volume 2 number 2 fall 2002 published by european wound
TRANSCRIPT
Volume 2Number 2Fall 2002
Published byEuropeanWound ManagementAssociation
2 EWMA JOURNAL 2002 VOL 2 NO 2
The EWMA JournalISSN number: 1609-2759
Volume 2, No. 2. Fall, 2002
The Journal of the EuropeanWound Management Association
Published twice a year
EditorE. Andrea Nelson
Editorial BoardCarol DealeyFinn Gottrup
Deborah HofmanSylvie Meaume
Joan-Enric Torra BouPeter Vowden
Editorial AdvisorMichelle Briggs
Legal ResponsiblePeter Vowden
EWMA Homepagewww.ewma.org
For membership application,correspondence,
prospective publications contact:EWMA Secretariat
PO Box 864, London SE1 8TTUnited Kingdom
Tel: +44 207 848 3496E-mail: [email protected]
Enquiries concerning advertisingshould be addressed to:
Congress ConsultantsMartensens Allé 8
DK-1828 Frederiksberg C · Denmark.Tel: (+45) 7020 0305Fax: (+45) 7020 0315
E-mail: [email protected]
Layout:Birgitte Clematide
Printed by:Kailow Graphic A/S, Denmark
Copies printed: 10,000
Prices:Distributed Free to Members of
the European Wound ManagementAssociation and members of
co-operating associations.Individual subscription: 7.50 €Libraries and Institutions: 25 €
The next issue will be publishedin Spring 2003. Prospective materialfor the publication must be with the
editors as soon as possible andin no case later than March 15th.
The contents of articles and lettersin the EWMA Journal do not
necessarily reflect the opinions ofthe Editors or the European
Wound Management Association.
The copyright of all published materialand illustrations is the property of
the European Wound ManagementAssociation. However, provided prior
written consent for their reproduction isobtained from both the Author and
EWMA via the Editorial Board of theJournal, and proper acknowledgementmade and printed, such permission will
normally be readily granted.Requests to reproduce material should
state where the material is to bepublished, and, if it is abstracted,summarised, or abbreviated thenthe proposed new text should besent to the EWMA Journal Editor
for final approval.
EWMA Council
For contact addresses, see www.ewma.org
Peter VowdenPresident
Christine MoffattImmediate Past
President
Marco RomanelliTreasurer
Sue Bale
Brian GilchristSecretary
Carol Dealey
Zena Moore Joan-Enric Torra Bou
Luc Gryson Deborah HofmanPeter Franks
Panel MembersNick Bosanquet Cost Effectiveness PanelMichelle Briggs Editorial BoardChristina Lindholm Educational PanelSylvie Meaume Editorial BoardHugo Partsch Educational PanelJohn Posnett Cost Effectiveness PanelPatricia Price Cost Effectiveness PanelWolfgang Vansheidt Co-operating Organisations Board
Conferences
EWMA news
Organisations
3 Editorial
5 The management of pain associated withdressings changes in patients with burnsJacques Latarjet
11 Evaluating Australian Clinical PracticeGuidelines for Pressure Ulcer PreventionPrentice JL, Stacey MC
17 Growth Factors and Interactive Dressingsin Wound RepairDavid Leaper, Battistino Paggi, Gregory A Comp-ton, Heather Orsted, Luc Teot, H. M. Ockenfels
25 Contemporary Research in PressureUlcer Prevention and Treatment from themeta Register of Clinical Trials (mRCT)E. Andrea Nelson
30 Welcome to Peter VowdenChristine Moffatt
32 13th Annual EWMA meeting in Pisain 2003 – Wound Care in ItalyMarco Romanelli
36 The EWMA Organisational Structure
38 Leaving/entering Council
40 New Corporate Sponsors in EWMA
40 EWMA Activity Report
42 EWMA Journal Previous Issues
43 Indexes from international journals
44 EWMA Pain Position Paper
46 EWMA Cost Effectiveness Panel
47 EWMA Corporate Sponsor Contact Data
48 EWMA Educational Development Project
49 EWMA/EPUAP Education Seminar
49 EWMA Grants
50 The 12th Conference of the EuropeanWound Management Association:Quality of Life
54 Conference Calendar
56 Report on the 6th European PressureUlcer Advisory Panel Open Meeting
57 Diabetic Foot Study Group (DFSG) meeting in Hungary (Lake Balaton)
58 First International Workshop on Multi-disciplinary Concepts in Wound Healing
59 Wound Healing Association in Latvia
60 The Cochrane Collaboration
62 Co-operating Organisations
Scientific Articles
Madeleine Flanagan
Finn GottrupRecorder
E. Andrea NelsonEditor

EWMA JOURNAL 2002 VOL 2 NO 2 3
The basic principles that underpin acute and chronic wound care aresimilar and both include optimising the overall management of thepatient and any associated disease processes. Despite this, the methods
employed to facilitate healing do vary considerably between individualpractitioners, within and between specialities, and across the individual statesthat constitute Europe. Why should these differences have arisen? Often theanswer lies in tradition and re-imbursement policies, which have unfortunatelybeen allowed to establish practice, and the failure of research to provideevidence of sufficient quality to categorically define “best” practice.
Through its individual members and by co-operation with other associationsand societies, EWMA has the opportunity to influence future wound carepractice by bringing together health care professionals, scientists and industry.Clearly this needs to be done through partnership, and to facilitate this EWMAhas continued to develop collaborations with national wound care groups andother pan-European sub-specialty societies. The development of these links isone of the cornerstones of EWMA’s strategy. Such links will, however, beineffective unless they are combined with a greater understanding of the factorsthat influence the provision of care within individual nations. To facilitate thegrowth of supporting information for the development of a pan-Europeanwound care strategy I hope that EWMA will be able to use existing grants andeducational award schemes to sponsor and assist specific research projectsaimed at providing epidemiological and cost-related data. My hope is that this,combined with the work of the educational and cost-effectiveness groups, willprovide both EWMA and the co-operating societies with a greaterunderstanding of the problems facing wound care specialists, from whicheverdiscipline they come, and will also demonstrate the skills and standardsavailable across Europe.
We have already made a start with the EWMA Position Paper on Pain atDressing Changes – this is now freely available i German, Spanish, Italian,French and English. It is a testament to what you can achieve by bringingtogether industry partners, researchers, educators and clinicians and we intendthis to be the first in a series of EWMA position papers.
Much of the necessary data is already in existence. My hope is that bydeveloping additional links and strengthening existing links with other woundcare societies EWMA can act as a data resource for existing local and nationalguidelines and can help societies develop and standardise care.
Peter Vowden, EWMA President

PROMOGRANPROTEASE-MODULATING MATRIX
For all chronic wounds
Active modulation of wound environment1,2
Protease inactivation
Growth-factor protection
Clinically proven3
Ease of application and storage3
Bioresorbable, natural components4,5
PROMOGRAN
APPLIES SCIENCE
TO THE FORCES
OF NATURE
1 Cullen B, Smith R, Silcock D, et al. The mechanism of action of PROMOGRAN*, a protease-modulating matrix for the treat-ment of diabetic foot ulcers. Wound Repair Regen. 2002; 10 (1): 16–25.
2 Cullen B, Watt PW, Lundqvist C, et al. Characterisation of collagen/ORC, a novel biomaterial for wound healing: An investigation of potential mechanisms of action. Int J Biochem Cell Biol. 2002; accepted for publication.
3 Veves A, Sheehan P, Pham H. A randomised controlled trial of acollagen/oxidised regenerated cellulose dressing PROMOGRAN vs standard therapy in the management of diabetic foot ulcers. Arch Surg. 2002; 137 (7): 822–7.
4 Bailey AJ. Perspective article: the fate of collagen implants in tissue defects. Wound Repair Regen. 2000; 8 (1): 5–12.
5 Dimitrijevich SD. A review of wound healing application of ORC and ORC based devices. In preparation.

EWMA JOURNAL 2002 VOL 2 NO 2 5
Scientific Article
Jacques Latarjet, MDConsultant inAnaesthesiology andIntensive CareChief, Burn CenterSt Joseph and St LucHospital, Lyon, France.Email: [email protected]
INTRODUCTIONIn a recent international wound care survey on pain and traumaat wound dressing changes, dressing removal was considered bypractitioners to be the time of greatest perceived pain1. Burninjuries cause intense and prolonged pain, made worse by theneed to change dressings frequently to prevent infection andaid healing. Modern techniques such as early excision and skinreplacement therapy have reduced the number of dressingchanges necessary to treat a burn injury2. Nevertheless, dailycleansing of the wound, topical applications and occlusive dress-ings remain the preferred recommended management tech-nique, especially for injuries where sufficient epidermal livingcells remain to ensure a degree of satisfactory spontaneous heal-ing. Because a burn injury can be heterogeneous, it may benecessary to wait eight to ten days before determining whichtissues need to be excised and grafted, and which will heal bythemselves.
Choinière et al3 examined the characteristics of pain experi-enced by burn patients and identified that the time of greatestpain is usually experienced during therapeutic procedures. Thestudy emphasised the need to distinguish between this type ofprocedural pain and background pain (at rest) that, once as-sessed and evaluated, can be managed pharmacologically withparacetamol, non-steroidal anti-inflammatory drugs (NSAIDs)and opioids. The aim of zero background pain in burn inju-ries is an achievable and perfectly realistic goal. However, pro-cedural burn pain as a result of dressing changes is difficult toassess and manage4, and there is no consensus among burnspecialists on how best to determine or control this pain. Studieshave shown that procedural pain is widely under treated, evenin specialised burn centres5, 6. In addition, pain control, evenwhen recognised as important, can be further constrained by alack of staff training, time and monitoring capabilities. Under-treated pain in burn patients can result in non-compliance withhospital treatment, disrupted care7 and increased risk of post-traumatic stress disorders 8,9.
The management ofpain associated withdressings changes inpatients with burns
Key wordsBurns; wound healing; procedural pain;pain assessment; analgesia
Key points1. Inadequate pain management is detri-
mental to burn patients. The differ-ence between continuous backgroundpain and pain due to therapeutic pro-cedures, such as dressing changes,must be evaluated and treated sepa-rately.
2. Control of procedural pain is impossi-ble without strong pharmacologicaltreatments, such as IV opioids. Non-pharmacological therapies shouldnever be used alone.
3. The management of burn pain atdressing changes is generally over-looked. The future of burn care mustfocus on the optimal control of pain toavoid patient suffering and reduce therisk of post-traumatic stress disorders.
This paper focuses on pain associatedwith dressings changes in burn patients.The pain experienced during such proce-dures is often excruciating, although thisissue is frequently overlooked. The authoremphasises the need for accurate painassessment in both children and adults,and describes a variety of pharmaco-logical and non-pharmacological methodsof pain management.
�

EWMA JOURNAL 2002 VOL 2 NO 26
PATHOPHYSIOLOGY OF BURN PAINThe immediate pain that follows a burn injury is due tothe stimulation of skin nociceptors (pain sensing nerves).Nerve endings that are completely destroyed will not trans-mit pain, but those that remain intact will trigger painthroughout the time and course of treatment, as will re-generating nerves – those still connected with intact affer-ent fibres10.
Primary hyperalgesiaA burn injury will immediately prompt an intense inflam-matory response and the release of chemical mediators thatsensitise the active nociceptors at the site of injury. Thiswill cause the wound to become sensitive to mechanicalstimuli such as touch, rubbing or debridement, as well aschemical stimuli such as antiseptics or other topical appli-cations11.
Secondary hyperalgesiaContinuous or repeated peripheral stimulation of nocic-eptive afferent fibres induces a significant increase in dor-sal horn excitability, partly via N-methyl-D-aspartate(NMDA) receptors12, leading to increased sensitivity in thesurrounding unburned areas of skin. This so called ‘wind-up pain’, as shown in recent studies by Pedersen andKehlet13 is a component of post-burn hyperalgesia, and isexacerbated by the mechanical stimulation that occurs asa result of frequent dressing changes. This ‘wind-up’mechanism may also be partly responsible for a patient’sincreased pain sensitivity observed during the course ofburn management and reflected in the greater opioid re-quirement for dressing changes over time14. Ketamine, apotent NMDA antagonist, works by blocking the paintransmission pathway implicated in the development ofcentral sensitisation. It has been used extensively in burnpatients for more than 40 years15, although this propertywas not recognised for some years.
Patients with severe burns who require dressings overa long period of time may continue to experience pain de-spite an escalation in opioid dose requirement. This phe-nomenon cannot be explained by the pharmacologicaleffects of burn injuries such as hypermetabolism13.Whether this is due to opioid tolerance or increased painsensitivity, it is important to be aware that the pain doesnot usually decrease over the time and course of treatment.
STAGES OF WOUND DRESSINGSIt is essential to recognise the significance of the clinicaltechnique used in the first dressing, which is usually ap-plied on admission. Inadequate pain management at thisstage will have lasting effects. The patient may, for exam-ple, dread subsequent dressing changes and lose confidencein the care team.
Atchison et al17 have analysed pain at different stagesof wound dressing and identified the most painful stageto be the removal of the innermost layer of gauze, whichusually adheres to some degree to the wound bed. This wasfollowed by debridement and topical applications.
TIME-COURSE OF PAINIt is important to note that post-dressing background painintensity is always greater than the pain experienced be-fore a dressing change. It has also been suggested that painincreases with the size of the burn17. The time it takes tochange the dressing will depend on the extent of tissuedamage, but dressings applied to the face and hands willtake longer than those applied to other parts of the body.In an unpublished study for the French national insurancesystem, burn specialists estimated that it took three peo-ple a total of 138 minutes (46 minutes per person) to dressa 10-30% burn (not involving the face or hands); 105minutes for three people to dress a facial burn (35 min-utes each); and 66 minutes for three people to change ahand dressing (22 minutes each) (this did not include theperson responsible for analgesia).
Skin graftingThe excision of non-viable tissue and the application ofskin grafts decreases the duration of a patient’s pain. Notonly will these procedures reduce the number of painfuldressings changes required, but the wound itself will alsofeel less painful, despite having undergone a surgical pro-cedure. The donor sites are likely to be painful for 48 to72 hours.
Fig. 1. 70% burn; first dressing with Alfentanyl alone.Total dose: 35 mg.

EWMA JOURNAL 2002 VOL 2 NO 2 7
Scientific Article
The first dressing following a skin graft is particularly sig-nificant, as the pain will be caused predominantly by theremoval of staples; an alternative is to use resorbablestitches to reduce trauma and pain. Donor-site dressingsshould be left in place until they peel away of their ownaccord.
Newly healed burnsIn a patient with newly healed burns, the pain and discom-fort experienced during dressing changes will originate inthe small unhealed areas or are related to other proceduressuch as concomitant physiotherapy.
ASSESSMENT OF PAIN INTENSITYIt is important that clinicians assess pain intensity to es-tablish the severity of pain and the effectiveness of anal-gesia. The pain experienced by burn patients varies greatlyfrom patient to patient3. For this reason treatmentprotocols stipulate low starting doses of analgesia, and al-low for adjustments to be made based on the individualpain assessment. For adults and children aged over seven,a visual analogue scale or a verbal numeric scale are excel-lent tools for assessing pain18. The picture-based ChildrenHospital of Eastern Ontario Pain Scale (CHEOPS)19 iswell suited to assessing burn procedural pain in youngchildren.
PHARMACOTHERAPYIV opioidsSome dressing changes are undertaken in a Hubbard tankor in theatre. However, because of the risk of cross-infec-tion, most dressings changes are carried out in the ward.Box 1 lists the requirements needed for optimal opioidanalgesic therapy at burn dressing changes.
Intravenous medications, especially IV opioids, are wellsuited to fulfill the requirements in Box 1. This is becauseIV morphine can be given in small incremental doses20,however, its delayed onset of action (10 minutes) and long-lasting effects (several hours) do not allow for the analge-sic therapy to be adjusted easily to meet individual needs.Therefore, short-acting medications such as fentanyl,alfentanil and remifentanil are more appropriate for painrelief in burn patients. When administered intravenously,alfentanil, a mu agonist, is a fast-acting medication – reach-ing peak effect in one minute. There is rapid pain relief andits relatively short duration of action (mean half-life 90minutes) fits well with the mean time taken to change adressing, providing good post-procedural analgesia. Clini-cal experience suggests a starting dose of 10mcg/kg, whichis repeated every minute according to the level of pain; themean starting dose for changing burn dressings has beenfound to be 22±12mcg/kg, with a mean total dose of29.9±18mcg/kg for procedures that take 41±20min21.Combining repeated boluses with a continuous infusionof 2mcg/kg/min is effective in improving pain relief (fig.1).
Remifentanil is even shorter acting; its quick and com-plete catabolism by plasmatic esterases makes it extremelyuseful in the case of high-risk patients, but because thedrug is short-acting it has the disadvantage of not beingcapable of providing lasting post-procedural pain relief.
Partial mu agonists or antagonists such as nalbuphineor buprenorphine are of little interest because of their lim-ited maximal efficacy (‘ceiling effect’).
The use of IV opioids for severe procedural pain does,however, have its drawbacks in that some patients mayrequire such high doses of analgesia, that there is an in-creased risk of apnoea and loss of consciousness. This canbe problematic during the first dressings of superficialburns, as patients may need to undergo extensive debri-dement of necrotic tissue. In these cases, to avoid subject-ing the patient to pain, the option of general anaesthesiashould be considered.
Box 1: Requirements for optimal analgesia atburn dressing changes• Ensure an adequately staffed and safe environ-
ment in which to care for sedated patients• Control severe acute pain due to nociception
(inflammatory response) during the painfulstages of the dressing (i.e. dressing removal,wound cleansing) by titrating analgesia topatient’s individual requirements
• Avoid over sedation during and following thedressing change, but ensure adequate post-procedural analgesia through frequent painassessment and monitoring of vital signs suchas respiratory rate and sedation level
• Avoid prolonged fasting whenever possible, asadequate nutrition and hydration is essentialfor the healing process
�

EWMA JOURNAL 2002 VOL 2 NO 28
Non-opioid IV drugsMidazolam and various anxiolytics should be used withgreat caution and only under expert supervision as they actsynergistically with opioids to potentially increase the riskof respiratory depression and reduced mental awareness.They should, therefore, be used to treat anxiety only, whichis usually anticipatory and can be reduced considerablywith efficient analgesia21 and thoughtful pre-procedurepreparation of the patient.
The option of involving a skilled anaesthetist in orderto use anaesthetic agents such as ketamine or propofolshould be considered for achieving ‘conscious sedation’22
versus general anaesthesia. Sub-anaesthetic doses ofketamine have been used extensively for many years, es-pecially in children in whom its unpleasant dysphoric sideeffects are less pronounced15,23. Low-dose propofol has alsobeen suggested for short procedures20, but its safety at thebedside remains questionable.
Oral medications for mild painOral morphine takes 30-90 minutes to reach peak effectand can be administered at least 60 minutes before thedressing change24; it is widely used in adults and children.The recommended starting dosage is 0.3mg/kg in chil-dren20, although clinical experience suggests that 0.5-1mg/kg may be more appropriate (fig. 2)21. The main draw-backs of oral morphine are:� its reduced and uncertain bioavailability (15%-50%)� it is not possible to give extra doses in response to
severe pain during the procedure (delay for peakplasma concentration: 30-90 minutes)
� the usually long post-procedural sedation.
For patients who have become intolerant to morphinethrough prolonged treatments, oral methadone25 can beused as an alternative.
Oral ketamine has also been used, although its effectscan be unpredictable. The recommended dosage is 10-20mg/kg)26.
Fentanyl lollypops are a more interesting alternative27;they have a rapid onset of action (within a few minutes)and a longer-lasting effect than IV fentanyl due to theirdouble mechanism of absorption (transmucosal and gas-tric).
Inhaled medicationsNitrous oxide (Entonox) is one of the most popular andsafest anaesthetic agents used with burn patients28. It hasa rapid onset of analgesia and can be used for the durationof the procedure. However, it has a very limited analgesicpotency and although it is widely prescribed there is no up-to-date published research on its use in burns29.
NON-PHARMACOLOGICAL THERAPIESRecent research30,31on the effects of distraction therapiesin reducing burn procedural pain shows that anticipationof pain increases pain intensity and discomfort, which canbe decreased by diverting the patient’s attention. Distrac-tion through use of interactive computerised virtual real-ity32, for example, can have a significant analgesic effect.The same is true for hypnosis, which is used extensivelyby a number of burn teams33. These supportive techniquesmay be time-consuming, but they can help to reduce thefeelings of fear and anxiety, especially during long proce-dures. However, they must always be used in conjunctionwith pharmacological treatments, and should never replacethem16.
PAEDIATRIC BURN PAINChildren aged between birth and four years old representapproximately 20% of all hospitalised burn patients34.Several studies show that procedural burn pain in childrenis largely underestimated and under treated4,5. However,these shortcomings can be overcome by adhering toprotocols similar to those used for adults, since thepharmacokinetic and pharmacodynamic differences be-tween children and adults are minimal.
For infants less than three months old, the adult opioiddosages must be divided by three because of hepatic andrenal immaturity35. In children older than three months,the pharmacokinetic effects are similar to those in an adult.In preschool-age children, the half-lives of morphine andalfentanyl are 50% those in adults, which explains the needfor higher dosages36. Despite some clinicians’ preconcep-tions, the pharmacodynamics of opioids, especially the
Fig. 2. 90 minutes after 1mg/Kg of oral morphine.

EWMA JOURNAL 2002 VOL 2 NO 2 9
effects of respiratory depression, are no different in infantsthan in adults37. Accidental over dosage mostly occursbecause of the difficulties of pain evaluation (overestima-tion) in children rather than the actual pharmacodynamicspecificity of a drug.
In addition, special attention should be paid to thechild’s environmental conditions. For instance, a parent’spresence and participation in the procedure can have ahighly beneficial effect38.
AMBULATORY PATIENTSAbout 95% of burn patients are treated on an outpatientbasis, but only 75% of these patients receive medicationat dressing changes39. There is scant literature on the sub-ject and, unfortunately, there are no published guidelinesfor best practice. In the author’s opinion, most protocolsinvolving short-acting IV opioids used at the bedside aresuitable for use in the outpatient setting provided there arefacilities for post-procedural surveillance.
14 Choinière, M. The pain of burns. In: Wall, P.D.,Melzack, R. (eds) Textbook of Pain (3rd edition).London: Churchill-Livingstone, 1994.
15 Latarjet, J., Lépine, O., Dorne, R. Use of ketamine inthe burned patient (1000 cases). Anesth Analg 1975;32: 763-781.
16 Choinière, M. Burn pain: a unique challenge.Pain Clinical Updates 2001; 9: 1-4.
17 Atchison, N.E., Osgood, P.F., Carr, D.B. Pain duringburn dressing changes in children: relationship toburn area, depth and analgesic regimen. Pain 1991;47: 41-45.
18 Choinière, M., Auger, F.. Latarjet, J. Visual analoguethermometer: a valid and useful instrument formeasuring pain in burned patients. Burns 1994;20: 229-235.
19 McGrath, P.A. Pain in Children. New York:Guilford Press, 1990.
20 Meyer, W.J., Marvin, J.A., Patterson, D.R. et al.Management of pain and other discomforts in burnedpatients. In: Herndon, D. (ed.) Total Burn Care.Philadelphia: W.B. Saunders, 1996.
21 Latarjet, J., Choinière, M. Pain in burn patients.Burns 1995; 21: 344-348.
22 Ebach, D.R., Foglia, R.P., Jones, M.B. et al.Experience with procedural sedation in a pediatricburn center. J Pediatr Surg 1999; 34: 955-958.
23 Slogoff, S., Allen, G.W., Wessels, J.V. et al. Clinicalexperience with sub-anesthetic ketamine. AnesthAnalg Curr Res 1974; 53: 354-358.
24 Nahata, M.C. Plasma concentrations of morphine inchildren with chronic pain. J Clin Pharmacol Ther1991; 16: 193-195.
25 Williams, P.I., Sarginson, R.E., Ratcliffe, J.M.Use of methadone in the morphine-tolerant burnedpaediatric patient. Br J Anaesth 1998; 80: 92-95.
26 Humfries, Y., Melson, M., Gore, D. Superiority of oralketamine as an analgesic and sedative for woundcare procedures in the pediatric patient with burns.J Burn Care Rehabil 1997; 18: 34-36.
27 Sharar, S.R., Bratton, S.L., Carrougher, G.J. et al.A comparison of oral transmucosal fentanyl citrateand oral hydromorphone for inpatient pediatricwound care analgesia. J Burn Care Rehabil 1998;19: 516-521.
References
1 Moffatt CJ, Franks PJ, Hollinworth H. Understandingwound pain and trauma: an international perspective.EWMA Position Document: Pain at wound dressingchanges 2002: 2-7.
2 Sheridan, R.L., Tompkins, R.G. Skin substitutes inburns. Burns 1999; 25: 97-103.
3 Choinière, M., Melzack, R., Rondeau, J. et al. Thepain of burns, characteristics and correlates. JTrauma 1989; 29: 1531-1539.
4 Foertsch, C.E., O’Hara, M.W., Stoddard, F.J. et al.Treatment-resistant pain and distress duringpaediatric burn-dressing changes. J Burn CareRehabil 1998; 19: 219-224.
5 Sheridan, R.L., Hinson, M., Nackel, A. et al.Development of a burn pain and anxiety manage-ment program. J Burn Care Rehabil 1997; 18:455-459.
6 Ulmer, J.F. Burn pain management: a guideline-based approach. J Burn Care Rehabil 1998; 19:151-159.
7 Andreasen, J.C., Noyes, R., Hart, C.E. et al.Management of emotional reactions in seriouslyburned adults. N Engl J Med 1972; 286: 65-69.
8 Schneiber, S., Galai-Gat, T. Uncontrolled painfollowing physical injury as the core trauma in post-traumatic stress disorder. Pain 1993; 54: 107-110.
9 Taal, L.A., Faber, A.W. Burn injuries, pain anddistress: exploring the role of stress symptomatology.Burns 1997; 23: 288-290.
10 Devor, M. The pathophysiology of damagedperipheral nerves. In: Wall, P.D., Melzack, R. (eds)Textbook of Pain (3rd edition). Edinburgh: ChurchillLivingstone, 1994.
11 Pedersen, J.L., Kehlet, H. Hyperalgesia in a humanmodel of acute inflammatory pain: a methodologicalstudy. Pain 1998; 74: 139-151.
12 Dickenson, A.H., Sullivan, A.F. Evidence of a role ofthe NMDA receptor in the frequency-dependantpotentiation of deep rat dorsal horn nociceptiveneurons following C-fiber stimulation. Neuropharma-cology 1987; 26: 1235-1238.
13 Pedersen, J.L., Kehlet, H. Secondary hyperalgesia toheat stimuli after burn injury in man. Pain 1998; 76:377-384.
28 Baskett, P.J.E. Analgesia for the dressing of burnsin children: a method using neuroleptanalgesia andEntonox. Postgrad Med J 1972; 46: 138-142.
29 Pal, S.K., Cortiella, J., Herndon, D. Adjunctivemethods of pain control in burns. Burns 1997; 23:404-412.
30 Peyron, R., Garcia-Larrea, L., Gregoire, M.C. et al.Haemodynamic brain responses to acute pain inhumans. Sensory and attentional networks.Brain 1999; 122: 1765-1779.
31 Rainville, P., Hofbauer, R.K., Paus, T. et al. Cerebralmechanisms of hypnotic induction and suggestion. JCogn Neurosci 1999; 11: 110-125.
32 Hoffman, H.G., Patterson, D.R., Carrougher, G.J. Useof virtual reality for adjunctive treatment of adult burnpain during physical therapy. A controlled study. ClinJ Pain 2000; 16(3): 244-255.
33 Patterson, D.R., Adcock, R.J., Bombardier, C.H.Factors predicting hypnotic analgesia in clinical burnpain. Int J Clin Exper Hypn 1997; 45: 377-395.
34 Van Rijn, O.J.L. The aetiology of burns in developedcountries: a review of the literature. Burns 1989; 15:217-221.
35 Kart, T., Christrup, L.L., Rasmussen, M. Recom-mended use of morphine in neonates, infants andchildren based on a literature review. PaediatrAnaesth 1997; 7: 5-11.
36 Olkkola, K.T., Hamunen, K., Maunuksela, E.L.Clinical pharmacokinetics and pharmacodynamics ofopioid analgesics in infants and children. ClinPharmacokinet 1995; 28: 385-404.
37 Lynn, A.M., Nemeska, M.K. Respiratory effects of IVmorphine infusion in neonates, infants and children.Anesth Analg 1993; 77: 695-701.
38 Doctor, M.E. Parents’ participation during painfulwound-care procedures. J Burn Care Rehabil 1994;15: 288-292.
39 Choinière, M. Prescribing Practices for Analgesia inAdults and Children with Minor Burns. Jerusalem:10th Congress of the International Society for BurnInjuries, 1998.
Scientific Article
CONCLUSIONThe question as to whether pain has a detrimental effecton the healing outcome for burn patients remains largelyunanswered and requires further investigation. The avoid-ance of patient suffering is, however, a key objective16 asunder-treated pain in burn patients can result in non-com-pliance with hospital treatment. This can disrupt care andincrease the risk of post-traumatic stress disorders.
In burn management the issue of pain at dressingschanges is generally overlooked. The future of burn carelies in ensuring optimal control of pain from the outset ofcare and application of the first dressing, through to theend of treatment. The process is technically feasible if cli-nicians, in the first instance, acknowledge that pain playsa crucial role in burn management. They must also acceptthe need to equip themselves with appropriate knowledge,and recognise the need to devote more time and fundingtowards the improvement of pain management for burnpatients. �

A JOINT MEETING BETWEEN EWMA, AISLeC and AIUCEWMA IN COOPERAZIONE CON AISLeC E AIUC
TEAMWORK INWOUND TREATMENT:THE ART OF HEALING
13TH CONFERENCE EUROPEAN WOUND MANAGEMENT ASSOCIATION
PISA 2003PISA’S
CONGRESS CENTER 22ND-24TH MAY·2003
www.ewma.org/pisa2003
The European Wound Management Association inco-operation with Italian Cutaneous Wounds Associationand Italian Association for Cutaneous Ulcers are verypleased to announce the 13th Conference of theEuropean Wound Management Association.
The conference gives the participants an opportunity tobenefit from high level scientific presentations, exchangedata and evaluate clinical practice.
The conference will be held in beautiful Italy in the cityof Pisa, world famous for its Leaning Tower. Combinedwith the Italian culture and cuisine the conferenceoffers the participants a unique experience both ona professional and social level.
Finn Gottrup, EWMA RecorderMarco Romanelli, Chairman, Local Organising Committee
Main Topics
What’s new in ResearchWound measurement
Gene-therapyEndpoints
Systemic Diseases, Wounds andInflammatory Ulcers
Management of Scarring &Burn Wounds
Diabetic Foot Management
Pressure Ulcers Management
Cost-Effectiveness &Reimbursement across Europe
•
•••••
Local Organising CommitteeMarco Romanelli, ChairmanGraziana Battaglia, SecretaryAldo CalossoAndrea CavicchioliRoberto PolignanoElia Ricci
Scientific CommitteeFinn Gottrup, RecorderSue BaleMadeleine FlanaganPeter FranksDeborah HofmanMarco RomanelliPeter Vowden

EWMA JOURNAL 2002 VOL 2 NO 2 11
�
Scientific Article
Prentice JL, Stacey MCResearch OfficerUniversity Department ofSurgery,Fremantle Hospital,Fremantle, PerthWestern Austalia 6160E-mail: [email protected]
INTRODUCTIONPressure ulcer research in Australia is in its infancy comparedto the cumulative bodies of work in the United Kingdom (UK)and United States of America (USA). Childs and Rimmington1,who conducted the first Australian pressure ulcer prevalencesurvey in 1983, recorded a prevalence of 4.5%. Since the mid1990’s the reported pressure ulcer prevalence in public hospi-tals has ranged between 4.5 and 19%.2-10 In private hospitalsthe range is 2 (personal communication H Purdy) to13.6%.11,12 Prevalence in the community is between 6 and8%.13,14 Prevalence in nursing homes is 3.4 and 5.4%.15,16
Incidence in hospitals ranges from 5.4 to 11%.9,17,18 Interpre-tation of the data from these surveys is difficult because of thediffering methodologies used as well as the differences withinthe clinical settings themselves.
In Australia, in 1997 and 1998, pressure ulcers were citedas the underlying cause of death in 101 cases. See Table 1. Theywere a contributing cause of death in a further 408 cases. (Per-sonal communication Australian Bureau of Statistics, Can-berra). Government expenditure on pressure ulcers in 1997 was$350M.19 In 1999 Porter and Cooter estimated that 60,000Australians annually would develop a pressure ulcer.28
Clinical practice guidelines (CPG’s) are systematically de-veloped statements that help clinicians and their patients tomake appropriate health care decisions in specific clinical cir-cumstances.21-24
They represent the clinical implementation of research andare applicable to clinical practice, preventative practice, anddiagnostic or prescribing practices. They made be used in acute,chronic or community care settings.21,25-27 CPG’s reportedlyimprove patient outcomes; reduce harmful, unsubstantiated orinconsistent clinical practice; reduce unnecessary use of goodsand services; improve knowledge; and promote continuity ofthe principles of care between institutions, clinicians, consum-ers, governing bodies and industry.21,24,26,28-35
Pressure ulcer guidelines were first developed in the Neth-erlands in 198536, the USA in 198923 and 199437,38 and inEurope in 1998.39 In 1996 the Australian Wound ManagementAssociation (AWMA) established a multidsciplinary Pressure
Evaluating AustralianClinical Practice Guidelinesfor Pressure UlcerPrevention
Summary
Aims: To prospectively evaluate the effec-tiveness of Australian guidelines for pre-dicting and preventing pressure ulcers, inconjunction with an education program,in reducing pressure ulcer prevalence.Secondly, to determine whether guide-lines improve clinician’s knowledge andmanagement of pressure ulcers.
Methods: A pre and postest approachwas used to assess pressure ulcer preva-lence and staff knowledge before andafter the release of the guidelines andeducation program in ten Australianteaching hospitals in 2000.
Results: In the pretest pressure ulcerprevalence survey the prevalence foundwas 26%. The postest prevalence wassignificantly reduced at 22% (p<0.01).Over 13,000 staff surveys have beendistributed over the two survey periods.Staff knowledge of pressure ulcer riskfactors is less than optimal. Constraintsto preventative pressure ulcer care havebeen identified.
Conclusion: A significant reduction inpressure ulcer prevalence has beendemonstrated following the introductionof the guidelines and education program.Staff knowledge is surprisingly poor.Constraints to clinical practice are lackof time, staff, education and supportsurfaces.

EWMA JOURNAL 2002 VOL 2 NO 212
Table 2Results of the Pre-test Prevalence Survey
Hospital Patients Seen Patients with Ulcers Prevalence
A (Perth) 579 78 13.4%
B (Melbourne) 231 72 31.1%
C (Sydney) 332 122 37%
D (Brisbane) 307 100 33.2%
E (Perth) 258 81 31.1%
Totals 1707 453 26.5%
Ulcer Interest Sub-Committee22, whose primary objectivewas to develop evidenced-based CPG’s for pressure ulcersfor Australian clinical settings. The guidelines contain rec-ommendations for clinical practice, which focus on riskfactors and risk assessment, skin care, support surfaces,documentation and risk management. The AustralianNational Health and Medical Research Council havereviewed these guidelines.
THE AIMS OF THIS STUDY WERE:1. To determine whether the introduction of Australian
guidelines for predicting and preventing pressureulcers together with an education program reducesthe prevalence of pressure ulcers.
2. To determine if there is a change in the clinicalpractice and knowledge of medical and nursing stafffollowing the introduction of guidelines for predict-ing and preventing pressure ulcers together with aneducation program.
METHODSHospital SelectionTen teaching hospitals in Perth, Melbourne, Sydney andBrisbane approved participation in this study. Selectionwas based on geographical location, like patient popu-lations, equitable case-mix loading, and other demographicsimilarities. Allocation of 5 hospitals to the prevalencesurvey group was based on patient numbers to meet sam-ple size requirements and the hospitals ability to fund oneprevalence survey.
Prevalence SurveysThese surveys were conducted on a specified day withineach facility on a rotational basis moving west to east acrossthe country. The pre and postest surveys were conductedsix months apart. The Study Investigator (SI) supervisedthese surveys to ensure consistency in interpretation of thestudy methods and data collection processes.
Interrater reliabilityInterrater reliability education and testing of surveyorsprior to the prevalence surveys was uniform across all sites.This involved theoretical and visual assessments of pres-sure ulcer staging according to the National Pressure UlcerAdvisory Panel of America’s definitions for Stage 1 to 4pressure ulcers. Potential surveyors were required to stage16 images of pressure ulcers from 35 mm colours slides andrecord their responses on a test paper. The test papers alsocontained 4 multiple choice questions about the NPUAPulcer staging framework. Nurses needed an eighty percentpass rate to function as a surveyor. Surveyors examined pa-tients in pairs and generally did not survey their own wardthus eliminating potential bias42.
Junior Medical and Nursing Staff Knowledge SurveysThese postal surveys were conducted on the same rota-tional basis as described above. They were, however, con-ducted in advance of the prevalence surveys in order toreduce any potential contamination of the data from aHawthorne effect. The survey forms were anonymous andincluded return addressed envelopes.
Education Program and Guideline DisseminationThe SI provided intensive in-service education on pressureulcers and the guidelines for one week after the first preva-lence survey at each site. Results of the prevalence surveyand reasons for the high prevalence were discussed at wardlevel. An Education Manual, that contains a series of in-dependent learning modules, tutorial notes and audiovisual aids, including a compact disk that supplementsinformation contained within the guidelines, was devel-oped to facilitate this program. The Co-Investigators at 4sites continued the education program for a further sixmonths and used a Logbook to record education given.
Data collection toolsThe prevalence survey instrument contained 24 variables.Data collected included patient demographics, electiveversus emergency admission, length of stay, risk status,
Table 1Australian deaths in 1997/98 with pressure ulcers asthe primary or secondary cause of death.
Age Range Male Deaths Female Deaths(years) 1997 1998 1997 1998
15-24 1 0 0 0
25-44 2 4 3 2
45-54 3 0 0 0
55-64 6 3 4 1
65-74 13 11 16 10
75-84 42 68 41 65
85+ 31 36 73 74
Totals 98 122 137 152

EWMA JOURNAL 2002 VOL 2 NO 2 13
Scientific Article
support surface in use and the location, stage and numberof ulcers found, and documentation of their management.
The staff questionnaires were a paper and pencil toolcontaining 26 variables. Staff have recorded their demo-graphics, use of risk assessment tools, knowledge of hos-pital pressure ulcer policies, constraints to clinical practiceand risk factors for pressure ulcer development. Two ad-ditional questions in the second survey will determine whoresponded to the first survey and who has seen the guide-lines. Data has been processed using the Optimal MarkRecognition Program (Remark™)
Inclusion and Exclusion criteriaThere are two study groups; inpatients on the day of thepoint prevalence survey in five hospitals, and junior medi-cal and nursing staff at all ten hospitals.
Pressure ulcer prevalence survey inclusion consisted ofall adult inpatients, who verbally consented to a full bodyskin inspection for evidence of pressure injury. If the pa-tient was unable to give consent this was sought from aclose relative or the patients’ doctor. Exclusion criteria werepaediatric, maternity and psychiatric patients. All nursingand junior medical staff at each hospital were eligible forinclusion in the staff survey. Return of the completed ques-tionnaire was taken as implied consent to participate.
Ethical ConsiderationsSkin inspection is a non-invasive everyday nursing action.With the exception of one hospital, verbal consent onlywas required for patient participation. All data has beenkept under secure conditions and no patient identifyingdata will be kept.
Sample Size and Statistical AnalysesThe sample size calculated for each prevalence survey wasa minimum of 1700 patients to give an 80% chance offinding a reduction of prevalence of 3% (from 12 to 9%)at 95% Confidence Intervals.
The sample size for the staff surveys was 70 respond-ents at each site to give an 80% chance of finding differ-ences in responses with 95% Confidence Intervals. Dataanalysis for each survey and comparison of the data be-tween the first and second surveys will be by Chi squaredanalysis.
Non-Responder SurveysDue to the low response rate to staff surveys non-respondersurveys were conducted to assess whether or not there wereany differences in responses given and to ascertain why staffdid not respond to the surveys.
Pilot StudyA Pilot Study was conducted in Fremantle Hospital in1999 to test study methods and data collection tools.Minor adjustments to the tools were made.
RESULTSIn the first prevalence survey 1707 patients underwent askin inspection; 453 patients were found to have one ormore pressure ulcers, a prevalence of 26.5% (range 13.4to37%). See Table 2.
A total of 884 pressure ulcers were found on these 453patients, 63% (n=555) were Stage 1, 31% (n=276) wereStage 2, 2% (n=17) were Stage 3 and 4% (n=36) wereStage 4. Sacral ulcers accounted for 25% of ulcers, heels20%, and elbows 10% with other sites constituting 45%of ulcers found. Eighteen per cent of ulcers were presenton admission. In 26% of cases clarification of the docu-mentation needs to occur before it can be determined ifthe pressure ulcer was present on admission or hospitalacquired. However, 251 patients were documented to nothave a pressure ulcer on admission, which is 56% of thetotal number of patients with pressure ulcers or 14% ofpatients surveyed. Fifty two per cent of patients had morethan one pressure ulcer and 23% had more than 3 ulcers.
Table 3Results of the Post-test Prevalence Survey
Hospital Patients Patients Prevalence PrevalenceSeen with Ulcers 2nd Survey 1st Survey
A (Perth) 599 101 16.8% 13.4%
B (Melbourne) 248 79 31.8% 31.1%
C (Sydney) 342 101 29.5% 37%
D (Brisbane) 319 55 17.2% 33.2%
E (Perth) 299 61 20.4% 31.1%
Totals 1807 397 21.9% 26.5%
�

EWMA JOURNAL 2002 VOL 2 NO 214
Prevalence rates were also analysed by sex and age. 24%male patients had a pressure ulcer, while 29% of femalesand a pressure ulcer. Amongst patients 64 and over, preva-lence was 16% and prevalence rose with age – 25% for65-74 year olds and 37% in people of more than 75 years.
Documentation of the existence, management orprogress of ulcers found, in the medical or nursing records,within the five days prior to the prevalence survey, wasabsent in 81.5% of cases. Risk assessments were completedon 36% of patients with pressure ulcers between the 1stand 3rd day of admission but had not been completed on60% of patients with a pressure ulcer. Only 59% of pa-tients with a pressure ulcer had a support surface in place.
Skin assessments were completed on 1807 patients dur-ing the second prevalence survey; 397 patients had one ormore ulcers: a prevalence of 22% (range 16.8 to 31.8%).See Table 3.
When comparing these two data sets by Chi-squaredanalysis the difference in prevalence found between the firstand second survey is statistically significant (p<0.01).
A total of 7,642 staff surveys were distributed across allten hospitals, in the first survey period.
Twelve hundred and twenty-one were returned givinga response rate of 16%.
Staff were asked to identify 10 risk factors, which theyfelt were most likely to predispose a patient to being at highrisk of developing a pressure ulcer. Their responses havebeen tabulated against the primary risk factors identifiedwithin the AWMA guidelines. See Table 4. Constraints toclinical practice that staff felt inhibited them in their abil-ity to provide preventative or correct treatment are listedin Table 5. A non-responder survey of this group identi-fied no differences in responses given.
Over 600 clinicians attended education sessions givenby the SI. Three hundred full versions of the guidelines and7,000 pocket guides were distributed across all ten hospi-tals.
DISCUSSIONA number of papers have reported that the introductionof pressure ulcer guidelines has led to reduced preva-lence.29,42-45 In Australia the Joanna Briggs Institute foundno significant change in prevalence with the introductionof guidelines in three Australian hospitals7. The methodo-logical approach they used to assess prevalence pre and postguideline intervention, may account for the low prevalencefound in both instances, and have been criticised by otherauthors.46
The prevalence of pressure ulcers found in the firstsurvey was considerably higher than expected. In particu-lar, the number of Stage 1 and 2 ulcers. In the interven-ing six months between the pre and post-test surveys hos-pitals C, D and E maintained a strong emphasis on edu-cation and guideline implementation and correction ofdeficits found at their respective sites. The resulting de-creases in prevalence at these sites are clearly identifiable,see Table 3. Less educational activity could be sustained inHospital B; consequently no change in prevalence wasachieved. The increase in Hospital A’s prevalence in thesecond survey may be due to several factors; lack of ongo-ing education and improved interrater reliability and datacollection. Consistency in the methodology used to assessprevalence in this study, adds validity to results found.
In the first staff knowledge survey pressure, shear andfriction have been poorly identified as risk factors by bothgroups; less than 1% for medical staff and less than 10%for nursing staff. Other factors most commonly identifiedwere peripheral vascular desease, changes in body mass in-dex, alterations in skin integrity and medications. Allmedical and 95% of nursing staff responded to this ques-tion, however, only 46% of medical and 40% of nursingstaff were able to list 10 factors. Data from the secondsurvey has yet to be analysed and compared to the firstsurvey.
Table 4Identification of Risk Factors by Medical and Nursing Staff(preliminary data)
Risk Factor % Medical Staff % Nursing Staff
Pressure 4.4% 4.4%
Shear 0.8% 6.5%
Friction 0.8% 9.3%
Immobility 84% 73%
Sensory Perception 69% 37.3%
Impaired Activity 43.3% 44%
Age 61% 55%
Chronic Illness 78% 57.2%
Nutrition 34% 70%
Moisture 42.4% 42.4%
Table 5Constraints to Providing Preventative Pressure Ulcer Strategies
Constraint % Medical % Nursing
Lack of in-service education 32% 31%
Lack of knowledge 28% 17%
Insufficient support surfaces 18% 88%
Lack of time 17% 32%
Lack of staff 12% 21%
Financial restraints 12% 11.5%

EWMA JOURNAL 2002 VOL 2 NO 2 15
Scientific Article
Education focused on the epidemiology of pressure ulcers in Australia andrelated costs. The chapters within the guidelines on aetiology, pathophysiol-ogy, risk factors, risk assessment, skin care, strategies for pressure offloading,documentation, collaborative practice and patient education and recommen-dations made were also summarised.
CONCLUSIONIt is evident that guidelines for the prevention and management of pressureulcers in Australian hospitals are required. Pressure ulcer prevalence remains highat 22%. Each site’s commitment to education and correction of deficits whichhave been identified correlate very clearly with changes in prevalence be they areduction, no change or an increase. Whether or not these guidelines haveengendered a change in clinician’s knowledge is yet to be determined.
It would appear, however, that clinical practice guidelines for pressure ulcerswhen introduced with an education program do reduce the prevalence of pres-sure ulcers. �
AcknowledgmentsCo-Investigators at each sitePatients who participatedNurse surveyorsRespondents to the staff surveys
The following organisations who haveprovided research funding for this project:
ConvaTec International ResearchNursing ScholarshipHuntleigh Foundation United KingdomHuntleigh Healthcare AustraliaNurses Memorial Centre Western AustraliaSmith & Nephew AustraliaWest Australian Wound Care AssociationWinifred Felle Education and Research Fund
References
1. Childs L & Rimmington PM. Decubitus Ulcers:a survey picture at two hospitals. ANJ 1983;13(1):35,52.
2. Martin RD & Keenan AM. The incidence andmanagement of pressure ulcers in a metropolitanteaching hospital. Primary Intention 1994; (2)2:31-34.
3. McGowan S, Hensley L & Maddocks J. Monitoringthe occurrence of pressure ulcers in a teachinghospital: A quality improvement project. PrimaryIntention 1996; 4(1):9-16.
4. Wright R & Tiziani A. Pressure ulcer pointprevalence study. Primary Intention 1996; 4(1):18-23.
5. Magazinovic N. Monitoring pressure sores – ahospital based audit. Proceedings: AustralianWound Management Associations Conference‘Breaking Down the Barriers’; 1996 Feb 21-23;Sydney.
6. Morey P, Porock D. A quality improvement surveyof pressure ulcers at a tertiary teaching hospital.Primary Intention 1997; 5(2):18-25.
7. Pearson A, Weichula R, Mitchell A & HodgkinsonB. Promoting best practice in the treatment andprevention of pressure ulcers. Evaluation CycleReport N1. Joanna Briggs Institute for EvidenceBased Nursing and Midwifery. 2000 In press.National Library of Australia Cataloguing-in-publication data ISBN Number: 0 9577796 4 x.
8. Pearson A, Francis K, Hodgkinson B & Curry G.Prevalence and treatment of pressure ulcers inNorthern New South Wales. Aust J Rural Health2000;8:103-110.
9. Charlier C. Prevalence, incidence and risk: a studyof pressure ulcers at a rural base hospital. PrimIntent 2001;9(1):12-21.
10. Young C, Stoker F. A four year review of pressureulcers prevalence. Primary Intention 2000;8(1):6-
11. Eves S. Prevalence of pressure ulcers in PrivateHospital. Primary Intention 2000;8(1):14-21.
12. Davenport J. Let’s take the pressure off. J ofStomaltherapy Aust 1999; 17(2):5-9.
13. Carville K & Lewin G. Caring in the community:A wound prevalence survey. Primary Intention1998;6(2):54-62.
14. Carville K. Wound Prevalence Survey: Departmentof Veterans Affairs Client Report. Silver ChainNursing Association 2000.
15. Madsen W & Leonard M. Monitoring pressureulcers in nursing homes. J Quality Clin Prac 1997;17:209-213.
16. Rice J. Where are the pressure ulcers? Posterpresentation: Australian Wound ManagementAssociations Conference ‘Breaking Down theBarriers’; 1996 Feb 21-23; Sydney.
17. Tobias T & Breakwell C. Predictors of pressure soredevelopment in an intensive care unit. 20th Australianand New Zealand Scientific Meeting on IntensiveCare. CACCN & ANZICS, 1995, Brisbane.
18. Young J, Morey P, Browne R & Nilolette S. A study onthe incidence of pressure ulcers in the acuteorthopaedic setting. Primary Intention 2000;8(4):142-147.
19. Woolridge M. Address at the Launch of the AustralianMedical Sheepskin, St Vincent’s Hospital, Melbourne,July 2nd, 1997.
20. Porter A & Cooter R. Surgical management ofpressure ulcers. Primary Intention 1999; 7(4):151-155.
21. National Health and Medical Research Council.A guide to the development, implementation andevaluation of clinical practice guidelines. AusInfoGovernment Bookshop 1998. Canberra ACT 2601.
22. Australian Wound Management Association. ClinicalPractice Guidelines for the Prediction and Preventionof Pressure Ulcers; 2001: Draft 8. In Press.
23. Bergstrom N, Allman RM, Carlson CE, et al. Pressureulcers in adults: prediction and prevention. Rockville,MD: Agency for Health Care Policy and Research,Public Health Service, US Department of Health andHuman Services; 1992. Clinical Practice Guidelines,No 3; vol AHCPR Publications No. 92-0047.
24. Marshall JK. A critical approach to clinical practiceguidelines. Can J Gastroent 2000;14(6):505-509.
25. Curry SJ. Organisational interventions to encourageguideline implementation. Chest 2000;118:40S-46S.
26. Grimshaw JM & Russell IT. Effect of clinical guidelineson medical practice: a systematic review. The Lancet1993;342:1317-22.
27. Mead P. Clinical guidelines: promoting clinicaleffectiveness or a professional. J Adv Nurs2000;31(1):110-6.
28. Roberts KA. Best practices in the development ofclinical practice guidelines. J Qual Healthcare1999;20(6):16-20.
29. Cervo FA. Pressure ulcers: Analysis of guidelines fortreatment and management. Geriatr 2000;55(3):55-60.
30. Costantini O. Attitudes of faculty, housestaff, andmedical students toward clinical practice guidelines.Academ Med 1999;74(10):1138-43.
31. Craft PS., Zhang Y., Brogan J., Tait N., BuckinghamJM & and the Australian Capital Territory and NewSouth Wales Breast Cancer Treatment Group.Implementing clinical practice guidelines:a community- based audit of breast cancer treatment.MJA 2000;172:213-216.
32. De Rosario JM. Overcoming 10 roadblocks toinitiating clinical practice guidelines. J HealthcareQual 1998;20(2):23-27.
33. Mitchell JP. Guideline implementation in theDepartment of Defense. Chest 2000;118(2):65S-69S.
34. Pearson MG. How can the implementation ofguidelines be improved? Chest 2000; 117(2):38S-41S.
35. Tillitson GS. Implementation and physician behaviourchange: An industry perspective. Chest 2000;118(2):59S-61S.
36. Clark M. Developing guidelines for pressure ulcerprevention and management. J Wound Care1999;8(7):357-9.
37. Bergstrom N, Bennett MA, Carlson CE, et al.Treatment of pressure ulcers. Rockville, MD: Agencyfor Health Care Policy and Research, Public HealthService, US Department of Health and HumanServices; 1994. Clinical practice guidelines No 15;vol AHCPR No 95-0652.
38. Rodeheaver GT. The US model for national standardsof care. J Wound Care 1995; 4(5):238-239.
39. European Pressure Ulcer Advisory Panel (EPUAP).Pressure ulcer guidelines 1998. London.
40. Joanna Briggs Institute for Evidence Based Nursing;1997(a). Pressure sores Part 1: Prevention of pressurerelated damage. Best Practice 1(1):1-6.
41. Joanna Briggs Institute for Evidence Based Nursing;1997(b). Pressure Sores Part 2: Management ofpressure related damage. Best Practice 1(2):1-6.
42. Xakellis GC, Frantz RA, Lewis A & Harvey P. Costeffectiveness of an intensive pressure ulcer preventionprotocol in long-term care. Adv Wound Care 1998;11(1):22-29.
43. Harrison MB, Wells G, Fisher A & Prince M. Practiceguidelines for the prediction and prevention ofpressure ulcers: evaluating the evidence. App NursRes 1996;9:1,9-17.
44. Sungkten G, Starr B & Ermer-Seltun J et al. Imple-mentation of a comprehensive skin care programacross care settings using the AHCPR pressure ulcerprevention and treatment guidelines. Ostomy &Wound Management 1996;42(2):20-30.
45. Regan MB, Beyers PH & Mayrovitz HN. Efficacy of acomprehensive pressure ulcer prevalence program inan extended care facility. Adv Wound Care 1995;8(3):51-55.
46. Whittington K, Patrick M & Roberts JL. A nationalstudy of pressure ulcer prevalence and incidence inacute care hospitals. JWCON 2000; 27:209-15.

