vision 20/22 epic implementation
TRANSCRIPT

Vision 20/22 Epic Implementation
Change Impact SnapshotsA quick overview of key exciting changes brought about by the new Epic EHR, and
how they will improve your day-to-day operations, roles, and responsibilities
*Please note that this is a high-level overview and not meant to replace your comprehensive end user training.

Section 1: Acute PhysicianTop Acute Physician Impacts....................................................................................................................................... 1Other Acute Physician Impacts.................................................................................................................................... 4
Section 2: Ambulatory PhysicianTop Ambulatory Physician Change Impacts................................................................................................................ 9Other Ambulatory Physician Change Impacts…………………………………………………………………………....... 12
Section 3: NursingTop Nursing Change Impacts...................................................................................................................................... 17Other Nursing Change Impacts................................................................................................................................... 20Section 4: Acute 26ASAP Emergency Center............................................................................................................................................ 27Bugsy Infection Control................................................................................................................................................ 29Care Everywhere......................................................................................................................................................... 30Case Management....................................................................................................................................................... 31Stork Labor & Development......................................................................................................................................... 32Willow Inpatient Pharmacy........................................................................................................................................... 33
Section 5: Ambulatory 35Beacon Oncology......................................................................................................................................................... 36Behavioral Health......................................................................................................................................................... 38Bones Orthopedic........................................................................................................................................................ 39EpicCare Ambulatory................................................................................................................................................... 40EpicCare Link............................................................................................................................................................... 42Healthy Planet.. ........................................................................................................................................................... 43MyChart……………………………………………………………………………………………………………………........ 44Rehab........................................................................................................................................................................... 46Urgent Care.................................................................................................................................................................. 47Wound Care................................................................................................................................................................. 48
Section 6: Ancillary 49Anesthesia................................................................................................................................................................... 50Beaker Laboratory........................................................................................................................................................ 51Endoscopy................................................................................................................................................................... 52Invasive Cardiology...................................................................................................................................................... 53Non-Invasive Cardiology.............................................................................................................................................. 55OpTime Surgery........................................................................................................................................................... 56Radiant Radiology........................................................................................................................................................ 58
Section 7: Front End 59Cadence Scheduling.................................................................................................................................................... 60Grand Central (ADT, Bed Planning) ........................................................................................................................... 61Grand Central (EVS) ................................................................................................................................................... 62Health Information Management (HIM) ....................................................................................................................... 63Prelude Registration..................................................................................................................................................... 64Welcome Patient Kiosk................................................................................................................................................ 66
2Table of Contents

Section 8: Billing 67Finance………………………………………….............................................................................................................. 68Resolute Claims / Remittance…………………………………………........................................................................... 69Resolute Hospital Billing………………………………………….................................................................................... 71Resolute Professional Billing…………………………………………............................................................................. 73Revenue Integrity & Payment Posting…………………………………………............................................................... 74
Section 9: New 3rd Party 75ePrescribing Controlled Substances (ePCS) ………………………………………….................................................... 76OnBase Document Management…………………………………………...................................................................... 77SoftBank…………………………………………............................................................................................................ 79
3Table of Contents 3Table of Contents

Top Acute Physician Change Impacts
1

Top Change Impacts#1. Termination of Dictation Services and Transcription with EpicAll Physician documentation will be completed directly into Epic, ensuring continuity of documentation. Current dictation andtranscription services will be replaced by front-end voice recognition. In Epic, Physicians have the option to use: • Epic note templates, which can pre-populate with previous documentation and be personalized (available for inpatient notes, outpatient notes,
and procedure documentation).• Front-end voice recognition via M*modal Fluency Direct that is integrated with Epic and available for use on mobile devices.• Procedure documentation forms, which are customizable ‘point and click’ templates that document procedures and file charges for the procedure.Timeliness of documentation will continue to be monitored per Joint Commission rules and regulations.
#2. ePrescribing Controlled Substances (EPCS) per Massachusetts regulationsEffective 1/1/2021 per Massachusetts regulations, all prescriptions with controlled substances must be ePrescribed.• When prescribing controlled substances, clinicians will be required to enter their Epic password and accept their push
Duo notification on their phones to complete their two-factor authentication.• An identity-proofing process is being established with the Medical Staff Office and Physicians will be identity-proofed and
enrolled in Duo advance of Epic go-live.
#3. Standard Physician Note TemplatesPhysicians will enter their own notes. For Acute settings, standard note templates will be developed for H&P, consult notes, progress notes, operative note, delivery summary, and discharge summary. The exception is for EC visits where there will be one note for the duration of the patient’s stay.
#4. Secure ChatToday, some CCHC Physicians use Tiger Text for Physician to Physician communication. In the future, Secure Chat will be enabled for any member of the Care Team that can document in the patient’s chart:• Secure Chat allows users to send secure text messages to each other in Epic, and can be used via Haiku, Canto, or from
the workstation. • Content captured in Secure Chat will be discoverable and can become part of the patient’s medical record.• For Acute settings, Secure Chat promotes interdisciplinary communication for brief, non-emergent messages, but it should not be used to
replace orders, e.g., request for a consult or communicate critical results.Physicians with EpicCare Link access only will not have access to Secure Chat.
#5. Single Patient Problem List with ICD-10 DiagnosisThere will be one patient problem list shared between acute and ambulatory care settings. PCPs are tasked with maintaining the problem list for chronic problems and diagnoses. All Physicians and APCs on a patient’s care team will be responsible forupdating the patient problem list for diagnoses that they are managing.
#6. Single Patient Medication ListThere will be one patient medication list shared between acute and ambulatory care settings.• PCPs will be responsible for maintaining the complete list, but Physicians, APCs, Pharmacy Techs, and Nurses, on a
patient’s care team will be responsible for updating the medication list.• Home medication information can be obtained via Care Everywhere for patients who receive care at other organizations that use Epic.• Patients will now be able to make updates to their current medications through history questionnaires. This can be done prior to an appointment
via MyChart. These additions won’t be added to a patient’s chart until they are verified by a Nurse or Physician.• Clinical staff will be able to obtain a prescription history via SureScripts as another external data source in addition to Care Everywhere.
Need-to-Know Top Change Impacts
Acute Physician Snapshot (Page 1 of 2)In one
glance…
You can find change impacts to your day-to-day operations as Acute Physicians (including Advanced Practice Clinicians and Physician Assistants) brought about by the new Epic EHR, and how they will improve quality of patient care and clinician satisfaction. It is important to read each change impact in detail as we prepare for go-live.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
Background of Change Impacts
As part of the implementation process, clinical advisory groups convened to oversee the governance of the Epic project and its impact on clinical operations. Decisions were reviewed and finalized during Advisory Group Meetings, including: Physician Advisory Group, Clinical Advisory Group, and Integrated Advisory Group. All groups consisted of Operational Subject Matter Experts that contributed their expertise and served as advocates for clinicians across CCHC.
Advisory groups aim to promote and standardize leading practices that contribute to a high quality of patient care and cliniciansatisfaction. Hence, these groups played a pivotal role in identifying, approving, and validating Change Impacts—also known as significant differences between current and future state practices—that will occur due to the Epic implementation. Based on a comprehensive review of all advisory group decisions, CCHC physician leaders identified the following change impacts as top impacts.
For changes occurring due to an Epic module, please refer to the Epic Module-level Change Impact Assessments found here.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 2

