volume 27 • number 8 in this issue - acep sso service · volume 27 • number 8 august 2013...
TRANSCRIPT

Volume 27 • Number 8
August
2013
ContributorsAdam D. Marks, MD, MPH, and Andrew R. Barnosky, DO, MPH, FACEP, wrote “Care of Adult Hospice Patients in the Emergency Department.” Dr. Marks is a clinical lecturer in the Division of Geriatric and Palliative Medicine, Department of Internal Medicine, at the University of Michigan Health System, in Ann Arbor, Michigan. Dr. Barnosky is an associate professor of emergency medicine and medical education, and director of Clinical Ethics Consultation Service at the University of Michigan Health System, in Ann Arbor.
George L. Sternbach, MD, FACEP, reviewed “Care of Adult Hospice Patients in the Emergency Department.” Dr. Sternbach is a clinical professor of surgery at Stanford University Medical Center in Stanford, California, and an emergency physician at Seton Medical Center in Daly City, California.
Anand K. Swaminathan, MD, MPH, and Jonathan van de Leuv, MD, wrote “Tourniquets versus Topical Hemostatic Agents in Hemorrhagic Trauma.” Dr. Swaminathan is an assistant professor of emergency medicine at NYU/Bellevue Emergency Medicine Department in New York, New York. Dr. van de Leuv is a resident at NYU/Bellevue Emergency Medicine Department in New York.
Daniel A. Handel, MD, MPH, FACEP, reviewed “Tourniquets versus Topical Hemostatic Agents in Hemorrhagic Trauma.” Dr. Handel is vice chair and director of Clinical Operations, and an associate professor in the Department of Emergency Medicine at Oregon Health & Science University, Portland, Oregon.
Frank LoVecchio, DO, MPH, FACEP, reviewed the questions for these lessons. Dr. LoVecchio is research director at the Maricopa Medical Center Emergency Medicine Program and medical director of the Banner Poison Control Center, Phoenix, Arizona, and a professor at Midwestern University/Arizona College of Osteopathic Medicine in Glendale, Arizona.
Louis G. Graff IV, MD, FACEP, is Editor-in-Chief of Critical Decisions. Dr. Graff is professor of traumatology and emergency medicine at the University of Connecticut School of Medicine in Farmington, Connecticut.Contributor Disclosures. In accordance with the ACCME Standards for Commercial Support and policy of the American College of Emergency Physicians, all individuals with control over CME content (including but not limited to staff, planners, reviewers, and authors) must disclose whether or not they have any relevant financial relationship(s) to learners prior to the start of the activity. These individuals have indicated that they have a relationship which, in the context of their involvement in the CME activity, could be perceived by some as a real or apparent conflict of interest (eg, ownership of stock, grants, honoraria, or consulting fees), but these individuals do not consider that it will influence the CME activity. Sharon E. Mace, MD, FACEP; Masimo, consulting fees; Gebauer, contracted research, non-CME services; Baxter, contracted research; Luitpold, contracted research. Joshua S. Broder, MD, FACEP; GlaxoSmithKline; his wife is employed by GlaxoSmithKline as a research organic chemist. All remaining individuals with control over CME content have no significant financial interests or relationships to disclose.Method of Participation. This educational activity consists of two lessons with a posttest, evaluation questions, and a pretest; it should take approximately 5 hours to complete. To complete this educational activity as designed, the participant should, in order, take the pretest (posted online following the previous month’s posttest), review the learning objectives, read the lessons as published in the print or online version, and then complete the online posttest and evaluation questions. Release date August 1, 2013. Expiration date July 31, 2016.Accreditation Statement. The American College of Emergency Physicians is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The American College of Emergency Physicians designates this enduring material for a maximum of 5 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Each issue of Critical Decisions in Emergency Medicine is approved by ACEP for a maximum of 5 ACEP Category I credits. Approved by the AOA for 5 Category 2-B credits. A minimum score of 75% is required.Commercial Support. There was no commercial support for this CME activity.Target Audience. This educational activity has been developed for emergency physicians.
■ Also in This Issue ∙ The LLSA Literature
Review / Page 9 ∙ The Critical Image
/ Page 19 ∙ The Critical ECG
/ Page 20 ∙ CME Questions
/ Page 21 ∙ The Drug Box / Page 24
■ Next Month ∙ Hernias ∙ Nontraumatic Hip Pain
In This IssueLesson 15 Care of Adult Hospice Patients in the Emergency Department. . Page 2
Every year, large numbers of patients enrolled in hospice seek care in an emergency department for reasons ranging from uncontrolled symptoms to caregiver fatigue. Emergency physicians must be able to manage these often complex situations, including being able to navigate complex goals-of-care discussions and provide empathetic care for patients at the end of life.
Lesson 16 Tourniquets versus Topical Hemostatic Agents in Hemorrhagic Trauma . . . . . . . . . . . . . . . . . . . . . . Page 11
Hemorrhagic shock with continued bleeding is a common scenario in modern emergency departments. Tourniquets have been used for more than a millennium to control bleeding but are not effective or safe for all patients. Recent advances in topical clotting agents offer an innovative and possibly more effective modality to control major hemorrhage.

Critical Decisions in Emergency Medicine
2
■ ObjectivesOn completion of this lesson, you should be able to:
1. Explain the role and scope of hospice care for patients with terminal disease.
2. Describe the role that emergency care plays in hospice care.
3. Identify common triggers that cause a patient enrolled in hospice to seek care in the emergency department.
4. Explain a step-wise approach to management of a hospice patient in the emergency department.
5. Demonstrate the components of effective communication when leading focused goals-of-care discussions.
6. Identify the hospice enrollment criteria for common conditions such as debility and cardiovascular, pulmonary, and oncologic diagnoses.
■ From the EM Model20.0 Other Core Competencies of the Practice of Emergency Medicine 20.4 Systems-based Practice
Adam D. Marks, MD, MPH, and Andrew R. Barnosky, DO, MPH, FACEP
Care of Adult Hospice Patients in the Emergency DepartmentLesson 15
The term “hospice” refers to a philosophy of care that is dedicated to maximizing comfort and quality of life for people approaching the end of life. The modern model of hospice care in the United State is relatively young, having started in 1974 when the first hospice program opened in Bradford, Connecticut. Since then, hospice programs have proliferated to more than 4,500 nationwide, caring for over 1.3 million patients. Today, more than 40% of all deaths in the United States occur in the context of hospice care. Although most hospice patients are cared for in the home, hospice care can also be delivered to patients in a variety of settings, including inpatient hospice facilities, skilled-nursing facilities, and acute-care hospitals.
Patients qualify for hospice care if they are deemed, based on their diagnosis and disease burden, to have less than 6 months to live and opt for a comfort-focused plan of care (Table 1). Typically, these patients and their families have made the decision to forgo disease-specific treatments such as chemotherapy, although treatments aimed at relief of symptoms such as palliative radiation to a painful bony metastasis may still be pursued. The specific treatments that a patient may be allowed vary from hospice agency to hospice agency; in general, interventions are permissible if they are indicated for the relief of suffering or for symptom management.
Although studies have shown that enrollment in hospice decreases the likelihood that a patient will seek care in an emergency department, roughly 3% of hospice patients will present to an emergency department for acute care.1 Nationwide, this equates to tens of thousands of hospice patients visiting emergency departments for care. Furthermore, upwards of 60% of patients will present to emergency departments in the last months of life. For these reasons, emergency physicians should feel comfortable not only with managing patients receiving hospice services, but also with knowing what situations warrant referring a patient to a hospice agency for care.
Case Presentations
■ Case OneA 64-year-old man with a history of metastatic mesothelioma who has been
receiving hospice services at home for the past 2 months comes to the emergency department because of increasing shortness of breath. His disease course has been complicated by a recurrent right-sided pleural effusion that has been managed by repeated thoracenteses, typically needed once per week. On the day prior to presentation, the hospice physician performed a thoracentesis but was unable to remove any fluid. A followup chest radiograph showed an unchanged moderate-to-large fluid collection on the right. In the past 24 hours, the patient has developed worsening shortness of breath not relieved with oxygen or morphine for dyspnea.
On physical examination, his vital signs are blood pressure 152/72, pulse
August 2013 • Volume 27 • Number 8
3
• What services can hospice provide to patients and families faced with a terminal diagnosis?
• What common triggers lead a hospice patient to seek care in the emergency department?
• How should hospice patients be managed while in the emergency department?
• How can goals of care be rapidly assessed in the emergency department?
• What criteria exist for determining hospice eligibility?
Critical Decisions
rate 118, respiratory rate 32, temperature 37.3°C (99.2°F), and oxygen saturation 88% on 6 liters of oxygen via nasal cannula (3 liters is his baseline). He is overweight and appears pale. Head and neck examinations are unremarkable. Lung examination reveals absent breath sounds on the right, with clear breath sounds on the left. The patient is tachypneic and using accessory muscles to breath. The right chest is dull to percussion, with increased egophony compared to the left. His cardiovascular examination reveals tachycardia without murmurs; his pulse is strong. His abdomen is obese, nontender and nondistended, with positive bowel sounds.
Transfer paperwork reveals that he was transported by ambulance at his own request, and that his code status is “do not attempt resuscitation” (DNAR).
■ Case TwoAn 84-year-old man with known
gastric carcinoma who has been enrolled in hospice for the past 4 months presents with severe abdominal bloating, pain, and vomiting. He is accompanied by his
wife who aids in the history. One year ago, the patient was diagnosed with a gastric cancer. Extensive discussions were held with him, his wife, and his children. At that time, he opted to forgo therapy and focus on quality of life. He has remained very functional, independent in his activities of daily living, and enrolled in hospice for symptom control, mostly consisting of abdominal pain. He was doing well until the day of presentation when he developed nausea, vomiting, abdominal distention, and worsening pain. He has not had a bowel movement or passed gas in the past 24 hours.
On physical examination, the patient’s vital signs are blood pressure 178/82, pulse rate 102, respiratory rate 22, temperature 37.1°C (98.9°F), and oxygen saturation 98% on room air. He is a thin man and is in acute distress, with retching during the examination productive of yellow-green fluid. Examination is remarkable for a distended abdomen tympanitic to percussion, diffusely tender, with high-pitching bowel sounds.
Transfer paperwork reveals that he was brought in by ambulance at his own request, and that his code status is DNAR.
■ Case ThreeA 92-year-old woman with
Alzheimer dementia is brought in after suffering a fall. She lives with her daughter, who relates a several-month history of declining health, characterized by decreased functional status, decreased oral intake with associated weight loss, and repeated
hospitalizations for a variety of medical problems, including urinary tract infections, dehydration, and falls. During your interview, the daughter makes it very clear she does not want her mother to undergo any invasive or intrusive testing, and provides documentation indicating that she is her mother’s medical durable power of attorney for health care (DPOA-HC). The daughter indicates that her mother’s code status is DNAR.
On physical examination, the patient’s vital signs are blood pressure 142/68, pulse rate 98, respiratory rate 18, temperature 36.4°C (97.5°F), and oxygen saturation 95% on room air. She is confused but in no acute distress. Head and neck examinations are unremarkable with the exception of mild temporal wasting. Lung examination reveals regular work of breathing with clear breath sounds bilaterally. Her cardiovascular examination reveals regular rhythm without murmurs and strong radial pulses. Her abdomen is soft, nontender, and nondistended. She has some bruising along her right flank but minimal tenderness. Examination of her extremities, including hips, shows no pain with passive range of motion. Neurologic examination reveals that she is alert and orientated to person only, which per the daughter is her baseline; otherwise the examination is nonfocal.
As you finish your examination, the patient’s daughter states that she no longer feels able to care for her mother in her home without assistance.
Table 1.Hospice-appropriate patients
Diagnosis and disease burden consistent with end of life
Prognosis of less than 6 months
Comfort-focused plan of care
Treatments for relief of suffering and symptom management

