xarelto clinical trial brochure
DESCRIPTION
Xarelto, rivaroxaban, noacTRANSCRIPT

© Bayer HealthCare Pharmaceuticals August 2013
BHP/100445/0613 L.NL.GM.08.2013.0187
Clinical Trials in the Venous Arterial Thromboembolic (VAT) Space

Disclaimer: Rivaroxaban is an oral, direct Factor Xa inhibitor and marketed as Xarelto®. The marketing authorization for Xarelto® may vary from country to country. In the European Union, Xarelto® is approved for the:
· Prevention of venous thromboembolism (VTE) in adult patients undergoing elective hip- or knee replacement surgery
· Prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrilliation with ≥1 risk factor, such as congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, earlier stroke or TIA (transient ischaemic attack)
· Treatment of deep vein thrombosis (DVT) and prevention of recurrent DVT and pulmonary embolism (PE) in adults
· Treatment of PE and prevention of recurrent DVT and PE in adults
· Prevention of atherothrombotic events (cardiovascular death, myocardial infarction or stroke) after an acute coronary syndrome (ACS) in adult patients with elevated cardiac biomarkers when co-administered with acetylsalicylic acid (ASA) alone or with ASA plus clopidogrel or ticlopidine
Whilst licenses may differ from country to country, across all indications Xarelto® is approved in more than 120 countries. Xarelto® was discovered by Bayer HealthCare, and is being jointly developed with Janssen Research & Development, LLC. Xarelto® is marketed outside the U.S. by Bayer HealthCare and in the U.S. by Janssen Pharmaceuticals, Inc. (a Johnson & Johnson Company).
Anticoagulant medicines are potent therapies used to prevent or treat serious illnesses and potentially life threatening conditions. Before initiating therapy with anticoagulant medicines, physicians should carefully assess the benefit and risk for the individual patient. Responsible use of Xarelto® is a high priority for Bayer, and the company has developed a Prescribers Guide for physicians and a Xarelto® Patient Card for patients to support best practices.
Xarelto® is a registered trademark of Bayer HealthCare Pharmaceuticals AG
To learn more, please visit: https://prescribe.xarelto.comTo learn more about thrombosis, please visit www.thrombosisadviser.comTo learn more about Xarelto, please visit www.xarelto.com
References
26
28
32
1
Xarelto®: Clinical Trials in the Venous Arterial Thromboembolic (VAT) Space
Introduction
Studies in Arterial Thromboembolism
Studies in Venous Thromboembolism
2
6
10
14
14
14
20
22
24

2 3
Xarelto is at the forefront of a new generation of oral anticoagulants targeting the high level of unmet medical need in the management of acute and chronic venous and arterial thromboembolic disease. The extensive Clinical Development Programme for Xarelto makes it the most studied, oral, direct Factor Xa inhibitor to date, with more than 100,000 patients in the Clinical Programme.1
Advancing the Management of SPAF and ACSsp*
In the rigorous, double-blind ROCKET AF study, once-daily Xarelto was non-inferior to warfarin for the prevention of stroke or non-CNS systemic embolism in patients with non-valvular atrial fibrillation (AF).2 Overall bleeding rates for Xarelto and warfarin were comparable, but importantly, intracranial and fatal bleeding were significantly lower with Xarelto.
The results of the ATLAS ACS 2 TIMI 51 study have opened a new perspective. Xarelto (2.5 mg and 5 mg BID), in combination with standard antiplatelet therapy, acetylsalicylic acid (ASA) alone or ASA in combination with clopidogrel or ticlopidine, was tested for secondary prevention in patients with ACS. The study demonstrated that the addition of Xarelto® 2.5 mg BID to standard antiplatelet therapy significantly reduced the composite primary efficacy endpoint of CV death, MI or stroke in patients after a recent ACS compared to those who received standard antiplatelet therapy alone.
Delivering Efficacy and Safety in VTE Treatment and Prevention
The results of studies in the management of venous thromboembolic disease showed that Xarelto offers significant benefits in the prevention of venous thromboembolism (VTE) following elective hip or knee replacement surgery (RECORD studies), in the treatment of patients with deep vein thrombosis (DVT) or pulmonary embolism (PE) (EINSTEIN DVT and EINSTEIN PE), and in the long-term secondary prevention of VTE (EINSTEIN EXT).
In the RECORD studies Xarelto 10 mg once daily was consistently superior to subcutaneous enoxaparin in preventing VTE and showed a comparable safety profile.3,4,5 In both EINSTEIN DVT and PE studies the single-drug solution with Xarelto has been shown to be a simple and effective alternative to the demanding dual-drug approach of injectable low molecular weight heparin (LMWH) followed by dose-adjusted vitamin K antagonist (VKA), without compromising safety.6,7 Indeed, in EINSTEIN PE there were significantly fewer major bleeds with Xarelto. In the EINSTEIN EXT study Xarelto significantly reduced the recurrence of DVT and PE compared with placebo, and importantly there was no significant difference in the occurrence of major bleeding.6
Clinical use Patients Randomised Outcomes Status / Findings
NEJM 2008
THE LANCET 2008
NEJM 2008
THE LANCET 2009
Primary Prevention of VTE: Hip Replacement Surgery
4,541
Efficacy: Composite of any deep vein thrombosis (DVT), non-fatal pulmonary embolism (PE), and all cause mortality.
Safety: Major bleeding
Superior efficacy to enoxaparin, comparable safety3
2,509Superior efficacy of long term (5 week) prophylaxis with rivaroxaban to short term (2 week) prophylaxis with enoxaparin, comparable safety9
Primary Prevention of VTE: Knee Replacement Surgery
2,531Superior efficacy to enoxaparin, comparable safety4
3,148Superior efficacy to enoxaparin, comparable safety5
NEJM 2010
NEJM 2012
NEJM 2010
Treatment of Deep Vein Thrombosis
3,449Efficacy: Symptomatic recurrent VTE
Safety: Composite of major and clinically relevant non-major bleeding
Equivalent efficacy to enoxaparin/ VKA, comparable safety6
Treatment of Pulmonary Embolism
4,833
Efficacy: Symptomatic recurrent VTE
Safety: Major bleeding
Equivalent efficacy to enoxaparin/ VKA, comparable safety7
Secondary Prevention of Venous Thromboembolism
1,197 Superior to placebo, comparable safety6
NEJM 2012
CIRC J 2012
NEJM 2011 Stroke Prevention in Atrial Fibrillation
14,264 Efficacy: Composite of stroke and non-CNS systemic embolism
Safety: Composite of major and clinically relevant non-major bleeding
Non inferior to warfarin and comparable safety2
1,280The primary endpoint of this study – to demonstrate comparable safety to warfarin – was achieved10
(J-ROCKET AF was not powered to test for differences in clinical efficacy)
Secondary Prevention in Acute Coronary Syndrome
15,526
Efficacy: Composite of CV death, MI, and stroke
Safety: Major bleeding events not associated with CABG surgery
Superior to dual antiplatelet therapy alone. Higher rates of TIMI major bleeding not associated with CABG but no increased risk of fatal bleeding8
Venous indicationsArterial indications
Advancing the Management of Venous Arterial Thromboembolism
* SPAF = Prevention of Stroke in Atrial FibrillationACSsp = Secondary Prevention of Acute Coronary Syndrome

4 5
Studies in Arterial Thromboembolism
Studies in Arterial Thromboembolism
SPA
F
Prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation with ≥1 risk factor, such as congestive heart failure, hypertension, age ≥ 75 years, diabetes mellitus,prior stroke or transient ischaemic attack (TIA)