Need-to-Know Top Change Impacts
Acute Physician Snapshot (Page 2 of 2)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Top Change Impacts#7. Care Everywhere Queries and Reconciling / Incorporating External Epic Organizations’ Patient DataPhysicians will be able to: • Review and reconcile external patient data (i.e. discrete allergies, medications, problems, and immunization history) with what is in the patient’s
CCHC chart.• Once the data is reconciled, it becomes a permanent part of the patient’s chart and can be used to drive future clinical decisions.
For Acute settings, when patients are arrived into EC or inpatient encounters, the patients’ demographic information will be queried to Care Everywhere. If there is a strong match with other Epic organizations, the external patient information will be made available within Epic. If there is no match, a manual query can be performed.
#8. Massachusetts PAT Prescription Drug Monitoring Program (PDMP) IntegrationMassPAT PDMP will be integrated into Epic, so prescribers will be able to access a patient’s prescription record in real time directly within the EHR system. Delegates will not be able to access the PDMP integration with Epic and will limit this to only those that are designated prescribers. Hence, delegates will need to continue to access Mass PAT outside of Epic as they do today.
#9. Order Set StandardizationToday, order sets have not been standardized between Cape Cod Hospital and Falmouth Hospital. In the future, standardized order sets are being developed in collaboration with the clinical specialties. Physicians will have the option to personalize these standardized order sets.
#10. Computerized Physician Order Entry (CPOE)Today, there are disparate practices for order management.
In the future, all Physicians, including Physician Assistants and Nurse Practitioners, enter orders directly into Epic. The use of verbal/telephone orders will be governed by policy but these orders are to be acted upon immediately and require subsequent physician signature within 24 hours. If an order cannot be found at the time of order entry, there is a general order that can be used.Paper based orders and ordering processes will only be made available as part of downtime procedures.
#11. Releasing Results to Patient PortalFor Acute settings, results are released to the patient portal 24 hours after they are resulted to the Provider.
Sensitive or abnormal results have a different release schedule. The patient will be able to see the results potentially prior to the Provider’s review.
#12. Surgical Case RequestsSurgeons are able to quickly place their case requests and enter the pre-operative orders at the same time within Epic. This is further enhanced by personalizing the case request order.
Surgical coordinators can place the case request orders electronically in Epic, but will still require cosign by the ordering Physician.
For add-on and urgent cases, surgeons will electronically place the case request and verbally communicate to the Center Core and Lead Anesthesiologist. The Center Core or Nursing staff will then schedule the case.
#13. Surgical Orders PlacementOnly surgeons, Physician extenders, PA/NP are able to sign pre-op orders into Epic. Surgical coordinators can pend pre-op orders in Epic for surgeons, extenders, PA/NP to sign.
#14. Appropriate Use Criteria (AUC) per regulationsCCHC will contract with National Decision Support Company (NDSC) for their CareSelect product which provides decision support based on appropriate use criteria for Radiology Orders. CareSelect will guide Physicians to place the correct modality based on reason for exam.
#15. Expected Discharge DateToday, Physicians do not identify or document patients’ expected discharge dates. In the future, Physicians and Case Managers will enter and modify an expected discharge date based on the patient’s progress. Case Managers will continue to manage the discharge process.
When preparing a patient for discharge, having an expected discharge date in the system will enhance Care Team coordination among Nurses, Physicians and Case Management.
#16. Massive Transfusion Protocol (MTP) and Blood Administration WorkflowsPhysicians and Nurses will follow the Mass Transfusion Protocol workflow and Blood Administration workflow (for non-MTP) to place orders.
For Massive Transfusion Protocol, Physicians will need to place order set in Epic. Nursing will document in Mass Transfusion flowsheet and will not be required to scan the blood unit or have dual sign-off.
For non-MTP Blood Administration workflows, there will be a seamless integration between SoftBank and Epic. There is an order to “Prepare Blood” and “Transfused Blood”, which are included in the blood transfusion order sets.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/20203

Other Acute Physician Change Impacts
4

Need-to-Know Change Impacts Categorized by Topics
Acute Physician Snapshot (Page 1 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Role in Epic SystemAdvanced Practice Clinician (APC) Supervision RequirementsPhysicians will be able to: • Review and reconcile external patient data (i.e. discrete allergies, medications, problems, and immunization history) with what is in the patient’s
CCHC chart.• Once the data is reconciled, it becomes a permanent part of the patient’s chart and can be used to drive future clinical decisions.
For Acute settings, when patients are arrived into EC or inpatient encounters, the patients’ demographic information will be queried to Care Everywhere. If there is a strong match with other Epic organizations, the external patient information will be made available within Epic. If there is no match, a manual query can be performed.Communicating with External EntitiesVisiting Physician AccessAccess for Locum Tenens Physicians will be the same as credentialed Physicians. Visiting Physicians will not have access to Epic.Patient Admission & Visit SchedulingCode Status DisplayCode status upon patient admission will default to assume full code when a patient presents to the inpatient unit without an active code status order. Physicians will still be required to enter Code Status orders for each inpatient encounter. “Partial” is a new code status that will display for the patient’s care team to update with any special restrictions.
The following two permutations are available: • “Prior full” will display when there is a previous full code order in the patient record.• “Prior” will display when there is a previous code status order other than full code. The “Prior” status is informational and not a code status order.
EC Providers will be alerted of a previous code status history when a patient presents to the EC.Transitions Across EncountersToday, Soarian does not have the ability to continue inpatient orders from a previous encounter. In the future, Epic will support transitions across two inpatient encounters that occur within a specified timeframe by providing the restart from previous admission functionality.
When a patient discharged and has a subsequent admission, the Restart from Previous Admission workflow can be used to re-activate orders from the prior admission if it is within 30 days of discharge.
Orders from the previous encounter are then carried forward and become active in the new encounter once they are reconciled by the Admitting Provider.
Patient RecordConfidentialityEpic includes different types of confidentiality functionality for patient information:
Confidential EncountersProviders have the ability to mark patient encounters as confidential. However, a subset of patient information—including allergies, medications, and problem list—may still be viewed by all Providers.
Patient encounters that will automatically be marked as confidential include:• Behavioral Health Clinic*• IP Psych*• Partial Hospitalization*• Infectious Disease• Occupational Health** Registration can also mark an encounter as confidential for specific patients, e.g., VIPs & Legal Reasons.
Break-the-Glass FunctionalityWhen an encounter is marked as confidential, it will trigger the break-the-glass functionality within Epic, which will prompt the Physician to enter a reason why they are viewing the record. Information about this “break-the-glass” encounter is then sent to the Health Information Management (HIM) team. All patient encounters that are automatically marked as confidential will have break-the-glass functionality except Occupational Health.The patient’s treatment team and clinicians who log into these departments to complete their work will not have to break the glass to view the patient’s chart.
Sensitive Notes: Psychiatry, Plastic Surgery, and Pediatrics will have the ability to mark notes as sensitive. Patient notes that are marked assensitive can be viewed by Care Team members but are not shared through Care Everywhere.Single Patient StoryboardEach patient will have a storyboard that includes key information previously available in the header of the patient chart. This information is moved to a user-friendly sidebar, making it easier to read and allowing key information to be highlighted quickly and easily. The storyboard will display information that is relevant to clinicians based on their role and care settings.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/20205

Need-to-Know Change Impacts Categorized by Topics
Acute Physician Snapshot (Page 2 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Patient Record (continued)Single Patient Storyboard AdditionsWithin the Storyboard, For Your Information (FYI) flags and ACO/PHO risk member indicators will also be displayed.FYI flags are manually added to the patient record and indicate that there is significant, actionable information available about the patient. Physicians can hover over the FYI flag to view additional details. The following flags may be used: • Custody Issues• Medication Contract• Blood Products Refusal• Hospice Patient• Palliative Care• Transgender Patient• Heart Failure Readmission Risk• Pain Contract• History of aggression/violence• Dismissed from PCP• Dismissed from specialist• No trespass orders• Hearing impairment• Vision impairment• Care Plan
Providers and Nurses (including case management) can add and remove specific FYI flags, and these flags are not visible to patients.Patient Lists (MyLists)Today, Physicians can manually add and remove patients to their rounding list and also use coverage groups. In Epic, Physicians will have MyListsthat include patients where there is an established relationship, e.g., attending provider, consulting provider. There is also the ability to have service based lists that facilitate cross coverage between Physicians. Notes & DocumentationSingle Patient Past History DocumentationNurses and clinical support staff will now document a single Past Medical and Surgical Patient History in Epic that crosses ambulatory and acute encounters. Physicians can incorporate patient history into their notes through SmartText and SmartLinks.Advanced Care Planning (ACP)ACP is an activity within Epic that provides a centralized area for all information related to the patient end of life treatment preferences, e.g., code status, advance directive, and patient wishes. The MOLST form remains the primary method for documenting the patient’s treatment preferences.
Physicians & APCs will be able to document in the following sections of advanced care planning: • Health care agent• Capacity for decision making• Code status• Documents (i.e., any documents the family provided that are related to end of life preferences/information)
Physicians & APCs can also generate an ACP note using the ‘Notes’ tool within the activity.Orders
Order and Medication ReconciliationFor Acute Settings, Physician will be responsible for order and medication reconciliation when patients are admitted, transferred to a different level of care, change clinical service and are discharged. During these events: • The admitting Provider should perform order and medication reconciliation upon patient admission.• The receiving Provider should perform the order and medication reconciliation when a patient is transferred to a different level of care or
changes primary clinical service. • The discharging Provider should perform order and medication reconciliation when a patient is discharged. The Nurse will not be able to print
the AVS until the discharge medications have been reconciled.Order Modes & Co-SignaturePhysicians, APCs, and CRNAs place medication and procedure orders using the standard order mode which does not require a Physician co-sign.
The exception is Admission order entered by an NP or PA that require co-signature.• Orders placed by clinicians that are not Physicians, APCs or CRNAs, require a per protocol Provider co-signature unless they use the "per
protocol no cosign required" order mode.• ED Scribes can no longer place any active orders, all of their orders will pend and not be communicated until signed.• Ambulatory orders entered by clinical staff that do not have order privileges will be pended for Providers’ signature unless per protocol.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 6