Critical Decisions in Emergency Medicine
4
CRITICAL DECISIONWhat services can hospice provide to patients and families faced with a terminal diagnosis?
Hospice services are designed to be delivered to a variety of locations. For almost 70% of enrollees, this care is delivered to the place of residence.2 Other common locations where hospice services are provided include nursing homes, hospitals, and hospice residences. When a patient enrolls in home hospice, much of the care is delivered at home and can include home visits from physicians, nurses, social workers, chaplains, health aides, and volunteers; hospice staff are on call 24 hours a day, seven days a week. Hospice provides not only skilled care in the home but also all medications deemed appropriate by the hospice medical director; durable medical equipment such as a hospital bed, bedside commode, or wheelchair; and any medical supplies required for patient care, such as gloves, wipes, and bandages. In addition, hospice staff often are able to perform certain procedures for comfort, such as paracentesis for abdominal distention or thoracentesis for a pleural effusion causing dyspnea. After a patient’s death, bereavement support is offered to the family or other involved parties and can include support groups and one-on-one counseling.
In general, although hospice can bring a great deal of care to the patient, the bulk of caregiving falls on the family or other support system caring for the patient. When making a decision about where a patient should reside when enrolling in hospice, a frank conversation is required about what a family can or cannot provide for the patient because many patients who approach the end of life need frequent if not 24-hour care.
CRITICAL DECISIONWhat common triggers lead a hospice patient to seek care in the emergency department?
Emergency physicians should not assume that arrival in the
emergency department implies a desire for aggressive or life-prolonging therapy; even when the patient or family requests such care, a careful assessment is needed to understand the underlying reason behind such a shift in care goals. Several studies have been done looking at why patients enrolled in hospice come to the emergency department to seek care. The most common reasons are, as follows:
∙ Poor symptom control (ie, acute pain crisis, dyspnea, etc.)
∙ Malfunction/loss of a support device, such as a gastrostomy or nephrostomy tube
∙ Failure of the hospice program to provide timely patient support and communication
∙ Stress/inability to cope with impending loss of life, often expressed as a request to start a life-prolonging treatment previously used and discontinued (ie, chemotherapy) or never begun (ie, dialysis).3
Poor Symptom ControlAs patients approach the end
of life, their symptom burden often becomes dynamic, at times overwhelming the ability of families or other care givers to manage. Despite the fact that patients who receive hospice services have telephone access to hospice providers 24 hours a day, the “learned behavior” of calling EMS services may be an automatic response to perceived distress. Common symptoms that trigger such a visit include pain, dyspnea, agitation, and/or decreased oral intake leading to dehydration.3
For hospice patients presenting with poor symptom control, efforts should focus on aggressive symptom control. This can include limited evaluation for reversible causes (ie, urinalysis for the elderly hospice patient presenting with worsening agitation) as well as procedures or even surgeries aimed at relief of symptoms. These can range from therapeutic thoracentesis/paracentesis to venting gastrostomy tubes for
malignant small bowel obstructions to surgical repair of a fractured hip. As in all cases, the potential benefits should be weighed against the risks and put into the context of the patients’ goals of care.
Malfunction/Loss of a Support Device
With the advances in and increased availability of excellent medical care, more people are living with medical devices such as feeding tubes, nephrostomy tubes, or indwelling intravenous lines. As these patients continue their decline, hospice staff are called on to care for such patients, and at times these devices fail, necessitating an emergency department evaluation. As in the case of therapeutic procedures mentioned above, the emergency physician should enter into frank conversations with the patient and/or family about whether an intervention is warranted in the name of relief of symptoms. For example, a peripherally inserted central catheter that comes out may not need replacement in a patient who can tolerate oral medications, while a suprapubic catheter almost always needs to be replaced to prevent painful bladder distention.
Failure of the Hospice Program to Provide Timely Patient Support and Communication
As previously mentioned, most hospice patients are cared for in the home and rely on visiting nurses and other support staff to aid in their care. The response time for a visiting nurse or other health care professional to reach a patient in the home, especially for those patients residing in rural areas, can be excessive when a patient is in distress. Likewise, if a patient or family is not properly prepared for what to expect during the dying process, they are more likely to experience panic or distress when common symptoms such as restlessness, terminal congestion, or apneas develop. This distress can often be preemptively addressed by appropriate and thoughtful education.

August 2013 • Volume 27 • Number 8
5
Stress/Inability to Cope with Impending Loss of Life
Although hospice agencies provide significant support, the bulk of care often falls on a patient’s family in the home. As the end of life approaches, the inherent uncertainty and ambiguity of the situation can cause caregiver distress leading to a visit to the emergency department. In these situations, caregivers should be screened for distress and their ongoing ability to care for the patient. As in all scenarios, if the family member cannot or will not be able to care for the patient at home, alternative placement should be arranged, either in a hospice facility or in the hospital itself.
CRITICAL DECISIONHow should hospice patients be managed while in the emergency department?
A great deal of literature has been generated about the general steps that an emergency physician should take when managing a hospice patient. Although there are no formal guidelines, a number of sources recommend the following steps:
1. Notify the hospice agency caring for the patient. This is most relevant for the patient or family who has bypassed the hospice team to seek emergency care. Under the Medicare hospice benefit, hospice agencies are still responsible for the patient’s plan of care and all medical costs incurred during the emergency department stay.
2. Determine the trigger. See above. Involve social work, chaplaincy personnel, or palliative care consulting services as needed (and as available) to treat any psychosocial or existential distress.
3. Treat distressing symptoms. Given that poor symptom control is a major reason hospice patients arrive in the emergency department, prompt and aggressive treatment of
symptoms should be a priority.4. Assess goals. This is especially
relevant in the patient for whom deterioration is imminent and decisions are needed about the use of life-sustaining treatments. See below for suggestions on how to complete a rapid goals-of-care discussion.
5. Thoughtful use of tests/interventions. Decisions about testing and interventions should be based on patient-defined goals of care. Broadly speaking, low burden and noninvasive testing to reveal reversible causes of distress (ie, urinalysis to diagnosis UTI) should be used first. Interventions should again be based on the patient’s goals of care rather than automatic emergency department practices (ie, antibiotics for pneumonia should only be used if they meet a patient’s or surrogate’s goals of
care).6. Plan disposition. This decision
should be made after a patient has been stabilized and in conjunction with the hospice agency, the patient/family, and emergency department staff and again should be based on the patient’s goals. Returning home or direct admission to an inpatient hospice facility may be preferable to admission to the hospital. Factors affecting this decision include the level of care needed, the family’s ability to provide care in the home, and patient preferences.
7. Notify appropriate parties. Once a final plan is made, the hospice agency should be notified of any changes in the patient’s medications, treatment plan, or goals of care. If the patient is admitted to the hospital, the palliative care consultant (if available) should
Table 2.Components of effective communication. Adapted from: McPhee SJ, Winker MA, Rabow MW, et al. Care at the Close of Life: Evidence and Experience. McGraw-Hill: New York, NY; 2011. Used with permission.
Establish trust/encourage families to talk
“Tell me what you understand of your illness.”
“I’m sure this illness has been a lot to absorb quickly. How are you coping with this?”
“You just mentioned being scared. Can you tell me more about what scares you most?”
Respect
“I’m impressed that with everything you’ve gone through, you’re thinking of your family.”
“I can tell that through all of this, you’ve been a strong advocate for your father.”
Support
“I want to reassure you that no matter what the road holds ahead, we will continue to offer the best care we can to ensure your comfort.”
Hope
“I know that you are hoping your disease will be cured. Are there other things you want to focus on?”
“I wish, too, that this disease would stay in remission. If we cannot make that happen, what other goals might we work towards?”
Attend to affect
“Is talking about these issues difficult for you?”
“Of course talking about this makes you feel sad. It wouldn’t be normal if it didn’t.”

Critical Decisions in Emergency Medicine
6
be contacted to continue to support the patient and family during admission.4
CRITICAL DECISIONHow can goals of care be rapidly assessed in the emergency department?
Not all hospice patients coming to an emergency department require a formal family meeting or goals-of-care assessment; however, emergency physicians should be comfortable leading a rapid evaluation of goals of care for those patients who express ambivalence or uncertainty about their wishes for continued aggressive care. Several general steps can be undertaken to facilitate such an assessment in a timely manner. At all stages, the key elements of effective communication should be used5 (Table 2).
Before starting the assessment, the emergency physician should review the patient’s medical situation, either with existing medical records or, if these are not available, by discussing the patient’s case with the hospice team. This review should include the patient’s diagnosis, treatments undergone, potential therapies available, any pertinent documents (advance directives, DNAR forms, living wills, etc.), and any relevant psychosocial information such as surrogate decision makers and family dynamics that may affect decision making. If needed, the patient’s primary care provider or subspecialist (ie, oncologist) can be contacted to aid in the gathering of information.
When possible, the discussion should occur in a quiet area with minimal interruptions. This may be difficult given the noise and activity inherent in most emergency departments; however, every effort should be made to have a focused discussion without disruptions.
Begin the meeting with introductions if this has not already been done, after which the meeting leader should determine from the patient (or surrogate) what they know about their disease. This can
allow the clinician to confirm what is already known or to provide new information and/or correct any misperceptions. As much as possible, avoid medical jargon and use “bottom line” statements, such as “is not going to get better” or “is getting worse.” The provider should be prepared for questions about prognosis (ie, “How long do I have left?”) or what to expect as the patient progresses to end of life.
Once a common understanding of diagnosis and prognosis is reached, the conversation can be broadened to include goals of care going forward. This can typically start with hope/fear questions to encourage a patient or surrogate to talk and can be focused to discuss specific modalities that might be considered such as artificial hydration/nutrition, dialysis, etc. The following is an example of hope/fear questions in a goals-of-care conversation:
We have discussed your current condition, and we know that your time may be short.
∙ Given that, what are you hoping for now?
∙ What is important to you? ∙ What are you afraid of when
you think about the future?The answers to these questions
can allow the emergency physician to make recommendations based on a patient’s or surrogate’s wishes. For example, if a patient or surrogate expresses a desire to avoid coming back and forth to the hospital or expresses a fear of dependence or suffering at the end of life, the emergency physician should feel comfortable recommending a palliative or comfort-based approach to care including continued hospice care. If, on the other hand, a patient or surrogate expresses a desire for continued medical treatment, the physician should feel comfortable recommending a plan of care that would include hospital admission and further evaluation by the appropriate subspecialists. At the end of the meeting, the physician should summarize the goals as discussed,
plans for care going forward, and invite any remaining questions from the patient or family members.
The conversations outlined above are more often than not fraught with emotion, and conflict (between patient and family, opposing family members, family and medical team) is common. As available, the emergency physician should feel comfortable calling on a palliative care consultant to aid in difficult or time-sensitive communication.
CRITICAL DECISIONWhat criteria exist for determining hospice eligibility?
As mentioned above, a patient qualifies for hospice services if, based on the expected course of a terminal diagnosis, the patient has an expected prognosis of 6 months to live or less. To assist physicians in determining prognosis and initiate a hospice referral, the National Hospice and Palliative Care Organization (NHPCO) has developed guidelines for many cancer and noncancer conditions (Table 3). It should be noted that these rules are meant as general guidelines and not strict criteria; at all times, a clinician’s judgment should be used when determining prognosis. When a referral is made to a hospice organization, the case is reviewed by the medical director for that agency. If the medical director agrees that the patient qualifies, then the patient is enrolled and begins receiving hospice services; if the director disagrees, then the patient’s enrollment is denied.
Of particular interest for emergency physicians is the “debility” criteria that refer to a chronically ill patient for whom no single terminal diagnosis can be identified (Table 3). These criteria denote patients who have had a decline in functional and nutritional status and have accelerating health care needs as evidenced by repeated hospitalizations or emergency department visits that are not due to a reversible cause. Case Three depicts a case that could meet hospice criteria

