vision t - the national association of catholic chaplains€¦ · reiki is valuable tool, not...
TRANSCRIPT

By Sr. Kathleen Hearn, SNJM
Too often, older adults age bythemselves. A typical nursing-home setting ensures that they
mostly see each other and the staff.The diversity and energy of society atlarge, which could provide much-needed stimulation and interest totheir lives, can be hard to replicate.
In Seattle, WA, however,Providence Mt. St. Vincentintentionally offers activities andopportunities for interaction andexchange between the generations.Residents have the opportunity tomix with children, young people andother adults of all ages at this uniqueand vibrant living care community forolder adults. It is home to over 400adults who need some assistance or24-hour care.
Throughout the day, residents of“the Mount” can interact with the125 preschoolers at theIntergenerational Learning Center(ILC), a day-care program located atthe facility for children ages 6 weeksto 5 years. Children come into contactwith residents informally in the halls,café, lobbies, around the fish tanksand in other shared spaces. Scheduledvisits and activities take place in the“neighborhoods,” which are the
residents’ small-group living areas.Both the children and the elders
benefit. Children learn to reach outand not be afraid of older people inwheelchairs and with walkers.Engagement with the children, inturn, lifts the spirit and brings joy tothe residents. It is wonderful to see aperson who generally exhibits a flataffect light up at the approach of awagon full of toddlers!
On the third floor is anintergenerational family roomdesigned to increase opportunities forinteractions. Residents can just wheelover to the door and watch thechildren play or go in and getinvolved. Older children’s visits to theneighborhood are times to sharemusic, art and stories with theresidents. For the children, theseexperiences give them a positiveportrayal of aging and they see theelderly as real people. And theresidents are given an opportunity tobe role models and increase theirsense of generativity. For those whodon’t have their own grandchildren inthe vicinity, the ILC children are agreat substitute.
The effort to integrate residentsinto the younger generation does not
In This Issue:
vision
Letters 2
Tom Landry 3
Karen Pugliese 4
Certification renewal fee 5
Prayers for healing 5
Interview team educators 6
2008 conference 7
Annual awards 7
Seeking, Finding 8
Research Update 10
First night on call 12
Briefs 13
Poem “Collecting Light” 13
Book review 14
In Memoriam 14
Call for authors 14
2007-08 certification 15
Positions available 16
National Association of Catholic Chaplains
June 2007Vol.17 No. 6
See Children on page 9
Children brighten attitudesat long-term care center
Mary Yellam, aresident ofProvidenceMount St.Vincent inSeattle, showsPugsley the dogto anIntergenerationalLearning Centerstudent.

Deacon appreciates his CPE experience
Editor:I recently completed a class in pastoral care at St. Joseph’s
Hospital of Atlanta with two other deacons and one information. We participated in seminars and discussions,visited patients in the hospital, wrote journals and verbatims,and also led devotions. We were expected to complete 40hours of visitation on the hospital floors.
The experience gave me an immense appreciation forhospital chaplains, and also a deeper spirituality. Jesus teachesus that we are all children of God through our baptism andour faith in Him. But just as in the parable of the GoodSamaritan, we are called to love even those people who arestrangers. Putting this into practice is the challenge and thereward of serving in pastoral care. When I talked with peoplewho were strangers, of a different faith, a differentbackground, sometimes even a different country, I learned thetrue meaning of loving your neighbor. When I tried tounderstand the suffering, pain, or the anxieties of the patients,I had to reach out beyond my fears, my doubts, and most ofall beyond my own selfishness to embrace them.
This is the call of the ministry of Christ. When we listento the sufferings and hopelessness of someone who is dying orin pain from surgery or illness, we offer ourselves to thatperson as Christ offered Himself to us. When we open ourhearts to love someone who will only be in our lives for five orten minutes, we are truly living as Christ would have us live.
I recommend this program for all deacons and those whoare aspiring to become deacons. It helped me to be a betterservant of the people in my congregation and a better servantto all people who are my neighbor. “Jesus replied: ‘Love theLord your God with all your heart and with all your soul andwith all your mind.’ This is the first and greatestcommandment. And the second is like it: ‘Love your neighboras yourself.’ ” Matthew 22:37-40.
Deacon Chester GriffinAtlanta, GA
Reiki is valuable tool, not quackery
Editor:I was certified by the NACC in 1980 and have ministered
in a variety of settings since then. I also have been a reikipractitioner for 15 years and a reiki Jin Kei Do master for thepast five years. I feel a need to respond to the letter in theFebruary issue regarding the practice of reiki in a medicalsetting.
When I worked with the HIV/AIDS community, I found
reiki was an incredible pastoral way to be with somebody intheir pain and the last stages of illness. Also, I have introducedreiki to the hospice where I now serve, as part of my pastoralrole. Many hospice nurses have shared how their clients havehad profound shifts after their sessions.
I have studied over 400 hours in my preparation for myreiki mastership and would not categorize it as quackery. Itevolved from the deep spiritual practices of a JapaneseBuddhist practitioner, Mikao Usui. I find no contradictions toany of my religious beliefs and do not hesitate to present it asa spiritual healing energy practice.
Many healthcare professionals are very interested in thismodality. More and more hospitals are offering it to theirpatients, especially before and after surgery, and have donestudies to show its effectiveness in reducing pain and causingearlier release from the hospital. For more information, visitwww.reikiinmedicine.org. It is a known fact, and myexperience as well, that cancer patients find reduction insymptoms from their chemotherapy and radiation treatmentsin conjunction with reiki treatments.
I would be very happy to speak with anyone about my ownexperience in giving reiki to people with HIV/AIDS, cancerpatients, and those at the end of life. Reiki is in my pastoraltoolbox, and I offer it whenever I feel it is appropriate. If welook at the fruits of this modality — peace, acceptance, painrelief, relaxation, etc. — it is hard to knock. Jesus sent hisdisciples out to heal others. I like to think that is what I amdoing as I teach others this wonderful healing modality.
Bill Stevens, CFC, NACC Cert.
Asbury Park, NJ
Defining chaplaincy is work in progress
Editor:Dean Marek’s summary of the work done on identifying
the unique functions of chaplaincy (April 2007 Vision)surfaced some significant issues — specifically for Catholicsengaged in active professional pastoral care. The apparent lackof consistency and consensus reflects chaplaincy as a work inprogress. The factors that will shape this work include variedand evolving institutional expectations of chaplaincy; the valuea chaplain places on a “personal call” to ministry vis-à-vis anecclesial endorsement to function in ministry; and acomplementary vision of integrated pastoral and sacramentalcare.
Regrettably, the workshop and breakout session did notgrapple with a fundamental question: What do patients andtheir loved ones ask of the Lord through His Church?Catholic chaplains are uniquely positioned to answer.Moreover we can answer while genuinely representing a“catholic” faith tradition that respects the universal good of allreligious and philosophical belief systems.
Rev. Thomas Powers, NACC Cert.Lynnfield, MA
2 Vision June 2007
Letters

June 2007 Vision 3
visionVision is published 10 times a year by theNational Association of Catholic Chaplains.Its purpose is to connect our members witheach other and with the governance of theAssociation. Vision informs and educatesour membership about issues in pastoral/spiritual care and helps chart directions forthe future of the profession, as well as theAssociation.
IISSSSNN:: 11552277--22337700
Executive EditorRev. Thomas G. Landry
EditorDavid [email protected]
Graphic DesignerGina Rupcic
The National Association of CatholicChaplains is a professional association forcertified chaplains and clinical pastoral educators who participate in the healingmission of Jesus Christ. We provide standards, certification, education, advocacy, and professional development forour members in service to the Church andsociety.
NNAACCCC NNaattiioonnaall OOffffiiccee5007 S. Howell Avenue Suite 120
Milwaukee, WI 53207-6159(414) 483-4898
Fax: (414) [email protected]
Interim Executive DirectorRev. Thomas G. [email protected]
Director of OperationsKathy [email protected]
Director of Education & Professional PracticeSusanne Chawszczewski, [email protected]
FinancesSue [email protected]
MembershipBarbara [email protected]
CertificationMarilyn [email protected]
Special ProjectsPhilip [email protected]
Executive AssistantCindy [email protected]
By Rev. Thomas LandryInterim Executive Director
We formally dedicated ournational office with acelebratory open house on
April 24. The national staff very muchenjoyed the time we spent with NACCmembers and friends, introducing youto the quarters that we have made ourhome in recent months. We trulyappreciate the effort made by so manyto be with us for this occasion, and wethank also the many members andfriends who sent us word of your warmwishes. A copy of the program that weused for “An Office Blessing” and forthe dedication of our new conferenceroom furnishings in memory of mymother, Georgianna E. Landry, can befound on the NACC website in thearea “for Members.”
This momentous occasion is a richsymbol of the work we have done tocarry out the Strategic Plan that was inplace as I began my ministry amongyou. We believe it also is a sign of thework that we are doing to move intothe future of the NACC that isaddressed creatively in the Vision andAction Initiative. I do believe it is asign of the fresh start that will arisefrom the planning process that is nowin its final stages. That plan will carryus forward in our work into 2012!
Behind the symbol, of course, is thebroader substance of our work to serveyou. We are pleased to announce to youthe dates and site of our 2008conference, found on page 7 of thisedition of Vision. We also are in thefinal stages of planning local educationdays in the fall of 2007; check the nextissue of Vision for more details.Whenever possible, we will bring youupdated information on local orregional educational offerings sponsoredby other chaplaincy organizations, or
co-sponsored by the NACC.Another milestone I am happy to
report is the revival of the NACCAnnual Awards. The GovernanceCommittee and the NACC AnnualAwards Task Force have completed thework of revision as approved by theNACC Board of Directors at itsMarch meeting in Portland, OR.
We will begin the new cycle withtwo awards: The Distinguished ServiceAward will go to an NACC member,and The Outstanding Colleague Awardwill be given to a non-NACC member.The full details of these awards andthe associated nomination andawarding processes can be found atpage 7, and will be availablethroughout the year on our website inthe “for Members” area.
A new plaque that recounts thewinners of awards given by the NACCin the years 1975-2001 is being craftedfor display in the national office. Aswe begin the newly revised awards andprocesses, another plaque will bedesigned to accommodate the namesof award recipients in years to come.We anticipate that at some time in thefuture, a third award may be added tothe current two with which we beginthis new cycle.
I conclude this month by offering asincere and public “Thank you!” to allwho have participated in making thesemilestones of achievement possible.You have helped move us forward inthe midst of a time of significanttransition! Board, committee, and taskforce members and the national staffhave continued and renewed theircommitment to the present and futureof the NACC. It is the nature of theChurch to celebrate and proclaim “thehere and now” AND “the not yet!”Thank you for the vitality of “the hereand now!” It is the promise of thestrength and beauty of “the not yet!”
Achievements continuein midst of transition