Need-to-Know Change Impacts Categorized by Topics
Acute Physician Snapshot (Page 3 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Orders (continued)Specialty Consultation ProcessToday, there is one consultation order for all specialties. In Epic, there is a separate consult order per specialty and a Physician name is required to route the consult to the appropriate Physician. Entering a consult note and linking it to the consult order completes the order. The system then automatically adds the consulting Physician to the patient’s treatment team, the consulting Physician’s patient list and the services’ consult system list. The Physician will place electronic consult order and verbally communicate, as per MEC guidance (per policy), the request to the consulting Physician.Marking Patients as ExpiredProviders, Nurses, and Unit Clerks can mark patients as expired within Epic, which will immediately cancel all future orders and appointments.Access for Medical StudentsToday, medical students cannot place orders, but may document notes that are co-signed by a Physician. In Epic, medical students can document notes using a special note type for medical students and place pended orders:• All orders entered by students will be pended and until signed by a Physician.• Attending or Supervising Physicians can review notes that are completed by medical students.Peri-Operative Phases of CareIn Epic, Peri-Operative orders are entered using Phase of Care functionality that associates orders to a specific phase, e.g., pre-operative holding, PACU, and releases the orders when the patient reaches that phase of care.Use Existing Specimen FunctionWhen a new order is placed within the system, Epic will check to see if there is a viable specimen for it to leverage. If one is found, the system will default to “Use Existing Specimen” over requiring a new specimen collection. However, Physicians will always have the option to request a new draw.Electronic Durable Medical Equipment (DME) OrdersDME orders will be entered electronically in Epic and not on paper. • Clinical staff (Nurses, therapists and/or case managers) are now allowed to enter and pend DME orders for Provider signature.• If a Provider does not sign the DME orders prior to discharge, a Best Practice Advisory (BPA) will display for Providers and Nurses letting them
know there are pended orders. This will also prevent Nurses from printing out the discharge After Visit Summary until the orders are signed. The DME orders include process instructions to meet medical supply vendors and payor requirements.Leave of Absence (LOA) Functionality & Medication OrdersLOA functionality is used when a patient in one CCHC facility travels to another CCHC facility for a procedure. Today, CCHC’s LOA process is to admit the patient in a new encounter when they arrive for their procedure while keeping their encounter at the original facility open for their return.In Epic, the Physician will be required to enter an order to place a patient on LOA when a patient is expected to return to the original facility following their procedure within a specified timeframe.• The maximum time a patient can be on LOA will be 24 hours.• While the patient is on LOA, the patient’s medications are placed on hold.The Physician will then reconcile medication orders when the patient returns from LOA.PrescriptionsPharmacy Benefits in Discharge PrescriptionsPrescribing Providers will receive the alternative option alert when prescribing a medication that is not covered by the patient’s pharmacy benefits plan.DischargeDischarge Order SetIn inpatient settings, a discharge order set will be used to populate the inpatient After Visit Summary (AVS) including discharge instructions and medications.• Discharge order set can be personalized to meet common discharge needs.• As with other order sets, Physicians can save defaults and use order sets created by others.
Tests and ResultsPoint of Care Tests (POCT)POCTs are any tests that are done outside of a traditional lab setting. Today, there are disparate processes for documenting these tests across each department. In the future, POCTs will be documented in Epic and results will be manually entered using “enter/edit results.” Entering the result this way makes it available for the care team to view within results review.For the Acute settings, Physicians / APCs (including Midwives & CRNAs) are the only clinicians that can edit results for the following POCTs:• Stool Occult Blood• FERN• Nitrazine Paper • ROM• Vaginal Wet Prep In addition, with other clinicians, Physicians / APCs can enter/edit results for: Urinalysis, ACT, and Hemoglobin.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/20207

Need-to-Know Change Impacts Categorized by Topics
Acute Physician Snapshot (Page 4 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Tests and Results (continued)Internal and External (i.e. Quest) Lab ResultsInternal and external lab results will be shown together on one line to facilitate trending except for a small group of select lab results.Review Test ResultsEpic includes enhanced features to ensure that test results are reviewed by the appropriate Provider:• Ambulatory test results should be reviewed by the ordering Physician. Each clinic determines if the results are routed to the clinic pool and/or
ordering Provider.• Tests resulted during the inpatient stay should be reviewed by the Attending responsible for the patient’s care as well as by the Physician who
ordered or recommended the test (per policy).• Tests resulted after the patient has been discharged will be routed to the patient’s PCP or Authorizing Provider of the order if there is no PCP.• In Results Review, Physicians can hover over a value to view the reference range and where the lab was resulted.
Charge CaptureCharge Capture & Level of ServiceCharge Capture & Level of Service: Physicians who use CCHC billing services will use Epic instead of previous methods to enter charges, level of service, and coding information for:• Inpatient visits• Bedside procedures • Ambulatory visitsPhysicians will have an option to mark an encounter for coder assistanceWorkspacesMaximum Number of Open ChartsEpic allows up to 5 workspaces (patient charts, reports, and/or activities) to be open at once, which translates into having up to 4 patients charts open simultaneously. If orders are entered on the wrong patient, the Provider must cancel and re-order for the correct patient.Citrix Timeout and Epic Hyperspace Workstation Timeout SettingsIn the Acute settings, a Citrix inactivity warning will pop up after 2 minutes of inactivity, and the workstation will lock after 3 or 4 minutes of inactivity (depending on the computer type). All information and screens that the user had opened prior to the time out will be maintained.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 8

Top Ambulatory Physician Change Impacts
9

Top Change Impacts#1. Termination of Dictation Services and Transcription with EpicAll Physician documentation will be completed directly into Epic, ensuring continuity of documentation. Current dictation andtranscription services will be replaced by front-end voice recognition.
In Epic, Physicians have the option to use: • Epic note templates, which can pre-populate with previous documentation and be personalized (available for inpatient notes, outpatient notes,
and procedure documentation).• Front-end voice recognition via M*modal Fluency Direct that is integrated with Epic and available for use on mobile devices.• Procedure documentation forms, which are customizable ‘point and click’ templates that document procedures and file charges for the procedure.
Timeliness of documentation will continue to be monitored per Joint Commission rules and regulations.#2. ePrescribing Controlled Substances (EPCS) per Massachusetts regulationsEffective 1/1/2021 per Massachusetts regulations, all prescriptions with controlled substances must be ePrescribed.• When prescribing controlled substances, clinicians will be required to enter their Epic password and accept their push
Duo notification on their phones to complete their two-factor authentication.• An identity-proofing process is being established with the Medical Staff Office and Physicians will be identity-proofed and
enrolled in Duo advance of Epic go-live.#3. Standard Physician Note TemplatesPhysicians will enter their own notes. For Ambulatory settings, Outpatient standard note templates will be developed for progress/consult notes and simplified office visit notes.#4. Secure ChatToday, some CCHC Physicians use Tiger Text for Physician to Physician communication. In the future, Secure Chat will be enabled for any member of the Care Team that can document in the patient’s chart:• Secure Chat allows users to send secure text messages to each other in Epic, and can be used via Haiku, Canto, or from
the workstation. • Content captured in Secure Chat will be discoverable and can become part of the patient’s medical record.
Physicians with EpicCare Link access only will not have access to Secure Chat.#5. Single Patient Problem List with ICD-10 DiagnosisThere will be one patient problem list shared between acute and ambulatory care settings. PCPs are tasked with maintaining the problem list for chronic problems and diagnoses. All Physicians and APCs on a patient’s care team will be responsible forupdating the patient problem list for diagnoses that they are managing.
For Ambulatory settings, patients may update their medical problem list prior to an appointment or via Welcome kiosk when checking in for their appointment. These additions won’t be added until they are verified by a Physician or Nurse.#6. Single Patient Medication ListThere will be one patient medication list shared between acute and ambulatory care settings.• PCPs will be responsible for maintaining the complete list, but Physicians, APCs, Pharmacy Techs, and Nurses, on a
patient’s care team will be responsible for updating the medication list.• Home medication information can be obtained via Care Everywhere for patients who receive care at other organizations that use Epic.• Patients will now be able to make updates to their current medications through history questionnaires. This can be done prior to an appointment
via MyChart. These additions won’t be added to a patient’s chart until they are verified by a Nurse or Physician.• Clinical staff will be able to obtain a prescription history via SureScripts as another external data source in addition to Care Everywhere.
Need-to-Know Top Change Impacts
Ambulatory Physician Snapshot (Page 1 of 2)In one
glance…
You can find change impacts to your day-to-day operations as Ambulatory Physicians brought about by the new Epic EHR, and how they will improve quality of patient care and clinician satisfaction. It is important to read each change impact in detail as we prepare for go-live.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
Background of Change Impacts
As part of the implementation process, clinical advisory groups convened to oversee the governance of the Epic project and its impact on clinical operations. Decisions were reviewed and finalized during Advisory Group Meetings, including: Physician Advisory Group, Ambulatory Advisory Group, Clinical Advisory Group, and Integrated Advisory Group. All groups consisted of Operational Subject Matter Experts that contributed their expertise and served as advocates for clinicians across CCHC.
Advisory groups aim to promote and standardize leading practices that contribute to a high quality of patient care and cliniciansatisfaction. Hence, these groups played a pivotal role in identifying, approving, and validating Change Impacts—also known as significant differences between current and future state practices—that will occur due to the Epic implementation. Based on a comprehensive review of all advisory group decisions, CCHC physician leaders identified the following change impacts as top impacts.
For changes occurring due to an Epic module, please refer to the Epic Module-level Change Impact Assessments found here.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 10

