world bank documentdocuments.worldbank.org/curated/en/571931468774968205/... · 2016-07-17 · bhs...
TRANSCRIPT

Document of
The World Bank
Report No.1 3 9 91-IND
STAFF APPRAISAL REPORT
INDONESIA
FOURTH HEALTH PROJECT
I1MPROVING EQUITY AND QUALITY OF CARE
MAY 22, 1995
East Asia and Pacific Regional OfficeCountry Department IIIPopulation and Human Resources Division
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

CURRENCY EQUIVALENTS(as of March 1995)
Currency Unit = Rupiah (Rp)
US51.00 = Rp 2,193Rp I million = US$456
FISCAL YEAR
April I - March 31
ABBREVIATIONS, ACRONYMS AND DEFINITIONS
APBD Regional budgetAPBN National government budgetARI Acute respiratory infectionASEAN Association of Southeast Asian NationsASKES Health insurance for government employeesBapelkes Provincial in-service training centersBAPPEDA I Provincial Development Planning AgencyBAPPEDA II District Development Planning AgencyBAPPENAS National Development Planning BoardBHS Basic health servicesBasic Awal An initial list of basic health intervention for HP IV fundingBupati Head of district administrationCAS Country Assistance StrategyCEM Country Economic MemorandumCHN III Third Community Health and Nutrition ProjectDALYs Disability-adjusted life yearsDinas Kesehatan I Provincial government health officeDinas Kesehatan II District government health officeDIP Development budgetDIP Terpadu Integrated development budget for basic health servicesDokabu Head of the District Health OfficeGOI Govemment of IndonesiaHD Health districtHIV Human Immuno-deficiency VirusHP III Third Health ProjectHP IV Fourth Health ProjectICB Intemational competitive biddingIDT Inpres Desa Tertinggal (Program for Lagging Villages)IHPB Integrated Health Plan and BudgetIMR Infant mortality rateINPRES Sectoral development grant to regional govemmentsJatim East JavaKalbar West KalimantanKaltim East KalimantanKandep District health officeKanwil Kesehatan Provincial health officeLPLPO An innovative drugs management system developed by HP I1
MOH Ministry of HealthNCB National competitive biddingNCH II Second Nutrition and Community Health ProjectNTB Nusa Tengarra BaratO&M Operations and maintenancePDE Program Development ExpendituresPerum Husada Bhakti Govemment insurance company for civil servantsPIU Project Implementation UnitPosyandu Monthly village preventive health sessions run by volunteers
and visited by puskesmas staffPusdilklat Center for Education and Training of Health PersonnelPuskesmas Health centerPustu Health subcenterQA Quality assuranceRepelita Five-year Development PlanSAE Special Assistance ExpendituresSAF Special Assistance FundsSKRT MOH's routine health survey of householdsSumbar West SumatraSUSENAS National Household Expenditure SurveyTA Technical assistanceWHO World Health OrganizationWSSLIC Water Supply and Sanitation for Low Income Communities
Proj ect

INDONESIAFOURTH HEALTH PROJECT:
IMPROVING EQUITY AND QUALITY OF CARE
LOAN AND PROJECT SUMMARY
Borrower: Republic of Indonesia
ImplementingAgency: Ministry of Health (MOH)
Poverty: Program of Targeted Interventions
Amount: US$88.0 million equivalent
Terms: Repayable in 20 years including five years of grace at theBank's standard variable interest rate.
Commitment Fee: 0.75 percent on undisbursed loan balances, beginning 60 daysafter signing, less any waiver
Financing Plan: See para. 4.6 in SAR
Economic Rateof Return: Not applicable
Staff AppraisalReport: No. 13991-IND
Map: IBRD No. 26852
Project IdentificationNumber: ID-PA-3965

- ii -
Project Description: The aim of the project is to improve health outcomes by givingprovinces, districts and puskesmas managers greaterresponsibility, authority, resources, and skills to enhance healthcare quality and equity. Specific project objectives are: (i) toincrease the authority and capacity of provincial and districthealth offices and health centers to plan and implement healthprograms as they deem appropriate to local conditions; (ii) toensure that the provision and consumption of key healthservices conform to affordable, cost-effective standards of care;(iii) to improve access and utilization of these health services bythe poor; and (iv) to improve efficiency in the delivery of basichealth services (BHS).
The project, which would be implemented in the provincesof West and East Kalimantan, West Nusa Tenggara, WestSumatra, and East Java, would operate through threemechanisms. First, it would seek to improve the workprocesses, attitudes and skills within publicly managed BHSfacilities, while providing the additional resources needed torender higher quality, more accessible services that fit the needsand demand of clients. A key element is the establishment ofquality assurance (QA) processes and supporting trainingprograms.
Second, to facilitate these changes, the project wouldstrengthen the institutional capability of provinces and districtsto supervise, support and reward frontline providers of care;and simultaneously make managers of districts and facilitiesmore accountable for their performance.
Third, the project would support resource mobilization anda reorientation of government spending to BHS and povertyalleviation. Indicative targets have been agreed, increasinggovernment health spending for BHS and the poor.
Benefits and Risks: By improving the delivery and quality of BHS, the projectwould increase the number of people utilizing them andbenefiting from their use. Covering about 886 health centers,HP IV could benefit an estimated 27 million people. Of these,about 20 percent are poor and another 13 percent are near-poor. While all demographic groups could benefit from theproject, the major beneficiaries are expected to be women andchildren from both poor and non-poor families. The poor,however, would benefit from the project disproportionately, assubsidies for health centers and their outreach activities arestrongly pro-poor.

- Hii -
The project has two salient risks. First, increasing cost-recovery rates to appropriate levels might be delayed in somedistricts, given that price increases for publicly providedservices represent a politically sensitive decision. Second, thetraining activities sponsored by the project could becomeburdensome on staff and disruptive of their work.
These risks have been reduced during project preparationby ensuring that enough funds have been allocated for thepromotion of price reforms and that both provincial, district andcentral officials are committed to them. Evidence for thiscommitment is shown by their involvement in advancing thisaspect of the project and by the decrees issued by Bupati (headof district government) of starter districts expressing support forprice adjustments. As to training, the project would emphasizedistance learning and other on-the-job approaches. It wouldalso establish mechanisms for controlling the number of daysstaff are away from work to attend off-the-job training.

- iv -
Estimated Project Costs: Local Foreign Total--------- US$ million -----------
Facility-Level Service ImprovementHealth Facility Construction and Upgrading 21.6 15.3 36.9Special Assistance Program for
Basic Health Services 27.5 9.8 37.3
Institutional DevelopmentSupport for Quality Assurance Mechanisms 6.1 1.4 7.5Support for Training and Curriculum Development 3.6 5.5 9.1Support for Performance-Linked Incentives 0.4 0.2 0.6Replication and Piloting Innovative Initiatives:
Dissemination and Adaptation ofHP III Innovations 1.5 0.3 1.8
Piloting Exemplary IntegratedDistrict Health System 12.1 1.6 13.7
Project Management Support 4.5 2.0 6.5
Better Resource Allocation andRevenue Generatior. 1.1 0.3 1.4
Total Base Costs 78.4 36.4 114.8
Contingencies:Physical 3.9 1.8 5.7Price increase 11.6 2.2 13.8
Total Cost /a 93.9 40.4 134.3
Financing Plan:
Government of Indonesia 44.6 1.7 46.3IBRD 49.3 38.7 88.0
Total 93.9 40.4 134-3
/a Includes identifiable taxes and duties estimated at US$3.0 million equivalent.
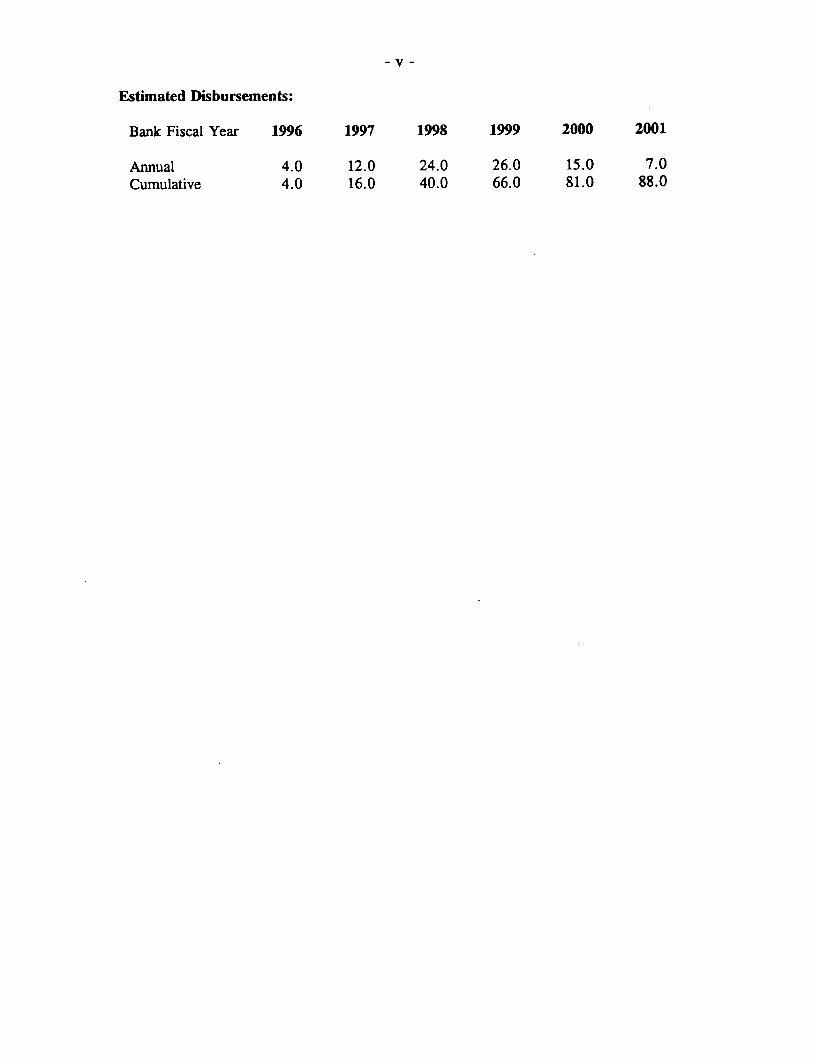
Estimated Disbursements:
Bank Fiscal Year 1996 1997 1998 1999 2000 2001
Annual 4.0 12.0 24.0 26.0 15.0 7.0Cumulative 4.0 16.0 40.0 66.0 81.0 88.0


- vi -
TABLE OF CONTENTS
Page No.
CHAPTER 1 HEALTH SECTOR ISSUES AND STRATEGY ...... 1....... A. National Health Trends ................................ 1B. Provincial Background ................................. 2C. Health Sector Issues and Challenges ........................ 6D. Health Sector Plan and Strategy .......................... 11
CHAPTER 2 BANK INVOLVEMENT AND LESSONS LEARNED ........ 13A. Background ...................................... 13B. Lessons Learned ................................... 14C. Rationale and Strategy for Bank Involvement .................. 16
CHAPTER 3 THE PROJECT ............. .. ................. 17A. Project Objectives .................................. 17B. Project Description .................................. 17C. Project Management and Implementation ...... .............. 25D. Monitoring and Evaluation ............................. 27E. Technical Assistance .................................. 30
CHAPTER 4 PROJECT COSTS AND FINANCING ................ 31A. Costs ........................................ 31B. Financing ........................................ 34C. Procurement ....................................... 35D. Disbursement ...................................... 39E. Accounts, Audits and Reports ....... .................... 40
This report is based on the findings of an appraisal mission which visited Indonesia inDecember, 1994 comprising Vicente Paqueo (Sr. Economist, Task Manager), Carol Ball(Operations Analyst, EA3PH), Dr. Iswandi (Operations Officer, RSI), Dr. James Heiby(Health Specialist, USAID), Patricia Daly (Health Specialist, consultant), and Dr. RobertNorthrup (Sr. Medical Officer, BASICS Project). The report was prepared by Vicente Paqueoand Carol Ball under the guidance of Samuel Lieberman (Principal Economist, EA3PH). Peerreviewers were Jose-Luis Bobadilla (PHN), Charles Griffin (AF2PH) and Willy de Geydnt(ASTHR). Marianne Haug, Director, EA3DR, and Himelda Martinez, Chief, EA3PH, haveendorsed the report.
This document has a restricted distribution and may be used by recipients only in the performance oftheir official duties. Its contents may not otherwise be disclosed without World Bank authorization.

- vii -
Page No.
CHAPTER 5 BENEFITS AND RISKS ........... .. ................ 41A. Benefits ........................................... 41B. Risks ............................................ 41C. Sustainability ........................................ 43D. Environmental Impact .................................. 43
CHAPTER 6 AGREEMENTS REACHED AND RECOMMENDATION ....... 44
TABLES IN TEXT
1.1 Socioeconomic and Health Indicators by Province ................... 34. la Summary of Project Costs by Components by Province ................ 324. lb Summnary of Project Costs by Component ........................ 334.2a Summary of Project Costs by Category of Expenditures by Province ... .... 344.2b Summary of Project Costs by Category of Expenditures ............... 354.3 Financing Plan ......................................... 364.4 Procurement Arrangements ................................. 38
CHARTS IN TEXT
3.1 The Expected Impact of HP IV on Health Care ..................... 18
ANNEXES
1. International and National Consultant Requirements .................. 462. Project Implementation Schedule .............................. 503. Monitoring and Evaluation: Performance Indicators ................... 624. Supervision Plan ........................................ 655. Project Activities by Component .............................. 676. Expenditure Accounts by Components and Year ..................... 717. Procurement Plan: Contracting and Review Responsibilities ............. 738. Estimated Schedule of Disbursements ........................... 749. Repelita VI Summary ..................................... 7510. SAF Operating Guidelines .................................. 7711. PDE Operating Guidelines .................................. 8112. Project Management ...................................... 8413. Basic HealIth Services.8713 Bsc elt eries ............................................... 814. Developing a Quality Assurance Program ........................ 8915. Selected Documents and Data in Project Files ...................... 98
CHARTS
1. Organization of Project Implementation Units ...................... 992. Organization of the Ministry of Health .......................... 100
- 1 -
CHAPTER 1HEALTH SECTOR ISSUES AND STRATEGY
A. NATIONAL HEALTH TRENDS
1.1 During its first 25-year development plan (1968/69-1993/94), Indonesiaachieved sustained economic growth rate averaging over 6 percent annually, and, in theprocess, reduced the poverty rate and the total number of poor people. During this period,Indonesia also registered advances in the health sector. The extent of improvement inhealth outcomes in the country is seen in the decline of infant mortality rate (IMR) froman estimated 145 per thousand live births in 1967 to 63 per thousand in 1990. A relatedindicator, life expectancy at birth, rose from 45.7 years to 62 years during the sameperiod. In addition, nutritional status improved, as illustrated by the decline in theprevalence of protein energy malnutrition and vitamin A deficiency.
1.2 As the economy grew, govermment was able to expand the number offacilities and the availability of modern health services throughout Indonesia. At thebeginning of Repelita I, there were 1,227 health centers (Puskesmas). By 1993, theirnumber reached 6,954, and there were also 19,977 health subcenters (Pustu). On average,there is now one health center per 27,000 people compared to about one per 96,000 in1968. Complementing this expansion of health facilities has been a rapid increase in thenumber of doctors, nurses, midwives and other health professionals relative to populationsize. Private provision of health services also expanded considerably, especially in urbanand peri-urban areas in Java and Bali.
1.3 As a result of increased accessibility of modern health care (combined withhigher fanily incomes and education), utilization of modem curative and preventive healthservices is greater today than in the past. For example, utilization of modern providerswhen sick has risen considerably among the poorest deciles in rural and urban areas, andin both Java and the Outer Islands. The use of certain preventive health measures suchas modern family planning has also increased at a rapid rate. For instance, thecontraceptive prevalence rate among married women of reproductive age rose to 55percent in 1994 from 10 percent in the 1960s, facilitating the reduction of total fertilityrate from 6.61 children in 1971 to 2.90 in 1994.
1.4 Despite these successes, Indonesia lags behind its comparator countries inhealth development and substantial gaps remain in the delivery of basic health services.After a sharp decline in the 1970s, IMR appears to have stabilized in the mid and late1980s at 75-80 deaths per thousand births. Current estimates suggest that IMR remains in

countries like China and Sri Lanka. Maternal mortality risks and malnutrition amongchildren remain high, and access to safe water and sanitation facilities by the poorcontinues to be a major concern.
B. PROVINCIAL BACKGROUND
1.5 Indonesia's provinces have shared to a greater or lesser extent in economicgrowth, improved access to modern health services and infant mortality rate decline. Thecountry's regional differences and commonalities are illustrated in the provinces includedin the project. As described below (see Table 1.1), these provinces must contend withdistinctive epidemiological and service delivery problems. (For a discussion of the choiceof these provinces, see para. 3.2). However, they also face comparable service deliverychallenges, including the need to improve quality of care within a common health caresystem. A second challenge is that of raising spending on basic health services, especiallyfor the poor.
1.6 East Java. This province, with the second largest population in Indonesia,had an infant mortality rate of about 64 deaths per thousand live births and a lifeexpectancy at birth of about 63.9 years in 1990. With an average poverty rate of about20.5 percent, East Java (Jatim) has over 7 million poor people (a fifth of Indonesia'spoor).
1.7 In Jatim, communicable and infectious diseases, particularly diarrhea andrespiratory infections, remain important causes of mortality and morbidity. Maternalmortality is high at 425 per thousand live births, suggesting continuing needs in thereproductive area. Moreover, malnutrition is common: more than half of pregnant womenhave anemia and iodine deficiency is endemic in 38 percent of villages.
1.8 East Java has an extensive network of health centers and associatedsubcenters, as seen in the relatively small average catchment area (Table 1. 1) and theavailability of doctors. Data show that almost all health centers have doctors. On thewhole, these facilities are highly utilized -- the average number of daily visits to healthcenters is among the highest in the country and health centers. Significant gaps, however,remain in the use of certain basic health services (BHS) by relevant population groups. Forexample, of the children under five years old, 10.7 percent had diarrhea in the past twoweeks prior to a survey in 1994, and many of them did not get needed oral rehydrationtherapy. In Probolinggo municipality (an urban area), less than half of pregnant womencompleted, the full cycle of recommended visits, compared to the provincial rate of 68percent.
1.9 Another aspect of the BHS gap is the low quality of health care beingprovided. A pilot study (Annex 14), using quality assurance (QA) techniques,demonstrates the low rate of compliance with recommended technical standards of care inthe management of acute respiratory infections (39 percent), antenatal care (66 percent),and vaccination (74 percent). Patient counselling, history taking and physical examinationwere found to be technically inadequate, decreasing the effectiveness of basic health

Table 1.1 Socioeconomic and Health Indicators By Province
East NTB W. E. West NationalJava Kalimantan Kalimantan Sumatra Average
Outputs and Outcomes I
IMR (1990 census) 64 145 81 58 74 71
% children under age five with diarrhea in past 10.7 15.2 14.6 7.6 12.4 11.1two weeks (1994) _
% pregnant women with anemia (1992 SKRI) 57.8 71.3 55.2 70 72.6 63.5
% births w/o antenaa] care 12.8 25.4 19.8 11.1 3.5 12.7
% delivery attended by doctors/midwives 34.7 13.1 29.2 52.1 69.5 36.1
llealth Delivery Features
Per capita health expenditures (1990/91 4,059 4,035 5,953 9,138 7,991 5,842Rupiah)
% health program expenditures for BHS 47 52 53 40 32 40(1990/91 Rupiah) _
Health center (HC) catchment area (1992): sq. 54 212 863 1,607 283 308km
Pop/HC (1992) 37,415 36,768 20,006 16,316 23,519 29,891
Number of daily visits to HC (1991) 75.4 24.9 31.3 53.0 50.3
Subcenter catchmcnt area (1992): sq. km 24 61 229 510 71 105
Doctor per HC (1992) 1.08 1.08 1.12 1.29 1.03 1.1
% HCs w/o doctors (1994) 0.8 2.8 3.7 7.5 3.2
% rural HCs w/o doctorc (1994) 0 0 0 5.0 5.9
% HC doctors less than 2 yearr. in current job 36 77 81(1992/93)
Socioeconomic Background
% poor (1990 Susenas) 21.8 27.6 33.8 16.0 15.1 19.6
% contribution to national poverty 20.5 2.7 3.2 1.5 1.5 100
Mcan household expenditures/month (1990) 26,805 23,164 29,409 40,792 31,628 30,338
% women 10 years old and over completed 32.7 28.6 33.4 36.7 51.1 35.3junior secondary or higher (1990)
Population density (1992) 691 173 23 10 83 97
% urban 1990 27.5 17.6 22.8 48.8 20.2 30.9

- 4 -
services in East Java. These findings indicate the need to establish quality assurancesystems in health facilities.
1.10 In regard health financing, consolidated public expenditures data (Table 1.1)suggest that recurrent government spending per capita amounted to only about two dollars.This is considerably less than the amount needed to finance the provision of essentialhealth services recommended by the 1993 World Development Report.
1.11 West Kalimantan. This province, which has the highest poverty rate in thecountry (33.8 percent), registered a decline in infant mortality in the last decade and gainsin education and other socioeconomic indicators. Moreover, despite its high poverty rate,West Kalimantan (Kalbar) has achieved a lower IMR (about 81 in 1990) than manyprovinces with lower rates of poverty.
1.12 Kalbar provides a sharp contrast to East Java in regard to geographic-,environmental and other characteristics. It is one of the largest provinces in the country(after Irian Jaya and East Kalimantan), but it has one of the smallest populations (3.2million in 1990). Over 50 percent of the population live along rivers. Few roads exist andtransportation and communications are difficult. In addition, environment sanitation is poorand safe water supply is not available for half of the population.
1.13 The main health problems of the province continue to be high infant andchild mortality from diarrheal disease, respiratory infections, tetanus, and malnutrition, andhigh maternal and perinatal mortality due to inadequate antenatal care, poor managementduring labor and delivery, unhygienic birthing conditions and poor nutritional status.Anemia is prevalent as a result of iron folate deficiency and of malaria and other parasiticdiseases. Diarrhea in West Kalimantan is the highest in the five project provinces,reflecting the need for improvements in water and sanitation. Malaria and tuberculosisremain common and are a major cause of adult mortality; Dengue fever and hepatitis areendemic and widespread through much of the province.
1.14 The number of health centers per person in Kalbar is higher than thenational average. However, the average catchment area is sixteen times larger than that inEast Java. The difficulty of transportation and the sparsity of the population in WestKalimantan explain why relatively fewer people visit these facilities. These facts also pointto the difficulty of providing basic health referral services and the need to adaptIndonesia's standard service delivery model. Data show that over 60 percent of womendeliver at home without a trained birth attendant. A fifth of pregnant women receive noprenatal care -- this figure is almost twice that in East Kalimantan. These findings are notsurprising considering that 60 percent of villages have no midwives.
1.15 Quality of health services is also a key concern. Standards of care are notclear to health staff (for example, many midwives lack the knowledge and skills for highquality antenatal care). About 80 percent of health centers have no laboratory techniciansand less than 40 percent of needed equipment are available in health staff centers.Moreover, a high percentage of doctors are inexperienced with less than two years in their

- 5 -
current assignment. Primary health care providers have inadequate knowledge in healtheducation and rational drugs use.
1.16 Funding for basic health services is inadequate, given the high cost ofservice delivery in Kalbar arising from transportation problems. The total per capita budgetfor BHS is only 65 percent that of East Kalimantan.
1.17 East Kalimantan. As with Kalbar, East Kalimantan (Kaltim) is a large andsparsely populated province with a density that is one percent of that in East Java. Healthcenters in Kaltim cover about 1,607 sq. km. on average, compared to East Java's54 sq. km. In 1990 about half of the population lived in urban areas, leaving the otherhalf of the population in the province's vast rural area. East Kalimantan is rich in naturalresources with the highest per capita provincial income. Kaltim's poverty rate is only halfthat of Kalbar and its IMR is 58 compared to 81 per 1,000 live births in Kalbar.
1.18 As in East Java where the highly urbanized areas are now exhibiting non-traditional morbidity profiles due to demographic transition, East Kalimantan is beginningto encounter the costly chronic and degenerative disease problems associated with higherincome areas. These morbidity patterns are emerging before Kaltim has adequately reducedthe infectious and acute diseases of developing areas. Cardiovascular disease, forexample, has now become the leading cause of death. Yet, infectious and parasiticdiseases continue to account for more than half of all reported episodes of disease anddeaths. Tuberculosis remains a major health problem and chloroquine-resistant malariais increasing.
1.19 Despite its large catchment area, basic health services are more available inEast Kalimantan than in West Kalimantan -- and even East Java in some respects. Kaltimhas more health centers and doctors per capita. Its immunization rate is the highest inIndonesia. Moreover, Kaltim has already pursued reforms in drugs management,decentralized planning and budgeting, and resource mobilization. And of the five projectprovinces, East Kalimantan has the highest public expenditures for health per capitaincluding large contributions by local governments.
1.20 Still, there are notable gaps in the provision and funding of basic healthservices. The coverage of maternal child health (MCH), for example, for safe delivery isestirnated to be only 65 percent in 1993. Kaltim has difficulty keeping experienced doctorsand paramedics in remote areas. As in other provinces, more needs to be done to improvethe quality of services and improve staff motivation to ensure compliance with standardsof care. Finally, providing adequate services to the rural population will require evenlarger operational subsidies.
1.21 Nusa Tenggara Barat (NTB). The province of NTB, with the country'shighest recorded infant mortality rate, has also made progress economically and socially.In the last five years, NTB along with East Kalirnantan has undertaken pioneeringinstitutional improvements, including decentralized and integrated budgeting, drugsmanagement, and resource mobilization, which should contribute to accelerated healthsector development.