*Trade Marks of Smith & Nephew©2002 Smith & Nephew
Wound Management Division,Smith & Nephew Medical Ltd.,PO Box 81, Hessle Road, HU3 2BNTel +44 (0)1482 225181 Fax +44 (0)1482 328326www.smith-nephew.com6551/CUTINOVAHYDRO/ADVERT/GLOBAL/0602
Hydro-selective*
- Incorporating a superfine polyurethane gel matrix, CUTINOVA Hydro selectivelyabsorbs mainly water from the wound fluid, leaving the patient’s own essentialgrowth factors and other proteins in the wound – important agents in woundhealing.1
H2OH2O
Clear- Semi-transparent polyurethane top layer allows for general observation
of the wound, saving nursing time, while reducing dressing changesand wound disturbance.2
No Gel Odour- CUTINOVA Hydro does not break down into a messy gel – a common source
of odour from wounds treated with hydrocolloids.6
Clean- Superabsorbing polymer within the polyurethane gel matrix retains excess
wound fluid in the dressing, preventing leakage and wound maceration.3,4,5
References:1. Achterberg V. et al. Hydroactive dressings and serum proteins:An in vitro study. Journal of Wound Care 1996;5:79-82. 2. McMullen D. et al.Clinical experience with a hydroactive dressing to treat stage II cutaneous ulcers. 3. Hutter M-J. Experiences with a hydroactive wounddressing. Vasomed Actuell 1991; 4:50-54. 4. Böttcher K. Experiences with the use of a hydroactive wound dressing for treating leg ulcers.Klinik Magazin 1991, No 2/3:44-46. 5. Andersson E. Report on a new hydroactive wound dressing for treating leg ulcers. Klinik Magazin1991;12: 20-22. 6. Thomas S et al. Hydrocolloids:A guide to the composition, properties and uses of hydrocolloid dressings and thecommercial presentations available. Journal of Wound Care 1992;1:27-30.
In an in vitro study, CUTINOVA Hydro outperformed other dressings in their ability to absorb mainly H2O from artificial wound fluid (i.e. human plasma),while leaving serum proteins behind.1
Con
cent
ratio
n(C
ontr
ol=
1.0)
00,0
ComfeelTM
CUTINOVA Hydro
VarihesiveTM
1,5
2,0
2,5
1,0
0,5
PDGF-AB (n≥7)Total protein (n≥10)
EGF (n≥6)bFGF (n≥5)
§
§§
§
§†
§ §† †
PDGF-AB: platelet-derived growth factor,EGF: epidermal growth factor,bFGF: basic fibroblast growth factor
§ Significantly different from control value (P<0.05)
† Significantly different from relative total protein value (P<0.05)
‡ Also branded DuodermTM
/ GranuflexTM
COMPARATIVE CONCENTRATIONS OF GROWTH FACTORS MAINTAINED IN THE WOUND FLUID1
CUTINOVA Hydro is a clear step forward in self-adhesive dressings for chronic, exudative wounds. It delivers the benefits of a hydrocolloid
without the drawbacks – no mess, no gel odour.
Cutinova* HydroYou may never
resort to hydrocolloids again.

EWMA JOURNAL 2002 VOL 2 NO 2 17
INTRODUCTIONThe work of Winter in the 1960s established theconcept of ‘moist wound healing.1 This principlehas contributed to the development of the pleth-ora of products that are currently available, amongwhich are hydrogels, hydrocolloids, alginates, andfoams or films. Some of these products also incor-porate antiseptics in their delivery systems.
However, it has become evident that ‘moistwound healing’ alone may not be sufficient toimprove wound healing outcomes. This is becauseeach wound type can have different barriers tohealing. Closure of surgical wounds is inhibitedby poor perfusion and infection. Delay in healingof a chronic wound, can result from pressure, ve-nous hypertension, poorly controlled diabetes,inadequacy of arterial inflow, vasculitis, repeatedtrauma or failure to debride necrotic tissue.
Recent advances in wound management incorpo-rate new technologies that “interact” with thewound either physically or at a cellular/molecu-lar level, rather than merely reducing moistureloss. These technologies include an array of phy-sical modalities such as ultrasound, hyperbaricoxygen, vacuum-assisted closure and woundwarming, as well as biological and tissue engi-neered materials that interact with the wound beddirectly to influence healing by delivering activeagents such as growth factors and protease inhibi-tors. Advanced wound dressings are becomingmore interactive, for example hydro-selective*dressings, which provide increased concentrationsof growth factors in the wound itself.
The integration of recent advances into clini-cal practice guidelines and protocols, combinedwith continuing education collaborations, makesthe future of wound management look very brightindeed. This paper reviews some of the recentadvances in wound management.
Professor David LeaperThe University Hospitalof North TeesStockton-on-TeesTS19 8PCUnited Kingdom
Mr. Battistino PaggiStrada Private Ghandi3 CameriNovara 28062Italy
Dr. Gregory A ComptonMedical DepartmentHebrew Home ofGreater Washington6121 Montrose RoadRockville MD 20852USA
Dr. Heather Orsted9003 33rd AvenueNorthwest CalgaryAlberta T3B 1M2Canada
Dr. Luc TeotService de Brules HospitalLapeyronie391 Avenue du doyenGiraud 34295Montpelier cedixFrance
Doz. Dr. med.H. M. OckenfelsLeimenstraße 2063450 HanauGermany
Growth Factors andInteractive Dressings inWound Repair
BACKGROUNDCare of wounds, including venous leg ulcers, dia-betic foot ulcers, and pressure ulceration, has beenestimated to consume £1 billion per year in theUK in direct costs alone2. In the USA, venous legulcers affect up to 2.5 million people3. They ac-count for 85% of all lower-extremity ulcers and areresponsible for treatment costs of $3 billion andloss of 2 million workdays per year4.
Delayed healing of wounds is common, especiallyin diabetes, venous and arterial insufficiency, andmay lead to infection, complications and disabil-ity as well as significantly increasing the cost ofcare5,6. Studies in both France7 and the USA8,9
have shown that larger wounds with delayed pres-entation take significantly longer to heal at ahigher cost.
Coordination of care and a high level of exper-tise are crucial to improving outcome in lowerlimb ulceration. Current treatment is widelyacknowledged to be fragmented, poorly taughtand inadequately researched10. Multidisciplinaryguidelines for the diagnosis and treatment of ve-nous leg ulcers have been shown in the USA andthe UK to improve accuracy in diagnosis and in-crease healing rates, resulting in significantly lowercosts4.
The fundamentals of wound care remain themost important elements of management andmust not be neglected in the drive for improvedtreatments2,11. Patients at risk or suffering frompressure ulcers require pressure relief. Those at riskof diabetic neuropathy require education in basicfoot care, pressure-off loading footwear and regu-lar debridement of calluses. Compression therapypromotes rapid healing of venous leg ulcers, givesreliable, cost-effective healing in most patients12
and is the first line treatment of choice for patientswithout significant arterial disease13.
* Trademark of Smith & Nephew plc
�
Scientific Article

EWMA JOURNAL 2002 VOL 2 NO 218
NEW UNDERSTANDING INWOUND CARE PATHOPHYSIOLOGYNormal wound healing is a well orchestrated and complexseries of events which passes through overlapping phasesof inflammation, granulation, epithelialisation and remod-elling2,11,14. Each phase is modulated by a vast array ofcytokines and growth factorsA, which form an elaboratecommunication network co-ordinating the healing proc-ess. New understandings in the complexities of woundhealing, and particularly the role of growth factors, areenabling clinicians to manage superficial wounds such asskin flaps and even the most difficult-to-heal wounds moreeffectively.
The inflammatory phase of wound repair starts almostimmediately after wounding and lasts for three to five days,when classic symptoms of oedema, erythema, heat andpain are prominent. Initially, blood vessels constrict to haltblood loss and platelet activation promotes fibrin clot for-mation. Then, substances released by platelets stimulatecoagulation, vasodilation and increased capillary perme-ability, allowing an outpouring of biologically active cellsand chemicals to the wound area. Protein-rich serum leaksinto the interstitial space and combines with the evolvingclot to produce a fibrin plug, temporarily closing thewound. Inflammatory cells build on the fibrin scaffold toproduce a temporary matrix for tissue repair.
Many growth factors also accumulate in the woundfluid. Growth factors are chemical signalling agents, mainlyproteins, released by platelets initially and then by cells at-tracted to the wound site. They have a wide variety of keyfunctions in cell growth and maintenance, cell migrationand healing. They stimulate and control many woundhealing processes including inflammation, epithelialisation(generating new epidermal skin), fibroplasia (forminggranulation tissue), angiogenesis (new blood vessel growth)and scar formation.
Wound fluid contains many growth factors including thefollowing:� platelet-derived growth factor (PDGF),� transforming growth factor alpha and beta
(TGF� and TGF�),� epidermal growth factor (EGF),� insulin growth factor 1 (IGF-1)14.These play an important role in initiating tissue repair byattracting cells such as white blood cells, macrophages,fibroblasts and smooth muscle cells to the wound site.They also promote cell division.
Cytokines such as granulocyte macrophage colonystimulating factor GM-CSF (are released from platelets,and interleukin-1 (IL-1), which is a cytokine promotingfurther growth factor secretion, is released from the epi-dermis of wounded skin14.
Neutrophils flood into the wound site early on to containcontaminating bacteria and release proinflammatorycytokines, including tumour necrosis factor alpha (TNF-�) and IL-1�. Along with PDGF, cytokines attractmacrophages which engulf debris and are essential towound healing. Once recruited the macrophages releasemore growth factors, including PDGF, TNF-� and TGF�.
These growth factors play a crucial role in stimulatingthe subsequent proliferative (granulation) phase in heal-ing, which may last three weeks or more. As granulationtissue is formed, the wound contracts and finally epithe-lial cells move across the newly formed wound bed to closethe wound. Until closure macrophages continue to pro-duce cytokines to stimulate fibroplasia, epithelializationand angiogenesis. Angiogenesis is under the control ofmultiple growth factors including VEGF, FGF2, FGF1,TGF� and TGF�.
Growth factors also attract and stimulate fibroblasts,cells that produce an extracellular matrix to give strengthand structure. These stimulated fibroblasts themselves pro-duce growth factors, including PDGF, creating a feedbackloop and amplifying the wound repair process. Fibroblasts
A. Cytokines are a unique family of growth factors. Secreted primarily fromleukocytes, cytokines stimulate both the humoral and cellular immuneresponses, as well as the activation of phagocytic cells.
The stages of wound healing

EWMA JOURNAL 2002 VOL 2 NO 2 19
then undergo sequential alterations to differentiate intospecialised cells, which have been named as myofibroblasts,which pull the wound edges together.
Other specialised cells called keratinocytes (epithelial)are also attracted by growth factors and re-epithelialise andrepair the epidermis, and secrete more growth factors.Gradually a closed but immature new surface of weak,temporary tissue is formed.
This immature scar tissue is finally shaped andstrengthened during the remodelling phase, which lasts forsix to 12 months or longer and involves a balance betweenmatrix degradation and formation, again controlled bygrowth factors, particularly TGF�, PDGF and FGF. Theultimate result is a stronger scar with ultrastructural andmechanical properties14, which has about 80% of the ten-sile strength5 of uninjured skin.
IMPAIRED HEALINGThe normal healing process can be impaired by many fac-tors including infection or ischaemia; systemic factors suchas malnutrition, diabetes and old age, and factors specificto chronic wounds such as impaired growth factor produc-tion, enzyme imbalance and the presence of senescentcells2.
Treatment protocols must address both intrinsic andextrinsic factors contributing to delayed wound heal-ing2,5,6. Adherence to the principles of good wound bedpreparation is equally important. Neglecting any one ofthese may delay or prevent wound closure6.
Chronic wounds contain decreased levels of some in-trinsic growth factors, including PDGF, basic fibroblastgrowth factor, EGF and TGF�, compared with acutewounds2, and such deficiencies are at least partly respon-sible for impaired healing in diabetic patients15 and otherchronic wounds. PDGF in particular is active at all stagesof wound healing6. Interventions such as moist woundhealing and external application of PDGF can increase thenumber of diabetic ulcers achieving complete healing andreduce the time taken to achieve complete healing16. Un-fortunately the relationship between the presence / absenceof growth factors and impaired wound healing is not sim-ple, as some chronic wounds have increased levels of in-flammatory cytokines, and have been described as high-turnover systems with high rates of cell deposition andhigher rates of cell remodelling, leading to overall tissueloss.
MAJOR ADVANCES IN DRESSINGTECHNOLOGYThe concept of moist wound healing, developed in the1960s, prompted the search for active wound dressings topromote healing11, and many products are still describedin terms of their ability to promote moist wound healing17.Occlusive and semi-occlusive dressings effectively create amoist wound healing environment and, in addition toincreasing re-epithelialization2, may promote dermal ma-trix synthesis and improve comfort18.
Dressings that claim to maintain a moist wound envi-ronment include films, hydrocolloids, alginates, foams andhydrogels. Hydrocolloids were first launched in the 1980sfor their abilities to maintain a moist wound environmentand provide a low oxygen tension at the wound interface19.However, this impermeability to oxygen makes them un-suitable for anaerobic infection, and their performance iscompromised by excessive exudate20. Hydrocolloid dress-ings are thought to reduce pain, rehydrate the skin19 andaid autolytic debridement21, but have generally beensuperceded by more advanced wound dressings.
I. Growth factorsBecaplermin (RegranexTM), a human PGDF launched in1998 to treat chronic diabetic neuropathic ulcers22, is thefirst recombinantB growth factor approved by the US Foodand Drugs Administration (FDA) for this purpose. It hassimilar activity to endogenous PDGF 5,16,23 and, in con-junction with good wound care, several small scale clini-cal trials have suggested an improvement in healing timein diabetic ulcers compared with standard wound careregimens5,16,22,23 and in wound closure rate in diabeticneuropathic ulcers6,23.
However, good wound care remains important evenwith new approaches. Wound debridement before becap-lermin application is directly correlated with healingrates23. Debridement removes necrotic tissue and increasesthe number of available receptors for applied drugtherapy6. Although clinical results from topical growthfactors have not been as dramatic as was first hoped2, andbecaplermin is expensive, its use combined with goodwound care is generally more cost-effective than amputa-tion.
B. produced by recombinant DNA technology
�
Scientific Article

EWMA JOURNAL 2002 VOL 2 NO 220
Other products at the research stage include granu-locyte colony stimulating factor (GCSF, FilgrastimTM),which aims to promote speedier resolution of infection indiabetic foot ulcers; fibroblast growth factor for pressureulcers, and epidermal growth factor for venous ulcera-tion2,24. In future, more sophisticated systems can be ex-pected, such as administering growth factors sequentially,in combination or at timed intervals in an attempt tomimic the normal healing process2.
Other wound-specific products include HyaffTM, an es-ter of hyaluronic acid, which is a major component of hu-man skin24. Dressings that deliver hyaluronic acid to thewound claim to promote healing by correcting abnormali-ties in the healing cascade2. There is little evidence to datethat this technology speeds healing.
The use of growth factors in different countries willvary depending upon the resources available to purchasethem and a demonstration of their cost effectiveness inlocal settings.
II. Skin substitutesAn alternative approach to regrowth and repair is to replacethe damaged skin. Autologous skin grafts have been suc-cessfully used for both venous and pressure ulcers for sometime2. There are a number of limitations including pain,scarring, infection and slow healing at the donor site25.
Cultured epidermal autografts, large sheets of skin cul-tured from a small biopsy sample, were developed to treatburns patients but have had limited success due to delay(3 weeks) in producing sufficient skin for a graft, fragilityand difficulty in application, poor uptake and high infec-tion rates2,25. Cultured epidermal allografts which can becryopreserved and banked, potentially avoid this delay25.
More recently, bioengineered skin equivalents havebeen developed using donor tissue with no reportedimmunogenicity and have improved success. Approvedindications include diabetic and venous ulcers and donorsites in burn patients.
DermagraftTM is a human fibroblast-derived dermalsubstitute containing metabolically active living cellsgrown on a 3-D scaffold that produce normal growth fac-tors and matrix proteins25,26 found in human dermis. Ithas been shown in randomised controlled clinical studiesto heal more diabetic foot ulcers and heal them faster thanconventional therapy, perhaps indicating an improvedquality of wound healing27. Demagraft is approved for thetreatment of diabetic foot ulcers in the USA and SouthAfrica. In Canada and Australia, the product is approvedfor use on chronic wounds.
Apligraf is a bilayered skin substitute consisting of twotypes of living human skin cells – epidermal keratinocytesand dermal fibroblasts. The manufacturing process enablesthe skin cells to establish the natural organisation they havein skin. Randomised controlled clinical studies have shownthat Apligraf heals more venous and diabetic foot ulcersthan conventional therapy. It is licensed for both types ofulcers in Canada Switzerland, USA and Israel. At the timeof going to press the manufacturers of Apligraf had termi-nated their distribution agreement with Novartis and hadfiled Chapter 11 bankruptcy protection. Novartis andOrganogenesis are currently in negotiations to try to en-sure that Apligraf is brought back to the market.
In future skin equivalents developed from stem cellsmay be developed, and there is potential for gene therapyto deliver genes important in healing directly into thewound2.
III. Hydro-selective* dressingsRecently, a new category of dressings has emerged as anaid to wound management. Hydro-selective dressings in-teract with serum proteins and cellular components in thewound exudate. They are fluid-retentive, to minimisemaceration and leakage, and semi-occlusive to promotemoist wound healing.
PDGF-AB: platelet-derived growth factorEGF: epidermal growth factorbFGF: basic fibroplast growth factor§ Significantly different from control value (P<0.05)† Significantly different from relative total protein value (P<0.05)‡ Also branded DuoDERM™/Granuflex™
CUTINOVA™ Hydro allows only watwer to passinto the dressing, whilst leaving behind the pa-tient’s own growth factors in the wound.
�
Scientific Article

Kick-startthe wound healing process with silver
When the healing of wounds is delayed or stop-ped, the antibacterial properties of the silver contained in Contreet can wake up the healing process by giving wounds the boost they need. Silver is released according to the amount of exudate and bacteria present in the wound. The more exudate present, the more silver is released.
Contreet offers the unique combination of:· Hydroactivated sustained silver release· Moisture control for optimal wound healing· Effective exudate management
This combination of features in one dressing is the most efficient way to deal with the bacterial burden of delayed healing wounds.
Contreet – get healing started
Coloplast A/SHoltedam 1DK-3050 HumlebækDenmark
www.contreet.com

EWMA JOURNAL 2002 VOL 2 NO 222
An early in vitro study28 incubated four types of dress-ing with artificial wound fluid, two based on hydrocolloidsand two on polyurethane. One of the two polyurethane-based dressings gave a two-fold increase over control val-ues of all proteins tested (albumin, immunoglobulin,PDGF-AB, bFGF and EGF). This dressing was Cutinova*Hydro, currently the only ‘Hydro-selective’ dressing avail-able. This is in comparison to other moist-wound dress-ings, which indiscriminately absorb wound fluid and itscontents.
Based on early studies, the increased concentration ofgrowth factors and proteins demonstrated by hydro-selec-tive dressings may enhance healing. The dressings wereshown to accelerate epithelialisation in experimentalwound models and to yield significantly better early heal-ing of acute facial wounds, with short-term improvementsin comfort and contour, less erythema and less potentialfor scarring compared with a dry-gauze dressing18.
A surveillance study by general practitioners treating874 patients, showed that hydro-selective dressings yieldeda 25% complete healing rate in those 612 patients with legulcers at five weeks, with a further 61% of these patientsshowing reductions in ulcer size. A reduction in woundarea was seen after five weeks in 93% of patients with pres-sure ulcers or diabetic leg ulcers, and out of a group con-sisting of 173 patients with chronic ulcers that have beenunresponsive to other treatment for more than a year, 138(79.8%) showed a reduction in wound area after fiveweeks. Overall, 86% of patients readily accepted the noveltreatment. These results demonstrate that hydro-selectivedressings can promote wound healing among a variety ofdifferent wound types and typical general practice patients,mostly elderly and often with chronic wounds.
Comparative studies are now required to quantify theimpact of these hydro-selective dressings compared withother dressing types.
Hydro-selective dressings have been used on neuro-pathic foot ulcers in diabetics and on leg ulcers, sacral pres-sure ulcers, traumatic and infected surgical ulcers, and
found to conform to the wound surface with ease in flator slightly depressed ulcers. Hydro-selective dressings havebeen designed so that when correctly applied, the sur-rounding skin remains dry despite the pressure exerted bythe wound exudate.
Hydro-selective dressings are designed to lose their ad-herence over the moist wound bed and this may reducepain at dressing changes. Moreover, the dressing materialdoes not liquefy and can be removed in one piece. Hydro-selective dressings do not react with wound fluid to createthe odorous gel associated with some hydrocolloids.
Reduction of pain and odour are desirable character-istics for a dressing given the importance of patient com-pliance to a successful outcome of wound treatment. Pa-tients generally report severe impairment of their qualityof life as a result of ulceration29 and around 30% reportpain during dressing changes.
CASE STUDY USING NEWHYDRO-SELECTIVE DRESSINGSIntroductionThis case study illustrates the use of Cutinova Hydro inthe management of a vasculitic ulcer.
PatientThe patient was a 77 year-old female with three progres-sively worsening wounds on the lower right limb and ahistory of hypertension. The wounds consisted of one me-dial, 18�14 cm, necrotic with exposed fascia, and twolateral, 5�5 cm, involving the subcutaneous fat (Figs. 1and 2). The wounds had been present for six months. Thepatient had previously been treating herself with local an-tiseptics, local antibiotics and gauzes.
The patient was admitted to hospital for diagnostictests, which revealed the presence of vasculitis. Pentoxi-fylline (oxpentifylline) and corticosteroids were adminis-tered orally.
Fig. 2. Medial wound at admission.Fig. 1. All three wounds at admission.

EWMA JOURNAL 2002 VOL 2 NO 2 23
Wound TreatmentInitially, wound treatment included surgical debridementand alginates. Low compliance was observed and the treat-ment phase required approximately three months.
Once the wound bed appearance had improved,Cutinova Hydro dressing was used. Dressing changes tookplace every 48 hours. A tubular bandage was used to keepthe medication in place and to obtain gentle compression(TensogripTM, size E).
After seven days, the patient showed good toleranceand acceptable comfort levels while moving around. Anexamination carried out at week eight revealed a reductionin exudate levels. As a result, frequency of treatment wasreduced to once every 72 hours.
ResultsAfter 12 weeks, the lateral lesions had healed (Fig 3) andthere was a marked reduction in the medial lesion. Dress-ing changes were consequently carried out once every fivedays. At week 16 the remaining lesion was 2�1 cm.
Conclusion / Outcome / Follow-up careThe topical treatment of vasculitis remains controversial;vasculitic wounds are often difficult to heal and theirprogress is not always linear.
In this patient’s case, Cutinova Hydro was importantas a bacterial barrier, while proper management of the exu-date allowed linear progress to be maintained.
CONCLUSIONChronic dermal wounds are difficult to heal and requirecomplex treatment procedures. Improved understandingof the pathophysiology of wound healing has enabled sig-nificant therapeutic developments. A wide variety of dress-ing options are available and new ones are being continu-ously introduced. Hydro-selective dressings build upon ourknowledge of the importance of growth factors in woundrepair and thus represent a major innovation in modernwound management. �
Fig. 3. Two lateral wounds healed after 12 weeks.
Scientific Article
References
1 Winter GD. Formation of the scab and the rate of epithelialisation of superficialwounds in the skin of the young domestic pig. Nature (Lond) 1962; 193: 293-4
2 Harding KG, Morris HL, Patel GK. Healing chronic wounds. BMJ 2002;324: 160-3
3 Phillips TJ. Current approaches to venous ulcers and compression. Dermatol Surg2001; 27 (7): 611-21
4 McGuckin M, Waterman R, Brooks J et al. Validation of venous leg ulcer guidelinesin the United States and United Kingdom. Am J Surg 2002; 183 (2): 132-7
5 Stegbauer CC. Enhanced wound healing using topical recombitant human platelet-derived growth factor. Nurse Pract. 2000;25(10):85-9
6 Mulder GD. Diabetic foot ulcers: old problems - new technologies. Nephrol DialTransplant. 2001;16:695-8
7 Levy E, Levy P. [Management of venous leg ulcer by French physicians, diversity andrelated costs: a prospective medicoeconomic observational study] J Mal Vasc 2001;26(1): 39-44
8 Pompeo MQ. The role of “wound burden” in determining the costs associated withwound care. Ostomy Wound Manage 2001; 47(3): 65-71
9 Phillips TJ, Machado F, Trout R et al. Prognostic indicators in venous ulcers. J AmAcad Dermatol 2000; 43(4): 627-30
10 Samson RH, Showalter DP. Stockings and the prevention of recurrent venous ulcers.Dermatol Surg 1996;22: 373-376
11 Natarajan S, Williamson D, Stiltz AJ, Harding K. Advances in wound care andhealing technology. Am J Clin Dermatol. 2000 Sep-Oct;1(5):269-75
12 Marston WA, Carlin RE, Passman MA et al. Healing rates and cost efficacy ofoutpatient compression treatment for leg ulcers associated with venous insufficiency.J Vasc Surg. 1999; 30(3): 491-8
13 Turner-Boutle M, Fletcher A, Sheldon T, Cullum N. Compression therapy for venousulcers: a systematic review. Nurs Times 1997;93(39):52-3
14 Moulin V. Growth factors in skin wound healing. Eur J Cell Biol 1995;68:1-7
15 Bitar MS, Labbad ZN. Transforming growth factor-beta and insulin-like growthfactor-I in relation to diabetes-induced impairment of wound healing. J Surg Res1996;61(1):113-9
16 Embil JM, Papp K, Sibbald G et al. Tecombinant human platelet-derived growthfactor-BB (becaplermin) for healing chronic lower extremity diabetic ulcers: an open-label clinical evaluation of efficacy. Wound Repair Regen. 2000;8:162-8
17 Rudolph D. Standards of care for venous leg ulcers: compression therapy and moistwound healing. J Vasc Nurs 2001; 19(1):20-7
18 Thomas DW, Hill CM, Lewis MA et al. Tandomized clinical trial of the effect of semi-occlusive dressings on the microflora and clinical outcome of acute facial wounds.Wound Repair Regen. 2000;8(4): 258-63
19 Moffatt CJ, Dickson D. A trial of a hydrocolloid dressing in the management ofindolent ulceration. J Wound Care 1992; 1(3):20-22
20 Tallon RW. Wound care dressings. Nurs Management 1996; 27(10):68-70
21 Hofman D. Know how: a guide to wound debridement. Nurs Times. 1996 Aug 7-13;92(32):22-3
22 Barry M. How growth factors help chronic wounds heal. Nursing. 2000 May;30(5):52-3
23 Ladin D. Becaplermin gel (PDGF-BB) as topical wound therapy. Plastic SurgeryEducational Foundation DATA Committee. Plast Reconstr Surg. 2000;105(3):1230-1
24 Edmonds M, Bates M, Doxford M et al. New treatments in ulcer healing and woundinfection. Diabetes Metab Res Rev. 2000;16 Suppl 1:S51-4
25 Bello YM, Falabella AF, Eaglstein WH. Tissue-engineered skin. Current status inwound haling. Am J Clin Dermatol 2001;2(5):305-13
26 Naughton G, Mansbridge J, Gentzkow G. A metabolically active human dermalreplacement for the treatment of diabetic foot ulcers. Artif Organs1997;21(11):1203-10
27 Gentzkow GD, Iwasaki SD, Hershon KS et al. Use of dermagraft, a cultured humandermis, to treat diabetic foot ulcers. Diabetes Care. 1996;19(4):350-4
28 Achterberg V, Meyer-Ingold W. Hydroactive dressings and serum proteins: and invitro study. J Wound Care. 1996;5(2):79-82
29 Phillips T, Stanton B, Provan A et al. A study of the impact of leg ulcers on quality oflife: financial, social and psychologic implications, J Am Acad Dermatol 1994;31: 49-53
The Tendra® product Mepilex® Border is a revolution in wound management.
Mepilex Border is a self-adherent, absorbent dressing with the soft silicone technology, Safetac®. The unique
Safetac technology combines sufficient adhesion with minimal trauma to the wound and to the surrounding skin
on removal.1, 2
Safe fixation, safe removal
®
References: 1) Dykes P et al. The Effect of Adhesive Dressings on the Stratum Corneum of Normal Skin. Journal of Wound Care, 2001;10:2:7-10.2) Karlsmark T. et al. Data on file.
Mölnlycke Health Care, Box 13080, 402 52 Göteborg, Sweden Phone. +46 31 722 30 00, Fax. +46 31 722 34 00, www.tendra.com
EWMA JOURNAL 2002 VOL 2 NO 2 25
When faced with a clinical question re-garding the best interventions to pre-vent and treat wounds, patients and
clinicians are probably best served by finding anup-to-date, reliable systematic review that summa-rises the reliable information available in this area.Fortunately, there are a number of useful system-atic reviews available; for example, the review byCullum et al of the effectiveness of beds, mat-tresses and cushions for preventing and treatingpressure ulcers1. But what if the question posedis not answered by the available evidence? Thereview by Cullum et al, for example,) includes ran-domised controlled trials evaluating support sur-faces in all healthcare settings for people of any ageand all levels of risk. However, there were no s thatevaluated the effectiveness of support surfaces inthe prevention of pressure ulcers in children. Theabsence of evidence does not help the clinician orpatient, although it can be reassuring if a quality,up-to-date systematic review has found no evi-dence. This means one’s lack of success was notdue to a lack of skill in finding the evidence orobtaining a copy of it, but in the research’s lackof evidence. That having been said, the clinicianand patient are still faced with their decision. Inthis case, there are a number of responses:1. look for ongoing trials that you could con-
sider joining.2. look for recently completed trials that are
about to be published – so that you can lookout for the information as soon as it reachesthe public domain.
3. if there are no ongoing, or recently com-pleted trials, in this area, alert the researchfunders that there is a desperate need forresearch in the area.
One way of identifying ongoing and recentlycompleted trials is to contact all the local organi-sations that might fund such research and askwhether they have funded research in that area.However, this is a mammoth undertaking; thereare dozens of research funders in each EuropeanCountry (Universities, Companies, Charities,Government etc) and this also misses out the
Contemporary Research in PressureUlcer Prevention and Treatment from themeta Register of Clinical Trials (mRCT)
research in the rest of the world that may also berelevant. One obvious solution is to use a com-bined register of research funders.
The meta Register of Clinical Trials (mRCT)is a major, international, searchable database of on-going randomised controlled trials in all areas ofhealthcare compiled from registers held by pub-lic, charitable and commercial sponsors of trials.At the moment, the mRCT also contains somecompleted trials. The mRCT is a free service thatallows users to search all participating registers, allof which are asked to submit trial records includ-ing specified essential data items. Where moredetailed entries are available in the original regis-ter, links are available to the source websites.
The mRCT has been set up to provide a serviceto the following groups:1. people using evidence from controlled trials
who want to be confident that they areaware of all of the trial evidence relevant toa particular question;
2. research funding agencies (public, commer-cial and charitable) who want to take theirfunding decisions in the light of informationabout relevant ongoing research, both toavoid duplication of effort and to promotecollaboration;
3. patients, participants, clinicians and otherdecision-makers who wish to be informedabout trials in which they can participate orto which they can contribute in other ways.
The mRCT was established in response to an ini-tiative taken in the UK in July 1998 that broughttogether representatives from the UK MedicalResearch Council, the National Health Service Ex-ecutive, medical charities, pharmaceutical compa-nies, the UK Cochrane Centre, and journals suchas the British Medical Journal and The Lancet.
The active involvement of a major interna-tional drug company – GlaxoSmithKline – andsubsequent commitments from other interna-tional organisations, meant that the scope of themRCT quickly extended outside Britain. �
E. Andrea NelsonPhD RGNResearch Fellow,Department ofHealth Sciences,University of York, UK.EWMA Treasurer andEditor of EWMA Journal.
Scientific Article