Need-to-Know Top Change Impacts
Ambulatory Physician Snapshot (Page 2 of 2)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Top Change Impacts#7. Care Everywhere Queries and Reconciling / Incorporating External Epic Organizations’ Patient DataPhysicians will be able to: • Review and reconcile external patient data (i.e. discrete allergies, medications, problems, and immunization history) with what is in the patient’s
CCHC chart.• Once the data is reconciled, it becomes a permanent part of the patient’s chart and can be used to drive future clinical decisions.For Ambulatory settings, when patients are scheduled for ambulatory encounters, the patients’ demographic information will be queried to Care Everywhere prior to their appointment. If there is a strong match with other Epic organizations, their information will then be auto-queried and matched to the other organizations’ data based on their appointment schedules. If there is no match, a manual query can be performed.#8. Massachusetts PAT Prescription Drug Monitoring Program (PDMP) IntegrationMassPAT PDMP will be integrated into Epic, so prescribers will be able to access a patient’s prescription record in real time directly within the EHR system. Delegates will not be able to access the PDMP integration with Epic and will limit this to only those that are designated prescribers. Hence, delegates will need to continue to access Mass PAT outside of Epic as they do today. #9. Order Set StandardizationToday, order sets have not been standardized between Cape Cod Hospital and Falmouth Hospital. In the future, standardized order sets are being developed in collaboration with the clinical specialties. Physicians will have the option to personalize these standardized order sets.#10. Computerized Physician Order Entry (CPOE)Today, there are disparate practices for order management. In the future, all Physicians, including Physician Assistants and Nurse Practitioners, enter orders directly into Epic. The use of verbal/telephone orders will be governed by policy but these orders are to be acted upon immediately and require subsequent physician signature within 24 hours. If an order cannot be found at the time of order entry, there is a general order that can be used.Paper based orders and ordering processes will only be made available as part of downtime procedures. #11. Releasing Results to Patient PortalFor Ambulatory settings, lab results will be released immediately, and radiology auto-released 48 hours after resulting. Sensitive or abnormal results have a different release schedule. The patient will be able to see the results potentially prior to the Provider’s review.#12. Surgical Case RequestsSurgeons are able to quickly place their case requests and enter the pre-operative orders at the same time within Epic. This is further enhanced by personalizing the case request order.Surgical coordinators can place the case request orders electronically in Epic, but will still require cosign by the ordering Physician. For add-on and urgent cases, surgeons will electronically place the case request and verbally communicate to the Center Core and Lead Anesthesiologist. The Center Core or Nursing staff will then schedule the case.
#13. Surgical Orders PlacementOnly surgeons, Physician extenders, PA/NP are able to sign pre-op orders into Epic. Surgical coordinators can pend pre-op orders in Epic for surgeons, extenders, PA/NP to sign.#14. Appropriate Use Criteria (AUC) per regulationsCCHC will contract with National Decision Support Company (NDSC) for their CareSelect product which provides decision support based on appropriate use criteria for Radiology Orders. CareSelect will guide Physicians to place the correct modality based on reason for exam.#15. Referral Process (Internal & External)Both in-network and out-of-network referrals will be done through Epic.• Referrals are completed by placing an electronic outpatient order (e.g., Referral to Cardiology) and entering the Provider if there is a specific
Provider they want to receive the referral. • If a specific Provider is not specified, the system defaults to the internal Cape Cod service where available. • If a department is specified, the order will be routed to the department. If a department is not specified, the order will drop to a referrals
workqueue for scheduling and follow-up with the patient.#16. Physicians must associate a diagnosis with Ambulatory Care ordersEpic will give Physicians the opportunity to add a diagnostic association for all Ambulatory (medication and non-medication). This will help save Physicians time and support documentation when placing orders.In the Ancillary workflow and office visits, some procedure orders need to be scheduled before the day of procedure as a future order.Advance Beneficiary Notice (ABN)When an ABN is triggered, Physicians will have to select an appropriate diagnosis for the diagnostic test or treatment. If an appropriate diagnosis is not available, the ordering Provider will discuss that the patient may be required to pay for the test or treatment, select an ABN status, and sign the order.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/17/202011

Other Ambulatory Physician Change Impacts
12
Need-to-Know Change Impacts Categorized by Topics
Ambulatory Physician Snapshot (Page 1 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Role in Epic SystemAdvanced Practice Clinician (APC) Supervision RequirementsPhysicians will be able to: • Review and reconcile external patient data (i.e. discrete allergies, medications, problems, and immunization history) with what is in the patient’s
CCHC chart.• Once the data is reconciled, it becomes a permanent part of the patient’s chart and can be used to drive future clinical decisions.
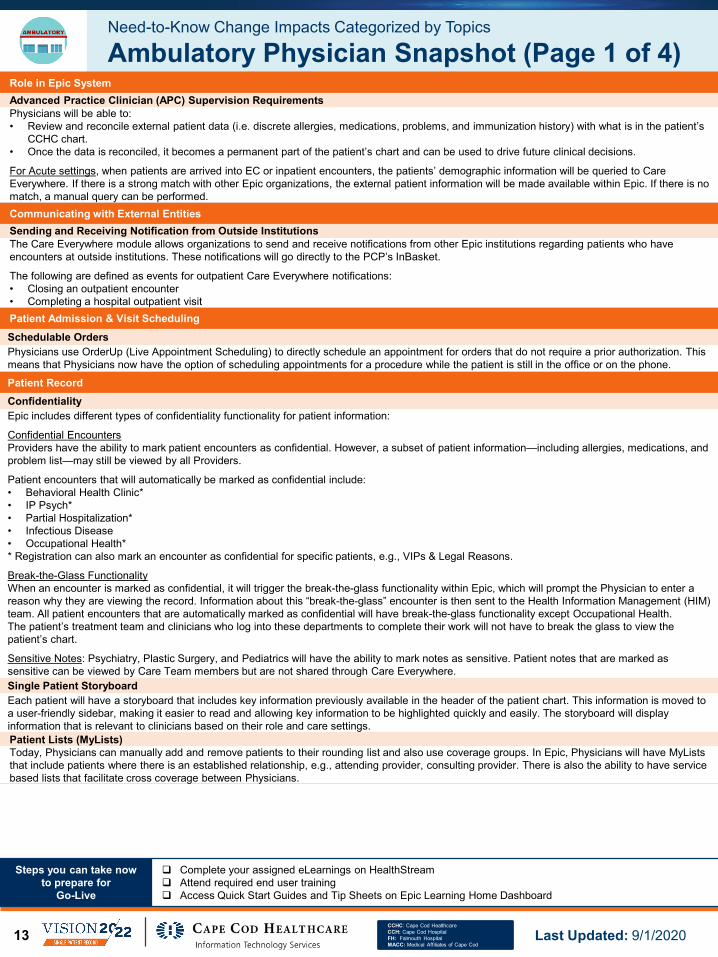
For Acute settings, when patients are arrived into EC or inpatient encounters, the patients’ demographic information will be queried to Care Everywhere. If there is a strong match with other Epic organizations, the external patient information will be made available within Epic. If there is no match, a manual query can be performed.Communicating with External EntitiesSending and Receiving Notification from Outside InstitutionsThe Care Everywhere module allows organizations to send and receive notifications from other Epic institutions regarding patients who have encounters at outside institutions. These notifications will go directly to the PCP’s InBasket.
The following are defined as events for outpatient Care Everywhere notifications:• Closing an outpatient encounter • Completing a hospital outpatient visit Patient Admission & Visit SchedulingSchedulable OrdersPhysicians use OrderUp (Live Appointment Scheduling) to directly schedule an appointment for orders that do not require a prior authorization. This means that Physicians now have the option of scheduling appointments for a procedure while the patient is still in the office or on the phone.
Patient RecordConfidentialityEpic includes different types of confidentiality functionality for patient information:
Confidential EncountersProviders have the ability to mark patient encounters as confidential. However, a subset of patient information—including allergies, medications, and problem list—may still be viewed by all Providers.
Patient encounters that will automatically be marked as confidential include:• Behavioral Health Clinic*• IP Psych*• Partial Hospitalization*• Infectious Disease• Occupational Health** Registration can also mark an encounter as confidential for specific patients, e.g., VIPs & Legal Reasons.
Break-the-Glass FunctionalityWhen an encounter is marked as confidential, it will trigger the break-the-glass functionality within Epic, which will prompt the Physician to enter a reason why they are viewing the record. Information about this “break-the-glass” encounter is then sent to the Health Information Management (HIM) team. All patient encounters that are automatically marked as confidential will have break-the-glass functionality except Occupational Health.The patient’s treatment team and clinicians who log into these departments to complete their work will not have to break the glass to view the patient’s chart.
Sensitive Notes: Psychiatry, Plastic Surgery, and Pediatrics will have the ability to mark notes as sensitive. Patient notes that are marked assensitive can be viewed by Care Team members but are not shared through Care Everywhere.Single Patient StoryboardEach patient will have a storyboard that includes key information previously available in the header of the patient chart. This information is moved to a user-friendly sidebar, making it easier to read and allowing key information to be highlighted quickly and easily. The storyboard will display information that is relevant to clinicians based on their role and care settings.Patient Lists (MyLists)Today, Physicians can manually add and remove patients to their rounding list and also use coverage groups. In Epic, Physicians will have MyListsthat include patients where there is an established relationship, e.g., attending provider, consulting provider. There is also the ability to have service based lists that facilitate cross coverage between Physicians.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202013