1.22 Despite IMR gains from 187 to 145 per thousand live births and itsachievements in institutional development, NTB continues to face serious community healthchallenges. The high levels of infant and maternal mortality in the province reflect thehigh prevalence of communicable and infectious diseases -- in particular of tetanusneonatorum, acute respiratory infection (ARI), diarrhea, malaria and TB. A part of NTB'sproblem lies in its socioeconomic disadvantages: education is low and poverty rate is highcompared to other provinces. But maternal health and the quality of all basic healthservices remain problematic as well. Only about 15 percent of births are delivered withthe assistance of trained birth attendant. Of the five provinces, it also has the highestpercent of births without antenatal care. In terms of quality of health services, the above-mentioned quality assurance pilot study shows that as in East Java compliance rates withrecommended standards of care (Annex 14) are also low: 45 percent (antenatal care), 45percent (ARI) and 60 percent (vaccination).
1.23 With respect to the issue of funding, the amount spent on health by thepublic sector is almost only half of that in Kaltim despite recent increases in expenditures,indicating the need to further increase BHS funding (Table 1. 1).
1.24 West Sumatra. West Sumatra (Sumbar) is less urbanized than the otherprovinces except for NTB. Its educational level and income, however, are even higher thanEast Java, and its poverty rate is lower. The number of health centers per thousandpopulation is also higher. Yet, Sumbar's IMR is about the same as that of East Java.
1.25 Communicable and infectious diseases continue to dominate Sumbar'sepidemiological profile. These include ARI, TB, diarrhea, immunizationable diseases,malnutrition and pregnancy-related health problems. Immunization coverage needs to beincreased and Maternal and Child Care services, malaria and ARI control and nutritionalprograms expanded further. To date, West Sumatra has one of the lowest immunizationrates in the country. Moreover, the percentage of pregnant women with anemia is quitehigh at 72.5 percent and many of them have not received antenatal care. Furthermore, alarge proportion of births are unattended by health professionals.
1.26 Field visits also revealed that the quality and utilization of its basic healthservices also need to be improved. As in East Java and NTB, recommended standards ofcare are often not followed and frontline health providers need to learn quality assessmentand problem-solving techniques to increase the effectiveness of Sumbar's health system.
C. HEALTH SECTOR ISSUES AND CHALLENGES
1.27 Systemic Problems. As mentioned, despite differences in mortality andmorbidity levels and epidemiological agendas, the project provinces face similar servicedelivery challenges, including the need to improve performance and quality of care withinthe common health care delivery system. As with other line ministries, there are provincialhealth offices (Kanwil Kesehatan) and district health units (Kandep) directed by the centralMinistry of Health (MOH) which pass along and enforce centrally set policy guidelines andprepare health budgets. Routine service delivery matters are directed by health offices,

-7-
Dinas Kesehatan I and Dinas Kesehatan II, that have been established under the provincialand district administrations, respectively. Within each district, services are actuallydelivered by a network of health centers (puskesmas) and associated sub-centers andoutreach programs. Services are financed by funds channeled to local health offices andimplementing units. Funds flow through at least ten separate budgetary channels, eachwith its own regulations and monitoring arrangement. Central government assistance isstill specified and controlled by the different divisions in the central MOH, which is alsolargely responsible for training, hiring and deploying the health work force.
1.28 As mentioned, health system efficiency is generally low, as evidenced bythe underutilization of government facilities and staff in some facilities. For example, inWest and East Kalimantan the number of visits to health centers averaged only about 31or less per day in 1991. On the other hand, centers in East Java recorded, on average,about 75 visits per day.
1.29 Variable health center performance, as evidenced by relatively lowutilization levels, is attributable to several factors, including availability of resources; staffcompetence, attitudes and behavior; and established operating procedures and processes.A common problem in the five provinces is the shortage of funds and materials foroperations and maintenance. Health centers may not have reliable and timely access todrugs and laboratory materials, two key determinants of service quality and facilityutilization. Also, follow-up and basic referral services especially in poor and remotecommunities often can not be conducted in accordance with recommended practice becauseoperational funds (e.g., for travel) are not sufficient.
1.30 These shortages in materials and operational funds in the five provinces aredue to the inadequate resources allocated to basic health services (BHS). From a nationalperspective the low budget allocation is partly due to the health sector's low absorptivecapacity. It is estimated that current per capita public expenditures for health overall areone-half or less of the cost of delivering a minimum package of health services to allIndonesians (using the 1993 World Development Report suggested package for low incomecountries as a benchmark).
1.31 But other factors, particularly those relating to institutional capacity andorganizational culture also contribute to performance problems. For example, servicequality is affected by lack of sensitivity to clients, inefficient work processes, poormanagement, and weak performance incentives. These weaknesses can make governmenthealth facilities less attractive and accessible to clients. The limited time spent byphysicians with patients, inadequate counselling efforts, and the inflexibility of facilityservice hours are all telltale indicators. A related problem that has been documented inEast Java and NTB is variable compliance with technical standards of care. Staff may notbe clear about case management protocols, and know little about quality assessment andproblem-solving methodologies. And, current assessment mechanisms and supervisionpractices often do not provide the feedback and assistance needed to improve serviceperformance. Consequently, diagnoses may be unreliable and treatment ineffective.
- 8 -
1.32 Finally, health centers are sometimes poorly managed, while staff may haveinsufficient incentives to provide high quality care and reach out to prospective clients.Facility managers (doctors) often are unable to sufficiently guide health workers on casemanagement protocols, data analysis, problem-solving and use of staff time. Health centermanagers do not have much power over priority setting and resource allocation.Consequently, they lack the motivation to develop sensible, locally appropriate plans andwork out innovative initiatives.
1.33 A further deficiency in health system performance is that the poor continueto lag behind. For example, in 1991 infant mortality for mothers who had completed somesecondary schools, a reasonable proxy for household income, was one half that for thosewho had not completed primary schools. This finding applies in the five projectprovinces. The utilization rate of modem health services, including those provided by thegovernment, is also less than that of the well-off, as illustrated by survey data on Kaltimand NTB.
1.34 Given the relatively low budgetary allocation for health, government servicesneed to be more focused on the needs of the poor. Currently, the poor receive adisproportionately low share of overall health subsidies. A 1993 Bank study of theincidence of the health spending showed that the amount of subsidy per capita going to thetop income decile is about three times that of the lowest decile. This is due in part to thesubstantial share of health spending going to hospital services that are used mostly by thewell-off.
1.35 Improving Performance. Given its mixed record of success, the questionis whether the government health system in the five provinces can meet the various healthchallenges facing the country. Fortunately, there are indications that the system can beimproved and that publicly managed health facilities can provide better quality care. Asmentioned (para. 1.28), there are numerous districts in which average facility utilizationrate is very high. In addition, field visits revealed that there are health centers inIndonesia that are well-managed and highly utilized, despite budgetary and otherinstitutional constraints. Second, the experience of Third Health Project in NTB andKaltim suggests that even partial steps towards decentralization, giving greaterresponsibility and authority to district managers, can have a positive impact on healthsector progress indicators (Chapter 2). Third, a pilot project in NTB and East Java (seeAnnex 14) demonstrates that a modest investment in the establishment of quality assuranceprocesses can yield notable improvements in the quality of care. In a short period of lessthan a year, compliance with recommended standards of care increased dramatically, andclinics began to take steps to address client satisfaction issues.
1.36 These observations imply that further progress in health can be achieved byimproving public provision of services. To realize this expectation, however, will requirechanges in work processes, staff motivation, budgetary focus, and institutional capacity.
1.37 Facility-level Changes. Improvements are needed, in the first instance, inthe way service provision is organized at the puskesmas level (including its outreachactivities). This is a fundamental condition for enhancing the utilization of health services,

-9-
especially among the poor, and the effectiveness and efficiency of care. Raising theproductivity of frontline workers will require additional funds for health centers andchanges in the ways service tasks are allocated, carried out and supervised. Facility-levelmanagers need to be made responsible for public health services. This means giving themthe necessary support, incentives, and authority to carry out solutions they deemappropriate to their local situation, while at the same time making them accountable. Inthis regard, funds for health centers should not only be adequate, but should be providedin a manner that would allow managers the freedom to allocate resources in accordancewith locally appropriate priorities. This strengthening of managerial authority needs totranslate into a commitment to team-building and quality improvement, and a greater focuson client needs, demands and outcomes.
1.38 Such changes in organizational culture can be facilitated through theapplication of quality assurance (QA) mechanisms and procedures. QA is an approach tobuilding organizational capacity and culture that focuses on continuous improvement inservice (product) quality and its ability to satisfy consumer requirements. Institution ofQA systems has been an element in the success of many firms in various industries andservices including health care. In Indonesia, some industries and a few hospitals havestarted to apply QA concepts and techniques.
1.39 In its application to health, quality assurance deals with compliance withcase management protocols and broader issues regarding efficient provision and utilizationof services. In practice, QA programs involve establishing cost-effective standards forfacility services; building capacity for data-based "systems analysis" (which meansenabling staff to methodically investigate problems in quality issues and systemicprocesses); enhancing skills and authority to solve problems and learning appropriatelessons from their experience; cultivating team work; and facilitating client feedbacks andcommunity participation to improve patient satisfaction.
1.40 More Effective Supervision and Support. To facilitate and reinforcefacility-level changes, support from the provincial and district management will now haveto focus on expediting and motivating the work of frontline providers of care. The changein responsibilities and the agenda for those working at this level will require enhancedprovincial and regional decision-making authority and capacity, and changes in supervisoryculture, learning opportunities and incentives. To this end, the first step will be to extendthe decentralization measures that have been successfully piloted in Kaltim and NTB bythe Third Health Project.
1.41 In addition, the supervision system will have to move away from theestablished inspection approach towards facilitation and coaching of subordinates on waysto improve services. Supervisors, for example, need to focus on communicating standardsof care and teaching puskesmas staff how to make reliable assessments of the care theyprovide. Meanwhile, monitoring and evaluation data need to be rationalized to enable thesupervisors to help frontline providers more effectively. Data should include measures ofservice quality, consumer satisfaction and demand, and facility-level resource use andefficiency.

- 10 -
1.42 Better support for frontline providers also means that learning opportunitiesfor continuing education, and incentives that reward competency and performance need tobe established. Current training has low relevance to providers' needs, while reliance onoff-the-job (residential) training has often been be disruptive of staff work and is quitecostly. To meet the learning requirements of health facility staff efficiently, it is vital todecentralize training activities and plan them in accordance with documented knowledgedeficits. It is also important to establish rigorous, regular evaluation of trainingeffectiveness; test alternative methodologies such as distance learning that are lessdisruptive of staff work; and institute better control mechanisms for minimizing themonetary and opportunity cost of staff training. Furthermore, incentives need to berestructured so that they are tied to measures of actual skills improvement, instead ofencouraging staff to attend off-the-job training.
1.43 To reinforce the above-mentioned facility-level changes and the ability ofthe district and higher level units to expedite achievement of those improvements, someadjustments in MOH's personnel policies will also be required. One change should includedevolution of decision-making authority to allow district and facility managers to allocatemanpower resources or their financial equivalent to support their local health serviceimprovement plan, including hiring contract (private) providers. These administrators needto be made responsible and accountable, initially in pilot areas, for deciding on the numberof staff, skill mix, in-service training and task assignments within facility budgetconstraints.
1.44 To ensure that decentralization of decision-making results in higherproductivity, effective performance assessment mechanisms and incentives need to be putin place. Current performance evaluation systems, which are based on self-assessment,are ineffectual, and need to be replaced by a credible evaluation systems, which can beused in conjunction with schemes for accrediting health centers and rewardingperformance.
1.45 Finally, improving support for frontline providers and managers entailstimely access to drugs and equipment that for practical reasons are more efficientlyprocured by units at the district level or higher. Lacking an effective inventorymanagement system and demand-driven process of ordering, available equipment oftendoes not match what health facilities actually need and, as a result, are often unused orunderutilized. Therefore, in addition to replicating nationally the drugs managementsystem (LPLPO) developed by the Third Health Project (HP III), an analogous system forequipment management needs to be instituted.
1.46 Better Resource Allocation and Health Financing. In a recent advance,the Integrated DIP (development budget) or DIP Terpadu (an initiative under the ThirdHealth Project) gives the Dokabu (health district head) the authority to reallocate resourcesbetween basic health programs funded through the DIP. Further steps, however, areneeded to give district and facility managers the authority to reallocate resources betweenexpenditure categories and to reduce the number of budgetary channels. Withoutadditional progress towards decentralized and integrated budgeting, accountability for

- 11 -
health performance will remain diffused, and local health managers will have littlemotivation to initiate service improvement.
1.47 In addition to improved budgetary processes, increased public funding forBHS is needed to ensure that the poor have access to adequate, good quality healthservices. The Repelita VI goal of improving the health status of the poor needs to beinterpreted in terms of the share of BHS in the health budget. Quantitative targets willhave to be specified and spending levels regularly monitored, requiring collection andanalysis of integrated budgetary data. At present, such information is not available.Accordingly, a system to routinely track the total amount of resources going to basic healthservices and to evaluate the impact of proposed budgetary decisions on their funding willbe required.
1.48 Support for BHS can also come by raising fees for nonessential healthservices provided by public facilities, particularly hospitals, and by permitting greaterretention of revenues from health service fee. Public facilities currently charge low pricesfor their services. For example, public hospitals charge fees that on average are less than30 percent of cost. Local government should be encouraged not only to return all healthrevenues to the sector, but also to guarantee health centers a fraction of their revenues foroperations and maintenance and staff incentives. Of course, the poor must be protectedfrom the impact of price increases. This can be done through: (i) geographic pricediscrimination, charging zero or low fees at facilities serving primarily poor householdsand higher prices at facilities with better-off clients; (ii) individual price discrimination,such as giving health fee exemption cards to poor households; (iii) charging differentialprices at different levels of care to encourage self-selection; and (iv) larger fees foridentifiable groups of better-off individuals such as civil servants. Pilot activities on priceadjustments and ways of protecting the poor from fee increases have been conducted inKaltim and NTB and need to be extended to other areas.
1.49 Finally, expanding health insurance for the better-off may enablegovernment to target more public resources towards the poor. In principle, provision ofinsurance would redirect the insured population towards higher quality private sectorservices, reducing their use of public facilities and increasing the public budget for thepoor. How best to promote this expansion, however, and address important design issuesneeds to be explored, for example, by testing self-financing prepaid health plans, usingprivate providers and capitation payments. Pilot efforts would allow Perum HusadaBhakti, the civil servants' health insurance system, to develop ways of reducing itsdependence on subsidized government services and would give MOH direct experience onhow to contract private providers to deliver prepaid packages of health services, ensurequality of care and deal with enforcement issues.
D. HEALTH SECTOR PLAN AND STRATEGY
1.50 The government is aware of the issues of equity and efficiency in healthsystem performance, and intends to address them during Repelita VI, the current five yeardevelopment planning period (I 994/95 - 98/99). The objectives and policies of RepelitaVI are consistent with the steps suggested above to improve health sector performance.

- 12 -
1.51 The general objective of Repelita VI is to raise the health status of thepopulation by increasing the quality and scope of health services and by paying greaterattention to the needs of the poor. It aims to achieve specific targets for infant mortalityrate, life expectancy at birth, maternal mortality rate, nutritional status and other healthoutcomes which are presented in Annex 9. For example, GOI aims at reducing IMR to50 deaths per thousand live births at the end of Repelita VI-current estimates put IMRin the 55-60 range.
1.52 As specified in Repelita VI, the Ministry of Health would focus onimproving equity and quality of health services, with particular attention to the poor,children, and neglected elderly. To achieve these ends, MOH is to emphasize cost-effectiveness in service delivery, by decentralizing health management and decision-makingauthority to provincial and district governments, and through greater mobilization ofavailable resources, including non-governmental capabilities. In allocating health budgets,MOH is to give priority to highly cost-effective basic health services and interventions thatdirectly benefit the poor. The Ministry will also promote intersectoral cooperation throughimproved participation of community, private sector and professional associations.
1.53 For GOI, the Fourth Health Project (HP IV) represents a vehicle throughwhich to test ways of attaining the goals of improving the quality and equity of health care.In particular, this project would enable GOI to:
(a) Effect facility level changes to raise the level of performance of basic healthservice (BHS) providers, specifically in rendering higher quality BHS andreaching out to the poor;
(b) Adjust institutional arrangements at the provincial and district levels so thatfrontline providers receive stronger support from higher level staff andaccountability of both health center and district management is enhanced;and
(c) Improve health financing by allocating a greater percentage of governmenthealth spending to highly cost-effective interventions (BHS) and raising theshare of health benefits of the poor, increasing local government financialsupport for health and raising the rate of retention of revenues from fees forhealth services to support and encourage their improvement, and adjustingbudgetary arrangements, in particular promoting the use of block grants forhealth services.

- 13 -
CHAPrER 2BANK INVOLVEMENT AND LESSONS LEARNED
A. BACKGROUND
2.1 The Bank has funded thirteen health projects in Indonesia since 1977. Theseinclude support for nutrition, community health, health manpower development, water andsanitation, referral facilities and family planning initiatives. Bank loans for these projectstotalled US$602 million. Thirty-eight percent of these loans financed "first generation"projects, which consist of loans approved before 1989.
2.2 These first generation or "start up" projects had a mixed record of success.The first four population projects have been implemented satisfactorily and havecontributed significantly to the success of Indonesia's family planning program. TheSecond Nutrition and Community Health Project (NCH II) also achieved its mainobjectives of promoting "Posyandu", a monthly community-based integrated delivery offive high priority health interventions at designated locations. On the other hand, theProvincial Health Project and the Second Health (Manpower Development) Project wererated as unsatisfactory due to both design and implementation problems.
2.3 Of the second generation (follow-up) projects, the Third Health Project (HP111) is now widely recognized as a well implemented, carefully designed operation. Thisinnovative project, which started in 1989 and is now in its last year of implementation, hassupported empowerment of provincial and district health authorities, management reformsand resource mobilization in the provinces of Kaltim and NTB. How HP III has helpedshape government policy and attitudes towards the above-mentioned issues is discussedbelow. Of the other second generation projects, Third Community Health and NutritionProject (CHN III) and Water Supply and Sanitation for Low Income Communities Project(WSSLIC), appear promising but are only in the second year of execution.
2.4 In addition to sector lending, the Bank has conducted several sector studieson health planning and budgeting, health insurance, social expenditures and poverty, andthe health workforce between 1989 and 1994. Furthermore, analytical work on the healthsector has been regularly undertaken for the Country Economic Memorandum (CEM) andthe Country Assistance Strategy.

- 14 -
B. LESSONS LEARNED
2.5 First Generation Projects. The following lessons have emerged from theexperience of the first cohort of health projects:
(a) Too rapid expansion of activities can jeopardize quality and lack of attentionto quality assurance and effectiveness issues seriously limits project impacton health outcomes. It is for this reason that despite the rapid expansion ofPosyandu and the accompanying dramatic increases in immunization,nutrition surveillance, and diarrhea control activities, infant mortality ratehas declined little in the last 10-15 years.
(b) A project is likely to be more effective if it is demand-driven. Much of theexplanation for the failures of the above-mentioned manpower developmentand hospital construction projects can be traced to past disregard of thisfactor. For example, hospital capacity was expanded by 30 percent, whenthere was little effective demand as evidenced by the fact that public healthfacilities in Indonesia were widely underutilized.
(c) Right from the start, project preparation and design should maximizeownership by concerned agencies and policy-makers to ensure timely andeffective implementation. This is a key characteristic of the successfulpopulation projects and the prime factor for NCH II's satisfactory andtimely completion-achieved despite unanticipated problems of counterpartfunding and other initial difficulties delaying project implementation.
2.6 Second Generation Projects. From the recent group of projects, the mostimportant lessons derive from the experience of HP III. The greatest success of HP IIIhas been the introduction of a process of institutional reforms that have had as a focusstrengthening the provincial and district health offices' role in health programimplementation. These reforms include measures for decentralization and drugmanagement, which have been accepted for national replication in Repelita VI.
2.7 Provincial and district strengthening was achieved by developing thefollowing instruments:
(a) the Integrated Health Plan and Budget (IHPB). This is a consolidatedframework depicting all flows of funds to health programs in the sector;
(b) the Integrated DIP or DIP Terpadu and the Basic Health Service Package.This is the consolidation of the central budgets (DIPs) for community healthinto a single budget for high priority basic health services.
(c) transfer of budget responsibility to the District Health Officer (Dokabu), astep that expanded the resource allocation authority of the Dokabu.

- 15 -
2.8 These measures have engendered a more decentralized planning process withprovincial, district and puskesmas staff becoming more involved in the process; greaterflexibility and decision making authority at the local level; and clearer sense ofaccountability and faster flow of funds. In addition, as provincial and district governmentsbecame more aware of health issues and more involved in their solutions, local fundingrose dramatically. Furthermore, drugs shortages at the health center have been minimizedin the HP III provinces, not only because of increased budgetary allocations but alsobecause of the development of an innovative system (LPLPO) of drug management andsupply.
2.9 Two overall lessons have emerged from these HP III outcomes:
(a) First, incremental steps towards decentralization, particularly strengtheningthe responsibility and authority for and the management and delivery ofhealth programs at the district level, have had considerable positive impacton health sector development.
(b) Second, local government involvement is vital to the success of anydecentralization effort. A substantial "marketing" effort is required fromthe outset of preparation and through project implementation.
2.10 The achievements of HP III, however, represent just a start towardsenhancing the capacity and organizational culture of health centers and improving supportfrom the district and provincial levels of government. Much remains to be done. Forexample, quality of care provided at puskesmas is still deficient in terms of compliancewith case management protocols, indicating the need for introducing quality assurancemechanisms. Furthermore, in spite of the freedom to shift budgets between programsincluded in the DIP Terpadu, district managers are still unable to reallocate these resourcesacross categories of expenditures as they see fit. Puskesmas managers also continue tofollow targets reflecting central level priorities, rather than determining their own prioritiesand allocating their DIP Terpadu budget in accordance with local disease patterns.Another lesson, therefore, emerges from HP III experience:
(c) Follow-up efforts may be needed to sustain institutional changes and extendthem to health facilities to achieve more satisfactory levels of health serviceperformance.
2.11 In conclusion, institutional and management advances have occurred inKaltim and NTB, which have already resulted in improved health services. Additionalefforts, however, are needed to supplement these achievements. From the nationalperspective, follow-up projects are needed to facilitate replication of the aforementionedinnovations in the other provinces. Equally important, the process of experimentation andinstitutional reforms would also have to be broadened to bring changes in other areas thatare critical for higher health system performance.

- 16 -
C. RATIONALE AND STRATEGY FOR BANK INVOLVEMENT
2.12 The health sector is an appropriate area for Bank involvement. Publicintervention in the sector is legitimate and necessary to maximize sector efficiency. Manybasic health interventions have public goods characteristics; moreover, marketimperfections in the health sector are quite serious due to the asymmetry of informationbetween consumers and providers. Some public interventions can also be justified ongrounds of equity. In particular, Bank analysis show that the provision of basic healthservices is a cost-effective way to alleviate poverty.
2.13 To realize more fully the benefits from government health interventions,GOI needs to make adjustments in its public health system and in its approach to healthcare. These changes involve a combination of policy changes, revised institutionalarrangements, strengthening of incentives structures, technical capacity building,procedural reforms, and improved health financing.
2.14 The Bank is well suited to provide the support needed to deal with thesevarious issues. First, it is at the forefront in assisting health sector reforms in Indonesiaand has accumulated relevant knowledge and experience. Its analytical work and recentinnovative lending operations have dealt with key sectoral issues. Second, the Bank hasestablished an excellent partnership with GOI and a credible approach to health sectorreform. Third, Bank involvement is consistent with its global health development policyand its country assistance strategy (CAS) for Indonesia.
2.15 In this regard, HP IV represents an excellent vehicle for pursuing theobjective, cited in the CAS, of helping Indonesia overcome human resource bottlenecksby strengthening the decentralized management, quality and utilization of basic socialservices. HP IV would contribute to the CAS agenda by:
(a) supporting GOI efforts to enable and motivate frontline health providers andmanagers in public facilities to deliver higher quality, more accessibleservices that fit the needs and demands of clients;
(b) promoting decentralization and enhancement of capacity of provinces anddistricts to supervise and support lower level managers and staff; and
(c) assisting in improving health financing by reorienting (a) publicexpenditures in health to assure that a larger share of sectoral allocationsgoes to the poor and provision of basic service packages, and (b) sectorfinancing mechanisms, with much greater reliance to be placed on directcost recovery and health insurance modalities.