August 2013 • Volume 27 • Number 8
7
under a debility diagnosis based on the reported loss of functional status, weight loss, and need for repeated emergency department evaluation. Other information that could support a hospice referral would be a serum albumin level below 2.5, repeated falls, and decubitus ulcers that
progress despite aggressive medical management.
Case Resolutions
■ Case OneIn the case of the apneic patient
with metastatic mesothelioma, after discussions with the family, patient,
and hospice agency, the decision was made to admit the patient to the hospital overnight for management of his dyspnea. His narcotic medication doses were adjusted, and an ultrasound-guided thoracentesis resulted in the removal of 1.5 L of fluid and significant symptom
Table 3.Hospice enrollment criteria6
General guidelines
Progression of life-limiting condition as documented by:
∙ Multiple/recurrent hospitalizations or emergency department visits
∙ Decline in functional status, increased dependence in activities of daily living (dressing, bathing, grooming, etc.)
∙ Impaired nutritional status: weight loss of more than 10% in the preceding 6 months, serum albumin level below 2.5 g/L
∙ Disease-specific markers: physical examination, laboratory tests, previous imaging
Disease-specific guidelines
Oncologic Disease with distant metastases at presentation or progression from an earlier stage of disease to metastatic disease with either a continued decline in spite of therapy or patient refusal for further disease-directed therapy
Cardiac NYHA class IV symptoms (symptoms at rest despite optimal medical therapy)
Ejection fraction less than 20% is helpful but not required
The following factors help predict increased mortality: symptomatic supraventricular tachycardia, previous cardiac arrest, unexplained syncope, cardiogenic shock
Pulmonary Dyspnea at rest despite optimal medical therapy
Oxygen-dependent at rest
Cor pulmonale or right-sided heart failure due to pulmonary disease
Hypercapnia (Paco2 >50 mm Hg)
Resting tachycardia
Dementia Patients with all of the following characteristics
∙ FAST stage 7a or beyond
∙ Unable to ambulate, dress, or bathe without assistance
∙ Urinary and fecal incontinence, intermittent or constant
∙ Verbal communication limited to six or fewer words
∙ Presence of comorbid conditions associated with decreased survival such as aspiration, pyelonephritis, septicemia, or pressure ulcers
∙ Nutritional impairment, characterized by decreased oral intake, weight loss of more than 10% in the preceding 6 months, or serum albumin less than 2.5 g/L
Renal Creatinine clearance less than 15 mL/min and serum creatinine above 8
Signs or symptoms of uremia
Persistent hyperkalemia
Intractable fluid overload
Not receiving dialysis or refusing dialysis
Debility In the absence of other terminal diagnoses, a patient over the age of 65 may qualify for hospice under debility criteria if the following criteria are met:
∙ Decreasing weight more than 10% over the past 6 months
∙ Albumin less than 2.5, with a decrease over the past 6 months
∙ Loss of functional status, including increasing need for assistance with activities of daily living
∙ Dysphagia leading to recurrent aspiration or chronic inadequate nutritional intake
∙ Progressive pressure ulcers despite appropriate nursing and wound care
∙ Increasing need for emergency visits or hospitalizations related to the chronic medical conditions (CHF, COPD, etc.)

Critical Decisions in Emergency Medicine
8
improvement. At the recommendation of the inpatient palliative care consulting team, interventional radiology was consulted for placement of a pigtail catheter in the pleural space, which allowed for continuous drainage of his fluid collection. With this in place, the patient was discharged home with hospice care where he died several weeks later.
■ Case TwoIn the case of the elderly man with
gastric carcinoma and abdominal pain, emergency department imaging revealed invasion of the known gastric carcinoma into the splenic flexure, resulting in a malignant small bowel obstruction. After discussion with the family and patient, the patient was admitted to the hospital for management of his symptom crisis, which included placement of a nasogastric tube to suction, initiation of a morphine infusion, and scheduled octreotide and antiemetics, including dexamethasone. With these measures, the patient’s symptoms improved significantly and he was able to rest comfortably and participate in goals-of-care
discussions. Surgery was consulted and offered placement of a venting gastrostomy tube, which was declined by the patient as he was tolerating his nasogastric tube without significant discomfort. Prior to the patient’s discharge, his hospice agency was contacted and arranged for him to be transferred home with home suction and morphine infusion, where he died peacefully several days later.
■ Case ThreeIn the case of the elderly woman
with Alzheimer dementia, after discussion with the patient’s daughter, a limited evaluation was undertaken including urinalysis, CBC, and basic metabolic panel. These tests revealed evidence of mild dehydration but were otherwise unremarkable. With the help of social work, a focused goals-of-care discussion was held with the patient, her daughter, and an out-of-state sibling who was able to participate by phone. Based on the stated goals of maximizing comfort and minimizing medical interventions, the emergency provider recommended enrollment in hospice under debility criteria,
which the family agreed to. A local hospice agency was contacted and arrangements were made for a hospice nurse to meet the family at home the following day to enroll the patient into hospice care.
Summary Patients enrolled in hospice
programs are occasionally transported to the emergency department for care. Because emergency physicians are predominantly focused on life-prolonging measures and the diagnosis of life-threatening diseases, a hospice patient can present a unique set of diagnostic, therapeutic, and ethical challenges. In addition, although emergency physicians may feel that a direct hospice referral from the emergency department is the best disposition in caring for patients with life-limiting illnesses, many remain ambivalent about making a referral directly from the emergency department. This lesson presents practical pointers to add clarity to these difficult clinical decisions.
References1. McNamara D. ED utilization high during last months of
life. ACEP News. 2010. Available at: http://www.acep.org/Clinical---Practice-Management/ED-Utilization-High-During-Last-Months-of-Life/. Accessed January 8, 2012.
2. NHPCO Facts and Figures: Hospice Care in America. 2012 Edition. Alexandria, VA: National Hospice and Palliative Care Organization; 2012:6. Available at: http://www.nhpco.org/sites/default/files/public/Statistics_Research/2012_Facts_Figures.pdf. Accessed February 27, 2013.
3. Wallace EM, Walsh J, Conroy M, et al. Why do palliative care patients present to the emergency department? Avoidable or unavoidable? Am J Hosp Palliat Care. 2012;6:1-4.
4. Lamba S, Quest TE, Weissman DE. Emergency department management of hospice patients. Fast facts and concepts #246. Available at: http://www.eperc.mcw.edu/EPERC/FastFactsIndex/ff_246.htm. Accessed January 8, 2012.
5. McPhee SJ, Winker MA, Rabow MW, et al. Care at the Close of Life: Evidence and Experience. McGraw-Hill: New York, NY; 2011.
6. National Hospice Organization Standards and Accreditation Committee Medical Guidelines Task Force. Medical guidelines for determining prognosis in selected non-cancer disease. Hosp J. 1996;11(2):47-63.
Pearls• Hospice patients present to the emergency department for a variety of
reasons including symptom control, device failure, and existential distress.
• If the goals of care have changed, a focused goals-of-care discussion using the elements of effective communication can help elucidate the patient’s or surrogate’s wishes.
• Coordination of care with a patient’s hospice agency can reduce misunderstandings and streamline the management of such patients in the emergency department.
• Hospice criteria exist for specific diseases that can guide clinicians in recognizing when a patient may qualify for hospice services.
Pitfalls• Assuming that a patient enrolled in hospice care who
presents to the emergency department wants to revoke hospice care and pursue aggressive care.
• Assuming that because patients are enrolled in hospice can they would not want a surgery or procedure that may add to comfort.
• Believing that emergency physicians cannot place a hospice referral.

August 2013 • Volume 27 • Number 8
9
The LLSA Literature Review“The LLSA Literature Review” summarizes articles from ABEM’s “2014 Lifelong Learning and Self-Assessment Reading List.” These articles are available online in the ACEP LLSA Resource Center (www.acep.org/llsa) and on the ABEM Web site.
Article 4
Preoxygenation and Prevention of Desaturation during Emergency Airway ManagementReviewed by J. Stephen Bohan, MD, MS, FACEP; Harvard Affiliated Emergency Medicine Residency; Brigham and Women’s Hospital
Weingart S, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012;59:165-175.
This review article sets a number of questions and provides literature-based answers about the process of preoxygenation for emergency intubation. It notes that a subject breathing room air will desaturate in 45 to 60 seconds between administration of medications and airway placement.
This period can be extended substantially if the fraction of inspired air is 90% to 100% oxygen. Masks commonly used in the emergency department, erroneously termed “nonrebreathers” and set at 15 L, deliver only 60% to 70% oxygen. Turning the gauge up to the limit beyond 15 L achieves a higher fraction.
Adding positive pressure in the air delivery apparatus substantially increased the amount of oxygen delivered and should be used in those who with impairments that prevent them from achieving an oxygen saturation of 93%.
Patient positioning is important; positioning the patient with the head elevated substantially increases the time to desaturation. Those immobilized for cervical spine precautions may be placed in Trendelenburg position. Whichever of the above positions is chosen, the patient’s external auditory meatus should be in the same horizontal plane as the sternal notch, thus maximizing airway dimensions. Nasal airways can provide additional increases in airway dimensions.
Regarding the choice of paralytic, rocuronium may provide a longer duration of safe apnea than succinylcholine.
Highlights ∙ Figure 3 (below) from the article summarizes the steps that
enhance oxygen delivery and thus prolong the period of safe apnea. Used with permission.
Sequence of Preoxygenation and Prevention of Desaturation (Assuming 2 oxygen regulators*)
Preoxygenation Period
∙ Position the patient in a semi-recumbent position (~20°) or in reverse Trendelenburg. Position the patient’s head in the ear-to-sternal-notch position using padding if necessary.
∙ Place a nasal cannula in the patient’s nares. Do not hook the nasal cannula to oxygen regulator.
∙ Place patient on a non-rebreather mask at the maximal flow allowed by the oxygen regulator (at least 15 L/min, but many allow a much greater uncalibrated flow).
∙ If patient is not saturating >90%, remove face mask and switch to noninvasive CPAP by using ventilator, noninvasive ventilation machine, commercial CPAP device, or BVM with PEEP valve attached. Titrate between 5-15 cm H2O of PEEP to achieve an oxygen saturation >98%. Consider this step in patients saturating 91%-95%.
∙ Allow patient to breathe at tidal volume for 3 minutes or ask the patient to perform 8 maximal exhalations and inhalations.
∙ Attach a BVM to oxygen regulator and set it to maximal flow (at least 15 L/min). If the patient required CPAP for preoxygenation, attach a PEEP valve to the BVM set at the patient’s current CPAP level.
Apneic Period
∙ Push sedative and paralytic (preferably rocuronium, if the patient is at risk for rapid desaturation).
∙ Detach face mask from the oxygen regulator and attach the nasal cannula. Drop the flow rate to 15 L/min.
∙ Remove the face mask from the patient.
∙ Performa a jaw thrust to maintain pharyngeal patency.
∙ If the patient is high risk (required CPAP for preoxygenation), consider leaving on the CPAP during the apneic period or providing 4-6 ventilations with the BVM with a PEEP valve attached. Maintain a two-hand mask seal during the entire apneic period to maintain the CPAP.
Intubation Period
∙ Leave the nasal cannula on throughout the airway management period to maintain apneic oxygenation.
*If three regulators are available, attach reservoir face mask, BVM, and nasal cannula to them. If only one regulator is available, consider using a stand-alone oxygen tank to offer a second source of oxygen.