6
3
5
1
4
2
0
Cum
ulat
ive
even
t ra
te (%
)
0 120 240 360 600 720 840
Time to event (days)480
warfarinXareltoHR=0.88 (95% CI 0.74-1.03)p<0.001 (non-inferiority)p=0.12 (superiority)
6
3
5
1
4
2
0
Cum
ulat
ive
even
t ra
te (%
)
0 120 240 360 600 720 840
Time to event (days)480
warfarinXareltoHR=0.79 (95% CI 0.66-0.96)p<0.001 (non-inferiority)
warfarin Xarelto
20
10
15
5
0
14.5 14.9
Even
t ra
te (%
per
yea
r)
not significant
warfarin Xarelto
1.0
0.5
0
0.7
0.5
Even
t ra
te (%
per
yea
r)
p=0.02
warfarin Xarelto
1.0
0.5
0
0.5
0.2
Even
t ra
te (%
per
yea
r)
p=0.003
N=14,264
Xarelto 20 mg once daily
Xarelto 15 mg once daily(CrCL 30–49 mL/min at entry)
R
warfarin target INR of 2.5 (INR range 2–3)
Included non-valvular AF patients with:
History of stroke, TIA, or non-CNS systemic embolism
OR
≥2 of the followingstroke risk factors:*• Heart failure • Hypertension• Age ≥75 years• Diabetes
Randomisation
Double-blind treatment 2-year median follow-up
End
of
stu
dy
* Enrollment of patients without prior stroke, TIA, or systemic embolism and only 2 factors capped at 10%.
6 7
CI = Confidence Interval HR = Hazard Ratio RRR = Relative Risk Reduction TTR = Time in Therapeutic RangeROCKET AF = Xarelto Once-daily oral direct Factor Xa inhibition Compared with vitamin K antagonism for the preventionof stroke and Embolism Trial in Atrial Fibrillation
Major bleeding was defined as clinically overt bleeding associated with any of the following: Fatal outcome, fall in haemoglobin ≥2 g/dl, transfusion of ≥2 units of whole blood or packed red cells, involvement of a critical anatomical site (intracranial, spinal, ocular, pericardial, articular, intramuscular with compartment syndrome, or retroperitoneal) or permanent disability. Non-major clinically relevant bleeding was defined as overt bleeding that did not meet the criteria for major bleeding but required medical intervention, unscheduled contact (visit or telephone) with a physician, temporary cessation of study drug, pain or impairment of activities of daily life.
* Safety on-treatment Population
performed in the intention-to-treat population. The principal safety outcome was the composite of major and non-major clinically relevant bleeding events.
Results
Once-daily Xarelto met the primary efficacy endpoint of non-inferiority compared with warfarin. This was achieved with a mean TTR of 55% among the patients taking warfarin, reflecting among other factors the high degree of comorbidity of the randomised patients.2
Overall bleeding rates were comparable between Xarelto and warfarin. Importantly, patients receiving Xarelto experienced significantly fewer intracranial haemorrhages and fatal bleeding events – the bleeding events of most concern to clinicians – compared with those receiving warfarin. Xarelto showed significantly more drops in haemoglobin levels of 2 g per deciliter or more, and increased transfusion rates, than warfarin. Patients receiving Xarelto experienced more mucosal bleeding events, which included significantly more upper GI, lower GI and rectal bleeds than those receiving warfarin.
There was no significant difference in the rates of MI, vascular death, and all-cause mortality between Xarelto and warfarin.2,18
In the ROCKET AF study, once-daily Xarelto met the primary endpoint of non-inferiority compared to warfarin in patients with non-valvular AF at risk of stroke.2 Overall bleeding rates were comparable between Xarelto and warfarin. Importantly, rates of fatal and intracranial bleeding were lower in patients receiving Xarelto.
Rationale
Atrial fibrillation (AF) has been shown to increase the risk of ischaemic stroke four to fivefold, and approximately 25% of patients who experience ischaemic stroke have AF.11,12 The incidence of AF-related stroke increases steadily with age, accounting for up to one third of strokes in those over 80 years of age.11-13 The vitamin K antaognist (VKA) can be effective in preventing strokes arising from AF.14-16 However, they are associated with a number of drawbacks and in consequence many patients remain at risk of stroke due to
inadequate anticoagulation.17 The aim of the ROCKET AF study was to compare the efficacy and safety of once-daily, oral Xarelto to dose-adjusted warfarin in the prevention of stroke and systemic embolism in patients with non-valvular AF at risk of stroke, and for whom guidelines recommend the use of oral anticoagulants.
Study Design
In the double-blind ROCKET AF study 14,264 patients with non-valvular AF were randomised to receive either Xarelto 20 mg once daily (15 mg once daily for patients with moderate renal impairment) or dose-adjusted warfarin.
Outcomes
The primary efficacy endpoint was the composite of all stroke and systemic embolism in the per-protocol on-treatment population. In addition, testing for non-inferiority and superiority was also
Intention-to-treat PopulationPer-protocol on-treatment Population
Intracranial Haemorrhage Fatal Bleeding
N ENGL J MED 2011; 365 (10): 883-891
Prevention of Stroke in Atrial Fibrillation (SPAF)
Study Design
Xarelto met its primary efficacy endpoint; it was non-inferior to warfarin for the primary composite endpoint of stroke and systemic embolism (p<0.001 for non-inferiority) in the per-protocol on-treatment population.
The rates of the principal safety outcome were similar for Xarelto and warfarin. Importantly, when compared to warfarin, Xarelto significantly reduced the incidence of the most devastating bleeds, intracranial haemorrhage and fatal bleeding.
u The findings of ROCKET AF indicate that once-daily Xarelto would be an effective alternative to warfarin for stroke prevention in patients with non-valvular AF
Principal Safety Outcome* Major and Non-Major Clinically Relevant Bleeding

8 9
Studies in Arterial Thromboembolism
Studies in Arterial Thromboembolism
Prevention of atherothrombotic events (cardiovascular death, myocardial infarction or stroke) after an acute coronary syndrome (ACS) in adult patients with elevated cardiac biomarkers when co-administered with acetylsalicylic acid (ASA) alone or with ASA plus clopidogrel or ticlopidine
AC
Ssp
0.2
n=9
0.1 0.1 0.1
n=6 n=5n=4
1.0
0.6
0.8
0.4
0.2
0
Perc
ent
(%)
Fatal Bleeding Fatal ICH
Placebo
Xarelto 2.5 mg BID (p=NS)
12
6
10
2
8
4
0
Cum
ulat
ive
even
t ra
te (%
)
0 6 12 18 24
Time to event (months)
Placebo
Xarelto 2.5mg and 5mg BID
10.7%
8.9%
HR = 0.84 95% CI = 0.74-0.96 mITT p = 0.008 ITT p = 0.002
5
3
1
4
2
0
Cum
ulat
ive
even
t ra
te (%
)
0 6 12 18 24
Time to event (months)
Placebo
Xarelto 2.5mg BID
4.5%
2.9%
HR = 0.68 95% CI = 0.53-0.87 mITT p = 0.002 ITT p = 0.004
p<0.001
0.6
1.8
3.0
1.5
2.0
2.5
1.0
0.5
0
Inci
denc
e (%
)
Placebo Xarelto2.5 mg BID
5
3
1
4
2
0
Cum
ulat
ive
even
t ra
te (%
)
0 6 12 18 24
Time to event (months)
Placebo
Xarelto 2.5mg BID
4.1%
2.7%
HR = 0.66 95% CI = 0.51-0.86 mITT p = 0.002 ITT p = 0.005
R
R
+ Placebo
Treatment period up to 31 months
+ Xarelto 2.5 mg BID
+ Xarelto 5 mg BID
End
of
tre
atm
ent
Stratum 1
ASA
+ Placebo
+ Xarelto 2.5 mg BID
+ Xarelto 5 mg BID
End
of
tre
atm
ent
Stratum 2
ASA andclopidogrel or
ticlopidine
Physician decides on Stratum
N=15,526 patients
7%
93%
10 11
BID = Twice dailyATLAS = Anti-Xa Therapy to Lower cardiovascular events in addition to ASA with/without thienopyridine therapy in subjects with Acute coronary Syndrome CI = Confidence Interval ITT = Intention To Treat* Acetylsalicylic acid (ASA) alone or ASA in combination with clopidogrel or ticlopidine In line with the EU Approval of Xarelto 2.5 mg BID for ACSsp, the charts focus on the 2.5 mg dosing regime data.
Secondary Prevention of Acute Coronary Syndrome (ACSsp)
Study Design
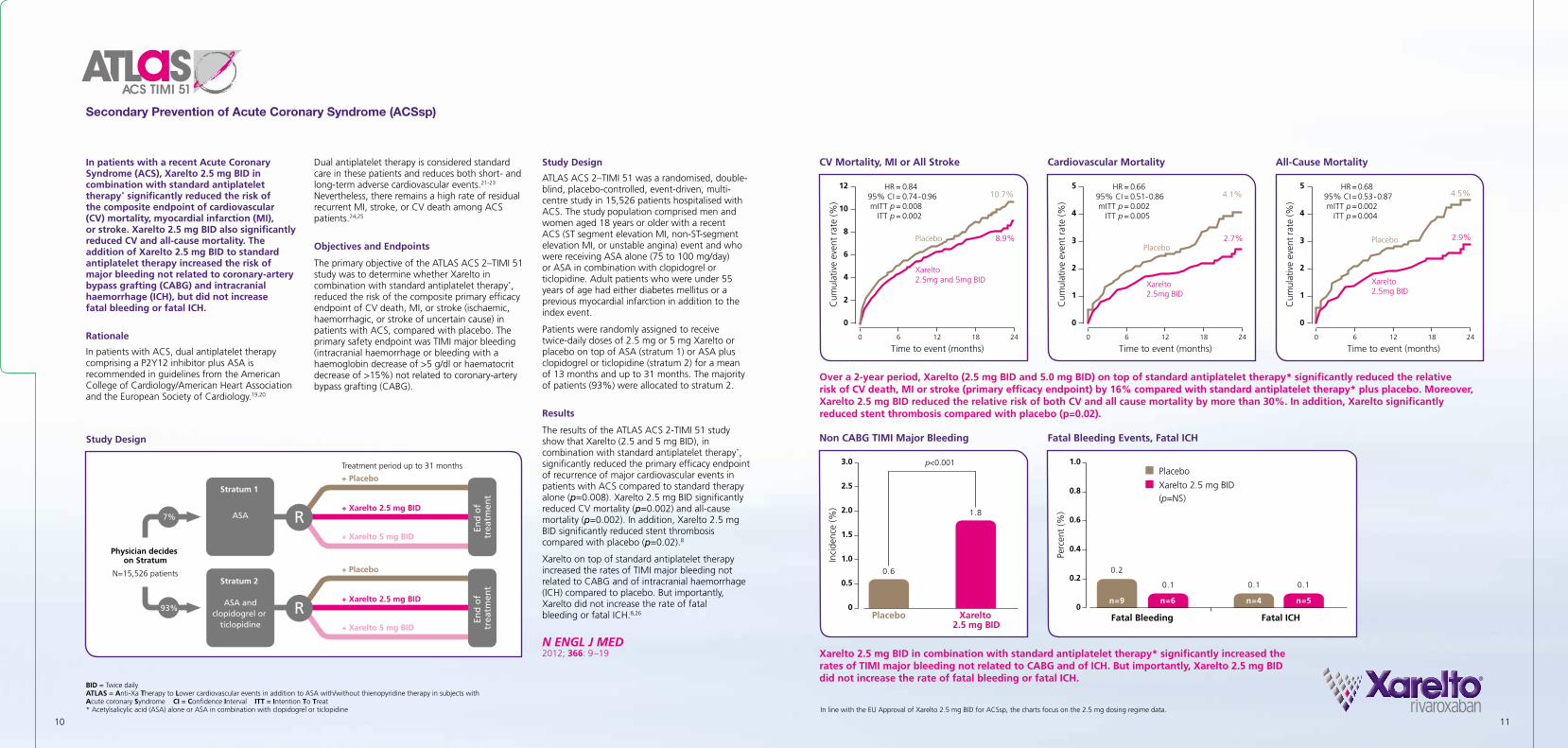
ATLAS ACS 2–TIMI 51 was a randomised, double-blind, placebo-controlled, event-driven, multi- centre study in 15,526 patients hospitalised with ACS. The study population comprised men and women aged 18 years or older with a recent ACS (ST segment elevation MI, non-ST-segment elevation MI, or unstable angina) event and who were receiving ASA alone (75 to 100 mg/day) or ASA in combination with clopidogrel or ticlopidine. Adult patients who were under 55 years of age had either diabetes mellitus or a previous myocardial infarction in addition to the index event.
Patients were randomly assigned to receive twice-daily doses of 2.5 mg or 5 mg Xarelto or placebo on top of ASA (stratum 1) or ASA plus clopidogrel or ticlopidine (stratum 2) for a mean of 13 months and up to 31 months. The majority of patients (93%) were allocated to stratum 2.
Results
The results of the ATLAS ACS 2-TIMI 51 study show that Xarelto (2.5 and 5 mg BID), in combination with standard antiplatelet therapy*, significantly reduced the primary efficacy endpoint of recurrence of major cardiovascular events in patients with ACS compared to standard therapy alone (p=0.008). Xarelto 2.5 mg BID significantly reduced CV mortality (p=0.002) and all-cause mortality (p=0.002). In addition, Xarelto 2.5 mg BID significantly reduced stent thrombosis compared with placebo (p=0.02).8
Xarelto on top of standard antiplatelet therapy increased the rates of TIMI major bleeding not related to CABG and of intracranial haemorrhage (ICH) compared to placebo. But importantly, Xarelto did not increase the rate of fatal bleeding or fatal ICH.8,26
In patients with a recent Acute Coronary Syndrome (ACS), Xarelto 2.5 mg BID in combination with standard antiplatelet therapy* significantly reduced the risk of the composite endpoint of cardiovascular (CV) mortality, myocardial infarction (MI), or stroke. Xarelto 2.5 mg BID also significantly reduced CV and all-cause mortality. The addition of Xarelto 2.5 mg BID to standard antiplatelet therapy increased the risk of major bleeding not related to coronary-artery bypass grafting (CABG) and intracranial haemorrhage (ICH), but did not increase fatal bleeding or fatal ICH.
Rationale
In patients with ACS, dual antiplatelet therapy comprising a P2Y12 inhibitor plus ASA is recommended in guidelines from the American College of Cardiology/American Heart Association and the European Society of Cardiology.19,20
Dual antiplatelet therapy is considered standard care in these patients and reduces both short- and long-term adverse cardiovascular events.21-23 Nevertheless, there remains a high rate of residual recurrent MI, stroke, or CV death among ACS patients.24,25
Objectives and Endpoints
The primary objective of the ATLAS ACS 2–TIMI 51 study was to determine whether Xarelto in combination with standard antiplatelet therapy*, reduced the risk of the composite primary efficacy endpoint of CV death, MI, or stroke (ischaemic, haemorrhagic, or stroke of uncertain cause) in patients with ACS, compared with placebo. The primary safety endpoint was TIMI major bleeding (intracranial haemorrhage or bleeding with a haemoglobin decrease of >5 g/dl or haematocrit decrease of >15%) not related to coronary-artery bypass grafting (CABG).
Study Design
CV Mortality, MI or All Stroke All-Cause Mortality
N ENGL J MED 2012; 366: 9–19
Cardiovascular Mortality
Fatal Bleeding Events, Fatal ICHNon CABG TIMI Major Bleeding
Over a 2-year period, Xarelto (2.5 mg BID and 5.0 mg BID) on top of standard antiplatelet therapy* significantly reduced the relative risk of CV death, MI or stroke (primary efficacy endpoint) by 16% compared with standard antiplatelet therapy* plus placebo. Moreover, Xarelto 2.5 mg BID reduced the relative risk of both CV and all cause mortality by more than 30%. In addition, Xarelto significantly reduced stent thrombosis compared with placebo (p=0.02).
Xarelto 2.5 mg BID in combination with standard antiplatelet therapy* significantly increased the rates of TIMI major bleeding not related to CABG and of ICH. But importantly, Xarelto 2.5 mg BID did not increase the rate of fatal bleeding or fatal ICH.