EWMA JOURNAL 2002 VOL 2 NO 226
The editors of the Lancet and British Medical Journal2
stated that ‘the case for registering all clinical trials, firstadvanced a decade ago – is now unanswerable. The pub-lic has the right to know what research is being funded.Researchers and research funders don’t want to waste re-sources repeating trials already underway. And those con-ducting systematic reviews need to be able to identify alltrials begun on a subject to avoid the problem of publica-tion bias. Otherwise clinicians may be deceived on whatthe evidence shows.’
The mRCT currently contains records from the registersof s of the following organisations:� Action Research� Alzheimer’s Society� Arthritis Research Campaign� British Heart Foundation� CTSU - trials being randomised by the Clinical Trial
Service Unit, Oxford� Canadian HIV Trials Network� Cardiosource� GlaxoSmithKline� Hong Kong Health Services Research Fund� Laxdale Ltd� Leukaemia Research Fund� Medical Editors’ Trials Amnesty� Medical Research Council (UK)� National Health Service Research and Development
Health Technology Assessment (HTA) Programme� National Health Service Research and Development
Programme ‘Time-Limited’ National Programmes� National Health Service Research and Development
Regional Programmes� National Institutes of Health (NIH) – records held
on NIH ClinicalTrials.gov website.� National Research Register (UK)� PPP Foundation� Schering Health Care Limited� Sir Jules Thorn Charitable Trust� South Australian Network for Research on Ageing� UK Co-ordinating Committee on Cancer Research� US Department of Veterans Affairs Co-operative
Studies Program
All trials records are in English; a brief introduction toCCT has been prepared in French, German, Spanish, andItalian, and other languages will be added in the future.
People, anywhere in the world, who wish to promoteand implement prospective registration of randomisedcontrolled trials, are invited to participate in this endeav-our. Please contact [email protected], or visit thewebsite at http://controlled-trials.com/
mRCT AND WOUND MANAGEMENTA search of mRCT on the 1st October 2002, found 120reports of trials in wound management, including evalu-ations as diverse as ‘Silicone Based Dressings in WoundHealing’ and ‘Assessment of Air and Wound BacteriaCount Methods in Ultraclean Air Using a Comparison ofBody Exhaust Suits vs. Occlusive Clothing’. Unfortunatelythere appear to be no records of trials sponsored by com-panies who supply or manufacture devices used in woundmanagement such as dressings, beds or bandages. It wouldbe a real step forward for wounds research if everyone whosponsored wounds trials made a prospective register of allstudies. Richard Sykes, the chairman for GlaxoSmithKlinesaid ‘As a knowledge-based industry we understand wellthe value of information, and we want to create a climateof openness where the evidence for prescribing our prod-ucts is clear.’ He too hoped that other companies wouldjoin this initiative, saying that ‘GlaxoWellcome has takenthe lead in disclosure of information, and I hope that therest of the pharmaceutical industry will join this initiative.’There appears to be no less an imperative for the healthcaredevices industry or wound care charities to be open aboutthe trials they sponsor.
The European entries are dominated by the UK, butthis is changing. The European Science Foundation PolicyStatement on Controlled Clinical Trials (May 2001) nowrecommends that member organisations make trial regis-tration a condition of funding. They also contribute itemsto the mRCT and support the use of International Stand-ard Randomised Controlled Trial Numbers (ISRCTN) sothat readers can identify where a particular trial has beenreported more than once, and where trials are unique.
The trials in the meta register represent a diverse cov-erage of clinical trials. In future editions of the EWMAjournal we will be highlighting some of the trials featured.In this edition, we summarise just three of the trials inpressure ulcer prevention and treatment on the mRCT.The level of detail provided varies according to the sourceof the original information. Typically, abstracts from theUK National Research Register (http://www.doh.gov.uk/research/nrr.htm) are briefer than the US source, ClinicalTrials (http://www.clinicaltrials.gov). All contain contactinformation for the principal investigator or research team,and some contain hypertext links to websites with moreinformation about the trial.
STUDY ATitle: Investigation of Sub-atmospheric Pressure Dressingon Pressure Ulcer HealingSponsor: Department of Veterans Affairs (USA)
Trial InformationStudy Design: Treatment, Randomized, Open Label, ActiveControl, Single Group Assignment, Efficacy Study �
Scientific Article

Not too dryNot too wet
www.convatec.com
®™Trademarks of E R Squibb & Sons, L.L.C. ConvaTec Limited, authorised user. 1 Data on File, ConvaTec: WHRI2334 AI1052 Versiva Phase II study. Data on File. ConvaTec. May 20013 Versiva Phase III study. Data on File. ConvaTec. September 20014 Data on File, ConvaTec: WHRI 2373 MA071
Versiva® dressing is a CE marked product.
Just right
An optimal moisture balance to support wound healing
Versiva® dressing is the only dressing that unites
three proven technologies to optimally manage
moisture - a unique foam-film layer, Hydrofiber®
layer and hydrocolloid. It combines effective
absorption and retention with controlled
evaporation to maintain a moist wound
environment,1 whilst also providing an effective
bacterial and viral barrier.4 Versiva dressing
- designed to prevent maceration, to protect and
to be incredibly gentle.1,2,3
Sizes available:9 x 9cm, 14 x 14cm, 19 x 19cm, 19 x 24cm, 19.5cm x 18.5cm/heel, 21 x 22.5cm/sacral

EWMA JOURNAL 2002 VOL 2 NO 228
Further Study Details: Many spinal cord injury (SCI) andotherwise debilitated patients develop pressure ulcers overthe course of their injury or disease. Despite enhancedwound care management, many pressure ulcers do not healcompletely and require surgical myocutaneous rotationalflap coverage. Even then they often recur.
Hypothesis: Sub-atmospheric pressure dressing (SPD) treat-ment applied to pressure ulcers will either completely closethem, or heal them to a point allowing for skin graft cov-erage, more often than 0.9% normal saline wet-to-moistdressing (WTMD) treatment.
Objectives: The objectives of this study are:1. to conduct a controlled comparative study of the
effectiveness of sub-atmospheric pressure dressing(SPD) in healing pressure ulcers versus conventionalsaline wet-to-moist dressing techniques;
2. to establish indications and contra-indications foruse of SPD in treating pressure ulcers;
3. to develop a non-invasive, clinically-usable opticaldigitiser and associated software for measurement ofwound geometry for standardised quantitative assess-ment and longitudinal monitoring of wound healing.
Research methods: 120 patients with stage III or IV pres-sure ulcers meeting the project selection criteria will berecruited for the project. Patients will be randomly assignedin a 3:1 (SPD to WTMD) ratio to either the control groupreceiving 0.9% normal saline wet-to-moist wound dress-ing and treatment, or to the sub-atmospheric pressure-dressing group. All subjects selected will be further strati-fied according to degree of wound severity, nutritional sta-tus, and evidence of wound infection. The WTMD groupwill receive 0.9% NS moistened gauze applied to thewound, which will be changed every 8 hours. The SPDgroup will receive SPD dressing with the VACTM systemset at a constant sub-atmospheric pressure of negative 125mmHg. The SPD device and dressing will be left in placeand changed every Monday, Wednesday, and Friday. Thesubjects’ pressure ulcers will be measured on day 0 and thenon a weekly basis. Ulcer surface shape, area, and colora-tion will be recorded with a digital camera and also by trac-ing the ulcer perimeter on a flexible translucent plastic filmwith grid overlaid on the wound. In addition, an opticallaser scanner will be used to record ulcer shape, area, andcoloration, and body/limb segmental volume in the regionof the wound. Volume will also be measured using alginatewound impressions to form silicone moulds for fluid dis-placement measurement. The moulds of the wounds willalso be optically digitised while the wound perimeter, topi-cal surface area, total 3-D surface area, and volume will becalculated using computer image processing, planimetry,and volumetry software developed in the project. Local
body/limb segment volume will also be calculated to moni-tor oedematous fluctuations. Based on these measure-ments, the wound responses will be scored, after onemonth or at the time of the patient’s withdrawal from thestudy. The association between response level and treat-ment type will be analysed using the Chi-square test ofassociation. Mantel-Haenszel, Chi-square and logisticregression will be used to control for prognostic variables.
EligibilityAges Eligible for Study: 18 Years and above,Genders Eligible for Study: BothExpected Total Enrolment: 120
Administrative informationLocation and Contact InformationMichael Longaker, M.D. (212) [email protected] York VAMC, New York, United States;Recruiting Michael Longaker, MD 718-584-9000
Study chairs or principal investigatorsJohn Fryer, Ph.D. asst. director, Program Analysis andReview Section (PARS), Department of Veterans Af-fairs, Rehabilitation Research & Development ServiceWijegupta Ellepola, Program analyst, Program Analysisand Review Section (PARS), Department of VeteransAffairs, Rehabilitation Research & Development Service
More Information:Study ID Numbers – A2108Date study started: January 2000Study Completion Date: December 2001NLM Identifier – NCT00011531ClinicalTrials.gov processed this record on 2002-10-01
STUDY BTitle: The Prevention of Hospital-Acquired Pressure Ulcersin Surgical Patients: A Randomised Clinical Trial Testingthe Effects of Preventing Hypothermia During Surgery.*
Trial InformationMain Research Question: Can pressure ulcers be preventedthrough preventing intraoperative hypothermia?Design: Randomised clinical trial with a concealed rando-misation process and blind outcome assessments.Sample Group Description: 324 patients having majorsurgery in one district general hospital.Multi-centre Trial? NO.Outcome Measures: Pressure ulcers and surgical woundinfections.
*NB: This trial was published as Melling AC, Ali B, Scott EM, and Leaper DJ. Effects ofpreoperative warming on the incidence of wound infection after clean surgery: arandomised controlled trial. Lancet 2001 Sep 15; 358(9285): 876-80.

EWMA JOURNAL 2002 VOL 2 NO 2 29
Administrative informationSource – National Research RegisterSerial number at source – N0159067148Current status of trial: CompleteStart date – 1/9/1997. End date – 31/3/2000
Funding organisation: Northern & Yorkshire region of theNHS Executive (UK)Supplementary information: This study was the final partof a doctoral research programme with the Centre forHealth and Medical Research, University of TeessideContact name(s): Mrs Eileen Margaret ScottContact details:
North Tees & Hartlepool NHS TrustClinical Governance UnitNorth Tees General HospitalStockton-on-Tees TS19 8PE UKTel: +44 (0) 1642 624090 Fax: +44 (0) 1642 624931Email:[email protected]
Further information:This record was taken from the National Research Register2002, Issue 3, published in September 2002 (http://www.doh.gov.uk/research/nrr.htm). Information about thistrial can be obtained from the lead researcher named above.
STUDY CTitle: Randomised Controlled Trial Comparing Alternat-ing Pressure Overlays with Alternating Pressure Mattressesfor Pressure Sore Prevention and Treatment
Trial InformationClinical objectives: The project will test the null hypoth-esis that there is no difference in clinical efficacy and cost-effectiveness between alternating pressure overlays (AO)and alternating pressure mattress replacements (AR).
Design: A multi-centre RCT in which 2100 patients atmoderate to high risk of developing a pressure sore will berandomised (stratified, 24 hour telephone) to either analternating pressure replacement mattress (AR) or an al-ternating pressure mattress overlay (AO).
Eligibility criteria:Inclusion: Patients aged > 55 years who are admitted to avascular, orthopaedic or care of the elderly ward with anexpected length of stay of at least 7 days AND who arecompletely immobile/have very limited mobility on admis-sion; or have a pre-existing grade 1, 2 or 3 pressure soreon admission. Patients admitted before elective surgerywho are expected to be completely immobile/have verylimited mobility for at least 3 days after surgery may alsobe included.
Exclusion: Patients who have a pre-existing grade 4 or 5pressure sore on admission, have participated in this trialpreviously, or are unable/unwilling to give full informedconsent.
Randomised interventionsI) an alternating pressure replacement mattress (AR)II) an alternating pressure mattress overlay (AO).
Endpoints/outcomes:Primary: The occurrence of a first or new sore at or abovethe level of superficial damage to the skin (break/blister)before discharge will be considered as a treatment failure.Secondary: Worsening/healing of existing sores, patients’perceptions, time to occurrence, site of sore, economiccosts including those incurred in the treatment of pressuresores in the community, post-discharge. Skin assessmentswill be made daily by qualified attendant nursing staff andvalidated twice weekly by research nurses. Health eco-nomic results comparing the costs and benefits of the ex-pensive with the cheaper mattresses will be expressed asincremental cost effectiveness ratios.
Administrative informationSource of record: National Health Service Research andDevelopment Health Technology Assessment ProgrammeSerial number at source: 97/06/14Current status of trial: Open (i.e. actively recruiting newparticipants)Proposed start date: 01/09/2000Proposed end date: 31/03/2003Sources of funding: UK NHS Health Technology Assess-ment ProgrammeContact name: Professor Nicky CullumContact details:
Department of Health Sciences,Centre for Evidence-Based Nursing, University of York,York, Y010 5DDTel: +44 (0) 1904 321343/4Email: [email protected]
Further information:The NHS R&D Health Technology Assessment Pro-gramme Register was updated in May 2002. Further in-formation on this trial may be obtained by contacting thelead researcher named above. �
Reference List
1 Cullum N, Nelson EA, Flemming K, and Sheldon T. Systematic reviews of woundcare management: (5) Beds: (6) Compression: (7) Laser therapy, therapeuticultrasound, electrotherapy and electromagnetic therapy. Health TechnologyAssessment 2001; 5(9): 1-221.
2 Horton R, Smith R. Time to register randomised trials. British Medical Journal 1999.319: 865-6.
Scientific Article

EWMA JOURNAL 2002 VOL 2 NO 230
We are delighted to welcomePeter Vowden as the newEWMA President. As a vas-
cular surgeon in Bradford in the UK,Peter is ideally qualified to lead the or-ganisation over the next few years. Fewvascular surgeons have shown such com-mitment and interest in the field ofwound care as Peter. He is well placed tounderstand the challenges of EWMAwhich in addition to its European remitalso represents the views of many differ-ent professional groups from basic scien-tists to nurses, doctors and allied profes-sions such as podiatry.
In 1990, Peter was given the task of establishing a re-gional vascular unit. This unit now serves a population wellin excess of 650,000. In addition to this demanding role,Peter has developed a truly collaborative, research-basedwound care service, embracing the individual contributionmade by all members of the multi-disciplinary team. Pe-ter’s research in wound care has included the developmentof a 3D wound imaging system and undertaking random-ised control trials of treatments including compression.The unit is currently examining ethnicity issues in vascu-
Welcome to Peter VowdenEWMA President
lar disease, thrombophilia in leg ulcera-tion and wound debridement. Peter hasbeen involved in a number of national andinternational wound journals and in thedevelopment of the UK National Guide-lines in Leg Ulcer Management.
To his new position as president, Peterbrings a very clear understanding of theneed to unite Europe and place woundcare on the European health care agenda.His work on the EWMA industry liaisoncommittee has already contributed to theexcellent financial support EWMA now
receives from its industry sponsors. Peter recognises the im-portance of creating healthy, effective alliances between ex-isting organisations as well as supporting the developmentof new areas. Under Peter’s direction, I believe we will see,EWMA consolidating and developing new relationshipsand areas of interest.
My thanks go to Peter for his personal support, encour-agement and wisdom during my presidency. I look forwardwith great anticipation to the next few years as EWMAgoes from strength to strength.
Christine Moffatt
EWMA Pain Position PaperEWMA was very proud to be able to present itsfirst Position Paper at the Granada 2002 conference.The topic selected for this issue was that of “Painat wound dressing changes”.The paper, which was sponsored by MölnlyckeHealth Care, was published in 5 different languagesand 50.000 copies were printed and distributed!Furthermore many have chosen to download afree copy on www.tendra.com/painposition
EWMA will in future years continue toproduce position papers on important aspects ofthe Wound Healing and Wound Management areaand thereby creating a series of practically usefuladvice for health care personnel across Europe.
EWMA news

AN ADVANCED THERAPY SYSTEM FOR WOUND HEALINGEasier to use. Maximum versatility.
Specific indications, contraindications, precautions and safety tips exist for this product and therapy. Please consult a physician, the V.A.C. Recommended Guidelines for Use/Physician and Caregivers
Reference Manual and the V.A.C.® ATS User Manual prior to dressing application and product use.
© 2002 KCI International, Inc. All rights reserved. 8023 Vantage Drive, San Antonio, TX 78230. All trademarks and service marks herein are the property of KCI, its affiliates and licensors.The V.A.C. (Vacuum Assisted ClosureTM) system is subject to patents and/or pending patents.
To learn more about the V.A.C.® ATS device and the T.R.A.C.TM System, please visit www.woundvac.com, call +1 210 255 6970or write us: KCI International Inc., Beech Avenue 54-80, 1119 PW Schiphol-Rijk, The Netherlands
Vacuum Assisted Closure™ (V.A.C.®) therapy from KCI is
one of the most innovative therapies available today for
effective wound healing. Applying controlled, localized
sub-atmospheric pressure to the wound site, V.A.C.® ther-
apy has been used effectively in treating thousands of wounds of
different aetiologies in all care settings.
The V.A.C.® ATS Advanced Therapy System was developed specifi-
cally to improve ease of use, effectiveness and versatility.
With touch screen controls and a sophisticated alarm sys-
tem, this new V.A.C.® therapy system addresses the needs
of wound care professionals. Each unit is equipped with
T.R.A.C.™ technology to accurately deliver pressure at the wound
site and enhance patient outcomes. The more powerful therapy
system helps to treat a wider range of wounds than ever.
acute/traumatic wounds • dehisced wounds • flaps and grafts • subacute wounds • pressure ulcers • chronic wounds • diabetic ulcers

EWMA JOURNAL 2002 VOL 2 NO 232
The problem of chronic wounds in Italyaffects around 1.5% of the popula-tion, a percentage that is on the rise.
Today there are two major national societies in-volved in wound care in Italy: the AssociazioneItaliana Ulcere Cutanee (AIUC) and theAssociazione Infermieristica Studio LesioniCutanee (AISLeC). The main objectives ofAIUC are focussed on the improvement oftraining medical and nursing staff in the man-agement of patients with skin ulcers, especiallyin the light of new etiopathogenetic concepts ofthe various diseases involved and the develop-ment of new therapeutic technologies. Rightfrom its conception, the Association has as-sumed a multidisciplinary identity in order torepresent, as widely as possible, the variousmedical specialities involved in the manage-ment of skin ulcer patients. AIUC also intendsto extend its working relationship with themain international wound care societies andthus favour and further cultural exchange.
AISLeC was established in 1995 as a nursing or-ganisation involved in wound care. The Associa-tion has carried out epidemiological studies toexamine the extent of the problem of chronicwounds in Italy. AISLeC worked with the Ital-ian Health Ministry, using this data, to integratethe prevention of pressure ulcers into the ItalianNational Health Program including a majorcampaign through national newspapers.
DISCOVER PISAEveryone knows the Leaning Tower of Pisa,but the city of Pisa is not just the Tower, or themarvellous Piazza dei Miracoli where it stands.With its Cathedral, Baptistery and MonumentalCemetery, Pisa has many other attractions to beenjoyed. It is the site of the ancient Etruscanand Roman Port at San Rossore, one of themost recent and important archaeological dis-coveries made to date.
Wound Care in Italy
Marco RomanelliMD PhD
ItalyChairman Local
Organising Committee
ConsultantDermatologist at theDep. of Dermatology
Univ. of Pisa.EWMA Council
member.President elect and
founding member ofEPUAP.
AIUC board member.Dir. of the Wound
Healing Service at twomajor hospitals.
Adjunct Assoc. Prof.,Univ. of Miami, Florida.Chairman of the Tissue
Repair School at theUniv. of Pisa.
Correspondence to:Epuap Business Office
Wound Healing UnitDepartment ofDermatology,
Churchill HospitalOld Road, HedingtonOxford 0X3 7LJ, UK
Tel: +44 1865 228269Fax: +44 1865 228233
E-mail:[email protected]
13th Annual EWMA meeting in Pisa in 2003
Aerial view of Piazza dei Miracoli.

EWMA JOURNAL 2002 VOL 2 NO 2 33
It is also the city where the art of modern sculpturewas born, and many valuable works can be admired ondisplay in the National Museum of San Matteo. It is thecity of the Maritime Republic, through which, thanksto the trading activities of Leonardo Fibonacci, the Ara-bic number system was brought to Italy and Europe. Itis also a city of medieval walls surrounding an historicalcentre rich in monuments and works of art of extraordi-nary value, starting from Piazza dei Cavalieri. In addi-tion, Pisa is one of the most famous university cities inthe world; offering its ancient University, which was es-tablished in 1363; the Scuola Normale Superiore wherenumerous Italian Nobel prize winners were trained; theSchool of Sant’Anna, and the CNR laboratories.
It is also the city of the Lungarni (the banks of theriver Arno), much loved by romantic poets, from Byronto Shelley, from Giacomo Leopardi to AlessandroManzoni, for its climate and traditions of tolerance.
Pisa is also a city strongly characterised by its envi-ronmental treasures - first of all its Marina, a tourist at-traction established during the years of Belle Époqueand Liberty, and the Environmental Park of SanRossore, with its homonymous estate, which is alsoknown as an equestrian competition ground and breed-ing centre ranked among the most important in Europe.All this, and much else besides, makes Pisa a uniquecity, and it offers tourists and visitors an infinite selec-tion of attractions, ranging from the historic to themodern covering history, art, leisure, commerce and,not forgetting, holidays.
HISTORYPisa, in the past an Etruscan settlement and subse-quently a Roman colony and, later still, the ancient andproud Maritime Republic, rises on the banks of the riverArno close to the Tirrenian Sea. In the Middle Ages,Pisa enjoyed its period of greatest splendour: the numer-ous civilian and religious edifices, the squares, the typi-cal narrow alleys running perpendicular to the Arno,testify, in the historic centre’s forma urbis, to a remark-able economic and political stability.
Traces of the Roman and medieval settlements werecompletely lost, partly because of bombing during theSecond World War, but there are still ample stretches ofthe town walls, built between 1154-1155 and the mid-fourteenth century.
In the ninth century, Pisa intensified trade in theMediterranean Sea, conquered Sardinia and the townsof Reggio Calabria, Palermo, Bona and Al Mahdiya inAfrica, and, furthermore, could boast of many victoriesagainst the Muslim ships.
Oriented towards Ghibelline politics, Pisa was theonly free commune in all of Tuscany to openly support
the Swabian sovereigns, Frederick I Barbarossa, HenryVI, Frederick II, Manfredi and Corradino, who were inopposition to the Papacy, and excommunicated in 1241for having captured and consigned to the EmperorFrederick II a few high-ranking priests on their way toRome to take part in a council.
The gradual decline of the city was decreed by its ri-val Genoa with the defeat of Meloria in 1284 and subse-quently also by Florence. The loss of Sardinia and pre-dominance over the sea placed Pisa in a kind of isolationfrom which it only emerged around 1500.
THE CITYPisa is situated on the banks of the river Arno, inNorth-West Tuscany. Just 80 km from Florence and 10km from the Mediterranean Sea, Pisa is a very wellknown tourist centre. The town is closely associatedwith the famous Leaning Tower, which was re-openedto visitors on December 15th 2001.
The climate, mild and temperate during the yearbecause of the vicinity to the sea and the protectionoffered by the mountains behind the city, has given Pisa
�
EWMA news
Pisa is known for its beautiful sculptures.