Critical Decisions in Emergency Medicine
10

August 2013 • Volume 27 • Number 8
11
■ ObjectivesOn completion of this lesson, you should be able to:
1. Discuss the application technique for tourniquets and their advantages in controlling hemorrhage.
2. Describe the types of hemostatic agents currently available and their mechanisms of action in stopping hemorrhage.
3. Explain the limitations of and the complications associated with the use of tourniquets.
4. Explain the limitations of and the complications associated with the use of topical hemostatic agents.
5. Discuss the role of topical hemostatic agents in military situations and the application of this technology in noncombat settings.
6. Describe future research directions for topical hemostatic agents.
■ From the EM Model19.0 Procedures and Skills Integral to the Practice of Emergency Medicine 19.4 Diagnostic and Therapeutic Procedures
Anand K. Swaminathan MD, MPH, and Jonathan van de Leuv, MD
Tourniquets versus Topical Hemostatic Agents in Hemorrhagic TraumaLesson 16
“The fate of the wounded lies with those who apply the first dressing.”
—Colonel Nicholas Senn (1844–1908)
The first recorded use of a tourniquet was by a Roman surgeon in the second century ad. A millennium and a half later, Jean-Louis Petit, a French physician, coined the term tourniquet to describe a device he used for hemostasis during surgical procedures. The creation of the pneumatic tourniquet by Harvey Cushing in 1904 represented a vital adjunct to extremity surgery as it allowed for improved identification of anatomical structures and decreased bleeding in surgery. The tourniquet is also extensively used in combat and civilian emergency settings as a stop-gap for extremity hemorrhage.
Despite the widespread use of tourniquets in emergency trauma settings, uncontrolled hemorrhage remains a leading cause of death in both military and civilian trauma patients.1,2 Significant blood loss leads to an increased risk of hypothermia, acidosis, and coagulopathy, as well as sepsis, multisystem organ failure, and death.3 Combat studies from Vietnam estimate that 10% of deaths were due to uncontrolled extremity trauma.4 More recent analyses of data from Afghanistan and Iraq suggest that 24% of casualties could have been avoided and 85% of these were the result of hemorrhage.5 How much of this excess mortality is due to improper tourniquet placement versus
failure of a properly placed tourniquet to stop bleeding is unclear. The literature underscores the need for a better understanding of hemorrhage control and expansion of treatment options. Emergency physicians should have a fundamental knowledge of the indications for and appropriate application of tourniquets.
Enter topical hemostatic agents. In the past 10 years, researchers have dedicated extensive efforts to creating agents that can rapidly stop severe bleeding that fails to respond to standard treatment. Hemostatic agents come in a variety of forms and applications. They could have an important role in the control of hemorrhage that is not amenable to tourniquet placement (ie, neck, trunk). Although frontline military medical personnel have extensive experience with these agents, they remain infrequently used in civilian hospitals. With the data and literature on these agents expanding, it is only logical that they will proliferate in trauma rooms and emergency departments. As topical hemostatic agents become more widely available, emergency physicians will face the challenge of deciding when to apply these agents rather than traditional tourniquets. An understanding of the various hemostatic agents, the physiology behind their activity, and their strengths and limitations is vital in the management of major hemorrhage.

Critical Decisions in Emergency Medicine
12
∙ How should a tourniquet be applied to a bleeding extremity in the prehospital or emergency department setting?
∙ After successful application of a tourniquet, what continuing management is necessary?
∙ What topical hemostatic agents are currently available and how are they applied?
∙ For which types of wounds should topical hemostatic agents be considered in the treatment of active hemorrhage?
Critical Decisions
Case Presentations
■ Case OneA 24-year-old man is brought in by
EMS after being found at the scene of a motor vehicle collision. The patient’s left arm was crushed in the accident, and he complains of severe pain in that limb. The patient states he cannot feel his first three fingers or make a fist. The EMTs state that there was significant bleeding at the scene; they applied a pressure dressing en route.
On examination, the patient is in pain but fully responsive. He is afebrile with blood pressure 145/95, heart rate 90, respiratory rate 20, and oxygen saturation 99%. The upper left extremity is bandaged with multiple layers of blood-soaked gauze. Removal of the dressing reveals a tattered, deep laceration to the forearm just distal to the elbow. The wound continues to bleed profusely, limiting exploration for a bleeding source. The patient’s airway, respiratory, and cardiac examinations reveal no concerning signs, and the abdominal examination is benign. The patient is unable to flex his fingers on the affected arm and has no sensation over the first three digits. There is no evidence of significant head trauma or other disability on secondary examination. Surgery is consulted and reports that they cannot fully evaluate the wound until the local bleeding is controlled.
■ Case TwoA 37-year-old man with a gunshot
wound is brought in by EMS. The patient states that he was hunting when a friend who was some distance away accidentally shot him in the
left upper leg with a shotgun. The patient complains of bleeding and pain in the leg. A dressing was applied with manual pressure at the scene; however, EMTs had difficulty controlling the bleeding secondary to the location of the wound.
The patient’s vital signs are blood pressure 90/55, pulse rate 110, and respiratory rate 15; he is afebrile. On examination, a blood-soaked gauze dressing is removed to reveal a persistently bleeding wound in the inguinal crease. The heart and lung examinations are normal. The abdomen is soft and nondistended. Secondary examination reveals no other injury, and sensation and motor strength are intact to all extremities. Two large-bore intravenous lines are placed, and uncross-matched blood is hung on the rapid infuser. The trauma surgeon and the emergency physician unsuccessfully attempt to place a tourniquet to control the hemorrhage. The patient now complains of feeling lightheaded and appears pale. Repeat blood pressure is 60 by palpation.
■ Case ThreeFlight paramedics call to report
that they are bringing in a 43-year-old woman who fell while rock-climbing. She sustained a large, deep laceration to her left leg, which was profusely bleeding. Her climbing partner used a rope as a makeshift tourniquet to control hemorrhage from the wound. It took the climbers 4 hours to reach a road and flight medics an additional hour to reach the patient and bring her in.
Her vital signs during transport are blood pressure 85/55, heart rate 130, respiratory rate 26, and oxygen
saturation 95%. The flight crew removed the rope and found a large defect in the popliteal fossae with massive, pulsatile bleeding. They were unable to stop the bleeding with manual pressure and placed a standard pneumatic tourniquet; direct pressure was held while they initiated resuscitation.
On arrival at the emergency department, the patient’s blood pressure is 100/60 with a heart rate of 115. She is awake and complains of pain in the left lower extremity as well as numbness. Her head is atraumatic except for some minor abrasions, her chest is clear, her abdomen is nontender, and her pelvis is stable. The patient’s leg is pale, and the emergency physician has difficulty palpating a dorsalis pedis or posterior tibialis pulse. Capillary refill is delayed. Removal of the tourniquet is accompanied by a return of strong distal pulses as well as brisk hemorrhage.
Two units of packed red blood cells (PRBCs) are hung, and blood is sent for the usual trauma panel. The trauma team reports that they are with another critically injured patient, and it will be another hour before a second surgical team can be there. Although the patient’s vital signs are improving with therapy, the emergency physician is concerned about ongoing ischemic injury to her leg.
Hemorrhage and Tourniquets
After brain injury, hemorrhage is the second leading cause of death among trauma victims.1 Hemorrhage