By Karen PuglieseNACC Board Chair
Each of us undoubtedly knows obviously gifted anduniquely prepared persons who have served in aparticular place for what appears to be a
disappointingly short time. A more graced and generousinterpretation, however,embraces the gifts andblessings of that moment intime and history. And, itwould seem, an enlightenedresponse would be not onlygratitude, but a commitmentto ensure thataccomplishments aresustained, and work wellbegun is successfullycompleted.
When Most Rev. RobertJ. McManus, STD, Bishop
of the Dioceseof Worcester,MA, graciously agreed to support Fr. TomLandry’s ministry as Interim ExecutiveDirector, we were all aware that Tom would bechallenged to invest wholeheartedly in therole, and at the same time, to hold hisresponsibilities lightly enough to turn themover to his successor at the completion of theVision and Action Initiative. The consensus?Tom has expertly struck this delicate balance.
A fitting tribute for the gift of Fr. TomLandry’s leadership this past year is to secure
an Executive Director for the NACC who willenergetically serve with wisdom and skill to meet theneeds of this new time in the life of our association. Iwould like to share the details of the search, to encourageyou to recommend and encourage prospective candidates(job description and application forms may be found onthe NACC website), and to invite your prayerful supportof the process.
Using our past experiences to guide us, the Board ofDirectors determined that NACC would be best served byengaging experienced consultants to facilitate the searchprocess. The Reid Group of Bellevue, WA, is not onlyhighly qualified, but has come to know us well whileassisting us in articulating our mission, vision, values, andplan for the future viability and vitality of ourorganization. In April, we contracted with John Reid andMaureen Gallagher for a five-phase consulting process toinclude the executive search, NACC board and office staffdevelopment, and clear transition plans throughout. In
addition to a focus on team building, John and Maureenwill assess Executive Director, Board, and staff roles andresponsibilities and make recommendations to ensure thesuccess of the Strategic Plan. They will lead us in assessingthe current governance structure, and offerrecommendations for effective and creative governance
models to support ourmission, goals, staff andmembership.
Phase One, the searchfor NACC executiveleadership, is well underway. The plan includes arealistic and high-qualityrecruitment, selection,hiring, and orientationprocess, with clearexpectations and timelines.The Core SearchCommittee includesBridget Deegan-Krause,Paul Marceau, Sr.Geraldine Hoyler, Alan
Bowman, and myself. However, the process will be highlyparticipative as it progresses, and will engage personswithin and beyond our membership. An evaluation of theneed for strong, visionary, and credible executiveleadership clarified the desired qualities and qualifications.Next we developed a job description, with clear roleresponsibilities, accountabilities, and expectations forworking with NACC staff, Board of Directors, bishops,the Spiritual Care Collaborative, CHA, health systemleaders, etc.
We continue to work at identifying the widest yet mostappropriate pool of qualified and credible applicants. Atthe annual conference in Portland, participants wereinvited to indicate their personal interest in the position orsuggest/recommend other individuals for consideration.John and Maureen have already involved NACC staff, aswell as Jo Schrader, Executive Director of APC, andTeresa Snorton, Executive Director of ACPE, amongothers, in dialogue about the position. Our consultantsdeveloped the advertising strategy, application forms,screening and interview process. They will conduct theinitial screenings and facilitate and debrief interviews inMilwaukee with the top three or four candidates. Inaddition to the Core Search Committee, an additional twoor three NACC members and the NACC staff willinterview the candidates and provide input to the CoreSearch Committee.
The Committee is responsible for recommendingcandidates to the board. The Reid Group will assist in thediscernment and decision-making processes, offering the
4 Vision June 2007
We continue to
work at
identifying
qualified and
credible
applicants
Search for new executive director under way
EXECUTIVE DIRECTORNATIONAL ASSOCIATION
OF CATHOLIC CHAPLAINS
Executive Director sought to provide senior executiveleadership and management of NACC’s activities.Location: Milwaukee, Wisconsin. Preferred start date:September 2007. Requirements: Catholic in goodstanding; graduate degree in theology; knowledge ofchaplaincy education; successful experience in upper-level administration. Competitive salary. For moreinformation call John Reid, Executive Search, The ReidGroup, 800-916-3472.

June 2007 Vision 5
position, and securing a firm commitment from the chosencandidate. John and Maureen will assure prompt andprofessional follow-up and prepare appropriate press releasesand articles. Finally, they will develop a comprehensiveprocess to welcome and orient the new Executive Director tothe position and the association. And in ritually welcomingour new leader, we will also honor and celebrate the gift Fr.Tom Landry has been and will continue to be to NACC. “Itis all one,” Paul reminds us, “who does the planting and whodoes the watering. … It is only God who makes thingsgrow.”
Personally, I acknowledge that this process, thoughexcellent, is bittersweet. I am often grateful for quietmoments of reflection in our hospital chapel. Two of ourbeautiful stained glass windows were designed to
represent “Transition,” both as an artistic transition ofdesign from one thematic area to another, as well as thestate of transition itself. As chaplains, those to whom weminister are often experiencing transition. Whether ashocking wake-up call requiring life changes, harsh newrealities imposed at the worst possible moment, or agentle, joyful passage from one phase of life to another,these winds of change are often unpredictable,uncontrollable, and stressful because of the unknownsthey leave in their wake. Our chapel windows have muchmovement, but no clear or even abstract image. Theyserve as a reminder to move forward in trust, knowingthat the spirit of God hovers over these passages, leadingus to goodness and wholeness. Knowing that, we will findour way.
Prayers for Healing
If you know of an association member who is ill and needsprayer, please request permission of the person to submit theirname, illness, and city and state, and send the information to theVision editor at the national office. You may also send in a prayerrequest for yourself. Names may be reposted if there is acontinuing need.
Judy NovakCudahy, WI
Metastatic colon cancer
Certification examiners Chaplain Beryl McHale, Sr. Marilyn Herr, OSF,and Rev. Michael Burns, SDS, take a break during certificationweekend at NACC headquarters in Milwaukee. Thirteen candidateshad their interviews at the association’s new office.
Fee assessed to extendcertification renewals
Effective immediately, chaplains whorequest an extension on their renewal ofcertification process will have to pay a fee.
The NACC’s Board of Directorsapproved the fee in May and set it at 20%of the renewal of certification fee. Thechange was made in order to support thelevel of work generated by requests forextensions at the national office. As thecurrent renewal of certification fee is $125,the extension processing fee that mustaccompany requests for a one-yearextension for renewal of certification thisyear is $25.

6 Vision June 2007
By Rod Accardi and Jane Mather
Who can ever forget their certification interview?Upon arrival at the interview site, you receivedPresenter’s Report Part I, with items for discussion
checked and clear, focused questions to ponder. As you enteredthe room, you were introduced to the certification interviewteam, consisting of Chair, Presenter, and Reader. After the briefyet intense 50 minutes, you were dismissed and began thewaiting and waiting and waiting some more for theinterviewers to complete their deliberations.After being called back into the room, you wereread Presenter’s Report Part II with the voteand recommendations for continued growth.
But a key person you didn’t meet that day,someone behind the scenes yet instrumental inthe certification process, was the InterviewTeam Educator.
There are currently nine ITEs around thecountry, chosen for this special role because oftheir expertise as a certification interviewer andtheir demonstrated proficiency with all currentNACC standards and processes forcertification. In the last four years, ITEs have facilitated 547interviews for candidates for certification and trained the 683interviewers necessary for the task. Together they contributedmore than 1,300 volunteer hours in 2006 to ensure that theNACC process for certification is the best it can be.
The NACC created the role of Interview Team Educator toprovide oversight, consultation, facilitation, and education toassure the quality of the certification process. To achieve thisgoal, the ITEs consults regularly with the lead ITE, theNACC certification specialist (Marilyn Warczak), certificationinterviewers, site coordinators, and the CertificationCommission liaison. They meet annually in Milwaukee toorient new ITEs, discuss ongoing issues of quality assurance,and meet with the Certification Commission, which theyfunction under and are accountable to.
In the words of Cathy Connelly, lead ITE for several years,“The reason ITEs exist is to ensure that our interview teamsallow each candidate the best possible opportunity todemonstrate readiness and competence for certification.” ITEssupport both the process and the participants. But at the end ofthe day, they help interviewers formulate importantrecommendations, holding the certification process in carefulbalance between the objectivity of the standards and thenecessary subjectivity and wisdom of experience and soundjudgment.
Months before your certification team was assigned to yourinterview, ITEs forwarded names of potential team membersto the national office and assisted in composing interviewteams before conducting the training sessions. Certificationinterviewers are required to participate in an annual training
program designed and led by the ITEs. New interviewers havea more extensive training module, while returning interviewershave a refresher module.
ITEs bring their experience and dedication to thecertification process as fresh eyes to analyze the candidate’smaterials and interactions. Educators draw out learning fromtheir students. Just as chaplains listen-their-patients-into-wordsthat flow from deep within their pain and joy, ITEs helpinterviewers draw from their certification candidates the words
that authentically articulate the candidate’stheory and practice of ministry — and then toreport that encounter in words thatauthentically express the process, content, andrecommendations of the certification interview.
The ITEs review and approve bothPresenter’s Reports Part I (the week before theinterview) and Part II (on the day of theinterview) to assure that they are professionallyprepared; include appropriate references toNACC Standards throughout; articulateappropriate recommendations that facilitate thecandidate’s ongoing growth; and are consistent
with the dynamics of the interview. They also resolve issuesrelating to interview process standards on-site.
Why do ITEs devote their time and energy to this specialministry of certification? One stated that the two things thatare most significant to her are professionalism andaccountability. Another echoed this sentiment by saying thatthe role helps “ensure the professionalism, quality andconsistency of the certification [process] for all our members.”Another expressed appreciation for the challenge of knowingthat in this work he is dependent on the Lord, while anotherreports, “I treasure the relationships developed through thisprocess with NACC chaplains across the country.”
Ongoing evaluation and feedback is vital to the certificationprocess. Each candidate, certification interviewer, ITE, and sitecoordinator completes an evaluation. ITEs facilitatecertification interview team self-evaluation, peer review, anddebriefing, and they provide ongoing individual feedback tointerviewers for continuous improvement. Though the ITEsare often in the background, their role is invaluable.
Since the NACC began the ITE program in 2003, thenumber of certification appeals and complaints has droppeddramatically. Throughout the recent Vision and Action process,participants in the focus groups mention their certificationexperience as a strength and highlight of NACC. Even ourcognate organizations, especially APC and ACPE, haveidentified our certification process as an area of excellence. Asyou can see, there is a whole cast of characters involved in thecertification process, and it is the Interview Team Educatorswho provide leadership to this ministry of certification.
Interview team educators help certification succeed
Current NACC ITEs
Cathy ConnellyDarwin Dupree
Cam HanemannMichele Ledoux-Sakurai
Jane Mather (Lead) Sharon Mason
Judi ShemkovitzJane SmithJim Willsey

