what is the most efficient immunotherapy to epstein-barr ... target … · and pathogensis? mtc,...
TRANSCRIPT

Ernberg 2016
Ingemar Ernberg Riga
May 2016 !!
Dept of Microbiology, Tumor and Cell Biology (MTC)!
What is the most efficient immunotherapy
to Epstein-Barr virus infection?

Ernberg 2016
Control and disruption!of EBV latent infection!
Latently infected B cell! Tumor!Lymphoma (+ mutation in !cellular genes)!Infection of wrong cell type?!CD4 T -helper 1 & 2!
Cytokines!Hormones!T regs; NK!
Host genetics!
CD8 CTLs!Immunosuppression!
Viral activity!Other infections!
Prevention/vaccination or Immunotherapy
Why? Who? When? How?

My points
EBV & infection in vivo
Vaccine?
Tumors High risk: transplant pat:s (& HIV-
carriers)
T-cell therapy

Ernberg 2016
Epstein-Barr virus!
Murray PG and Young LS (2001)
The paradoxes! EveryBodies Virus!!! Most common virus in the human
population (>90% of all adults, life long persistence)!
! Tumor-associated virus!
80% of carriers secrete biologically active virus (saliva)!
Very efficient in immortalizing B-cells!

Stability!A sutibable vaccine target
50+ complete DNA-sequences
Two major types: type I=type A and type II=type B (98 % homology)
Subtypes ill-defined: a chinese?, deletions in critical genes (LMP 1)
Variants: appr = familiar isolates (recombination between large repeats in latency genes)
EBV(s) has(ve) adapted over millions of years to a very successfull life within the immune
system.
The viral strategy for survival, latency and spread in the population has evolved numerous mechanisms to master this
challenging situation.
EBV-associated tumors are a rare trade off of this normally balanced virus-host
interaction

Ernberg 2016
Proliferation of EBV !activated blasts!
Latent reservoir of EBV !
CTL!
T cell mediated control of !proliferation CD8, CD4!!, others?!
oropharyngeal epithelium!
Ag?!
Infection of !circulating B cells!
IgA?!Corresponds!To neuronal!Axon of neurotropic!Herpesvirus!
Virus replication in !
EBV life cycle in vivo !
infected resting B cells!

Ernberg 2016
Control of the latency-switch, !latency I to III and reverse!
Latency III!Latency I! Tumor cell!?

Ernberg 2016
Model system for transformation in vitro !§ HBV/HCV -!§ HPV ! ! (+)!§ EBV ++!§ HHV 8/KSHV ! ! -!§ HTLV +!
§ H.Pylori ! ! -!§ Parasites (liver fluke,! Shistsomiasis) -!!

Latency in vivo
One infected B-lymphocyte/
100ul-10 ml of blood (0,1-10/100.000 B-cells)
5000 infected cells in blood in a healthy carrier (+ X in lymphoid
system) Increases 100-10.000-fold in high
risk groups MTC, Karolinska Institute, Sweden. Ernberg, 2010
Host-virus interaction & diseases!
Childhood infection subclinical
Primary infection > 5 yrs 35% risk of infectious mononucleosis (“an acute autoimmune syndrome”)
In immunosuppressed: (Fatal/Chronic) lymphoproliferative syndrome
Lymphomas, epithelial cancers as a result of accidents of the host-virus interaction

To think about
Most biologically active EBV on earth is swallowed with the saliva.
300-500 ml/day, appr 500 infectious units entering the GI every day in
80% of humans. “Part of the normal flora”
Role in infection, immune boosting, and pathogensis?
MTC, Karolinska Institute, Sweden. Ernberg, 2010

Ernberg 2016
Infectious agents Number of new tumors annually & globally
!§ HBV/HCV 500,000!§ HPV! ! ! 450.000!§ EBV 200.000!§ HHV 8/KSHV 45.000!§ HIV ! 10.000!§ HTLV ! ! 2.200!
§ H.Pylori ! 460,000!§ Cl.psitacci, Borrelia! burgdorfei, ! Campylobacter jejenum 500?!§ Parasites (liver fluke,! Shistsomiasis) 11,000 ! !

