wound care lecture
TRANSCRIPT

بسم هللا الرحمن الرحيم•

Wounds and Dressings
Dr.Nadir Mehmood
Asstt Prof of Surgery
RMC
Leaning objectives
At the end of this discussion a student shall be able to;
• Define acute n chronic wounds, dressings, wound care, healing and related terms
• Enumerate types of wounds and classification
• Describe pathophysiology of wound healing
• Define wound care and enlist its components
• Enlist ideal characteristics of dressings
• Enumerate different types of dressings

WOUND
A TRAUMATIC BREECH IN THE CONTINUITY OF TISSUES
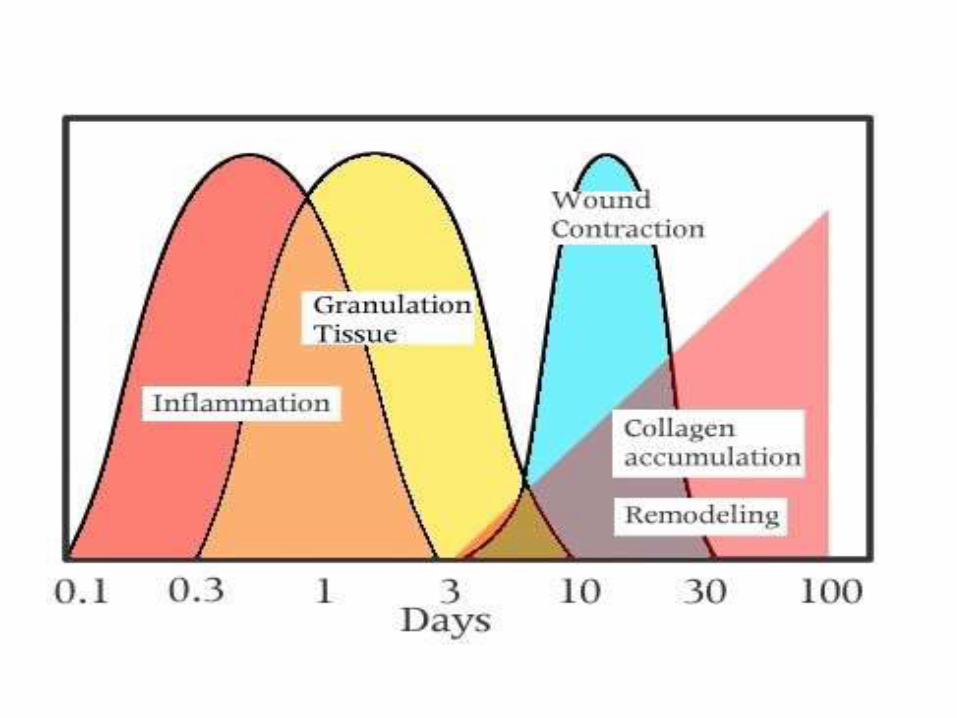
PHASES OF WOUND HEALING
Wounding
Hemostasis - coagulation: immediate response
Inflammation: 0-4 days
Proliferation: 4-21 days
Granulation-angiogenesis (Epithelialization) :4-21 days
Matrix synthesis
Fibrosis
Remodeling: up to 2 years

TYPES OF WOUNDS
• PENETRATING WOUNDS– STAB WOUNDS
– MISSILE INJURIES• LOW VELOCITY
• HIGH VELOCITY
• PERFORATING WOUNDS
• NON-PENETRATING WOUNDS– BLUNT INJURIES
– BLAST INJURIES
– CRUSH INJURIES

CLINICAL APPROACH TO A WOUND
• ARREST OF HEMORRHAGE
• SKELETAL STABILITY
• GENERAL ASSESSMENT
– HISTORY• TIME SINCE INJURY
• MODE OF INJURY
– SITE
– SIZE
– DEPTH

CLINICAL APPROACH TO A WOUND (Contd.)
– POSSIBLE ORGAN INJURY
• VISCERA
• DISTAL NEUROVASCULAR DEFICIT
– FOREIGN BODIES, DEBRIS ETC.
– PRESENCE OF DEAD TISSUE

THE WOUND CHART
BACTERIAL CONTAMINATION
• CLEAN
• CLEAN-CONTAMINATED
• CONTAMINATED
• DIRTY

Hairmyres A&E
Evaluation
• Always check and document distal neurovascular function
• Always X-Ray for glass
• Ask about Tetanus status
Evaluation
• Good light essential
• Remove all foreign material, blood clot etc
• Shave hair if necessary (NOT EYEBROWS)
• Local anaesthetic may be necessary
• Incised wounds in hands- what was the position at the time of injury ?
WOUND TOILET
• USE OF ANAESTHESIA
• THOROUGH IRRIGATION OF WOUND WITH WATER/SALINE/RINGER’S SOL
• REMOVAL OF SURFACE CONTAMINATION AND DUST PARTICLES ETC.
• APPLICATION OF TOPICAL ANTISEPTICS
DEBRIDEMENT(WOUND EXCISION)
• LAYING OPEN THE WOUND
• REMOVAL OF ALL DEAD TISSUES
• REMOVAL OF ALL FOREIGN MATERIAL
• START FROM SURFACE AND PROCEED TO DEPTH