12 13
Studies in Venous Thromboembolism
Studies in Venous Thromboembolism
Treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and prevention of recurrent DVT and PE in adults
DV
Tx &
PEx

N=1,197
Treatment period 6 or 12 months
Xarelto 20 mg OD
R
Placebo
Randomisation
Day 30after last dose
Qualifying patientsreferred from outside
of the EINSTEINProgramme (47%)
Patients fromEINSTEIN DVTstudy (34%)
Patients fromEINSTEIN PEstudy (19%)
Follo
w u
p
End
of
trea
tmen
t
N=4,832*
* 4,833 pat ients were randomized but one pat ient was exc luded because of inval id consent
Eligible patientsN=3,449
Predefined treatment period of 3, 6, or 12 months
Xarelto 15 mg BID for three weeks
Xarelto 20 mg OD thereafter
R
enoxaparin BID for at least 5 days, plus VKA target INR 2.5 (INR range 2–3)
Randomisation
Day 1Day 30
after last dose
Acute DVT Study (EINSTEIN DVT)
Acute PE Study (EINSTEIN PE)
Acute symptomatic PEwith or without
symptomatic DVT
Acute symptomatic DVT
withoutsymptomatic PE
Follo
w u
p
End
of
trea
tmen
t
14 15
Acute symptomatic DVT without symptomatic PE (EINSTEIN DVT)
Acute symptomatic PE with or without symptomatic DVT (EINSTEIN PE).
The primary efficacy endpoint was symptomatic, recurrent VTE – the composite of recurrent DVT and fatal or non-fatal PE. The principal safety outcome was the combination of major and non-major clinically relevant bleeding.
Study Design
EINSTEIN DVT and EINSTEIN PE were designed as randomised, open-label, event-driven, non-inferiority studies, with a pre-defined study treatment duration of 3, 6, or 12 months.
Following randomisation, patients allocated to Xarelto received an oral 15 mg twice daily regimen for 21 days, followed by oral Xarelto 20 mg once daily – a regimen based on the phase II dose finding studies.28,29
The large EINSTEIN Programme was designed to investigate the clinical utility of Xarelto in the acute treatment and long term prevention of deep vein thrombosis (DVT) and pulmonary embolism (PE). The Programme comprised three studies involving almost 10,000 patients: EINSTEIN DVT, EINSTEIN PE, and EINSTEIN EXT.
EINSTEIN DVT and PE – Overview
EINSTEIN DVT and EINSTEIN PE were two independent studies sharing a single protocol to compare oral Xarelto with the dual-drug approach of enoxaparin/vitamin K antagonist (VKA) in patients with acute, symptomatic DVT6 or PE.7 EINSTEIN DVT included 3,449 patients and EINSTEIN PE 4,832 patients.
Rationale
In acute DVT or PE, current treatment is based on the dual-drug approach of an injectable anticoagulant, such as low molecular weight heparin (LMWH), unfractionated heparin (UFH), or fondaparinux, together with a VKA. The injectable anticoagulant should be discontinued when the international normalized ratio (INR) is ≥ 2.0 for at least 24 h (Grade 1A).27 EINSTEIN DVT and EINSTEIN PE were designed to investigate a new, oral single-drug solution with Xarelto as a potential replacement for dual-drug standard therapy in a large population of patients with DVT and PE.6,7
Objectives and Endpoints
The main objective in both studies was to determine whether Xarelto was at least as effective and safe as enoxaparin/VKA in the treatment of patients with:
EINSTEIN EXT – Overview
The EINSTEIN EXT (EXT = extension) study was designed to assess the relative efficacy and safety of Xarelto versus placebo in patients who had completed 6 to 12 months of anticoagulant treatment for their acute episode of VTE.6
Rationale
In a large proportion of patients who have completed 6 to 12 months of treatment with an anticoagulant for their acute episode of DVT or PE, there is some uncertainty as to whether to stop or continue this treatment. On one hand it is known that DVT or PE can recur, but on the other hand there is a risk of bleeding, besides the impact of a prolonged therapy with VKA on the patient’s daily life. New oral anticoagulants may provide a similar efficacy profile combined with a lower risk of bleeding and easier treatment logistics that could allow a longer treatment duration.
Objectives and Endpoints
The main efficacy objective of the EINSTEIN Extension study was to demonstrate that oral Xarelto once daily was superior to placebo in the long-term prevention of recurrent DVT or PE in patients with symptomatic DVT or PE who had already completed 6 to 12 months of treatment with a VKA or Xarelto. The primary efficacy endpoint was symptomatic recurrent VTE – the composite of recurrent DVT and fatal or non-fatal PE. The principal safety outcome was major bleeding.
OD = Once daily BID = Twice daily INR = International Normalised Ratio
Study Design
The EINSTEIN EXT study was a randomised, double-blind, event-driven, placebo-controlled superiority trial in 1,197 patients. Potential patients for inclusion in the study were those who participated in the EINSTEIN DVT and EINSTEIN PE studies, but also patients from outside of these studies who received treatment with VKA following an initial diagnosis of DVT or PE , and who continued on treatment up to randomisation. Following randomisation, patients received either oral Xarelto 20 mg once daily, or a matching placebo tablet once daily.
u The large EINSTEIN Programme was designed to investigate the clinical utility of Xarelto in DVT or PE treatment
Study Design – EINSTEIN DVT / PE Study Design – EINSTEIN EXT
Venous Thromboembolism Treatment (VTEx)