- 17 -
CHAPTER 3THE PROJECT
A. PROJECT OBJECTIVES
3. 1 The aim of the project is to improve health outcomes by giving provinces,districts and puskesmas managers greater authority, responsibility, resources, and skillsto enhance health care quality and equity. Specific project objectives are: (i) to increasethe authority and capacity of provincial and district health offices and health centers to planand implement health programs as they deem appropriate to local conditions; (ii) to ensurethat the provision and consumption of key health services conform to affordable, cost-effective standards of care; (iii) to improve access and utilization of these health servicesby the poor; and (iv) to improve efficiency in the delivery of basic health services (BHS).These objectives address key issues that are essential to further health sector developmentand poverty alleviation.
3.2 The project would cover five provinces: West and East Kalimantan, NusaTenggara Barat (NTB), West Sumatra (Sumbar), and East Java (Jatim). Except for Jatim,all districts in each province would be covered. Fourteen districts in Jatim would beincluded, chosen in accordance with selection criteria that gave highest priority to povertyand BHS gap indicators, and commitment to price reforms and facility fee retention foroperations and maintenance (O&M) and staff incentives. -The choice of the five provinceswas based on the following considerations. First, Kaltim and NTB were included tofollow up assistance provided under HP III with additional innovative activities deemednecessary to bring about required changes in organizational culture and institutionalcapacity at the facility level. Second, GOI chose the remaining three provinces from thosethat did not have any major donor-assisted health project. Within this group, priority wasgiven to those provinces with the worst poverty indicators (Kalbar) and the largest numberof poor families (East Java).
B. PROJECT DESCRIPTION
3.3 Project Design. The Fourth Health Project (HP IV) adopts a systemsapproach (see Chart 3.1) to quality and equity improvement and employs variousmechanisms to bring about facility-level changes and adjustments (described below) at theprovincial, district and central levels to achieve its objectives. Provincial and district healthoffices would be given enhanced responsibility and authority for planning andimplementing most of HP IV's activities, including the processing of contracts. The roleof the Central Ministry would be to provide general guidance and technical assistance and

Chart 3. 1: The Expected Impact of HP IV on Health Care
leiath Pollcyv Supervldon and SuPoort Tnsitutions peliver of Basic lealth Services (BIIS) Outputs Outcomes
1 2 3 4 9 toCentral Provincia llealth District Health District Hospital basic referral services Effectlve nue of BHS by Mortali nd
Ministry of Ofmces omce population. esp. the poor morbidityllealth
-Program pr~~~~~~~~~~~~~~~~~~~-ovidtraer wihLiS fe expectancy at birth-Program. . providcrn Infant mortality rate
-Health policy Supervision Implenmentation llealth Center (Subcenter sad Outreach) Immunuiation rate Maternal mortality rate-Tech gidance Monitoring gemnt Annknatal care -DLsablty rateNatL budget lealth budgeting -Hlealth center & 6 7 8 coverage DlabIity-adjustedprog-mming -01lospital fe-e district hospital *-Inputs Worik Proes au Service Features Births delivered by i c fe yean (DALYs)
-Overnl gh t regultion supervslotk trained health-Training -Health budgeting -Staf7xskllh -Management -Accessibility praectioners
-hlospital fee -Buildings -Quality asurance -QUlity lealth center visitsregulation -Equtpment mechanisms Technical Others
-Drugs -Learning Interpersonal-Supplies -Community and -Efciency -Compliance rate with n-Salaries patient interactions -Equity mcommen ed standards-Incentive of car-OtherO&M
Other key projed outputadncators
-Rate of adoption of
Projcct support for provincial, district, and central level changes Project support for facility-level changes quality asuranceprocesses
Shamr of Central,provincial and district
Instiuti onal Developmerni Conponent * Resouroe Allocafion and Facility-level Service Imnprovanent Component bealth subs toSuppoet for Revenue Oenaalional Coonent Support for. BHS and the poor
Support for
* Quality auran mechnins - Hcalh facility cowssnction nd upgrdingTraining nd curriculum - TA/studies for iareased feet -Spe assistance program for basic healh
- Performanc-linked inetives and targding of health spending sevice, e.g, discretionary health cenler funb- RephiciLion and platling imovatim to BHS and the poor oprtaiona rcauitment cost suppot
e.g., discretionary health fundsfor distsicts
FOURTH HEALTH PROJECT ASSISTANCEhp4-cht3.doc
- 19 -
to disseminate innovations and lessons learned from the experience of provinces anddistricts. Fourth Health Project's design is highly cost-effective, compared to otheralternatives for improving health outcomes and poverty alleviation. First, the basic healthinterventions (currently underutilized) the project would support are highly cost-effectiverelative to other health services, as shown by the 1993 World Development Report.Second, a Bank study of the incidence of health subsidy benefits in Indonesia reveals thatspending on health center and subcenter services, which is currently low, are strongly pro-poor compared to other public subsidies. Hence, reorienting government healthexpenditures towards improving basic health services would not only be efficient but alsobe equitable. Third, a pilot study (see Annex 14) reveals that a modest amount ofinvestment in establishing quality assurance processes could lead to considerableimprovements in quality of care and, hence, in enhancing the cost-effectiveness of theabove-mentioned basic health services. Fourth, greater efficiency could be achievedthrough the following district, central and facility level changes and mechanisms.
3.4 Facility-Level Change. The first project mechanism is improvement ofbasic health services provided by puskesmas and, to a limited extent, by district hospitalsin the five provinces. (In this report, the term puskesmas or health center also refers toassociated sub-centers and outreach programs.) Here, the agenda is to change the workprocesses, attitudes, skills and other aspects of organizational culture of these facilities,while giving them additional resources that would enable the provision of higher quality,more accessible services that fit the needs and demands of clients.
3.5 To this end, the project would introduce and establish facility-level qualityassurance (QA) processes suitable to the Indonesian situation. The QA program, whichhas been based on lessons from a small pilot project in NTB and East Java (see Annex14), would be directed at five areas: technical competence, client satisfaction, efficiency,coverage/access, and effectiveness. Health center staff would initially learn to analyze andresolve simple problems of non-compliance with clinical standards and would progress tomore complex issues pertaining to priority-setting and health outcome problems. Toachieve the aims of this quality assurance program, the project would support on-the-jobtraining and encourage self-learning in areas of concern.
3.6 HP IV would finance expenditures needed to carry out service improvementplans drawn up by frontline providers through problem-solving and priority settingexercises. For this purpose, a program would be established providing Special AssistanceFunds (SAF) for health centers. SAFs comprise discretionary resources that puskesmasmanagers could use to purchase eligible expenditure items (mainly for operations) neededto initiate and implement their plans. Agreed SAF Operating Guidelines in Annex 10present the list of eligible expenditures together with the operating procedures and theassignment of oversight responsibility. (Expenditures made through the SAF would bereferred to in the cost tables below as SAE or Special Assistance Expenditures.)Furthermore, additional assistance for improving physical facilities, equipment, and otheractivities needed to reduce BHS quality and coverage gaps would be provided throughother (less flexible) budgetary arrangements.

- 20 -
3.7 To maximize their impact, use of the above funds would be concentrated onselected basic health interventions that are expected to be highly cost-effective. Annex 13presents an initial list of these interventions (Basic Awal). This list would be used duringthe first year of the project and revised on the basis of a more systematic analysis ofdisease burdens and the relative cost-effectiveness of health interventions.
3.8 Provincial, District, and Central Level Changes. Improvements in thecurrent institutional processes and the attitudes and technical assistance capacity of staffin health districts and provincial units comprise the second mechanism and agenda.Assistance would be geared towards building the ability of provinces and districts tosupervise, support, and reward frontline providers of care, while at the same time makingdistrict and facility managers more accountable for their performance.
3.9 To bring about these changes, HP IV would reorient the way supervisorsdo their job. They would be encouraged to change their role from acting as workinspectors (mainly noting bureaucratic shortcomings) to coaches who would help frontlinestaff improve their services, treating them as internal clients and sharing with themproblem-solving responsibility. In this new role, supervisors would become sources ofnew ideas and conduits for communicating standards of care to puskesmas staff.Accordingly, HP IV would provide supervisors learning opportunities to acquire a clearunderstanding of recommended clinical standards, the ability to analyze complianceproblems and other more complex service quality issues, as well as skills in team-buildingand monitoring. In addition, an evaluation system would be developed whereby frontlinestaff would be able to provide feedback on the effectiveness of their supervisors incarrying out their new role.
3.10 The project would give provincial and district health offices the additionalfunds needed to support the above agenda. Resources would be provided in ways thatwould advance decentralization and make resource allocation decisions more demand-driven. Hence, in funding equipment and drugs, the project would institute (prior to majorpurchases of these items) reforms of their inventory and management not only to minimizewastage and increase reliability of supply, but also to give provincial, district and facilitymanagers a voice in the procurement process to ensure that it is responsive to frontlineneeds. HP IV training prograns would be decentralized, emphasizing on-the-jobapproaches tailored to address knowledge and skills deficits identified by health staffthrough their QA exercises.
3.11 Furthermore, discretionary special assistance funds (SAFs) would beprovided to health districts to finance eligible expenditures they deem necessary (withinthe parameters set out in the SAF Operating Guidelines) to carry out BHS improvements.These expenditures would include, inter alia, outlays for supervision, monitoring andevaluation, and redeployment of staff, for which HP IV provinces and districts would begiven the necessary authority. Through these special assistance funds, HP IV would helpprovinces and health districts establish a track record that could eventually help acceleratefurther budgetary integration and decentralization of resource allocation and personneldecisions. During negodations, GOI gave assurances that it would carry out the
- 21 -
activities under the SAF in accordance with the SAF Operating Guidelines, agreed withthe Bank.
3.12 As authority is devolved to provincial, district and frontline managers, HPIV would simultaneously strengthen their accountability and enhance their motivation toimprove health service performance. Accordingly, as part of the quality assurance andother initiatives to bring about changes at the provincial and district levels, the projectwould develop new health center accreditation and performance-linked incentive systems.These systems would be based on an agreed list of performance indicators (para. 3.41 andAnnex 3) and linked to various incentives that GOI would like to test. One scheme wouldbe for districts with excellent performance to receive their Integrated DIP in a form thatwould increasingly look like a block grant. Another is to raise their SAFs as the districtsshowed greater absorptive capacity, while freezing or reducing that of consistently non-performning districts at initial levels until remedial measures have been taken and the lattershowed evidence that they can absorb additional funds efficiently. In addition, based onthe experience of Balikpapan and other puskesmas in Kaltim regarding their use of facilityfees, districts would be encouraged to guarantee staff of accredited health centers a fractionof their revenues from health service fees and allow them to use the money for theiroperations and maintenance as well as staff incentives.
3.13 Finally, to lay the ground for further health system advances, the projectwould support trials of bolder innovations and QA studies (e.g., on standards of care anddocumentation of best practices). In this regard, a limited amount of funds would beallocated to finance program development expenditures (PDE) needed to pilot the testingof managed care schemes using private providers, a system for their accreditation, MOHhiring processes, and other high priority issues specified in the PDE Operating Guidelines(see Annex 11). The list of eligible expenditures, the criteria for approval of proposalsand the process of review are described in these guidelines. During negotiations, GOIprovided assurances that it would carry out the Program Development activities inaccordance with the Program Development Expenditures Operatng Guidelines, agreedwith the Bank.
3.14 Increased Financial Support for BHS and Poverty Alleviation. The thirdmechanism and agenda are resource mobilization and the reorientation of governmentspending to raise funding of basic health services (BHS). The above initiatives wouldcontribute to this agenda by establishing provincial and district capacity to deliver effectivehealth services and, thereby, making the health sector an attractive area for publicinvestment. These steps are crucial to overcome the reluctance of concerned planning andfinance officials to boost public spending on health because of their view that the healthsector does not have the absorptive capacity to use additional funds effectively.
3.15 HP IV would also encourage increased provincial and district funding ofBHS by fostering greater local government awareness of health sector issues andinvolvement in their solution. Fees would be increased for non-BHS personal healthservices provided by publicly managed facilities and the return of all health revenues tothe sector would be promoted. At the same time, measures would be taken to develop and

- 22 -
institute schemes (e.g., geographic price discrimination or use of health cards for feeexemption) to protect the poor from the impact of fee increases.
3.16 A further step to raise funding of basic health services to the poor is theexpansion of self-financing health insurance schemes among the better-off, which includecivil servants, to reduce their dependence on highly subsidized government health services.The PDE funds mentioned above would be available to finance such proposals. Anexample of these proposals is building the capacity of Perum Husada Bhakti to develop andmarket self-financing prepaid health plans for the well-off and in the process shift thedelivery of the civil servants' health insurance benefits to private sector providers.
3.17 Lastly, HP IV would introduce a budgetary practice of giving more financialassistance to health facilities which attend primarily to the needs of the poor than thoseserving the better-off. The SAF would, therefore, be structured so that health centers anddistricts serving primarily poor communities would be allocated relatively more funds.This design feature would reinforce the equity impact that might be expected fromallocating a larger proportion of public funds to basic health services. In Indonesia, theincidence of benefits from these services, which are primarily delivered by health centersand their subcenters, strongly favor the poor.
3.18 GOI brought to negotiations a Statement of Policy of the Ministry of Healthand a Statement of Provincial Government Support for the project, showing thecommitment of MOH and the Governors of participating provinces to an increase in theamount of Central and provincial health subsidies going to the poor as well as to theprovision of basic health services. In this regard, annual targets were agreed atnegotiations for increasing health related public spending for the poor and for basic healthservices.
3.19 Agreement was also reached with GOI at negotiations, providing for higherSAFs per capita for health centers and health districts in poor areas than those in well-offareas. Moreover, assurances were provided during negotiations that GOI would: (a) notlater than December 31, 1995, furnish to the Bank a classification, on the basis ofpoverty issues, of health centers and health districts in the project provinces, as referredto in the aforementioned Statement of Policy and Provincial Government Support; (b)not later than October 31, 1996, furnish to the Bank guidelines for pricing personalhealth services provided by health centers and hospitals and protecting the poorfrom theimpact of price adjustments; and (c) not later that October 31, 1996 implement thesystem for the annual collection of consolidated budgetary information to monitorachievement of the above-mentioned targets and for assessing the impact of proposedcentral and provincial budgetary allocations on the funding of BHS.
3.20 Furthermore, assurances were provided by GOI during negotiations that itshaUl cause the local governments of the participating provinces to take aU actionsrequiredfor the implementation of the Provincial Government Statement in each districtselected to participate in the project, including the requirement: (a) that the share ofdistridc health budget going to BHS and the poor be increased annually; (b) that healthservice fees be adjusted upwards and that such revenues be used for purposes of the

- 23 -
health sector; and (c) tW part of the earnings of the health centers be used by suchfacilites for health center perfornance incenfives.
3.21 Components. In each province, the project consists of facility-level serviceimprovement, institutional development, and resource allocation and revenue generationcomponents. (For a detailed description of each component, see Annex 5.) In the facility-level service component, funds would be used: (i) to improve the physical facilities ofhealth centers, subcenters and, to a limited extent, district hospitals, including support forneeded equipment, water supply, storage facilities, vehicles and furniture; and (ii) reducethe current BHS gaps in quality and coverage by providing discretionary health centerSpecial Assistance Funds (SAFs) and other additional resources for operational andrecurrent costs (on a declining rate) to support implementation of quality assurance andother BHS programs initiated by frontline providers.
3.22 Funds for institutional development would finance improvements in thecapacity of provincial, district, and Central-level agencies to assist, motivate, and supervisefrontline health providers in delivering accessible high quality packages of basic healthservices. Specifically, project expenditures would go to: (i) establishing quality assurance(including health center accreditation systems) and supporting training/curriculumdevelopment activities; (ii) developing effective performance-linked incentives systems;(iii) financing discretionary district SAFs, replication of HP III innovations, and other pilotprograms that could lead to improvements in the organizational culture of the public healthsystem and its role in the provision of basic health services; and (iv) strengthening thecapacity of Central-level MOH units to give technical guidance, disseminate qualityassurance and other HP IV innovations, and carry out oversight functions.
3.23 Finally, funds would be provided in the resource allocation and revenuegeneration component for technical assistance (TA), data collection and analysis, materialsand workshops to design and promote facility-level fee increases and revenue retention,and institute more effective targeting of health subsidies to appropriate recipients andactivities. Funds under this component would help MOH: (i) to develop and establishmechanisms for monitoring and reporting the total health subsidies going to BHS and thepoor, especially their corresponding share in Central and local health budgets for thenation as a whole and for each of the five provinces; and (ii) to develop a system foranalyzing annual APBN (National Budget) and APBD (Regional Budget) budgetarydecisions in terms of the above financial indicators.
3.24 Provincial Health Improvement Programs. Project activities and outlaysby province are described below (amounts in parentheses are base costs; see Table 4.1(a)for detailed breakdown):
3.25 East Java (US$23.1 million equivalent): The project would mainly fundoperational and incremental recurrent costs (73 percent) to meet the drugs and otherrequirements of an expanded BHS coverage program and developmental expenditures (13percent) needed to establish quality assurance practices and supporting training programs.Over a fifth of Jatim's project cost would finance discretionary SAFs for health centers anddistricts which support GOI's decentralization efforts. Outlays would be directed at existing

- 24 -
deficiencies in the quality and coverage of ten basic health services, which includenutrition, maternal and child care/family planning, immunization, health education, controlof communicable diseases (dengue, malaria, TB, diarrhea, ARI and school healthservices). Other uses of the above amount include inter alia funding of supervisionimprovements and pilot activities involving private health providers, health insurance,district-determined redeployment of health staff, the development of performance-linkedincentives and replication of the drugs management and other HP III innovations.
3.26 West Kalimantan (US$29.6 million equivalent): A distinctive feature ofKalbar's program is its support for technical assistance and other components that wouldaddress systemic issues arising from the application of Indonesia's conventional healthdelivery system and approaches to an area characterized by non-standard geographicconfigurations. Kalbar's SAFs (30 percent) and budget for QA and supporting activities(10 percent) would be the vehicle to enable the province to tailor its approaches to thedistinctive environment within which its health programs operate. In addition, the projectwould support civil works (40 percent) and equipment provision more heavily than in otherprovinces to improve the physical infrastructure of its publicly managed basic healthservices facilities. Referral facilities for maternal and child services would be strengthened.Water and sanitation programs would be improved to reduce the high prevalence rate ofwater-borne diseases.
3.27 Nusa Tenggara Barat (US$9.0 million equivalent): NTB would furtherdevelop, expand and institutionalize the quality assurance program that it has successfullypiloted. In addition, it would try out Referral Health Centers and develop a program toenhance the ability of traditional birth attendants (the predominant source of birth deliveryassistance) to conduct their practice safer and to make timely and appropriate referrals ofhigh risk pregnancies. NTB's SAFs (28 percent), quality assurance efforts (15 percent),and support for health equipment and recurrent costs for supervision and medical supplies(21 percent) would provide funds to promote safe motherhood, child immunization, ARIinterventions and other BHS activities.
3.28 East Kalinantan (US$14.5 million equivalent): As in the other provinces,the project would support the development of effective systems of performance evaluationand associated incentive schemes linked to service improvements in terms of bothutilization and quality assurance-based indicators. Kaltim would further develop andexpand its pioneering efforts to use health center fees as a source of extra-budgetaryresources and incentives for improved service performance by health staff. Like East Java,it also plans to use project funds for Program Development Expenditures to pilot amanaged prepaid health care system in Balikpapan that would utilize private providers ofhealth services.
3.29 However, project funds allocated for this province would be used largelyto establish quality assurance processes and supporting activities (about 10 percent) andfinance recurrent costs for health supplies (15 percent), SAFs (23 percent) and equipment(17 percent) purchases to address Kaltim's remaining problems of communicable andinfectious diseases. As in other provinces, the SAFs would not only increase discretionaryresources available to district offices and health center managers to respond more quickly

- 25 -
to quality problems documented through the application of QA methodologies; they wouldalso be used as a vehicle for developing and instituting a budgetary practice of providingextra operational resources for underserved areas. In this regard, East Kalimantan plansto initially give poor health districts 50 percent more SAFs per health center than those innon-poor areas.
3.30 West Sumatra (US$27.5 million equivalent): This fund would support:(i) the development of an institutionalized QA program; (ii) the expansion of outreachactivities, particularly in the remote areas; (iii) training to address skills deficits that affectquality of care; (iv) expanded supervisory contacts with service providers to facilitate theQA program and development of interventions to make these contacts more productive andaccountable; (v) redeployment of staff to underserved areas; (vi) the provision of adequatehealth supplies and greater availability of functional equipment in health centers; and (vii)decentralized problem-solving initiatives by health center, district and provincial managers.
3.31 Sumbar would use the above funds among others to raise immunization rateand utilization of cost-effective health interventions to strengthen MCH services andcontrol of communicable and infectious diseases such as ARI, TB, malaria, and diarrhea.In this regard, about a quarter of the above funds would finance discretionary SAFs thatthe province can use to expand its BHS programs, especially to poor communities. Inaddition, another third of the US$27.5 million would be allocated for drugs and otherrecurrent costs to meet shortages of supplies. West Sumatra would further spend about12 percent to develop the skills of its health staff to analyze and address service utilizationissues, in addition to technical quality problems.
3.32 Although training expenditures would be focused on QA methodologies,these funds would be used, selectively, to develop programs with clearly defined goalsexpressed in terms of objectively measurable competencies and aimed at addressing staffdeficiencies in technical skills and knowledge that have been demonstrated to hamper theability of district and frontline health staff to provide effective care. With technicalassistance from Pusdiklat (the national center for health in-service training), Sumbar alsoplans to use HP IV funds to try out and evaluate innovative approaches such as distancelearning and on-the-job training to meet the learning needs of health staff. The cost-effectiveness of providing incentives based on measured skills and knowledge acquiredthrough training or self-learning would be examined and successful innovations would beexpanded in future years. (Sumbar's training strategy illustrates the approach that the otherprovinces also intend to take to support HP IV's learning requirements.)
C. PROJECT MANAGEMENT AND IMPLEMENTATION
3.33 Project management. The Ministry of Health would be the executingagency with the Secretary-General as Project Director (Annex 12). He would beresponsible for the overall direction of the project and for making decisions on policyissues involving the project. He would appoint a Project Officer (the Head of the Bureauof Planning, MOH) who with the assistance of a Deputy Project Officer would manage theproject and would be responsible for all technical and administrative aspects of the project.

- 26 -
A Project Secretariat with several full-time staff headed by an Executive Secretary wouldmanage routine administrative matters. Many HP IV innovations deal with issues outsidethe purview of the Secretary-General and most of them are the responsibility of theDirector-General for Community Health (DG-CH). Consequently, to ensure smoothcoordination and timely implementation of HP IV activities, a Central Technical TaskForce under the leadership of the DG-CH would be established to review and guide keytechnical and policy innovations involving the aforementioned issues.
3.34 At the provincial level, the Chief of the MOH Provincial Health Office(Kanwil) would be the Provincial Project Officer. He would be ultimately responsible forall project-related activities in the province. He would be assisted by an AdministrativeOfficer (the Head of the Provincial Health Office Planning Division) who would be incharge of project administration, specifically reporting, planning, coordination, andmonitoring of project activities. A small full-time staff would be assigned to theAdministrative Officer to assist him in carrying out his project responsibilities. As regardsactivities under Dinkes I (the Provincial Health Services), its head would be the ProjectImplementation Officer. Moreover, a Provincial Technical Task Force, chaired by theProvincial Project Officer, with the Head of the Division of Health Services in theProvincial Health Office (Kanwil) as first secretary, would be established to monitor andguide all technical innovations involved in HP IV with the help of some consultants.
3.35 The center of gravity of HP IV activities would be at the district level andbelow. The Head of the District Health Office (Dokabu) with the help of a DistrictImplementation Officer would be in charge of all HP IV activities at this level and wouldreport directly to the Provincial Project Officer. The Dokabu's responsibility includesplanning and implementation of project activities. He would also be in charge ofproposing, testing and evaluating district innovations. A District Health DevelopmentCommittee, an intersectoral team with active participation from the Bupati (Head ofDistrict Administration) and the head of the district development planning agency(BAPPEDA II), would be established to guide the overall development of health within thedistrict. Finally, the Head of the Health Center would manage HP IV activities undertakenat the facility and would be accountable to the Dokabu.
3.36 During the course of the project, efforts would be made to developmechanisms to promote active community involvement in health services, with theobjective of making health providers more accountable to the community they are serving.To this end, local government representatives and non-governmental community leaderswould be mobilized.
3.37 Channeling of funds. Loan funds would be channeled through the DIP.Specifically, these funds would be channeled through the Integrated DIP (locally referredto as DIP Terpadu), with the exception of funds to support activities under the Centralunits. The choice of the Integrated DIP, which is a HP III innovation for integrating anddecentralizing GOI funding of basic health services, is based on its workability. Incontrast to the usual DIP, which rigidly earmarks funds for specific activities, theIntegrated DIP is less complex and allows the health district to reallocate resources acrossprograms as it sees fit. In this regard, the Dokabu would have the authority to disburse

- 27 -
funds and the responsibility for their accounting. The translation of the HP IV COSTABallocations into GOI's budget is easier and their release to implementing units is faster.The initial experience of GOI and the Bank regarding the Integrated DIP has been positive.Some civil works, however, to be funded 100 percent by GOI would be financed throughINPRES.
3.38 Implementation schedule. The project would be implemented for a periodof five years starting effectively about September 1995. The number of districts and healthcenters that would be provided with special assistance funds (SAFs) and other HP IVassistance would be phased according to the schedule laid out in Annex 2. Poor areaswould be given priority for early coverage.
3.39 Implementation would begin in two starter districts per province (three forEast Java) during the first one and a half years of the project. By focusing initially on afew districts, the collaborating agencies would have the time to lay out a solid foundationfor accelerated project implementation in later years.
3.40 The first one and a half years would focus on: (i) provision of technicalassistance; (ii) finalizing the detailed design of QA, training and other components; (iii)putting in place supporting policy actions; (iv) conducting orientation workshops and socialmarketing key project messages; (v) establishing the necessary implementationarrangements, including the institution of the drugs (LPLPO) and equipment managementsystem and Integrated Planning and Budgeting; and (vi) development of the districtperformance evaluation and incentive system, as well as the redesign of MOH's healthsurvey (SKRT) and collection of baseline data.
D. MoNrroRING AND EVALUATION
3.41 Several indices of performance were agreed with GOI during negotiations.Of these, intensive project monitoring and evaluation will focus on the following corevariables, which are key, proximate determinants of health outcomes:
(a) Quality of care: This will be measured by the extent to which healthproviders and patients comply with recommended standards of care or casemanagement protocols (See Annex 14 for examples). Health interventionscan be thought of as a series of steps involving history taking,- physicalexamination, treatment, counseling and patient knowledge. Within each ofthis step are activities which if carried out correctly would maximize theprobability of safe and effective care. An observation form, which has beendeveloped and tested for quality assessment, has several items (about 40 to60) for each health intervention detailing the activities that should beperformed. The quality of care provided by a health staff will be measuredas the ratio of the number of recommended activities performed correctlyrelative to the total items in the observation form. Quality measurementwould be applied to vaccinations, ARI, antenatal care, diarrhea and otherhealth interventions included in HP IV's BHS list (Annex 13). Initially, a

- 28 -
simple average of the various compliance rates for all of the HP IV basichealth services would be used as a summary indicator of the quality of care.During the course of project implementation other aggregation schemes willbe tried and consumer satisfaction measures will be developed and factoredin. Quality of care indicators will be measured annually.
(b) Rate of adoption of QA processes. This indicator is intended to monitorthe extent to which health center staff and their supervisors know andpractice key quality assurance principles and processes. These are likely toinclude: clinical competency measures, number of staff trained in QA,knowledge of the standards of care, applications of QA techniques,problem-solving skills of staff, frequency of QA meetings, number ofprocess improvement teams. This indicator will be refined and tested duringthe first year of the project. The key challenge here that needs to beaddressed is measuring the effectiveness with which health facilities areapplying these QA processes. An approach that will be explored by theproject will be the use of an expert review panel to rate the effectiveness ofthe QA procedures and process being established in a small sample of healthfacilities.
(c) Basic health services utilization rate: This measure would consist ofcontact rate and visit rate. Contact rate is defined as the number of personsin contact with health facilities in the last month relative to the number ofpeople in the catchment area. Contact rate will be obtained throughSUSENAS and, if necessary, a specially designed survey. Visit rate isdefined as the total number of visits made to health facilities in the previousfour weeks relative to the total number of people in the catchment area.The BHS list contains at least ten classes of health interventions. Therefore,there will also be at least ten different BHS related utilization measures.Aggregating these into a single indicator is not straightforward, becausethey differ in relative importance. The project will formulate a scoringsystem for aggregating these various measures into a single indicator duringthe first year of project implementation. For practical reasons, emphasis willbe put on visit rate, using data from the facilities monitoring system whoseimprovement has already been started under the Third Health Project.
(d) Share of Central, provincial, and district health subsidies going to basichealth services and the poor. The percentage share of the consolidatedCentral, provincial, and district health subsidies would be monitoredannually. The share of these subsidies going to the poor would be measuredevery other year, starting in the first year.
3.42 To monitor equity improvements, the quality and utilization indicators wouldbe measured separately for the poor and better-off, using income/expenditure povertythresholds based on GOI's current estimate. The MOH Bureau of Planning would developa socioeconomic classification of households and communities to identify the poor,building on the government's IDT program.