August 2013 • Volume 27 • Number 8
13
causes a well-described progression of hemodynamic changes that occur as the body attempts to compensate for blood loss. The progression of hemorrhage has been divided into four classes to help clinicians identify the severity of blood loss. In class III and IV hemorrhage, significant blood loss leads to hypotension and tachycardia, which further leads to organ hypoperfusion. Due to the morbidity and mortality associated with this process, control of hemorrhage represents one of the central aspects of trauma resuscitation. Frequently, this requires a trauma surgeon and an operating suite but, in the case of extremity trauma, the emergency physician has a vital piece of equipment at his disposal: the tourniquet.
A tourniquet is any circumferential, constricting or compressing device used to control venous and arterial circulation in an extremity. The device applies pressure to the skin that is transmitted to the underlying tissue and structures. The transmitted pressure leads to progressive occlusion of both veins and arteries. Once the pressure applied by the tourniquet exceeds the pressure within the vessel, the vessel is occluded and blood flow is terminated. The pressure required to completely occlude a vessel depends on both the type of vessel (vein versus artery) and the patient’s blood pressure.
Tourniquets are most frequently used to occlude venous flow prior to peripheral venous cannulation for diagnostic serum testing and intravenous infusion of fluids and medications. Additionally, their utility in controlling extremity hemorrhage has been recognized for over two millennia. Tourniquet application in traumatic hemorrhage is widely recognized as a life- and possibly limb-saving intervention. A thorough understanding of these devices is critical in trauma resuscitation.
CRITICAL DECISIONHow should a tourniquet be applied to a bleeding extremity in the prehospital or emergency department setting?
The decision to apply a tourniquet can save lives. Reviews from battlefield trauma have found that the use of tourniquets in patients with significant extremity bleeding can increase survival.2-5 Healthcare providers must use caution, however, in the choice of size, style, and dimensions of the tourniquet, as well as the location of tourniquet application. These aspects have been demonstrated to significantly alter the efficacy of the device and quality of care.
Before applying a tourniquet, hemorrhage control with direct manual pressure and pressure dressings should be attempted. Pressure dressings have been demonstrated to stop moderate bleeding in most cases and stop profuse bleeding in a majority of cases.6 A tourniquet is indicated for hemorrhage in which direct pressure to the wound has failed or is not possible.
Tourniquets are only effective when applied to extremities. The function of a tourniquet relies on occlusion of arterial flow upstream from the injury. Therefore if flow to any aspect of the wound cannot be compressed proximally, the tourniquet is less likely to be effective.2,7 Care must be taken to apply the tourniquet proximally to wound location and not over any part of the wound. Hemorrhage from junctional anatomic regions (ie, axilla, groin) is notoriously difficult to control with pressure dressings and tourniquets, and the use of tourniquets in these regions is contraindicated.8 Care should also be taken to avoid placing lower extremity tourniquets over the adductor canal (Hunter canal), as decreased efficacy of the tourniquet has been documented with this placement.2 This canal carries the femoral artery, vein, and nerve and is located on the
medial aspect of the distal third of the thigh. Tourniquet effectiveness decreases with limb circumference, with efficacy rates of 100%, 92%, 81%, and 73% for the leg, forearm, arm, and thigh respectively.2,9 Tourniquets should never be placed over joints or any obvious deformities.
The next decision that providers must make is what kind of tourniquet to use. The preponderance of evidence suggests that wider devices are better.2,7,10 The two types of tourniquets most commonly used in the civilian and military setting are a windlass style tourniquet and a pneumatic style. The windlass style is a strap that is tightened by winding a rod (windlass). It is 1.5 inches wide. The pneumatic style tourniquet is inflated in a manner similar to a blood pressure cuff. It has a width of 3.5 inches.11 In a review of application of tourniquets from the Iraq war, a pneumatic tourniquet was effective 92% of the time. A windlass-style product was effective in 79% of patients. Efficacy at halting blood flow decreased further with use of makeshift and alternative tourniquets, with a 67% effective rate for devices such as cravats, windlasses, string, and intravenous tubing.2 The pneumatic tourniquet should be inflated to the minimum pressure necessary to stop active hemorrhage. A professionally made tourniquet is always preferable to an improvised tourniquet, as improvised tourniquets tend to have sharp edges and apply pressure unevenly, decreasing efficacy and increasing the risk of tissue injury.7 In the event that the initial tourniquet is ineffective, two side-by-side tourniquets should be applied. This maneuver increased efficacy by 34% in one study.2
CRITICAL DECISIONAfter successful application of a tourniquet, what continuing management is necessary?
Successful application of a tourniquet leading to cessation of active hemorrhage from an extremity represents a temporizing measure

Critical Decisions in Emergency Medicine
14
in a patient’s management. It is essential that the patient be moved to definitive care as rapidly as possible. A tourniquet should not be left in place for more than 2 hours. Whereas tourniquets in place for 1 hour or less have been shown to be relatively safe, those left in place longer than 2 hours have detrimental effects. Lactate, potassium, and creatine phosphokinase can accumulate, and on release of the tourniquet these substances can enter into circulation and can cause organ dysfunction, including renal failure (from creatinine phosphokinase) and lethal arrhythmias (from potassium). Additionally, prolonged use increases the risk of tourniquet palsy, post-tourniquet syndrome, gangrene, and the need for amputation.2,7,12,13
Tourniquets in place for longer than 3 hours are associated with amputation rates between 62% to 80%; those left in place longer than 6 hours almost always necessitate amputation of the limb.2,14,15
Tourniquets left in place for prolonged periods of time in the prehospital setting, without rapid transport to definitive care, have historically led to the aforementioned complications. The American Heart Association and National Association for EMS Physicians warn against routine tourniquet use, stating that they are only to be used as a last resort; the tourniquet has been referred to as “an instrument of the
Devil that sometimes saves a life.”7,16,17
The initial provider placing the tourniquet must clearly document the time of application and place a tag noting the time in a prominent location. Care must be taken at transfer of care to convey the presence of the tourniquet and length of time it has been in place. The tourniquet should never be covered as this can conceal its use. Some advocates recommend instructing a conscious patient to remind all new providers of the tourniquet.7 In the event of prolonged tourniquet use, 30-minute intervals of tourniquet deflation have been shown to reduce risk of complications; however, the utility of this in patients with known hemorrhage has not been evaluated.12
If definitive care is delayed and the tourniquet cannot be removed without resumption of brisk bleeding, the tourniquet should remain in place, and the risk of loss of limb should be accepted in order to save the patient’s life.
Topical Hemostatic AgentsAlthough tourniquets continue to
have a central role in management of traumatic bleeding, ongoing combat operations in the Middle East have led to increased efforts to improve hemorrhage control. A recent review of combat deaths showed that 24% of combat deaths were preventable, and that a third of those deaths were from compressible hemorrhage.18 A similar civilian study also demonstrated
that most deaths from extremity hemorrhage may be preventable by early control of bleeding.19 As a result of these observations, research and development have resulted in the introduction of a number of new topical hemostatic agents over the past 20 years.
CRITICAL DECISIONWhat topical hemostatic agents are currently available and how are they applied?
The hemostatic dressings currently available work by enhancing the patient’s innate serum clotting activity. It is critical to the function of these agents that the patient has intact intrinsic clotting activity. Topical agents augment the clot-formation process by two methods as follows: rapidly absorbing water and concentrating clotting factors, and via chemical reactions to enhance intrinsic clotting. Numerous formulations have been developed to achieve this goal (Table 1).18 All of these formulations have long shelf life and do not require refrigeration, making them ideal for field use.
Chitin-based products represent one formulation of topical hemostatic agents. Chitosan is a de-acetylated version of chitin, which is found in abundant amounts in shellfish such as shrimp. These products function by becoming mucoadhesive when exposed to blood, forming strong attachment to bleeding sites and enabling clot formation.18,20
Table 1.Topical hemostatic agents
Active Ingredient Mechanism of Action Advantages Disadvantages
Chitosan dressing Vasoconstriction, mechanical sealing, mobilizes clotting factors, RBCs, platelets
Successfully stops bleeding in up to 97% of wounds that failed direct pressure
Hemostasis fails in 1 hour in up to 70% of wounds.Not effective for arterial hemorrhage
Zeolite mineral dressing Absorbs water at the site of wounds, increasing concentration of clotting factors, platelets, RBCs
92% efficacy in stopping wounds refractory to direct pressure
Exothermic reaction can cause local burns (less so with newer formulation)
Mineral based—embedded with kaolin
Similar to zeolite-based products. Accelerates speed of clot formation.
Increased survival in animal models versus the zeolite formulation
Delayed onset of action