Placebo Xarelto
4
8
10
6
2
0
7.1%
2.0%
Inci
denc
e (%
) (pr
imar
y ef
ficac
you
tcom
e +
maj
or b
leed
s)
p<0.001
Netclinicalbenefit
enoxaparin/ VKA
Xarelto
5
2
4
6
3
1
0
4.2%
2.9%
Inci
denc
e (%
) (pr
imar
y ef
ficac
you
tcom
e +
maj
or b
leed
s)
p=0.03
Netclinicalbenefit
3.0
1.5
2.5
0.5
2.0
1.0
0
Cum
ulat
ive
even
t ra
te (%
)
0 60 120 180 240 300 360
Time to event (days)
enoxaparin/VKA (n=2,405)Xarelto (n=2,412)HR 0.49; 95% CI, 0.31-0.79; p=0.003
51%RRR
15
9
3
12
6
0
Cum
ulat
ive
even
t ra
te (%
)
0 60 120 180 240 300 360
Time to event (days)
enoxaparin/VKA (n=2,405)Xarelto (n=2,412)HR 0.90; 95% CI, 0.76-1.07; p=0.23
14
6
10
2
8
12
4
0
Cum
ulat
ive
even
t ra
te (%
)
0 60 120 180 240 300 360
Time to event (days)
enoxaparin/VKA (n=1,711)Xarelto (n=1,718)HR 0.97; 95% CI, 0.76-1.22; p=0.77
5
2
4
3
1
0
Cum
ulat
ive
even
t ra
te (%
)
0 60 120 180 240 300 360
Time to event (days)
enoxaparin/VKA (n=1,718)Xarelto (n=1,731)HR 0.68; 95% CI, 0.44-1.04; p<0.001 for non-inferiority
12
6
9
3
0
Cum
ulat
ive
even
t ra
te (%
)
0 60 120 180 240 300 360
Time to event (days)
Placebo (n=594)Xarelto (n=602)HR 0.18; 95% CI, 0.09-0.39; p<0.001
82%RRR
3.0
1.0
1.5
2.0
2.5
0.5
0
Cum
ulat
ive
even
t ra
te (%
)
0 60 120 180 240 300 360
Time to event (days)
enoxaparin/VKA (n=2413)Xarelto (n=2419)HR 1.12; 95% CI, 0.75-1.68; p=0.003 for non-inferiority
16 17
OD = Once daily BID = Twice daily INR = International Normalised Ratio RRR = Relative Risk Reduction CI = Confidence Interval HR = Hazard Ratio
recurrent VTE occurred in 1.3% of patients receiving Xarelto compared with 7.1% of patients receiving placebo. There was no significant difference in the principal safety outcome of major bleeding between Xarelto and placebo (4 vs. 0; p=0.11).
Favourable Benefit-Risk Profile
In all three studies, the pre-specified outcome of net clinical benefit was measured as the total number of events (primary efficacy outcome plus major bleeding events) for each treatment arm. Xarelto delivered a significantly greater net clinical benefit in EINSTEIN DVT (p=0.03) and EINSTEIN EXT (p<0.001). In EINSTEIN PE there was a trend towards net clinical benefit with Xarelto (3.4%) compared to enoxaparin/VKA (4.0%), though this did not reach clinical significance (p=0.28).
Venous thromboembolism (VTE) is a serious and life-threatening condition that accounts for approximately one in ten hospital deaths.30 Recurrence is common, with approximately 12% of patients experiencing a second VTE within 5 years.31 Current VTE treatment regimens, although effective, suffer from a number of significant drawbacks.32 The findings of EINSTEIN DVT, PE and EXT show that Xarelto provides a simple and effective single-drug solution to the acute treatment and long-term prevention of VTE.6,7
Results
In the two acute treatment studies (EINSTEIN DVT and EINSTEIN PE) oral, single-drug treatment with Xarelto was found to be as effective as the current standard dual therapy of enoxaparin and VKA in patients with acute symptomatic DVT or PE, and with a similar safety profile.6,7
In the DVT acute treatment study (EINSTEIN DVT) the primary efficacy outcome of symptomatic, recurrent VTE occurred in 2.1% of patients receiving Xarelto compared with 3.0% of patients treated with enoxaparin/VKA. The principal safety outcome of major and non-major clinically relevant bleeding was similar in both groups at 8.1%.
In the PE acute treatment study (EINSTEIN PE) the primary efficacy outcome of symptomatic, recurrent VTE occurred in 2.1% of patients receiving Xarelto compared with 1.8% of patients treated with enoxaparin/VKA. The principal safety outcome of major and non-major clinically relevant bleeding was similar in both groups (Xarelto 10.3%; enoxaparin/VKA 11.4%). Importantly, there were significantly fewer major bleeds with Xarelto (1.1% vs 2.2% for enoxaparin/VKA; p=0.003).
In the continued treatment study (EINSTEIN EXT) the primary efficacy outcome of symptomatic
Principal Safety Outcome Einstein DVT
Principal Safety Outcome Einstein PE
Net Clinical Benefit Einstein EXT
Major Bleeding Einstein PE
N ENGL J MED 2010; 363: 2499–2510 2012; 366: 1287–1297
Net Clinical Benefit Einstein DVT
There was no significant difference in principal safety outcomes between oral Xarelto and enoxaparin/VKA in either of the acute treatment studies (EINSTEIN DVT and EINSTEIN PE), or between Xarelto and placebo in the secondary prevention of VTE (EINSTEIN EXT). Importantly, there were significantly fewer major bleeds with Xarelto compared to enoxaparin/VKA in EINSTEIN PE.
Net Clinical Benefit in both EINSTEIN DVT and EINSTEIN EXT was significantly in favour of Xarelto.
Efficacy in Acute Treatment Einstein PE
Efficacy in Continued Treatment Einstein EXT
Efficacy in Acute Treatment Einstein DVT
The single-drug approach with oral Xarelto was at least as effective as the dual-drug approach of enoxaparin/VKA in the acute treatment of DVT and PE, and significantly more effective than placebo in the secondary prevention of recurrent DVT and PE.
u The single-drug approach of oral Xarelto combines good efficacy with a favourable safety profile in the acute treatment of DVT and PE, and the long-term secondary prevention of VTE.
Venous Thromboembolism Treatment (VTEx)
18 19
Studies in Venous Thromboembolism
Studies in Venous Thromboembolism
VTE
p O
S
Prevention of venous thromboembolism (VTE) in adult patients undergoing elective hip- or knee replacement surgery

enoxaparin40 mg OD
Xarelto10 mg OD
5
4
3
2
1
0
3.7%
1.1%
Inci
denc
e (%
)
p<0.001
70%RRR*
enoxaparin40 mg OD
Xarelto10 mg OD
5
4
3
2
1
0
2.0%
0.2%
Inci
denc
e (%
)
p<0.001
88%RRR*
enoxaparin40 mg OD
Xarelto10 mg OD
5
4
3
2
1
0
Inci
denc
e (%
)
0.1%0.3%
not significant
enoxaparin40 mg OD
Xarelto10 mg OD
8
6
4
2
0
5.8% 5.8%
Inci
denc
e (%
)
not significant
N=4,541
Double blind
Mandatory bilateral
venography
Oral Xarelto 10 mg OD
enoxaparin 40 mg OD
R
Evening before surgery
SURGERY
FOLLOW
UP
6–8 hourspost surgery
Last dose one day before venography
6–8 hourspost surgery
Last dose one day before venography
Day 1 Day 36±6 Day 65+5
enoxaparin40 mg OD
Xarelto10 mg OD
4
3
2
1
0
1.7%1.5%
Inci
denc
e (%
) not significant
§ Composite of excessive wound haematoma and reported surgical site bleeding
20 21
OD = Once daily RECORD = REgulation of Coagulation in major Orthopaedic surgery reducing the Risk of DVT and PE
Outcomes
The primary efficacy outcome was total VTE – the composite of any deep vein thrombosis (DVT), non-fatal pulmonary embolism (PE), and all cause mortality up to Day 36±6. The main secondary efficacy outcome was major VTE – the composite of proximal DVT, non-fatal PE, and VTE-related death. The main safety outcome was the incidence of major bleeding events while on treatment, and up to 2 days post-treatment.
Results
In RECORD1, one tablet of Xarelto 10 mg once daily was superior to subcutaneous enoxaparin 40 mg in the prevention of VTE in adult patients undergoing elective hip replacement surgery, while maintaining a comparable and low rate of major bleeding.3
The results of RECORD1 showed that when compared with enoxaparin over the same period of therapy (35±4 days), Xarelto delivered a significant:
70% reduction in the relative risk of the primary efficacy endpoint of total VTE
88% reduction in the relative risk of the main secondary efficacy outcome of major VTE.
Importantly, the safety profile of Xarelto was comparable to enoxaparin, including a low rate of major bleeding. RECORD1 was the first pivotal study to demonstrate the efficacy and safety of a fixed, unmonitored dose of oral Xarelto for extended thromboprophylaxis following elective hip replacement surgery.
Venous thromboembolism (VTE) remains a significant cause of morbidity and mortality in patients undergoing major orthopaedic surgery.33 RECORD1 was designed to investigate the efficacy and safety of extended thromboprophylaxis (up to 35±4 days) with oral Xarelto once daily compared with injectable enoxaparin following elective hip replacement surgery.3
Rationale
Extended thromboprophylaxis after elective hip replacement surgery is known to reduce symptomatic VTE.34-36 Current American College of Chest Physicians (ACCP) Guidelines recommend in patients undergoing elective hip or knee replacement surgery thrombo-prophylaxis for a minimum of 10 to 14 days
(Grade 1B), extending thromboprophylaxis in the outpatient period for up to 35 days (Grade 2B).33 However, in some countries VTE prophylaxis is not used routinely once the patient leaves hospital.37
Study Design
Patients were randomly assigned to this multinational, double-blind, double-dummy trial and received oral Xarelto 10 mg tablets once daily, or subcutaneous injections of enoxaparin sodium 40 mg once daily. Xarelto was started 6–8 h after wound closure or after adequate haemostasis had been achieved; enoxaparin was initiated 12 h before surgery and restarted 6–8 h after wound closure. Thereafter, study medications were administered every 24±2 hours until Day 35±4 following surgery, with the day of surgery being Day 1. Patients also received placebo tablets or injections.
Total VTE – Primary Efficacy Outcome
Major VTE – Secondary Efficacy Outcome
Major Bleeding Non-Major Bleeding Haemorrhagic Wound Complications§
Venous Thromboembolism Prevention (VTEp) in Elective Hip Replacement Surgery
Study Design
Xarelto was significantly more effective than enoxaparin for thromboprophylaxis in patients undergoing elective hip replacement surgery.
The superior efficacy of Xarelto was not associated with any significant increases in the incidence of major bleeding or other bleeding events.
u One tablet of Xarelto 10 mg once daily was superior to subcutaneous enoxaparin 40 mg
u The safety profile of Xarelto was comparable to enoxaparin, including a low rate of major bleeding
*RRR = Relative Risk Reduction
N ENGL J MED 2008; 358: 2765–75