June 2007 Vision 7
Indianapolis in 2008
T he Board of Directors is pleased to announce thenew cycle of Annual Awards, which will be givenat our Annual Conference April 5-8, 2008 in
Indianapolis, IN (see above).Following a hiatus of six years, this new cycle will
begin with two awards. The Distinguished Service Awardwill be given to an NACC member who has“demonstrated leadership through participation in localand/or national activities, committees, or task forcesthat further the goals and mission of the NACC or theministry of chaplaincy.” The Outstanding ColleagueAward will be given to a non-NACC member,individual or group, who has “demonstrated outstandingleadership in her/his/their professional field, supportingor making a significant contribution to furthering themission of the NACC or the field of ministry.”
The nomination process for each award will run from
June 1 through Nov. 1, 2007. All nominations must bereceived in the national office by Nov. 1. Completedetails of the awards process, along with printableforms, are available on our NACC website,http://www.nacc.org/aboutnacc/awards.asp. There is aCriteria and Process sheet for each of the two awards,and a corresponding nomination form for each award. Ifyou wish to nominate more than one person for eitheraward, you must fully complete a form for eachnominee.
The NACC Annual Awards Task Force will beappointed by the Executive Director. The names ofthose on this year’s group will be published in the nextedition of Vision. If you have questions about the awardscriteria or process after reviewing them online, you maydirect your questions to Fr. Tom Landry, the InterimExecutive Director.
Association to reinstitute Annual Awards
The NACC will hold its next annualconference in Indianapolis, IN
from April 5-8, 2008.
Mark your calendars now,and watch future issues of Vision
for more details.
8 Vision June 2007
By Paula Caron
In moments when I feel at peace with theworld and my troubles seem few, I oftenthink of people I know who are not
feeling safe and secure — often patients inmy palliative care practice. I wonder why Ishould be so blessed with this momentarypeace and they should be struggling withsome type of personal challenge. It is quitethe reverse of the proverbial question,
“why me?’ that people in distress often throw out to their God,or anyone who will listen. Just as the existential “why me?”hangs without response, my question of “why me — why am Iso at peace in this moment?” also hangs unanswered.
But life has a way of throwing curve balls — one momentall is well, and in no longer than it takes to draw in a breath, apeaceful reverie can be shattered. And in those momentaryflashes of time, any one of us could become the one whose
peace is destroyed.Last year I received a call reporting that my
routine chest x-ray from the day before hadfound a “density” in my lung. I listened indisbelief to the words I had said to my oncologypatients uncountable times over the years — “Itis probably nothing. We’ll just get a CT scan toget a better look. Don’t worry.” And thus myreverie was shattered; in a flash everything in mylife looked different. In that moment I wasblessed to be in session with my belovedcolleagues in CPE for Healthcare Providers, whostopped the session to rally around and embrace
me with love and caring. I was too worried to have defenses,but I realized that neither did they. In that moment ofconnectedness they embraced my pain with me, and I was notalone in my fears.
While I waited for my CT scan, I experienced a panoply ofemotions, thoughts, fears and realizations, and it felt as if Iwere two different people. By far, most of the time I lived inthe fear of the unknown and how it could change or end mylife. Sometimes I felt like I couldn’t take a breath because thefear was so intense. But every so often I was able to summonmy observing self and watch the minutes of my life unfold. Inthose observing moments I was still aware of the cauldron ofemotions churning in my gut, but I was also able to study andwatch those emotions in the larger framework of myrelationships and interactions with people.
In my basic nursing training I was taught to be professional— which meant maintaining a distance between me and thepeople I cared for. We threw the word “empathy” around in
classroom discussions like a Frisbee and we talked about howmuch more appropriate an emotion it was towards our patientsthan sympathy, which suggested more emotional involvement.We were taught to strike a concerned approach towards apatient in need and all the right platitudes to say, but that weshould never become emotionally involved. But somewhere inthere, someone forgot to tell us that life is messy and that wewould all need human compassion at some point in our lives.The stark reality that we are all in this life together was noteven suggested. For years I carried this as the standard of whatepitomized “the good nurse.”
Now this unwelcome news was forcing me to re-examineone of the basic attributes that I felt had made me an effectiveprofessional all these years. The most profound moment ofconnection and realization came as I was walking through themall of the medical center where I work on my way to seepatients. And I was amazed that from outward appearances,everything seemed normal. Life had not stopped for mypersonal crisis. Fellow employees rushed by, some lookingstressed while clutching their coffee cups, some chatting andlaughing, but all oblivious to the fear that I felt enveloping me.
Some of the people who were there for medical care wereobvious — their wheelchairs, canes, bandages, and physicaldeformities gave them away. I realized that my white coat, withpockets full of reference cards and self-important businesscards, could not protect me from being a vulnerable humanbeing like everyone else around me. How desperately I wishedthat my status as a healthcare provider could somehow shieldme. Alas, I was no different from anyone in that mall area, andwithin a few fleeting weeks I could be in a wheelchair too,hairless and weak from chemotherapy and a patient to thepeople I consider colleagues. My son, who had alreadyexperienced the sudden death of his father two years before,might now have to face losing his other parent before he evenfinished high school. But wait — all of these other people hadchildren who depend on them, too. Why should my son bedifferent? This wasn’t fair!!! I try to live a healthy life and Ihave years of training which has prepared me to help others. Ihave many good intentions and so many plans to do goodthings that will benefit others. Shouldn’t I have some type ofimmunity?
In that moment, I realized that I was truly no differentfrom anyone in the hall. I am human, after all — nothingmore. Compassion and empathy in that moment becameredefined concepts for me. I felt like I truly could join my hallcompanions with the fear of the unknown, the powerlessnessand the feeling that my body was betraying me. I felt the panicof events hurtling out of my control and realized that what feltmost important to me was the love, compassion, andconnection of the few people around me who knew what I was
Seeking,
Finding
Fear of illness shatters professional façade
Someone forgot
to tell us that life
is messy and
that we would all
need human
compassion
June 2007 Vision 9
stop with small children, however. The Mount participateswith the Seattle Public Schools in a worksite training programfor special education high school students. These young peopleare around the building five days a week, working with thechildren, taking care of the resident cats, assisting with activitieswith the residents and transporting them to the beauty salonand from the chapel back to the Neighborhoods after the dailyMass. Here again, relationships are formed and there are mutualbenefits. Each year, a few students are inspired to pursue careersin elder care because of their work experience at the Mount.
Although many nursing homes have volunteer programs, onefunction of ours is also to bring the generations together. Atpresent, we have more than 220 active volunteers, ranging inage from 14 to 95. They accompany residents on outings, callnumbers for bingo, lead reminiscing groups, to name just a fewactivities. We have many volunteers who come in as a friend forone-on-one conversations. Rich relationships result as theyshare, often easing some of the loneliness, depression orboredom that residents can experience.
Being with people of different ages helps residents stay asphysically and mentally active as possible. I believe thatresidents are nourished spiritually in this wonderful mingling ofthe generations. God’s love and care are made real in a multi-generational environment.
Sr. Kathleen Hearn, SNJM, NACC Cert., now lives in Portland,OR.
ChildrenContinued from page 1
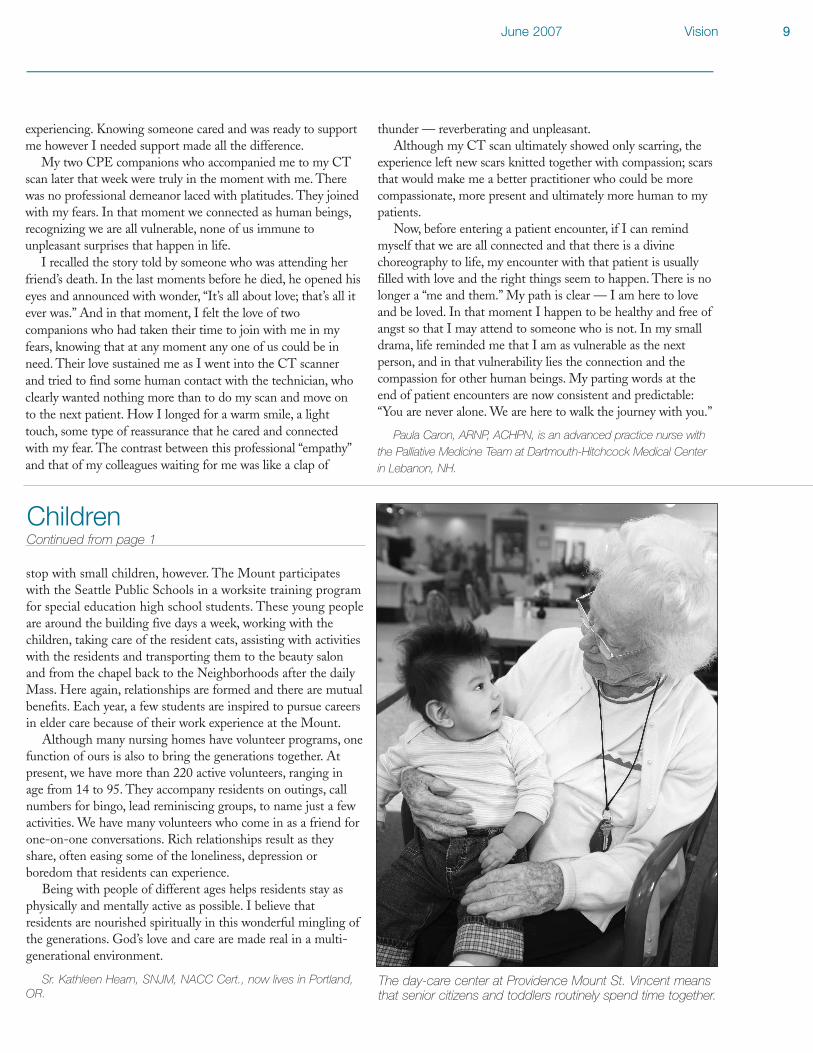
The day-care center at Providence Mount St. Vincent meansthat senior citizens and toddlers routinely spend time together.
experiencing. Knowing someone cared and was ready to supportme however I needed support made all the difference.
My two CPE companions who accompanied me to my CTscan later that week were truly in the moment with me. Therewas no professional demeanor laced with platitudes. They joinedwith my fears. In that moment we connected as human beings,recognizing we are all vulnerable, none of us immune tounpleasant surprises that happen in life.
I recalled the story told by someone who was attending herfriend’s death. In the last moments before he died, he opened hiseyes and announced with wonder, “It’s all about love; that’s all itever was.” And in that moment, I felt the love of twocompanions who had taken their time to join with me in myfears, knowing that at any moment any one of us could be inneed. Their love sustained me as I went into the CT scannerand tried to find some human contact with the technician, whoclearly wanted nothing more than to do my scan and move onto the next patient. How I longed for a warm smile, a lighttouch, some type of reassurance that he cared and connectedwith my fear. The contrast between this professional “empathy”and that of my colleagues waiting for me was like a clap of
thunder — reverberating and unpleasant.Although my CT scan ultimately showed only scarring, the
experience left new scars knitted together with compassion; scarsthat would make me a better practitioner who could be morecompassionate, more present and ultimately more human to mypatients.
Now, before entering a patient encounter, if I can remindmyself that we are all connected and that there is a divinechoreography to life, my encounter with that patient is usuallyfilled with love and the right things seem to happen. There is nolonger a “me and them.” My path is clear — I am here to loveand be loved. In that moment I happen to be healthy and free ofangst so that I may attend to someone who is not. In my smalldrama, life reminded me that I am as vulnerable as the nextperson, and in that vulnerability lies the connection and thecompassion for other human beings. My parting words at theend of patient encounters are now consistent and predictable:“You are never alone. We are here to walk the journey with you.”
Paula Caron, ARNP, ACHPN, is an advanced practice nurse withthe Palliative Medicine Team at Dartmouth-Hitchcock Medical Centerin Lebanon, NH.

