4) of substance misuse later in life
(Biederman et al 1999)

54
Heritability from twin studies 65 – 90% (Thapar et al 2001)
Parents and siblings x4 more likely to have ADHD also (Faraone et al 2000)

55
MTA Study Results (n = 579 Children)
Meds had strongest effect on the core symptoms of ADHD - adding psychosocial treatment did not improve effects
- in non-ADHD areas combining behavioural and medicine showed a modest advantage over medication alone

56
Methylphenidate has a therapeutic to toxic ratio of 100:1
making it one of the safest paediatric drugs on the market
(Greenhill 1992)

57
Monotherapy- methylphenidate – Concerta, Equasym, Medikinet or dexamfetamine - Vyvanse
Antidepressant – Bupropion (McCellan & Werry 2003)
Alpha agonists – clonidine (Riddle et al 1999) guanfacine (Posey & McDougle 2007)
maintenancemaintenance
Texas Treatment Algorithm
NSRI - Atomoxetine (Kratochvil et al 2002)
Antidepressant (2) – imipramine (Geller et al 1999)

58
OutcomesOutcomes
Stimulants improve 70% of children (Miller 2002)
Reduce overactivity & impulsivity; increase academic productivity & cognitive functioning (O’Toole et al 1997)
Improves social interaction and sensitivity in perceiving communications (Wilens et al 2007)
85% reduction in drug misuse if treated (Biederman et al 2007)

59
60
(NICE) Guidance on ADHD Treatments
ADHD affects children and adolescents in different ways and degrees but the consequences of severe ADHD can be serious both for the individual and family
Children with severe ADHD often have low self esteem, develop emotional and social problems, and frequently underachieve at school
ADHD may persist into adolescence and adulthood and is often associated with continuing emotional and social problems, substance misuse, unemployment and involvement in crime
www.nice.org.uk
61
Onset in early childhood,
but up to 70% of children may have
difficulties into adulthood
(Searight et al 2000; Clarke et al 2005; Kooij et al 2005)

62
Child -focussed Treatments Task orientated - social skills, self esteem
Individual psychotherapy
Behaviour management
Drug therapy
– Risperidone increasingly recognised as an effective
intervention for Conduct Disorder
(Pappadopulos et al., 2003;European Consensus 2007)

63
treatment ___ control
improvement improvement
Effect size = ------------------------------------------Effect size = ------------------------------------------
((dd) pooled standard) pooled standard
deviationdeviation

64
Effect Size
less than 0.5 = small effect
0.5 – 0.80.5 – 0.8 = medium effect= medium effect
greater than 0.8greater than 0.8 = large effect= large effect
65
Effect Size
less than 0.5 = small effect
0.5 – 0.80.5 – 0.8 = medium effect= medium effect
greater than 0.8greater than 0.8 = large effect= large effect
Risperidone’s reduction of Risperidone’s reduction of
conduct problems = 0.79 conduct problems = 0.79
(Aman et al 2004)

66
Child -focussed Treatments
Parent -focussed Treatments parent training courses
marital therapy (Relate)
problem focussed - e.g. alcoholism

67
Child -focussed Treatments
Parent -focussed Treatments
Family-focussed Treatments Solution focussed therapy
Family therapy
68
Do they work?Do they work?

69
Effect Size
less than 0.5 = small effect
0.5 – 0.80.5 – 0.8 = medium effect= medium effect
greater than 0.8greater than 0.8 = large effect= large effect

70
Depression - Adults
Psychotherapy – minor 0.83 major 0.02
(Pinquart et al 2006)
Cognitive Behaviour Therapy 0.82 (Cuijpers 1997)
Medication (SSRI) 0.55 (Otto et al 2001)

71

72

73
Depression – Child & Adolescent
Psychotherapy – 0.34 (Weisz et al 2006)
Cognitive Behaviour Therapy 0.32
Medication (SSRI) 0.68
-- combined 0.98 (March et al 2006)

74
Can these children be managed
in mainstream classrooms?

75

76
Questions?Questions?