- 29 -
3.43 During negotiations, indicative targets for the above core performanceindicators were agreed. Agreement was also reached as to the frequency with which theywould be monitored.
3.44 In addition, GOI gave assurances that it would: (i) not later thanMarch 31 in each year, starting March 31, 1997, furnish to the Bank evaluation reports,covering approximately a two-year evaluation period, of the health districts'perfornancein terms of agreed performance indicators; and (ii) thereafter, review with the Bank thereports and take all measures required to ensure imnprovements in the health districts'performance in terms of the agreed performance indicators, including, if necessary, thereduction of Special Assistance Funds to non-perfonning health districts.
3.45 Supervision and technical audit. Like other projects in Indonesia, Banksupervision (Annex 4) would be conducted twice a year. Midterm and final projectreviews would be undertaken, using local and international consultants as necessary.Assurances were given by GOI during negotations that it would submit the reports ofthe midterm review, acceptable to the Bank, not later than December 31, 1997, anddiscuss with the Bank the results of the review not later than February 28, 1998.
3.46 Supervision requirements would not be excessive. Supervision would needto focus on Kalbar and Sumbar, because East Java has many experienced local healthofficials and NTB and Kaltim (Third Health provinces) will have fewer activities. Theproject would also use simplified budgetary arrangements (the DIP Terpadu) andredesigned systems of ordering and managing drugs and health equipment. HP IIIintroduced these innovations in NTB and Kaltim and found them to be reliable andefficient.
3.47 Furthermore, the project by design has built-in mechanisms to ensuredevelopment effectiveness. These include: (i) the establishment of a quality assurancesystem, which would improve supervision effectiveness; (ii) the aforementionedperformance-linked incentive system, which would create incentives for districtmanagement (particularly, the Dokabu) to effectively supervise and guide health centersin the cost-effective use of their available resources; (iii) greater attention by the MOHInspectorate-General to the technical audit of HP IV implementation; (iv) theimplementation schedule has been worked out in a way that before coverage of activitiesis expanded significantly, most of the above arrangements would have already been put inplace; and (v) a team of local and international experts who would annually review (audit)HP IV implementation and recommend corrective actions. GOI has agreed that thistechnical audit would be funded by the project and that the selection of the externalauditors would be subject to Bank's agreement.
3.48 Bank supervision would include an annual meeting with all of the provincialdelegations at once to review expenditures, policy reform and work programs. Tofacilitate this review and ensure adequate involvement of the provinces, agreement hasbeen reached with GOI during negotiations that a joint consultative meeting among theBank and the central and provincial teams be held annually to provide a venue wherebykey achievements by the provinces would be recognized, lessons learned would be shared,

- 30 -
and suggestions for corrective and other future actions discussed. The terms of referencefor this meeting was agreed during negotiations.
E. TECHNICAL ASSISTANCE
3.49 Provision for technical assistance (Annex 1) is crucial for the success of HPIV. It is needed to develop and institutionalize the various innovations to be introducedby the project. Hence, local and international consultants would be hired to assist bothCentral and local implementation units.
3.50 The cost of this technical assistance (TA) is moderate at about US$8.5million equivalent or less, which is about 6 percent of total project cost. Expenditures forconsultants are estimated to be less than 10 percent of Bank loan. Internationalconsultants, which were limited to what is critically needed, would be contracted for about148 person months (about a quarter of total consultancy). They would be deployed mostlyduring the first half of the project period and would be geared towards creating localcapacity by teaming them up with domestic consultants and dedicated key MOH staff.
3.51 In general, consultants, both local and international, would help MOH to:(i) formulate suitable standards of care (BHS case management protocols) and establishquality assurance programs based on international and Indonesian experience; (ii) developthe capacity of Pusdiklat and Bapelkes to provide supporting QA training programs andinstructional materials based on distance learning and on-the-job training approaches; (iii)redesign and test performance assessment and staff incentives systems; (iv) develop andtest capitation-based prepaid health benefit plans using private providers of care; (v) reformthe drugs and equipment inventory and management systems; and (vi) design anappropriate framework for pricing health services of government facilities and targetinghealth subsidies to BHS and the poor.

- 31 -
CHAPTER 4PROJECT COSTS AND FINANCING
A. COSTS
4.1 The total cost of the project is estimated at US$134.3 million equivalent(Rp 294.4 billion), including contingencies and identifiable taxes and duties. Tables 4.1 and4.2 summarize the estimated costs by province and by project component and category ofexpenditure, respectively. Detailed project costs by year, purpose and components are givenin Annex 6.
4.2 Bases of Cost Estimates. Baseline costs are estimated at March 1995 prices.Civil works costs are based on average square meter construction costs in the project provincesfor government buildings. The cost of land is not included in the above costs. Furniture costsare based on lists of standard locally available items. Medical and office equipment, andvehicle costs are based on current prices for similar imported or locally available items. Costsfor international and domestic consultants are in line with recent health projects forappropriately qualified experts. Unit cost for domestic fellowships is about US$5,000 per staff-year for long-term programs, and US$500 to US$1,000 per month for short-term programs.Overseas training and fellowships range from US$5,000 per staff-month for short-term trainingto US$25,000 per staff-year for long term programs. Operational costs are consistent withcurrent government practices and recent health projects. Costs for short-term, in-countrytraining costs vary widely depending on the type of training being given and its location, andaverage between US$25-45 per training day. Amounts for special assistance and programdevelopment expenditures, and project management costs have been agreed between the Bankand the Planning Bureau of the Ministry of Health. Drug costs are based on INPRES priceschedules. Recurrent costs are based on standard government allowances for travel, per diem,O&M, and consumable materials.
4.3 Contingency Allowances. Physical contingencies (US$5.7 million) represent5 percent and price contingencies (US$13.8 million) 12 percent of baseline costs. Physicalcontingencies of 5 percent have been allowed for all categories, as actual expenditures for allproject components are expected to differ from current estimates, given HP IV's programmaticapproach. Price contingencies have been calculated at 5.0 percent per year for local costs and2.2 percent per year for foreign costs.
4.4 Foreign Exchange Costs. Foreign exchange costs are estimated at US$40.4million (representing about 30 percent of total project costs) based on the following percentages:(a) overseas fellowships and vehicles - 90 percent, (b) equipment and international consultants -80 percent, (c) drugs included in recurrent costs - 50 percent, (d) civil works and furniture -
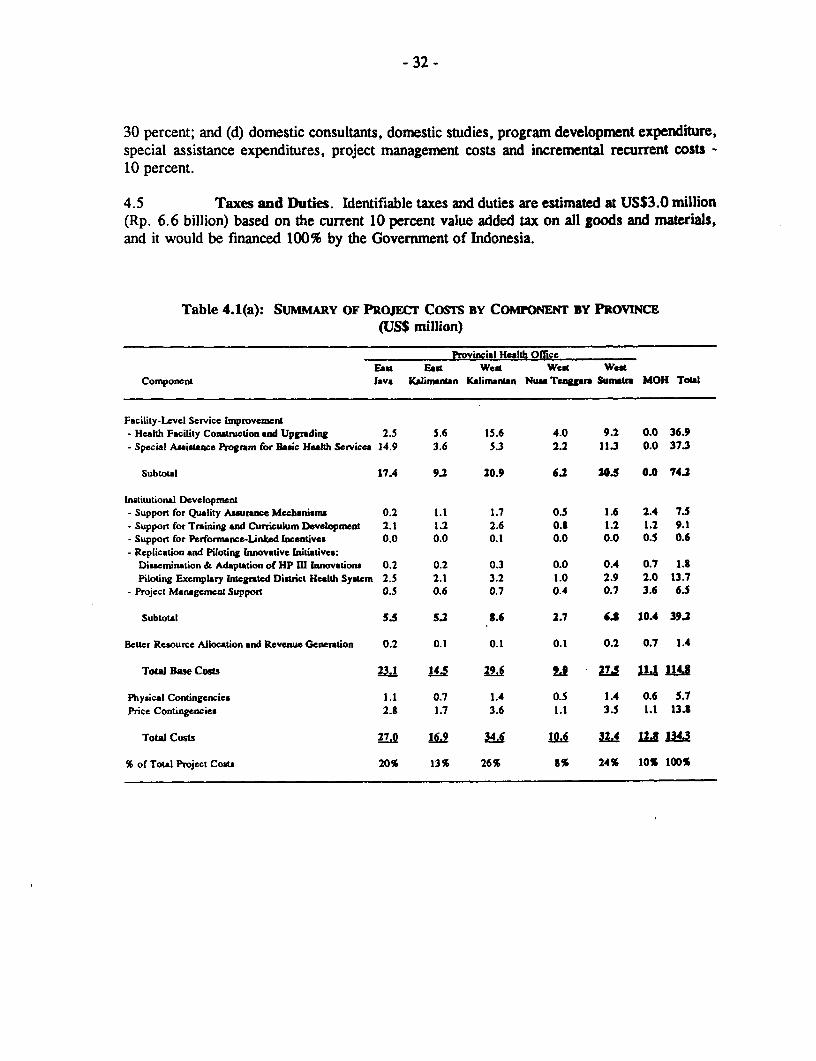
- 32 -
30 percent; and (d) domestic consultants, domestic studies, program development expenditure,special assistance expenditures, project management costs and incremental recurrent costs -10 percent.
4.5 Taxes and Duties. Identifiable taxes and duties are estimated at US$3.0 million(Rp. 6.6 billion) based on the current 10 percent value added tax on all goods and materials,and it would be financed 100% by the Government of Indonesia.
Table 4.1(a): SUMMARY OF PROJECr COSTS BY COMPONENT BY PROVINCE
(US$ million)
Provincil Health OfLeeEast East West Wtd West
Component Java KClinantan KaliranLan Nun Tenggara Sumatra M{OH Total
Facility-Level Service Improvenent- Health Facility Construction and Upgrading 2.5 5.6 15.6 4.0 9.2 0.0 36.9- Special Assistace Program for Basic Health Services 14.9 3.6 S.3 2.2 11.3 0.0 37.3
Subtotal 17.4 9.2 20.9 6.2 20.5 0.0 74.2
Institutional DevelopmentSupport for Quality Assurnee Mechanisms 0.2 1.1 1.7 0.5 1.6 2.4 7.5
- Support for Training and Curriculum Development 2.1 1.2 2.6 0.S 1.2 1.2 9.1Support for Perfonnance-Linked Incentives 0.0 0.0 0.1 0.0 0.0 0.5 0.6
- Replication and Piloting Innovative Initiatives:Dissrnination & Adaptation of HP III Innovations 0.2 0.2 0.3 0.0 0.4 0.7 1.3Piloting Exenplary Integrated Dictrict Health System 2.5 2.1 3.2 1.0 2.9 2.0 13.7
- Project Management Support 0.5 0.6 0.7 0.4 0.7 3.6 6.5
Subtotal 5.5 5.2 3.6 2.7 6.8 10.4 39.2
Better Resource Allocation and Revenue Generation 0.2 0.1 0.1 0.1 0.2 0.7 1.4
Totl Base Coss 23.1 145 29 6 275 Ll 114.8
Physical Contingencies 1.1 0.7 1.4 0.5 1.4 0.6 S.7Price Contingencies 2.S 1.7 3.6 1.1 3.5 1.1 13.3
Total Costs 27.0 16.9 MA H 32.4 IL I
% of Total Project Coats 20% 13% 26% S% 24% 10% 100%

- 33 -
Table 4.1(b): SUMMARY OF PROJECr COSTS BY COMPONENT
%TotalRD BiDion USS Million %Foreign Base
Component Local Foreign Total Local Foreign Total Exchange Costs
FwAilty-Levd Service Improvement:- Heakh Facility Construction
and Upgrading 47.3 33.5 80.8 21.6 15.3 36.9 41 32- Special Assistance Program
for Baic Health Servies 60.5 21.3 81.8 27.5 9.8 37.3 26 32
Subtotal 107. 8 162.6 49.1 25.1 74 2 34 65
Istitutional Devlopment- Support for Quality Assuranee
Mechanisms 13.4 3.2 16.6 6.1 1.4 7.5 19 6- Support for Training and
Curriculum Development 7.9 12.1 20.0 3.6 5.5 9.1 60 8- Support for Performance-Linked
Incentives 1.0 0.4 1.4 0.4 0.2 0.6 33 1- Replication and Piloting
Innovative Initiatives:Dissemination and Adaptationof HP IIl Innovations 3.2 0.8 4.0 1.5 0.3 1.8 17 2
Piloting Exemplary IntegratedDistrict Health System 26.4 3.5 29.9 12.1 1.6 13.7 12 12
- Project Management Support 9.8 4.4 14.2 4.5 2.0 6.5 31 6
Subtotal 61.7 24A4 86 1 2.2 11.0 39.2 18 34
Better Resource Allocationand Revenue Generation 2.3 0.6 2.9 1. 0.3 1.4 21 1
Total Base Costs 171.9i8 251.6 78.4 &.4 114 8 32 100
Physical Contingencies 8.6 4.0 12.6 3.9 1.8 5.7 32 5Price Contingencies 25.5 4.7 30.2 11.6 2.2 13.8 16 12
Total Cost La 2 9 .5 2944 93 9 40 4 134 3 30 117
/' Includes identifiable taxes and duties estimated at USS3 .0 million equivalent.

- 34 -
Table 4.2(a): SUMMARY OF PROJECT COSTS BY CATEGORY OF EXPENDITURES BY PROVINCE(US$ million)
Provincial Health OfficeCategory of East East West West WestExpenditures Java Kalimanatan Kalimantan Nusa Tenggara Sumatr MOH Total
Civil Works 0.5 3.2 12.1 2.9 8.0 0.0 26.7Equipment and Fumiture 2.1 2.5 3.7 1.2 1.3 0.3 11.1Drugs 10.0 0.0 1.6 0.0 5.3 0.0 16.9Vehicles 0.1 0.0 0.0 0.0 0.0 0.0 0.1Consultant Services and Studies 0.1 0.1 0.4 0.3 0.5 4.3 5.7FeUowships 2.0 0.9 2.4 0.8 1.0 1.5 8.6Training and Workshops 0.5 0.3 0.3 0.2 0.8 1.1 3.2Program Development Expenditures 0.6 1.4 0.6 0.0 0.2 1.4 4.2Special Assistance Expenditures 5.2 3.3 5.8 2.5 6.7 0.0 23.5Program Management 0.5 0.6 0.7 0.4 0.7 1.5 4.4Incremental Recurrent Costs 1.5 2.2 2.0 0.7 3.0 1.0 10.4
Total Base Costs 23.1 14.5 29 6 2 27.5 11,1 114.8
Physical Contingencies 1.1 0.7 1.4 0.5 1.4 0.6 5.7Price Contingencies 2.8 1.7 3.6 1.1 3.5 1.1 13.8
Total Costs 27.0 1 1.0.6 324 12,8 134.3
% of Total Project Costs 20% 13% 26% 8% 24% 10% 100%
B. FiNANCING
4.6 The total project cost of US$134.3 million equivalent would be financed by aproposed loan of USUS$88.0 million equivalent, covering 67 percent of total project costsexcluding taxes (96 percent of foreign and 53 percent of local expenditures). The Governmentwould finance from its annual budget the remaining costs of US$46.3 million equivalent (33percent of the total project costs excluding taxes or 34 percent of total project costs includingtaxes).
4.7 Incremental Recurrent Costs. Incremental recurrent costs are additional costsassociated with the MOH and its PlUs. These account for 24 percent of total base costs. Allspecial assistance expenditures and project-related incremental recurrent costs would be financedon a declining basis in order to ensure sustainability.
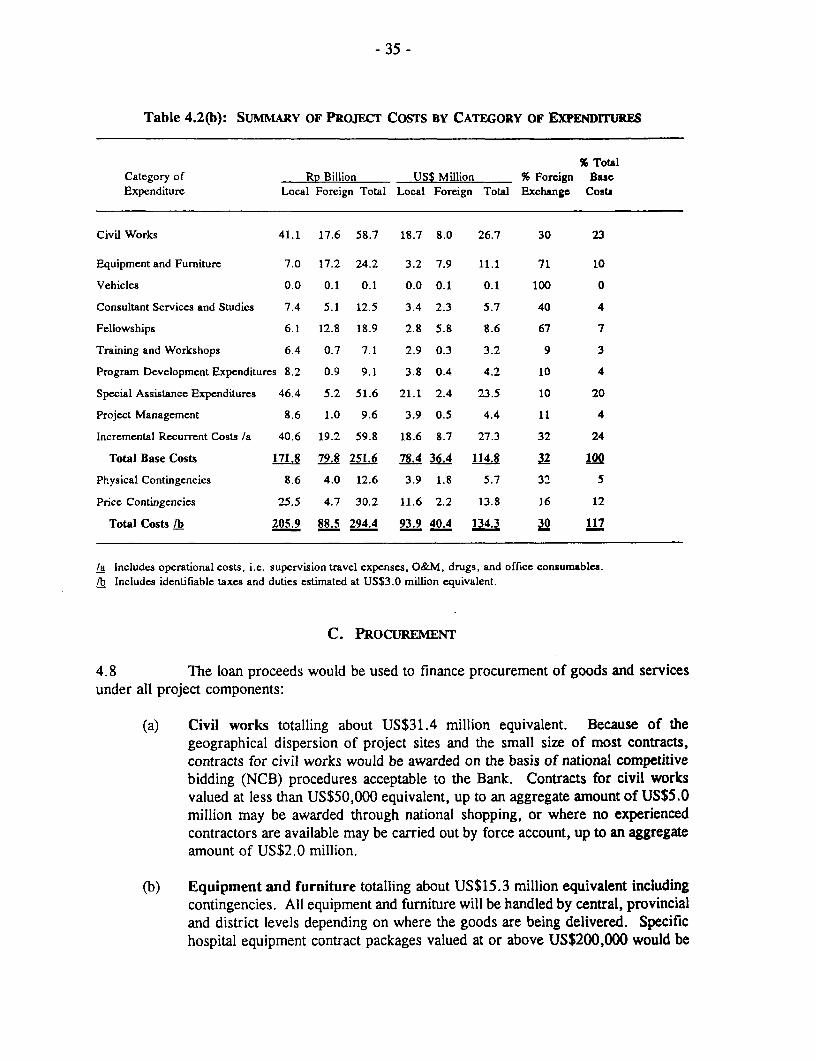
- 35 -
Table 4.2(b): SUMMARY OF PROJECT COSTS BY CATEGORY OF EXPENDITURES
% TotalCategory of Rp Billion USS Million % Foreign BaseExpenditure Local Foreign Total Local Foreign Total Exchange Costs
Civil Works 41.1 17.6 58.7 18.7 8.0 26.7 30 23
Equipment and Furniture 7.0 17.2 24.2 3.2 7.9 11.1 71 10
Vehicles 0.0 0.1 0.1 0.0 0.1 0.1 100 0
Consultant Services and Studies 7.4 5.1 12.5 3.4 2.3 5.7 40 4
FeUowships 6.1 12.8 18.9 2.8 5.8 8.6 67 7
Training and Workshops 6.4 0.7 7.1 2.9 0.3 3.2 9 3
Program Development Expcnditures 8.2 0.9 9.1 3.8 0.4 4.2 10 4
Special Assistance Expenditures 46.4 5.2 51.6 21.1 2.4 23.5 10 20
Project Management 8.6 1.0 9.6 3.9 0.5 4.4 11 4
Incremental Recurrent Costs /a 40.6 19.2 59.8 18.6 8.7 27.3 32 24
Total Base Costs 171.8 79.8 251.6 78.4 114.8 32 100
Physical Contingencies 8.6 4.0 12.6 3.9 1.8 5.7 32 5
Price Contingencies 25.5 4.7 30.2 11.6 2.2 13.8 16 12
Total Costs /b 205.9 88.5 294.4 93.9 40.4 134.3 30 117
/a Includes operational costs, i.e. supervision travel expenses, O&M, drugs, and office consumables./b Includes identifiable taxes and duties estimated at US$3.0 million equivalent.
C. PROCUREMENT
4.8 The loan proceeds would be used to finance procurement of goods and servicesunder all project components:
(a) Civil works totalling about US$31.4 million equivalent. Because of thegeographical dispersion of project sites and the small size of most contracts,contracts for civil works would be awarded on the basis of national competitivebidding (NCB) procedures acceptable to the Bank. Contracts for civil worksvalued at less than US$50,000 equivalent, up to an aggregate amount of US$5.0million may be awarded through national shopping, or where no experiencedcontractors are available may be carried out by force account, up to an aggregateamount of US$2.0 million.
(b) Equipment and furniture totalling about US$15.3 million equivalent includingcontingencies. All equipment and furniture will be handled by central, provincialand district levels depending on where the goods are being delivered. Specifichospital equipment contract packages valued at or above US$200,000 would be

- 36 -
Table 4.3: FINANCING PLAN
(US$ million)
Govermnent IBRDof Share
Indonesia IBRD Total (S)
Civil WorksINPRES-financed 7.8 0.0 7.8 0Others 2.0 20.3 22.3 911b
Equipment/Furniture 3.1 8.9 12.0 75Vehicles 0.1 0.0 0.1 0Consultant Services and Studies 0.0 6.1 6.1 100Fellowships
Domestic 2.6 0.0 2.6 0Overseas 0.0 6.6 6.6 100
Training and Workshops 0.0 3.6 3.6 100Program Development Expenditures 0.0 4.7 4.7 91/bSpecial Assistance Expenditures /a 14.1 13.1 27.2 48Project Management Costs 0.0 4.9 4.9 100Incremental Recurrent Costs /a 15.1 15.6 30.7 51Unallocated 1.5 4.2 5.7 74
Total 46.3 88.0 134.3 66
/a Declining absolute amount financing of 75%,75%,50%,50%,25% of five-year annual total expenditures.lb Excluding taxes.
awarded under international competitive bidding (ICB) procedures. Localmanufacturers would be granted a 15 percent of domestic margin of preference.Contract packages valued at less than US$200,000 and up to an aggregatedamount of US$5.4 million would be awarded through national competitivebidding (NCB) procedures acceptable to the Bank. Contract packages valued lessthan US$50,000 or equipment of a specialized nature for which NCB is notpractical, up to an aggregate limit of US$7.9 million including taxes, may bepurchased through international and national shopping on the basis of three pricequotations.
(c) Vehicle costs totalling about US$0.1 million equivalent. The Government ofIndonesia considers the procurement of vehicles as reserve procurement andtherefore Bank financing would not be used to purchase vehicles. Duringnegoiations, the Government gave assurances th it would provide therequired vehicles for the project in accordance with a schedule agreed with theBank.
(d) Consultant services and studies totalling about US$8.5 million equivalent,would be selected and contracted in accordance with Bank Guidelines.