EWMA JOURNAL 2002 VOL 2 NO 234
Luminara, an occasion marking the feast of the PatronSaint (June 16th) a suggestive decoration on the banksof the Arno River with wax candles, and the Palio di SanRanieri, a regatta with special boats through the historicparts of town.
On the last Sunday in June, at the end of a processioncomprising over seven hundred actors in historical cos-tumes, two factions of six teams face each other on thetwo opposite banks of the Arno, each pushing a heavycart. Thus the Game of the Bridge, an ancient tourna-ment game, is re-enacted.
The Pisa’s Congress Building is one of only a tinynumber that belong to an Italian university. It stands inone of the most attractive parts of the city and, beingonly two kilometres from the airport, the railway stationand the exit of Florence-Pisa highway, it is easy to reachby all forms of transport. A walk of the same distancealong the river Arno and through the fascinating medi-eval town centre takes you to the Leaning Tower in thePiazza dei Miracoli. The Congress Building is three sto-reys high: on the first floor there are the simultaneoustranslators’ booths catering for up to five languages, onthe second are the press room and other rooms for workand study. The auditorium is on the ground floor withseating for 1000 people, which, when required, can bedivided by sliding walls into three smaller independentsoundproof sectors, two with seating for 250 and onefor 500 people. Further smaller rooms with from 20 to170 places are also available for meetings. Equipment inthe building is technologically of the first order and cansatisfy every congress need. Set in attractive open sur-roundings, the building is fully air-conditioned and isideal for receptions, dinners and other social events.
The scientific programme committee has developedan extensive programme that will provide a diverselearning opportunity with something for everyone. TheEWMA annual meeting is the most intensive educa-tional event in the field of wound care. The high qualityof the programme has been firmly established in theEWMA Congresses of the last few years, and the 2003meeting will certainly continue that tradition of excel-lence.
I would personally like to welcome you all to the 13thAnnual EWMA meeting in Pisa in 2003 and I look for-ward to seeing you in Italy for what I believe will be anoutstanding educational and social event.
Marco RomanelliChairman Local Organising Committee
a primary place in national and international tourism.Pisa International Airport, Galileo Galilei, has domesticand international air links with Rome, Milan, Cagliari,Amsterdam, Barcelona, Madrid, Bruxelles, LondonGatwick and Stansted, Frankfurt, Munich and ParisCharles de Gaulle. The airport is very close to the citycentre and the terminal is directly connected to PisaRailway Central Station and thence to the Italian rail-way network.
As the fulcrum of an area astride the provinces ofLucca and Livorno, Pisa’s territory is particularly suit-able for farm-holidays, trekking, cycling, horse riding,bird watching, golf, open-air and water sports. The cityis sited on a fantastic coast with sandy beaches, and isperfectly equipped with bathing establishments, hotelsand restaurants. The Regional Natural Park ofMigliarino, San Rossore, Massaciuccoli, extends for23,00 hectares along the coast from Viareggio toLivorno, with tree groves and Mediterranean shrubs,deer, bears and over two hundred varieties of migratorybirds. Pisa preserves, with the complex of Piazza deiMiracoli, cultural patrimony of all humanity, numerousmasterpieces of medieval history and both civil andmilitary architecture. To these treasures can be addedthe Certosa of Pisa, at Calci (10 km from Pisa) and theBasilica of San Piero a Grado (5 km from Pisa), requiredstops for all lovers of Romanesque art.
Pisa’s cultural and academic traditions boast, besidesthe most ancient botanic garden in all of Europe, a pres-tigious athenaeum flanked by the Scuola Superiore diStudi Universitari Sant’Anna and the Scuola NormaleSuperiore, unique in Italy and instituted by NapoleonBonaparte in 1813.
A city of art and history, Pisa commemorates its tra-ditions during the month of June with numerous folk-loristic and religious events, among which are the
EWMA news
The impressive cathedral is placedright next to the Leaning Tower.
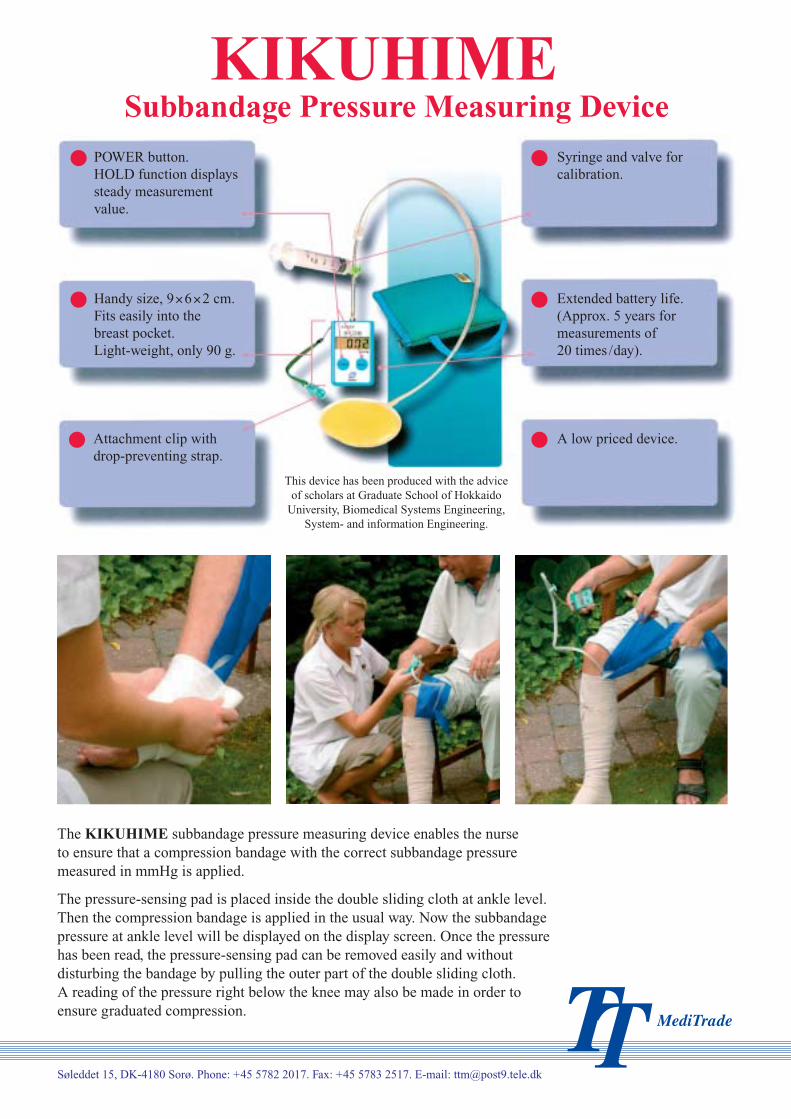
Søleddet 15, DK-4180 Sorø. Phone: +45 5782 2017. Fax: +45 5783 2517. E-mail: [email protected]
POWER button.HOLD function displayssteady measurementvalue.
Handy size, 9�6�2 cm.Fits easily into thebreast pocket.Light-weight, only 90 g.
Attachment clip withdrop-preventing strap.
Syringe and valve forcalibration.
Extended battery life.(Approx. 5 years formeasurements of20 times /day).
A low priced device.
This device has been produced with the adviceof scholars at Graduate School of Hokkaido
University, Biomedical Systems Engineering,System- and information Engineering.
Subbandage Pressure Measuring DeviceKIKUHIME
The KIKUHIME subbandage pressure measuring device enables the nurseto ensure that a compression bandage with the correct subbandage pressuremeasured in mmHg is applied.
The pressure-sensing pad is placed inside the double sliding cloth at ankle level.Then the compression bandage is applied in the usual way. Now the subbandagepressure at ankle level will be displayed on the display screen. Once the pressurehas been read, the pressure-sensing pad can be removed easily and withoutdisturbing the bandage by pulling the outer part of the double sliding cloth.A reading of the pressure right below the knee may also be made in order toensure graduated compression.
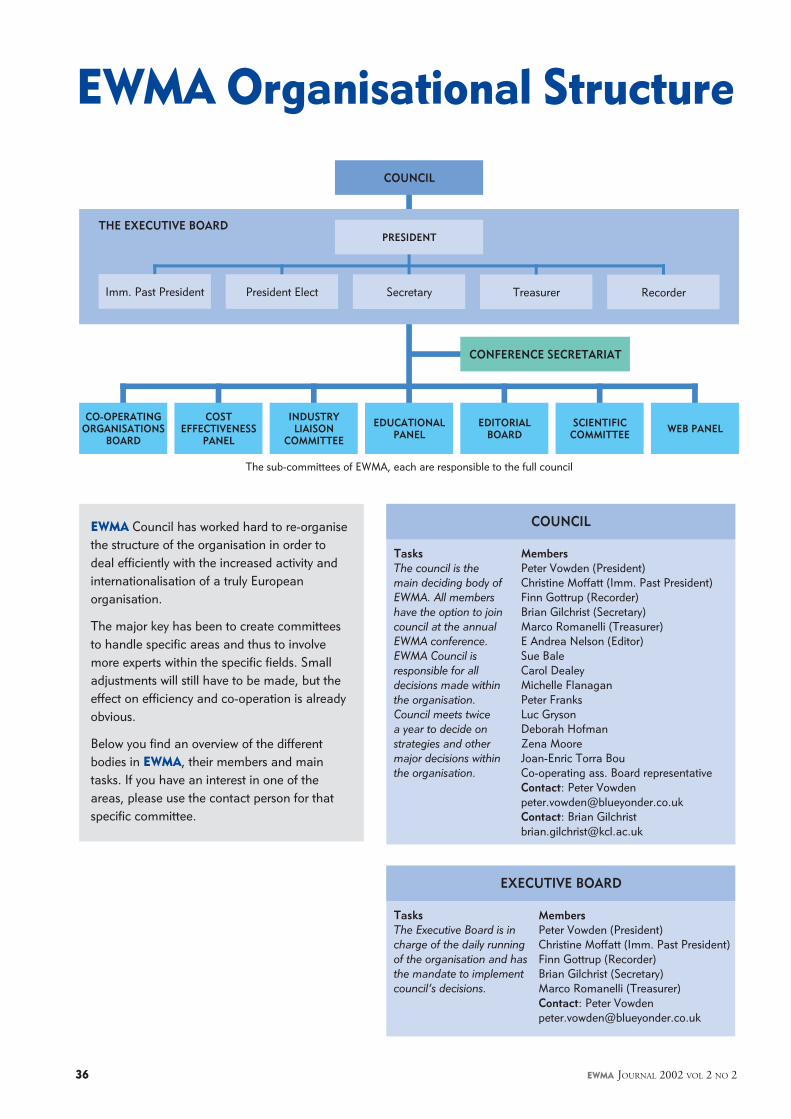
EWMA JOURNAL 2002 VOL 2 NO 236
EWMA Council has worked hard to re-organisethe structure of the organisation in order todeal efficiently with the increased activity andinternationalisation of a truly Europeanorganisation.
The major key has been to create committeesto handle specific areas and thus to involvemore experts within the specific fields. Smalladjustments will still have to be made, but theeffect on efficiency and co-operation is alreadyobvious.
Below you find an overview of the differentbodies in EWMA, their members and maintasks. If you have an interest in one of theareas, please use the contact person for thatspecific committee.
EWMA Organisational Structure
COUNCIL
THE EXECUTIVE BOARD
CO-OPERATINGORGANISATIONS
BOARD
COSTEFFECTIVENESS
PANEL
INDUSTRYLIAISON
COMMITTEE
EDUCATIONALPANEL
EDITORIALBOARD
SCIENTIFICCOMMITTEE WEB PANEL
PRESIDENT
Imm. Past President President Elect Treasurer RecorderSecretary
CONFERENCE SECRETARIAT
TasksThe council is themain deciding body ofEWMA. All membershave the option to joincouncil at the annualEWMA conference.EWMA Council isresponsible for alldecisions made withinthe organisation.Council meets twicea year to decide onstrategies and othermajor decisions withinthe organisation.
COUNCIL
MembersPeter Vowden (President)Christine Moffatt (Imm. Past President)Finn Gottrup (Recorder)Brian Gilchrist (Secretary)Marco Romanelli (Treasurer)E Andrea Nelson (Editor)Sue BaleCarol DealeyMichelle FlanaganPeter FranksLuc GrysonDeborah HofmanZena MooreJoan-Enric Torra BouCo-operating ass. Board representativeContact: Peter [email protected]: Brian [email protected]
MembersPeter Vowden (President)Christine Moffatt (Imm. Past President)Finn Gottrup (Recorder)Brian Gilchrist (Secretary)Marco Romanelli (Treasurer)Contact: Peter [email protected]
EXECUTIVE BOARD
TasksThe Executive Board is incharge of the daily runningof the organisation and hasthe mandate to implementcouncil’s decisions.
The sub-committees of EWMA, each are responsible to the full council

EWMA JOURNAL 2002 VOL 2 NO 2 37
TasksOne of the pillars of EWMAis the close co-operationwith the co-operatingorganisations. In this groupnational representativeswill discuss and plan theEuropean development.
CO-OPERATING ORGANISATIONS BOARD
MembersChristine Moffatt (Chair)Wolfgang VansheidtRepresentatives from each co-operating organisation tobe elected.Contact: Christine [email protected]
TasksThe Panel aims to provide acentre for cost effectivenessstudies within Wound Careby initiating projects andoffering support to thosewho wish to undertake costeffectiveness studies.
COST-EFFECTIVENESS PANEL
MembersPeter Franks (Chair)Nick BosanquetJohn PosnettHugo PartschPatricia PriceElia RicciContact: Peter [email protected]
TasksAll editorial decisionsregarding EWMAJournal are made bythis board. Works inclose co-operation withthe Web Panel.
EDITORIAL BOARD
MembersE. Andrea Nelson (Chair)Carol DealeyFinn GottrupDeborah HofmanSylvie MeaumeJoan-Enric Torra BouPeter VowdenMichelle BriggsContact: E. Andrea [email protected]
TasksThe responsibility ofdeveloping and main-taining a high-classweb site lies with thisgroup.
WEB PANEL
MembersJoan-Enric Torra Bou (Chair)E Andrea NelsonMarco RomanelliContact: Joan-Enric Torra [email protected]
TasksFor all practical mattersregarding conferences orprojects, please contactthe EWMA conferencesecretariat.
CONFERENCE SECRETARIAT
Contact: Congress [email protected]
TasksThe aim of this panelis to create and imple-ment an educationalframework consistingof a flexible curriculumto students and health-care professionals. Thecurriculum will be thebase for future educa-tion by EWMA in theco-operating countries.
EDUCATIONAL PANEL
MembersMadeleine Flanagan (Chair)Finn Gottrup (Co-chair)Deborah HofmanChristina LindholmCarol DealeyLuc GrysonZena MooreHugo PartschContact: Madeleine [email protected]
TasksThe co-operationbetween EWMA andthe industry is organisedin this committee.
INDUSTRY LIASON COMMITTEE
MembersPeter Vowden (Co-chair)Christine Moffatt (Co-chair)Corporate A sponsor representativesContact: Peter [email protected]
TasksThe Scientific Committeeis responsible for scientificprogrammes & evaluationof abstracts in relation toEWMA meetings.
SCIENTIFIC COMMITTEE
MembersFinn Gottrup (Recorder)Sue BaleMadeleine FlanganPeter FranksDeborah HofmanMarco RomanelliPeter VowdenContact: Finn [email protected]
EWMA news

EWMA JOURNAL 2002 VOL 2 NO 238
Michelle Briggs has contributedto EWMA since its inception – forexample by attending every EWMAConference, presenting at plenarysessions, oral papers and practicalworkshops. Recently, Michellestepped down after serving threeyears on Council, and we wish to ex-press our gratitude. During her time
on EWMA Council Michelle made many contributions.One of her gifts is the ability to ask the question that is oneveryone else’s mind. Like the boy who shouted ‘the em-peror is not wearing any clothes’, Michelle is able to remainclearly focussed on EWMA’s mission – to help people ineducation, practice and research into wound management.She worked with Joan Enric Torra I Bou in the early days ofour EWMA web site and was a founding member of theEditorial Board of the EWMA Journal. Michelle will re-main involved in the Journal as an advisor.
Michelle’s real passion is pain management, both re-search and clinical practice and she has made some lastingcontributions in this area. As one of the first recipients ofthe EWMA / Seton Healthcare Research Award, Michelleprepared a systematic review of the effect of dressings andtopical agents in managing the pain of venous leg ulcers.She subsequently published this as a Cochrane Review andin this format it has been consulted internationally.Michelle also made a massive contribution to the firstEWMA position paper on Pain and Dressing Changes, asan author and editorial adviser to the development group.Michelle managed to do all this while working on her doc-toral thesis ‘the prevalence and characteristics of painful legulceration’ as well as numerous extracurricular activities.
Michelle is taking up a new challenge in early 2003,when she will become Research Fellow in Pain in OlderPeople at the Division of Nursing / School of HealthcareStudies, at the University of Leeds. We wish her all the bestin this endeavour.
E. Andrea Nelson
George Cherry was oneof the invited participants ina series of meetings whichculminated in the foundingof the European WoundManagement Association.He can therefore genuinelylay claim to being one of thefounder members of the
Association. From the outset George was an enthusi-astic and active participant, who was very keen toensure that any conferences or study days werealways of high scientific content, while at the sametime always having a practical aspect.
His contribution to the Association has beenconsiderable: he was one of the editors of the confer-ence proceedings from 1992 until 1996; he was theRecorder from 1993 to 1995; and he became thePresident in 1996. He has served on the councilcontinuously from the inception of the Associationuntil finally retiring at the 2001 Annual GeneralMeeting.
The role of the Recorder is to chair the Pro-gramme Committee and to organise the Confer-ence, both tasks requiring a considerable amount ofenergy, tact and diplomacy. During George’s term ofoffice he was often called on to exercise all of thesein great measure as the Association struggled to gainfull control of its own affairs, especially in relation tothe annual conference. The hugely successful confer-ences in Copenhagen (the first EWMA venture out-side the UK) and the following year in Harrogatewere the tangible results of his endeavours.
George has been one of the Association’s staunch-est supporters. EWMA Council would like to recordits sincere thanks for all the hard work, and for theimpressive results he has achieved and wishes him allthe best in the future.
Brian Gilchrist
Leaving/entering
COUNCIL

EWMA JOURNAL 2002 VOL 2 NO 2 39
Geoff Keye retired this yearfrom EWMA Council after serv-ing the organisation close to adecade. During this time heserved on several committees andwas the local organiser for ourvery successful conference inDublin in 2001.
In writing this appreciationof his work, I tried to think of a suitable anecdote thattypified Geoff ’s commitment and contribution toEWMA. The most obvious is all the hard work he putinto ensuring that the conference in Dublin was such asuccess. However, I think the one I have chosen demon-strates the dedicated way in which Geoff worked withinCouncil.
EWMA Scientific Committee is responsible forjudging all the abstracts submitted for both oral andposter presentations at conference. The committee metearly in 2001 in Birmingham, UK in order to judge toabstracts for the conference in Dublin. The weather wasnot good and Geoff ’s flight into Birmingham was di-verted to Manchester where the passengers were put ona coach to Birmingham Airport (a journal of severalhours). He then had to travel another 40 kilometres bytaxi. Geoff finally arrived very late, but immediately satdown to work on the abstracts and was able to advise ona number of abstracts that required his specialist knowl-edge. To me, that is real commitment; I would havegone back home from Manchester!
The Council will miss Geoff greatly and wish himwell for the future.
Carol Dealey
This year ChristinaLindholm has left EWMACouncil but continues her workfor the organisation through herinvolvement in EWMA’s Educa-tional Panel and, as an ambassa-dor of EWMA, she assists woundhealing societies in the Balticcountries.
Christina is a warm and enthusiastic person whosesense of humour and engagement make her a pleasantand inspiring colleague. Being a member of EWMACouncil since the early stages, she has taken part in thedifferent stages of the development of EWMA. In 2000Christina chaired the important meeting in Stockholmwhere the future of EWMA was decided. The Stock-holm meeting was a great success, which was partly dueto Christina’s enormous efforts.
During her career Christina has worked in the indus-try as well as in clinical work. She is an RN tutor ofNurses, and her involvement in research has resulted ina PhD degree in medicine performed in Malmo, Swe-den in 1993. Christina is the author of a textbook onwound healing for nurses and of a national pressure ul-cer State of the Art document. Her postgraduate re-search including her PhD focuses on leg and pressureulcers. Education has always been vital to Christina, andshe is engaged in courses for nurses on the care of differ-ent types of wounds. She is also the founder of UppsalaWound Healing Centre in 1999.
Thank you Christina, for the efforts you have madeso far. We hope you will continue to support and workfor EWMA in the future.
Finn Gottrup
It is with great pleasure EWMA welcomesSue Bale (UK),Luc Gryson (BE)and Zena Moore (IE)as new members of council.We look forward to the contributionsthey will bring to our organisation.
EWMA news
Sue Bale Luc Gryson Zena Moore
At the same time EWMA would like to express the organisation’s appreciationto the four members who have chosen to leave the board. A heartfelt thank you toall for the hard and enthusiastic work, which has contributed to make EWMA whatit is today. Michelle Briggs, George Cherry, Geoff Keye and Christina Lindholm.
EWMA JOURNAL 2002 VOL 2 NO 240
EWMAActivity ReportIn this section you can follow activities takingplace in EWMA. Many of these projects aredescribed in detail elsewhere in the journal.
Latest activities� 12th EWMA Conference – ‘Chronic
Wounds and Quality of Life’� Re-organisation of EWMA, to fit the
changed structure of the organisation.� New co-operating organisations:
• Czech Society of Wound Management(CSWH)
• Belgian Federation of Wound Care(BFWC)
� New Corporate A sponsors• KCI• Lohmann & Rauscher
� New Corporate B sponsors• Nutricia Healthcare
� Educational EWMA seminar in co-opera-tion with EPUAP, Budapest, Sep 2002
� Educational Meeting 28.09.2002� Corporate Sponsor Meeting 01.10.2002� Meeting with the Latvian Wound Healing
Organisation in Riga 24.10.2002� EWMA position paper on “Pain at wound
dressing changes” published
FUTURE ACTIVITIES� Meeting with the Czech Society of Wound
Management 08.11.2002� Corporate sponsor meeting 11.03.2003� Educational meeting 10.03.2003� EWMA conference in Pisa in co-operation
with AIUC and AISLeC 22-24.05.2003� Co-operating organisations meeting
23.05.2003
New Corporate Sponsors inEWMA
EWMA is pleased to announce thatKCI and Lohmann & Rauscher havechosen to join the Corporate A-sponsorship programme from2003. Lohmann & Rauscher alreadyholds a Corporate B-sponsorship.
EWMA recognizes the importance of close co-operationbetween the organisation and the corporate industry andlook forward to working with KCI and Lohmann & Rauscherin the efforts to profile the wound healing and manage-ment area.
Only by giving the industry a useful and positive outcomefor their investment will it be possible for both parties tobenefit from their association in the long run.
We would like to officially thank our new corporate spon-sors for choosing to help us in our efforts. We hope thateverybody associated with EWMA will support this co-oper-ation in any way possible.
Furthermore Nutricia has chosen tojoin on the corporate sponsor B level.
Use the Journal toprofile your companyThe EWMA Journal is a bi-annual European informa-tional source within woundhealing and Management.10,000 copies are distributed free of charge to allmembers of organisations co-operating with EWMA.This makes the Journal a unique communicationchannel from which your company could benefit greatly.
If you are interested in more informationon rates and possibilities please contact:
Congress ConsultantsMartensens Alle 8DK-1828 Frederiksberg C, DenmarkTel: +45 7020 0305Fax: +45 7020 0315e-mail: [email protected]
Please observe that the deadline fornext issue is March 15th
EWMA news

Polyurethane foam woundcare dressing. The onlywound care dressingcontaining an FDA approvedwound cleanser F68(Poloxamer 188), amoisturizer (glycerin)and Super Absorbent StarchCo-Polymer.
PolyMax ® is the new thicker moreabsorbent non-adhesive dressing withthe same benefits of F68, Glycerol andthe Super-absorbent Starch Co-Polymeras PolyMem dressings.
PolyMax ® absorbs up to 60% morethan PolyMem and over 80% more thanother foam dressings.
Today, Ferris features a full lineof latex free PolyMem Dressings,which are available in numerousshapes, sizes and configurationsfor a wide variety of woundapplications.
Continual in-house research andextensive clinical testing assureconsistent performance of everyPolyMem Dressing, recognizedworldwide as “The Pink Dressing,”
PolyMem is available through aglobal network of sales offices andhealthcare distributors. For furtherinformation, contact Ferris Mfg.Corp. Europe office at:
email:[email protected]
www.FerrisCares.com
DISTRIBUTORS INQUIRIESWELCOME FOR:Spain, France, Portugal, Austria,Slovenia and Czech Republic
The Super-Absorbent Starch Co-Polymercontained in the dressing, draws, absorbsand holds excess fluids in the hydrophilicmembrane while allowing the body’snatural growth factors and nutrients toconcentrate at the wound site.
The F-68 Surfactant, is a mild wound cleansingagent activated by moisture and gradually releasedinto the wound bed. Interfacial tension betweenhealthy tissue and debris is reduced, looseningeschar and necrotic tissue, supporting autolyticdebridement and keeping the wound bed cleanthroughout the entire wound healing process.
The Glycerin, a moisturizer, keeps thedressing from adhering to the wound bed,providing comfort at the wound site.Glycerin also reduces odor, conservesliving fat cells, reduces hypergranulation,soothes traumatized tissues and supportsautolytic debridement.
PolyMemnon adhesive dressing
NEW!
PolyMemfilm backedadhesive dressing
PolyMemcloth backedadhesive dressing
PolyWicsuper-absorbentwound cavity filler
PolyMemnon adhesivecalcium-alginatedressings
PolyMem® PolyMax ®
EWMA JOURNAL 2002 VOL 2 NO 242
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Payment accepted in pound sterling only, drawn on UK bank.
I enclose a cheque of £15. Please indicate cheque no.:
Please make cheques payable to:European Wound Management Association
Or:
Please debit my account by £15:Credit Card type: (Delta, Master Card or Visa)Credit card no:
Expiry Date:
Exact name and initials on the credit card:
Please return formand enclose cheque to: EWMA
PO Box 864,London SE1 8TT,United Kingdom
Surname:
First name(s):
Profession:
Physician Surgeon Dietician Nurse Pharmacist Other
Work Address:
Address for Correspondence (if different from above):
Tel:
Fax:
E-mail:
EWMA Membership application
Volume 1Number 1Spring 2001
The EWMA StrategyChristine Moffatt
The Slovenian ProjectChristine Moffatt
Zinc Oxide Augments in WoundsDr. Magnus Ågren
Malignancy and Pre-Malignancy inLeg UlcerationJanice Cameron and Deborah Hofman
The Meaning of Living withVenous Leg UlcerBritt Ebbeskog
Cost-effectiveness in WoundManagementProf. Peter Franks
The Cochrane Wounds GroupMichelle Briggs
Pressure Sore ReferencesAndrea Nelson
Review: The Foot in DiabetesAndrea Nelson
EWMA Journal Previous Issues
Volume 1Number 2Fall 2001
Experimental Wound Healing ResearchFinn Gottrup
Larval Intervention in the ChronicWoundJohn C. T. Church
An Update on Pressure UlcerManagementJeen Re Haalboom
Wound ClosureDavid J. Leaper
The Profile of Wound CareEducational Development ProjectMadeleine Flanagan, Finn Gottrup
The Lymphoedema Support Network– A Patient PerspectiveChristine Moffatt
Review: Acute and Chronic WoundsUna Adderley
Progress Report from the CochraneWound GroupAndrea Nelson
Diagnosis/Prognosis Papers in 2001
Volume 2Number 1Spring 2002
Health Related Quality ofLife MeasurementAndrea Nelson
The use of Compression Therapy inthe Treatment of Venous Leg Ulcers –a recommended Management PathwayMichael Stacey et al
The Professional Role and Competenceof Tissue Viability Nurses in FinlandSalla Seppänen
A Review of Advances in FungatingWound Management since EWMA 1991Patricia Grocott
Multi-center Research on WoundManagement in Home Care in ItalyA. Bellingeri
Wound Healing in Moorish SpainCarol Dealey
Treatment studies from 2001Review: Guide to the Medical Literature.A Manual for Evidence-Based ClinicalPracticeSally Bell Syer
Previous issues can be acquired for £7 or 11.5 € per copy. Please contact:Congress Consultants, Martensens Allé 8, DK – 1828 Frederiksberg C, DenmarkTel: + 45 70200305, Fax: + 45 70200315, [email protected]
EWMA JOURNAL 2002 VOL 2 NO 2 43
Index of October issue of
Journal of Wound Care:
Volume 11,Number 9
Interface pressure measurement:testing and selecting sensorsT. Bethaves, Medical Electronics Research Student (PhD)
Meeting the complex care needs of a patientwith Darier’s diseaseG. Wicks, MSc, RN, Dip HE, Tissue Viability Specialist Nurse
Healing properties of Promogran in venous leg ulcersF. Vin, MD, Angiologist; L. Téot, MD; S. Meaume, MD
The use of oxidised cellulose as a topicalhaemostatic dressing on a bleeding stomal woundN. Lawrentschuk, MB, BS; P.M. Hewitt, FRACS
A survey of tissue viability nurses’ role andbackground in one regionL. Austin, MSc, RN, MRC
Advanced wound care materials: developingan alginate fibre containing branan ferulateM. Miraftab,1 PhD; Q. Qiao, PhD; J.F. Kennedy,PhD, Professor; M.R. Groocock, Product Manager; *S.C. Anand, PhD, Director of Research
Making multimedia work for you: a wound manage-ment CD-ROMA. Hopkins, MSc, RN, DN Cert, Clinical Nurse SpecialistB. (Tissue Viability); M. Vogel, MPhil, Research Fellow.
Index of October issue of
SÅR:
SÅR,Number 3, 2002
The diabetic Charcot foot: incidence and treatment of ulcersKirsten Larsen, Jesper Fabrin, Per E. Holstein
The use of Low Level Laser in the treatment of venous ulcersHanne Storm
News from NIFS; Swedish Wound Care Society
Summary: Chronic wounds and quality of life.12th EWMA conference, Grenada, Spain 2002Bo Jørgensen
NIFS-nyttTheis Huldt-Nystrøm
Award-recipient: Grenada, Spain 2002Rie Nygaard
Summary on the 4th meeting in Jysk Wound Forum,Denmark, September 2002Rolf Jelnes
www.dsfs.orgMichael Bitsch
Information on Danish Nursing SocietyKirsten Müller
www.molnlyckehc.comRolf Jelnes
Call for annual general meetingDanish Wound Healing SocietyAGM agenda – Danish Wound Healing Society
EWMA news
The Leg Ulcer Reference CD
The Leg Ulcer Reference CD gives you access tothe world of leg ulcer management.
• Picture gallery with high-resolution photos ofleg ulcers, which range from common ailmentsto rarely seen disease processes
• 10 video-case studies on the differing aspectsof caring for patients with leg ulcers.
• Illustrated glossary with instant access tothe terminology used.
Get Access to the world of leg ulcer managementfor only 25 GBP including shipment.
Order your copy of the CD today by filling in theorder form on www.cricp.org