enoxaparin40 mg OD
Xarelto10 mg OD
12
8
10
6
4
2
0
9.3%
2.0%
Inci
denc
e (%
)
p<0.0001
7.3%ARR*
enoxaparin40 mg OD
Xarelto10 mg OD
2
1
0
1.2%
0.2%
Inci
denc
e (%
)
p=0.004 1.0%ARR*
enoxaparin40 mg OD
Xarelto10 mg OD
2
1
0
Inci
denc
e (%
)
<0.1% <0.1%
not significant
enoxaparin40 mg OD
Xarelto10 mg OD
8
6
4
2
0
5.5%6.5%
Inci
denc
e (%
)
not significant
N=2,509
Double blind
Mandatory bilateral
venography
Oral Xarelto 10 mg OD
enoxaparin 40 mg OD
Placebo
R
Evening before surgery
SURGERY
FOLLOW
UP
6–8 hourspost surgery
Last dose one day before venography
6–8 hourspost surgery
Last dose one day before venography
Day 1 Day 36±6 Day 65+5Day 12±2
enoxaparin40 mg OD
Xarelto10 mg OD
4
3
2
1
0
1.7% 1.6%
Inci
denc
e (%
) not significant
§ Composite of excessive wound haematoma and reported surgical site bleeding
22 23
OD = Once daily RECORD = REgulation of Coagulation in major Orthopaedic surgery reducing the Risk of DVT and PE
Outcomes
The primary efficacy outcome was the composite of any deep vein thrombosis (DVT), non-fatal pulmonary embolism (PE), and all cause mortality up to Day 36±6. Secondary efficacy outcomes included major VTE – the composite of proximal DVT, non-fatal PE, and VTE-related death – and symptomatic VTE. The main safety outcome was the incidence of major bleeding events while on treatment, and up to 2 days post-treatment.
Results
In RECORD2 extended duration thromboprophy-laxis (5 weeks) with one tablet of Xarelto 10 mg once daily was significantly more effective than short-term therapy (2 weeks) with subcutaneous enoxaparin 40 mg for the prevention of VTE in adult patients undergoing elective hip replacement, with a similar and low rate of major bleeding.9
When compared with short-term VTE prevention with enoxaparin (10–14 days), extended thromboprophylaxis with Xarelto (35±4 days) was associated with a significant:
7.3% absolute risk reduction of the primary efficacy endpoint of total VTE
4.5% absolute risk reduction of major VTE
1.0% absolute risk reduction of symptomatic VTE
The incidences of major and non-major bleeding were similar in both the Xarelto and enoxaparin groups, with a low rate of major bleeding.
This trial clearly demonstrated the substantial benefit of extended thromboprophylaxis for patients undergoing elective hip replacement surgery.
Venous thromboembolism (VTE) remains a significant cause of morbidity and mortality in patients undergoing major orthopaedic surgery.33 The aim of the RECORD2 study was to compare the oral, once-daily Xarelto used for 31–39 days, with injectable enoxaparin for 11–15 days in patients undergoing elective hip replacement surgery.9
Rationale
Extended prophylaxis is recommended for all patients undergoing elective hip replacement surgery.33 However, in some countries such preventive treatment is not widely used once the patient leaves hospital.37
Study Design
Patients were randomly assigned to this multinational double-blind, double-dummy trial and received oral Xarelto 10 mg tablets once daily or subcutaneous injections of enoxaparin sodium 40 mg once daily. Xarelto was started 6–8 h after wound closure or after adequate haemostasis had been achieved and continued until Day 35±4 following surgery, with the day of surgery being Day 1; enoxaparin was initiated 12 h before surgery and restarted 6–8 h after wound closure and continued until Day 12±2. Patients also received placebo tablets until Day 35±4 starting 6–8 h after wound closure (or after adequate haemostasis had been achieved) or injections until Day 12±2, starting 12 h before surgery.
Total VTE – Primary Efficacy Endpoint
Symptomatic VTE – Secondary Efficacy Endpoint
Major Bleeding Non-Major Bleeding Haemorrhagic Wound Complications§
Venous Thromboembolism Prevention (VTEp)in Elective Hip Replacement Surgery
Study Design
Extended thromboprophylaxis with Xarelto significantly reduced the incidence of total VTE and symptomatic VTE compared with short-term enoxaparin.
The incidence of major bleeding and any bleeding was similar in both groups.
u Extended duration thromboprophylaxis (5 weeks) with Xarelto was significantly more effective than short-term therapy (2 weeks) with enoxaparin
u The safety profile of Xarelto was comparable to enoxaparin with a low rate of major bleeding
*ARR = Absolute Risk Reduction
LANCET 2008; 372: 31–39

N=2,531
Double blind
Mandatory bilateral
venography
Oral Xarelto 10 mg OD
enoxaparin 40 mg OD
R
Evening before surgery
SURGERY
FOLLOW
UP
6–8 hourspost surgery
Last dose one day before venography
6–8 hourspost surgery
Last dose one day before venography
Day 1 Day 13±4 Day 42+5
enoxaparin40 mg OD
Xarelto10 mg OD
25
20
15
10
5
0
18.9%
9.6%
Inci
denc
e (%
)
p<0.001
49%RRR*
enoxaparin40 mg OD
Xarelto10 mg OD
4
3
2
1
0
2.0%
0.7%Inci
denc
e (%
)
p=0.008 66%RRR*
enoxaparin40 mg OD
Xarelto10 mg OD
8
6
4
2
0
4.4% 4.3%
Inci
denc
e (%
)
not significant
enoxaparin40 mg OD
Xarelto10 mg OD
4
1
2
3
0
Inci
denc
e (%
)
0.5% 0.6%
not significant
enoxaparin40 mg OD
Xarelto10 mg OD
4
3
2
1
0
1.9% 2.0%
Inci
denc
e (%
)
not significant
§ Composite of excessive wound haematoma and reported surgical site bleeding
24 25
OD = Once daily RECORD = REgulation of Coagulation in major Orthopaedic surgery reducing the Risk of DVT and PE
Outcomes
The primary efficacy outcome was the composite of any deep vein thrombosis (DVT), non-fatal pulmonary embolism (PE), and all cause mortality within 13 to 17 days after surgery. Secondary efficacy outcomes included major VTE (the composite of proximal DVT, non-fatal PE, and VTE-related death), and symptomatic VTE.
The main safety outcome was the incidence of major bleeding events while on treatment, and up to 2 days post-treatment.
Results
In RECORD3, one tablet of Xarelto 10 mg once daily was superior to subcutaneous enoxaparin 40 mg in the prevention of VTE in adult patients undergoing elective knee replacement surgery, while maintaining a similar and low rate of major bleeding.4
The results of RECORD3 show that compared with enoxaparin, Xarelto achieved a:
49% reduction in the relative risk of total VTE – the primary efficacy endpoint
62% reduction in the relative risk of major VTE
66% reduction in the relative risk of symptomatic VTE
Similar and low incidence of major bleeding.
Venous thromboembolism (VTE) remains a significant cause of morbidity and mortality in patients undergoing major orthopaedic surgery.33 The objective of RECORD3 was to evaluate the efficacy and safety of oral, once-daily Xarelto compared with injectable enoxaparin once daily for VTE prevention following elective knee replacement surgery.4
The day of surgery was defined as Day 1, and study medications were continued until at least Day 10 and up to Day 14.
Rationale
Traditional anticoagulants used for thromboprophylaxis require parenteral administration. Thus an oral anticoagulant with predictable pharmacology may offer an advantage over existing options.
Study Design
Patients were randomly assigned to this multinational double-blind, double-dummy trial and received oral Xarelto 10 mg tablets once daily or subcutaneous injections of enoxaparin sodium 40 mg once daily. Xarelto was started 6–8 h after wound closure or after adequate haemostasis had been achieved; enoxaparin was initiated 12 h before surgery and restarted 6–8 h after wound closure. Study medications were administered every 24±2 hours until Day 12±2 following surgery, with the day of surgery being Day 1. Patients also received placebo tablets or injections.
This is in accordance with the ACCP Guidelines 2008 recommending thromboprophylaxis for at least 10 days after surgery (Grade 1A) in total knee arthroplasty.38 Current ACCP Guidelines suggest extending thromboprophylaxis for up to 35 days after surgery (Grade 2B).33
Total VTE – Primary Efficacy Endpoint
Symptomatic VTE – Secondary Efficacy Endpoint
Major Bleeding Non-Major Bleeding Haemorrhagic Wound Complications§
Venous Thromboembolism Prevention (VTEp)in Elective Knee Replacement Surgery
Study Design
Xarelto was significantly more effective than enoxaparin in patients undergoing elective knee replacement surgery.
There were no clinically significant differences in the incidence of bleeding outcomes between the Xarelto and enoxaparin groups.
u One tablet of Xarelto 10 mg once daily was significantly superior to subcutaneous enoxaparin 40 mg
u The safety profile of Xarelto was comparable to enoxaparin with a low rate of major bleeding
*RRR = Relative Risk Reduction
N ENGL J MED 2008; 358: 2776–86