August 2013 • Volume 27 • Number 8
15
A battlefield chart review study of a chitin-based product reported an efficacy of 97% in stopping or improving bleeding when initial manual pressure and pressure dressings failed.20 Animal studies have demonstrated chitin-based dressings to be ineffective at stopping arterial bleeding, and it has been noted that up to 70% of dressings fail after 1 hour.21 Chitin-based products are available as pads impregnated with the active ingredient.
The mineral-based agents function by rapidly absorbing water and concentrating clotting factors. One such is a microporous, aluminosilicate mineral adsorbent or zeolite agent that comes as a granular powder inside a packet. This agent showed increased efficacy in comparison to manual pressure dressings in animal studies; however, it was ineffective at stopping high-pressure arterial bleeding. A combat-based study demonstrated 92% efficacy.22 Zeolite products were initially well known for causing an exothermic reaction on contact with blood. This side-effect caused significant burns often requiring additional treatment. Newer zeolite formulations come in synthetic beads and do not have this side effect.18
A newer, mineral-based dressing has demonstrated superior efficacy to both chitin-based and zeolite products in animal models. This gauze is embedded with kaolin, which is an aluminum silicate. It functions by activating the intrinsic clotting cascade and increasing the speed of clot formation. Studies show that cessation of bleeding is not as rapid with this dressing, but overall survival in animal models was significantly higher. The kaolin-based product is produced as a 3-inch-wide, 4-yard-long roll of gauze; it has largely replaced the use of other clotting agents in the battlefield.18
Other formulations of clotting agents have been tested and may come to the market. Numerous elements that make use of clotting factors have been developed. Agents
that make use of fibrin and thrombin have been developed; however, numerous reports of immunogenicity and risk of viral transmission have prevented widespread use.18,23 Granular clay materials were shown to have the highest efficacy overall in reducing mortality in swine studies. Significant safety concerns developed, however, when embolic events and local tissue thrombosis were reported, resulting in removal of these products from the market.18,24
CRITICAL DECISIONFor which types of wounds should topical hemostatic agents be considered in the treatment of active hemorrhage?
Topical hemostatic agents show the greatest utility in difficult-to-control bleeding in which standard management has failed or is not possible. Hemorrhage from certain anatomical locations can be difficult to manage, and this is when topical agents are ideal. Injury to junctional regions of the body (groin, axilla, neck) are notoriously difficult to manage because a circumferential dressing or tourniquet cannot be applied and because of the presence of large vascular structures. Wounds to these areas are a significant cause of mortality in penetrating trauma, causing approximately 20% of potentially preventable deaths in recent combat operations.25 Topical hemostatic agents were developed with support from the military to treat hemorrhage from these historically difficult-to-control injuries.8 These agents have also been used in wounds with diffuse venous bleeding and no identifiable source. Additionally, case series have shown that use of chitosan-based bandages is effective in stabilizing extremity bleeding while life-saving procedures and secondary surveys are performed.25
It must be emphasized that conventional management is effective in most cases of extremity bleeding. This includes direct pressure, pressure dressings, and tourniquet
application if needed. Topical hemostatic agents should be used only when these measures have failed or are not applicable.
The military has updated its Tactical Combat Casualty Care doctrine to include the use of topical hemostatic agents, and these agents are now included in the first aid kits of their medics. As of 2009, over 800,000 units of chitosan-based and zeolite-based topical hemostatic agents were deployed to combat operations.25 More recently, the kaolin-embedded dressings were deployed for use in the place of these older agents.18 To date, the civilian use of topical hemostatics in traumatic hemorrhage has not been initiated on any system-wide basis.
Case Resolutions
■ Case OneThe emergency physician in
the case of the 24-year-old with the actively hemorrhaging upper extremity injury recognized the high likelihood of nerve injury as well as vascular compromise and the need for surgical intervention. The patient was given 8 mg of morphine for pain control. The physician obtained an ulnar arterial Doppler pulse and applied a pneumatic tourniquet to a pressure of 160 mm Hg, at which point the Doppler signal extinguished and the bleeding stopped. With the hemorrhage controlled, the surgeon and emergency physician were able to visualize a lacerated radial artery. The patient was given a unit of PRBCs and immediately transferred to the operating room for emergent vascular repair. The tourniquet remained in place for less than 90 minutes, and two days after surgery, the patient began to have return of sensation and motor function in the affected hand.
■ Case TwoThe 37-year-old man with the
shotgun wound had a subclavian introducer placed and was intubated because of decreased mental status. A second unit of PRBCs was infused. The trauma surgeon suggested
Critical Decisions in Emergency Medicine
16
using a topical hemostatic agent for hemorrhage control. The emergency physician then applied a zeolite-based dressing to the wound. Recognizing this topical agent’s reliance on intrinsic clotting, fresh frozen plasma (FFP) and platelets were administered to reverse any trauma-induced or hemodilutional coagulopathy. Application of the topical hemostatic
agent led to a drastic reduction in bleeding.
Repeat vital signs showed a blood pressure of 92/43 and a heart rate of 100. Because of the proximity of the injury to the abdomen, the patient was taken for an abdominal CT scan, which revealed a small bowel injury and bladder rupture. The patient was then taken to the operating room for an exploratory laparotomy with primary repair of the abdominal injuries and was also found to have a transection of the femoral vein that was repaired as well. During removal of the hemostatic dressing, the surgeons later notice first- and second-degree burns in the groin.
The patient did well postoperatively and was extubated the following day. The burns were monitored but did not require any intervention other than local wound care.
■ Case ThreeThe 43-year-old woman who
presented with a laceration to the popliteal fossae after falling while rock climbing had repeated episodes of hypotension despite additional administration of PRBCs, FFP, and platelets. The patient was intubated for airway protection while resuscitation continued. Thirty minutes into her emergency department course, the tourniquet was again removed, which resulted in brisk bleeding and hypotension. The tourniquet was removed, and constant pressure by multiple providers and the addition of a kaolin-embedded dressing stopped obvious bleeding. The patient’s INR at this time was 3.6 secondary to hemorrhage and hemodilution. Additional FFP and platelets were administered.
The trauma team arrived in the emergency department 45 minutes after presentation and the patient was rapidly transported to the operating room. At this point, tourniquet time was approaching 6 hours and it was thought that the patient’s limb could not be salvaged. A below-the-knee amputation was performed by
Pearls ∙ Direct pressure should be
attempted prior to the application of a tourniquet or topical hemostatic agent.
∙ Tourniquets should be removed within 2 hours of application to prevent serious limb complications.
∙ Document results of a neurologic examination prior to tourniquet application.
∙ Topical hemostatic agents show the greatest utility in difficult-to-control bleeding in which standard management has failed or is not possible (eg, injury to junctional regions of the body such as the groin, axilla, and neck).
∙ Replace clotting factors and platelets in patients with hemorrhagic shock in order for topical hemostatic agents to be effective.
Pitfalls ∙ Failing to obtain information
from prehospital providers on tourniquet application time.
∙ Delaying definitive care because the tourniquet has controlled bleeding.
∙ Relying on topical hemostatic agents in patients with coagulopathy, either intrinsic, medication related, or from loss of factors in hemorrhagic shock and hemodilution.
the trauma team. The patient had a tenuous postoperative course but was extubated 3 days later and was discharged to a rehabilitation facility 2 weeks after her initial presentation.
SummaryTraumatic hemorrhagic shock
continues to be a major cause of morbidity and mortality in the civilian setting. In spite of advances in trauma surgery, resuscitation, and pharmacologic intervention, initial control of hemorrhage remains a critical step in caring for these patients. Tourniquet application is a fundamental but inadequately taught skill for emergency physicians. Commercially available devices should be applied early in the patient’s course, proximal to the bleeding area and should be considered as a temporary measure pending surgical intervention. Prolonged tourniquet times are associated with tissue ischemia, neuropathy, and reperfusion injury.
Topical hemostatic agents should be considered for wounds that are not amenable to tourniquet placement. Many of these agents undergo exothermic reactions when applied, resulting in local thermal injuries. Additionally, all these agents rely on the patient’s underlying clotting factors and platelets. Intrinsic, extrinsic, hemorrhagic, and dilutional coagulopathies should be appropriately treated to maximize the efficacy of topical hemostatic agents.
References1. Evans JA, van Wessem KJ, McDougall D, et al.
Epidemiology of traumatic deaths: comprehensive population-based assessment. World J Surg. 2010;34(1):158-163.
2. Kragh JF, Walters TJ, Baer DG, et al. Practical use of emergency tourniquets to stop bleeding in major limb trauma. J Trauma. 2008;64(2 Suppl):S38-S49; discussion S49-S50.
3. Kragh JF, Walters TJ, Baer DG, et al. Survival with emergency tourniquet use to stop bleeding in major limb trauma. Ann Surg. 2009;249(1):1-7.
4. Beekley AC, Sebesta JA, Blackbourne LH, et al. Prehospital tourniquet use in Operation Iraqi Freedom: effect on hemorrhage control and outcomes. J Trauma. 2008;64(2 Suppl):S28-S37; discussion S37.
5. Bellamy RF. The causes of death in conventional land warfare: implications for combat casualty care research. Mil Med. 1984;149(2):55-62.
6. Naimer SA, Tanami M, Malichi A, Moryosef D. Control of traumatic wound bleeding by compression with a compact elastic adhesive dressing. Mil Med. 2006;171(7):644-647.
August 2013 • Volume 27 • Number 8
17
7. Doyle GS, Taillac PP. Tourniquets: a review of current use with proposals for expanded prehospital use. Prehosp Emerg Care. 2008;12(2):241-256.
8. Schrager JJ, Branson RD, Johannigman JA. Lessons from the tip of the spear: medical advancements from Iraq and Afghanistan. Respir Care. 2012;57(8):1305-1313.
9. Shaw JA, Murray DG. The relationship between tourniquet pressure and underlying soft-tissue pressure in the thigh. J Bone Joint Surg Am. 1982;64(8):1148-1152.
10. Crenshaw AG, Hargens AR, Gershuni DH, Rydevik B. Wide tourniquet cuffs more effective at lower inflation pressures. Acta Orthop Scand. 1988;59(4):447-451.
11. Delfi Medical Innovations, Inc. Hospital safety & performance in the field. Available online at: http://delfimedical.com/pts-ii/emt. Accessed on March 13, 2013.
12. Horlocker TT, Hebl JR, Gali B, et al. Anesthetic, patient, and surgical risk factors for neurologic complications after prolonged total tourniquet time during total knee arthroplasty. Anesth Analg. 2006;102(3):950-955.
13. Heppenstall RB, Scott R, Sapega A, et al. A comparative study of the tolerance of skeletal muscle to ischemia. Tourniquet application compared with acute compartment syndrome. J Bone Joint Surg Am. 1986;68(6):820-828.
14. Chisholm JJ. A Manual of Military Surgery. Richmond, VA: West & Johnston; 1861:140-143.
15. Klenerman L. The tourniquet in surgery. J Bone Joint Surg Br. 1962;44-B:937-943.
16. Coupland RM, Molde A, Navein J. Care in the Field for Victims of Weapons of War: A Report from the Workshop Organized by the ICRC on “Prehospital Care for War and Mine Wounded.” Geneva: International Committee of the Red Cross; 2001.
17. Markenson D, Ferguson JD, Chameides L, et al. Part 17: first aid: 2010 American Heart Association and American Red Cross guidelines for first aid. Circulation. 2010;122(18 Suppl 3):S924-S946. Available online at: http://circ.ahajournals.org/content/122/18_suppl_3/S934.full.pdf+html. Accessed on March 13, 2013.
18. Kheirabadi B. Evaluation of topical hemostatic agents for combat wound treatment. US Army Med Dep J. 2011:25-37.
19. Dorlac WC, DeBakey ME, Holcomb JB, et al. Mortality from isolated civilian penetrating extremity injury. J Trauma. 2005;59(1):217-222.
20. Wedmore I, McManus JG, Pusateri AE, Holcomb JB. A special report on the chitosan-based hemostatic dressing: experience in current combat operations. J Trauma. 2006;60(3):655-658.
21. Acheson EM, Kheirabadi BS, Deguzman R, et al. Comparison of hemorrhage control agents applied to lethal extremity arterial hemorrhage model in swine. J Trauma. 2005;59(4):865-874; discussion 874-875.
22. Rhee P, Brown C, Martin M, et al. QuikClot use in trauma for hemorrhage control: case series of 103 documented uses. J Trauma. 2008;64(4):1093-1099.
23. Spotnitz WD, Burks S. Hemostats, sealants, and adhesives: components of the surgical toolbox. Transfusion. 2008;48(7):1502-1516.
24. Schreiber MA, Neveleff DJ. Achieving hemostasis with topical hemostats: making clinically and economically appropriate decisions in the surgical and trauma settings. AORN J. 2011;94(5):S1-S20.
25. Cox ED, Schreiber MA, McManus J, et al. New hemostatic agents in the combat setting. Transfusion. 2009;49 Suppl 5:248S-255S.

