wilson’s disease ho yin calvin chu, sanghyuk (simon) oh, soojin oh, zi teng (steven) shao phm142...
TRANSCRIPT
Wilson’s DiseaseHo Yin Calvin Chu, Sanghyuk (Simon) Oh,
Soojin Oh, Zi Teng (Steven) Shao
PHM142 Fall 2015 Instructor: Dr. Jeffrey Henderson
What is Wilson’s Disease?
• Autosomal recessive disorder of hepatic copper disposition
• Prevalence of about 30 per million in population• Early onset and late onset well documented
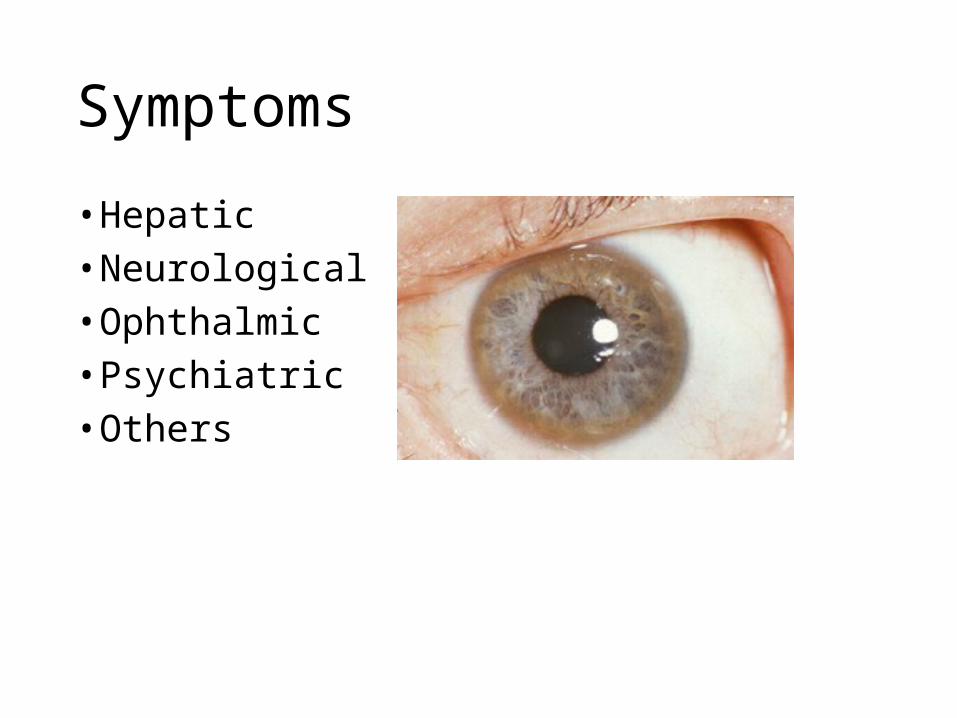
Symptoms
• Hepatic• Neurological• Ophthalmic• Psychiatric• Others
Diagnosis
• Number of methods in diagnosis
•Biochemical Findings•Genetic Screening•Kayser Fleischer Rings•Liver Biopsy•Imaging
Pathogenesis
• Chromosome 13 is responsible for Wilson’s Disease• Mutations in the ATP7B
• ATP7B is a gene responsible for producing P type ATPase
• Participates in incorporation of copper into budding ceruloplasmin
• Speeds up biliary excretion of copper
• Mutation in P type ATPase leads to copper accumulation

Pathogenesis
Brief History
• In 1956 John Walshe found that penicillamine can be used for Wilson's disease
• Found penicillamine in urine of patient who took penicillin
• Discovered penicillamine stimulates copper excretion by chelation

Chelation
• A particular way that ions and molecules bind metal ions
• Porphyrin rings in Hemoglobin is a chelating agent where it’s chelating to iron with 4 bonds
• Peniciillamine chelates excess copper from tissue and secrete it through urine