Need-to-Know Change Impacts Categorized by Topics
Ambulatory Physician Snapshot (Page 2 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Patient Record (continued)Patient RegistriesPhysicians may leverage registries to evaluate specified outcomes for a population defined by a particular disease, condition, or exposure and that serve predetermined scientific, clinical, or policy purpose(s). The following patient registries will be available in Epic:• Wellness: Male, Female, and three age-based Pediatric Registries (<1 year, 1-4 years, 5-12 years)• Contact Based: Inpatient Admits and Emergency Encounters• Chronic Disease: Asthma, Cancer, Chronic Heart Failure, Chemotherapy Infusion Visits, Chronic Opioid Use, Chronic Kidney Disease, COPD,
Coronary Artery Disease, Diabetes, Depression, Hypertension, and HIV• Payor Specific: Medicare Advantage (CMS-HCC) and Managed Care MembersSingle Patient Storyboard AdditionsWithin the Storyboard, For Your Information (FYI) flags and ACO/PHO risk member indicators will also be displayed.FYI flags are manually added to the patient record and indicate that there is significant, actionable information available about the patient. Physicians can hover over the FYI flag to view additional details. The following flags may be used: • Custody Issues• Medication Contract• Blood Products Refusal• Hospice Patient• Palliative Care• Transgender Patient• Heart Failure Readmission Risk• Pain Contract• History of aggression/violence• Dismissed from PCP• Dismissed from specialist• No trespass orders• Hearing impairment• Vision impairment• Care Plan
Providers and Nurses (including case management) can add and remove specific FYI flags, and these flags are not visible to patients.Pedigree FunctionalityFor patients up to 13 years old, the Pedigree functionality allows a patient’s family history to be copied into the patient’s record.Patient Record Updates via MyChartPatients will now be able to make updates to their medical, social, surgical, and family history through on-line history questionnaires after they have been verified by a Nurse or Physician. This can be done prior to an appointment via MyChart or at a Welcome kiosk. Notes & DocumentationSingle Patient Past History DocumentationNurses and clinical support staff will now document a single Past Medical and Surgical Patient History in Epic that crosses ambulatory and acute encounters. Physicians can incorporate patient history into their notes through SmartText and SmartLinks.Standardized Letter TemplatesCCHC will implement the Epic Foundation system letter templates for Ambulatory Care Physicians. Physicians can leverage letter templates for: • Various Referrals• Test Results• Reminders• Drug Recalls• School/Work ExcusesSample Medication ProcessPhysicians will order Sample Medications in Epic for documentation and tracking purposes.OrdersMedication ReconciliationFor Ambulatory Settings, Office clinical support staff will continue to record home medications, dose, and frequency with the patient during the rooming process. Ambulatory Provider will be responsible for validating and reconciling medications during office encounters. Medical Assistants will not be able to delete medications.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 14

Need-to-Know Change Impacts Categorized by Topics
Ambulatory Physician Snapshot (Page 3 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Orders (continued)Order Modes & Co-SignaturePhysicians, APCs, and CRNAs place medication and procedure orders using the standard order mode which does not require a Physician co-sign.
The exception is Admission order entered by an NP or PA that require co-signature.• Orders placed by clinicians that are not Physicians, APCs or CRNAs, require a per protocol Provider co-signature unless they use the "per
protocol no cosign required" order mode.• ED Scribes can no longer place any active orders, all of their orders will pend and not be communicated until signed.• Ambulatory orders entered by clinical staff that do not have order privileges will be pended for Providers’ signature unless per protocol.Specialty Consultation ProcessToday, there is one consultation order for all specialties. In Epic, there is a separate consult order per specialty and a Physician name is required to route the consult to the appropriate Physician. Entering a consult note and linking itto the consult order completes the order. The system then automatically adds the consulting Physician to the patient’s treatment team, the consulting Physician’s patient list and the services’ consult system list. The Physician will place electronic consult order and verbally communicate, as per MEC guidance (per policy), the request to the consulting Physician.Marking Patients as ExpiredProviders, Nurses, and Unit Clerks can mark patients as expired within Epic, which will immediately cancel all future orders and appointments.Access for Medical StudentsToday, medical students cannot place orders, but may document notes that are co-signed by a Physician. In Epic, medical students can document notes using a special note type for medical students and place pended orders:• All orders entered by students will be pended and until signed by a Physician.• Attending or Supervising Physicians can review notes that are completed by medical students.PrescriptionsPharmacy Benefits in Discharge PrescriptionsPrescribing Providers will receive the alternative option alert when prescribing a medication that is not covered by the patient’s pharmacy benefits plan.Patient CommunicationPhysician Out of ContactOut of Contact is an InBasket feature that enables Providers to:• Mark themselves as unavailable for an extended period.• Designate a covering group or user.
A Provider must manually set up each out of contact event and is expected to specify whether a user or a group will cover their InBasket messages. If a patient tries to contact their Provider via MyChart, they will receive a system-generated “out of office message” that will state: “Expect a response 2 business days from either your Provider or a member of your Provider’s team.”MyChart Patient Self-TriageMyChart patient self-triage tools help direct patients to the right level of care for their symptoms and requires limited intervention from Providers or staff. After the patient completes Self-Triage, actionable recommendations are presented to the patient (e.g. scheduling a visit). Physicians can review these recommendations in Chart Review.
Tests and ResultsPoint of Care Tests (POCT)POCTs are any tests that are done outside of a traditional lab setting. Today, there are disparate processes for documenting these tests across each department. In the future, POCTs will be documented in Epic and results will be manually entered using “enter/edit results.” Entering the result this way makes it available for the care team to view within results review.During an Ambulatory encounter, if a POCT is ordered, it must also be resulted in order to close the encounter. If the test is not done, the order must be canceled. In an ambulatory setting, Physicians can enter/edit POCT results for the following: • Glucose • HGB A1C• Hemoglobin• INR• Occult Blood• Rapid Flu• Rapid Mono• Rapid RSV• Rapid Strep • Urine Dipstick• Urine Pregnancy Test
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202015