enoxaparin30 mg BID
Xarelto10 mg OD
14
10
6
12
8
4
2
0
10.1%
6.9%
Inci
denc
e (%
)
p=0.016
31.4%RRR*
enoxaparin30 mg BID
Xarelto10 mg OD
4
3
2
1
0
1.2%
0.7%Inci
denc
e (%
)
p=0.187
N=3,148
Double blind
Mandatory bilateral
venography
Oral Xarelto 10 mg OD
enoxaparin 30 mg BID
R
SURGERY
FOLLOW
UP
12–24 hours after wound closure
6–8 hours after wound closureor adequate hemostasis
Last dose one day before venography
Last dose one day before venography
Day 1 Day 13±4 Day 42+5
enoxaparin30 mg BID
Xarelto10 mg OD
4
1
2
3
0
Inci
denc
e (%
)
0.3%0.7%
not significant
enoxaparin30 mg BID
Xarelto10 mg OD
15
10
5
0
9.2%10.2%
Inci
denc
e (%
)
not significant
enoxaparin30 mg BID
Xarelto10 mg OD
4
3
2
1
0
1.5% 1.4%
Inci
denc
e (%
) not significant
§ Composite of excessive wound haematoma and reported surgical site bleeding
26 27
OD = Once daily BID = Twice dailyRECORD = REgulation of Coagulation in major Orthopaedic surgery reducing the Risk of DVT and PE
non-fatal pulmonary embolism (PE), and all cause mortality up to Day 13±4 after surgery. The secondary efficacy outcomes included major VTE (the composite of proximal DVT, non-fatal PE, and VTE-related death), and symptomatic VTE. The main safety outcome was the incidence of major bleeding events while on treatment, and up to 2 days post-treatment.
Results
In RECORD4, one tablet of Xarelto 10 mg once daily was significantly more effective than enoxaparin, at the North American dose of 30 mg twice daily, in reducing the incidence of VTE in adult patients undergoing elective knee replacement surgery, while maintaining a comparable and low rate of major bleeding.5
The results of RECORD4 show that despite being compared to the higher daily dose of enoxaparin used in North America, Xarelto achieved a:
31% reduction in the relative risk of the primary efficacy endpoint of total VTE
Comparable and low incidence of major bleeding.
Venous thromboembolism (VTE) remains a significant cause of morbidity and mortality in patients undergoing major orthopaedic surgery.33 RECORD4 was designed to determine the efficacy and safety of once-daily Xarelto in adult patients following elective knee replacement surgery compared with enoxaparin 30 mg administered twice daily – the preferred North American dosing regimen.5
Rationale
RECORD4 differs from its companion study RECORD3 in that the dose of the comparator agent is 1.5 times as high (total daily enoxaparin dose in RECORD4 is 60 mg – 30 mg BID – compared to 40 mg OD in RECORD3).5
Study design
Patients were randomly assigned to this multinational double-blind, double-dummy trial and received oral Xarelto 10 mg tablets once daily or subcutaneous injections of enoxaparin sodium 30 mg every 12 h. Xarelto was started 6–8 h after wound closure or after adequate haemostasis had been achieved; enoxaparin was initiated 12–24 h after wound closure. Thereafter, study medications were administered until Day 12±2 following surgery (Xarelto once daily, enoxaparin twice daily), with the day of surgery being Day 1. Patients also received placebo tablets or injections.
Outcomes
The primary efficacy outcome of total VTE was the composite of any deep vein thrombosis (DVT),
Total VTE – Primary Efficacy Endpoint
Symptomatic VTE – Secondary Efficacy Endpoint
Major Bleeding Non-Major Bleeding Haemorrhagic Wound Complications§
Venous Thromboembolism Prevention (VTEp)in Elective Knee Replacement Surgery
Study Design
Xarelto was significantly more effective than enoxaparin in patients undergoing elective knee replacement surgery.
There were no clinically significant differences in the incidence of bleeding outcomes between the Xarelto and enoxaparin groups.
u One tablet of Xarelto 10 mg once daily was significantly more effective than enoxaparin, at the North American dose of 30 mg twice daily
*RRR = Relative Risk Reduction
THE LANCET 2009; 373: 1673–80
enoxaparin40 mg OD
Xarelto10 mg OD
2.0
1.0
1.5
0.5
0
1.3%
0.5%Inci
denc
e (%
)
p<0.001
62%RRR*
enoxaparin40 mg OD
Xarelto10 mg OD
2.0
1.0
1.5
0.5
0
0.8%
0.4%Inci
denc
e (%
)
p=0.005 56%RRR*
Pooled primaryoutcome
Day 12 (10–14)
Follow-up – Day 42 (42–47)
Secondary outcome (RECORD1, RECORD2 end of
planned medication)
Follow-up
Day 35 (30–42)30–35 days
after thelast dose
Xarelto Follow-up
enoxaparin Follow-upHip
Xarelto Follow-up
enoxaparin placebo Follow-upHip
Xarelto Follow-up
enoxaparin Follow-upKnee
up to Day 17 Secondary outcome
(RECORD3 end of planned medication)
enoxaparin40 mg OD
Xarelto10 mg OD
2.0
0.5
1.0
1.5
0
Inci
denc
e (%
)
0.2%0.3%
not significant
enoxaparin40 mg OD
Xarelto10 mg OD
2.0
0.5
1.0
1.5
0
Inci
denc
e (%
)
0.2% 0.2%
not significant
28 29
OD = Once daily RECORD = REgulation of Coagulation in major Orthopaedic surgery reducing the Risk of DVT and PE
post-operatively and until the end of the planned medication period. Other safety outcomes included any on-treatment bleeding up to 2 days after last intake of study medication, excessive wound haematoma, surgical-site bleeding, adverse event, and all-cause mortality over the entire study period (planned medication period plus 30 days follow-up).
Results
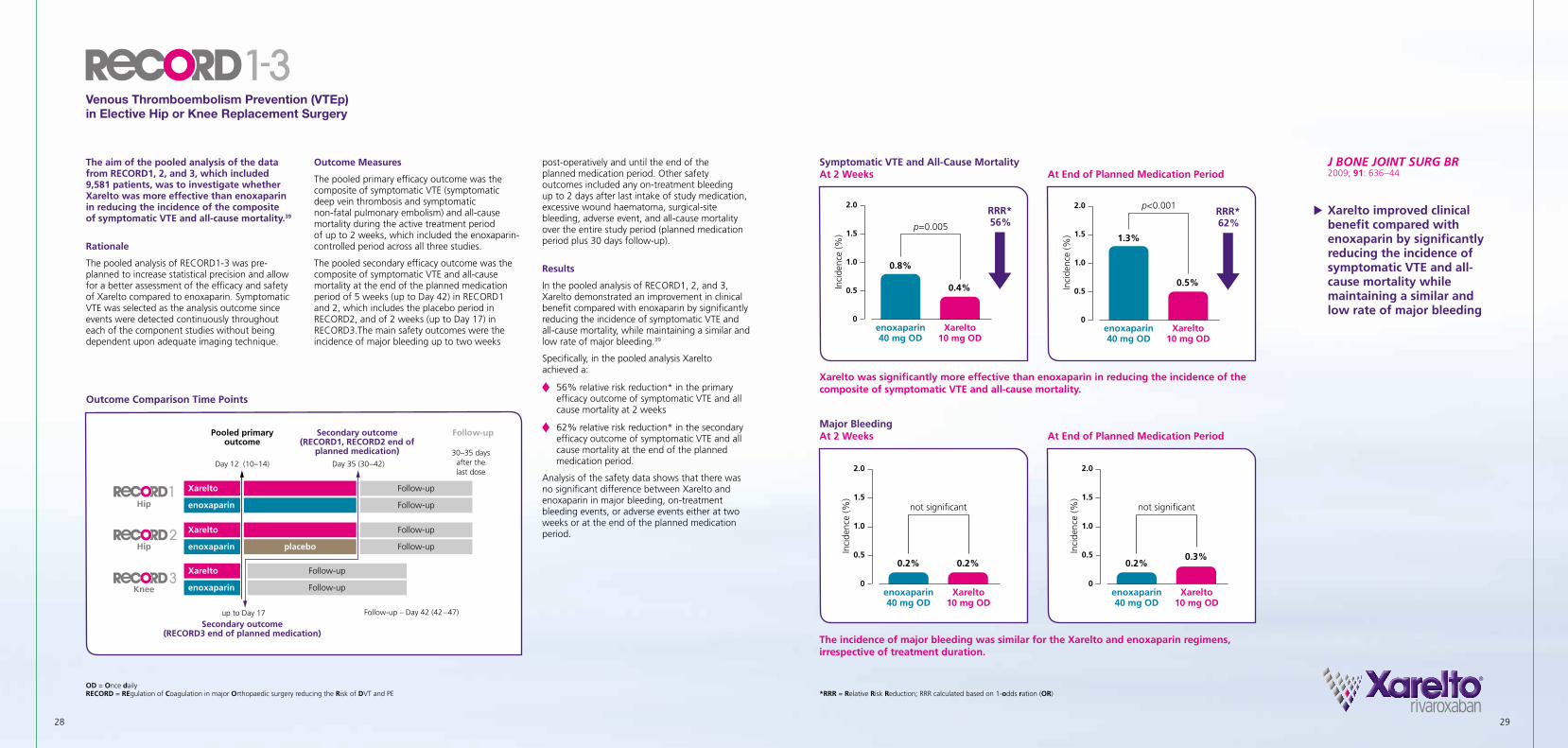
In the pooled analysis of RECORD1, 2, and 3, Xarelto demonstrated an improvement in clinical benefit compared with enoxaparin by significantly reducing the incidence of symptomatic VTE and all-cause mortality, while maintaining a similar and low rate of major bleeding.39
Specifically, in the pooled analysis Xarelto achieved a:
56% relative risk reduction* in the primary efficacy outcome of symptomatic VTE and all cause mortality at 2 weeks
62% relative risk reduction* in the secondary efficacy outcome of symptomatic VTE and all cause mortality at the end of the planned medication period.
Analysis of the safety data shows that there was no significant difference between Xarelto and enoxaparin in major bleeding, on-treatment bleeding events, or adverse events either at two weeks or at the end of the planned medication period.
The aim of the pooled analysis of the data from RECORD1, 2, and 3, which included 9,581 patients, was to investigate whether Xarelto was more effective than enoxaparin in reducing the incidence of the composite of symptomatic VTE and all-cause mortality.39
Rationale
The pooled analysis of RECORD1-3 was pre-planned to increase statistical precision and allow for a better assessment of the efficacy and safety of Xarelto compared to enoxaparin. Symptomatic VTE was selected as the analysis outcome since events were detected continuously throughout each of the component studies without being dependent upon adequate imaging technique.
Outcome Measures
The pooled primary efficacy outcome was the composite of symptomatic VTE (symptomatic deep vein thrombosis and symptomatic non-fatal pulmonary embolism) and all-cause mortality during the active treatment period of up to 2 weeks, which included the enoxaparin-controlled period across all three studies.
The pooled secondary efficacy outcome was the composite of symptomatic VTE and all-cause mortality at the end of the planned medication period of 5 weeks (up to Day 42) in RECORD1 and 2, which includes the placebo period in RECORD2, and of 2 weeks (up to Day 17) in RECORD3.The main safety outcomes were the incidence of major bleeding up to two weeks
Symptomatic VTE and All-Cause Mortality At 2 Weeks
At End of Planned Medication Period
Major Bleeding At 2 Weeks
At End of Planned Medication Period
Venous Thromboembolism Prevention (VTEp)in Elective Hip or Knee Replacement Surgery
Outcome Comparison Time Points
Xarelto was significantly more effective than enoxaparin in reducing the incidence of the composite of symptomatic VTE and all-cause mortality.
The incidence of major bleeding was similar for the Xarelto and enoxaparin regimens, irrespective of treatment duration.
u Xarelto improved clinical benefit compared with enoxaparin by significantly reducing the incidence of symptomatic VTE and all-cause mortality while maintaining a similar and low rate of major bleeding
*RRR = Relative Risk Reduction; RRR calculated based on 1-odds ration (OR)
J BONE JOINT SURG BR 2009; 91: 636–44