- 37 -
(e) Overseas and domestic fellowships totalling about US$9.6 million equivalent.Placement of candidates in foreign and domestic institutions would be made onthe basis of the relevance and quality of the programs offered, costs, and priorexperience, according to government administrative procedures acceptable to theBank. Training contracts totalling about US$3.8 million equivalent would beawarded to local providers in accordance with Government administrativeprocedures acceptable to the Bank.
(f) Project management totalling about US$5.2 million equivalent. Projectmanagement expenses, including travel allowances, office costs, and otheroperational costs, meetings, and administrative support, would be spent followinggovernment administrative procedures acceptable to the Bank.
(g) Incremental recurrent costs totalling about US$60.4 million equivalent.Incremental recurrent costs including supervision travel expenses, operations andmaintenance, office consumables and eligible expenditures under the SAFoperating guidelines, would be spent following government administrativeprocedures acceptable to the Bank.
4.9 Procurement Review. Review by the Bank would be as follows:
(a) By loan effectiveness, the Bank will carry out a prior review of (i) standardbidding documents for civil works and goods contracts to be awarded under ICBand NCB procedures, and (ii) letters of invitation for consultant services, toascertain their conformity with the Bank guidelines. The approved documentswould be used as master documents for all future bidding;
(b) All civil works contracts valued at or over US$1,000,000, if any, and goodscontracts valued at or over US$200,000 would be subject to prior review by theBank, whereas all other contracts for civil works and goods would be subject torandom post-review. However, the first contract for civil works in eachprovince and the first contract for goods in each province estimated to cost theequivalent of $50,000 or more will be subject to prior review. Roughly 20% ofcivil works contracts, and 25% of goods contracts are likely to be covered byprior review. The largely successful province-level procurement experience inthe HP III Project suggests that these prior review percentages are sufficient. Inaddition, standard bidding documents will be used for both ICB and NCBprocedures, and regular random post review would be carried out by the residentmission and supervision missions;
(c) Consultant contracts valued at or over US$100,000 for firms and US$50,000 forindividual would be subject to prior review by the Bank. All other consultantcontracts would be subject to random post review. However, all consultants'terms of reference would be subject to prior review;
(d) Fellowships would be subject to random post-review by the Bank; and
(e) Annual training plans for each year would be included in the annual report fordiscussion with the Bank.

- 38 -
Table 4.4: PROCUREMENT ARRANGEMENTS
(US$ million)
ProcurementProcedures Total Cost
Category of Expenditure ICB NCB Other/a N.B.F. includingContingencies
Civil Works 24.4 7.0 31.4(16.8) (4.5) (21.3)
Equipment and Furniture 2.0 5.4 7.9 lb 15.3(1 .5) (4. 1) (5.9) (1 1.5)
Vehicles 0.1 0.1
Consultant Servicesand Studies /c 8.5 8.5
(8.5) (8.5)Fellowships
Domestic 2.7 2.7(0.0) (0.0)
Overseas 6.9 6.9(6.9) (6.9)
Training and Workshops 3.8 3.8(3.8) (3.8)
Project Management 5.2 5.2(5.2) (5.2)
Incremental Recurrent Costs /d 60.4 60.4(30.8) (30.8)
Total 2.0 29.8 102.4 0.1 134.3(1.5) (20.9) (65.6) (88.0)
Notes: Figures in parentheses are the respective amounts financed by the Bank.N.B.F - not Bank financed.
/a Includes direct contracting, force account, shopping, hiring of consultants, andadministrative expenditures.
/b Includes small equipment for the SAF and PDE programs.Ic Includes contract services for PDE programs./d Includes supervision travel expenses, O&M, drugs, office consumables and expenditures for
the SAF program.

- 39 -
D. DISBURSEMENT
4.10 The proposed loan of US$88.0 million equivalent would be disbursed over aperiod of about 5 years (Annex 8). The project is expected to be completed by September 30,2000, and the Loan would be closed six months later on March 31, 2001. The disbursementschedule is based on the implementation schedule and the disbursement profile for health projectin Indonesia. It is somewhat faster to reflect the establishment of the special account and thetimely implementation experience of HP IV Project team. Disbursements estimated for the firstsemester of FY96 are based on the proposed initial deposit into the project Special Account.Disbursements would be made as follows:
(a) civil works US$20,300,000 91 % of total expenditures(non-INPRES financed)
(b) equipment and furniture US$ 8,900,000 100% offoreignexpenditures(excluding vehicles) 100% of local expenditures
(ex-factory cost)65 % of local expenditures forother items procured locally
(c) consultant services and US$ 6,100,000 100% of total expendituresstudies
(d) overseas fellowships US$ 6,600,000 100% of total expenditures
(e) training and workshops US$ 3,600,000 100% of total expenditures
(f) program development US$ 4,700,000 91 % of total expendituresexpenditures /a
(g) special assistance 100% incurred in:expenditures /b US$ 3,000,000 FY1995/96 and FY1996/97
US$ 6,500,000 FY1997/98 and FY1998/99US$ 3,600,000 FY1999/2000 and thereafter
(h) project management support US$ 4,900,000 100% of total expenditures
(i) incremental operating costs 100% incurred in:US$ 4,500,000 FY1995/1996 and FY1996/97US$ 7,600,000 FY 1997/1998 and FY1998/99US$ 3,500,000 FY 1999/2000 and thereafter
(j) unallocated US$ 4,200,000
/a See eligible expenditures of PDE in Annex II./b See eligible expenditures of SAF in Annex 10.
- 40 -
4.11 Disbursements from the Loan for the following contracts would be made againstfull documentation: (a) civil works contracts valued at or more than US$1,000,000; (b) goodscontracts valued at or more than US$200,000; and (c) consultant services contracts withindividual consultants valued at or more than US$50,000 and consulting firm contracts valuedat or more than US$100,000. All other disbursements would be made against statements ofexpenditures (SOE) for which relevant documents would be retained by responsible agenciesand made available for review as requested by visiting Bank missions. To facilitatedisbursements, a Special Account in an amount of US$4.0 million would be established at BankIndonesia. This Special Account would be held in the name of Directorate General of Budget,Ministry of Finance, following established procedures. The Special Account would be used forall eligible foreign and local expenditures. Replenishment to the Special Account would bemade on a monthly basis or when 20 percent of the initial deposit has been used, whicheveroccurs first.
E. ACCOuNTS, AuDrrs AND REPORTS
4.12 MOH would establish project accounts for all project expenditures at both theprovincial and central levels, to be maintained in accordance with sound accounting practices.Accounts for the SOEs and Special Account would be maintained separately for annual audits.Each provincial PIU would send financial statements for all project expenditures for each fiscalyear to the Project Secretariat. The Project Secretariat would consolidate the five provincialfinancial statements with the central level financial statement and prepare a consolidatedfinancial report. The financial statements and consolidated financial reports would be auditedby independent auditors acceptable to the Bank, including a separate audit opinion on SOEexpenditures. Certified copies of the financial report on the project for each Government fiscalyear, together with the auditors' statements, would be furnished to the Bank as soon asavailable, but not later than six months after the end of each government fiscal year startingJune 30, 1996. MOH would also monitor progress in project implementation and report to theBank each semester on this progress. Within six months after the completion of disbursement,the Ministry would submit an implementation completion report (ICR) to the Bank.
4.13 Technical Audits. MOH has the primary responsibility to monitor all projectactivities and routine monitoring would be added through annual reviews. However, given alarge number of contracts that will be financed under SOE procedures implemented by eachproject management level, an independent, qualified firm with external technical assistancewould be hired to conduct technical audits of key project activities. These includeimplementation of QA, SAF, PDE, health finance and management reforms, and trainingprograms. The above audits would cover activities in progress and post review of completedactions to examine whether from the substantive, technical standpoint implementation of thevarious project components are appropriate and to recommend corrective measures, ifnecessary. These audits would be conducted annually on a random sample basis. Duringnegotiations, the Government provided assurances that it would cause technical audits to becarried out, in a manner acceptable to the Bank, by April I in each year during theirnplementation of the project and furnish a copy of such audit to the Bank for comments,by July 31 of each such year.

- 41 -
CHAPTER 5BENEFITS AND RISKS
A. BENEFTS
5.1 By empowering provincial, district and facility authorities and therebyimproving the delivery and quality of basic health services, the project would increase thenumber of people utilizing them and benefitting from their use. Consequently, mortalityand suffering from pain and disability due to illness could be reduced significantly. Thepoor particularly would gain from the project, as one of the worst aspects ofpoverty-premature death, disability and debility from illness-would be considerablyalleviated by the project's emphasis on the extension of cost-effective packages of goodquality basic health services to the poor.
5.2 The expected health service improvements would benefit a wide range ofpotential clients. The major beneficiaries, however, are expected to be women andchildren from both poor and well-off families. At present, maternal, infant and childhooddiseases are major causes of mortality and morbidity. It is precisely these diseases thatmost of the health interventions supported by the project are directed against (e.g.,immunization, ante-natal care, treatment of diarrhoea, health education, de-worming andprovision of selected micronutrients).
5.3 The total population that could benefit from the project is estimated to beabout 27 million. This is the number of persons covered by the 886 health centersincluded in HP IV. Of the 27 million potential beneficiaries, about 20 percent are poorand another 13 percent are near-poor. In the long-term, the benefits from HP IV wouldlikely go well beyond these districts. As the project proves to be successful, its initiativeswould most likely be adopted by other provinces. The experience of Third Health in thisrespect is very encouraging. Innovations that moved successfully under that project thenbecame part of GOI's national policy.
B. RISKS
5.4 Health Finance. A major step towards increasing resources for BHS andreorienting government health spending towards the poor is to raise the prices of healthservices provided by public facilities, while protecting the poor from their impact. Theproblem is that it is difficult to predict the pace and extent of price reforms that could beaccomplished under HP IV. Raising prices of government health services is politicallysensitive and some local governments, which are responsible for the prices of publicly

- 42 -
managed health services, may be reluctant to make substantial price increases. Therefore,increasing cost-recovery rates to appropriate levels might be delayed or could becomeimpossible in some districts.
5.5 Despite this risk, the chances that targeted cost-recovery rates will beincreased significantly as a result of the project remain good, primarily because of GOI'sstrong commitment. Both the Ministry of Health and BAPPENAS have been involved informulating this policy and has actively campaigned for the support of provincial anddistrict officials from the outset of project preparation. The results of this effort, whichreinforced provincial and district support for price reform, are reassuring. For example,the Bupati of the starter districts have already submitted to the Bank signed decreesaddressed to local staff supporting price adjustments. Another encouraging factor is thatthe Third Health experience showing the feasibility and beneficial effects of price increaseshas proven to be an effective material for promoting price reforms. This experiencetogether with the recent introduction of health cards exempting the poor from paying feesfor government health services provides HP IV an effective tool for assuaging concernsabout the impact of fee increases. Finally, sufficient funds have been allocated inprovincial and central government expenditure programs to support activities promotingcost recovery and appropriate targeting of health subsidies.
5.6 Training. There is a large but manageable training challenge involved intransferring skills and information needed for a QA program. As currently practiced,training has several features that are counter-productive. Absences of staff from work dueto training overload are becoming a problem. Staff have a perverse incentive to participatein unnecessary training to augment their incomes through training-related honoraria andper diems. Promotion credits are also awarded on the basis of simple attendance. Theactual acquisition of competencies is rarely measured and recorded.
5.7 The risk that off-the-job training activities could become excessive,disrupting the provision of services in the health centers, was highlighted during appraisaland was well-appreciated by concerned GOI officials. Consequently, GOI intends to usethe project to develop and assess alternatives to off-the-job training such as distancelearning and other on-the-job training approaches. The project will also test direct, skill-based incentives that have proved feasible in other settings. The credit points system forpromotion, which rewards mere attendance in training events, would also be reviewed andrevised to take into account actual competencies learned. Furthernore, assurances wereprovided during negotiations by GOI that it would: (a) not later than January 31, 1996,furnish to the Bank a proposal for a scheduling and management mechanism for thetraining of staff which minimizes disruption in the facilities' activities and whichensures: (i) that training courses under the project address documented skills deficitscritical to BHS improvement and have defined and measurable outcomes; and (ii) thattraining courses are evaluated on the basis of the trainees' measurable acquisition ofrelevant gains in skills and knowledge; and (b) before implementing the training, havethe relevant course materials available for the trainees.

- 43 -
C. SUSrAINABxLrrY
5.8 Prospects for project sustainability are very good. Indonesia's outlook foreconomic growth is bright, and the cost of the project's various initiatives is modest andaffordable. Moreover, there is a strong sense of project ownership and a firm commitmentby participating provincial governments and GOI to carry on successful HP IV initiativeswith local funds and retained earnings of health facilities. Furthermore, as the projecteases current concerns about the public health sector's inability to efficiently absorbadditional funds, resistance to budgetary increases for basic health services could bereduced considerably. Finally, through its promotion of higher cost recovery, greaterretention of revenues earned by public health facilities, as well as intensified mobilizationof private resources (e.g., health insurance), the project is expected to facilitate budgetaryreallocations that would increase health subsidies to basic health services and povertyalleviation.
D. ENVIRoNMENTAL IMACT
5.9 The project does not pose any significant environmental threat. Thepossibility of hospital wastes impacting on the environment is unlikely to be significant,since there will be no major hospital construction under HP IV. On the contrary, HP IVcould contribute to the quality of the environment to the extent that the project strengthensthe ability of health centers to deal with communicable diseases and pathogens in theenvironment.

-44 -
CHAPTER 6AGREEMENTS REACHED AND RECOMMENDATION
6.1 During negotiations, the Government of Indonesia gave the followingassurances that it would:
(a) not later than December 31, 1995, furnish to the Bank a classification, onthe basis of poverty issues, of health centers and health districts in theproject provinces (para. 3.19);
(b) not later than October 31, 1996, furnish to the Bank guidelines for pricingpersonal health services provided by health centers and hospitals andprotecting the poor from the impact of price adjustments (para. 3.19);
(c) not later than October 31, 1996, implement the system for the annualcollection of consolidated budgetary information to monitor achievement ofthe targets referred to in paragraph 3.18(a) and for assessing the impact ofproposed central and provincial budgetary allocations on the funding of BHS(para. 3.19);
(d) cause the local governments of the participating provinces to take all actionsrequired for the implementation of the Provincial Statement in each districtselected to participate in the project, including the requirement:
(i) that the share of district health budget going to BHS and the poor beincreased annually;
(ii) that health service fees be adjusted upwards and that such revenuesbe used for purposes of the heaith sector; and
(iii) that part of the earnings of the health centers be used by suchfacilities for health center performance incentives (para. 3.20).
(e) not later than January 31, 1996, furnish to the Bank a proposal for ascheduling and management mechanism for the training of staff whichminimizes disruption in the health facilities' activities and which ensures:(i) that training courses under the project address documented skills deficitscritical to BHS improvement and have defined and measurable outcomes;and (ii) that training courses are evaluated on the basis of the trainees'measurable acquisition of relevant gains in skills and knowledge (para. 5.7);

- 45 -
(f) before implementing the training, have the relevant course materialsavailable for the trainees (para. 5.7);
(g) (i) not later than March 31 in each year commencing on March 31, 1997,furnish to the Bank evaluation reports, covering approximately a two-yearevaluation period, of the health districts' performance in terms of agreedperformance indicators; and (ii) thereafter, review with the Bank the reportsand take all measures required to ensure improvements in the healthdistricts' performance in terms of the agreed performance indicators,including, if necessary, the reduction of Special Assistance Funds to non-performing health districts (para. 3.44);
(h) undertake midterm and final project reviews, acceptable to the Bank, andsubmit copies of reports of the midterm review not later than December 31,1997, and discuss with the Bank the results of the review not later thanFebruary 28, 1998;
(i) cause technical audits of project implementation to be carried out, in amanner acceptable to the Bank, by April 1 in each year during theimplementation of the project; and furnish a copy of such audit to the Bankfor comments, by July 31 of each such year (para.4.13); and
(j) provide the required vehicles for the project in accordance with a scheduleagreed with the Bank (para. 4.8(c)).
(k) carry out the activities under the Special Assistance Fund (SAF) inaccordance with the SAF Operating Guidelines, agreed with the Bank (para.3.11);
(1) carry out the Programn Development activities in accordance with theProgram Development Expenditures Operating Guidelines, agreed with theBank (para. 3.13).
6.2 Subject to the above agreements, the proposed project is suitable for aBank loan of US$88.0 million equivalent to the Republic of Indonesia for a term of 20years, including a grace period of five years, at the Bank's standard variable interestrate.

- 46 -
ANNEX 1. INTERNATIONAL AND NATIONAL CONSULTANT REQUIREMENTS

INDONESIA
FOURITh IIEALTIll PRIOJECT:IMPROVING EQUITY AND QUALITY OF CARE
Tecluiical Assistance Table
Number MonthsTA Activity Purpose/Objectivc Supervisor/lmplcmcnting Forcign Domestic Foreign Domestic Estimated Cost
Agency (Rp/000)
A. Implementation Support1. Local project managemcnl Management support to Chiic/MOI I Planning Bureau 1 60 500,000.00
consultant project secretariat
B. Institutional Capacitv BuildingI. Project Tccluhical Advisor Assist in maniagement of lI' Chief/MOI-l Plauuning Bureau 1 60 1,500,000.00
IV teclhnical activities2. QA Consultanits
(a) CenLral QA int'l expert QA program development Chicf/MOH Planning Bureau 1 24 600,000.00(b) Central natl QA consultant QA program dev. and Chief/MOl Planning Bureau 2 120 1,000,000.00
instituitionalization support(c) IPrivate sector QA consultant QA assistance to private 1 15 125,000.00
sector3. P rovincial Advisors
(a) bit'l QA experts Support development of QA llead/Kanwil 2 20 500,000.00programn in the I -ovinces
(b) Local QA consultarits 4 96 888 000.00(c) Health educationi expert Develop healii education 1 12 102,000.00
program for BI3S(d) I Icalth planniing expert Assist with needs assessmin.t 1 12 300,000.00
anid development ofprovincial hcalthi sector plan
4. T'raining Consultants Prepare training curriculum Director/Pusdiklat 2 14 350,000.00and materials on QAprinciples, metiods andpractices; develop teachingmodules, distance learningand other innuovative training ) ;approaches o -

! !o!1!iMCC 1I, Ci1t1vS NxI)et 1 I)cvCH Develop and lest (hicilI NIanpo\cr litczin i 6 15(,(00.00pIdInL) III;IIc i111C'11t11%C- !,I
lrotliii:e iiocitcrs
t) Di)ngs Managemient Consultiants (a) Assist expansion ol the ChietIl)rugs Cotirol ltireau 2 60 420,000.00drugs management and
logistics rcforms. (b) developa program to improveprescription and self-medication practices
7. Computer Consultant Preparc computerized drugs Chief/Drugs Control Burcau 1 5 40,000.00_managemeint systems ___
8. Irepaid Health Carc Experts Develop managed prepaidcarc schemes I
(a) Int'l managed care expert Director/Cotmnunity . 12 300,000.00I'articipation Directorate _ _
(b) Local health insurance 2 48 384,000.00consultants
9. 1 luman Resoturce (1 II) PlanningConsut;ltants(a) HR Infonnation Specialist Develop computerized ChiieUMOH Manpower Bureau 1 12 100,000.00
information system for 81R 1Management ___
(b) HR Development Consultant Develop HR planning and 1 6 35,000.00__managemiienit program
C. Policv Advice/Studics
(a) Economic/flinanicial Analyst Prepare analysis of 131 IS Clhi cI0l I Finance 13Bureau 1 40 300,000.00ex\pnditures and program
for reveritie generation; |establish s%stein for arnutialcollection of consolidatedbudgetary data and impactanalysis of budgetary
decisions on 131 IS funding.D. TOTAL 9 17 148 474 7,594,000.00
w

Status of TOR Short List
TA Activity Prepared Expected Prepared Expected
A. Implenmentation Support 4/01/95 3ly eilectiveness
I Local project mnanagemeitconsultant
B. Institutional Capacity By elTcctiveness
Building1. Project Technical Advisor 2/24/95 _-
2. QA Consultants(a) Central QA intll expert 2m795(b) Central nat'i QA consultant 2/27/95(c) Private sector QA consultant 3/13/95
3. Provincial Advisors(a) Ilt'I QA experts(b) Local QA consultants(c) I lealti education expert(d) lIcalth planning expert 2m95
4. Training Consultants 3/13/95 _ _
5. Performance Incentives Expert 27g/5 6. Drugs Management Consultants 2/7957. Computer Consultant8. Prepaid Health Care Experts
(a) hit'l managed care expert 2/27/95(b) Local health insturaice 2/27/95
consultants . .
9. Human Resource (HR) PlanningConsultants . _.-
(a) HR hiformationl Specialist 2n/95(b) HR Development Consultant 2/795
C. Policy Advice/Studies 8/1/95 B effectiveness
(a) Econonmic/Financial Analyst __
c,J3

- 50 -
ANNEX 2. IMPLEMENTATION SCHEDULE

Annex 2Page 1 of 10
- 51 -
C.' 1,
a
a.-0 U X - I t0
|1;~~~~~ ~~~ 7- ----------.-.--. 1. . ............................... C0el s!- 1 1 12 1 1 1 1- 1^ lo 1= 1 1 t1 1 1 1 Io lo A 1 *
Cy~~~~~~~~~~~~~~~~~~~~~~~~~C
a~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ L
I ______~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~E
. . ....................... .............. .... ....... H
ci~~~~~~~~~~~u u~~~~~1*LU~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~L<~~~~~ -u~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~a
'C I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I
pi~~~ z

* mm -_ _ n _ S m m _ _
acm~~~~~~~~~~~~~~~~~~r
Gi 11 Wg S I :! e iI -1|t
:~~ ~ IZ 0 __:
-
flfl-4
z4 a0
r r Uv 0C a:
Hi~~~~~~~~~~~~~~~~~~~~~~~~~~~~II~~~~~~~~~~~~~~~~~I512:0 0 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
01 Jo a,o 0 Z9 Z X.Iu
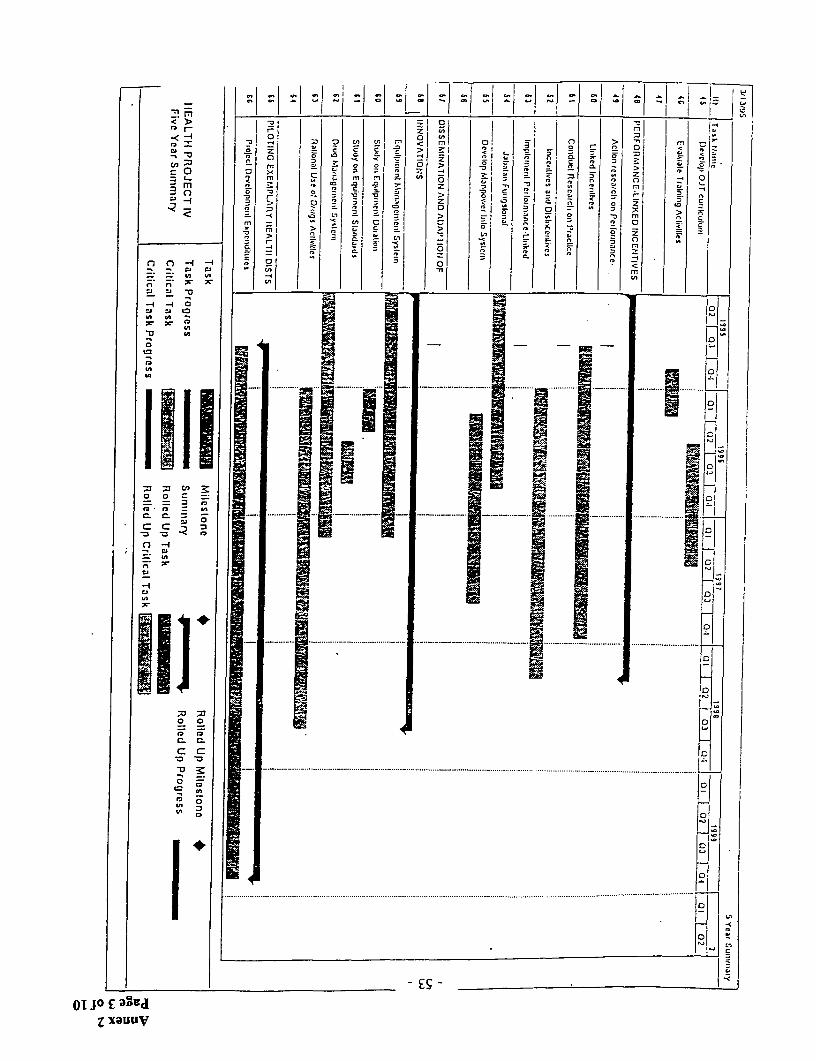
< >~~~~~~~~~~~~~~~~~~~~~~
m
-2 0: = -
zo L~~~~~0 l
C C ~ ~ ~ ~~ ,
Ci~~~~~~~~~~~~~~~~~~~~ l
- ;-4-a II
I n
ol Jo E a a rZ a a