Need-to-Know Change Impacts Categorized by Topics
Ambulatory Physician Snapshot (Page 4 of 4)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Tests and ResultsInternal and External (i.e. Quest) Lab ResultsInternal and external lab results will be shown together on one line to facilitate trending except for a small group of select lab results.
Review Test ResultsEpic includes enhanced features to ensure that test results are reviewed by the appropriate Provider:• Ambulatory test results should be reviewed by the ordering Physician. Each clinic determines if the results are routed to the clinic pool and/or
ordering Provider.• Tests resulted during the inpatient stay should be reviewed by the Attending responsible for the patient’s care as well as by the Physician who
ordered or recommended the test (per policy).• Tests resulted after the patient has been discharged will be routed to the patient’s PCP or Authorizing Provider of the order if there is no PCP.• In Results Review, Physicians can hover over a value to view the reference range and where the lab was resulted.
Charge CaptureCharge Capture & Level of ServiceCharge Capture & Level of Service: Physicians who use CCHC billing services will use Epic instead of previous methods to enter charges, level of service, and coding information for:• Inpatient visits• Bedside procedures • Ambulatory visitsPhysicians will have an option to mark an encounter for coder assistanceWorkspacesMaximum Number of Open ChartsEpic allows up to 5 workspaces (patient charts, reports, and/or activities) to be open at once, which translates into having up to 4 patients charts open simultaneously. If orders are entered on the wrong patient, the Provider must cancel and re-order for the correct patient.Citrix Timeout and Epic Hyperspace Workstation Timeout SettingsIn the Ambulatory settings, a Citrix inactivity warning will pop up after 3 minutes of inactivity, and the workstation will lock after 8 minutes of inactivity. All information and screens that the user had opened prior to the time out will be maintained.
After 30 minutes of inactivity, the workstation will time out and the system will revert to the login screen.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 16

Top Nursing Change Impacts
17

Top Change Impacts#1. Medication Administration Time DecreaseThe time window for when a medication is considered overdue will reduce from 2 hours to 1 hour. After 1 hour, Nurses can still document the administration, they will just have to provide justification for why it is overdue. #2. Medication Dose AdjustmentsNurses are now able to adjust the next scheduled medication dose without contacting the pharmacy. The Nurse will need to enter a reason for adjusting a scheduled medication time within the Single Patient MAR.
If the Nurse wants to adjust the entire medication schedule, they will still have to contact the pharmacy via the Rx message link on MAR and select “Adjust Times” as the reason for the message.#3. Single Patient MARMedication administration documentation is shared between the EC, Inpatient Care Areas, OR and procedural areas through the use of a Single Patient MAR. This will allow Nurses and other clinicians to view medications that were given in these care settings to include the last time given and the dose administered. #4. Secure ChatToday, Nurses use ASCOM phones to communicate verbally. In the future, Secure Chat will be enabled for any member of the Care Team that can document in the patient’s chart:• Secure Chat allows users to send secure text messages to each other in Epic, and can be used via Rover or from the workstation.• Content captured in Secure Chat will be discoverable and can become part of the patient’s medical record. • Secure Chat promotes interdisciplinary communication for brief, non-emergent messages, but it should not be used to replace orders, e.g.,
request for a consult or communicate critical results.#5. Interdisciplinary Care Plan DocumentationToday, CCHC uses Nursing-only care plan documentation. In the future, CCHC will use Elsevier interdisciplinary care plan documentation. Care Plans will be reviewed daily and during interdisciplinary rounds.The following roles will contribute to and update the inpatient Care Plan: Nurses, Therapists (PT, OT, SLP, RT), Nutritionists, Case Managers, Social Workers, Palliative Team, IV team, and Spiritual Care. Care plans should be updated per policy, e.g., daily, as patient goals and plan of care needs change. The Nurse validates and is overall responsible for the care plan.#6. Lines, Drains, and Airways (LDA) insertion DocumentationToday, CCHC uses disparate systems. It is common to receive a patient that had an LDA placed in another area, e.g., procedure area, without associated documentation about its placement.
In the future, Epic allows for one patient record, which stays with the patient:• The clinician who places an LDA will be responsible to document the associated LDA information in Epic. When the LDA is added to the patient
record, the associated flowsheet rows are automatically added to support ongoing documentation. • Wounds are also considered an LDA within Epic and clinicians can document wound associated information within the LDA activity.• To document an IV infusion on the Single Patient MAR, the nurse will need to link the line to the infusion. #7. Epic Risk ScalesCCHC will use the Hester Davis fall risk scale for Inpatient Adults (including maternity) instead of John Hopkins fall risk scale. CCHC will also be retiring Sedation Agitation Scale (SAS) and will be using Richmond Agitation Sedation Scale (RASS) in all areas.
Need-to-Know Top Nursing Change Impacts
Nursing Snapshot (Page 1 of 2)In one
glance…
You can find change impacts to your day-to-day operations as Nurses brought about by the new Epic EHR, and how they will improve quality of patient care and clinician satisfaction. It is important to read each change impact in detail as we prepare for go-live.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
Background of Change Impacts
As part of the implementation process, clinical advisory groups convened to oversee the governance of the Epic project and its impact on clinical operations. Decisions were reviewed and finalized during Advisory Group Meetings, including: Nursing Workgroup, Physician Advisory Group, Ambulatory Advisory Group, Clinical Advisory Group, and Integrated Advisory Group. All groups consisted of Operational Subject Matter Experts that contributed their expertise and served as advocates for clinicians across CCHC.
Advisory groups aim to promote and standardize leading practices that contribute to a high quality of patient care and cliniciansatisfaction. Hence, these groups played a pivotal role in identifying, approving, and validating Change Impacts—also known as significant differences between current and future state practices—that will occur due to the Epic implementation. Based on a comprehensive review of all advisory group decisions, CCHC Nursing leaders identified the following change impacts as top impacts.
For changes occurring due to an Epic module, please refer to the Epic Module-level Change Impact Assessments found here.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 18

Need-to-Know Top Nursing Change Impacts
Nursing Snapshot (Page 2 of 2)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Top Change Impacts#8. Copy Forward DocumentationToday, there are no policies that govern what can be copied forward within a given timeframe. There is some documentation available in Soarian for Copy Forward.
In Epic, Nurses will be able to copy forward LDA group assessments and Head-to-Toe assessments. In addition, copy forward will be restricted to only the same clinician within their shift (ex: Nurse A can only copy forward his/her assessment). Epic will be able to track user activity according to the new governing policies. #9. Nurse-Patient AssignmentsToday, Charge Nurses pre-assign nurses on paper and whiteboards, and Nurses can assign themselves to their patients in ATSS. Paper assignments are kept for 7 years before they are archived in IronMountain. If the Charge Nurse is unable to make the Nurse assignments, another Nurse from the previous shift will complete the assignment.
In Epic, Charge Nurses will assign patients using one of the several methods (e.g., Nurse Assignment Wizard, Sign-In, and Patient List) to Nurses prior to the start of shift and update assignments throughout the shift.
• If not automatically assigned, Nurses will create their own patient list when they first sign in at the start of shift & continue to update throughout the shift
• Assignments made in the Nursing Assignment Wizard automatically flow into Treatment Teams workflows• Charge Nurses can search within Epic for CCHC Nurses to assign• The Treatment Team Activity allows Nurses to find all clinicians currently or previously assigned to the patient's team along with their contact
number• Clinicians are expected to keep the treatment team information up to date by updating during shift changes, and modifying the start and end
times of a clinician's assignment#10. Barcode ScanningBarcode scanning will be expanded to support positive patient identification for blood product transfusion. The areas that will implement bar code scanning for medication and/or blood product transfusions include the inpatient units, Emergency Care, perioperative units, and IV Therapy Centers.#11. Massive Transfusion Protocol (MTP) and Blood Administration WorkflowsPhysicians and Nurses will follow the Mass Transfusion Protocol workflow and Blood Administration workflow (for non-MTP) to place orders. • For Massive Transfusion Protocol, Physicians will need to place order set in Epic. Nursing will document in Mass Transfusion flowsheet and will
not be required to scan the blood unit or have dual sign-off.• For non-MTP Blood Administration workflows, there will be a seamless integration between SoftBank and Epic. There is an order to “Prepare
Blood” and “Transfused Blood”, which are included in the blood transfusion order sets.#12. Nurse BrainThe Brain is a home activity that helps Nurses and other roles plan their day. Inspired by what Nurses commonly jot down on paper at the start of their shifts, the Brain presents a timeline view of the orders, events, and requirements for each patient the Nurse is assigned to. The Brain facilitates more efficient documentation workflows through inline flowsheets to satisfy documentation requirements and the ability to complete bar code medication administration without leaving the Brain.#13. RoverRover is a net new functionality that provides Nurses and other clinicians the ability to complete select workflows using mobile devices. The workflows that utilize Rover include medication administration (barcode scanning), nurse specimen collections, vital sign documentation and communication with other clinicians. The Rover Functions by Role/Area Matrices are as follows:
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202019