30 31References
References

32 33
References
1. http://clinicaltrial.gov/ct2/results?term= rivaroxaban.
2. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, Becker RC, Nessel CC, Paolini JF, Berkowitz SD, Fox KA, Califf RM; ROCKET AF Investigators. Xarelto versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365(10): 883-891.
3. Eriksson BI, Borris LC, Friedman RJ, Haas S, Huisman MV, Kakkar AK, Bandel TJ, Beckmann H, Muehlhofer E, Misselwitz F, Geerts W, for the RECORD1 Study Group. Xarelto versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med 2008; 358: 2765–75.
4. Lassen MR, Ageno W, Borris LC, Lieberman JR, Rosencher N, Bandel TJ, Misselwitz F, Turpie AGG, for the RECORD3 Investigators. Xarelto versus enoxaparin for thromboprophylaxis after total knee arthroplasty. N Engl J Med 2008; 358: 2776–86.
5. Turpie AG, Lassen MR, Davidson BL et al. Xarelto versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial. Lancet 2009; 373: 1673–80.
6. Bauersachs R, Berkowitz SD, Brenner B, Büller HR, Decousus H, Gallus AS, Lensing A, Misselwitz F, Prins MH, Raskob GE, Segers A, Verhamme P, Wells P, Agnelli G,Bounameaux H, Cohen A, Davidson BL, Piovella F, Schellong S, on behalf of the EINSTEIN Investigators. Oral Xarelto for Symptomatic Venous Thromboembolism. N Engl J Med 2010; 363 (26): 2499–2510.
7. The EINSTEIN–PE Investigators. Oral Xarelto for the Treatment of Symptomatic Pulmonary Embolism. N Engl J Med 2012; 366:1287–1297.
8. Mega JL, Braunwald E, Wiviott SD, Bassand J-P, Bhatt DL, Bode C, Burton P, Cohen M, Cook-Bruns N, Fox KAA, Goto S, Murphy SA, Plotnikov AN, Schneider D, Sun X, Verheugt FWA, Gibson CM, for the ATLAS ACS 2-TIMI 51 Investigators. Xarelto in patients with a recent acute coronary syndrome. N Engl J Med 2012; 366: 9–19.
9. Kakkar AK, Brenner B, Dahl OE, Eriksson BI, Mouret P, Muntz J, Soglian AG, Pap ÁF, Misselwitz F, Haas S, for the RECORD2 Investigators. Extended duration Xarelto versus short-term enoxaparin for the prevention of venous thromboembolism after total hip arthroplasty: a double-blind, randomised controlled trial. Lancet 2008; 372: 31–39.
10. Hori M, Matsumoto M, Tanahashi N, et al. Xarelto vs. Warfarin in Japanese Patients With Atrial Fibrillation. Circ J 2012 Jun 5.
11. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991; 22: 983–88.
12. Marini C, De Santis F, Sacco S et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke 2005; 36: 1115–19.
13. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly. The Framingham Study. Arch Intern Med 1987; 147: 1561–64.
14. Camm AJ, Lip GY, De Caterinal R et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation developed with the special contribution of the European Heart Rhythm Association, Eur Heart 2012; 33: 2719-2747.
15. Fuster V, Ryden LE, Cannom DS et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2011; 123: e269–e367.
16. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have non-valvular atrial fibrillation. Ann Intern Med 2007; 146: 857–867.
17. Hylek EM. The need for new oral anticoagulants in clinical practice. J Cardiovasc Med 2009; 10(8): 605–9
18. Xarelto [summary of product characteristics]. Berlin, Germany: Bayer Pharma AG; June 2013
19. Smith SC Jr, Benjamin EJ, Bonow RO et al. AHA/ACCF Secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation, Circulation 2011; 124: 2458-2473.
20. Hamm CW et al, ESC Guidelines NSTEMI/UA, Eur Heart J 2011; 32: 2999-3054
21. Chen ZM, Jiang LX, Chen YP, Xie JX, Pan HC, Peto R, et al. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005; 366 (9497): 1607–21.
22. Sabatine MS, Cannon CP, Gibson CM, Lopez-Sendon JL, Montalescot G, Theroux P, et al. Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation. N Engl J Med 2005; 352(12): 1179–89.
23. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med 2001; 345 (7): 494–502.
24. Wallentin L, Becker RC, Budaj A et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndrome. N Eng J Med 2009; 361 (11): 1045–57.
25. Wiviott SD et al; TRITON-TIMI 38 Investigators: Prasugrel versus Clopidogrel in patients with acute coronary syndrome. N Engl J Med. 2007 Nov 15; 357 (20): 2001–15.
26. Gibson CM, Mega JL, & Braunwald E on behalf of the ATLAS ACS 2 TIMI 51 Investigators. ATLAS – Thrombolysis in Myocardial Infarction 51 Trial (ATLAS-ACS 2 TIMI 51): A Randomized, Double-Blind, Placebo Controlled Study to Evaluate the Efficacy and Safety of Rivaroxaban in Subjects with Acute Coronary Syndrome. Presented at: American Heart Association (AHA), November 12-16, 2011; Orlando, USA
27. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines, Chest 2012; 141(2): e419S-94S.
28. Agnelli G, Gallus A, Goldhaber SZ, et al. Treatment of proximal deep-vein thrombosis with the oral, direct Factor Xa inhibitor, rivaroxaban (BAY 59–7939): the ODIXa-DVT (Oral Direct Factor Xa Inhibitor BAY 59–7939 in Patients With Acute Symptomatic Deep-Vein Thrombosis) study. Circulation 2007; 116: 180–187
29. Büller HR, Lensing AW, Prins MH et al. A dose ranging study evaluating once-daily oral administration of the factor Xa inhibitor rivaroxaban in the treatment of patients with acute symptomatic deep vein thrombosis: the EINSTEIN-DVT Dose Ranging Study, Blood; 112(6): 2242-7.
30. House of Commons Health Committee. Second report of session 2004–05. London: The Stationary Office; March 2005.
31. Heit JA, Mohr DN, Silverstein MD, et al. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med 2000; 160: 761–768.
32. Holbrook A, Schulman S, Witt DM et al. Evidence-based management of anticoagulant therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines, Chest 2012; 141(2): e152S-84S.
33. Falck-Ytter Y, Francis CW, Johanson NA; et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines, Chest 2012; 141(2)(Suppl): e278S-e325S.
34. Eikelboom JW, Quinlan DJ, Douketis JD. Extended-duration prophylaxis against venous thromboembolism after total hip or knee replacement: a meta-analysis of the randomised trials. Lancet 2001; 358: 9–15.
35. Hull RD, Pineo GF, Stein PD, et al. Extended out-of-hospital low-molecularweight heparin prophylaxis against deep venous thrombosis in patients after elective hip arthroplasty: a systematic review. Ann Intern Med 2001; 135: 858–69.
36. O’Donnell M, Linkins LA, Kearon C, Julian J, Hirsh J. Reduction of out-of-hospital symptomatic venous thromboembolism by extended thromboprophylaxis with low molecular-weight heparin following elective hip arthroplasty: a systematic review. Arch Intern Med 2003; 163: 1362–6.
37. Warwick D, Friedman RJ, Agnelli G, et al. Insufficient duration of venous thromboembolism prophylaxis after total hip or knee replacement when compared with the time course of thromboembolic events: findings from the Global Orthopaedic Registry. J Bone Joint Surg Br 2007; 89: 799–807.
38. Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Base Clinical Practice Guidelines. Chest 2008; 133: 381S–453S.
39. Eriksson BI, Kakkar AK, Turpie AG et al. Oral rivaroxaban for the prevention of symptomatic venous thromboembolism after elective hip and knee replacement. J Bone Joint Surg Br 2009; 91: 636–44.