By Kelly M. Trevino and Kenneth I. Pargament
Individuals often use religious coping methods to deal withdifficult or stressful events (see Pargament, 1997). Researchindicates that the prevalence of religious coping ranges from
30% to almost 80% across various samples (Harrison, Koenig,Hays, Eme-Akwari, and Pargament, 2001). Medical chaplainsare in a unique position to incorporate these coping strategiesinto medical care. This paper will review research on religiouscoping and will discuss implications of this research forhealthcare chaplains.
Researchers have identified two types ofreligious coping techniques: positive religiouscoping and spiritual struggle. Positive religiouscoping consists of methods that reflect asecure relationship with God, a belief in life’s
larger meaning, and a sense ofspiritual connectedness withothers. Positive religious coping includes strategiessuch as seeking spiritual support, benevolentreligious reappraisals (e.g., trying to find a lessonfrom God in the event), and purification rituals(Pargament, Smith, Koenig, and Perez, 1998).
Spiritual struggle occurs when stressful lifeevents shake the individual’s spiritual framework.This kind of struggle is an expression of conflict,question, and doubt regarding matters of faith,God, and religious relationships. Spiritual strugglecan be understood as an effort to conserve or
transform spiritual beliefs that have been threatened or harmed(Pargament, Murray-Swank, Magyar, and Ano, 2005).
Three types of spiritual struggle have been identified:interpersonal, intrapersonal, and divine. Interpersonal struggleincludes spiritually-related conflicts with family, friends, andcongregation members. Intrapersonal struggle consists ofquestions and doubts about spiritual issues and beliefs. Divinestruggle is characterized by expressions of tension in anindividual’s relationship with God. Positive religious coping andspiritual struggle are not mutually exclusive; use of positivereligious coping strategies does not indicate an absence ofspiritual struggle (Fitchett et al., 2004). Nevertheless, spiritualstruggle tends to be less common than positive religious coping(Meisenhelder and Marcum, 2004).
Effects of Religious CopingThe helpfulness of religious coping depends on the nature of
the coping technique. Positive religious coping is often associatedwith beneficial outcomes, while spiritual struggle is typicallyassociated with detrimental outcomes. For example, positivereligious coping has been repeatedly associated with fewerdepressive and anxious symptoms and greater emotional well-being and life satisfaction. Spiritual struggle has been associatedwith higher levels of depression, distress, and anger (Smith,McCullough, and Poll, 2003; Ano and Vasconcelles, 2005).
Religious Coping with an IllnessThis general pattern of findings also applies to individuals
coping with an illness. For example, in one sample of elderlymedical inpatients, positive religious coping was associated withless depressed mood, better quality of life, and more stress-relatedgrowth, cooperativeness, and spiritual growth (Pargament,Smith, Koenig, and Perez, 1998). In another medical sample,positive religious coping was associated with better religiousoutcomes and more stress-related growth over a two-year period(Pargament, Koenig, Tarakeshwar, and Hahn, 2004).
Conversely, spiritual struggle increases therisk of psychological distress in individualsdealing with an illness. For example, spiritualstruggle has been associated with higherlevels of depression, lower levels of lifesatisfaction, and greater emotional distress invarious medical samples, including patientsundergoing inpatient rehabilitation (Fitchett,
Rybarczyk, DeMarco, and Nicholas, 1999), patients withdiabetes, congestive heart failure, or cancer (Fitchett et al., 2004),and medically ill elderly inpatients (Koenig, Pargament, andNielson, 1998).
Individuals coping with an illness may be especially vulnerableto the detrimental effects of spiritual struggle because illnessesoften place considerable strain on the orienting system. Anorienting system consists of the beliefs, practices, relationships,and values that shape the way individuals view the world(Pargament, 1997). Spiritual beliefs, practices, relationships, andvalues are a significant part of many people’s orienting system.Although orienting systems can guide people through diverse lifeexperiences, they are vulnerable to stress. Each individual has abreaking point, a point at which he or she becomes “disoriented”and unable to successfully cope with stressful experiences. Thisbreaking point is determined by two factors: the magnitude ofthe stressor and the strength of the orienting system. Forexample, for many people, the belief in a loving God who ensuresthat bad things do not happen to good people is central to theirview of the world (Pargament, 1997). An illness may threatenthis belief and lead to questions such as “How could [this illness]happen if I am a good person and God truly watches over me?”(Pargament, 1997, p. 222).
Psychospiritual InterventionsResearch on psychospiritual interventions that incorporate
religious coping is just beginning (Pargament, Murray-Swank,Magyar, and Ano, 2005). For example, a recent comparison ofvarious types of meditation suggests that spirituality can add totreatment effectiveness. In a study comparing a secularmeditation (e.g., I am loved, people love me) to a spiritualmeditation (e.g., God is love, God loves me), participants usingthe spiritual meditation reported greater declines in anxiety andincreases in spiritual well-being than participants using thesecular meditation (Wachholtz and Pargament, 2005). Inaddition, participants using the spiritual meditation exhibited
10 Vision June 2007
The helpfulness
of religious
coping depends
on the nature of
the coping
technique
ResearchUpdate
Religious coping carries implications for chaplains