Lrn I);<R
0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
C) 0-4 -~ ~ ~~- -, r.t ~~~~~~~~~~~~~~~~~~~~~
~~. ;; ~~~~~~- ~~~~-
0o -~~~~~~~~~~~~~~~~~~~~
ii~~~~~~~~~~~~~~~~F ;o 0U =n3
= = 9o7 ii
0~~~~~~~~~~~~~~~~~~~~~~~~
C.C.
ID Lii~~.. ........................... .... ........... .... ......... ...................
0
0O JO t7 33ydZ xauuv
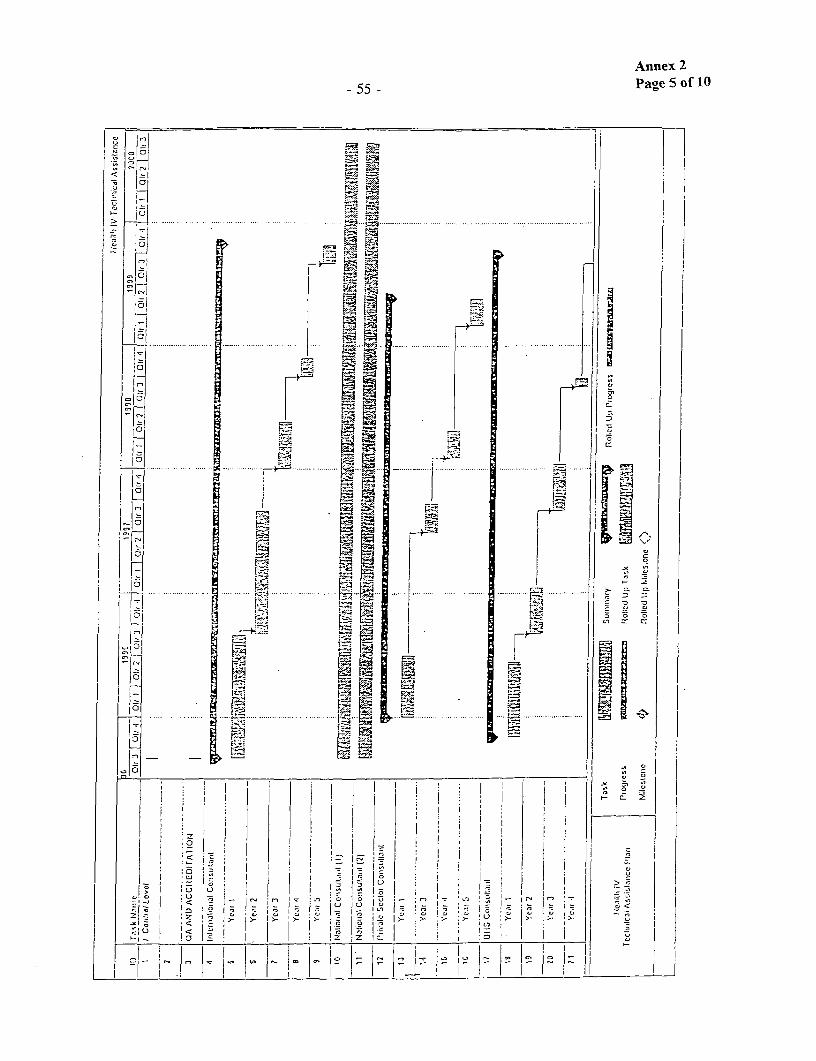
Annex 2
55 Page 5 of 10
_~~~~~~~~~~~~~~~~~~~~~~~~~~ ..... ...... _
0;~~~~~~~~~~~~~~~~~
* X * n C - ] f n | : i ; F
0.~~~~~~~m
0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
4 I)
10 -
4~~~~~~2J~

Annex 2
-56 - Page 6 of 10
: ' .~~~~~~~~~~~~~~~~~~~~~~~~~~~~.......{
~ =m -It.- C
alO~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~L
LiS l ~......:
|' 7 a, > ; >- Xr i >' >' >' $ > 5 i
L~~~~~~~~~~~~~~~~~~~~~~~~~~~~S
21 ~~Z I I J;Z I ;zI
1~~~I
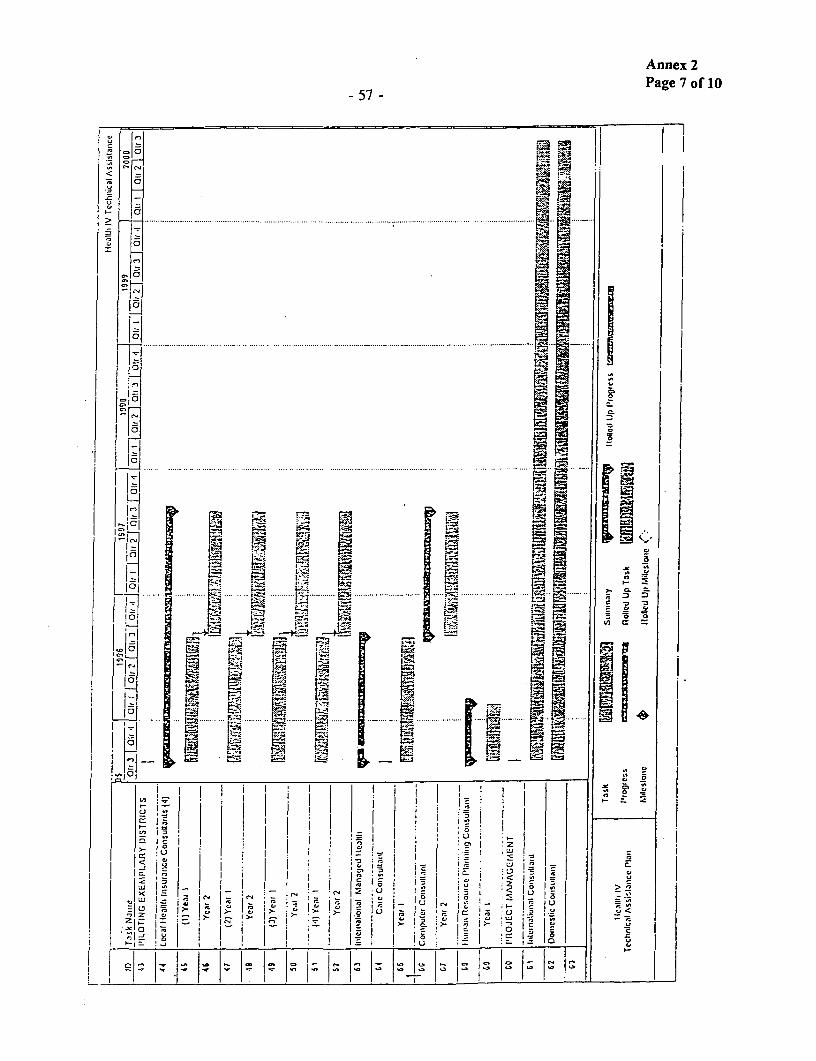
Annex 2Page 7 flO
0 ' I0I
1 0 ....... ... ..... . . . ............ ._. . [e .. .
C . - - * - -_ _ C _ S _ - _ - , S
...... .... ... ... .. -.
Li~hLIi
iI~~~~~~~~~~~~~~~~~~~~~~~~~I ~~~~ ~ ~ L
ul~~~~~~~~~~~~m
I . .'

Annex 2
- 58 - Page of 10
o I~~~I:X1 r ,oP
0 ..... .. .. ..... .. ... ... ....
. ... .... ....+
1 -
a - ~~~~~~~~~~~~~~~~~~~~~~~~~~~0
I -1t~ Is .0 l
C3~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
0I~
Liu -I u

;~ ~ ~ ~~ ~ ~~~~~ .. ........... ... . ....... .. , - I t
i 1-'s '' '''''''''''...... " ........ . ' ' ' ' ' ' .. ..'.''.' . ......... .... ....
Of JO 6 ;!u 6.l *1'
z xauuv

Annex 2
-60 - Page 10 of 10
2 .......... ...... 1...
101 1
*:~~~~~~~~.... .. 3'
10- 0 0
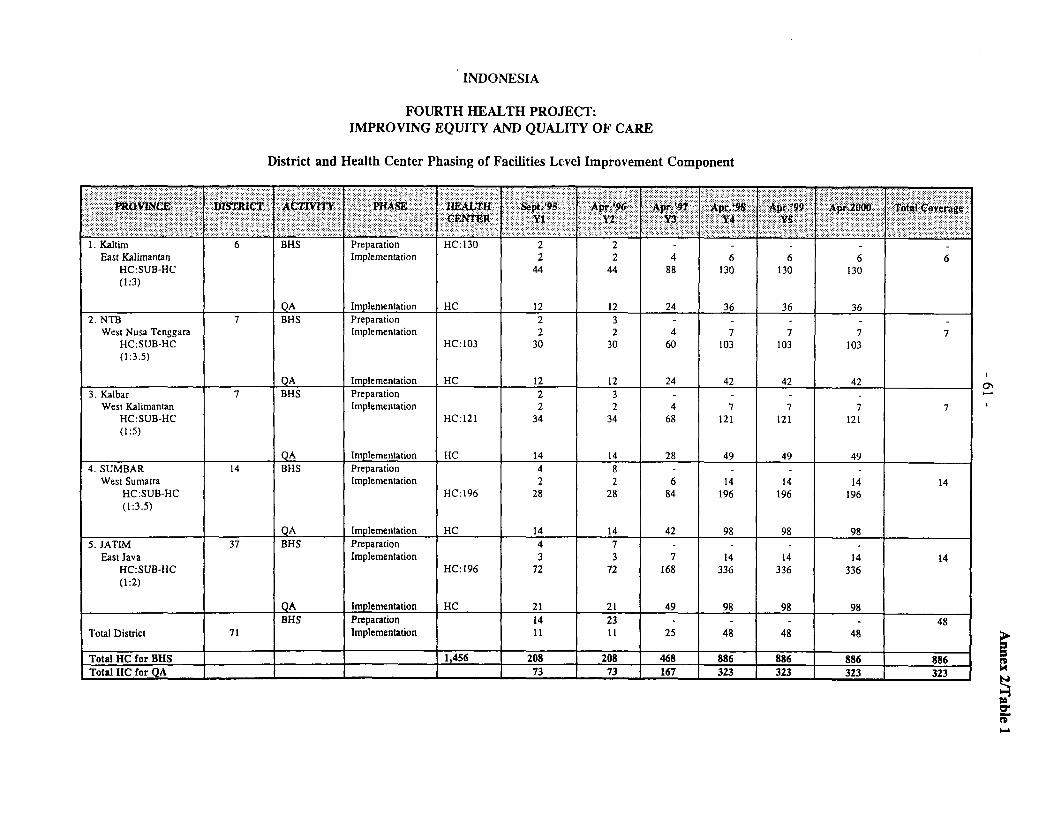
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
District and Health Center Phasing of Facilities Lcvel Improvement Component
P11OYNt.IV .!DISTRICT AIVIPJAg 1ALU St.9 06r2 ':A::'~ kp, p.9 p1200 T1tCvr
1. Kaltim 6 BHS Preparation HC:130 2 2East Kalimantan Implemnentation 2 2 4 6 6 6 6
HC:SUB-H-C 44 44 88 130 130 130(1:3)
QA Implementation HC 12 12 24 36 36 36..._........2. NTB 7 BHS Preparation 2 3HC 10- 2 -
West Nusa Tenggara Implementation 2 2 4 7 7 7 7HC:SUB-HC HC:103 30 30 60 103 103 103(1:3.5)
QA Implementation HC 12 12 24 42 42 42 33. Kalbar 7 BHS Preparation 2 3 - - - -
West Kalimantan Implementation 2 2 4 7 7 7 7HC:SUB-HC HC:121 34 34 68 121 121 121(1:5)
QA Implementation HC 14 14 28 49 49 494. SUMBAR 14 BHS Preparation 4 8 - - -
West Sumatra Implementation 2 2 6 14 14 14 14HC:SUB-HC HC:196 28 28 84 196 196 196(1:3.5)
QA Implementation HC 14 14 42 98 98 98
4. JATIM 37 BHS Preparation 4 7 - - - -
East Java Implementation 3 3 7 14 14 14 14HC:SUB-HC HC:196 72 72 168 336 336 336(1:2)
QA Implementation HC 21 21 49 98 98 98BHS Preparation 14 23 - -48
Total District 71 Implementation I I1 25 48 48 48
Total HC for BHS 1,456 208 208 468 886 886 886 886Total HC for QA 73 73 167 323 323 323 323 14

-62 -Annex 3
Page 1 of 3
CORE PERFORMANCE INDICATORS ANDINDICATIVE TARGETS FOR
MONITORING AND EVALUATION
This note describes indicative targets for the following core performance indicators. Theseindicators are part of a broader list of performance indicators (agreed with GOI) for the project.As with the other performance indicators these will be collected annually by the district healthoffices and compiled at the provincial level.
QUALITY OF CARE
The Fourth Health Project will seek to raise the rate of compliance to standards of care oroperating procedures (SOP) to at least 80%. This means that if in the SOP there are 30different kinds of activities to be carried out, 24 of them will be correctly implemented.
2. RATE OF ADOPTION
The project would measure the rate of adoption of QA mechanisms. The number ofinterventions in the basic health package for which QA would be established over theproject period is as follows:
Number of Interventions in the BHS Listwith Established QA Mechanisms
List of Basic Health Year 1 Year 2 Year 3 Year 4 Year 5Services/a
1 + + + ± +2 ++ + + +3 + + + + +
4 + + + +5 + + + +
6 + + +7 + + +
8 + +9 + +10 + +
/a The phasing of the interventions for which QA will be established will be decided by eachprovince.

- 63 - Annex 3Page 2 of 3
3. BASIC HEALTH SERVICES UTILIZATION RATE
Utilization rate will be broken down into contact rate and visit rate. Contact rate is definedas the number of individuals who had contact with govermnent health facilities in the lastmonth divided by the number of people in their catchment area. Visit rate is defined as thetotal number of visits made to government health facilities in the previous month divided bythe total number of people in their catchment area. For practical reasons, emphasis duringthis project will be put on visit rate. Data from the health facilities' monitoring system,whose improvement has been already started by the Third Health Project, will be used toestimate visit rate. Contact rate can be obtained through SUSENAS or a specially designedsurvey, if deemed necessary. The project will seek to increase the visit rate at a minimumof 10% annually.
4. SHARE OF CENTRAL, PROVINCIAL AND DISTRICT HEALTH SUBSIDIESGOING TO BASIC HEALTH SERVICES AND POOR
The percentage share of the consolidated central, provincial, and district health subsidiesgoing to BHS would be imonitored annually. The share of these subsidies going to the poorwould be measured every other year, starting in the first year. Indicative targets, whichwill be reviewed annually and adjusted as needed, have also been set for BHS recurrentexpenditures per capita (see attached Fourth Health Project Financing Plan).

- 64 - Ann= 3Page 3 of 3
FOURTH HEALTH PROJECT FINANCING PLAN
PER CAPITA EXPENDrIURES FOR RECURRENT COSTS OF BASIC HEALTHSERVICES
(in Rp., excluding salaries)
93/94 95/96 96/97 97/98 98/99 99/00 00/01 01/02
APBN DIP &INPRES
NTB 1,630 1,972 2,170 2,386 2,625 2,888 3,176 3,494Jatim 1,110 1,343 1,477 1,625 1,788 1,966 2,163 2,379Kaltim 2,750 3,328 3,661 4,027 4,430 4,873 5,360 5,896Kalbar 2,200 2,662 2,928 3,221 3,543 3,897 4,287 4,716Sumbar 2,250 2,723 2,995 3,294 3,624 3,986 4,385 4,823
APBD I & APBD IINTB 245 296 420 546 582 715 759 900Jatim 190 230 567 906 933 1,278 1,312 1,662Kaltim 1,000 1,210 1,572 1,947 2,093 2,495 2,672 3,109Kalbar 300 363 708 1,057 1,101 1,458 1,511 1,878Sumbar 250 303 695 1,091 1,128 1,530 1,575 1,986
World BankNTB 0 0 281 188 188 94 94 0Jatim 0 0 941 628 628 314 314 0Kaltim 0 0 724 483 483 241 241 0Kalbar 0 0 926 618 618 309 309 0Sumbar 0 0 1,088 725 725 363 363 0
TOTALNTB 1,875 2,269 2,871 3,120 3,395 3,697 4,029 4,394Jatim 1,300 1,573 2,985 3,158 3,349 3,558 3,788 4,042Kaltim 3,750 4,538 5,957 6,456 7,005 7,069 8,273 9,004Kalbar 2,500 3,025 4,563 4,895 5,262 5,664 6,107 6,594Sumbar 2,500 3,025 4,778 5,110 5,476 5,879 6,322 6,809
Note: These number represent indicative targets for the course of the project and show the format that will beused. Annual reviews of these targets will be undertaken and changes will be agreed by the center, localgovernments and the Bank.

- 65 - Annex 4
Page 1 of 2
INDONESIA
FOURTH HEALTH PROJECT:IPROVING EQUITY AND QUALITY OF CARE
Supervision Plan
Timing Length Mission Purpose Team Composition
I. Oct. 1995 2 Start-up and review of: Economiststaffing; budget proposal; Health Specialistconsultants' deployment; RSI Operations Officertraining plan/arrangements;and M&E planField visit
2. Apr. 1996 2 Review of Procurement & Financial Status EconomistReview of Contracting Processess Implementation SpecialistField visit RSI Operations Officer
3. Oct. 1996 2 Discussion of Annual Report EconomistReview of Work/ Expenditures/Policy Reform Health SpecialictPrograms RSI Operations OfficerPost Review of ContractsTechnical auditField visit
4. May 1997 2 Review of Procurement & Financial Status EconomistReview of Contracting Processess Implementation SpecialistField visit RSI Operations Officer
5. Oct. 1997 2 Discussion of Annual Report EconomistReview of Work/ Expenditures/Policy Reform RSI Operations OfficerProgramsPost Review of Grants and Discussion of Health SpecialistTechnical Audits RSI Operations OfficerField visit
6. May 1998 2 Review of Procurement & Financial Status EconomistReview of Contracting Processes Implementation SpecialistField visit RSI Operations Officer
7. Oct. 1998 2 Mid-term Review Discussion EconomistPost Review of SAE and Discussion of Health SpecialistTechnical Audits RSI Operations OfficerField visit
8. May 1999 2 Review of Procurement & Financial Status EconomistReview of Contracting Processes Implementation SpecialistField visit RSI Operations Officer

- 66 - Annex 4
Page 2 of 2
Timing Length Mission Purpose Team Composition
9. Oct. 2000 2 Discussion of Annual Report EconomistReview of Work/Expenditures/Policy Reform Health SpecialistPrograms RSI Operations OfficerPost Review of SAE and Discussion ofTechnical AuditsField visit
10. May 2001 2 Review of Procurement & Financial Status EconomistPreparation of the Implementation Health SpecialistCompletion Review RSI Operations OfficerField visit
11. Dec. 2001 2 Discussion of the Implementation EconomistCompletion Review Health Specialist
RSI Operations Officer

Annex 5- 67 - Page I of 4
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
Project Activities by Components
I. Facility-Level Service Improvement (65%): US$74.2 million equivalent
To ensure that frontline staff are able to deliver locally appropriate, highly cost-effective BHS, funding would be provided for:
(a) Health Facility Construction and Upgrading (32%): US$36.9 millionequivalent
This amount would support investment costs for upgrading, renovation andbuilding of health centers, subcenters, storage facilities (e.g., for drugs) and, to alimited extent, district hospitals. It would also finance equipment, water supply,vehicles and furniture needed to outfit these facilities.
(b) Special Assistance Program for Basic Health Services (33%): US$37.3million equivalent
This program would fund expenditures on equipment and furniture,operational expenses and recurrent costs (on a declining rate) necessary to meet theresource requirements of reducing current gaps in the quality and provision of basichealth services. These expenditures would include expenses for institutionalizingQA practices, improving BHS utilization, strengthening outreach activities andcarrying out on-the-job training in QA/BHS problem-solving, management andplanning, laboratory, supervision, etc.
US$14.1 of these funds would be provided to health facilities throughdiscretionary Special Assistance Funds (SAF). These funds would be used forfinancing eligible expenses listed in the SAF Operating Guidelines (Annex 10) andclassified as Special Assistance Expenditures (SAE) in the cost tables' category ofexpenditures. Each eligible health center would initially be allocated an annual HCSAF that ranges from Rp 6 million (East Java) to Rp. 10 million (WestKalimantan).
II. Institutional Development (34%): US$39.2 million equivalent
This component would improve the capacity of Central, provincial and district levelagencies to assist, motivate, and supervise frontline health providers in deliveringaccessible high quality packages of basic health services. The following would besupported:

Annex 5- 68 - Page 2 of 4
(a) Support for Quality Assurance Mechanisms: US$7.5 million equivalent
HP IV would assist in building the capacity of the above agencies topromote and help establish quality assurance practices in health facilities and unitsin charge of their supervision. This component will fund workshops, materials,consultant services, incentives, fellowships, travel and other expenses to carry outthe following activities: (i) review of current standards as applied to clinicalprotocols, and management and support procedures; (ii) establishment of a formalaccreditation process in which health centers and their staff will receive someincentives based on documented quality improvements; (iii) training of clinic staffand field supervisors and enhancement of field support for the application ofmodern quality assurance techniques; (iv) development of Central and provincialstaff dedicated to QA and professional organizations as sources of technicalassistance; and (v) documentation and dissemination of problem-solving experiencesthrough a professionally produced QA newsletter.
(b) Support for Training and Curriculum Development: US$9.1 millionequivalent
This component would develop institutional capacity at the district level andabove to provide training support required by the quality assurance program andother key HP IV initiatives. The project will fund expenditures for instructionalmaterials and equipment, workshops, consultant services, fellowships, incentivesand other expenses needed for the following activities: (i) building a capacity inPusdiklat and Bapelkes to train trainers and to develop learningmaterials/methodologies needed by the QA program; (ii) assessment of clinicaltraining needs; (iii) development of QA learning packages and alternatives toresidence/off-the-job training courses such as distance learning; (iv) training,evaluation and certification of trainers; (v) monitoring and evaluation of post-training performance; (vi) revision of incentives to learning; and (vii) institution ofa training information system and approval process to control training activitiesbetter.
(c) Support for Performance-Linked Incentives: US$0.6 million equivalent
Under this subcomponent, HP IV would finance activities designed toestablish a system for measuring and rewarding district performance. The projectwould fund expenditures for consultants services, travel, materials, computers,software, equipment, surveys, incentives and other expenses for: (i) formulatingsystem design and ways of measuring the performance criteria in Annex 3; (ii) datacollection and analysis; and (iii) provision of performance-based incentives.
(d) Replication and Piloting Innovative Initiatives: US$15.5 million equivalent
HP IV would support several efforts to replicate HP III innovations and tryother initiatives that could lead to improvements in the organizational culture of thepublic health system and its role in the provision of basic health services. Thissubcomponent would finance expenditures related to the following activities:

Annex 5- 69 - Page 3 of 4
(i) Dissemination and Adaptation of HP III Innovations: US$1.8 millionequivalent
This amount would support workshops, local consultants, travel and othercosts of disseminating and advancing selected innovations that have beensuccessfully developed and tried under the Third Health Project. These wouldinclude among others: (i) integrated planning and budgeting; (ii) drugs management(LPLPO); and (iii) equipment inventory, ordering and procurement system. Alongwith the institution of these new drug and equipment management systems, HP IVwould fund some facility upgrading to support these systems and procurement ofbasic drugs and other materials.
(ii) Piloting Exemplary Integrated District Health System: US$13.7 millionequivalent
The project would also support a program providing health districts withdiscretionary Special Assistance Funds (HD SAF). Dokabus can use these fundsas they deem appropriate to improve their supervision, support and motivation offrontline managers and staff, provided their expenditures conform to the SAFOperating Guidelines (see Annex 10). Eligible expenditures, referred to as SpecialAssistance Expenditures in the cost tables below, include operational costs,instructional materials and equipment, incentives, health providers' fees, and otherexpenses for: QA development, strengthening of outreach activities andsupervision, building of the district's capacity to provide on-the-job trainingsupport, staff re-deployment, and improved monitoring and evaluation. A total ofUS$9.4 million will be allocated for the Health District SAF.
In addition, this subcomponent would fund a limited number of pilotprograms and QA studies. Under this component, the project would financeprogram development expenditures (PDE) needed to carry out proposals approvedin accordance with the process of review and approval laid out in the OperatingGuidelines for PDE (see Annex 11) and for eligible expenses listed therein. A totalof US$4.7 million equivalent would be allocated for PDE.
e. Project Management Support (6%): US$6.5 million equivalent
Funds under this subcomponent, which represent about 6 percent of totalbase cost or less than 5 percent of total project cost, would be used to financeproject management activities. These activities include the provision of technicalassistance to local implementing units; project oversight and administration;coordination and policy support; monitoring and evaluation; and management of thereview and approval process for PDE-funded pilot activities funded.
III. Better Resource Allocation and Revenue Generation (1%): US$1.4 millionequivalent
Funds would be provided for technical assistance (TA), data collection and analysis,materials and workshops to design and promote facility-level fee increases and revenue
Annex 5-70- Page4of4
retention, and institute more effective targeting of health subsidies to appropriate recipientsand activities. The project would also help MOH: (i) to develop and establishmechanisms for monitoring and reporting the total health subsidies going to BHS and thepoor, especially their corresponding share in Central and local health budgets for thenation as a whole and for each of the five provinces; and (ii) to develop a system foranalyzing annual APBN (National Budget) and APBD (Regional Budget) budgetarydecisions in terms of the above financial indicators.