Other Nursing Change Impacts
20

Need-to-Know Change Impacts Categorized by Topics
Nursing Snapshot (Page 1 of 5)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Patient AdmissionPreferred PharmacyPharmacists, Pharmacy Techs, MAs, Nurses, and Physicians will be able to document/verify the patient’s preferred pharmacy, but:• The expectation for Emergency Care and Acute Care is that the first touch clinician will collect preferred pharmacy information while capturing the
medication history.• The expectation for Ambulatory Care will be that the MA or Nurse confirms and/or captures the patient’s preferred pharmacy as part of the
rooming process.• Patients may modify their preferred pharmacy during the eCheck-in process and via MyChart.Code Status Default and DisplayCode status upon patient admission will default to assume full code when a patient presents to the inpatient units without a prior code status order. Physicians will still be required to enter Code Status orders for each inpatient encounter. “Partial” is a new code status that will display for the patient’s care team to update any special restrictions.The following two permutations are available: • “Prior full” will display when there is a previous full code order in the patient record.• “Prior” will display when there is a previous code status order other than full code. The “Prior” status is informational and not a code status order.Patient RecordBreak-the-Glass FunctionalityWhen an encounter is marked as confidential in Epic, it will trigger the break-the-glass functionality, which will prompt the Nurse to enter a reason why they are viewing the patient’s record. Information about this “break-the-glass” encounter is then sent to the Health Information Management team. Patient encounters that will automatically be marked as confidential include:• Behavioral Health Clinic*• IP Psych*• Partial Hospitalization*• Infectious Disease* Registration can also mark an encounter as confidential for specific patients, e.g., VIPs & Legal Reasons.The patient’s treatment team members and clinicians who log into these departments to complete their work will not have to break the glass to view the patient’s chart.Single Patient StoryboardEach patient will have a storyboard that includes key information previously available in the header of the patient chart. This information is moved to a user-friendly sidebar, making it easier to read and allowing key information to be highlighted quickly and easily. The storyboard will display information that is relevant to clinicians based on their role and care settings.Single Patient Storyboard AdditionsWithin the Storyboard, For Your Information (FYI) flags and ACO/PHO risk member indicators will also be displayed.FYI flags are manually added to the patient record and indicate that there is significant, actionable information available about the patient. Physicians can hover over the FYI flag to view additional details. The following flags may be used: • Custody Issues• Medication Contract• Blood Products Refusal• Hospice Patient• Palliative Care• Transgender Patient• Heart Failure Readmission Risk• Pain Contract• History of aggression/violence• Dismissed from PCP• Dismissed from specialist• No trespass orders• Hearing impairment• Vision impairment• Care Plan
Providers and Nurses (including case management) can add and remove specific FYI flags, and these flags are not visible to patients.Patient Record Updates via MyChartPatients will now be able to make updates to their medical, social, surgical, and family history through on-line history questionnaires after they have been verified by a Nurse or Physician. This can be done prior to an appointment via MyChart or at a Welcome kiosk.Single Patient Past History DocumentationNurses and clinical support staff will now document within a single Past Medical and Surgical Patient History in Epic that crosses ambulatory and acute encounters.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202021

Need-to-Know Change Impacts Categorized by Topics
Nursing Snapshot (Page 2 of 5)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Patient Record (continued)Single Patient Problem List with ICD-10 DiagnosisThere will be one patient problem list shared between acute and ambulatory care settings. PCPs are tasked with maintaining the problem list for chronic problems and diagnoses. All Physicians and APCs on a patient’s care team will be responsible for updating the patient problem list for diagnoses that they are managing.
For Ambulatory settings, patients may update their medical problem list prior to an appointment or via Welcome kiosk when checking in for their appointment. These additions won’t be added until they are verified by a Physician or Nurse.Single Patient Medication ListThere will be one patient medication list shared between acute and ambulatory care settings.• PCPs will be responsible for maintaining the complete list, but Physicians, APCs, Pharmacy Techs, and Nurses, on a patient’s care team will be
responsible for reviewing the medication list with the patient.• Home medication information can be obtained via Care Everywhere for patients who receive care at other organizations that use Epic.• Patients will now be able to make updates to their current medication list through history questionnaires. This can be done prior to an appointment
via MyChart. These additions won’t be added to a patient’s chart until they are verified by a Nurse or Physician.• Clinical staff will be able to obtain a prescription history via SureScripts as another external data source in addition to Care Everywhere.Admission AssessmentOverdue Patient Admission Assessment NotificationNurses are responsible for completing the admission assessments within 24 hours. The Epic system will prompt Nurses at 18 hours post-admission with an icon to remind them that they have clinical documentation that is still outstanding. Observation patients will have the full admission assessment completed.Care PlanCare Plan Goals & End DatesToday, Care Plan goals do not require end dates. In the future, end dates in the care plan will default to 4 days for general care plans only.Case ManagementPredictive ModelsRisk of Unplanned Readmission will be used for Case Management to identify patients at high risk for readmission with the goal of focusing on discharge planning and increasing transitional care.
Note: Sepsis Predictive Model and Deterioration Index for Acute are pending further workflow reviews.Continued Care and Services Coordination (CCSC) Discharge ModuleCCHC is moving from Allscripts to Epic’s Case Management CCSC module for patient care coordination, utilization review, discharge planning, and extended care facility placement. This will provide Nurses with the ability to view discharge planning information previously documented within Allscripts.Electronic Durable Medical Equipment (DME) OrdersClinical staff (Nurses, therapists and/or case managers) are now allowed to enter and pend DME orders for Provider signature.
If a Provider does not sign the DME orders prior to discharge, a Best Practice Advisory (BPA) will display for Providers and Nurses letting them know there are pended orders. This will also prevent Nurses from printing out the discharge After Visit Summary until the orders are signed.
The DME orders include process instructions to meet medical supply vendors and payor requirements.OrdersOrder Modes & Co-SignaturePhysicians, APCs, and CRNAs place medication and procedure orders using the standard order mode which does not require a Physician co-sign. The exception is Admission order entered by an NP or PA that require co-signature.• Orders placed by clinicians that are not Physicians, APCs or CRNAs, all require a Provider co-signature unless they use the "per protocol no
cosign required" order mode.• ED Scribes can no longer place any active orders, all of their orders will pend and not be communicated until signed.Ancillary Consult OrdersEpic will not automatically place consults based on patient assessment but will recommend (via Best Practice Advisory) that the Nurse enter a consult order based on patient assessment or risk screen findings for Nutrition, Social Work, and Spiritual Care.Acknowledging OrdersToday, Nurses acknowledge all orders, and Therapies are not required to acknowledge orders.
In the future, Nurses will acknowledge all new patient orders.• Therapies, Dieticians, and Social Work will acknowledge orders relevant to their area. As a result, Nurses will not acknowledge other clinicians’
orders.• Nursing Assistants can view new orders but not acknowledge orders.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 22