June 2007 Vision 11
greater pain tolerance than participants using the secularmeditation.
Interventions that focus primarily on divine spiritual strugglehave also been developed. For example, Cole and Pargament(1999) developed a psychospiritual intervention for cancersurvivors that targets spiritual struggle by encouragingparticipants to explore feelings of abandonment by and angertowards God. This psychospiritual intervention was comparedto a secular intervention. The psychospiritual interventionmaintained participants’ well-being over time, while the well-being of participants in the secular intervention declined overtime. However, in individuals suffering from a fainting disorder,the secular intervention was more effective at reducing anxietythan the psychospiritual intervention (Cole, Pargament, andBrownstein, 2000). These results suggest that psychospiritualinterventions may be more beneficial for individuals sufferingfrom uncontrollable illnesses.
The goal of interventions targeting spiritual struggle is notnecessarily to eliminate it. In spite of its negative correlates,spiritual struggle has been associated with posttraumatic growth(Pargament, Smith, Koenig, and Perez, 1998), suggesting thatindividuals can benefit. However, research also suggests that thelonger individuals struggle spiritually, the more likely they are tosuffer from it (Pargament, Koenig, Tarakeshwar, & Hahn,2004). Therefore, the most appropriate goal for psychospiritualinterventions may be to help people resolve their struggles beforedetrimental effects occur.
Practical Implications for ChaplainsResearch on religious coping and psychospiritual
interventions has practical implications for chaplains in medicalsettings. First, it is important to attend to positive religiouscoping and spiritual struggle in the initial assessment process.Specific questions can be incorporated into an initial assessmentto evaluate whether patients have positive religious copingstrategies or are experiencing spiritual struggle (Pargament, inpress). For example, chaplains can ask whether the illness isaffecting the individual’s religiousness and in what ways, orwhether religion has been involved in the way they have coped.
Hospital chaplain George Fitchett (1999) advocates activelyscreening people in healthcare settings to identify individuals at“spiritual risk.” This screening is especially important in light ofresearch indicating that patients with a great need of spiritualintervention are less likely to request spiritual assistance thanindividuals with less need (Fitchett et al., 2004). Fitchett (1999)recommends asking brief screening questions about anger atGod, fear of punishment by God, disappointments in faith orreligious institutions, and lifetime changes in the importance ofspiritual or religious faith. Depending on the individual’sresponse to these questions, the chaplain can explore particularreligious issues in greater detail.
After assessing the religiousness of the individual, chaplainscan encourage religious coping to promote well-being. Patientswith positive religious coping should be encouraged.Strengthening these resources can improve individuals’ currentwell-being and prepare them to cope with future hardships.Since patients in the midst of spiritual struggle are at greater riskfor poor outcomes, chaplains should actively intervene.
Various interventions are appropriate. First, spiritual struggleis a source of guilt and shame for many people, but it is a naturalpart of life. People often respond with relief and gratitude whentheir struggles are met with understanding and acceptance ratherthan threat and rebuke. By normalizing spiritual struggle andcreating opportunities for individuals to talk, chaplains canencourage people to move beyond guilt, shame, and silence.
Second, chaplains can teach individuals to anticipate spiritualstruggle and draw on personal spiritual resources before seriousproblems occur. This anticipation may be particularly relevantwhen patients’ medical status and prognosis can change overtime. Individuals who deny spiritual conflict initially may beginto question their beliefs as their physical condition declines.Chaplains can help them strengthen their spiritual resources inpreparation for the future by informing that their feelings maychange over time and encouraging them to contact the chaplainshould this occur.
Research on positive religious coping and spiritual struggleindicates that these religious processes are related to individuals’health and well-being. However, research on interventions thatincorporate positive religious coping and target spiritual struggleis just beginning. Initial studies suggest that these interventionsimprove psychological and emotional well-being. As research onpsychospiritual interventions continues, medical chaplains are ina unique and important position to address religious coping.They can encourage people to utilize positive religious copingstrategies while helping them process and understand spiritualstruggle. In this way, chaplains can work to improve individuals’psychological, emotional, and religious well-being.
Kelly Trevino recently earned her Ph.D. in psychology fromBowling Green State University in Bowling Green, OH. KennethPargament is a professor of psychology at Bowling Green StateUniversity.
ReferencesAno, G. G., & Vasconcelles, E. B. (2005). Religious coping
and psychological adjustment to stress: A meta-analysis.Journal of Clinical Psychology, 61, 461-480.
Fitchett, G. (1999). Screening for spiritual risk. ChaplaincyToday, 15, 2-12.
Fitchett, G., Murphy, P. E., Kim, J., Gibbons, J., Cameron,J. R., & Davis, J.A. (2004). Religious struggle: Prevalence,correlates and mental health risks in diabetic, congestive heartfailure, and oncology patients. International Journal of Psychiatryin Medicine, 34, 179-196.
Pargament, K. I. (in press). Spiritually integratedpsychotherapy: Understanding and addressing the sacred. NewYork: Guilford Press.
Pargament, K. I. (1997). The psychology of religion and coping:Theory, research, practice. New York: The Guilford Press.
Smith, T. B., McCullough, M. E., & Poll, J. (2003).Religiousness and depression: Evidence for a main effect andthe moderating influence of stressful life events. PsychologicalBulletin, 129, 614-636.
By Ida Louise Landeta
I am in the room where we have our CPE meetings, butthe building is swaying back and forth wildly in the midst ofa major earthquake. I am scared and shaking. Then I hearGod saying to me, “Don’t be afraid. They have had manyserious earthquakes here before, and people have survived. Youwill survive it too.” Then I felt better.
This dream followed one of the most bizarre eveningsof my life — my first night on call at the hospital as aresident chaplain. After an intense week of introductionsto new people, technologies, systems and hospitalverbiage, I was emotionally and physically exhausted. Ihad seen a few patients on the units with my supervisorin tow, but had not yet been with any patients by myself.No matter what they had taught me during those firstfew days, nothing could ever have prepared me for whatwas about to take place.
The room I was going to rent for on-call nights wouldnot be ready for another week. Thus I wasgoing to spend the night on a rollaway in thechaplain’s office at the extended care facilitywhere I would be stationed for the rest of theyear. I really hoped that no one would needanything that night. But that was not to be.
The first call came at 20:30 to see a manwho was brain-damaged and depressed. Iarrived at the main hospital without incidentand ministered successfully to the patient,returning to the extended care facility at 21:30.I had begun preparing for bed when the beeperwent off again.
A woman was in her final stages of death, and herfamily wanted me to perform a commendation. I quicklyprinted out the ritual from my computer (good thing wehad received it that day), got dressed, grabbed my purse,and left. I planned to stop at the chaplains’ office in thehospital, get the things I needed, and then go to thepatient’s room.
But upon exiting my car once there, I realized I hadleft my badge at the extended care facility. Even worse, Ihad also forgotten both the key to the office in thehospital where the supplies were kept, and the key to thechaplain’s office at the facility I had just left, where I wasgoing to stay for the night. As adrenalin and cortisolflooded every bodily tissue, my feet just wanted to turnaround and run away as fast as they could. Nevertheless,my head won out. Two city police officers were outsidethe hospital, and God bless them, they believed I was achaplain and let me in.
So I collected myself to be present with the dyingwoman and her family — a truly blessed and privileged
experience. They never noticed that I was distracted.Perhaps they were so absorbed in their grief, so gratefulto have someone with them to provide prayer, comfortand emotional support that it didn’t matter. In any case, Iwas mightily grateful.
I returned to my quarters around 23:00 and asked thenurses for a key to the chaplains’ office. But neither theynor the maintenance staff had one. Anyone who mighthave had a key worked on the day shift, because normallyno one would be in the chaplains’ office at night. At thispoint I was so exhausted that all I could think of was tosleep in my car in the garage downstairs. But the nurseswould have none of that. Instead they got a geri chair,sheets, pillow and blanket, and made a bed for me in anempty classroom. They provided a pair of pajamabottoms, and one nurse went to her car, where she had adress from her country (the Philippines). She actuallygave me the dress, both to wear for a top and to keep.
It was around midnight by this time, and I was justsettling into the geri chair. But it kept flopping aroundand would not stay put Every time I started to nod offthe chair came back to attention. I didn’t want to disturbthe nurses any more, so I lined up four classroom chairsin a row and bedded there for the night. You can imaginehow comfortable that must have been — who knows,maybe it contributed to the nightmare I described above,which woke me around 2:30 a.m. I finally went back tosleep, but later woke to hear a siren going off. I looked atthe clock. It was 6:00 a.m. In my glorious outfit ofpatient pajama bottoms and dress from the Philippines,with hair going every which way, I opened the classroomdoor only to face a huge crowd of people. Theloudspeaker was announcing “Code Red, Code Red.”Quite literally I wondered for a few seconds if I wasdreaming again. It felt like the Twilight Zone.
“What is Code Red?” I wondered. The little card withall the codes and their meanings was attached to mybadge — which was locked in the chaplains’ office. Great.One more evidence of my utter incompetence. I wasfeeling like a total failure at this chaplain thing. Then thenurse who gave me the dress ran up and said, “Don’tworry, chaplain, it’s just a fire drill. You don’t have to beconcerned. Go back to bed.” Another nurse whom Ihadn’t seen before said, “That dress looks like it’s frommy country.” I said, “It is.” She looked puzzled.
I was overjoyed to see the maintenance man from theday shift, who had just arrived for work. I asked him toopen my office. He said, “Haven’t they given you a keyyet?” I said, “Yes, and don’t ask.” He laughed.
I entered my office, never so happy to see a badge andkeys, and pulled out the rollaway bed. But by now I was
12 Vision June 2007
I lined up four
classroom
chairs in a row
and bedded
there for the
night
First night on call was bizarre from start to finish

June 2007 Vision 13
wide awake and could not go back to sleep. Needless to say Icontinued in an even more exhausted state for the rest of theday.
However, even then I recognized the humor in theevents, and I had great fun all day long repeating the storyto everyone who would listen. My fellow CPE residents
were relieved because they knew anything they encounteredwould be mild by comparison. My CPE supervisor said shehad heard a lot of stories in her day but this was absolutelythe topper.
Ida Louise Landeta, NACC Cert., is a chaplain for San DiegoHospice & Palliative Care in California.
Collecting LightBy Deborah Gordon Cooper
I see the way the chickadeestake turns at the feeder.I watch a neighbor take
her husband’s hand.
I see the way the sun will find the only interruption
in dark cloudsto toss this amber light
across the pines.
I see a row of carsstop on the road
until the orange cathas safely crossed,
then take off slowly, shouldshe change her mind.
I watch the way my brotherlifts our mother from
the wheelchairto the car,
the shawl he laysacross her lap.
I save up every scrapof light,
because I know that it will takeeach tiny consolation
every dayto mend the world.
Deborah Gordon Cooper, NACC Cert., is achaplain emerita in Duluth, MN
NACC member publishes book on sexualityNACC member Gordon Hilsman has written a book about
the spiritual aspects of sexuality. Titled Intimate Spirituality: TheCatholic Way of Love and Sex, it is published by Sheed & Wardand is available from Amazon.com.
The book “combines the two primary themes of my life,Christian culture and intimate love,” Hilsman wrote in an e-mail.“This is a very positive book, offering a spiritual view of sexualitythat augments the moral view that has dominated religious circlesforever.”
Hilsman, the manager of CPE at St. Joseph Medical Centerin Tacoma, WA, wrote, “Issues relating to sexuality will remain aprimary concern for Christians at all levels for the foreseeablefuture. This book is for all people who are serious about theirfaith and spiritual life and are seeking guidance on how tointegrate their love life with their spirituality. It is also a greatbook for those who counsel them.”
In the foreword, Eugene C. Kennedy writes, “GordonHilsman is a wise, compassionate, and unhurried companion whospeaks to our depths about what it means to be human, spiritual,and sexual at the same time. … Dr. Hilsman affirms the essentialhealth and goodness of our sexuality. He illuminates the groundthat is made sacred not by a far-off God but by up-close humanslike us as we share the intimacy at the core of religious mystery”
Palliative care symposium scheduled in Cleveland
South Pointe Hospital, Cleveland Clinic Health System, ishosting a palliative care symposium on October 22, 2007. Theevent is funded through a grant provided through the AETNAFoundation for professional chaplains and community clergy.There will not be a fee to attend, but pre-registration is required.
The keynote speaker will be Declan Walsh, director of theHarry R. Horvitz Center for Palliative Medicine at the ClevelandClinic. Four other speakers will also make presentations. Formore information, contact Charles W. Sidoti, coordinator ofpastoral care at South Pointe Hospital, at (216) 491-7924 [email protected].
Briefs