Ernberg 2016
EBV-associated tumors!in man!
Epithelial tissues!!Oral hairy leukoplakia 100%!!Gastric adenocarcinoma 5-10%!!Nasopharyngeal carcinoma,!undifferentiated 100%!!Salivary gland carcinomas <100%!!Smooth muscle tissue!!Leiomyosarcoma in!immunosuppressed 100%!
Lymphoid tissues!!Burkitt´s lymphoma, endemic 98%!!Burkitt´s lymphoma, sporadic 30%!!AIDS-immunoblastic lymphoma 30%!-in CNS 100%!!Post-transplant lymphoma 100%!!Hodgkin´s lymphoma 50%!!T-cell lymphomas 10-30%!--lethal midline granuloma >90%!!Primary effusion lymphomas >90%!

Ernberg 2016
EBV-associated tumors!in man!
Epithelial tissues!!Oral hairy leukoplakia 100%!!Gastric adenocarcinoma 5-10%!!Nasopharyngeal carcinoma,!undifferentiated 100%!!Salivary gland carcinomas <100%!!Smooth muscle tissue!!Leiomyosarcoma in!immunosuppressed 100%!
Lymphoid tissues!!Burkitt´s lymphoma, endemic 98%!!Burkitt´s lymphoma, sporadic 30%!!AIDS-immunoblastic lymphoma 30%!-in CNS 100%!!Post-transplant lymphoma 100%!!Hodgkin´s lymphoma 50%!!T-cell lymphomas 10-30%!--lethal midline granuloma >90%!!Primary effusion lymphomas >90%!

HD!
BL !TCL!NPC!
Geographic distribution of !EB virus-associated tumors!
IBL, Transpl ., AIDS (CNS) lymphomas!
NPC!
AIDS lymphomas!

u Conventional cancertherapy u Anti-viral drugs: spec DNA-polymerase inhibitors
(acyclovir etc.) clears replication but not latent infection. Effect on lymphoproliferative syndrome
u Bone marrow transplantation can clear out the whole EBV-infection including latency
u Therapeutic vaccines
u Adoptive transfer of EBV-specific cytotoxic T-lymphocytes (CTL) reeducated in vitro
(Check point-blockers PD1/CTLA4)
EBV - therapeutic strategies!
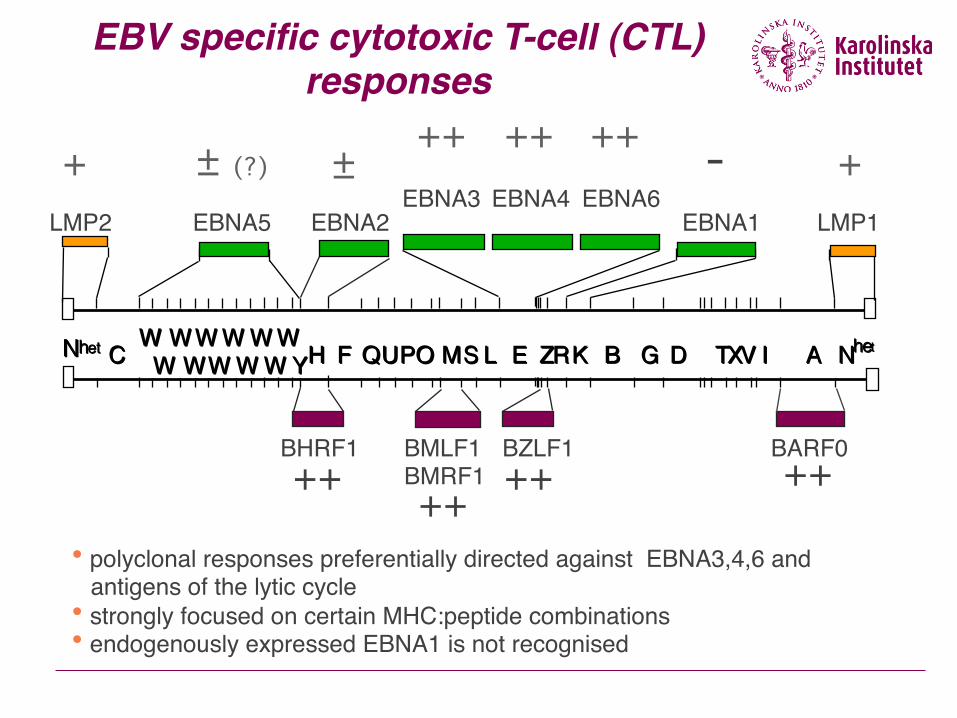
EBV specific cytotoxic T-cell (CTL) responses!
• polyclonal responses preferentially directed against EBNA3,4,6 and ! antigens of the lytic cycle!• strongly focused on certain MHC:peptide combinations!• endogenously expressed EBNA1 is not recognised!
++!
EBNA3!EBNA5! EBNA2!
W!W!W!W!W!W!W!W!W!W!W!W!Z!Z!W!W!W!W!W!W!W!W!W!W!C!C! Y!Y!H!H! F!F!Q!Q!U!U!P!P!O!O!M!M!S!S!L!L! E!E! R!R!K!K! B!B! D!D! T!T!X!X!V!V!I!I! A!A!G!G! N!N!h!h!e!e!t!t!N!N!h!h!e!e!t!t!
EBNA6!EBNA1!LMP2!
EBNA4!LMP1!
+! ± (?)! ±!++! ++! ++! -! +!
BZLF1!BMLF1!BMRF1!
BHRF1!++! ++!
BARF0!++!
Antibodies are efficiently neutralizing infection (anti-gp 350; anti-MA)
Antibodies + complement/LAK-cells eliminate virus replicating cells
Earlier dogma: Cytotoxic T-lymphocytes are instrumental in controlling the life-long latency (Masucci, Rickinson, Moss)
Recent discovery: CD4 cells producíng specific cytokines (IL21) control the latent infection (Nagy, Kis, Klein; KI)
Components of !immunity to EBV!