INDONESIAFOURTH HEALTH PROJECT:
IMPROVING EQUITY AND QUALITY OF CAREExpenditure Accounts by Components
(USS '000)
InsKiutlonal Development
Facility-Level Service Replicatlon & PilotingImprovement Innovative Initlatives
PllotingSpeclal Support for Dlsseminatio Exemplary Better
Assistance Support for Tralning Support for n and Integrated ResourceHealth Facility Program for Quality and Performance- Adaptation of Dlstrdct Project AllocationConstruction Baslc Health Assurance Curriculum Linked HP iII Health Management & Revenue
and Upgrading Services Mechanisms Dev. Incentives Innovatlons System Support Generatlon Total
I. Investment CostsA. CMIl Worts 31270 122 68 31458B. Equlpment 11,107 19 418 107 252 101.4 12,002C. Fumiture 398 8 16 421D. Vehicles 64 64E. Consultant Services & Studies
1 DormesticConsutant Services 50 1,072 247 261.1 165.3 1,7952 Intemational Consultant Services 548 326 74 295.3 1539.4 2,7803 Studies 274 20 310 188 117.8 134.7 839.4 1,881
Subtotal Consultant Services & Studles - 50 1,a91 346 384 432 674 1,674 1,005 6,456F. Fellowships
1 Domestic Feliwships 2,599 28 132.1 2,7582 Overseas Fellowships 467 5,687 78.5 562.9 91.9 6,887
Subtotal Fellowships - 467 8,285 - 28 79 695 92 9,645G. Tralning and Workshops 1,289 900 631 128 503 101.3 209.5 3,761H. Program Development Expendiures 4903.2 4,903I. Special Assittance Expendiures 17,014 769 10544.4 28,328G. Project Management 5173.8 5,174Total Investment Costs 42,838 18,372 4,027 9,607 618 1,297 16,301 7,543 1,408 102,211
II. Recurrent CostsA. Otflce Consumablea 9 323 58 1 95 3.2 489B. Supervislon - Travel 2,396 1,324 232 58 525 13.7 4,549C. Operations and Maintenance 19 3,784 3,238 91 28 163 90.3 7t413D. Drugs 19,614 19,614Total Recurrent Costs 19 25,804 4,884 381 87 782 - - 107 32,065
Total Project Costs 42,857 44,178 8,912 10,188 706 2,079 16,301 7,543 1,515 134,278
Taxes 1051.7 1785.7 29.3 43.8 9.8 33 9.5 2,963Foreign Exchange 17005.7 10872.4 1588.7 6034 188.7 371.5 1792 2227.8 281.2 40357.9
o O>

INDONESIAFOURTH HEALTH PROJECT:
IMPROVING EQUITY AND QUALITY OF CAREExpenditure Accounts by Years
(US$ '000)
Total Including Contingencies95/96 96/97 97/98 98/99 99/00 Total
I. Investment CostsA. Civil Works 3,666 5,229 7,704 7,547 7,311 31,457
Water Supply Construction 337 229 199 166 173 1,104New Building 1,758 2,903 4,551 4,567 4,467 18,246Renovation/RehabilitationlUpgradelExtenti 1,571 2,097 2,954 2,814 2,671 12,107
B. Equipment 2,291 2,066 2,794 2,734 2,118 12,002C. Furniture 238 76 58 43 6 421D. Vehicles 64 - - - - 64E. Consultant Services & Studies
I Domestic ConsuHtant Services 419 494 327 342 212 1,7952 International Consultant Services 1,115 586 385 343 352 2,7803 Studies 667 419 377 281 136 1,881 N
Subtotal Consultant Services & Studies 2,201 1,500 1,089 966 700 6,456F. Fellowships
1 Domestic Fellowships 667 713 696 611 72 2,7582 Overseas Fellowships 1,759 1,775 1,727 1,224 402 6,887
Subtotal Fellowships 2,426 2,489 2,422 1,835 474 9,645G. Training and Workshops 1,063 723 851 581 543 3,761H. Program Development Expenditures 892 934 979 1,025 1,073 4,9031. Special Assistance Expenditures /a 1,664 4,461 7,102 7,438 7,663 28,328G. Project Management 939 971 1,044 1,105 1,116 5,174Total Investment Costs 15,443 18,448 24,041 23,273 21,005 102,211
II. Recurrent CostsA Office Consumables 158 67 112 30 122 489B. Supervision - Travel 773 754 1,010 1,008 1,005 4,549C. Operations and Maintenance 284 977 1,982 2,036 2,133 7,413D. Drugs 2,046 3,415 4,682 5,509 3,964 19,615Total Recurrent Costs Ia 3,261 5,212 7,785 8,583 7,224 32,065
Total Project Costs 18,704 23,660 31,826 31,856 28,229 134,276
o O'

- 73 - Annex 7
INDONESIAFOURTH HEALTH PROJECT:
IMPROVING EQUITY AND QUALITY OF CARE
Procurement PlanContracting and Review Responsibilities
Contract
Total Estmated Bank DocumentsValue Contract DIPMNPRES Procurement Kind of Review required for
No. Category (USS M) Quantity Allocation Method Review /b By Disbursement
1 Civil Works 31.4 165
Small contract <$50,000 7 135 District National Shopping Random Post SPN/c SOEForce Account
Medium contract >$50,000 -<S1,000.000 24.4 30 Province/District LCB Random Post RSI SOELarge contract >$1.000,000 (if any) 0 0 Province/District LCB Prior RSI FullFirst contract regardless of the amount of each province 5 Province TBD Prior RSI Full
2 Equipment/Furniture 12.4 32
Small package <$50,000 5 District Shopping Random Post SPN SOEMediun package >550,000 - <$200,000 5.4 25 Province LCB Random Post RSI SOESpecific and large package>'$200,000 2 7 Central/Province ICB Prior TM FullFirst contract >$50,000 of each province 5 Province TBD Prior RSI Full
3 Consultancy Service & Studies 6.5 87
Firm <'100,000 2.5 25 Center/Province Short listing Limited Prior RSI SOEIndividual <550.000 3 60 Center/Province Others Limited Prior RSI SOEOthers 1 2 Center Others Prior TM Full
4 Fellowships 9.6 N/A Center/Province Others Limited Prior RSI SOE
5 Local Training and Workshops 3.8 N/A Center/Province/ Others Random Post SPN SOEDistrict
6 Special Assistance Expenditures (SAE) la 28.3 N/A
Health center 17 District Others Random Post SPN SOEHealth district 11.3 District Others Random Post SPN SOE
7 Program Development Expenditure (PDE) la 4.9 N/A Central/Province Others Limited Prior TM SOE
8 Project Management Expenditures 5.2 N/A Center/Province Others Random Post SPN SOE
9 Incremental Recurrent Costs 32.1 N/A Province/District Others Random Post SPN SOE
Total Costs excluding vehicles US$0.1 million 134.2 284
/a Using agreed operating guidelines and action plan, and list of eligible expenditures./b Prior review, random post review and limited prior review (TOR, proposed program and draft contract)./c Supervision missions/d Task Manager/e Office consumables. O&M. and travel expenses

Annex 8- 74 -
INDONESIA
FOURTH HEALTH PROJECT:IMNPROVING EQUITY AND QUALITY OF CARE
ESTIMATED SCHEDULE OF DISBURSEMENTS
DisbursementsIBRD fiscal year Amount per Cumulative Disbursement profile /a
semester Amount % %----------- (US$ million) -----------
19961 1.0 1.0 0 0
2 3.0 4.0 5 3
19971 6.0 10.0 11 62 6.0 16.0 18 10
1998l 12.0 28.0 32 142 12.0 40.0 45 30
1999
l 13.0 53.0 60 382 13.0 66.0 75 50
2000
1 7.5 73.5 84 622 7.5 81.0 92 74
20011 3.5 84.5 96 822 3.5 88.0 100 90
Project Completion Date: September 30, 2000Project Closing Date: March 31, 2001
/a Latest standard disbursement profile for health projects in Indonesia (June 1994).

Annex 9Page 1 of 2
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
The Sixth Five-Year Development PlanRepelita VI Summary
HEALTH
OUTCOMES TARGETS BY END OF REPELITA VI
(a) Life expectancy at birth: increase to 64.6 years.(b) Crude death rate: decrease to 7.5/1000 population.(c) Infant mortality rate: decrease to 50/1000 live births.(d) Under-five mortality: decrease to 66/1000 population under five years old.(e) Maternal mortality decrease to 255/100,000 births.(f) Energy and protein malnutrition among under-five children: decrease to 30 percent.(g) Low birth weight: decrease to 10 percent.(h) Anemia: decrease to 40 percent among under-five children.(i) Prevalence of iodine deficiency: decrease to 18 percent and no new cretinism.(j) Vitamin A deficiency among under-five children: decrease 0.1 percent.
2. POLICIES
(a) Improvement of equity and quality of health services:
- improvement of equity and quality of health services for the poor, children andneglected elderly
* development of health technology
(b) Increase community nutritional status through nutrition improvement program forhigh risk groups.
(c) Improvement of participation of community, private sector, and professionalassociations.
* development of health habits and clean environment* improvement of the role of private enterprises in health services* empowerment of professional associations
(d) Improvement of health management, especially decentralization to the district level.

- 76 - Annex 9Page 2 of 2
3. PROGRAMS
a. Principal programs:* community health education* community (basic) health services* hospital and health referral services* nutrition improvement* communicable diseases control* food and drug control* traditional medicine development
b. Supporting programs:* water supply* environmental health* training and education* health research development* youth in health development* women role in health development* health information system

- 77 - Annex 10
Page 1 of 4
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
SAF OPERATING GUIDELINESSUMMARY
Introduction
1. HEP IV would finance expenditures needed to carry out service improvement plans drawn up byhealth centers and districts through problem-solving and priority setting exercises. The aim is to enhancethe ability and motivation of frontline providers and managers to render higher quality, more accessiblebasic health services (BHS) that efficiently meet the needs and demands of clients and that effectively reachthe poor. For this purpose, a program would be established providing Special Assistance Funds (SAFs) forhealth centers (HC) and health districts (HD).
2. SAFs comprise discretionary resources that puskesmas and health district managers could use foreligible expenditures (mainly for operations) needed to initiate and implement their plans. This annexsummarizes the list of eligible expenditures, the operating procedures regarding the use of SAFs, and theassionment of oversight responsibility. (Expenditures made through the SAF are referred to in the costtables and below as SAE or Special Assistance Expenditures.)
3. HC and HD managers are expected to use SAFs as they deem appropriate within the parametersdescribed in these guidelines.
Eligible Expenditures and Criteria for Awarding SAFs
4. The above funds could be spent only on goods and services described in the attached Tables I and2 of this Annex.
Limitations
5. Allocation to staff incentives should not exceed 25 percent of the HC special assistance fund.
Administration, Technical Review and Record Keeping
6. The Dokabu is responsible for the administration of both HC and HD SAFs. Required documents(see below) should be kept at one designated District Health Office location for spot-checking by Banksupervision missions and for audit purposes.

- 78 - Annex 10
Page 2 of 4
Documentation Requirements
7. The following documents should be submitted before SAFs are budgeted in the DIP:
(a) Health center proposals signed by the Puskesmas head and countersigned by the Dokabu,briefly indicating his comments,
(b) Health district proposals signed by the Dokabu and countersigned by the Kakanwil alongwith brief comments from him.
Financial Accountability Procedures
8. Financial audit will be conducted according to standard government operating proceduresacceptable to the Bank.
Disbursement
9. Special assistance expenditures (SAE), which are outlays paid for by SAFs, would be financed bythe Bank through standard SOE (Statement of Expenditures) procedures, on a declining rate basis. Theseexpenses would be financed by the Bank only if they follow the SAF operating guidelines.
Dokabu's Annual HC SAF Report
10. The Dokabu will submit a report to the Kakanwil not later than September 1 of each year. It willsummarize the accomplishments of the recipient health centers, highlighting the health district's analysis offive most important problems for which the SAFs were used, separately for HC and HD. The report alsoshould describe the solutions implemented, key lessons learned, and corrective steps taken or proposed toimprove efficient utilization and effectiveness of SAFs.

-79 - Annex 10
Page 3 of 4
Table 1Expenditures Items Eligible for SAE Funding
Those items which can be financed by SAE funds are listed below, for both health centers anddistrict or municipal health offices:
1. Health Centers
* Travel costs
* Maintenance of health center and sub-centers (maximum Rp. 5 million per year per health centerand Rp. 1 million per sub-center); equipment and vehicle maintenance
* Cost of materials and supplies
* Incentives for existing staff and wages for non-professional contract/daily workers (maximum of 25percent of total SAE funds)
* Other costs, including meetings, prizes for kader and community organizations, transport foremergency referral cases (based on need)
2. District or Municipal Health Offices
. Travel costs for supervision and consultations with health center staff, delivery costs for drugs andequipment
. Incentives for staff placement in remote or undesirable areas, including moving costs or postallowances; to attract professional staff to district health office; home leave allowance forprofessional staff from. outside area, especially for outstanding performance
. Maintenance of vehicles, computer and office equipment and medical equipment
l Materials: Recording and reporting forms, computer supplies
l Contract work for health professionals who are not civil servants (special permission needed)
| Books, journals and computer software
. Others: rewards or prizes for health centers, meetings with government or community groups

- 80 - Annex 10
Page 4 of 4
Table 2Criteria for Awarding SAE Funds
1. Health Centers - SAF funds should not be awarded equally to all health centers in the district. The levelof funds should be based on the following:
* Ability of the community to paY for health services. Those areas covering poor villages should be allocatedmore funds. Percent of population in poor villages (desa miskin) or the number of people with health cardsmight be used as ways to measure this.
* Difficulty in covering service area. Those health centers in areas which cover a large geographic area andhave difficult transportation should be given higher allocations. This might be done by giving a high unitcost for travel.
. High volume of services provided and high coverage of key prorrams. Health centers and sub-centers witha large number of visits might be given high allocations to reflect their higher need for materials, supplies,staff incentives and so forth. This also promotes greater efficiency. Special health centers with beds, alarge number of sub-centers or providing extra services (referral laboratory, etc.) should also receive higherallocations.
* Management including performance and implementation of previous allocations. Special considerationsshould be given to health centers with high performance levels or where there have been substantialimprovements from previous years.
2. Districts and Municipal Health Offices - The basic criteria involved in determining the funds for the districtl SAF involve the size of the service area, the number of health centers and the relative wealth of the district or
municipality. In addition, special considerations are needed for staff incentives and the employment ofcontract workers.
^ The ability of the district or municipality to fund its own recurrent costs for the district health office.
. The number of health centers to be supervised and the unit cost of travel to health centers
. The number of district health staff involved in supervision and the amount of time they are expected totravel.
. The number of areas where special assignment incentives are needed.
The difficulty in attracting staff to the district health office
The justification for special contract workers, mainly involving the need for critical staff and the lack ofalternatives.
The total population served in the district or municipality.
The performance of district staff in managing health services.
- 81 - Annex 11
Page 1 of 3
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
Program Development Expenditure (PDE) Operating Guidelines
1. The PDE is intended to support innovative experiments that could lead tobreakthroughs in the development of exemplary health districts. It is hoped that takentogether these innovations and their documentation would strengthen the implementationof Repelita VI policies.
Eligible Expenditures
2. The PDE can be used to finance expenditures needed to carry out approved pilotactivities and research. Eligible expenditures are limited to the following items: officeequipment (including PC computers), data collection and analysis, training, supplies andmaterials, fees for private service providers, consultants, travel costs, staff redeploymentcosts, and experimental incentives. Civil works and equipment other than computers arenot eligible.
3. Pilot activities eligible for funding are limited to the formulation and testing ofinnovative schemes related to the development of: (i) prepaid care; (ii) decentralized staffdeployment and recruitment system; (iii) private sector participation, including contractingwith private health service providers; and (iv) performance-based incentive schemes andJabatan Fungsional.
4. To be eligible for Bank financing, purchases must be in accordance withprocurement procedures acceptable to the Bank.
Proposals
5. To facilitate their evaluation, proposals should be prepared in the following format:
(a) Objectives
(b) Statement of the problem and the proposed solution to be explored
(c) Relevance to the implementation of Repelita VI policies and developmentof an exemplary District Health System
(d) Scope of work: design and implementation plan
(e) Cost estimates and budget, following standard format;

- 82 - Annex 11
Page 2 of 3
(f) Monitoring and evaluation plan
6. A proposal could be a joint undertaking between the province or the center andother agencies, including Perum Husada Bhakti, academic/research institutions, andprofessional health organizations. Consultants from either the province or the centerwould assist in preparing proposals as needed.
Criteria for Evaluation
7. Each proposal submitted in the above format will be evaluated using the followingcriteria:
(a) Clarity of its objectives
(b) Relevance to the purposes for which PDE has been established and HP-IVobjectives
(c) Appropriateness and feasibility of the proposed design and implementationplan
(d) Adequacy of the monitoring and evaluation plan
(e) Scaling-up potential and sustainability
(f) Reasonableness of cost-estimates
(g) Competence and experience of the proponents and implementors of theproposal
Review and Approval of Proposals
8. In the five HP-IV provinces, prepared proposals will be submitted to theProvincial Project Officer (Kakanwil) for review by the Provincial Technical TaskForce and Project consultants. The Task Force will provide brief written commentsabout each proposal. The Provincial Project Officer is responsible for submitting to theProject Officer proposals for PDE funding. Proposals prepared at the central level willalso be submitted to the Project Officer.
9. The Project Officer, assisted by the Deputy Project Officer and Projectconsultants, will review proposals to ensure that the formats are followed and that thebudgets use standard unit costs. He will also prepare a written technical review of eachproposal.

- 83 - Annex 11
Page 3 of 3
10. All proposals, along with written comments, will be submitted to the CentralTechnical Task Force for final approval or rejection. Proposals approved by theTechnical Task Force will be returned to the Project Officer who will prepare them forsubmission to the World Bank for limited prior review.
11. In the case of proposals, such as prepaid health care, which involve sectors outsidethe Ministry of Health, the Project Officer will be responsible for obtaining commentsand approvals from all relevant departments and agencies.
Funds channeling, disbursement and accountability
12. PDE funds will be allocated in the DIP (provincial as well as the central level) forapproved proposals. The Provincial Project Officer, assisted by the ProvincialAdministrative Officer and the Executive Secretary, will be responsible for thedisbursement of funds for approved proposals and their accounting. The Provincial andCentral Technical Task Forces will be responsible for monitoring the implementation ofthese projects, recommending changes if necessary. The Bank will finance, through PDEfunds, eligible expenditures incurred in accordance with this operating guidelines and theprocurement and disbursement procedures laid out in Chapter 4 of the Staff AppraisalReport. The PDE funds will be audited following standard government practice vis-a-visBank-funded projects in Indonesia.
Reporting
13. The Provincial Project Officer, assisted by the Provincial Technical TaskForce, will submit to the Central Project Officer annual progress reports and thecompletion reports on the implementation of approved proposals. Release of PDE fundswill be contingent on acceptable progress reports and satisfactory execution of thoseproposals.
Evaluations and recommendations
14. The Project Officer, assisted by the Central Technical Task Force, will reviewreports, and will make recommendations regarding needed revisions and follow-upactions. The Bank will be sent a copy of the final report from each project, along with thetask force's review.

- 84 - Annex 12
Page 1 of 3
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
PROJECT MANAGEMENT
I . The management of the project is based on three principles. First, it should use theexisting structure of the Ministry of Health (MOH) whenever possible to facilitate projectimplementation and to make its innovations sustainable. Second, management arrangementsshould be clear and simple to prevent responsibilities and accountability from becomingdiffused. Third, special emphasis on strengthening district management of health services, witheffective technical support from the provincial and central levels, should continue.
Central Level Management
2. Project Director - The Project Director will have ultimate responsibility for theProject. This position will be held by the Secretary General of MOH. He will be responsiblefor making decisions involving the overall direction of the Project, as well as relevant policyissues.
3. Project Officer - The Chief of the Bureau of Planning in the Secretariat General willbe in-charge of managing the Project and will be accountable for its technical andadministrative aspects.
4. Deputy Project Officer - The Project Officer would be assisted by a Deputy ProjectOfficer who would oversee day-to-day technical and administrative activities of HP IV. Inaddition, he would be responsible for ensuring coordination of HP IV activities with othergovernment initiatives and donor-assisted projects to prevent unnecessary duplication and topromote exchange of experience. An echelon III official in the Bureau of Planning would beappointed as Deputy Project Director and would be assigned on a part-time basis.
5. Project Secretariat - HP IV would establish a unit with full-time staff responsible forroutine administrative matters, including submittting required reports to the Bank and supportfor technical activities. An Executive Secretary would be responsible for the management ofthe Project Secretariat at the center and for coordinating work with the AdministrativeOfficers in the five provinces. Administrative and Financial Officers as well as other full-timestaff would be recruited to work for the Project Secretariat.
6. A Central Technical Task Force would be organized to review and guide keytechnical and policy innovations which involve Directorates General outside the SecretariatGeneral. Since most of the planned project initiatives concern Basic Health Services, theDirector General of Community Health would lead this Technical Task Force.

- 85 - Annex 12
Page 2 of 3
7. An Advisory Board, consisting of Echelon I officials from various departments andagencies involved in the project, would also be set up to ensure support for policy reformsthat need intersectorial consultation. The Board would be led by the Deputy for HumanResource Development in BAPPENAS and would serve not only HP IV but also other Bank-assisted health projects.
8. A Steering Committee, consisting of Echelon II officials of MOH units involved inHP IV would be established and attached to the Project Officer. This committee would meetregularly to advise the Project Officer about various technical and administrative issues.
Provincial Level Management
9. Provincial Project Ofricer - The head of the Provincial Health Office (Kakanwil)would be the Provincial Project Officer, which would be the provincial equivalent of theProject Director. The Kakanwil would ultimately be accountable for all project-relatedactivities in the province; he would be responsible for solving problems that cannot beresolved at lower levels.
10. Provincial Project Implementation Officer - The head of the Provincial HealthServices (Dinas Kesehatan I) would be in-charge of the implementation of all province-level.
11. Administrative Officer - The head of the Provincial Health Office Planning Divisionwould oversee the overall administration of the project in the province and would beresponsible to the Provincial Project Officer. This part-time assignment would be in additionto his structural duties. His project responsibility includes reporting, planning, coordination,monitoring and reporting of HP IV activities. The Administrative Officer would be assisted bya small, full-time administrative staff.
12. Provincial Steering Committee - This would be an intersectoral committee withrepresentatives from local departments and agencies involved in project planning andimplementation.
13. Provincial Technical Task Force - This task force would be responsible formonitoring and guiding all technical aspects of HP IV innovations. It would be led by theProvincial Project Officer, with the Head of the Division of Health Services in the ProvincialHealth Office (Kanwil) as the first secretary. HP IV consultants would work closely with thistask force.
District Level Management
14. District Project Officer - The head of the District Health Office (Dokabu) would beresponsible for the planning, implementation and administration of district-level projectactivities. He would also oversee HP IV health center activities. The Dokabu would also be

- 86 - Annex 12Page 3 of 3
in charge of proposing, testing and evaluating district health innovations. As District ProjectOfficer, he would report directly to the Provincial Project Officer (Kakanwil).
15. District Health Development Committee - This body would be established to guidethe overall development of the health sector in the district. This would be an intersectoralteam with strong participation from the Bupati (Head of District Administration) and the headof the district planning agency (BAPPEDA II).
16. District Implementation Officer - He would be responsible for the day-to-dayimplementation of project activities within the district and would report to the District ProjectOfficer.
Health Center Level
17. The Puskesmas head would be responsible for project activities at the health center,and associated sub-centers and community. He would be accountable to the District ProjectOfficer (Dokabu).
18. During the course of project implementation, efforts would be made to developmechanisms to promote active community involvement in health services, with the objectiveof making health facilities more accountable to the community they are serving. To this end,participation by local government and community organizations would be mobilized,particularly the LKMD and village and sub-district leaders. Where appropriate, CommunityHealth Committees would be formed.
- 87 - Annex 13
Page 1 of 2
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
Basic Health Services
I. A key mechanism through which BP IV would attain its goals of equity and qualityimprovement is to reorient public spending on health towards basic health services (BHS). Tothis end, GOI would raise the share of BHS in total health subsidies according to agreedtargets, the achievement of which would be reviewed regularly. The issue is what shouldcomprise BHS. This is important not only for setting those targets and monitoring theirachievement (a key result area), but also for defining the interventions for which the SpecialAssistance Funds should be used.
2. BHS and the DIP Terpadu. At present, GOI regards the primary health servicesincluded in the DIP Terpadu as its BHS. Adjustments, however, are needed to sharpen thefocus of government health spending on highly cost-effective interventions, including somebasic referral services provided by district hospitals. In this regard, MOH plans to formulate aBHS list based on both epidemiological and cost-effectiveness principles. The newformulation would draw from the experience of the 1993 World Development Report,particularly in regard its concept of essential health services and the DALY (disability-adjustedlife years) methodology. HP IV would support this initiative, which would be started soonafter project effectiveness.
3. Completion of the above effort, however, would take time. It was agreed, therefore,that the BHS would meanwhile comprise activities funded.in the current DIP Terpadu forpurposes of implementing and monitoring HP IV's agenda of raising BHS funding. Theseessentially are activities conducted through the Puskesmas, including all outreach activities.
4. The Basic Awal. In allocating limited HP IV funds, MOH would give top priority toa subset of health services covered by the DIP Terpadu. The ten health services in this subset,which are listed below and are referred to as Basic Awal, were chosen because they arecurrently regarded as national priorities. Specifically, they were selected on the followinggrounds:
(a) their contribution to the IMR and MNR reduction;(b) GOI's international commitments of GOI (e.g., World Summit for Children
along with its Mid-Decade Goal; Polio Eradication by the Year 2000;Elimination of Leprosy by the year 2000); and
(c) Inclusion of other communicable diseases with high morbidity and mortalityrates, but low program coverage such as malaria in provinces outside Java-Baliand tuberculosis.