14 Vision June 2007
Medical Care at the End of Life: A Catholic PerspectiveBy David F. Kelly. Georgetown University Press, Washington,
DC, 2006, paperback, 172 pages, $16.95.
By Rev. James F. Buryska
In the wake of the furor – much of it caused by people whoshould know better – occasioned by the final months of TerriSchiavo’s life, a balanced review of Catholic moral teaching
about end-of-life care has been much needed. David Kelly’sbook succinctly and readably fills that need. In just over 170pages, he manages to address with remarkable completeness theimportant ethical aspects of medical care at the end of life, asrooted in the Roman Catholic moral tradition. In the book’sintroduction, Kelly says that the context for his approach is“Roman Catholic medical ethics, since much of what hasbecome American policy in the area was taken from Catholicsources. … But it is not intended only or even primarily forthose interested in Catholic issues. It is a book about the ethicsof end-of-life care in America.”
In his opening chapter the author makes what may arguablybe the book’s most valuable contribution to the literature – one Ihave not previously seen in this form, though it makes a greatdeal of sense. He characterizes the current and emergingAmerican ethical consensus about end-of-life care as being builton three pillars:
t the recognition that not all possible treatments arebeneficial (the distinction between ordinary andextraordinary means);
t the agreement that there is a moral difference betweenkilling and allowing to die;
t the legal concept of the right to autonomy, privacy andliberty.
He then proceeds to devote one or more chapters to each“pillar” and its implications for specific ethical questions familiarin the field of medicine – ordinary/extraordinary means, patientautonomy, advance directives, surrogate decision-making,physician-assisted suicide and euthanasia, nutrition andhydration, and the concept of medical futility.
As he examines each issue, Kelly maintains a solid groundingin the mature teaching tradition of the Catholic church;specifically, he resists the creeping vitalism so abundantlydisplayed in the way some Roman Catholic commentators haveattempted to apply Pope John Paul II’s allocution on nutritionand hydration to the Schiavo case. Along the way he does nothesitate to challenge the positions of judges, theologians,legislators, bishops and the courts, taking as his sources cases thathave become familiar to all of us: Cruzan, Brophy, Schiavo,Quinlan and others. Kelly’s arguments are lucid and his languagereadable. An additional benefit of the book for the general readeris to demonstrate how much the ethical discourse on end-of-lifeissues has been drawn from and influenced by, the RomanCatholic tradition in moral theology.
For those concerned about the ethical dimensions of caringfor persons at the end of life, this book is valuable. In addition, itis indispensable for those who are seeking insight about Catholicmoral teaching on these issues, and how that teaching hascontributed to the broader secular conversation.
Rev. James F. Buryska, NACC Cert., is an NACC and ACPEsupervisor at the Mayo Clinic in Rochester, MN.
Book Review
In Memoriam
Book fills need for discussion of end-of-life teaching
Vision regularly runs reviews of newly published books, as a service to helpour readers sort through the flood of useful (and not so useful) material thatkeeps arriving in stores and catalogs.
But we know that all of our members have trusted old favorites that theykeep returning to. Maybe it’s a book that you press into the hands of agrieving family; maybe it’s a well-thumbed spiritual volume that you take onevery retreat; maybe it’s a CD or movie that always makes you feel better.
If it helps you or your patients, we’d like to give you the opportunity to tellyour colleagues about it, whether it’s as new as Robert Wicks or as old as St.Augustine. We plan to run a compilation of our members’ favorite resourcesin a future issue of Vision, and we could possibly make it a regular feature,depending on the level of interest.
Contributions should be a maximum of 250 words and should describeone book, CD, or DVD that is currently in print and that you find helpful inyour job. Please send them to [email protected] or to David Lewellen,National Association of Catholic Chaplains, 5007 S. Howell Ave. Suite 120,Milwaukee, WI 53207.
Vision seeks reports of helpful books
Please remember in your prayers:
Sr. Mary B. Philbin, IHM, who diedMarch 23 in Monroe, MI, at age 85. Sheworked as a teacher in Michigan beforebecoming an ACPE supervisor in 1975. Sheworked at hospitals in Terrell, TX, andCorpus Christi, TX, joined the NACC in1978, and was certified as a supervisor in1985. She retired in 1991.
In a letter in 2006, she wrote, “I have onebig, beautiful memory of my connectionswith NACC. … We were a small,conscientious caring group learning togetherto be sensitive to the sick and trying tofollow Jesus in prayer, healing, and humility.”

June 2007 Vision 15
NACC Certification Interview Dates – 2007/2008
1. Full membership in the NACC is required before applyingfor certification. Inside the membership application youmay indicate that you would like to receive a certificationapplication.
2. Submit the original certification application, copies of yoursupportive materials (see Checklist for Supportive MaterialsRequired for Certification Interview), and the certificationapplication fee to the national office by the due date formaterials listed above. Materials must be postmarked nolater than July 1, 2007, or February 15, 2008.
3. Include a short cover letter indicating your first and secondpreference for an interview site.
4. Retain a copy of all materials submitted to the nationaloffice, including the application form, as additional copies(3) must be made and sent to your interview team memberswhen you are notified that a team has been assigned.Please request that any recommendation letters sent directlyto the national office be copied to you for your file.
5. Materials are reviewed to verify that you have met all theformal requirements for an interview.
6. After your materials are determined to be in compliance, aninterview date, location, and interview team will beassigned.
7. When you receive notice of your interview team, you areresponsible for sending copies of your certification materialsto each of the team members. Your materials mustduplicate those sent to the national office with your originalapplication. This includes the binder, table of contents, andtabs for each section. These copies should be mailed byFed Ex, UPS, or certified mail, at least 30 days before yourinterview date. The copies will be returned to you after theinterview. The office copy will be kept until the process isclosed, and then this copy will be destroyed.
There is a chance that you may not receive your firstpreference for an interview location. The number ofinterviews scheduled at any one site will be determined bythe number of available interview team members living in,or close to, the interview site.
The Certification Commission recommends that youseek mentoring from a certified NACC chaplain orsupervisor as you enter the certification process.
Procedure for Certification Process
Fall Locations and Dates
Saturday/Sunday October 6-7, 2007
Boston, Massachusetts
Milwaukee, Wisconsin
Portland, Oregon
St. Louis, Missouri
Due date for materialsJuly 1, 2007
Fall Locations and Dates
Saturday/Sunday October 4-5, 2008
LOCATIONS FOR 2008 ARE TO BE DETERMINED
Due date for materialsFebruary 15, 2008