34 35
Xarelto 2.5 mg film-coated tablets.(Refer to full SmPC before prescribing.)
Composition: Active ingredient: 2.5 mg rivaroxaban. Excipients: Microcrystalline cellulose, croscarmellose sodium, lactose monohydrate, hypromellose, sodium laurilsulfate, magnesium stearate, macrogol 3350, titanium dioxide (E171), iron oxide yellow (E172). Indication: Prevention of atherothrombotic events in adult patients after an acute coronary syndrome (ACS) with elevated cardiac biomarkers, co-administered with acetylsalicylic acid (ASA) alone or with ASA plus clopidogrel or ticlopidine. Contraindications: Hypersensitivity to the active substance or any of the excipients; clinically significant active bleeding; lesion or condition at significant risk of major bleeding; concomitant treatment with any other anticoagulant agent except under the circumstances of switching therapy to or from rivaroxaban or when unfractionated heparin is given at doses necessary to maintain a patent central venous or arterial catheter; concomitant treatment of ACS with antiplatelet therapy in patients with a prior stroke or a transient ischaemic attack (TIA); hepatic disease associated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B and C; pregnancy and breast feeding. Warnings and Precautions: Treatment in combination with other antiplatelet agents than ASA and clopidogrel/ticlopidine has not been studied and is not recommended. Clinical surveillance in line with anticoagulation practice is recommended throughout treatment. Xarelto should be discontinued if severe haemorrhage occurs. Not recommended: in patients with severe renal impairment (creatinine clearance <15 ml/min); in patients receiving concomitant systemic treatment with strong concurrent CYP3A4- and P-gp-inhibitors, i.e. azole-antimycotics or HIV protease inhibitors; in patients with increased bleeding risk; due to lack of data: in patients below 18 years of age; in patients concomitantly treated with dronedarone. Use with caution: in conditions with increased risk of haemorrhage; in patients with severe renal impairment (creatinine clearance 15 - 29 ml/min) or with renal impairment concomitantly receiving other medicinal products which increase rivaroxaban plasma concentrations; in patients treated concomitantly with medicinal products affecting haemostasis or with strong CYP3A4 inducers; in patients > 75 years of age or with low body weight. Patients on treatment with Xarelto and ASA or Xarelto and ASA plus clopidogrel/ticlopidine should only receive concomitant treatment with NSAIDs if the benefit outweighs the bleeding risk. In patients at risk of ulcerative gastrointestinal disease prophylactic treatment may be considered. Although treatment with rivaroxaban does not require routine monitoring of exposure, rivaroxaban levels measured with a calibrated quantitative anti-Factor Xa assay may be useful in exceptional situations. Xarelto film-coated tablets contain lactose. Undesirable effects: Common: anaemia, dizziness, headache, eye haemorrhage, hypotension, haematoma, epistaxis, haemoptysis, gingival bleeding, gastrointestinal tract haemorrhage, gastrointestinal and abdominal pains, dyspepsia, nausea, constipation, diarrhoea, vomiting, pruritus, rash, ecchymosis, cutaneous and subcutaneous haemorrhage, pain in extremity, urogenital tract haemorrhage, renal impairment, fever, peripheral oedema, decreased general strength and energy, increase in transaminases, post-procedural haemorrhage, contusion, wound secretion. Uncommon: thrombocythemia, allergic reaction, dermatitis allergic, cerebral and intracranial haemorrhage, syncope, tachycardia, dry mouth, hepatic function abnormal, urticaria, haemarthrosis, feeling unwell, increases in: bilirubin, blood alkaline phosphatase, LDH, lipase, amylase, GGT. Rare: jaundice, muscle haemorrhage, localised oedema, bilirubin conjugated increased, vascular pseudoaneurysm (uncommon in prevention therapy in ACS following percutaneous intervention). Frequency not known: compartment syndrome or (acute) renal failure secondary to a bleeding. Classification for supply: Medicinal product subject to medical prescription. Marketing Authorisation Holder: Bayer Pharma AG, D-13342 Berlin, Germany Further information available from: [email protected] Version: EU/1
Xarelto 10 mg film-coated tablets.(Refer to full SmPC before prescribing.)
Composition: Active ingredient: 10 mg rivaroxaban. Excipients: Microcrystalline cellulose, croscarmellose sodium, lactose monohydrate, hypromellose, sodium laurilsulfate, magnesium stearate, macrogol 3350, titanium dioxide (E171), iron oxide red (E172). Indication: Prevention of venous thromboembolism (VTE) in adult patients undergoing elective hip or knee replacement surgery. Contraindications: Hypersensitivity to the active substance or to any of the excipients; active clinically significant bleeding; lesion or condition considered as significant risk for major bleeding; concomitant treatment with any other anticoagulants except under the circumstances of switching therapy to or from rivaroxaban or when unfractionated heparin is given at doses necessary to maintain an open central venous or arterial catheter; hepatic disease associated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B and C; pregnancy and breast feeding. Warnings and Precautions: Increasing age may increase haemorrhagic risk. Not recommended: in patients with severe renal impairment (creatinine clearance <15 ml/min); in patients receiving concomitant systemic treatment with strong concurrent CYP3A4- and P-gp-inhibitors, i.e. azole-antimycotics or HIV protease inhibitors; due to lack of data: in patients below 18 years of age, in patients undergoing hip fracture surgery, in patients concomitantly treated with dronedarone. Use with caution: in patients with increased bleeding risk; in patients with severe renal impairment (creatinine clearance 15 - 29 ml/min) or with renal impairment concomitantly receiving other medicinal products which increase rivaroxaban plasma concentrations; in patients treated concomitantly with medicinal products affecting haemostasis or with strong CYP3A4 inducers; when neuraxial anaesthesia or spinal/epidural puncture is employed. In patients at risk of ulcerative gastrointestinal disease prophylactic treatment may be considered. There is no need for monitoring of coagulation parameters during treatment with rivaroxaban in clinical routine, if clinically indicated rivaroxaban levels can be measured by calibrated quantitative anti-Factor Xa tests. Xarelto contains lactose. Undesirable effects: Common: anaemia, dizziness, headache, syncope, eye haemorrhage, tachycardia, hypotension, haematoma, epistaxis, gastrointestinal tract haemorrhage, gastrointestinal and abdominal pains, dyspepsia, nausea, constipation, diarrhoea, vomiting, pruritus, rash, ecchymosis, pain in extremity, urogenital tract haemorrhage, fever, peripheral oedema, decreased general strength and energy, increase in transaminases, post-procedural haemorrhage, contusion, wound secretion. Uncommon: thrombocythemia, allergic reaction, dermatitis allergic, cerebral and intracranial haemorrhage, haemoptysis, dry mouth, hepatic function abnormal, urticaria, cutaneous and subcutaneous haemorrhage, haemarthrosis, renal impairment, feeling unwell, localised oedema. increases in: bilirubin, blood alkaline phosphatase, LDH, lipase, amylase, GGT. Rare: jaundice, muscle haemorrhage, bilirubin conjugated increased. Frequency not known: pseudoaneurysm following percutaneous intervention, compartment syndrome or (acute) renal failure secondary to a bleeding. Classification for supply: Medicinal product subject to medical prescription.Marketing Authorisation Holder: Bayer Pharma AG, D-13342 Berlin, GermanyFurther information available from: [email protected]: EU/6

36
Xarelto 15 mg / 20 mg film-coated tablets.(Refer to full SmPC before prescribing.)
Composition: Active ingredient: 15 mg / 20 mg rivaroxaban. Excipients: Microcrystalline cellulose, croscarmellose sodium, lactose monohydrate, hypromel-lose, sodium laurilsulfate, magnesium stearate, macrogol 3350, titanium dioxide (E171), iron oxide red (E172). Indication: Prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation with one or more risk factors, such as congestive heart failure, hypertension, age ≥ 75 years, diabetes mellitus, prior stroke or transient ischaemic attack. Treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and prevention of recur-rent DVT and PE in adults. Contraindications: Hypersensitivity to the active substance or any of the excipients; clinically significant active bleeding; lesion or condition at significant risk of major bleeding; concomitant treatment with any other anticoagulant agent except under the circumstances of switching therapy to or from rivaroxaban or when unfractionated heparin is given at doses necessary to maintain a patent central venous or arterial catheter; hepatic disease associated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B and C; pregnancy and breast feeding. Warnings and Precautions: Clinical surveillance in line with anticoagulation practice is recommended throughout treatment. Xarelto should be discontinued if severe haemorrhage occurs. Not recommended: in patients with severe renal impairment (creatinine clearance <15 ml/min); in patients receiving concomi-tant systemic treatment with strong concurrent CYP3A4- and P-gp-inhibitors, i.e. azole-antimycotics or HIV protease inhibitors; in patients with increased bleeding risk; due to lack of data: in patients below 18 years of age, in patients with prosthetic heart valves, in patients with PE who are haemodynamically unstable or may receive thrombolysis or pulmonary embolectomy; in patients concomitantly treated with dronedarone. Use with caution: in conditions with increased risk of haemorrhage; in patients with severe renal impairment (creatinine clearance 15 - 29 ml/min) or with renal impairment concomitantly receiv-ing other medicinal products which increase rivaroxaban plasma concentrations; in patients treated concomitantly with medicinal products affecting haemo-stasis or with strong CYP3A4 inducers. In patients at risk of ulcerative gastrointestinal disease prophylactic treatment may be considered. Although treatment with rivaroxaban does not require routine monitoring of exposure, rivaroxaban levels measured with a calibrated quantitative anti-Factor Xa assay may be useful in exceptional situations. Specific dose recommendations apply for patients with moderate to severe renal impairment and in case of DVT/PE-patients only if the patient’s assessed risk for bleeding outweighs the risk for recurrent DVT and PE. Xarelto contains lactose. Undesirable effects: Common: anaemia, dizziness, headache, eye haemorrhage, hypotension, haematoma, epistaxis, haemoptysis, gingival bleeding, gastrointestinal tract haemorrhage, gastrointes-tinal and abdominal pains, dyspepsia, nausea, constipation, diarrhoea, vomiting, pruritus, rash, ecchymosis, cutaneous and subcutaneous haemorrhage, pain in extremity, urogenital tract haemorrhage, renal impairment, fever, peripheral oedema, decreased general strength and energy, increase in transaminases, post-procedural haemorrhage, contusion, wound secretion. Uncommon: thrombocythemia, allergic reaction, dermatitis allergic, cerebral and intracranial haemorrhage, syncope, tachycardia, dry mouth, hepatic function abnormal, urticaria, haemarthrosis, feeling unwell, increases in: bilirubin, blood alkaline phosphatase, LDH, lipase, amylase, GGT. Rare: jaundice, muscle haemorrhage, localised oedema, bilirubin conjugated increased, vascular pseudoaneurysm (uncommon in prevention therapy in ACS following percutaneous intervention). Frequency not known: compartment syndrome or (acute) renal failure second-ary to a bleeding.Classification for supply: Medicinal product subject to medical prescription. Marketing Authorisation Holder: Bayer Pharma AG, D-13342 Berlin, GermanyFurther information available from: [email protected] Version: EU/3.1

Disclaimer: Rivaroxaban is an oral, direct Factor Xa inhibitor and marketed as Xarelto®. The marketing authorization for Xarelto® may vary from country to country. In the European Union, Xarelto® is approved for the:
· Prevention of venous thromboembolism (VTE) in adult patients undergoing elective hip- or knee replacement surgery
· Prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrilliation with ≥1 risk factor, such as congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, earlier stroke or TIA (transient ischaemic attack)
· Treatment of deep vein thrombosis (DVT) and prevention of recurrent DVT and pulmonary embolism (PE) in adults
· Treatment of PE and prevention of recurrent DVT and PE in adults
· Prevention of atherothrombotic events (cardiovascular death, myocardial infarction or stroke) after an acute coronary syndrome (ACS) in adult patients with elevated cardiac biomarkers when co-administered with acetylsalicylic acid (ASA) alone or with ASA plus clopidogrel or ticlopidine
Whilst licenses may differ from country to country, across all indications Xarelto® is approved in more than 120 countries. Xarelto® was discovered by Bayer HealthCare, and is being jointly developed with Janssen Research & Development, LLC. Xarelto® is marketed outside the U.S. by Bayer HealthCare and in the U.S. by Janssen Pharmaceuticals, Inc. (a Johnson & Johnson Company).
Anticoagulant medicines are potent therapies used to prevent or treat serious illnesses and potentially life threatening conditions. Before initiating therapy with anticoagulant medicines, physicians should carefully assess the benefit and risk for the individual patient. Responsible use of Xarelto® is a high priority for Bayer, and the company has developed a Prescribers Guide for physicians and a Xarelto® Patient Card for patients to support best practices.
Xarelto® is a registered trademark of Bayer HealthCare Pharmaceuticals AG
To learn more, please visit: https://prescribe.xarelto.comTo learn more about thrombosis, please visit www.thrombosisadviser.comTo learn more about Xarelto, please visit www.xarelto.com

© Bayer HealthCare Pharmaceuticals August 2013
BHP/100445/0613 L.NL.GM.08.2013.0187
Clinical Trials in the Venous Arterial Thromboembolic (VAT) Space