Receptors
B-cells: C3d (CR2)-receptor, CD 21 MHC Class II (co-receptor)
Epithelial cells: MHC Class II
Unorthodox mechanisms
Virus envelope receptor: gp 350/220

EBV vaccine!Primary preventive
Recombinant gp350, major envelope glycoprotein,
receptor binding, neutralizing epitope (prevents lymphomasin monkey models)
To be used when, where and how? Risk groups for NPC, EBV-negative adolescents (IM)

Therapeutic “Polytope”, several MHC Class I epitopes combined in a vaccinia-vector based vaccine (D.Moss et al)
Peptide-loaded dendritic cells (NPC; A.Rickinson et al)
Adoptive cytotoxic T-cell transfer (C.Rooney; M.Masucci et al)
Recombinant gp350, major envelope glycoprotein, receptor binding, neutralizing epitope (therapeutic in post-transplants?; A.Morgan et al +CRC, UK)
CTL modulation combined with demethylation (Rich Ambinder et al.)?
EBV vaccines….!

Ernberg 2016
Groups with high risk for EBV positive lymphomas
!§ Bone-marrow/HSC transplanted pat:s (with
minor mismatch)!§ HIV-carriers (before HAART; 15-20 % CNS
lymphomas)!
§ Children with chronic malaria!
§ Immunodisregulation+Chronic antigen stimulation!

Ernberg 2016
W!W!W!W!W!W!W!W!W!W!W! Z!C! Y!H!F!Q!U!P!O!M!S!L!E! R!K!B! D! TXV!I! A!G! N!het!N!het!
Qp!Q! U!
Proliferation-rest is regulated by viral! expression programs in latency!
W1/!2!W0!
EBNA5 !
UY1/2/3!
EBNA2 !
EBNA1 !
EBNA6 !EBNA4 !
EBNA3 !
Cp!Wp!
C1/2!
Latency I!0-4 genes!Resting!
Latency III!12 genes!Proliferation!
EBER 1&2!
Cell proliferation!

Ernberg 2016
Incidence of post-transplant lymphoproliferative disease (PTLD) depending on type of
transplant § Kidney 1 %!§ Liver 2 %!§ Heart 3 %!§ Lung 1 – 8 %!§ Heart and lung 9 %!§ Intestine 7 – 11 %!§ Multivisceral 13 – 33 %!§ BMT 1 % (up to 30 %)!