EWMA JOURNAL 2002 VOL 2 NO 244
Pain at wounddressing changes:a guide tomanagementby M Briggs, JE Torra i Bou
This paper draws on the authors'clinical experience and the basicscience of pain physiology to offerrecommendations for good practicewhen managing pain at wounddressing changes. Because of thecomplexity and size of the topic, thefocus is specifically on managingpain at dressing removal in adultpatients with chronic and non-burnwounds.
Key points
1. Pain control methods at wounddressing changes are oftenunder-utilised by practitioners.
2. Pain arising from wounds ismultidimensional in nature andpractitioners should adopt abroad holistic approach tomanagement.
3. It is vital that patients are sup-ported by a combination oftechniques to help them throughthe dressing procedure includinggood preparation, appropriatechoice of dressing materials andadequate analgesia.
The theory of painby H Wulf, R Baron
This article explores the complexnature of the underlying mecha-nisms involved in both nociceptive(inflammatory) and neuropathicpain to enhance our understandingof patients' pain experiences.
Key points
1. The pathophysiology of paininvolves an alteration of paintransmission pathways.
2. Tissue damage and inflam-mation sensitises nerve endingsthat transmit pain signals.
3. Increased sensitivity of neuronsto a repeated stimulus cancause benign sensations tobecome painful.
4. Injury to the peripheral nerves isoften associated with abnormalsensory function, causinga marked increase in patients’perception of pain.
5. An understanding of how thenervous system responds andadapts to pain is vital if we areto make sense of patients’ painexperiences.
Understandingwound pain andtrauma:an internationalperspectiveby CJ Moffatt, PJ Franks,H Hollinworth
This article discusses the resultsof an international collaborativesurvey which sought to explorepractitioners' understanding of painand trauma at wound dressingchanges.
Key findings
1. Dressing removal is consideredto be the time of most pain.
2. Dried out dressings and adher-ent products are most likely tocause pain and trauma at dress-ing changes.
3. Products designed to be non-traumatic are most frequentlyused to prevent tissue trauma.
4. Gauze is most likely to causepain. New products such ashydrogels, hydrofibres, alginatesand soft silicone dressings areleast likely to cause pain.
5. Awareness of product range andability to select dressings ishighly variable between coun-tries.
6. Use of valid pain assessmenttools is considered a low priorityin assessment with greaterreliance on body language andnon-verbal cues.
The first position document from EWMA
Pain at wound dressing changesis a peer-reviewed publication on the clinicalmanagement of pain in chronic wound care.
The EWMA position document Pain at wound dressing changes is down loadable on www.tendra.com/painposition

Silicone gel sheeting
First-line therapy in scar management 1
An international group of leading scar clinicians recommends silicone gel sheeting as first-linetherapy on immature, linear and widespread burn hypertrophic scars and minor keloids.1
Furthermore, silicone gel sheeting should be considered as first-line prophylaxis, initiated soon after surgical closure. Mepiform® is a self-adherent and discreet soft silicone dressing for scar care.It is widely used among professionals around the world.
Reference: 1) International Clinical Recommendations on Scar Management.Mustoe T A, et al. Plast. Reconstr. Surg, 2002, Vol 110, No. 2. 560-571.
Mölnlycke Health Care, Box 13080, 402 52 Göteborg, SwedenPhone. +46 31 722 30 00, Fax. +46 31 722 34 00, www.tendra.com

EWMA JOURNAL 2002 VOL 2 NO 246
The EWMA Cost Effectiveness Panel hasbeen established to address a need forevidence to support the use of appropri-
ate products within the field of wound care. Whilethe quality of clinical studies and trials of inter-ventions (of both products and systems) has,without doubt, improved greatly over the last 10years, there remains a dearth of quality publishedinformation on the costs and, more importantly,the cost effectiveness of wound care interventions.With increasingly more stringent limits on healthservice spending, and ever increasing expectationsfrom consumers, the gap between what is ex-pected of health care provision and what can beprovided is widening. European governmentsneed to judge health care interventions not onlyon their effectiveness, but also on their cost effec-tiveness in terms of maximum output in healthgains for the financial input provided.
THE AIMS OF THE PANELInitially the Cost Effectiveness Panel was devisedas a means of involving health professionals in costeffectiveness studies. There were several reasonsfor this approach:� to develop an understanding in health pro-
fessionals of the need for undertaking healtheconomic analysis.
� to provide them with appropriate under-standing of the types of studies being under-taken.
� to be able to use HE information when jus-tifying use of products within their services.
There has been great interest shown by EWMA’sindustrial partners; raising the profile of cost ef-fectiveness clearly has important consequences forindustry. These include:� using the cost effectiveness argument when
discussing reimbursement with govern-ments.
� ensuring greater usage of effective productsin existing services.
� developing new markets, where modernwound care products are not currentlyavailable.
The EWMA perspective is to work towards devel-oping the uptake and usage of cost-effective woundcare products. The Panel is interested in examin-ing models of care for new and existing services.The models would include use of products, but alsodelivery of care issues such as who delivers care,how the care is delivered, and what training is re-quired etc.
GETTING THE RIGHT TREATMENT TOTHE PATIENT AT THE RIGHT COSTThe initial work of the Cost effectiveness Panel willbe to undertake a scoping exercise throughoutEurope. Key opinion leaders, industrial partnersand council members of EWMA will be contactedto provide information on some of the key issuesof cost effectiveness and reimbursement withinEurope. The key themes to this study will be:� which types of product are available within
each country.� which clinical areas have access to the
particular product types.� which patients receive particular products,
and which do not.� who pays for each product type.� what reimbursement systems are in operation
within the countries.
From the generated data we hope to be able toanswer some of the key questions about the deliv-ery of products to patients. Key themes include:� Similarities and differences between countries
of Europe� Needs which are not met within countries� Equity of access to products based on:
wound type, age, ability to payhealth insurance, treatment location(community versus hospital)
� Opportunities for developing new marketsand expanding existing markets
We are still keen to hear from individual cliniciansabout developing cost effectiveness studies. TheCost Effectiveness Panel has representation fromthe EWMA Council, health economists, cliniciansand industrial partners. �
EWMA COST EFFECTIVENESS PANEL
Prof. Peter J. FranksCo-director of the Centre forResearch & Implementationof Clinical Practice, Thames
Valley University, UK.EWMA Council member
Correspondence to:Prof. Peter J Franks
Thames Valley UniversityCentre For Research and
Implementation of ClinicalPractice
Wolfson Institute of HealthSciences
32-38 Uxbridge RoadGB-W5 2B London
United KingdomTel: +44 181 280 5020Fax: +44 181 280 5020

EWMA JOURNAL 2002 VOL 2 NO 2 47
EWMA Corporate Sponsor Contact Data
EWMA news
Corporate A
ColoplastHoltedam 1-3DK-3050 HumlebækDenmarkTlf: +45 49 11 15 88Fax: +45 49 11 15 80www.coloplast.com
ConvatecSwekelys House Milton Road,IckenhamUB 10 8NS UxbridgeUnited KingdomTlf: +44 (0) 18 95 62 83 87Fax: +44 (0) 18 95 62 83 45www.convatec.com
Johnson & JohnsonCoronation RoadSL5 9EY AscotBerkshire, United KingdomTlf: +44 1344 871 000Fax: +44 1344 872 599www.jnj.com
KCI InternationalBeech Avenue 54-801119 PW Schiphol-RijkNetherlandsTlf: +31 (0) 20 658 6484Fax: +31 (0) 20 658 6701www.kcimedical.com
Corporate B
3M Health CareMorley Street, LoughboroughLE11 1EP LeicestershireUnited KingdomTlf: +44 1509 260 869Fax: +44 1 509 613326www.mmm.com
Cook limitedMonroe HouseLetchworthSG6 1LN HertfordshireUnited Kingdomwww.cookgroup.comTlf: +44 1462 473 100Fax: +44 1462 473 190
1e. Stationsstraat 18b2700 MAZoetermeerThe netherlandsTlf: +31 (0)79-3539600Fax: +31 (0)79-3539650www.nutricia.com
Mölnlycke Health Care AbBox 13080402 52 Göteborg, SwedenTlf: +46 31 722 31 08Fax; +46 31 722 3000www.tendra.com
Smith & NephewPo Box 81, Hessle RoadHU3 2BN Hull, United KingdomTlf: +44 (0) 1482 225 181Fax: +44 (0) 1482 328 326www.snwmd.com
Tyco HealthcareVia Cristoforo Colombo 45600145 Rome, ItalyTlf: +39 335 72 95 110Fax: +39 0654 608 262www.tycohealthcare.com
Lohmann & RauscherP.O. BOX 23 43 NeuwiedD-56513 GermanyTlf: +49 (0) 2634 99-6205Fax: +49 (0) 2634 99-1205www.lohmann-rauscher.com

EWMA JOURNAL 2002 VOL 2 NO 248
European Wound Management Association
EducationalDevelopment Project
Progress so farOver the last year, the EWMA Educational De-velopment Panel has completed a needs analysisto identify the wound management educationalrequirements across Europe. This was carriedout using a sample of European countries in-cluding Belgium, Denmark, Hungary, Italy,Latvia, Portugal, Sweden and the United King-dom. The project’s general aims and generallearning outcomes have been updated to reflectthe new knowledge obtained from this analysis.
General aims1. Provide students and healthcare profession-
als with the knowledge and skills to equipthem to perform their role in the delivery ofoptimal wound care.
2. Provide contemporary interdisciplinarywound management education that is en-dorsed by organisations affiliated toEWMA.
3. Provide quality standards against whichother organisations can evaluate existingwound management programmes.
4. Achieve European acceptance by developingan educational framework that harmoniseswith the European Commission’s educa-tional initiatives in order to disseminate bestpractice in wound care.
General learning outcomesThe overall EWMA educational frameworkprovides opportunities for students and healthprofessionals to develop and demonstrateknowledge, understanding, skills and otherattributes in the following areas:1. The aetiology, epidemiology, prevention and
management of a variety of commonlyoccurring wounds.
2. The science of wound prevention/repair andassociated problem solving and clinical re-search.
3. The management, treatment and care of peo-ple with wounds and related tissue problems.
4 The psychological, legal, ethical and economicimpact that wounds have on the patient, fam-ily and society as a whole and the implicationsthese have for health care.
The next stepThe second stage of the Educational Develop-ment Project is the development of the actualcurriculum. It is envisaged that the curriculumwill be interdisciplinary, focusing on processesinstead of profession. The aim is to develop aflexible curriculum consisting of a number ofmodules each focusing on a specific aspect ofwound management.
Based on the knowledge obtained from theneeds analysis, a standard template has been de-veloped that will form the basis for each module.The first modules on which development hasalready begun are:� Physiology of Wound Healing & Tissue Repair� Wound Assessment� Acute Wounds� Leg Ulcer Management� Diabetic Foot� Pressure Ulcer Prevention & Management� Oncology Wounds
Each module will be developed by a small groupof advisors drawn from related wound organisa-tions and key opinion leaders. To strengthen thevalue of the modules we aim to affiliate at leastone organisation with module-specific knowledgeto each module. Furthermore we welcome inputfrom other key persons within each area, so if youfeel you have valuable input to offer any of theabove modules, please contact MadeleineFlanagan at [email protected].
Prof. Finn GottrupMD, DMSci
Professor of WoundHealing and Surgery,
and Director ofCopenhagen Wound
Healing Center,Bispebjerg University
Hospital, Copenhagen,Denmark
Specialist in GeneralSurgery and Surgical
Gastroenterology.Assoc. Prof. of
Anatomy, University ofAarhus.
Chair of CopenhagenWound Healing Center,
University ofCopenhagen.
EWMA Immediate PastPresident
Council Member of theEPUAP.
President of DSFS.President of ETRS
1998-99
Madeleine FlanaganMSc, BSc (Hons)
Nursing, Dip NursingRGN, Principal Lecturer,Div. of Post-Registration
Nursing, University ofHertfordshire, UK.
Certification Education,Scheme Leader for BSc(Hons) Tissue Viability,
MSc Advancing Practicein Tissue Viability.
Editorial Advisor for theJournal of Wound Care
and Journal of TissueViability.
Update
EWMA JOURNAL 2002 VOL 2 NO 2 49
The European Pressure Ulcer Advisory Panel(EPUAP) invited EWMA to organise aseminar on the EWMA Education Project to
be held prior to the EPUAP conference in Budapest inSeptember this year. Attended by approximately 30delegates travelling from almost as many countries, theseminar was very successful. All the delegates showed agreat eagerness to improve the education provision inwound care for all health care professionals, patients,carers and the wider public.
Carol Dealey provided the background and aims of theproject that are underpinned by the philosophy that‘EWMA aspires to establish a framework to createeducational standards for wound healing/managementwithout taking away any professional autonomy indifferent countries for determining how these standardsare achieved.’
Christina Lindholm graphically demonstrated the needfor education and educational materials by describingher visit to Latvia and the work there. Sue Bale thendescribed the position of EPUAP in relation to educa-tion and information regarding pressure ulcers. She alsoexplained the view that EPUAP’s role was to collatewhat educational materials/courses are available in rela-tion to pressure ulcers and then to ensure their member-ship was kept informed. This role potentially comple-ments that of the EWMA Education Project.
A lively discussion followed these presentations. Themain points of discussion centred around the need tovalidate what is already available and to have a central(web-based) reference point, preferably in a variety oflanguages.
Perhaps the most encouraging aspect of the seminar wasthe genuine desire expressed by many to collaborate andco-operate in order to improve patient care.
Carol Dealey
EWMAGrantsEWMA will in 2003 hand out awardswithin following areas:
EWMA news
EWMA/EPUAPEducation Seminar
Research� Salary Support� Research expenses� The Award will not cover overheads or
capital grants.� The agreed term of the Award should provide
for preparation of a final report to EWMA.
Education� Expenses incurred while following wound care
courses such as, purchase of books, travel andsubsistence.
� The award will not cover course fees, overheadsor the cost of attending conferences.
EWMA panel awards� If a relevant project is presented to EWMA Coun-
cil, council may decide to donate a grant in orderto help the objectives of EWMA panels. For thepanels and their objectives please see the articlein this issue or refer to the EWMA homepage.
EligibilityAwards are only open to current full members of theEuropean Wound Management Association (EWMA).
ApplicationFor information on application, please refer to:www.ewma.org
Application dateClosing date for applications, March 1st 2003.

EWMA JOURNAL 2002 VOL 2 NO 250
At the EWMA meeting in Dublin 2001,representatives from GNEAUPP andEWMA met to discuss the joint
GNEUAPP/EWMA conference in Granada2002. Dublin was a major step towards a trueEuropean co-operation within the field ofwound healing and management. EWMA be-lieves that only by fully involving the nationalorganisations will it be possible to develop thedelivery of care across Europe.
One year later the first participant registered atthe impressive Granada Exhibition Centre.Many more were to follow; in fact 2300 del-egates from all over Europe joined the event,surpassing even the most optimistic forecasts.The huge amount of work put in by EWMAand GNEAUPP, and especially by Javier A.Soldevilla, president of GNEAUPP and vicepresident Joan-Enric Torra Bou, paid off hand-somely.
The official programme was opened on Thurs-day at 10 a.m. by the presidents of GNEAUPPand EWMA, Javier Soldevilla and ChristineMoffatt. In the following two and a half days,10 plenary sessions, 139 free papers and 222posters were presented. Added to this, the largeexhibition, the many satellite symposia, and thewealth of information presented was very im-pressive and, at times, overwhelming.
The number of interesting presentations couldhave called for more prizes and made the selec-tion process a positive challenge.
One of the major impediments to internationalco-operation has been the language barrier. Anew initiative at the EWMA conference to ad-dress this matter was the introduction of a totalbi-lingual concept including translation of allmaterials, programme, abstracts etc., as well as
The 12th Conference of theEuropean Wound Management Association
QUALITY OF LIFEMay 23rd-25th, 2002 Granada Spain
simultaneous translations during all sessions.Based on the very positive reaction of the par-ticipants there is no doubt that this will becomean integrated part of future EWMA confer-ences.
The cost of simultaneous translations is high,but when you experience a challenging discus-sion between a Spanish speaker and an English-speaking participant, you understand that it is aworthwhile expenditure. Communication be-tween two people of different languages wouldotherwise be very difficult if not impossible.EWMA feels that opening communication willcontribute to the development of a true pan-Eu-ropean knowledge exchange.
Finn GottrupEWMA Recorder
Javier Soldevilla AgredaGNEAUPP President
Joan-Enric Torra I BouGNEAUPP
Vice President
Entrance to the beautiful Granada conference centre.
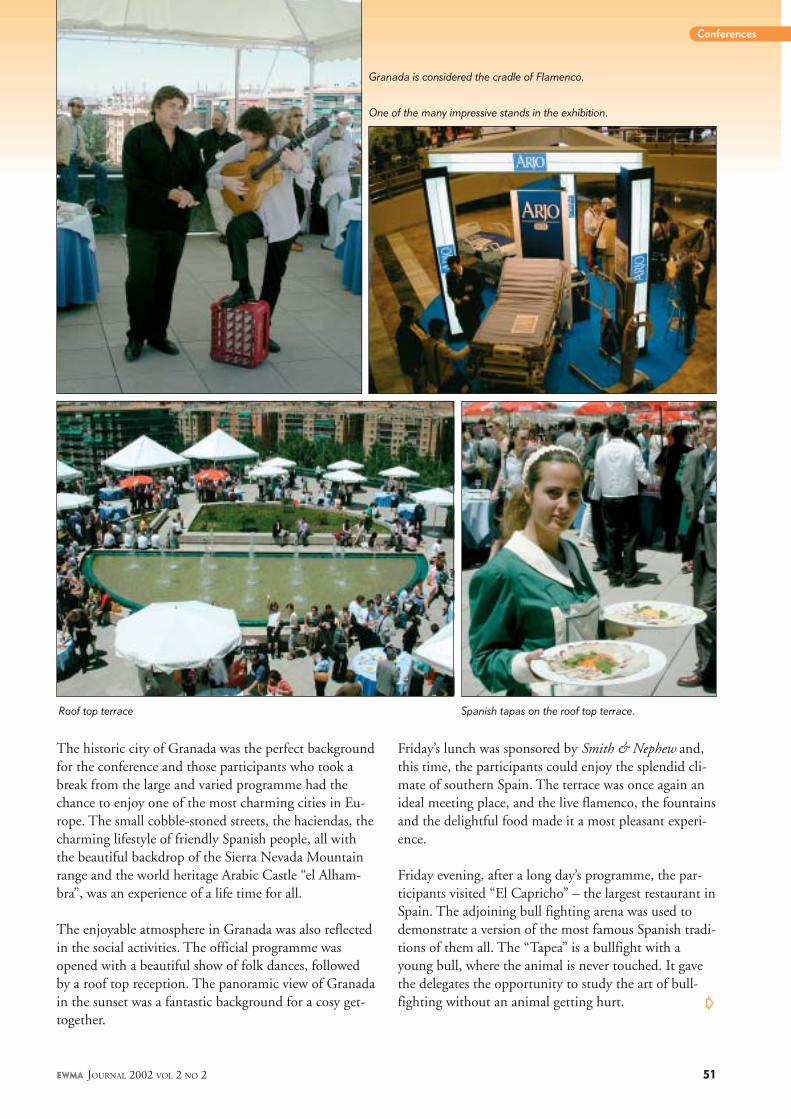
EWMA JOURNAL 2002 VOL 2 NO 2 51
The historic city of Granada was the perfect backgroundfor the conference and those participants who took abreak from the large and varied programme had thechance to enjoy one of the most charming cities in Eu-rope. The small cobble-stoned streets, the haciendas, thecharming lifestyle of friendly Spanish people, all withthe beautiful backdrop of the Sierra Nevada Mountainrange and the world heritage Arabic Castle “el Alham-bra”, was an experience of a life time for all.
The enjoyable atmosphere in Granada was also reflectedin the social activities. The official programme wasopened with a beautiful show of folk dances, followedby a roof top reception. The panoramic view of Granadain the sunset was a fantastic background for a cosy get-together.
Friday’s lunch was sponsored by Smith & Nephew and,this time, the participants could enjoy the splendid cli-mate of southern Spain. The terrace was once again anideal meeting place, and the live flamenco, the fountainsand the delightful food made it a most pleasant experi-ence.
Friday evening, after a long day’s programme, the par-ticipants visited “El Capricho” – the largest restaurant inSpain. The adjoining bull fighting arena was used todemonstrate a version of the most famous Spanish tradi-tions of them all. The “Tapea” is a bullfight with ayoung bull, where the animal is never touched. It gavethe delegates the opportunity to study the art of bull-fighting without an animal getting hurt.
Conferences
Roof top terrace Spanish tapas on the roof top terrace.
Granada is considered the cradle of Flamenco.
One of the many impressive stands in the exhibition.
�

EWMA JOURNAL 2002 VOL 2 NO 252
Peter Vowdenwas constitutedas new EWMApresident.
Part of the EWMA Council at the conference dinner.
President of the Italian Nurse Association for the Study ofCutaneous Wounds and co-organiser of the EWMA 2003conference in Pisa, Andrea Bellingeri with company.
Conferences
After the show the guests were led into the dining roomnext door – an impressive sight with more than 1900beautifully decorated tables in the same room. The rest ofthe evening was spent on a brilliant dinner and a variety ofentertainment from GNEAUPP and EWMA.
The Granada conference was an ambitious meeting offeringall delegates interesting, stimulating and enjoyable days inSouthern Spain. Next year the EWMA conference will beheld in Pisa, Italy, and we hope that you, once again, willjoin the event to contribute to the growing development ofinternational wound healing and wound management.For a detailed description of Pisa, please refer to the articleby Dr. Marco Romanelli elsewhere in this Journal.
Kind regards Finn Gottrup, EWMA recorder
Session in the Manual de Falla Hall. GNEAUPP President Javier A. Soldevilla.