Penicillamine
D-penicillamine L-penicillamine
Pharmaceutical Drug Toxic
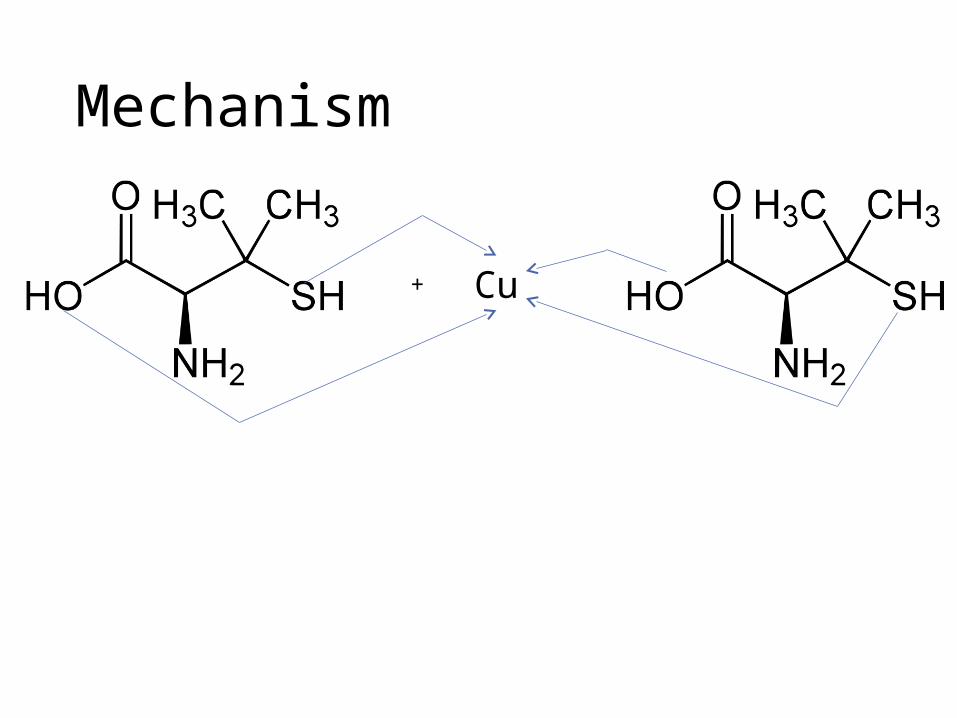
Mechanism
+ Cu
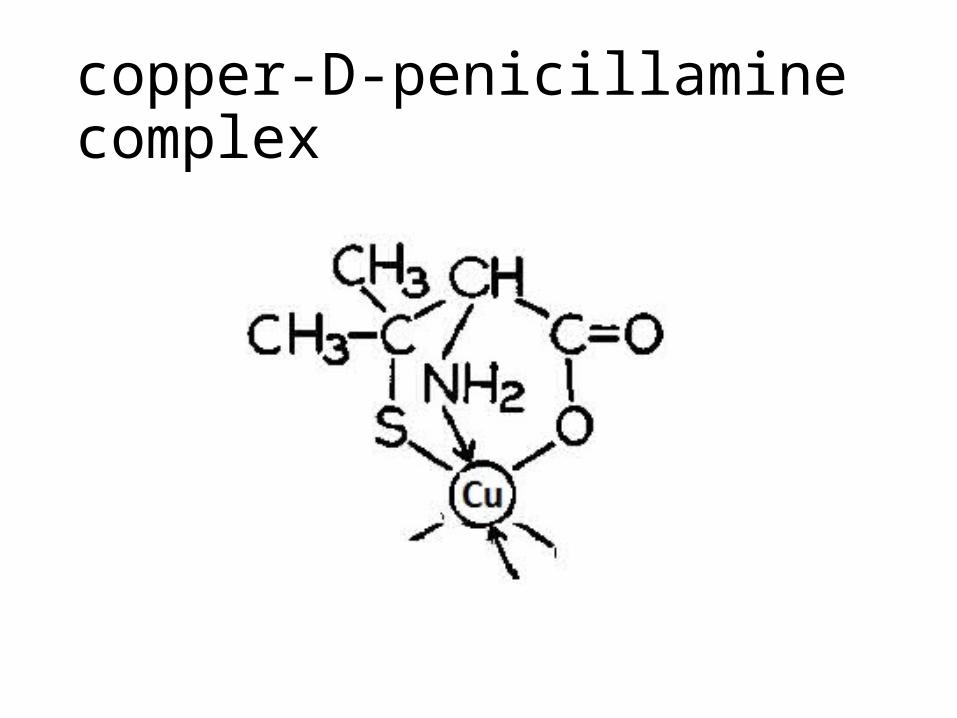
copper-D-penicillamine complex

Excretion of penicillamine
• copper-D-penicillamine complex is very stable, excreted readily through urine
• Amount of copper excreted can be measured in urine
• Based on result, dosage of penicillamine can be adjusted