TYPES OF WOUND DEBRIDEMENT
• SURGICAL
• MECHANICAL
• AUTOLYTIC
• ENZYMATIC
• CHEMICAL
• BIOLOGICAL

DEBRIDEMENT (contd.)
• EXCISE THE IRREGULAR SKIN MARGINS
• EXCISE THE SUBCUTANEOUS TISSUE
• LIBERALLY EXCISE THE SKELETAL MUSCLE
• DO NOT EXCISE VESSELS AND NERVES

DEBRIDEMENT (contd.)
• LIGATE SMALL VESSELS
• REPAIR LARGE VESSELS
• REPAIR OR LABEL TENDONS
• REPAIR OR LABEL NERVES
• THOROUGH IRRIGATION WITH WATER/SALINE ETC.
• FILL/PACK WITH SOAKED GAUZE
THE SCARS
• A SCAR IS THE CONNECTIVE TISSUE AREA, COVERED BY EPITHELIUM, THAT REPLACES A NORMAL EPITHELIAL AREA RESULTING FROM WOUND HEALING.

WOUND HEALING (6Hrs)
UNTREATEDTREATED

WOUND HEALING (1d)
UNTREATED TREATED

WOUND HEALING (2d)
UNTREATED TREATED

WOUND HEALING (7d)
UNTREATED TREATED

FACTORS AFFECTING WOUND HEALING
• LOCAL FACTORS
– MORPHOLOGY OF WOUND
– BLOOD SUPPLY
– INFECTION
– FORIGN BODIES
– MALIGNANCY
– MOISTURE
– PRESSURE
– LOCAL TREATMENT/RADIOTHERAPY

FACTORS AFFECTING WOUND HEALING
• SYSTEMIC FACTORS
– AGE
– DIABETES MELLITUS
– UREMIA
– LIVER DISEASE
– NUTRITIONAL DEFICIENCY
– SYSTEMIC DRUG THERAPY• IMMUNOSUPPRESSIVES
• CYTOTOXIC THERAPY
REQUIREMENTS OF WOUND DRESSINGS
• PROTECTIVE
• MAINTENANCE OF MOISTURE
• ALLOW GAS AND FLUID EXCHANGE
• NON ADHERENT
• NON TOXIC
• NON ALLERGENIC
• NON ODOROUS
• ABSORBANT
• STERILE

TYPES OF WOUND DRESSINGS
• DRY DRESSINGS
– GAUZE
– NON ADHESIVE MESHES
– MEMBRANES
– FOAMS
• MOIST DRESSINGS
– CREAMS & OINTMENTS
– PASTES
– HYDROCOLLOIDS & HYDROGELS, ALGINATES etc

SPECIAL DRESSINGS
• AMNIOTIC MEMBRANE
• ACELLULAR HUMAN DERMIS
• XENOGRAFTS (PORCINE SKIN)
• ACELLULAR INORGANIC DRESSINGS– SILICONES
– BARRIER FILMS
– FOAMS