Critical Decisions in Emergency Medicine
18
August 2013 • Volume 27 • Number 8
19
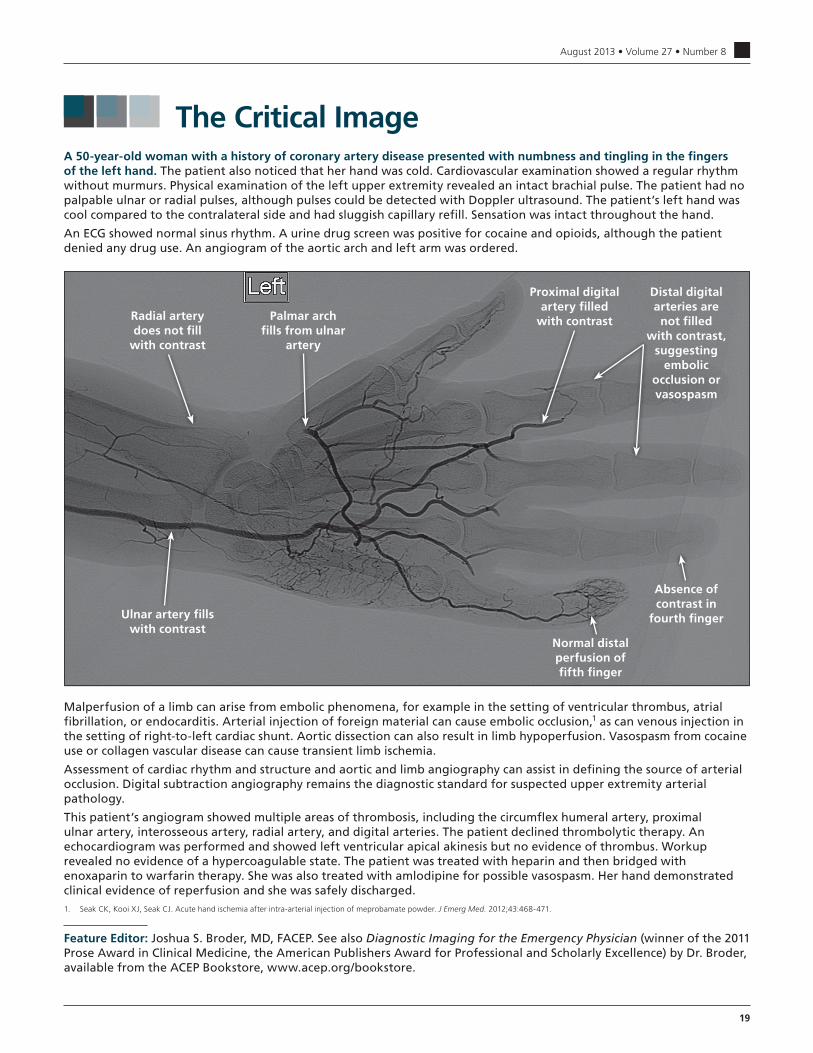
The Critical ImageA 50-year-old woman with a history of coronary artery disease presented with numbness and tingling in the fingers of the left hand. The patient also noticed that her hand was cold. Cardiovascular examination showed a regular rhythm without murmurs. Physical examination of the left upper extremity revealed an intact brachial pulse. The patient had no palpable ulnar or radial pulses, although pulses could be detected with Doppler ultrasound. The patient’s left hand was cool compared to the contralateral side and had sluggish capillary refill. Sensation was intact throughout the hand.
An ECG showed normal sinus rhythm. A urine drug screen was positive for cocaine and opioids, although the patient denied any drug use. An angiogram of the aortic arch and left arm was ordered.
Normal distal perfusion of fifth finger
Radial artery does not fill
with contrast
Palmar arch fills from ulnar
artery
Ulnar artery fills with contrast
Proximal digital artery filled
with contrast
Distal digital arteries are not filled
with contrast, suggesting
embolic occlusion or vasospasm
Absence of contrast in
fourth finger
Malperfusion of a limb can arise from embolic phenomena, for example in the setting of ventricular thrombus, atrial fibrillation, or endocarditis. Arterial injection of foreign material can cause embolic occlusion,1 as can venous injection in the setting of right-to-left cardiac shunt. Aortic dissection can also result in limb hypoperfusion. Vasospasm from cocaine use or collagen vascular disease can cause transient limb ischemia.
Assessment of cardiac rhythm and structure and aortic and limb angiography can assist in defining the source of arterial occlusion. Digital subtraction angiography remains the diagnostic standard for suspected upper extremity arterial pathology.
This patient’s angiogram showed multiple areas of thrombosis, including the circumflex humeral artery, proximal ulnar artery, interosseous artery, radial artery, and digital arteries. The patient declined thrombolytic therapy. An echocardiogram was performed and showed left ventricular apical akinesis but no evidence of thrombus. Workup revealed no evidence of a hypercoagulable state. The patient was treated with heparin and then bridged with enoxaparin to warfarin therapy. She was also treated with amlodipine for possible vasospasm. Her hand demonstrated clinical evidence of reperfusion and she was safely discharged.1. Seak CK, Kooi XJ, Seak CJ. Acute hand ischemia after intra-arterial injection of meprobamate powder. J Emerg Med. 2012;43:468-471.
Feature Editor: Joshua S. Broder, MD, FACEP. See also Diagnostic Imaging for the Emergency Physician (winner of the 2011 Prose Award in Clinical Medicine, the American Publishers Award for Professional and Scholarly Excellence) by Dr. Broder, available from the ACEP Bookstore, www.acep.org/bookstore.
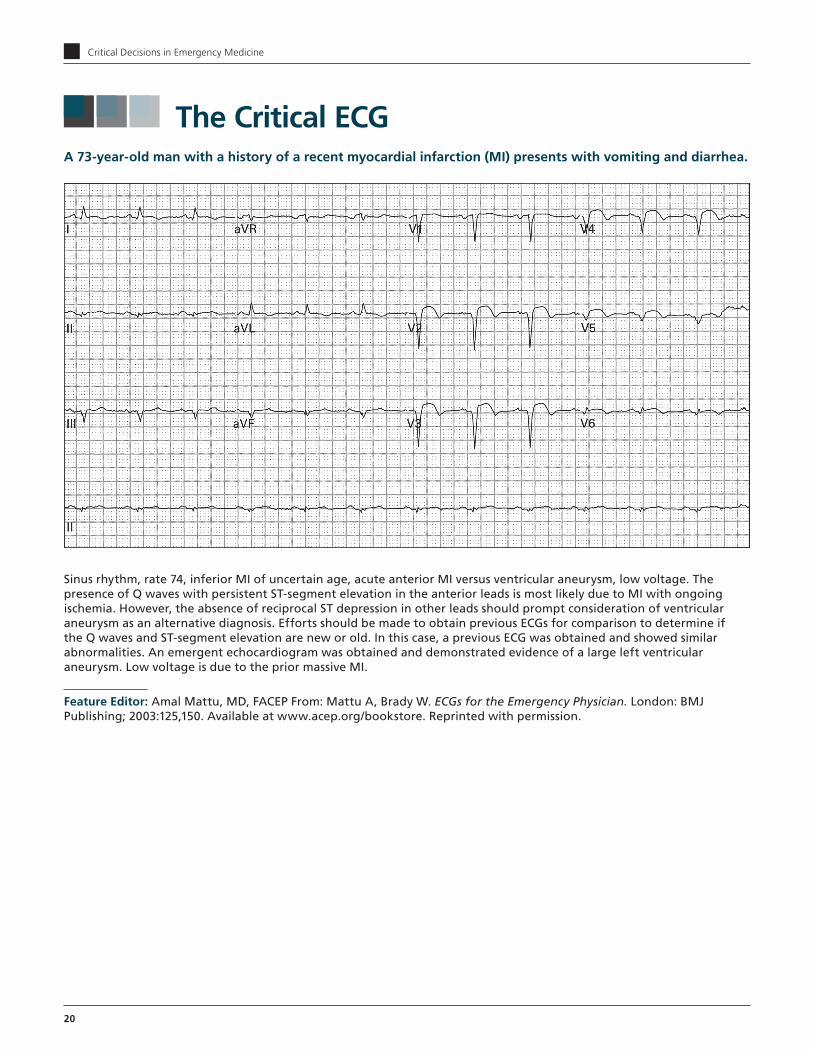
Critical Decisions in Emergency Medicine
20
The Critical ECG
Sinus rhythm, rate 74, inferior MI of uncertain age, acute anterior MI versus ventricular aneurysm, low voltage. The presence of Q waves with persistent ST-segment elevation in the anterior leads is most likely due to MI with ongoing ischemia. However, the absence of reciprocal ST depression in other leads should prompt consideration of ventricular aneurysm as an alternative diagnosis. Efforts should be made to obtain previous ECGs for comparison to determine if the Q waves and ST-segment elevation are new or old. In this case, a previous ECG was obtained and showed similar abnormalities. An emergent echocardiogram was obtained and demonstrated evidence of a large left ventricular aneurysm. Low voltage is due to the prior massive MI.
Feature Editor: Amal Mattu, MD, FACEP From: Mattu A, Brady W. ECGs for the Emergency Physician. London: BMJ Publishing; 2003:125,150. Available at www.acep.org/bookstore. Reprinted with permission.
A 73-year-old man with a history of a recent myocardial infarction (MI) presents with vomiting and diarrhea.

August 2013 • Volume 27 • Number 8
21
Qualified, paid subscribers to Critical Decisions in Emergency Medicine may receive CME certificates for up to 5 ACEP Category I credits, 5 AMA PRA Category 1 Credits™, and 5 AOA Category 2-B credits for answering the following questions. To receive your certificate, go to www.acep.org/newcriticaldecisionstesting and submit your answers online. On achieving a score of 75% or better, you will receive a printable CME certificate. You may submit the answers to these questions at any time within 3 years of the publication date. You will be given appropriate credit for all tests you complete and submit within this time. Answers to this month’s questions will be published in next month’s issue.
CME Questions
1. The term “hospice” refers to:A. A benefit offered in Medicare Part DB. A mechanism to categorize patients when there are no further
curative options available to treat themC. A philosophy of care that is dedicated to maximizing comfort
and quality for individuals approaching the end-of-lifeD. A physical structure used to house patients in the final days of
life
2. Most hospice patients are cared for in the:A. Acute-care hospitalB. HomeC. Inpatient residential hospice facilityD. Nursing home
3. Patients qualify for hospice if they are deemed (based on diagnosis and disease burden):A. To have 6 to 12 months to live while pursuing aggressive careB. To have an unknown prognosis yet agree to “do not attempt
resuscitation” (DNAR) statusC. To have less than 6 months to live and are opting for a
comfort-focused plan of careD. To have less than 6 months to live while pursuing aggressive
care
4. Many potential goals of care exist for patients seen in an emergency department. The most common goals of care for hospice patients in the emergency department are:A. Cure of diseaseB. Prevention of diseaseC. Prolongation of lifeD. Symptom reduction and maximization of comfort
5. When hospice patients present to the emergency department because of poor symptom control:A. Efforts should focus on aggressive symptom control, including
limited evaluation for reversible causes (including procedures or surgeries aimed at relief of symptoms)
B. Efforts should be minimal in consideration of the patient’s DNAR status
C. Efforts should be minimal so as not to exceed the Medicare hospice benefit
D. The level of care should be based on patients’ willingness to revoke their DNAR status
6. Although hospice agencies and their health care professionals provide significant support to hospice patients, the bulk of home-based care often falls on a patient’s:A. Attending physicianB. Community volunteersC. FamilyD. Friends
7. When a hospice patient’s deterioration is imminent and decisions are needed about the use of life-sustaining treatments, the most important initial step to take is:A. Gaining a complete set of vital signsB. Notification of the hospice agency regarding change of statusC. Palliative care consultation D. Rapid goals-of-care assessment
8. When a DNAR patient presents from an inpatient hospice because of acute symptoms, the emergency physician can assume:A. A goals-of-care discussion has previously been carried out and
need not be repeatedB. The DNAR status of the patient diminishes the patient’s
worthiness of a timely evaluation by the emergency physicianC. The DNAR status of the patient has no bearing on the patient’s
need for a timely assessment of the presenting complaintD. The DNAR status of the patient is automatically revoked
because the patient is seeking acute care
9. An example of a palliative surgical procedure performed exclusively for maximization of comfort and relief of symptoms in a dying patient includes which of the following?A. CholecystectomyB. Total mastectomy with axillary node dissection for breast
cancerC. Tumor resection of the colon with end-to-end anastomosis for
adenocarcinomaD. Venting gastrostomy for malignant bowel obstruction
unrelieved by medical means
10. A hospice patient with a days-to-weeks prognosis presents because of the loss of function of a peripherally inserted central catheter (PICC). The patient can tolerate oral medications. This patient would initially benefit most from:A. Declogging of the PICC with thrombolytic therapyB. A goals-of-care discussion to determine whether continuation
of a PICC is appropriate at this timeC. PICC removal with venogramD. Removal of the PICC and insertion of a new PICC