Ernberg 2016
Risk factors for post-transplant lymphoproliferative disease (PTLD)
§ Mismatched, unrelated stem cell grafts § Primary immune deficiency § T-cell depletion techniques which do not
concomitantly reduce the B-cell content § Use of anti-T-cell antibodies ( ATG, OKT-3 ) § Heavy immune suppression § High levels of circulating EBV-infected cells * § EBV-seronegative recipient § CMV infection / Young age ?/ GVHD treatment

Ernberg 2016
EBV-DNA load and relapse in EBV-associated lymphoma (HIV-infected patient)

Increased EBV load in patients receiving T-cell depleted BMT!
2!1!0!1!8!9!1!6!8!1!4!7!1!2!6!1!0!5!8!4!6!3!4!2!2!1!0!-!2!1!
0!1!2!3!4!5!6! 2!3!1! 2!5!2! 2!7!3! 2!9!4!
*!
Patient 4!
EBV
load
! [l
og c
ells
con
tain
ing
1 EB
V ge
nom
e]!
Days post transplant!
Maximal EBV load recorded in BMT recipients !with high or low risk of PTLD!
Donor !Type of BM graft Maximal EBV load Days post BMT!
(genomes/106 cells) ! !!High risk patients JBa TCD 1,250 31 UH TCD 6,250 129, 149, 366 PL TCD 31,250 53, 63 OL TCD 31,250 49, 125 RG TCD 156,250 42, 52 GL TCD 31,250 80 HSa U 156,250 80 mean±SE 59107±25963 Median 31250 Low risk patients !MU U 50 34 !NJ U 250 51, 62 !SG U 1250 62, 79, 93 !RT U 50 95 !EE U 1250 55 !PZ U 1250 335 !LS U 250 13, 27, 53, 62, 73, 81
!GS U 1250 67 !mean±SE 700±269 Median 750
Several log-fold increase of EBV-load post-BMT…!!…. related to T-cell depletion of graft!!….only latency 1 & 2 (restricted, non-proliferating in blood)!

EBV specific cytotoxic T-cell (CTL) responses!
• polyclonal responses preferentially directed against EBNA3,4,6 and ! antigens of the lytic cycle!• strongly focused on certain MHC:peptide combinations!• endogenously expressed EBNA1 is not recognised!
++!
EBNA3!EBNA5! EBNA2!
W!W!W!W!W!W!W!W!W!W!W!W!Z!Z!W!W!W!W!W!W!W!W!W!W!C!C! Y!Y!H!H! F!F!Q!Q!U!U!P!P!O!O!M!M!S!S!L!L! E!E! R!R!K!K! B!B! D!D! T!T!X!X!V!V!I!I! A!A!G!G! N!N!h!h!e!e!t!t!N!N!h!h!e!e!t!t!
EBNA6!EBNA1!LMP2!
EBNA4!LMP1!
+! ± (?)! ±!++! ++! ++! -! +!
BZLF1!BMLF1!BMRF1!
BHRF1!++! ++!
BARF0!++!

Early administration of EBV-CTLs prevents the increase of EBV load!
5!
0!1!2!3!4!
315!
CSA
ser
um le
vels
!(n
g/m
l) x1
0!
Patient 5!
210!189!168!147!126!105!84!63!42!21!0!-21!
EBV-CTLs!GVHD II!
0!
1!
2!
3!
4!
5!
6!
EBV load!CSA !
231! 252! 273! 294!
*! *!*!
EBV
load
[log
]!
Days post transplant!