VACUUM ASSISTED CLOSURE(VAC)(NEGATIVE PRESSURE WOUND THERAPY)
• SPECIAL SYSTEM
• FOAM DRESSING WITH ATTACHED TUBE
• PROVIDES CONTINUOUS LOW PRESSURE SUCTION TO SEALED WOUND
When Does a Wound Become Chronic?
• Healthy individuals with no underlying factors
an acute wound→ heal within three weeks remodelling → over the next year or so
• Working Definition – wound lasting >3 months
• Chronic wound – Fail to heal due to various local and systemic causes
– Healing process arrests at different levels of healing
– Wound may appear at different colours
Time
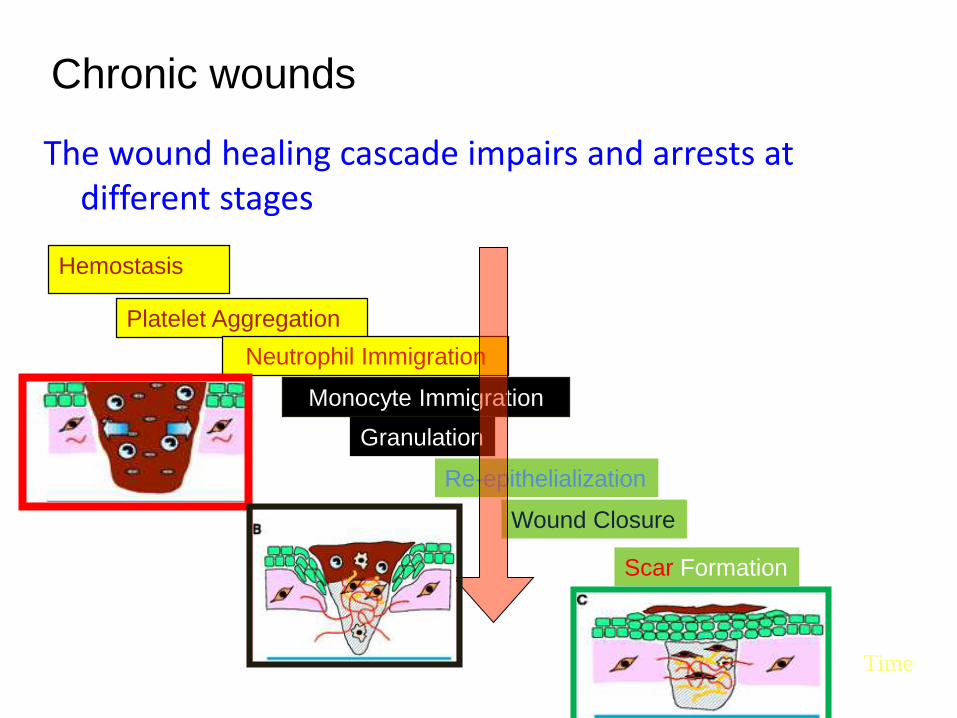
Hemostasis
Platelet Aggregation
Neutrophil Immigration
Monocyte Immigration
Granulation
Re-epithelialization
Wound Closure
Scar Formation
Remodeling
Minutes Hours Days Weeks Months Years
The wound healing cascade impairs and arrests at different stages
Chronic wounds
CHRONIC WOUND

Dressing Selection
• Primary Dressing – A dressing that touches the wound
• Secondary Dressing – Keeps the primary dressing in site – Fasten it to the wound
• Some dressings function as primary dressings only
• Some could function as primary and secondary dressings as well - adhesive

Dressing Selection
• Depend on
– Type of wound
– Patient preference/Dr preference
– Stage of healing of the wound
• Proliferation or Granulation phases
• Remodelling or Maturation phases
• Presence or absence of Infection or Colonization –Bio film
Dressings
Three types
• Inactive Dressings
• Active dressings
• Interactive
35
Inactive dressings
• Dry dressings
• wet to dry dressings
• Polyurethane film dressing –Breathable and non breathable film dressings
• Vaseline tulles
• Antibiotic impregnated tulles
36
Dry dressings……
1. Tend to absorb wound moisture 2. Tightly Adherent to granulation Tissue –
will break upon removal

37
Vaseline Gauze
PU Film Dressings

38
Active dressings
• Plays a role in wound healing
– Provide a covering,
– enhance granulation tissue formation,
– Reduce slough formation
– Inhibits bacteria
– Keep wound moist
– Some provide growth factors
39
Examples
• Hydrogels –fibre and Foams
• Hydrocellular dressings
• Foams
• Alginates
• Crystaline Silver and Slow Iodine releasing materials

• Topical products :Hydrocolloids , Hydrogels ,Calcium alginates/hydrofibers , Foams , Starch dressings , Enzymatic debriders
• Surgical debridement• Renewed interest in ancient remedies → honey• Renewed interest in maggots (“Biosurgery” )• Ultraviolet light• Laser• Hydrotherapy• Electrical stimulation• Ultrasound• Growth factors impregnated dressings


• Skin substitutes → synthetic and biologic
• Growth factor revolution –actively manipulate wound healing → angiogenesis
• Gene therapy
• Nanotechnology : Drugs directed to specific aspects of wounds , Manipulating of angiogenesis
43
Principles of Dressing andBandaging
• The dressing is opened carefully and handled so it does not get contaminated. • The dressing adequately covers the entire wound.• Bandages are not placed directly against the wound.• Wounds are bandaged snugly, but not too tightly.• Bandages are not too loose; neither the dressing nor the bandage should shift or
slip.• There are no loose ends of cloth, gauze, or tape that could get caught.• The bandage covers all edges of the dressing.• Tips of the fingers and toes are left exposed when arms and legs are bandaged. • A small bandage on an arm or leg is covered with a larger bandage to more evenly
distribute the pressure and to avoid causing a pressure point. • Start a bandage on an arm or leg at the end nearest the hand or foot, then work
upward to prevent applying the bandage too tightly. • The body part is bandaged in the position in which it is to remain.• Ask the victim how the bandage feels.• Never use a circular bandage around the neck.