EWMA JOURNAL 2002 VOL 2 NO 2 53
Germany, 12Italy, 19Japan, 8Mexico, 456Netherlands, 11Perú, 94Portugal, 95Puerto Rico, 17
Spain, 3822Sweden, 24Switzerland, 11United Kingdom, 21Unknown, 279Uruguay, 60USA, 262Venezuela, 38
The 2002 GNEAUPP/EWMA conference was the firstconference for these organisations that was broadcastedthrough the Internet. Interested from all around the world
were able to follow the lectures in cyberspace. This was made possi-ble due to the co-operation of salutmultimedia.com and the Socie-dad Española de Enfermería en Informática e Internet (Spanish In-ternet and Informatics Nursing Society) www.seei.es
Grenada’s web cast files, which are available on www.gneaupp.organd www.ewma.org, have been visited by more than 6000 personssince the conference:
Argentina, 328Belgium, 21Bolivia, 12Brazil, 38Chile, 239Colombia, 73Costa Rica, 21El Salvador, 16
Data updated the 30th of September
The Internet has given us a great possibility for spreading the mate-rials from the conference to the many colleagues unable to attend,especially to those from South America. It also offers great valuedocuments. Videos of the conferences and discussions are usuallyare not included in abstracts or proceedings, but can now beaccessed and used in the future.
Before the end of the year EWMA’s web site, with a new design, willalso include PDF files of all the abstracts of oral presentations andposters accepted for the conference.
Joan-Enric Torra I Bou, EWMA website group
Granada Conference 2002in Cyber Space

EWMA JOURNAL 2002 VOL 2 NO 254
Year City Country Theme President
1991 Cardiff United Kingdom Advances in Wound Management Terrence Turner
1992 Harrogate United Kingdom Advances in Wound Management
1993 Harrogate United Kingdom Advances in Wound Management Carol Dealey
1994 Copenhagen Denmark Advances in Wound Management David Leaper
1995 Harrogate United Kingdom Advances in Wound Management Chris Lawrence
1996 Amsterdam Holland Wound Healing Therapy:a critique of current practice and opportunities for improvement George Cherry
1997 Milano Italy New Approaches to the Advancement of Chronic Wounds Finn Gottrup
1997 Harrogate United Kingdom Improving Clinical Outcomes through Education
1998 Madrid Spain Acute and Chronic Wounds: Is there a Difference?
1998 Harrogate United Kingdom Patient Centred Wound Care
1999 Harrogate United Kingdom Taking Wound Care into the 21st Century Christine Moffatt
2000 Stockholm Sweden Advances in Wound Management
2001 Dublin Ireland Back to the Future
2002 Grenada Spain Chronic Wounds and Quality of Life Peter Vowden
2003 Pisa Italy Team-work in Wound Care – The Art of Healing
Terrence Turner Carol Dealey Chris Lawrence George Cherry Finn Gottrup Christine Moffatt Peter Vowden
EWMA Past Presidents & Conference History
Conference CalendarConference 2002 Place Country
2nd European Medical & Biological Engineering Conference (EMBEC’02) Nov. 22-26 Boston USA
2003 Place Country
8th NPUAP National Conference Feb. 21-22 New Orleans USA
Tissue Viability Society Spring Conference 2003 April 8-9 Blackpool United Kingdom
Symposium on Advanced Wound Care Apr./May 28-1 Las Vegas USA
The Wound Healing Society 13th Annual Educational Symposium & Exhibition May 3-8 Seattle USA
European Wound Management Association May 22-24 Pisa Italy
Diabetic Foot May 22-24 Noordwijkerhout The Netherlands
ETRS Annual Meeting Sept. 24-26 Amsterdam The Netherlands
European Pressure Ulcer Advisory Panel Sept. Tampere Finland
2004 Place Country
2nd World Union of Wound Healing Societies’ Meeting July 8-13 Paris France
David Leaper
Conferences

A Novel Antibacterial TA Novel Antibacterial TA Novel Antibacterial TA Novel Antibacterial TA Novel Antibacterial Trrrrreatment for Difeatment for Difeatment for Difeatment for Difeatment for Difficult to Heal Wficult to Heal Wficult to Heal Wficult to Heal Wficult to Heal WoundsoundsoundsoundsoundsEWMA 2002, Granada: Satellite Symposia 24th May - Sponsored by Coloplast A/S
Edited by Mette Qvist Jensen & Flemming Wilhelmsen, ColoplastThe Satellite symposium ‘A Novel Antibacterial Treatment for Difficult to Heal Wounds’ sponsored by Coloplast A/S was held during the 12th annual
EWMA Conference on the 24th May in Granada. In the following some of the main issues are highlighted. A comprehensive review will be presented later.
IntrIntrIntrIntrIntroduction by the chairman:oduction by the chairman:oduction by the chairman:oduction by the chairman:oduction by the chairman:Prof. Finn Gottrup, MD., DMSci, Copenhagen Wound Healing Centre, Denmark
The symposium was introduced with a discussion of delays in the normal healingprocess that may be caused by local as well as systemic factors like local bloodsupply, tissue damage and not least infection.
The aim of this symposium was to explore these issues by focusing on thewound bed preparation principle, the use of silver as a topical antiseptic andfinally the clinical experience of two new dressings containing silver.
1. W1. W1. W1. W1. Wound Bed Pround Bed Pround Bed Pround Bed Pround Bed Preparation – Principle & Practiceeparation – Principle & Practiceeparation – Principle & Practiceeparation – Principle & Practiceeparation – Principle & PracticeAssociate professor Gary Sibbald, MD, Department of Medicine, University ofToronto, Canada.
WBP is really a synthesis of existing knowledge but “viewed with new eyes”:debridement, bacterial balance or control and moisture balance.
Debridement in a chronic wound is essential for the outcome of furthertreatment and may be facilitated by autolytic, enzymatic, mechanical and/orsurgical procedures.
All chronic wounds are contaminated. Multiplying bacteria will at a certainstage begin to cause damage and delayed healing. The wounds may stophealing typically before we have the clinical signs of infection. The bacterialimbalance may be caused by the number of bacteria, their virulence and themost important is host resistance.
There are probably two ‘bacterial compartments’ in a chronic wound that canbe out of balance: a superficial compartment and a deep one. If thesuperficial wound bed is out of balance, a non-healing situation may occurwith exuberant friable bright red granulation tissue, and increased amount ofexudate addressing the need for moisture balance. In the deepercompartment warmth and tenderness may be present along with pain,erythema greater than 2 cm beyond ulcer margins or probing to bone.
2. Silver as a Moder2. Silver as a Moder2. Silver as a Moder2. Silver as a Moder2. Silver as a Modern Antibacterial Agentn Antibacterial Agentn Antibacterial Agentn Antibacterial Agentn Antibacterial AgentMrs Liz Scanlon, RGN, RM, Cert D.N., M.Sc., Leeds CMHS Trust, England
Silver is generally considered to be effective against a wide spectrum of bacteriaand fungi, protozoa and endospores, including antibiotic resistant bacteria MRSA,VRE. Further the development of resistance or sentisation is limited comparedto antibiotics.
ModerModerModerModerModern antisepticsn antisepticsn antisepticsn antisepticsn antiseptics are recognised as having an important role in wound bedpreparation by reducing the bio-burden and participate in the active debridementthat is key to effective wound management and exudate reduction by reducingthe inflammatory response. They are also easy to apply and they are morestable and provide sustained release of antiseptic and some also maintain amoist wound environment.
Silver as an anti-micrSilver as an anti-micrSilver as an anti-micrSilver as an anti-micrSilver as an anti-microbialobialobialobialobialThe benefit of using sustained release of silver is that it ensures a constant lowdose of silver decreasing the risk of cellular and tissue damage. It also ensuresa constant antiseptic effect and combines the benefits of the carrier dressingwith the silver e.g. ContrContrContrContrContreeteeteeteeteet Hydrocolloid has all the benefits of slow release ofsilver as well as the hydrocolloid features, i.e. exudate management and creation
of moist wound healing environment.The release of silver from the ContrContrContrContrContreeteeteeteeteetHydrocolloid is shown in figure1.
Figure 1. The Silver release profile of ContreetContreetContreetContreetContreet Hydrocolloid.
It can be concluded that the new modern silver dressings, such as ContrContrContrContrContreeteeteeteeteetHydrocolloid, are far safer and more efficacious than the old fashionedantiseptics.
3. Clinical Experience with Contr3. Clinical Experience with Contr3. Clinical Experience with Contr3. Clinical Experience with Contr3. Clinical Experience with Contreet Hydreet Hydreet Hydreet Hydreet Hydrocolloid and Controcolloid and Controcolloid and Controcolloid and Controcolloid and Contreet Foameet Foameet Foameet Foameet FoamProfessor Finn Gottrup, Denmark
ContrContrContrContrContreeteeteeteeteet Hydrolloid was tested in 2 studies, including in total 67 venous legulcer patients (ABI>0,8) in 9 European centres.
ContrContrContrContrContreeteeteeteeteet Foam has been investigated in 1 study on 25 patients with venousleg ulcers (ABI>0,8) in 3 Danish centres.
The ulcers included had a delay in healing compared to expectations, unhealthyand dull looking granulation tissue. Many were malodorous and some painfulwith a high amount of exudate. As such the ulcers were judged to be in abacterial imbalance.
ContrContrContrContrContreeteeteeteeteet HydrocolloidThe included ulcer had not been showing progress before treatment withContrContrContrContrContreet.eet.eet.eet.eet. The overall reduction in the mean ulcer area in study 1 was 41,7 %after 11 days of treatment. In study 2, 31% healed after 8 weeks of treatmentand the overall reduction in wound area was 74,5%. Hence a remarkableclinical improvement in both studies was observed.
The odour almost disappeared and the amount of exudate decreased as well.Pain experience was also significantly reduced (from 40% to 15%). No infectionsoccurred. Finally no adverse events were related to the dressings.
ContrContrContrContrContreeteeteeteeteet FoamAt first the patients were treated with BiatainBiatainBiatainBiatainBiatain for one week and then 4 weekswith ContrContrContrContrContreeteeteeteeteet Foam, and finally 1 week with BiatainBiatainBiatainBiatainBiatain again.
No other antiseptics or antibiotics were used during the treatment period.
The relative reduction of the ulcer area after 4 weeks of treatment was 56% onthese ulcers with delayed healing. One ulcer healed completely during thisperiod. Interestingly when changing to standard treatment after 4 weeks withContrContrContrContrContreeteeteeteeteet Foam the relative ulcer area increased in size.See figure 2.
Figure 2. ContreetContreetContreetContreetContreet Foam clinical studies, median wound area reduction.
The treatment demonstrated effectiveness in reduction of necrotic tissue,unhealthy granulation tissue along with increase in healthy granulation tissue.
No adverse events were reported and no patients developed infections duringthe study period.
It can be concluded that ContrContrContrContrContreeteeteeteeteet Foam ‘kick starts’ ulcers with delayedhealing by effectively killing bacteria and by managing the exudate due to theaction of silver and the high absorption capacity. Further the fast wound healingis accompanied by a reduction in odour and pain.
Release of Silver
0
100
200
300
400
0 10 20 30 40 50
Time, hours
Am
ou
nt S
ilv
er
rele
as
ed
µg
/9.1
cm
2
Release of Silver
0
100
200
300
400
0 10 20 30 40 50
Time, hours
Am
ou
nt S
ilv
er
rele
as
ed
µg
/9.1
cm
2
Contreet
week follow-
Relative Ulcer Area
0
20
40
60
80
100
120
0 1 2 3 4 +1
Week
Median
Contreet
week follow-
Relative Ulcer Area
0
20
40
60
80
100
120
0 1 2 3 4 +1
Week
Median
ContrContrContrContrContreeteeteeteeteet - Get healing started

EWMA JOURNAL 2002 VOL 2 NO 256
The 6th Open Meeting of the EuropeanAdvisory Panel (EPUAP) was held inBudapest, 18-21st September 2002.
The theme of the meeting was ‘Pressure Ulcers– a quality of care indicator?’ This theme domi-nated the first day of the conference duringwhich a number of speakers addressed this issuefrom a range of perspectives, including, mostimportantly, the patients’. Patricia Price (Car-diff, UK) presented what little research has beenundertaken in looking at quality of life issues inpatients with pressure damage and some of thechallenges faced in trying to improve under-standing in this area.
Following presentations regarding pressureulcer management and prevention in differentparts of Europe, USA and Japan, the LifetimeAchievement Award was presented to ProfessorJoe Barbenel of Strathclyde University, Scotland.This annual award is presented to those whohave made a significant contribution to thefield of pressure ulcers. Professor Barbenel thenaddressed the conference presenting his viewson the use of prevalence surveys in measuringpressure ulcers and the effectiveness of currentprevention strategies.
The following two days were a mixture ofplenary and concurrent sessions with free pa-pers and updates on various EPUAP workinggroups and projects. One project is the PEPUS(Pan-European Pressure Ulcer Study of patientswith hip fracture) Survey, which has been un-dertaken in six countries across Europe (Fin-land, Portugal, Sweden, Italy, Spain and UK)with the aim of gaining greater understandingof the causes of pressure ulcers in patients withhip fractures. Christina Lindholm (Stockholm,Sweden) presented the preliminary results fromthose centres that have completed their surveys.However, centres in other countries have alsoexpressed an interest in participating, so thestudy is still ongoing at present.
Another project undertaken by EPUAP hasbeen to develop a tool for undertaking a pres-sure ulcer prevalence survey that could be usedin any country. To date, this tool has been pi-loted across five countries (Belgium, Italy, Por-tugal, Sweden and UK) and surveyed a total of5947 patients. Several papers were presented bythe working group, which explained the projectin some detail, and stressed that the patientssampled were not a representative group as thepurpose was to test the data collection tool.However, within the survey 18.1% of patientshad a pressure ulcer and, of these patients, only4.6% were being provided with adequate pre-ventative care. There certainly seems to be scopefor improvement. Some members of this grouphad also produced a draft position paper onmonitoring the prevalence and incidence ofpressure ulcers*.
The final group to report to the conferencewas the Support Services Working Group com-prising a mixture of scientists, manufacturers ofpressure redistributing equipment and clini-cians. The Group has produced draft guidelineson the laboratory evaluation of pressure redis-tributing support surfaces*. These guidelineswere presented for further discussion and de-bate.
As with all such conferences there was muchdebate both within and outside the sessions.The conference ended with the presentation ofposter prizes and details of the venue for nextyear’s conference: Tampere, Finland. And, asthis was Hungary, there were also a number ofmagnificent cakes served with champagne! �
Report on the 6th European PressureUlcer Advisory Panel Open Meeting
*Both these papers can be found on the EPUAP website(www.epuap.org/review4_1/index.html)
Carol DealeyMA BSc (Hons) RGN
RCNTSchool of Health
SciencesUniversity ofBirmingham
andUniversity Hospital
Birmingham NHS Trust

EWMA JOURNAL 2002 VOL 2 NO 2 57
Conferences
In association with the Budapest meeting ofthe parent organisation European Associa-tion for the Study of Diabetes (EASD) the
DFSG held a joint meeting with NEURO-DIAB (Diabetic Neuropathic Study Group) atHotel Balatonfured. 157 participants from 29countries from Europe, North and South-america, Australia, Asia and Africa attended themeeting. There were 103 scientific papers and 3symposia, each with 4-5 invited speakers.
On the first day there was a joint symposiumon basic research in peripheral neuropathy andan update on the effect of alpha-lipoic acid.Following this symposium each of the two or-ganisations had a series of separate sessions.
Major sponsors Johnson & Johnson andBristol-Myers Squibb Company each had asymposium of 1 hour for the DFSG:Johnson & Johnson: Advanced wound healingtherapies inducing alteration in wound bio-chemistry.Bristol Myers Squibb: Diabetic infections inrelation to a new antibiotic: Garenoxacin.
For the DFSG 103 papers had been selected:36 for oral presentations and 67 for postersessions over a period of 2 days. There were6 DFSG oral sessions on
Basic and Clinical ScienceClassification, Foot Clinic and EpidemiologyOrthopedic SurgeryUremia and InfectionRevascularization and BiomechanicsCharcot
In order to reinforce the importance of posters,10 of these had been selected for short andbrisk oral presentation with 4 minutes allocatedfor each and with the maximum of 4 slides.This experiment running over 1 and 1/2 hourturned out to be very satisfactory. Moreover,
Diabetic Foot Study Group (DFSG)meeting in Hungary (Lake Balaton)
increased time had been allocated for usualposter presentations with guidance of chairmen.Thus there was 2 sessions of 1 hour, each with6 simultaneous poster sessions. The topics were
Epidemiology/screening 2 sessionsWound healing/Outcome 2 sessionsDiagnostics 2 sessionsFoot clinic 2 sessionsSurgery 1 sessionVaria 2 sessionsClassification 1 session
The meeting evaluation was satisfactory.The programme received ratings of:
Excellent 21%, above average 60%, average 9%,fair 9%, poor 0%
Local organisersProfessor Peter Kempler, Dr Eva Kadar,dr. Zsolt Hermanyi.
NEURODIAB executive committee:Chairman professor Dan Ziegler,Vice Chairman Professor Goran Sundkvist,Professor Johannes Jacobsen,Dr. Bert Bravenboer, Professor Poul Valensi,Professor Norman Cameron
DFSG executive committee:Chairman Dr Michael Edmonds,Vice Chairman Dr Per Holstein,DMSc, secretary Professor Max Spraul,treasurer Dr. Luigi Uccioli, Dr Irina Gourieva,chiropodist Kirsten Larsen, Dr. Manes Christos,Dr Alberto Piagessi, Dr Nicholas Schaper,Dr. Vilma Urbancic-Rovan.
DFSG organising secretariat:Anne Roscoe, Eve Stamm
You can access the programme on the internet on:http://dialex.co.uk/conferences/diabetic_foot_study_group_2002/programme.pdf
�
Per E Holstein, DMScVice Chairman DFSG
August 29th - September 1st 2002

EWMA JOURNAL 2002 VOL 2 NO 258
April 24th 2002 the Danish WoundHealing Society hosted the “first Inter-national Workshop on Multidisci-
plinary Concepts in Wound Healing”. Thebackground for the meeting was the growinginternational understanding of the importanceof a definition of a multidisciplinary approachand structure of the wound healing area in thefuture.
More than 60 key opinion leaders withinthe area were gathered in the beautiful sur-roundings on the coast of North Sealand, todefine a strategy for a general acceptanceapproach and structure for the wound healingarea.
Various important topics were coveredamong which the following can be mentioned.
Professor Finn Gottrup was chairman andstarted the day with a brief overview of theproblems faced in Denmark. In spite of anexpected well functioning treatment systemmany patients suffering of problem wounds stillhas not received a correct diagnosis. This andother problems can be solved by a betterorganisation of the treatment area by establish-ment of a structure including centers andteams. Clinical work, education and researchwith cost effectiveness assessments are impor-tant parts of such a structure.
Professor John Posnett from the UnitedKingdom talked about cost effectiveness. Heintroduced the terms “cost effectiveness” and“clinical effectiveness”. Methods that can docu-ment knowledge must be used to maximiseWound Healing and treatment within the exist-ing framework. Cost effectiveness is not alonesaving money, but optimising the result withthe current funds available.
Professor Luc Teot from France, clinical headnurse Kirsten Müller, Denmark and professorKeith Harding United Kingdom spoke on theimportance of well-educated health care per-sonnel, and how such an education could beestablished.
Professor Christine Moffatt, United Kingdomaddressed the problem on a European level. Notsurprisingly, very few are interested in thishealth care problem in Europe, and the concep-tion of best practice is very diverse.
Professor Vincent Falanga and professor GertKövecker described the initial steps of organisa-tion in the US and Germany. The reimburse-ment problem for the American wound patientand the need for academic based wound healingcenters are main problems in the US. A compu-terised registration system between differenthospitals in the southern part of Germany is theinitial step of organisation in this country.
The final panel discussion chaired by dr.George Cherry and Professor Christine Moffattcovered many important questions for thefuture structure of Wound Healing area.
At the end of the day professor Finn Gottrupcould conclude that it had been an interestingand promising workshop, which clearly hadshown the need for a strong future strategy forthe organisation of the wound healing area.In the next issue of EWMA Journal a moredetailed description of this workshop and theproject will be published. �
First International Workshopon Multidisciplinary Conceptsin Wound Healing
Finn GottrupProfessor of Wound
Healing and Surgery
President [email protected]
Danish WoundHealing Society

EWMA JOURNAL 2002 VOL 2 NO 2 59
Meeting in Latvia 2001 (from left): Sergejs Kolesnikovs, Ieva Kabuce,Ints Undris, Tatjana Ivanova, Finn Gottrup, Christina Lindholm,Pauls Bartulis, Henrik J. Nielsen.
The Melngalvju Nams in Riga. The building was destroyed duringWorld War II but has now been reconstructed in its original image.
Finn Gottrup, Christina Lindholm and HenrikNielsen lectured and represented EWMA. Dr IntsUndris, Dr Sergejs Kolesnikovs and RN TatjanaIvanova also lectured. A model for the LatvianWound Treating Organization was proposed andaccepted with great enthusiasm by the audience.
On the 3rd of May 2002, the Latvian WoundTreating Organization was officially established. Theaims of the Organization are:1) to promote education in wound management
among nurses and physicians2) to promote reimbursement for wound care
materials3) to increase the involvement of nurses in
wound management4) to coordinate wound management among
different specialists (surgeons, GPs etc).
This year on October 24, the Organization hasorganised a study day at which participants willdiscuss and examine many aspects of pain man-agement and ulcer care. Christina Lindholm hasbeen invited to attend as a guest speaker.
The EWMA meeting in Granada was attendedby Drs Undris and Kolesnikovs, and RN TatjanaIvanova. Their enthusiasm for, knowledge of andinterest in wound healing is impressive and bodeswell for the future of wound-care as a specialism inLatvia.
EWMA welcomes the Latvian Wound TreatingOrganization as an important associated memberorganization, and wishes our Latvian colleaguesgood luck in their important future work. �
L atvia, one of the Baltic countries previ-ously behind the “iron curtain” has thebeautifully restored city of Riga as its
capital. Riga benefits from a genuine atmos-phere of “Old Town”, and also features an ex-ceptionally good museum of medical history.
The population of Latvia, approximately 2,5million comprising a 54/46% ratio of womento men, is supported by 150 hospitals and12000 physicians. Of the 150 hospitals 72 aremajor and of the 12000 doctors 2000 are GPs.Twenty-three percent of the population is be-tween 18-60 years and half a million people areretired; many living on minor pensions. Thephysicians belong to 90 different associations.In addition there are 15000 nurses in Latvia,belonging to 11 different associations.
As is the case in most European countries,the trends in Latvian Health Care, are towardscutting costs by closing hospital beds, and fo-cusing on home care and GP-run clinics. Untilnow, wound-care has not been seen as aspecialism – dressings are not reimbursed forthe patients, and education in wound manage-ment has not been specifically addressed. How-ever, this situation is chaanging as interest inwound healing has been raised by a small groupof interested doctors and nurses.
The 2001 EWMA meeting in Dublin wasvisited by a Latvian delegation, and in Decem-ber 13, 2001, EWMA was invited to join thefirst meeting of the proposed Latvian WoundHealing Organization. Approximately 60 physi-cians and nurses attended the meeting, at which
Wound Healing Association in Latvia
Christina Lindholm
Conferences
Christina LindholmRN, PhD, AssociateprofessorDirector R&D,Caring Sciences,Karolinska hospitalStockholm, [email protected]

EWMA JOURNAL 2002 VOL 2 NO 260
ABSTRACT
BackgroundVarious solutions have been recommended forcleansing wounds, however normal saline isfavoured as it is an isotonic solution and does notinterfere with the normal healing process. Tapwater is commonly used in the community forcleansing wounds because it is easily accessible,efficient and cost effective, however, there is anunresolved debate about its use.
ObjectivesThe objective of this review was to assess the effectsof water compared to other solutions for woundcleansing.
Search strategyRandomised and quasi-randomised controlledtrials were identified by electronic searches ofCochrane Wounds Group Specialised TrialsRegister, MEDLINE, EMBASE, CINAHL, andthe Cochrane Controlled Trials Register. Primaryauthors, company representatives and contentexperts were contacted to identify eligible studies.Reference lists from included trials were alsosearched.
Selection criteriaRandomised and quasi randomised controlledtrials that compared the use of water with othersolutions for wound cleansing were eligible forinclusion. Additional criteria were outcomes thatincluded objective or subjective measures ofwound infection or healing.
Data collection & analysisTrial selection, data extraction and quality assess-ment were carried out independently by tworeviewers and checked by a third reviewer. Differ-ences in opinion were settled by discussion. Somedata were pooled using a random effects model.
WATER FORWOUND CLEANSING
DEBRIDEMENTOF DIABETIC FOOTULCERS
ABSTRACT
BackgroundFoot ulceration is thought to affect 15% of people with diabetesat some time in their lives.
ObjectivesTo assess the evidence for debridement diabetic foot ulcers.
Search strategySearches of electronic databases, hand searching journals, bibli-ographies and identification of unpublished work by contactingexperts in the diabetic foot.
Selection criteriaRandomised controlled trials (RTCs) evaluating of debridementin the treatment of diabetic foot ulcers. The outcome had to in-clude either complete healing or rate of healing. There was norestriction on articles, on language or publication status.
Data collection & analysisData extraction and assessment of study quality were undertakenby one reviewer and checked by an Editor of the Wounds Group.
Main results5 RCTs of debridement were identified; 3 RCTs assessed theeffectiveness of a hydrogel as a debridement method, 1 RCTevaluated surgical debridement and 1 RCT evaluated larvaltherapy. Pooling the 3 hydrogel RCTs suggested that hydrogelsare significantly more effective than gauze or standard care inhealing diabetic foot ulcers (absolute risk difference 0.23; 95%CI: 0.10,0.36). Surgical debridement and larval therapy showedno significant benefit in these small trials. Other debridementmethods such as enzyme preparations or polysaccharide beadshave not been evaluated in RCTs of people with diabetes.
Reviewers’ conclusionsThere is evidence to suggest that hydrogel increases the healingrate of diabetic foot ulcers. More research is needed to evaluatethe effects of a range of widely used debridement methods andof debridement per se.
This review should be cited as: Smith J. Debridement of diabeticfoot ulcers (Cochrane Review). In: the Cochrane Library, Issue 4,2002. Oxford: Update Software.
Updates from the Cochrane Wounds Group. Two new reviews are abstracted here –for more informaton on the Cochrane Wounds Group go to www.cochranewounds.org

EWMA JOURNAL 2002 VOL 2 NO 2 61
Main resultsThree trials were identified that compared rates ofinfection and healing in wounds cleansed withwater and normal saline, two compared cleansingwith no cleansing and one compared procainespirit with water. There were no standard criteriafor the assessment of wound infection across thetrials which limited the ability to pool the data.The major comparisons were water vs normalsaline, and tap water vs no cleansing. For chronicwounds, the odds of developing an infection whencleansed with tap water compared with normalsaline was 0.16,95% Confidence Interval (CI)0.01, 2.96. (No difference.) Use of tap water tocleanse acute wounds was associated with a lowerrate of infection than saline (OR 0.52, 95% CI0.28, 0.96). No statistically significant differencesin infection rates were seen when wounds werecleansed with tap water or not cleansed at all (OR1.06, 95% CI 0.06, 17.47). Similarly there was nodifference in the infection rate in wounds cleansedwith water or procaine spirit and those cleansedwith isotonic saline, distilled water and boiledwater (OR 0.55, 95% CI 0.18,1.62).
Reviewers’ conclusionsAlthough the evidence is limited one trial hassuggested that the use of tap water to cleanse acutewounds reduces the infection rate and other trialsconclude that there is no difference in the infec-tion and healing rates between wounds that werenot cleansed and those cleansed with tap water andother solutions. However the quality of the tapwater should be considered prior to its use and inthe absence of potable tap water, boiled and cooledwater as well as distilled water can be used aswound cleansing agents.
This review should be cited as: Fernandez R,Griffiths R, Ussia C. Water for wound cleansing.(Cochrane Review). In: the Cochrane Library,Issue 4, 2002. Oxford: Update Software. �
Organisations
European Co-operation
As a part of the EWMA strategy, we have, within the last year, worked hard
to create closer bonds between thenational wound healing and management organi-sations.
Through co-operating with EWMA thenational organisation receives a large numberof benefits including:
■ The members of the organisation register asEWMA members at conferences
■ The members will receive the EWMA Journal■ A quarter page or half a page in the EWMA
Journal for association data or national news■ Link at EWMA web-site■ Invitation for EWMA co-operating
organisation workshop at the annualEWMA conference
■ 1-2 free invitations to the annual EWMAConference
■ Participation in the European CurriculumGroup, developing guidelines for educationwithin the wound management area
■ Co-operative status in relation to EWMAresearch funding
■ The organisation is free at any time to co-operate with other wound managementassociations
■ EWMA expects no financial obligations fromthe co-operating organisation
On the following pages you will find apresentation of some of the organisations whichhave agreed to co-operate with EWMA. Otherswill be presented in the following issues of theEWMA Journal.
We are very happy that so many organisationswithin such a short time have agreed on the needfor closer co-operation within Europe. We are alsoconvinced that the number will keep rising, andthat we are well on our way to create a truly Euro-pean forum for the improvement of wound man-agement.
We hope that more associations will see the op-portunities and contact us, so that we can all ben-efit from the synergy that is being created aroundEWMA.
Christine Moffatt, EWMA Past President

EWMA JOURNAL 2002 VOL 2 NO 262
Co-operating Organisations
Organisations
Name Abbr. www. CountryAssociação Portuguesa de Tratamento de Feridas ATPS aptferidas.no.soupo.pt PortugalAssociazione Infermestica per lo Studio delle Lesioni Cutanee AISLeC aislec.it ItalyAssociazione Italiana Ulcere Cutanee AIUC aiuc.it ItalyCzech Society of Wound Management CSWH – CzechBelgian Federation of Wound Care BFWC – BelgiumDansk Selskab for Sårheling DSFS dsfs.org DenmarkDeutsche Gesellschaft für Wundheilung und Wundbehandlung DGfW dgfw.de GermanyFinnish Wound Care Society FWCS personal.inet.fi/yhdistys/haava FinlandGrupo Nacional para el Estudio y Asesoramiente en Ulceraspor Presión y Heridas Crónicas GNEAUPP gneaupp.org SpainLatvian Wound Healing Society LWHS LatviaLeg Ulcer Forum LUF legulcerforum.org UKLymphoedema Support Network LSN lymphoedema.org UKNorsk Interessefaggruppe for Sårheling NIFS saar.dk/norsk.html NorwaySlovenian Wound Management Association SWMA – SloveniaSociété Française et Francophone des Plaies et Cicatrisations SFFPC sffpc.org FranceSvenskt Sårläknings Sällskap SSS sarlakning.com SwedenTissue Viability Society TVS tvs.org.uk UKWound Management Association of Ireland WMAI wmaoi.org Ireland
American Academy of Wound Management AAWM aawm.org USAAmerican Burn Association ABA ameriburn.org USAAssociation for the Advancement of Wound Care AAWC aawc1.org USAAustralian Wound Management Association Inc. AWMA awma.com.au AustraliaBritish Burn Association BBA – UKCanadian Association of Wound Care CAWC cawc.net CanadaEuropean Burn Association EBA – EuropeEuropean Pressure Ulcer Advisory Panel EPUAP epuap.org EuropeEuropean Tissue Repair Society ETRS etrs.org EuropeGrupo ULCESUR ulcesur.com SpainHong Kong Council of Enterostomal Therapists H.K.C.E.T – Hong KongICNA ICNA – EuropeKorean Association of Wound Ostomy Continence Nurses KAWCON – KoreaMediterranean Burns Club – Southern EuropeNational Decubitus Foundation NDF decubitus.org USANational Pressure Ulcer Advisory Panel NPUAP npuap.org USAPediatric Tissue Society – EuropePERSE PERSE – FranceSocietà Italiana Riparazione Tissulate – ItalySouth Australian Wound Management Association SAWMA wound.sa.edu.au AustraliaWound Care Institute, Inc. woundcare.org USAWound Care Society WCS woundcaresociety.org UKWound Care International, Inc. woundcareinternational.com USAWound Care Society of Thailand – ThailandWound Healer woundhealer.com USAWound Healing Society woundhealsoc.org USAWound Healing Society (Singapore) – SingaporeWound, Ostomy and Continence Nurses Society WOCN wocn.org USAWoundcare Consultant Society WCS wcs-nederland.nl Holland/Belgium