Oral Zinc Therapy
• Zinc Salts (zinc acetate, zinc phosphate)• GalzinTM (zinc acetate)• Used in:
• Presymptomatic phase• Maintenance phase
• Following initial phase of aggressive decoppering using copper chelating agents
• During initial therapy: zinc therapy is less effective than chelating agents
• Toxicity is rare, preferred treatment in pregnancy • Over treatment leads to copper deficiency

Paradigm Shift
• Copper Chelating agents = “Decoppering”• Zinc Salts = “Copper Intoxication”• Copper bind to ceruloplasmin (copper carrying
protein) is non-toxic• Free bound copper in blood is toxic

Mechanism of Action
• Metallothionein• Metal-binding protein• higher affinity for dietary copper than zinc
• Zinc induces metallothionein in hepatocytes in the liver and enterocytes in the gut
• Liver:• Promote sequestration of free serum copper in a non-
toxic metallothionien-bound form
Mechanism of Action
• Intestine: • Oral zinc binds and traps metallothionein within the
mucosa• Metallothionein sequesters copper within the
enterocyte• Sequestered copper is excreted in the intestinal lumen
as the enterocytes are sloughed• Excretion via the stools

Drug Interactions• Penicillamine
• Chelating agent that targets both copper and zinc• Decreased effect with zinc therapy
• Solution• Avoid using penicillamine and zinc together • Penicillamine as initial treatment• Zinc as maintenance treatment

Management Therapy
Anti-copper Therapy •Diet •Vitamin E
Future Directions
• Liver transplant• Restores liver function• Normal copper excretion
• Gene therapy
• Wilson’s disease is mutation in the gene ATP7B which affects production of P-type ATPase.
• P-type ATPase is responsible for copper excretion and incorporation of copper into ceruloplasmin
• Peniciillamine chelates excess copper from tissue and secrete it through urine
• Copper-D-penicillamine complex is stable and therefore it can be secreted readily, amount of copper excreted can be measured in urine
• Oral zinc therapy is used in presymptomatic and maintenance phase• There is a paradigm shift from decoppering to copper intoxication as bound
copper is intoxic• Zinc salts induces metallothionein, a metal-binding protein, in enterocytes
and hepatocytes, which renders copper intoxic • Method of therapy management has to be carefully monitored in order to
avoid a potential drug interaction• Even after initial treatment, maintenance therapy is needed for
symptomatic treatment and to keep copper levels low
Summary

References• Ala, A., Walker, A. P., Ashkan, K., Dooley, J. S., & Schilsky, M. L. (2007). Wilson’s disease. The
Lancet, 369(9559), 397–408. http://doi.org/10.1016/S0140-6736(07)60196-2• Bandmann, O., Weiss, K. H., & Kaler, S. G. (2015). Wilson’s disease and other neurological
copper disorders. Lancet Neurol, 14(1), 103–113. http://doi.org/10.1016/S1474-4422(14)70190-5
• Brewer, G. J. (2013). Movement Disorder Emergencies, 305–318. http://doi.org/10.1007/978-1-60761-835-5
• Brewer, G. J., & Askari, F. K. (2005). Wilson’s disease: clinical management and therapy. Journal of Hepatology, 42(1), S13–S21. http://doi.org/10.1016/j.jhep.2004.11.013
• Dalvi, A., & Padmanaban, M. (2014). Wilson’s disease: Etiology, diagnosis, and treatment. Disease-a-Month, 60(9), 450–459. http://doi.org/10.1016/j.disamonth.2014.07.002
• European Association for Study of, L. (2012). EASL Clinical Practice Guidelines: Wilson’s disease. J Hepatol, 56(3), 671–685. http://doi.org/10.1016/j.jhep.2011.11.007
• Hoogenraad, T. U. (2006). Paradigm shift in treatment of Wilson’s disease: Zinc therapy now treatment of choice. Brain and Development, 28(3), 141–146. http://doi.org/10.1016/j.braindev.2005.08.008
• Roberts, E. A. (2011). Wilson’s disease. Medicine, 39(10), 602–604. http://doi.org/10.1016/j.mpmed.2011.08.006
• Schilsky, M. L. (2014). Liver transplantation for Wilson’s disease. Annals of the New York Academy of Sciences, 1315(1), 45–49. http://doi.org/10.1111/nyas.12454