- 88 - Annex 13
Page 2 of 2
5. The ten basic health services in the Basic Awal, for which MOH would like to providethe funds needed to close existing gaps in utilization and quality, include:
(i) immunization;(ii) antenatal care, including TT vaccination, provision of iron tablet and
referral of high risk pregnancy;(iii) treatment for TB cases;(iv) treatment for malaria cases;(v) treatment for ARl/pneumonia and diarrhea among under fives;(vi) iodine, vitamin A and iron tablets for pregnant women and under fives;
(vii) vector control (especially, malaria and dengue);(viii) health education;(ix) family planning services; and(x) school health, including antihelmintics.
6. Improvement in these services through direct and indirect means would be the initialfocus of HP IV financial support. During the course of HP-IV implementation, modifications(acceptable to the Bank) of the composition of the Basic Awal would be made as the resultsof the aforementioned cost-analysis become available.
Annex 14- 89 - Page 1 of 9
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
Developing a Quality Assurance Program
1. To improve the quality of basic health services provided by publicly managed healthfacilities in Indonesia, it is necessary to change work processes, attitudes, skills and otheraspects of their organizational culture. A key to bring about this change is to establish facility-level quality assurance (QA) processes. This annex briefly outlines HP IV's strategy fordeveloping and instituting QA mechanisms and practices and then presents initial results of aQA pilot conducted by MOH as part of project preparation.
Quality Assurance Strategy
2. Quality assurance is an approach to building institutional capacity and organizationalculture that focus on continuous improvements in service (product) quality and on its abilityto satisfy consumer requirements. In HP IV, this approach would be applied to problemsrelating to compliance with case management protocols for effective care and broader issuesregarding efficient provision and utilization of services.
3. The HP IV quality assurance program would seek to improve technical competence,client satisfaction, efficiency, coverage/access, and effectiveness. The program would be anevolutionary one, beginning with frontline health staff learning to analyze and resolve simpleproblems of non-compliance with clinical standards and progressing to more complex issuespertaining to priority-setting and health outcome problems. Its specific configuration would beshaped through a series of structured learning-by-doing activities. Improving technicalcompliance is good place to start: standards of care recommended on the basis of availablescientific information, if followed, provides the best chance to the patient of a speedy and saferecovery.
4. In broad outline, the establishment of QA mechanisms and practices in health facilitieswould be phased as follows:
(a) Phase 1. A detailed methodical analysis - referred to as "systems analysis" in theQA literature -of the technical quality of health services would be conducted ineach participating health center. Observation guides, based on accepted treatmentnorms, would be used to document where patient care fell short of the standard.Based on the results of this analysis, each health center would develop its own planof action to correct lapses in technical quality and would implement those plansthrough direct supervision and on-the-job training. The objective in this phase is to

Annex 1490 - Page 2 of 9
bring the provision of clinical services into compliance with recommendedstandards of care. For example, if one of the standards for ARI (acute respiratoryinfection) were to count the respiration rate, during phase 1 health centers wouldensure that all service delivery personnel would be able to perform this correctlyand do it for all ARI cases.
(b) Phase 2. Supervisors would assist health centers in monitoring and improvingtechnical service quality. The supervisors would be trained to support and monitorthe improvements in activities and processes; they would also receive training inhow to analyze more complex quality problems (the difference between simple andcomplex quality problems is described below). The objective of this phase is tocomplete the work on compliance with technical standards of quality, and to moveon to somewhat more complex quality issues.
(c) Phase 3. In the final phase of implementation, health center staff would be trainedto analyze and resolve complex service quality problems. While they would still beassisted by the supervisors, the importance of the supervisor as a coach orfacilitator would diminish during this phase as health center staff acquire the skillsneeded to analyze and solve complex problems. The objective of this phase is toconsolidate a sustained and effective effort at the health center level to improveservice quality.
Coverage
5. The program would cover as many clinical activities as possible from the start of the loanand technical performance standards will be adopted and disseminated for the following sevenhealth services: immunization, ante natal care (ANC), tuberculosis, malaria, ARI, nutrition, andfamily pianning. Two districts in each province (three in East Java) would implement the QAprogram during the first year of the loan; additional districts would be added each year until all ofthe districts (included in HP IV) in a province have been incorporated into the program by the endof year four.
The Experience of the Pilot Project
6. To build a strong foundation for HP IV's quality assurance program, a pilot projectfunded by resources from the Japan Grant Facility and USAID's International QualityAssurance Program was undertaken to try out some QA models in ten health centers. Theaim was primarily to assist MOH develop its own QA program for HP IV funding. Asecondary objective was to get a head start in building MOH capacity to carry out its QAprogram by providing key staff and domestic consultants some QA experience and bydocumenting local case materials for QA training and promotion purposes.

Annex 14- 91- Page 3 of 9
7. The following discussion of the above-mentioned QA pilot activity illustrates how theQA program will work in the field and lend substance to the concept of quality assurance.
(a) The systems analysis: Ten health centers participated in the pilot project, fivein East Java and five in Nusa Tenggara Barat (NTB). A baseline survey, orsystems analysis, of the quality of care in three basic health services -antenatal care (ANC), management of acute respiratory infections (ARI), andvaccination -was conducted in May and June of 1994. Three health workersfrom each health center were trained in the use of observation forms that werebased on detailed service standards (these were adapted from internationalsources through field testing in both provinces). An observation formcontained from 40 to 60 items for each health intervention detailing theactivities that should be performed. As an example, the section on ANChistory taking was checked to see if the health worker asked the expectantwoman six questions about her reproductive history (number of pregnancies,previous complications, etc.) and ten questions on maternal risk factors(spotting, kidney problems, use of medications, etc.). The three trained healthworkers then spent two or more days in a neighboring clinic observing thetreatment given twenty-five patients for each of the three health interventions.The assumption was that this number would provide an adequate sample toidentify deficiencies in health care. The large number of deficiencies reported inthis peer evaluation encourages confidence in the results.
(b) Plans of action: The results of the systems analyses were given to the seniorstaff of the health centers. The staffs were then asked to prepare plans of actionto address the deviations from standards. Consequently, they tried to identifythe most pressing quality problems and then sought to resolve them. In general,they found they could address nearly all of the problems uncovered by thesystems analysis and correct those by themselves without additional resources.
(c) Supervisory support: District supervisors were trained in the use ofchecklists based on the standards. It was assumed that the supervisors wouldperform two functions: they would communicate standards and they wouldmonitor supervision of standards in the health centers. In several of the healthcenters they were permitted to perform only the first function, that ofcommunicating standards. Apparently, direct supervision of staff is often aprerogative, jealously guarded, of the health center director. The supervisors,almost none of them physicians and typically of less tenure than the clinicdirectors, encountered subtle and overt resistance to their efforts to monitorhealth worker performance. They were able to supervise long enough toprovide a model for direct observation of care, but once that model wasunderstood by the health center staff, the supervisor was displaced in that role.

Annex 14- 92 - Page 4 of 9
(d) Clinic-level activities: Within all of the health centers, a similar set ofactivities evolved to improve quality. The clinic director, a doctor, discussedthe plan of action with clinic staff and a QA team was usually formed. Some ofthese teams functioned as true quality improving teams; in other instances theirrole was limited. The director then conducted informal training on thestandards. This training was followed up by monitoring of the health workers,usually with the same checklists used by the supervisors. In most instances thehealth workers were also provided with new job aids to provide visual re-minders of the standards. In some instances these job aids were simplereproductions of the supervisory checklists, in others the director developednew aids that focused on specific deficiencies and in one instance the directorcreated innovative flow diagrams that guided the health worker throughhistory-taking, examination, classification, and treatment. In several clinicsthere were initial problems of resistance from one or more health workers.This resistance was overcome through persistent monitoring and directsupervision. All of the clinics were visited periodically by the researchers. A"circuit rider" visited each clinic approximately every ten days. Aninternational research consultant visited each of the NTB clinics two or moretimes at the start of the pilot. And two national researchers made additionalperiodic visits to the clinics. During the three-month experimental period(August - October) each clinic received a dozen or more of these drop-in visits.The frequency of these visits, necessary to monitor processes within theclinics, almost certainly affected staff behavior.
Results
8. Even the most optimistic expectations were surpassed by the results of the pilotproject (see Table 1/Annex 14). A second survey of clinical service quality was conducted inNovember 1994. The sample sizes were reduced to 12 observations for each service in aclinic; this is the minimum sample size consistent with LQAS (lot quality assurance sampling)methodology. In most areas compliance with standards reached or approached 100 percent.In all areas there was a marked improvement.
9. There was concern that the clinic staffs might not undertake quality improvementsbeyond simple adherence to standards. This concern was partly allayed by the findings. Infour of the ten clinics the staff tackled complex problems and all of the clinics took haltingsteps toward addressing client satisfaction issues. The following cases are relevant examples:
* Chloroquine resistant (p. falciparum) malaria is a growing problem in someareas of NTB. Prior to the pilot project, a clinic in an endemic area had treatednearly all malaria patients based on clinical signs since the patients wereunwilling to wait 90 minutes for the blood analysis to be completed;consequently nearly all patients were treated with chloroquine. This wasobviously an unsatisfactory situation and the clinic staff initiated a program of

Annex 1493 Page 5 of 9
aggressive counseling of patients to await the results of the slide examination.At the end of three months over 70 percent of malaria patients waited for theslide results. Fears that the increased wait might depress utilization wereunfounded as the visit rate increased slightly. The health impact of this changeon the incidence of p. falciparum malaria, which was found in the clinic to be50 percent during December, is clear. These patients now receive effectivetreatment which is fansidar and primaquine.
A clinic discovered, as it applied the standards for counseling, that patients didnot understand the messages. This discovery was followed by directobservation of the counseling session and, from this observation, changes weremade. First, awareness of the problem encouraged health workers to be moredirective and to probe for understanding. Second, where they could, healthworkers removed crying children from the room during the counseling ofmothers. A third change, group counseling, will be implemented after a specialroom for the purpose has been prepared. The results are encouraging. As anexample, nearly 100 percent of ARI patients now return for the two-daycontrol visit; formerly the return rate was less than 25 percent.
Concluding Remarks
10. The consistency of the above findings encourages several conclusions. Specifically, thefollowing lessons emerge:
(a) It is possible to get immediate and significant improvements in the quality ofbasic health services provided by government facilities, which can be achievedwith a little investment in the development and establishment of a QA program.
(b) A corollary to this lesson is that staff are quick to learn about technical qualityand need little external support to improve compliance with standards. Clinicstaff find the presence of clear standards of care reassuring. Consequently,once motivated, they develop a variety of ingenious ways to remind themselvesof the standards and improve compliance. This experience has made frontlinehealth workers realized that they are the key to solving a lot of the qualityproblems facing their facilities.
(c) A common initial perception of health staff is that they can do little to improvequality of care because of lack of resources. This resource-dependent mentalitywas quickly broken by their systems analysis and problem-solving exercises.
(d) A key to motivate staff is for high-level authorities to show that they arestrongly committed to quality improvement, and they will hold health centerdirectors accountable for establishing quality assurance mechanisms and

Annex 14-94 Page 6 of 9
practices in their facilities. In the field trial, while seven of the ten clinicdirectors moved rapidly ahead in their quality improvement efforts, the threeothers showed little or no inclination to get started. The appearance of seniorofficials in the three clinics to make polite inquiry about the progress of the QAprogram had a galvanizing effect.
11. The pilot ran for only a few months; and the durability of the improvements is not yetknown. Therefore, a caveat is needed in making these conclusions. This notwithstanding, thefact that the QA pilot performed as well as it did, and the weaknesses revealed are easy tocorrect, provides a good empirical basis for BP IV's quality assurance program. MOH is nowready to move ahead with a program that it finds suitable to Indonesia and regards as its own.
Table 1: Standards of Care Compliance Rate by Health Intervention
NTB East JavaBaseline Follow-up Change Baseline Follow-up Change
ANC 45% 86.6% +41.6 66.9% 96.4% +29.5Vacc 59.3% 86.4% +27.1 73.7% 95.6% +21.9ARI 45% 81.1% +36.1 38.75% 90.95% +52.2
Table 2: Standards of Care Compliance Rate by Clinical Activity
Baseline Follow-up Change
History taking 41.5% 92% +50.5Physical exam 56.1 90.3 +34.2Treatment 74.4 83.1 +8.7Counseling 33.5 83.1 +49.6Patient knowledge 31.1 74.1 +43

Annex 14Page 7 of 9
Table 3: Standards of Care Compliance Rate by Health In erventions and Clinical Activity
NTB East JavaAntenatal care Baseline Follow-up Change Baseline Follow-up Change
Total observations AHC 124 60 125 60Reproductive history
Review OB record 87% 95% +8 91% 100% +9Update age 95 100 +5 100 100 0Last delivery 83 98 +15 100 100 0No. prev. pregs. 95 100 +5 100 100 0Baby's condition 69 67 -2 94 100 +6Prev. complications 26 63 +37 91 97 +16Vomiting 29 80 +51 86 100 +14
Risk factorsSpotting 14 62 +46 17 97 +80Diabetes 1 87 +86 18 100 +82Lung disease 1 92 +91 36 100 +64Cardiovascular problems 2 93 +91 n/a n/aLiver problems 4 90 +86 32 100 +68Kidney problems 2 90 +88 31 100 _69Malaria history 2 93 +91 n/a n/aCurrent medications 29 50 +21 12 83 +71Smoking 0 90 +90 6 90 +84Alcohol 1 88 +87 6 90 +84
Preventive measuresTT immunization 87 100 +13 92 98 +6Malaria prophylaxis 65 90 +25 n/a n/aDelivery plans 44 93 +49 70 100 +30Who will delivcr 0 43 +43 70 98 +28Explain value HW delivery 19 93 +74 48 100 +52Explain danger signs 10 85 +75 42 98 +56Go to HC or hosp. in emerg. 15 88 +73 40 100 +60
Physical examinationMeasure height and weight 85 97 +12 100 100 0Blood pressure 100 100 0 99 100 +1Pulse 28 82 +54 99 100 +1Measure fundus 99 100 +1 100 100 0Check for edema 26 80 +54 61 100 +39Calculate due date 60 95 +35 94 98 +4
Preventivc care givenTT 99 98 -I 96 98 +2Kept vaccinc in thermos 64 100 +36 99 100 +1Iron tablet 94 100 +6 94 100 +6Explain howv take iron 94 100 +6 91 100 +9Gave malaria prophylaxis 21 92 +71 n/a n/a
CounselingExplain imporlance of ANC 35 97 +62 64 93 +29Wt. gain during pregnancy 77 95 +18 90 100 +10Dict 64 92 +28 68 90 +22Where and when next visit 83 97 _14 96 100 +4Ask if any qucstions 1 64 +63 21 83 +62
Exit InterviewTT explained 37 85 +48 45 72 +27Plan to have HW at delivery 40 65 +25 77 85 +8Knows danger signs 8 48 +48 46 83 +3Total observations, vacc. 125 60 125 60Rcviewed health record 98% 100% +2 79% 100% +21Rccomm. vacc. Even if sick 89 100 +11 100 83 -17

~ 96 - Annex 14Page 8 of 9
NTB East JavaAntenatal care Baseline Follow-up Change Baseline Follow-up Change
TechniqueSterilizer kept covered 78 100 +22 71 98 +27Used sterile needle 98 100 +2 94 100 +6Used sterile syringe 98 100 +2 82 100 +18Needle attached properly 62 81 +19 96 98 +2Load syringe w/o contam. 52 100 _48 86 100 14Vaccine on ice and closed 56 100 +44 94 100 +6Covered the thermos 62 100 _38 87 100 +13Prepared injection site 98 100 +2 96 100 +4Apply vaccine to right level 90 98 +8 98 100 +11Used good syringe 83 100 +17 99 100 +1Is needle good 70 88 +18 100 100 0Sterilizer good 89 100 +11 98 100 +2Properly dispose of syringe 44 90 +46 72 100 +28and needle
DocumentationRecord on patient's card 98 100 +2 100 100 0Record on clinic's card 98 100 +2 99 100 +1
CounselingTold pt. which vaccine 19 93 +74 85 93 +8Told side effects 50 93 +43 49 100 +51For BCG, told scab 23 57 +34 17 100 +83Where to go if reaction 21 55 +34 16 96 +80Import. to complete series 2 62 +60 12 87 +75If DPT3, remind measles 39 69 +30 61 92 +31Explain sick child can vacc. 41 78 +37 39 83 +44Tell when ncxt visit 35 76 +41 53 100 +47Ask if any questions 0 35 +35 0 70 +70
Exit interviewKnows what vacc. received 18 67 +49 70 88 +18Knows when next visit 36 64 +28 58 98 +30Says another hcalth service 23 60 +37 40 65 +25was promoted
HW InterviewKnows correct age for BCG 58 90 +32 93 100 +7Knows correct age for DPT 58 100 +42 100 100 0Knows measles age 100 100 0 100 100 0Knows correct polio age 63 100 +37 100 100 0Knows vacc. ill child 63 80 +12 60 100 +40

Annex 14- 97 - Page 9 of 9
Acute Respiratory Baseline Follow-up Change Baseline Follow-up ChangeInfections
Total observations, ARI 127 60 125 60History
Asked age of patient 98% 100% +2 99% 100% +1Coughing? 98 100 +2 94 100 +6Duration of cough 84 100 +17 83 100 17Child conscious? 3 90 _87 98 100 +2Able to drink 17 90 +87 98 100 +2History of resp. problems? 13 83 +70 9 92 +83Family history of ARLITB? 0 77 +77 1 97 +96Current medications? 17 67 +50 12 90 +78
Physical exam.General status 38 88 +50 27 100 +73Respiration rate 16 83 +67 4 97 +93Temperature 86 97 +11 40 98 +58Chest indrawing 35 83 +48 44 100 +56Stridor/wheeze 24 80 +56 44 97 +53Auscultate chest 20 30 +10 92 100 +8Exam. throat for discharge 5 53 +48 40 97 +57Exam. neck glands 2 68 +56 8 92 +84
Classify and treatClassify child 68 90 +22 16 97 +81Give antibiotic for pneum. 87 80 -7 93 100 -7Not give antib. for cold 44 83 +39 32 98 +66Medicine for fever 98 93 -5 78 98 +20Refer severe pneumonia 100 100 - nla n/aInjection 100 100 0 20 5 +15Injection done correctly 84 100 +16 70 100 +30Referred complications 29 47 +18 0 80 +80Gave correct drug 59 90 +31 7 100 +93Prescribed night dosage 67 90 +31 27 100 +73
CounselingHow administer antibiotic 52 84 +32 1 80 +79Import. complete treatment 8 87 +79 5 100 +95How to clear blocked nose 0 61 +61 2 75 +73When to stop medicine 1 67 +66 2 98 +96Give food, fluids, breast 26 78 +52 1 97 +96Maintain neutral temp. 5 82 +77 9 97 +88Tell 3 signs mod/see. ALRI 0 55 +55 2 83 +81Return if child worsens 32 82 +50 18 98 +80Any questions 0 43 +43 2 40 +38
Exit interviewKnows how to treat child 46 70 +24 30 70 +40Knows signs to return 31 37 +6 36 65 +29How to admin. medicine 93 90 -3 95 93 -2When stop medicine 23 63 +40 38 70 +32
HW knowledgeSigns/symptoms pneumon. 83 100 +17 81 100 +19Difference cold, pneumon. 83 100 +17 75 100 +25Duff. pncu. and sev. pneu. 44 100 +56 38 100 +62When give antibiotic 89 91 +2 75 100 +25Home treat cold, pneu. 28 100 +72 50 100 +50When refer to hospital 89 100 +11 100 100 0

- 98 - Annex 15
INDONESIA
FOURTH HEALTH PROJECT:IMPROVING EQUITY AND QUALITY OF CARE
Selected Documents and Data in Project Files
1. COSTABs
(a) Project expenditures summary(b) Central-level expenditures(c) Provincial-level expenditures: East Java, West Kalimantan, East Kalimantan,
NTB and West Sumatra
2. Computerized Project Management timelines
(a) Five-year summary(b) Detailed October 1995-September 1997 schedule(c) Central-level schedule of activities(d) Provincial-level schedule of activities(e) District-level schedule of activities
3 Terms of Reference
(a) Key consultants(b) Technical audit
4. Statement of Policy of MOH and Statement of Provincial Government Support
5. Provincial and Central HP IV project preparation documents
6. Reports on the Quality Assurance Pilot Project
7. Management of the Fourth Health Project

- 99 -Chart 1
Project ManagementCentral level
Intersectoral Project Director entra
Advisory Board (Secretary General) Force
Central Intersectoral Project Officer--Steering Committee (Chief, Bureau of Planning)
tecrin~~~ Executivee
Provincial Level
/ rovincial / Provincial Project: rovincial -___ -P --- rovincial Project Office - - - _
Provinca Pr Implementation OfficerSteer-Ing ComnmitteeVteenng CommitteeKa4AKANWIL) 2 l \ (Ka Dinkes Tk I)
t Officer J l t Task Force
Distsrict/Municipalitv LevelDistrict Project Officcr
-\ (Dokabu/Dokodya) --------------------[-I{caith Development r--'
Committee /
Head o the
Health Center

INDONESIAFOURTH IIEALTII PROJECT
Ministry of Health Organizational Structure
Minitru of Health
Seacetariat Genertal
l l l ' IsffXGe Aff
irrectrae a t note of Bureau or Bureau of Bureau of Bureu of nBurea of Bureu of c G Bureau ofor Pnsior of Finafe f Logistics y AfEain o Printing Pec oMel CFinae | oLogilic | | Luw Public | | Organizdion | Aft i
| Daredat Gel Directorate ODae or or o I| of ConuT Jty H¢thh l | or MedicalI Care | Cmn DseeC o| oo hD Cnto
ectirte o S Diredtorate of| Spec. Vector Boi a ot Diredo of Food
| Family Heshh| | Healhh Centcrs| loerL osphals | PCt Hospitals Infectiour Dleae |Dg Control Bev. Control
Direclorate of Directoraie of -Directorate of Directorate of |rDirectorate of ectorate of Dirctorte of Directorate ofCommninrty __ Commtunity |Dental Ieh |.& |Mealw Heh hpid A= lttuL nvir. h Unit Comm. h HRE - Trad DrugNutrition Participation Equiprr Control
:)irraie of ~~~~Dietrexte of__Center for Ed- Centtt for Redearl I WatRr Santtai n Ra.uition Dc ee ofh Training of _ _ Education of Nat Lnstit. of |Ntics Control}Ihh Petsnnel Illth. Manpowver Hhh Reserrch
Health Dia Heathh Lb. &DvlpirCenter Ctntcr
C&cfer or Hhh | Catnteof CDC | tf ||Ctnof | |C4nter of |SeoNn
| Heahh Educ. | | Ptvincisl Hetith n Ses. Rew4chr Rese rch | clg eh||PhumL ResdL | |Nutrition RefL ||D ecd
Developmenl Offioe
|Distrid Heathh|Development Ofrice
| He hth Centrie | (PUSKFSMAS) |

IBRD 26852
-^14AIAND PA nC INDONESIA
R37nds Ao.hO J 4 °PHILIPPINES U i* FOURTH HEALTH PROJECT
2 BRUN = PROJECT PROVINCES
\> SModan kMALAyslA | ttX /\ f S s PROVINCE CMEALS~~~~~~~~~~~~~~~~~~~~~~~~~D ROINC CPIAL
MALAYSIA 9, *. \ t / j / j iL Cele NATIONAL CAPITAL
MALAYSIAot \\ < / 7 S 6 e\ SOC o ./ - - INTERNATIONAL BOUNDARIES
1 2 < \ MALAYSIA ) 9 \ 4SINGAPORE 1lO 7o
P Ad jr3 1 -> t O / P on tsonokt 14 r ' Somonndc g I$¢ a / (&k cuf~9 2 N O R T H P A C IF IC O C E A N
1 SENKULUAR - . Paoolooy .C.,n > 5'
2 JSUARABRA T 25
2 JAWA UTAAI .7
4 KAMYOGYAKARA
5 AIMWANTATIMUR Rn l AlV SULAWESIllENGAH Ban v-
10 21 RanD cl UofnicSe l
7 BENGKUL.U YA SUMATERASELATAtA Ron6okJoa S h
9RIAU Ju-gn.I J AMBI tooo inpnoo ,I- od
Ii SUMATERA BAPAT '
22 W Dnw~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ooM v
1 2 SLMATE-A UTARAAART 1 3 I IACEH14 NKAUMAN BARAT V d nof FInn.t
I5 KLMALUKU 4 TENAI World~ 2=n GC=.on ugmn
9 KALMANTAN SELATA on N oar
17 IIMANTAN TIlMUR Un
er S-
A 8SUIAWESi TENGAH m
1 9SULAWEV LJTARA oobnS '
20 SULAWESI SELATAN 22 ISULAWESI TENGGAtAA22 RAL Dnoor* 22 NUSA TENGGARA BARAT Th.a b .. d.n,. cooo,do,io- , INDIAN OCEAN23 7424 NUSA TENGGABtA nMUR ;d nyoAa ,noooh.-no op
26 iRkAN JAYA AT-mp o nt mpy.on hapaS..225 MALLJ U Tha Wonl= Go1Oo.ny dr.OC
27 TIMORTIMUR nynosnnoccooco.c .,-- ASTRALIA
4/21/1993 io 24 bx u 5 Rm



IMAGING
Report No: 13991 INDType: SAP