Ernberg 2016
Study of ”EBV” at transplant unit of Karolinska University Hospital South (Huddinge)
Question Can we identify better tools for PTLD risk prediction at individual patients level? T cell phenotyping on EBV-related immune reconstitution (tetramers, FCM) Cohort Entered so far: 350 adults & 50 children entered (open) Sampled 1,2,3,6, 12 and 24 months > transplantation Colaborators Markus Maeurer, Olle Ringdén, Johan Matsson, Jacek Winiarski,

Ernberg 2016
EBV DNA load over time: TWO patterns
Type I TypeII
0
10
0 1 2 3 4 5 6 7 8 9 10 11 12 EBV/
1000
cell
month(M)
ADULT 6 EBV/1000cell
0
100
0 1 2 3 4 5 6 7 8 9 10 11 12 EBV/
1000
cell
month(M)
ADULT 17
0
100
0 1 2 3 4 5 6 7 8 9 10 11 12 EBV/
1000
cell
month(M)
ADULT 19
0
100
0 1 2 3 4 5 6 7 8 9 10 11 12 EBV/
1000
cell
month(M)
ADULT 7
0,0
10,0
1 2 3 4 5 6 7 8 9 10 11 12
ADULT 31
l
0
10
20
30
1 2 3 4 5 6 7 8 9 10 11 12
EBV/
1000
cell
month(M)
ADULT 12
0
20
40
0 1 2 3 4 5 6 7 8 9 10 11 12
EBV/
1000
cell
month(M)
ADULT 16
0 5 10 15 20 25
1 2 3 4 5 6 7 8 9 10 11 12
EBV/
1000
cell
month(M)
ADULT 18
0,0
50,0
1 2 3 4 5 6 7 8 9 10 11 12
ADULT 20 E
BV
/100
0cel
l
0,00
10,00
20,00
1900/01/01 1900/01/02 1900/01/03 1900/01/04
CHILD 2
0,00
50,00
100,00
150,00
200,00
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
CHILD 3

Ernberg 2016
0
20
40
60
80
100
CD3+,Freq. of Parent, 1m CD3+,Freq. of Parent, 2m CD3+,Freq. of Parent, 3m CD3+,Freq. of Parent, 6m CD3+,Freq. of Parent, 12m
6
16
19
20
B2
B7
B8
0
20
40
60
80
100
1 2 3 6 12
1
2
3
5
B5
0
20
40
60
80
100
CD3+,Freq. of Parent, 1m
CD3+,Freq. of Parent, 2m
CD3+,Freq. of Parent, 3m
CD3+,Freq. of Parent, 6m
CD3+,Freq. of Parent, 12m
7
17
Fraction CD3+ cells
Intermediate Low High

Ernberg 2016
0 10 20 30 40 50 60 70 80
CD4-CD8- T cells
0
20
40
60
80
100
1 2 3 6 12
0
20
40
60
80
100
Intermediate Low High

0 365 730 1095 1460 1825
Days after HSCT
0,0
0,2
0,4
0,6
0,8
1,0C
umul
ativ
e Pr
opor
tion
Surv
ivin
g0 RF n=7, 100%
1 RF n=18, 83%
2 RF n=21, 81%
3 Risk factors: High/low EBV load+ total body irradiation + GVHD III-IV n=5, 0%

Ernberg 2016
Concluding remarks
Target population for vaccination against EBV not identified; efficient vaccine exist (rec gp350); duration of protection not known Normalization of EBV load in risk groups depends on functional immunereconstitution (cART; post-BMT) Adoptive (EBV-specific) T-cell therapy prevents PTLD and cures some lymphomas (post HSCT) New possibilities: check point inhibitors, CD4, interleukins (IL21?) Extreme low or high EBV load in blood (B-cell bound) post-BMT/HSCT poor prognosis. With aGCVD & TBI predicts (100%) failure

Collaborators Huddinge Transplantation & Pediatric clinic Jacek Winiarski Olle Ringdén CTL work Maria Masucci, CMB Teresa Frisan, CMB Viktor Levitsky, CMB EBV Jie-Zhi Zou, MTC HIV Anna Friis Börje Åkerlund T-cell phenoptyping Nalini Vudattu, SMI &MTC Markus Maeurer, SMI & MTC
Members; now and recent Andrey Alexeyenko Rozina Caridhe Sun Di Nguyen van Do Ziming Du Anna Friis Elvira Grigorieva Sven Grüzmier LiFu Hu Qin Li Liudmila Matskova Tore Midtvedt Imran Nawaz Elisabeth Norin Jian-Yong Shao Anders Wennborg Xiao Xue Jie-Zhi Zou Xiaoying Zou