Critical Decisions in Emergency Medicine
22
Answer key for July 2013, Volume 27, Number 7
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20B A A C A D A C A B A C B A D B C B B B
11. A 23-year-old man presents with lacerations to the wrist after he punched a window. Vital signs are blood pressure 120/75, heart rate 110, and respiratory rate 20. EMS was unable to control the bleeding en route with direct pressure. On presentation, the patient has active arterial bleeding from the radial aspect of the wrist. Which of the following describes the most appropriate next steps in the patient’s management?A. Apply a commercial tourniquet proximal to the injury with a
pressure of 140 mm Hg and await surgery consultationB. Apply a commercial tourniquet proximal to the injury with the
minimal required pressure to stop active hemorrhage and await surgery consultation
C. Apply a topical hemostatic dressing and await surgery consultation
D. Attempt to tie off bleeding vessel with vessel ties and await surgical consultation
12. A 45-year-old woman who was involved in a motor vehicle collision on a remote stretch of highway is being transported to the emergency department via ambulance. The patient sustained a partial amputation of her right upper extremity at the elbow and had a tourniquet placed in the field. The patient has no other injuries. The EMTs report that because of difficulty extricating the patient from the vehicle, the tourniquet has been in place for 60 minutes and they will arrive at the emergency department in about 45 minutes. On arrival, the patient’s blood pressure is 90/40, and her heart rate is 136. Removal of the patient’s tourniquet is followed by brisk hemorrhage. Which of the following is correct?A. The tourniquet should be removed and vessel repair should be
attempted immediately by the emergency physicianB. The tourniquet should be removed because the patient is at
high risk for amputationC. The tourniquet should not be removed regardless of
hemorrhage control as the patient’s tourniquet time already makes the limb non-viable
D. The tourniquet should not be removed unless hemorrhage can be controlled by direct pressure or topical hemostatic agents
13. An 18-year-old woman is brought in by EMS after sustaining a gunshot wound to her left thigh. Her vital signs are blood pressure 100/63 and heart rate 113. Removal of the field dressing reveals a large wound to the mid-thigh with active bleeding. The patient is neurovascularly intact distally. Which of the following represents appropriate initial management of the wound?A. Apply a topical hemostatic agent to the wound while primary
and secondary surveys are completedB. Apply a tourniquet and topical hemostatic agent to the wound
while primary and secondary surveys are completedC. Apply direct pressure to the wound while primary and
secondary surveys are completedD. Place a tourniquet proximal to the wound while primary and
secondary surveys are completed
14. Which of the following injuries would most likely benefit from a topical hemostatic agent?A. Gunshot wound to the upper armB. Laceration to the face with non-arterial bleedingC. Laceration to the thigh with non-arterial bleedingD. Laceration to the wrist with arterial bleeding from the ulnar
artery
15. Which of the following is correct regarding tourniquet application?A. Makeshift tourniquets are equivalent in efficacy to
commercially available tourniquetsB. Tourniquets are more effective in smaller diameter limbs than
in larger diameter limbsC. Tourniquets may be placed over joints if clinically warrantedD. Tourniquets may be placed over open or closed fractures if
clinically warranted
16. Mineral-based topical hemostatic agents work by which of the following mechanisms?A. Attach to bleeding sites and provide mucoadhesive activity for
clot formationB. Rapidly absorb water and activate intrinsic clotting C. Supply additional, extrinsic clotting factors to area of
applicationD. Supply additional, extrinsic platelets to area of application
17. A 38-year-old woman is brought in by EMS after sustaining a gunshot wound to her right groin. Her vital signs are blood pressure 80/47 and heart rate 136. Removal of the field dressing reveals a large wound to the groin with active, nonpulsatile bleeding. The patient is neurovascularly intact distally. Blood is observed continuously oozing from the patient’s intravenous sites. Which of the following represents the best initial management of the wound?A. A chitosan-based topical hemostatic agent is the first method
of hemorrhage controlB. A zeolite topical hemostatic agent should be the first method
of hemorrhage controlC. Application of a commercial tourniquet is likely to stop
bleedingD. Replacement of the patient’s lost clotting factors is necessary
to maximize the efficacy of any topical hemostatic agent
18. A 58-year-old man presents with a large laceration to his thigh after a motor vehicle collision. His vital signs are blood pressure 113/64, heart rate 112, and respiratory rate 20. EMS was unable to control the bleeding en route with direct pressure. On presentation, the patient has active arterial bleeding from the mid-thigh. A tourniquet is placed proximal to the wound but does not control the bleeding. Which of the following should be considered to increase the efficacy of the tourniquet?A. Apply a second proximal tourniquetB. Apply a tourniquet directly over the lacerationC. Apply a tourniquet distal to the lacerationD. Replace the tourniquet with a narrower tourniquet

August 2013 • Volume 27 • Number 8
23
19. Which of the following is true regarding tourniquet times?A. A tourniquet should never be applied unless definitive care can
be arranged within 1 hourB. Application of a tourniquet for longer than 1 hour almost
always results in amputationC. Removal of a tourniquet that has been in place for longer than
2 hours may result in hemodynamic decompensation or lethal arrhythmias
D. Tourniquet time is unrelated to limb survival
20. Which of the following represents a distinct advantage of topical hemostatic agents in military medicine?A. Can effectively be self-applied by a wounded soldier in the
fieldB. Does not need to be removed prior to definitive surgical careC. Effectively stops arterial bleedingD. Has a long shelf life and does not require refrigeration

NONPROFITU.S. POSTAGE
P A I DDALLAS, TXPERMIT NO.
1586
The Drug Box
August 2013 • Volume 27 • Number 8
Critical Decisions in Emergency Medicine is the official CME publication of the American College of Emergency Physicians. Additional volumes are available to keep emergency medicine professionals up-to-date on relevant clinical issues.
Editor-in-ChiefLouis G. Graff IV, MD, FACEP Professor of Traumatology and Emergency Medicine, Professor of Clinical Medicine, University of Connecticut School of Medicine; Farmington, Connecticut
Section EditorJ. Stephen Bohan, MS, MD, FACEP Executive Vice Chairman and Clinical Director, Department of Emergency Medicine, Brigham & Women’s Hospital; Instructor, Harvard Medical School, Boston, Massachusetts
Feature EditorsMichael S. Beeson, MD, MBA, FACEP Program Director, Department of Emergency Medicine, Akron General, Akron, Ohio; Professor, Clinical Emergency Medicine, Northeastern Ohio Universities College of Medicine, Rootstown, Ohio
Joshua S. Broder, MD, FACEP Associate Clinical Professor of Surgery, Residency Program Director, Division of Emergency Medicine, Duke University Medical Center, Durham, North Carolina
Amal Mattu, MD, FACEP Professor and Vice Chair, Department of Emergency Medicine, Director, Faculty Development and Emergency Cardiology Fellowships, University of Maryland School of Medicine, Baltimore, Maryland
Robert C. Solomon, MD, FACEP Core faculty, Emergency Medicine Residency, Allegheny General Hospital, Pittsburgh, Pennsylvania; Assistant Professor (adjunct) Emergency Medicine, Temple University School of Medicine, Philadelphia, Pennsylvania
Associate EditorsDaniel A. Handel, MD, MPH, FACEP Vice Chair and Director of Clinical Operations; Associate Professor, Department of Emergency Medicine; Oregon Health & Science University, Portland, Oregon
Frank LoVecchio, DO, MPH, FACEP Research Director, Maricopa Medical Center Emergency Medicine Program; Medical Director, Banner Poison Control Center, Phoenix, Arizona; Professor, Midwestern University/Arizona College of Osteopathic Medicine, Glendale, Arizona
Sharon E. Mace, MD, FACEP Associate Professor, Department of Emergency Medicine, Ohio State University School of Medicine; Faculty, MetroHealth Medical Center/Cleveland Clinic Foundation Emergency Medicine Residency Program; Director, Pediatric Education/Quality Improvement and Observation Unit, Cleveland Clinic Foundation, Cleveland, Ohio
Lynn P. Roppolo, MD, FACEP Associate Emergency Medicine Residency Director, Associate Professor of Emergency Medicine, University of Texas Southwestern Medical Center, Dallas, Texas
Robert A. Rosen, MD, FACEP Medical Director, Culpeper Regional Hospital, Culpeper, Virginia; Associate Professor, Emergency Medicine, University of Virginia School of Medicine, Charlottesville, Virginia
George Sternbach, MD, FACEP Clinical Professor of Surgery (Emergency Medicine), Stanford University Medical Center, Stanford, California
Kathleen Wittels, MD Instructor, Harvard Medical School, Boston, Massachusetts
Editorial StaffMary Anne Mitchell, ELS, Managing EditorMike Goodwin, Creative Services ManagerJessica Hamilton, Educational Products AssistantLexi Schwartz, Subscriptions CoordinatorMarta Foster, Director, Educational Products
Critical Decisions in Emergency Medicine is a trademark owned and published monthly by the American College of Emergency Physicians, PO Box 619911, Dallas, TX 75261-9911. Send address changes and comments to Critical Decisions in Emergency Medicine, PO Box 619911, Dallas, TX 75261-9911, or to [email protected]; call toll free 800-798-1822, or 972-550-0911.Copyright 2013 © by the American College of Emergency Physicians. All rights reserved. No part of this publication may be reproduced, stored, or transmitted in any form or by any means, electronic or mechanical, including storage and retrieval systems, without permission in writing from the Publisher. Printed in the USA.The American College of Emergency Physicians (ACEP) makes every effort to ensure that contributors to its publications are knowledgeable subject matter experts. Readers are nevertheless advised that the statements and opinions expressed in this publication are provided as the contributors’ recommendations at the time of publication and should not be construed as official College policy. ACEP recognizes the complexity of emergency medicine and makes no representation that this publication serves as an authoritative resource for the prevention, diagnosis, treatment, or intervention for any medical condition, nor should it be the basis for the definition of, or standard of care that should be practiced by all health care providers at any particular time or place. Drugs are generally referred to by generic names. In some instances, brand names are added for easier recognition. Device manufacturer information is provided according to style conventions of the American Medical Association. ACEP received no commercial support for this publication. To the fullest extent permitted by law, and without limitation, ACEP expressly disclaims all liability for errors or omissions contained within this publication, and for damages of any kind or nature, arising out of use, reference to, reliance on, or performance of such information.ISSN 2325-0186 (Print) ISSN 2325-8365 (Online)
Mechanism of Action Acts on viral replication through incorporation into DNA in place of thymidine and inhibition of thymidylate synthetase.
Indications HSV (I or II)-related keratitis and keratoconjunctivitis
Dosing Adults (and children ≥6 years old): Available as 1% solution; 1 drop to affected eye every 2 hours while awake, up to 9 drops daily while corneal ulcer presentOnce re-epithelialization has occurred then 1 drop every 4 hours for 7 days
Side Effects Ocular: Pain (stinging/burning), palpebral edema, irritation, stromal edema, increase in ocular pressure, hypersensitivity reactions
Contraindications/Precautions
If no improvement in 1-2 weeks consider altering therapy, do not prescribe for more than 21 days.Contraindications: Hypersensitivity to trifluridine or components of solutionPregnancy Category CLactation: Unknown if excreted in breast milk; not recommended
Feature Editors: Michael S. Beeson, MD, MBA, FACEP; Steven Warrington, MD
TrifluridineSteven Warrington, MD; Akron General Medical Center
Trifluridine, also known as trifluorothymidine, is an ophthalmic medication often used for treatment of keratitis and keratoconjunctivitis related to herpes simplex virus (HSV) I and II. Because of its relatively few side effects and high efficacy, it is a useful medication in patients with ophthalmic manifestations of HSV. Emergency physicians should remember the frequent dosing, though, and stress the importance of this to their patients.