t CHAPLAINNationwide – Be a chaplain in the Army National Guardand fulfill a higher calling – serving the men and women ofthe United States military with spiritual guidance andministry. You will act as staff officer for all matters onwhich religion has an impact, including commandprograms, personnel, policies, and procedures. You willcoordinate/direct a complete program of religiousministries, including workshops, pastoral counseling,religious education, and other activities for militarypersonnel and their families. Additionally, as a chaplain,you will be responsible for providing leadership foressential moral, ethical, and human self-developmentprograms. The Army National Guard is an elite group ofcitizen-soldiers who dedicate a portion of their time toserving their nation. As an officer, you will train part-timeto be ready full-time, should your state or nation call youto serve. The Army National Guard is based incommunities in every State, the District of Columbia,Guam, Puerto Rico and the U.S. Virgin Islands. When youjoin the Guard, you’ll do your monthly training close tohome so you’ll be ready to serve wherever your spiritualleadership is needed. Professional Duties: Performsduties as outlined above as staff, deputy staff, orassistant chaplain at all levels of command; supervisesother chaplains and staff in providing a broad religiousprogram designed to meet the needs of the organizationand military community. Benefits: $6,000 officer bonus;$10,000 affiliation bonus for current chaplains transferringfrom another military service; chaplain candidates canqualify for up to $4,500 per year for graduate seminarytuition. Requirements: B.S. or B.A. from an accrediteduniversity; master’s of theology or M.Div. with 72-pluscredit hours from an accredited university; individuals withno prior military service must be no older than 40(however, applicants up to age 50 will be considered on acase-by-case basis for critical faith group needs);individuals with 10-plus years of prior military service maybe up to 50 years of age; must be a U.S. citizen; must beable to pass a physical exam and meet legal and moralstandards. Visit www.1800goguard.com/clergy for moreinformation.
t DIRECTOR OF SPIRITUAL CARESeattle, WA ¬– Providence Mount St. Vincent is aresident-directed care facility for elders sponsored by theSisters of Providence and serving over 300 residents inassisted living and long-term care. We are a care modelfor creating a “home environment” for our residents, wholive in small communities or neighborhoods in our facility.Our ministry is to our staff, families and residents in dailycollaboration with hospice in supportive care of the dying.The Director of Spiritual Care provides spiritual, religiousand personal counseling or guidance to residents, familymembers and employees, in accordance with currentapplicable federal, state and local standards, guidelines
and regulations, and as may be directed by theadministrator, to assure the highest degree of quality careat all times. The function of the position activelyincorporates the mission and vision of Providence HealthSystems. Core values – respect, compassion, justice,excellence, and stewardship – are reflected within allworking relationships by demonstrating teamwork,dedication, and service excellence. The Director directsand supervises the Pastoral Care Program; coordinatesreligious observances; i.e. scheduling of services andrites, seasonal observances, memorial services andcommunity celebrations for clients, employees, familymembers, etc.; maintains and submits records/reports ofpastoral activities as required, and prepares necessaryinformation for client’s medical records; informs theresident’s pastor of admission, or condition, uponrequest, and seeks her/his assistance in providingspiritual care; reviews pastoral care programs/services toassure spiritual objectives are being met, and participatesin making recommended changes; acts as a liaisonbetween staff and client’s family/friends during periods ofcrisis, adjustment, etc.; assists in planning and schedulingreligious programs provided by community churchesand/or religious organizations; establishes and maintainrelationships with clergy from the many faiths; submits abudget and administers the Pastoral Care Departmentwithin the budgetary limitations and policy andprocedures of the facility/agency; organizes opportunitiesfor clients to participate in religious services and activitiesof their choice; organizes a program of personal spiritualcounseling to clients of all faiths; consults, as needed,with clergy of all faiths to assure a broad spectrum ofspiritual services; coordinates continuing educationprograms relative to resident’s spiritual welfare andmedical ethical issues; and promotes conferences, in-services, discussions and educational programs as theypertain to the spiritual care of the sick and dying.Minimum qualifications: Bachelor’s degree in theology orspirituality of pastoral ministry, master’s degree preferred;completion of an accredited NACC or CPE program;certification by NACC or other qualifying body; two years’experience in pastoral ministry; a minimum of fourquarters of clinical pastoral education; oriented to healthcare practices and procedures; advanced study ofcounseling of psychology. Apply online atwww.providence.org/careers (job #9007). EOE
t PRIEST CHAPLAINIndianapolis, IN – This position includes both Catholicand general ministry responsibilities. Clarian Health seeksa full-time Roman Catholic priest chaplain to serve thespiritual and sacramental needs of our Roman Catholicpatients, loved ones and staff as a member of our large,well-established Chaplaincy and Pastoral EducationDepartment. Position primarily serves two 200-bedhospitals: high-acuity children’s hospital and a universityhospital in a three-hospital system located in downtownIndianapolis. Evening on-call responsibility for these twohospitals; rotation of duties with Clarian’s other priest-chaplain. Competitive salary and benefits. Qualifications,knowledge, skills, abilities: Master’s degree in theology,
16 Vision June 2007
Positions Available

June 2007 Vision 17
pastoral ministry, divinity or religious studies to meetcertification requirements by APC or NACC within 2 yearsof hire; endorsement, ordination and eligibility for faculties;minimum of 4 units of Clinical Pastoral Education;knowledge of good educational practices, assessment ofneeds and implementation of programs of education;knowledge of the action/reflection model of ClinicalPastoral Education; effective written and verbalcommunication skills; knowledge in fields of theology andethics in health care and behavioral science; qualitypatient care, communication and crisis intervention skills;knowledge of diverse religious traditions and the ability tominister to persons with diverse religious and culturalbackgrounds. Please apply online atwww.clarian.org/clarianjobs. For further informationcontact Karen Morrow at (317) 962-3723.
t DIRECTOR OF PASTORAL CARE Baraboo, WI – Responsible for directing the pastoral careservices at St. Clare Hospital and St. Clare Meadows,Baraboo, WI, located about 45 minutes northwest ofMadison, WI. Includes budgeting, goal setting, policies,standards of care, supervising staff and pastoraleducation programs for employees and the community.Must have the willingness and ability to collaborate withothers on the health care team to bring loving care tothose with physical, mental, social and spiritual needs.Certified professional chaplain or working towards CPErequired. Two or more years of healthcare ministry,master’s in theology or divinity and prior managementexperience preferred. Apply online at www.stclare.com orcontact the Human Resources Department at (608) 356-1428 for more information.
t PASTORAL CARE MANAGER Chewelah, WA – St. Joseph’s Hospital, a critical accessfacility of 25 licensed beds and a 40-bed long-term carefacility, is seeking a full-time pastoral care manager toprovide leadership for the department and meet thespiritual/religious needs of our patients, residents andfamilies. Qualifications include current certification inNACC, a degree in theology, religious studies, pastoralcounseling or related field from an accredited college oruniversity, three to five years of experience as a chaplainin a healthcare setting and one to two years managementexperience. Please forward resume to: HumanResources, P.O. Box 197, Chewelah, WA 99109 or byemail to [email protected]. St. Joseph’s Hospital is anEqual Opportunity Employer, minority/female,veteran/handicapped.
t DIRECTOR OF PASTORAL CARE ANDMISSION INTEGRATIONHastings, MN – Regina Medical Center, a comprehensivehealthcare campus including senior living, hospital,surgery center, and clinics, is located just 20 minutessoutheast of the Twin Cities. A scenic river town with apopulation of 20,000, Hastings enjoys spectacular viewsat the junction of the Mississippi, St. Croix and VermillionRivers. As a member of the leadership team, the Directorof Pastoral Care and Mission Integration will assess and
plan pastoral services, programs and ministry to supportthe spiritual and emotional needs of residents, patients,families and staff, and will develop and promote theintegration of Regina’s mission and values throughout theorganization. This position is also responsible for day today leadership of Pastoral Care staff and operations,conducting religious services, presenting educationalprograms, and managing the departmental budget.Requirements include master’s degree in theology, divinity,religious studies, pastoral ministry, spirituality, ethics or aclosely related field. Must be a practicing Catholic andcertified as chaplain by the NACC, APC or ACPE with 3 –5 years of healthcare experience; management andmission integration experience is preferred. Must possessstrong communication, program development and groupfacilitation skills. Regina Medical Center offers acompetitive salary plus a full benefits package. If you areinterested in becoming a part of a progressive facility witha great work environment, please contact: Debra Foster,Human Resources Consultant, 1175 Nininger Road,651.480.4108; 651.480.4258 fax;[email protected]
t CHAPLAINSpokane, WA – Sacred Heart Medical Center(Providence Health and Services) has an opening for a 2evenings/2 nights benefited position (32 hours per week,64 hours per pay period). Qualifications include boardcertification with NACC or APC (or ability to be certifiedwithin 18 months of hire), master’s degree in theology orrelated field, a minimum of 4 units of CPE, ecclesiasticalendorsement. The successful candidate will be proficientin spiritual assessment, computer documentation, end oflife care, and committed to working as a member of aninterdisciplinary team. Prefer experience in an acutecare/trauma setting. Please refer to our website atwww.shmc.org if you would like more information on ourfacility or are interested in applying.
t CPE/CHAPLAIN RESIDENCY Anchorage, AK – At Providence Alaska Medical Center,the state’s largest medical center with 364 beds, you’llfind a comprehensive and advanced range of servicesand a unique setting that is truly supportive to yourpersonal and professional development as a spiritual caregiver. Our diverse Spiritual Care staff and CPE programare well integrated into the multi-disciplinary care team.As a CPE Student/Chaplain Resident, you minister to theemotional and spiritual needs of patients, families, andstaff. You learn how to assess and address emotional andspiritual needs through pastoral care interventions,sacramental and ritual care. CPE Residency 2007/08(Level 1/Level 2/Second Year Residency possible):September 4, 2007 – August 30, 2008. One previous unitof CPE required. Application fee: $25. We offer a$2,000/month stipend with full benefits. The beauty andadventure of Alaska awaits you. From hiking to skiingsnow-capped mountains, fishing in wild streams toexploring the open wilderness, Alaska offers a spectacularway of life. If you're looking for a rewarding learningexperience in a beautiful setting, consider PAMC in