EWMA JOURNAL 2002 VOL 2 NO 2 63
Organisations
AISLeCAssociazione
Infermestica per loStudio delle Lesioni
Cutanee
Italian NurseAssociation for the
Study of CutaneousWounds
Andrea Bellingeri, PresidentBattistino Paggi, Vice-president
Correspondence to:AISLeC
Via Flarer n 627100 Pavia
Italy
Tel.: +39 382 422 133Fax: +39 382 523 203
AISLeC 2002 ActivitySince AISLeC was founded it has worked towards itsobjectives of promoting the quality of care through exten-sive research. Using data from Italy and abroad, AISLeChas done this following the AHCPR guidelines.
In its eight years of activity, AISLeC has trained over9000 professional health workers, been involved in manyquality assurance initiatives throughout Italy, and withover 200 courses and 13 editions of University courses inwound care. In addition, AISleC has established multi-centre researches involving a total of over 140 hospitals.
The first three studies involved a total of 1,760 col-leagues and 8,240 patients from 297 wards. Fromthese studies we have been able to observe if thepatients, while confined to their beds, have had theirpositions changed at regular intervals whether assistedby professional health workers or moving by themselves.We have also checked if pressure redistribution equip-ment was used and if medications were used. In addition,we have evaluated the level of assistance given topatients in home care treatment programmes. We havelooked at mobilization and the use of assistance forpreventive treatment of PS in Home Care.
The fourth multi-centre research is actually in progressand its focus is on home care and nursing homes.In the preparatory home research over 56% of thesubjects examined had skin ulcers. In evaluating pressuresore lesions and comparing the home care setting to thehospital setting, we can see that the presence of low-grade lesions (stage 1 and stage 2) has been confirmedto be around 50%, as in the 1996 study. We alsoconfirmed an increase of 50% in stage 3 and an increaseof 100% in stage 4 lesions when comparing the twosettings.
These studies have enabled us to inform patients, clini-cians, healthcare workers and the Italian Health Ministryabout this important problem and to work towardsimproving quality assurance in home care.
To improve our clinical knowledge it is necessary to investin research programs and, for this reason, some researchgroups like ours are carrying out multi-centre researchprojects to draw attention to the work done by ourAssociation. In Italy, the Vulnus Foundation is being setup to research and operate projects in line with the workdone by us. The aim of the Vulnus Foundation is to bringabout and promote clinical research projects as well astraining programmes, in order to improve the quality ofthe care and treatment offered to thousands of citizens.There is also a synergy between the Foundation and a lotof Health Centres and Hospitals.
The integral data on the latest research in home care isalso available in English. It contains over 50 pages oftables and comments on the largest research project in tohome care in Italy. For a CD copy of the research data,fax your details to: +39 382 523 203.
AISLeC is this year co-operatingwith EWMA to arrange the
2003 EWMA meeting in Pisa
13th conferenceEuropeanWound Management AssociationPISA · ITALY · 22-24 May · 2003
TEAMWORK IN WOUND TREATMENT:THE ART OF HEALING
IL LAVORO DI GRUPPONEL TRATTAMENTO DELLE FERITE:L’ARTE DELLA CURA

EWMA JOURNAL 2002 VOL 2 NO 264
13th conferenceEuropeanWound Management AssociationPISA · ITALY · 22-24 May · 2003
TEAMWORK IN WOUND TREATMENT:THE ART OF HEALING
IL LAVORO DI GRUPPONEL TRATTAMENTO DELLE FERITE:L’ARTE DELLA CURA
In the last years the problem of cutaneousulcers (venous, arterial, diabetic, pressureulcers) has assumed an increasing importance,above all due to the progressive increase in theelderly population and therefore of the preva-lence of pathologies. Cutaneous ulcers repre-sent an important clinician problem of growingimportance.
The Italian Association for Cutaneous Ulcers,taking advantage of famous experts in thefield, wants to be a center and national refer-ence point for all those who daily engage andface the difficult challenge of cutaneous ulcers.It wants to be an organisation of major impactand focus on research, diagnostic and therapyof cutaneous ulcers. This will be done with aclinician-diagnostic approach in an interdisci-plinary environment, where respect, profession-alism and enthusiasm and the devotion to thearea will come together.
Directive Council AIUC
President Luca Maximum Chinni
Elect President Piero Bonadeo
Past President Giovanni Micali
Secretary George Guarnera
Treasurer Papi Maximum
Councilmen Anna RemaindersMaura BonventoRoberto CassinoAndrea CavicchioliAlexander FarrisMark MasinaBattistino PagesClement PowerElia CurlyMark Romanelli
Revisers of Paul Cuffarothe accounts Raffaele Trulli
Maria Teresa Viviano
President AIUCLuca Maximum Chinni
AIUCAssociazione Italiana
Ulcere Cutanee
Italian Association forCutaneous Ulcers
Luca Maximum ChinniPresident
Correspondence to:Marco RomanelliUniversity of Pisa
Dept. of DermatologyVia Roma 67I-56126 Pisa
ItalyTel: +39 0 50 992436Fax: +39 0 50 551124E-mail: [email protected]
www.aiuc.it
AIUC is this year co-operatingwith EWMA to arrange the
2003 EWMA meeting in Pisa
III° National ConferenceItalian Association Ulcere CutaneousCutaneous Ulcera:Search, Clinical and TherapyAcireale, Catania, 14-15-16 November2002
The Italian Association for Cutaneous Ul-cers, has from the beginning always faceda pathology great social importance, of-ten invalidating the patient, and at thesame time difficult approach.
The Conference of Catania is an impor-tant verification of the work in AIUC andwill touch subjects such as, research,physio pathology, diagnostic and maintherapy. As the character of the pathologymainly hits the elderly, the organisationwished to involve several Institutions withthe objective of of giving the patients bet-ter service, without excessive burdens,attendance and therapeutic garrisons ofquality. A particular thanks to GiovanniMicali, Past President and founding mem-ber of AIUC, who will be in Catania, andwill be honoured by the organisation atour III° National Scientific Conference.
Organisations
CHARCOAL CHECK. SILVER MATE.
No other dressing works like ACTISORB Silver 220, with the unique
combination of activated charcoal and silver. Activated charcoal
traps bacteria, then silver effectively kills them.1 activated charcoal
also adsorbs the resultants bacterial toxins, which are known to
impair wound healing.2 Charcoal, check. Silver, mate. The
combination to help you win in the management of infected and
colonised wounds.
1. Russelss AD et al. Progress in Medical Chemistry 1994, 31
2. Robson MC et al. Wound healing alteration by infection. Clinics in Plastic Surgery 1990, 17: 485-492
Johnson & Johnson
Advanced Wound Care
Coronation Road
Ascot SL5 9EY
United Kingdom
Tlph +44 1344 871 000
EWMA JOURNAL 2002 VOL 2 NO 266
NEWS BULLETIN FROM NIFS
NIFSNorwegian
Wound HealingAssociation
Theis Huldt-NystrømChairperson
Correspondence to:NIFS Secretariat, Kirsti Espeseth
SårpoliklinikkenBuskerud Sentralsykehus
N-3004 DrammenTel: +47 3280 3339Fax: +47 3280 3344
E-mail: [email protected]/norsk.html
NIFS Norsk Interessefag-gruppe For Sårheling NIFS’s annual Wound Healing Seminar will be
held in Stavanger (Norway) on February 6th
and 7th, 2003 – with the title:
Ischemic Wounds– A Challenge In The Health Care
This seminar is aimed at physicians, nurses,foot therapists or others working with woundcare with an interest in learning more aboutwound healing. Most lectures will be held inNorwegian.
The program is packed with fascinating andinteresting facts and will address the followingtopics:– Etiologies, diagnostic procedures and
treatment of chronic foot and leg ulcerscaused by diseases affecting the arteries aswell as the microcirculation
– The effects of physical exercise, smokingand medical treatment, including throm-bolysis as well as surgical treatment onvascular disease
– practical issues concerning compressiontherapy for combined arterial and venous
ulcers– pain treatment and treatment for necrotic
ulcers and amputation– Microcirculatory disturbances in vasculitic
disease and diabetes– practical treatment of arterial ulcers
(will be considered in a panel discussion)
In addition to the professional agenda wepromise a pleasant social program and thelatest from “the Industry”. NIFS will also beholding its general annual assembly.
For a detailed program, information orseminar registration, please log in to:nifs-saar.no or contactNIFS/Kirsti Espeseth,Saarpoliklinikken Kir. avd.,Sykehuset Buskerud,N-3004 DRAMMENFax +4732803344.
Last year was very difficult for the Wound Man-agement Association of Slovenia. During theformation process, it became clear that therewere some differences of opinion, goals andobjectives between members and the repre-sentatives of different health professions.These differences, regarding what teamworkmeans, what the association is really about,and who should lead the association, led toanother association being established by medi-cal doctors. Many WMAS members were dis-couraged and many joined the other associa-tion. In addition, many of the WMAS membersare also active in other, well-established, asso-ciations. For example, the Association of Nurs-es of Slovenia has many divisions, includingEnterostomal Therapists and Surgical Nurses –both of which had seminars and workshops onwound care in the past year. Some other divi-sions also included wound care in their semi-nars, e.g. the Division of Community Nurses.These facts weakened our association.
However, the WMAS successfully partici-pated in the meeting of different wound careassociations in May in Granada, where the
REPORT FROM WMASEWMA congress took place. It was encourag-ing to find that many countries have facedvery similar problems to ours and we receiveda lot of support to overcome our problemsand to continue our work. We appreciatedEWMA’s support and the support from othercountries’ associations very much.
Recently there has been some interest inuniting WMAS and the alternative association,formed by the medical doctors. It must be saidthat the association of medical doctors hasbeen very active in the past year and hasachieved some great results – one of the mostimportant being that we will soon see somepositive changes in our reimbursement systemfor wound care. WMAS and the medical doc-tors’ association are planning a meeting to-gether later this month. Hopefully, we will beable to achieve a compromise that will enableus to join forces and start working together asequal team members and partners with acommon goal: to improve and standardisewound care for better results and a higherquality of life for our patients.
Greetings from Slovenia!
WMAS Wound
ManagementAssociationof Slovenia
Correspondence to:SIMPS’S
Motnica 3SLO-1236 Trzin
Slovenia
Tel: +38 66 11 62 13 39Att: Helena Peric
Organisations

ALLEVYN* SYMPOSIUM
Eight hundred clinicians learned about Smith & Nephew's
latest development in exudate management, at
a symposium held in May as part of the official programme of
the European Wound Management (EWMA) conference in
Granada, Spain.
The symposium, called ‘Chronic Wound Management -
Shaping The Future', was led by a number of medical
experts and opinion leaders from throughout Europe and the
USA. They presented wound care research findings and
spoke about the importance of a good quality of lifefor patients undergoing treatment.
The focus of the presentations was ALLEVYN, and the new
shape ALLEVYN Adhesive, which was also launched
at EWMA.
The symposium acted as an additional profile-raising vehicle for the brand, whose imagery on the
Smith & Nephew stand was an unmissable feature of the
EWMA exhibition preceding the symposium.
Among the speakers at the symposium were Joan Enric
Torra I Bou, from the Consorci Sanitari de Terrassa, Spain,
who talked about the use of ALLEVYN to prevent pressure
ulcers on heels; Vicki Vasquez from the Regent Care Center
of Laredo, Texas, who spoke of the rewards of using the
new ALLEVYN Adhesive; and Professor Wolfgang
Vanscheidt of the Rheintalklinik Astroia-Privatkliniken,
Germany, whose presentation looked at the role of a
hydrocellular dressing in Wound Bed Preparation.
WOUND BED PREPARATIONSYMPOSIUM
In the course of the joint IV National Symposium on
Pressure Ulcers and the 12th. Congress of the
European Wound Management Association held in Granada
on 23 - 25 May under the motto "Chronic Lesions and Quality
of Life", Smith & Nephew organised a symposium to
discuss wound bed preparation.
The concept of wound bed preparation has aroused much
interest over the last few years amongst healthcare
professionals concerned with the healing of chronic
wounds. First presented by Vincent Falanga, (Falanga,
20001) it is a process that evaluates and removes barriers to
healing so that wound repair can take place.
This symposium focused on one of the barriers in wound bed
preparation, the importance of debridement and was
analysed from various perspectives: cellular biology, nursing,
surgery and dermatology. A panel of distinguished
international experts, provided informative and
interesting presentations. One of the highlights was the
presence of the eminent professor from the University of
Wales, Keith Harding, Chairman of the symposium.
Professor Harding addressed general points encompassing
the concept of wound bed preparation, indicating how
necessary it is both to eliminate barriers that
prevent healing and to stimulate physiological processes that
encourage it. The other speakers at the symposium were
Professor Peter Vowden, the current EWMA President, who
spoke on debridement from a surgeon's perspective;
Fernando MartÌnez Cuervo, speaking on debridement from a
nursing perspective in Spain; Senen Vilaro, Professor of
Biology, University of Barcelona, investigated the role ofcells in wound bed preparation and Professor Wolfgang
Vanscheidt, Chairman of the German Wound Healing Society,
looked at the role of enzymatic debridement in combination
with a hydrocellular dressing in Wound Bed Preparation.
SMITH & NEPHEW GNEAUP-EWMA SYMPOSIUMGRANADA MAY 2002
1Falanga V. Classifications for wound bed preparation and stimulation of chronic wounds.Wound Repair and Regeneration 2000; 8(5): 347-52.

EWMA JOURNAL 2002 VOL 2 NO 268
10 YEAR ANNIVERSARY SYMPOSIUM
A NON-PROFIT ASSOCIATION IN PROGRESSwedish Wound Healing Society (SvensktSårläkningssällskap) is Sweden’s nationalorganisation in the subject area of wound andwound management/treatment. SWSH is anon-profit association that aims to widenknowledge on the subject area, and to contrib-ute to enhanced competence, to actively sup-port research and to ensure scientific develop-ment in the area of wound healing. Further-more, one of SWHS’s objectives is to arrangefor a standardisation and consensus in thetreatment and evaluation of patients withdifferent types of wounds.
HistoryIn 1994 Swedish Wound Healing Society wasfounded by five specialists with differentresearch and occupation areas, namely:Dermatology/venerology
Docent Carita Hansson, GöteborgDocent Harry Beitner, Stockholm
Diabetology /endocrinologyProf. Kerstin Brismar, StockholmDocent Jan Apelqvist, Lund
Geriatric/gerontologyDocent Vivianne Shubert, Stockholm.
Nurse Barbro Hemgren and Prof. Finn Gottrupattended the first meeting.
SWHSSvensk
Sårläkningssällskap
Swedish WoundHealing Society
Vivianne SchubertMD PhD, Chairperson
Correspondence to:SWHS SecretariatKarin Andersson
Länssjukhuset,Department of Dermatology
301 85 Halmstad, [email protected]
www.sarlakning.com
Additional development– a part of the association’s activitiesBased on science and profound experience,SWHS has since 1995 been actively focusingon developments. Each year since 1995, theassociation has arranged a symposium, whichtook place in November/December. Interna-tional researchers have been invited asspeakers.
Themes for the symposiaarranged by the association1995 Venous leg ulcers1996 Chronic wounds– pressure ulcers1997 Diabetic foot ulcers1998 Differential diagnosis at leg and foot
ulcers1999 Alternative wound management2000 Chronic wounds – nutrition and
infection2001 Circulation and pain
DWHSDanish Wound
Healing Society
Finn GottrupPresident DWHS
Correspondence to:Niels Müller
Cypresvej 18DK-3450 Allerød, Denmark
Tel: +45 4817 7025Fax: +45 4817 7025
The Danish Wound Healing Societywas founded in 1992 and in April 2002paying member no. 1000 was passed.The Society therefore felt that a 10 yearanniversary symposium should beorganised. Participants from all ofScandinavia were invited to the beautifulsurroundings of the north Zealand coastin Denmark.
The three-day meeting was filled tocapacity by more than 300 attendingand 25 exhibitions, which confirmedthe development that DWHS hasexperienced the last decade.
The main topics in the official programme were:� Education� Venous Leg Ulcers� Diabetic Wounds� Research methods� Surgical Wounds� New Treatment Techniques� Microbiology� Pressure Ulcers
The meeting was a manifestation of the impor-tance of this area in Denmark. From the responseof the participants the meeting was a great suc-cess in relation to scientific content as well as so-cial programme.
DWHS hopes that this meeting will help the jointeffort to increase the focus on Wound Healingand Treatment in the future.
Professor Finn Gottrup,Chairman DWHS
Danish WoundHealing Society

EWMA JOURNAL 2002 VOL 2 NO 2 69
Organisations
GNEAUPPGrupo Nacionalpara el Estudio y
Asesoramienteen Ulceras por
Presión yHeridas Crónicas
Spanish PressureUlcers and
Chronic WoundsAdvisory Panel
Javier SoldevillaPresident
Correspondence to:Joan Enric Torra Bou
Consord Sanitari De TerrassaC/Citra De Torrebonica E-8227
Terrassa, Barcelona, SpainTel: +34 45 49 11 17 68Fax: +34 45 49 11 17 07
E-mail: [email protected]
In 1994, in order to highlight the importance of the problem of chronicwounds, and specially pressure ulcers, the Grupo Nacional para elEstudio y Asesoramiento en Úlceras por Presión y Heridas CrónicasGNEAUPP (Spanish Pressure Ulcers and Chronic Wounds AdvisoryPanel) was created. This is an interdisciplinary society with more than1500 health care professionals. The aim of the GNEAUPP is to focuson the promotion of evidence-based comprehensive approaches for theprevention and treatment of chronic wounds involving different typesof disciplines.
Every two years the GNEAUPP organizes a national meeting aboutpressure ulcers and chronic wounds and is involved in other Europeanorganisations like the European Pressure Ulcers Advisory Panel(EPUAP) and the European Wound Management Association (EWMA).
The GNEAUPP has published several guidelines:� The prevention of pressure ulcers� The staging of pressure ulcers� The treatment of pressure ulcers� Obtaining samples from chronic wounds� Epidemiological indicators
GNEAUPP has funded several research projects about pressure ulcersand is developing a white report about pressure ulcers in Spain.
The GNEAUPP has its own website: www.gneaupp.org, it producesa newsletter and publishes a scientific journal, Gerokomos-Helcos, inconjunction with the Sociedad Española de Enfermería Geriátrica yGerontológica (Spanish Geriatric and Gerontologic Nursing Society).
The evolution of Wound Care in Spain has produced an increaseof research activities in fields like clinical, epidemiological and basicsciences.
Previous meetings and conferences:1. Meeting 1996 Logroño 700 Delegates2. Meeting 1997 Barcelona 1200 Delegates3. Meeting 1998 Logroño 1300 DelegatesFirst Summer school 2000 La RiojaSecond Summer school 2001La Rioja
The videos and the PowerPoint presentations of the lectures andpanel debates regarding infections and Chronic Wounds which werepresented at the IV meeting on Moist Wound Care and Treatment ofChronic Wounds on the 29th of October at the Hospital de Terrassa inco-operation between the Unidad Interdisciplinar de Heridas Crónicasdel Consorci Santari de Terrassa (UIFC-CST) and the Grupo Nacionalpara el estudio y asesoriamiento en Ùlceras por presión y Heridascrónicas (GNEAUPP) are now available on the GNEUAPP homepage,www.gneaupp.org
In GNEAUPP and UIFC-CST we are convinced that the distributionof scientific activities via the internet opens a new way of sharingknowledge and can be a great help in the day to day work in thetreatment centres.
If you wish to participate in the first national prevalence study on LegUlcers in Spain, please go to our website and fill in the questionnaire.
Joan-Enric Torra I BouVice president of GNEAUPP

EWMA JOURNAL 2002 VOL 2 NO 270
CWMSCzech WoundManagement
Society
APTFAssociaçatoPortuguesa
de Tratamentode Feridas
PortugueseWound
ManagementAssociation
Correspondence to:Associaçato Portuguesa de
Tratamento de FeridasRua Alvares Cabral,137, sala 14
4050-041 Porto PortugalTelephone +351-2-22026725
Fax +351-2-22007890aptferidas.no.soupo.pt
The Portuguese WoundManagement Association(A.P.T.F.) was born due tothe need felt by the healthprofessionals in the treat-ments of wounds and hasas its main aim the trainingand diffusion of newsservices within this area.
The Finnish Wound CareSociety is a forum formulti-professionaldiscussion and debateconcerning wound care.The society also co-operates with nationalhealth authorities and,through this co-operation, contributes tothe promotion of thedevelopment of woundcare in Finland.
FWCSFinnish
Wound CareSociety
Correspondence to:PL BOX 16
02201 EspooFinland
Tel: +358 9 412 5074Fax: + 358 9 412 5074e-mail:[email protected]
http://personal.inet.fi/yhdistys/haava
NEW WOUND MANAGEMENT ASSOCIATIONIN THE CZECH REPUBLIC
Milada FrancuPresident
With its more than 10 million people the CzechRepublic had an urgent need for a new WoundManagement Society. The start-up of a neworganisation can be difficult, and many re-sources are necessary. EWMA has thereforetried to assist as much as possible in the hugework laid down by the founding members.The result was that President M.D. MiladaFrancu and vice chairman Alena Pospisilováfounded the new organisation with the officialname Czech Wound Management Society inOctober 2001.
Not only has a new wound management soci-ety been founded with 340 members, but theSociety has also managed to hold its 1st Con-ference. The well-organised conference washeld from the 8th to the 9th of November thisyear, and the number of participants showedhow well functioning the organisation alreadyis: 480 participated in total. The topics werereports on the Czech Wound Management
Society, the diabetic foot, wound infectiontreatment and wound infection prophylaxis,nutrition and wound healing and aspects ofchronic venous insufficiency. There were alsoseveral workshops and a poster section.Furthermore, Prof. Peter Franks representingEWMA, gave a lecture about the EWMAOrganisation and future co-operation.
The Society has started many projects ofwhich one is a comparative study betweenconservative treatment of pressure ulcers andsurgical treatment. Furthermore, the societyis aiming at publishing a textbook for bothnurses and physicians, as the Czech Republicis lacking a local text book on wound man-agement.
A profound article on the Czech Republic andthe Wound Management Society can befound in the spring 2003 issue of the EWMAJournal.

EWMA JOURNAL 2002 VOL 2 NO 2 71
The Wound ManagementAssociation of Ireland(WMAI) is organising allcategories of health areastaff: doctors, nurses,therapists etc. in bothSouthern and NorthernIreland.WMAI
WoundManagement
Associationof Ireland
Bernadette KerryChairperson
Correspondence to:Anne Witherow
Altnagelvin HospitalGlen Shane Road
BT47 6SBLondonderry
Northern Irelandwww.wmaoi.org
SFFPCLa Société Française
et Francophonede Plaies et
Cicatrisations
The French andFrancophone Society
of Wounds andHealing
Luc TéotPresident of the SFFPC
www.sffpc.org
Correspondence to:46, rue de la Béjonnière
AngersF-49000
FranceTel: + 33 2 4168 2060
The first Conférence Plaies et Cicatrisa-tions (CPC) Conference on Wounds andHealing was organised in Paris in 1997and La Société Française et Francoph-one de Plaies et Cicatrisations (SFFPC)The French and Francophone Society ofWounds and Healing was founded.
Today SFFPC is a well functioninginstitution with almost 3000 delegatesattending the meetings. The aim of theconferences is to encourage the trainingof non-specialist nurses, doctors andpharmacists, to help them to establish asystem of reference for their practicesand understand advances in terms ofdressings and research. Another mutualbenefit these days is the high number ofinternationally renowned colleagues whoattend the conferences.
SFFPC has a well functioning websitewww.sffpc.org and many other activitieswhich will be described in followingissues of the EWMA Journal.
LYMPHOEDEMA
Do your patients sufferfrom this swelling of thelimbs and body?
The LymphoedemaSupport Networkprovides support and up-to-date informationabout lymphoedema topatients and health careprofessionals.
For further informationplease contactThe LymphoedemaSupport Network.
LSNThe Lymphoedema
Support Network
Correspondence to:The Lymphoedema
Support NetworkSt. Luke’s Crypt
Sydney StreetLondon SW3 6NH
UK
Tel: +44 20 73514480Fax: +44 20 7349 9809
E-mail: [email protected]
www.lymphoedema.org/lsn
LUFThe Leg Ulcer
Forum
Mark CollierChairperson
Correspondence to:Leg Ulcer Forum Secretariat
c/o PO Box 337Hartford
HuntigdonPE29 1FX
United KingdomTel: +44 1480 [email protected]
The Leg Ulcer ForumA national forum toadvance clinical practicefor the management ofpatients with leg ulcersand associatedconditions through theeducation and support ofall relevant professionals.
Organisations

Conferences
EWMA news
Organisations
3 Editorial
5 The management of pain associated withdressings changes in patients with burnsJacques Latarjet
11 Evaluating Australian Clinical PracticeGuidelines for Pressure Ulcer PreventionPrentice JL, Stacey MC
17 Growth Factors and Interactive Dressingsin Wound RepairDavid Leaper, Battistino Paggi, Gregory A Comp-ton, Heather Orsted, Luc Teot, H. M. Ockenfels
25 Contemporary Research in PressureUlcer Prevention and Treatment from themeta Register of Clinical Trials (mRCT)E. Andrea Nelson
30 Welcome to Peter VowdenChristine Moffatt
32 13th Annual EWMA meeting in Pisain 2003 – Wound Care in ItalyMarco Romanelli
36 The EWMA Organisational Structure
38 Leaving/entering Council
40 New Corporate Sponsors in EWMA
40 EWMA Activity Report
42 EWMA Journal Previous Issues
43 Indexes from international journals
44 EWMA Pain Position Paper
46 EWMA Cost Effectiveness Panel
47 EWMA Corporate Sponsor Contact Data
48 EWMA Educational Development Project
49 EWMA/EPUAP Education Seminar
49 EWMA Grants
50 The 12th Conference of the EuropeanWound Management Association:Quality of Life
54 Conference Calendar
56 Report on the 6th European PressureUlcer Advisory Panel Open Meeting
57 Diabetic Foot Study Group (DFSG) meeting in Hungary (Lake Balaton)
58 First International Workshop on Multi-disciplinary Concepts in Wound Healing
59 Wound Healing Association in Latvia
60 The Cochrane Collaboration
62 Co-operating Organisations
Scientific Articles