Anchorage, Alaska. Apply online atwww.providence.org/careers or contact Mary Ann Kiehnat 907-565-6462, [email protected]. Providenceis an Equal Opportunity Employer.
t COORDINATOR CHAPLAINArlington Heights, IL ¬– An expanding, 346-bed facilityin the Alexian Brothers Hospital Network seeks a full-timeCoordinator Chaplain to plan, organize and implementpastoral care with an ecumenical perspective. Through aninterdisciplinary team approach, you will assess spiritualneeds and offer support to patients, their families, andstaff of all faith traditions. The position requires excellentadministrative and team-building skills, a knowledge ofdiversity in religious practices, presiding at prayer serviceswith sensitivity, coordinating sacramental and liturgicalneeds, contributing to staff education and development,and mentoring CPE and other students. Qualifiedcandidates will have pastoral care experience in a healthcare setting; master’s degree in theology or religiousstudies; three to four units of CPE; certification (oreligibility); and ecclesiastical endorsement. Please sendresume with cover letter to Stan Kedzior, ABHN Directorof Mission Integration, 3040 Salt Creek Lane, ArlingtonHeights, IL, 60005 or e-mail [email protected]
t CPE RESIDENCYMilwaukee, WI – At Aurora St. Luke’s Medical Center, weserve a varied and interesting patient mix and have a richtradition of providing spiritual care. As a large urbanreferral center, many patients come to us with criticaltertiary needs for heart care, cancer, digestive diseasesand hyperbaric treatments. As part of Aurora Health Care,Aurora St. Luke’s Medical Center is supported by asystem-wide commitment to providing the tools andresources needed to deliver leading-edge health care tothe communities we serve. Our Clinical Pastoral EducationResidency program offers a unique emphasis onintrapsychic and family systems theory integrationcongruent with ACPE outcomes and the resident’slearning goals. Four positions in Level I and II are availablefor September 2007 through August 2008. The benefits ofthis position include paid time off, a stipend of $25,168and health and dental insurance. A relevant master’sdegree is preferred. Written ecclesiastical endorsementand the completion of one CPE unit are required. Forinformation on how to apply, please contact Bill Tallevast,D.Min., ACPE Supervisor, Aurora St. Luke’s MedicalCenter, Pastoral Care Department, 2900 W. OklahomaAve., Milwaukee, WI 53215; or call (414) 649-6567.
t CPE RESIDENCYRochester, MN – Mayo Clinic CPE residency positionsbeginning August 23, 2007 through August 20, 2008, fourconsecutive quarters. Residents are offered a broad array
of clinical opportunities, which include medical andsurgical subspecialties, diverse intensive care unitministries, organ transplantation, a children’s hospital, apsychiatric hospital and a regional trauma center. Twodifferent hospital campuses and three different certifiedsupervisors make this a uniquely powerful learningenvironment. Mayo Clinic health and dental benefitsavailable to residents at a reasonable rate. The residentstipend is $26,200 for 12 months, four consecutivequarters of CPE. For program information [email protected], or write Mayo Clinic CPE, 201West Center Street, Rochester, MN 55902, phone: (507)266-7275; fax: (507) 266-7882; website: www.mayo.edu
t CHAPLAINWarwick, NY – Saint Anthony Community Hospital andthe Warwick Healthcare Campus need a certified chaplainto promote the ministry of Bon Secours CharityHealthcare System and the Pastoral Care Departmentacross our acute care hospital, our long-term care centerand our assisted living facility. This new position will reportdirectly to the Director of Pastoral Care and will beresponsible for providing pastoral care to patients,residents, families, staff, and visitors in a mannerconsistent with the universal standards for the certificationof chaplains. Please respond by forwarding your coverletter and resume to: St. Anthony Community Hospital, 15Maple Ave., Warwick, NY 10990; or [email protected], or fax to (845) 987-5312.
t STAFF CHAPLAIN Cincinnati, OH – Mercy Health Partners of SouthwestOhio is seeking a staff chaplain for our Mercy Andersonand Clermont Hospitals. Qualifications include master’sdegree in a theological, ministerial, or related field; fourunits of clinical pastoral education; certification (oreligibility) with the National Association of CatholicChaplains (NACC) or the Association of ProfessionalChaplains (APC); appropriate ecclesiastical endorsementfor ministry. Previous experience in a health care setting ispreferred. Catholic chaplain preferred, as duties includecoordination of programs, services, volunteers, etc.related to Catholic ministry. This full-time staff chaplainserves as a member of an ecumenical pastoral care teammeeting the needs of patients, families and staff. Skillsinclude capacity to foster program development skills,conflict management, group dynamics, and griefcounseling skills. Must be comfortable in crisis situationsand have ability to work under stress in difficult situations.Excellent listening and communication skills required.Ability to minister to the whole person by promotingphysical, emotional, social and spiritual well being isessential. Mercy Health Partners offers a competitivebenefits package, including: immediate benefits; 403(b)plan with organizational match; pension plan; enhancedtuition reimbursement benefits; generous paid-time-offprogram; and more. Interested candidates should contactKay O’Rourke at (513) 735-7521. For more information orto apply online please visit our website at www.e-mercy.com.
18 Vision June 2007
Positions Available

June 2007 Vision 19
t INTERFAITH CHAPLAINBarre, VT – Central Vermont Medical Center has anexcellent opportunity for an experienced professional toprovide chaplain services to the Medical Center, under thegeneral supervision of the Director of ICU and PalliativeCare. This position is responsible for providing spiritualcounseling and guidance to Central Vermont Hospitalpatients, Woodridge Nursing Home residents, and CVMCstaff. This candidate will work with local religious leadersas a referral source, initiate contacts with theirparishioners or members, and assist to promote a senseof CVMC community that is rooted in spiritual values.Specific responsibilities include visiting new admissions,providing ongoing spiritual care, and assisting families andpatients with advance care planning, end of life care,decision making, and support during periods of crisis orloss. Also responsible for conducting in-services for staff,implementing Chaplain Program policies and procedures,preparing periodic reports, and serving on designatedcommittees. Requires Master of Divinity or equivalent froman accredited seminary, and experience as an institutionalchaplain including familiarity with needs and concerns ofpatients and residents. Clinical pastoral educationaccredited by ACPE is required. Ability to workcollaboratively with employees, medical staff and localreligious leaders. Board certification as a chaplain orwillingness to obtain such is necessary. The MedicalCenter offers a competitive salary and a flexible benefitprogram that includes options in health, dental, vision,disability, and life insurance. You would be eligible for agenerous paid time off program, tuition reimbursement,wellness incentive program and defined benefit retirementplan and 403(b) TSA options. Qualified applicants areencouraged to apply online at our website,www.cvmc.hitchcock.org. For more information, pleasecontact Human Resources Department, Central VermontMedical Center, P.O. Box 547, Barre, VT 05641; (802)371-4191. EOE.
t MANAGER OF SPIRITUAL CAREKenmore, NY – The Catholic Health System, the premierhealth care service in western New York, is currentlyseeking a full-time manager of spiritual care at KenmoreMercy Hospital. The Manager of Spiritual Care isresponsible for the development and implementation of acontinuum of pastoral services aimed at meeting thegoals and objectives of the department. Otherresponsibilities would include providing timely delivery ofsupportive emotional and spiritual services to patients,their families, and the Kenmore Mercy Hospitalcommunity. The ideal candidate must possess a master’sdegree in theology, religious studies, or a related field aswell as certification by the National Association of CatholicChaplains, Association of Professional Chaplains, or acognate group. Two years management experience andpastoral experience in a healthcare setting is required.Organizational and communication skills are a must.Interested applicants are encouraged to apply via theCHS website: www.chsbuffalo.org or send resume/coverletter to J. Mungo at Kenmore Mercy Hospital, HR Dept.,2950 Elmwood Ave., Kenmore, NY 14217.
t PRIEST CHAPLAINLebanon, NH – Dartmouth-Hitchcock Medical Center, a380-bed teaching, research and referral hospital, isseeking a second Roman Catholic priest to join a team ofsix professional chaplains. Pastoral care is a well-established and valued program in this compassionateand highly regarded medical center. DHMC is recognizedas a magnet hospital and a top employer in the state ofNew Hampshire. Requirements include ordination,denominational endorsement, four units of clinical pastoraleducation, and certification by NACC. Contact Rev.Patrick McCoy, Dartmouth-Hitchcock Medical Center,Lebanon, NH 03756. Telephone 603.650.7939. [email protected]. Web: www.Hitchcock.ORG
t DIRECTOR OF SPIRITUAL CARE Beaumont, TX – If you would like to work with anorganization that sets high standards for service andperformance, then CHRISTUS Health Southeast Texas isthe place to be. It just takes one step to begin a journeythat will transform your life. We are seeking a Director ofSpiritual Care for an immediate opening. This positiondevelops departmental goals, objectives, policies andprocedures; organizes the department in accordance withadministrative guidelines in order to provide spiritualministry to patients, their families and associates. Amaster’s degree in theology or related field is required. Inaddition, must be a member of the Roman CatholicChurch (ERD #22). Must have a minimum of five (5) years’spiritual care experience in a healthcare setting. Certifiedby NACC with active membership in the NationalAssociation of Catholic Chaplains. Must possessknowledge of computers and word processing skills. Thisindividual will supervise the Spiritual Care staff atCHRISTUS Hospital St. Elizabeth in Beaumont andCHRISTUS Hospital St. Mary’s staff in Port Arthur. Toapply, please visit www.christushealth.org and go to St.Elizabeth facility. EOE.
t PASTORAL CARE DIRECTORAurora, IL – Provena Fox Knoll seeks a director toprovide leadership in the planning, implementation, andevaluation of programming to enhance the spiritual healthof our independent living, assisted living, and dementiaresidents, their families, and staff. The director reflects theorganizational mission of the ministry and the CatholicChurch itself in providing an atmosphere of Christianconcern and respect for the dignity of each person. As avital component on the health team, he/she ensures aholistic approach to care. Bachelor’s degree in theology orrelated field is required, master’s preferred. Minimum ofone unit CPE required. NACC, APC or similar certificationpreferred. Experience in health care and clinical chartingdesirable. Must have a passion for working with theelderly and willingness to work with clergy of all faiths.Part-time, 32 hours per week, with benefits. Please sendresume to Fran Corn, fax (708) 478-5143, [email protected], or apply online at our website,www.provena.org/seniors. EOE.

CHAIRKaren PuglieseChaplainCentral DuPage HospitalWinfield, IL [email protected]
VICE CHAIRBridget Deegan-KrauseFerndale, [email protected]
SECRETARYPaul MarceauVice President, Mission Services and EthicsTrinity HealthNovi, [email protected]
TREASURERSr. Geraldine Hoyler, CSCNotre Dame, [email protected]
EPISCOPAL LIAISONMost Rev. Dale J. Melczek, DDBishop of GaryMerrillville, IN
INTERIM EXECUTIVE DIRECTORRev. Thomas G. Landry IIINational Association of Catholic ChaplainsMilwaukee, [email protected]
Patrick H. BoltonDirector of Pastoral CareMercy Medical CenterDaphne, [email protected]
Alan Bowman Vice President, Mission IntegrationCatholic Health InitiativesDenver, CO [email protected]
Sr. Barbara Brumleve, SSNDCPE SupervisorAlegent Health CareOmaha, NE [email protected]
Sr. Norma Gutierrez, MCDPChaplainSt. Mary Medical CenterLong Beach, [email protected]
Sr. Mary Eileen Wilhelm, RSMPresident EmeritusMercy MedicalDaphne, [email protected]
Board of Directors Calendar
NONPROFIT ORGU.S. POSTAGE PAID
MILWAUKEE, WIPERMIT NO. 48725007 S. Howell Avenue Suite 120
Milwaukee, WI 53207-6159
ADDRESS SERVICE REQUESTED
July1 Chaplain certification materials due
at NACC office
4 Independence Day; national office closed
9-11 Standards Commission meeting inMilwaukee
11-13 Board of Directors meeting in Milwaukee
12-14 Interview Team Educator training inMilwaukee
12-15 Certification Commission meeting in Milwaukee
23 Copy deadline, September Vision