Need-to-Know Change Impacts Categorized by Topics
Nursing Snapshot (Page 3 of 5)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Orders (continued)Diet OrdersWhen placing an “advance as tolerated” diet order, Physicians will now be required to enter a target diet to advance to. For example, “advance as tolerated to a cardiac diet”. This is considered a communication order and is not routed directly to Dietary.
Nurses and Registered Dieticians may modify the original diet order, and this will not require a cosign. They will use the “per protocol no cosign required” order mode when modifying the diet order to achieve the target diet.TestsPoint of Care Test (POCT) DocumentationPOCTs are any tests that are done outside of a traditional lab setting. Today, there are multiple non-interfaced POC tests being performed in the acute and ambulatory settings. Documentation is department-specific on paper spreadsheets, flowsheets, or directly into Nursing notes.
In the future, Nurses will document POCT electronically in Epic using “enter/edit results.” Entering the result this way makes it available for the care team to view within results review. Lab Specimen CollectionWhen a specimen is unfit for testing for a Nurse collect specimen, the lab will send the Nurse an order redraw request that will place a specimen collection task on the worklist. The lab will continue to call the Nursing unit for awareness.Documentation ToolsCode NarratorNurses will document codes electronically in real-time in all acute areas using a tool within Epic known as the code narrator. At the end of the code, the Physician who is leading the code is required to sign the document which includes medications administered during the code.
Two sign-off options are available: • Real-time sign off that occurs on the RN’s screen (preferred option)• From an InBasket message to sign off the code or code report
The recording RN will need to update any documentation prior to the Physician sign off. The Physician will not be able to edit any code documentation from the code report that they receive in their InBasket.Advance Care PlanningAdvance Care Planning is an activity within Epic that provides a centralized area for all information related to the patient end of life treatment preferences, e.g., health care agents, capacity to make own care decisions, code status, documents on file. CCHC will continue to collect the MOLST form and scan it into the patient record. Nurses can also write a note using the “ACP Note” within the activity.Nurse AcuityCCHC will replace Clairvia with Epic’s Nurse Acuity functionality.Documentation TasksPatient Hand-Off Documentation During Patient TransferToday, both the receiving Nurses and sending Nurses document that a hand-off of the patient occurred via a transfer assessment, transfer note, or an event note. Nurses do not document hand-off at change of shift, but document hand-off for transfers, e.g., EC to inpatient.
In the future, Nurses will document patient hand-off communications during transfers using flowsheet documentation within the transfer navigator. The receiving Nurse will document patient hand-off communications and contact information for the sending Nurse in case there are follow-up questions. Nurses will not document patient hand-off communications that occur at change of shift.Flush Documentation & VolumesAll central line flushes (heparin, normal saline) will be documented on the Single Patient MAR. Prior to administration, the flush is linked the associated line. If patient has an order for I/O monitoring, the Nurse will manually enter the volume of the flush within the I/O flowsheet that is embedded in the MAR.Clinical Documentation Within Defined Limits (WDL)Today, CCHC utilizes 4 versions of WDL definitions – Soarian (Inpatient), Centricity (OB), PulseCheck (Emergency Care), and Aria (Oncology). WDL definitions are standardized for select departments but not across the organization.
In the future, Epic foundation WDL definitions will be standardized across the organization and replace current systems’ definitions. Definitions can be viewed by end users in the row information in Epic.Interpreter Services DocumentationToday, Interpreters document within Midas. Nurses are expected to document interpreter information but this is not consistently completed.
In the future, Interpreters will document within Epic. Nurses will document the need for an interpreter and interpreter contact information within Epic using the validated flowsheet rows.Required DocumentationToday, Nurses can continue to document if some required documentation is missing and saved as in progress. However, documentation will not be saved as complete until all required documentation is complete.
In Epic, there will be a hard stop in the documentation process if the required fields are not filled.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202023

Need-to-Know Change Impacts Categorized by Topics
Nursing Snapshot (Page 4 of 5)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Documentation TasksClinical Documentation Security for StudentsToday, Nursing student assessment documentation does not require a co-sign and their documentation is viewable to other clinicians in Soarian.
In Epic, Nursing students may document following the guidelines below: • All student documentation will require a co-signature.• Student documentation is not viewable in-patient summary reports until verified by the instructor but is viewable within flowsheets in pink font
indicating it is student documentation.• Students will have their own log-in to document.Post-Discharge Outstanding DocumentationThe patient record will not be closed at discharge. This allows clinicians to complete their documentation for up to 365 days after discharge and medication administration documentation for up to 72 hours post discharge. The documentation will reflect the date and time that the information was entered.Medication Administration & ManagementMAR Documentation Given by OthersToday, there is no functionality for clinicians to document medication administration for other clinicians. In the future, Providers will enter the medication order and the Nurse will document the medication administration on the Single Patient MAR, indicating that the medication was given by another clinician.Medication Administration Documentation After Due TimeIn Epic, Nurses can document medication administration up to 72 hours after the scheduled due time, instead of the 8 hours hard stop in Soarian today.Medication Profile Display within PyxisToday, all of a patient’s active medication orders display within the Pyxis with medications that are dispensed by the Pharmacy displaying as greyed out. In the future, Pyxis will only display orders for a patient where there is an active order and the medications are stocked within the Pyxis cabinet. The active orders report, medication orders report, and Single Patient MAR can be referenced for active medication orders. The Single Patient MAR will be considered the source of truth. Discontinuation of Maintenance IV FluidsMaintenance IV fluids will now have a default stop time of 48 hours from when the order is placed. At the 24th hour, the order will move into the “expiring medications” section of the orders activity where Physicians can renew or discontinue the order. If no action is taken, the order will auto-discontinue at 48 hours.Dual Signatures on High Risk Medication AdministrationsDual signatures require two Nurses to be physically present at a patient’s bedside to enter their login and password information. This process is a hard stop that is only required prior to initiating the highest risk medications, with dose changes, and bag/syringe changes.*Insulin co-sign will now be completed within Epic and not in the Pyxis.Nursing Student Medication AdministrationToday, Nursing Instructors administer medication with the Nursing students and sign off as themselves (Instructors). In the future, Nursing students may document medication administration on the MAR but will require instructor oversight and dual signature.Medication-Related Reassessment FunctionalityWhen pain medications are administered and documented on the Single Patient MAR, a reassessment is triggered and displays on the Nurses’ worklist. The Nurse will also use a link within the task to access the documentation flowsheet and complete the reassessment.
Timings for reassessments will also change:• Document reassessment within one hour after administering oral pain medications• Document reassessment within 30 minutes after administering IV or SQ pain medications• Document reassessment within one hour of administering nausea medications (IV & PO)Patient EducationSingle Patient Education Content SourceMicromedex Care Notes is the single patient education content source for patient education materials that are provided to the patients and their families at discharge (can be attached as references/attachments directly in Epic).DischargeAfter Visit Summary (AVS) WorkflowNurses will not be required to initial individual pages of the AVS, and patients will no longer need to sign that they received their AVS or discharge instructions. In Epic, there will be a flowsheet row that Nurses check to indicate the information was reviewed and given to the correct patient.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/2020 24

Need-to-Know Change Impacts Categorized by Topics
Nursing Snapshot (Page 5 of 5)
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
New Tools & FunctionalityWorklist FeaturesNurses will have the following features that appear on their worklist / “Brain”:• Tasks that need to be completed to meet regulatory requirements such as pain assessment, restraint documentation, care plan reminders• Reminders for one-time, non-medication administration tasks that are not part of a standard routine and can be easily overlooked, e.g., Specimen
Collection• Tasks that are populated by orders, Best Practice Advisories, or by a user who creates a task on the fly• Tasks that they manually added to their worklistThe worklist should be reviewed at change of shift hand-off report.Nursing ScorecardsStaff Nurses and Clinical Leaders utilize their own scorecards. Nurse Managers will see the supervisor scorecard.
Workspace & DevicesMaximum Number of Open ChartsEpic allows up to 5 workspaces (patient charts, reports, and/or activities) to be open at once, which translates into having up to 4 patients charts open simultaneously.
Citrix Timeout and Epic Hyperspace Workstation Timeout Settings• In inpatient settings, a Citrix inactivity warning will pop up after 2 minutes of inactivity, and the workstation will lock after 3 or 4 minutes of inactivity
(depending on the computer type). All information and screens that the user had opened prior to the time out will be maintained.• In outpatient settings, a Citrix inactivity warning will pop up after 3 minutes of inactivity, and the workstation will lock after 8 minutes of inactivity.
All information and screens that the user had opened prior to the time out will be maintained.• After 30 minutes of inactivity, the workstation will time out and the system will revert to the login screen.
Epic MonitorInstead of the current whiteboard, CCHC will add an electronic Epic “Patient List” Monitor on all Med/Surg, ICU, and Maternity Unit Nursing stations to display the patient list. The following columns will be shown on the patient list monitor: • Patient name (will display as last name, first initial)• Attending Provider will display as the last name• Nurse will display as first name and last initial• Patient Room Number• Current Location (where the patient is if off unit)• Age/Sex• Fall Risk Screen• Code Status• Isolation/Precaution Status
Biomedical Device IntegrationCardiac monitors, fetal monitors, ventilators, dialysis machines, and many vital sign devices will be integrated with Epic. This will allow automated download of vital signs, other patient parameters, and device settings that become part of the patient record when reviewed and verified by the nurse. Vitals collected as part of intake or at the bedside will be wirelessly integrated into Epic (i.e. the vital information and the collecting clinicians' credential information will be automatically updated and reflected on the patient chart). Nurses will be able to scan their badge following the patient's barcode on the vitals machine to accomplish this. This integration will eliminate the time used to manually enter vitals and will be a secure seamless method for all clinicians.
Downtime Procedures for Clinical DocumentationIf the system is down, Nurses will transcribe from an Epic-provided downtime paper form into the charts when the system is available on: • Height, weight, and allergies • 4 hours of vital signs• Add/remove any new or discontinued LDAs• Last patient assessment• Medication Administrations (4 hours, last 3 days for chemotherapy)• I/O for last shift• New orders
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202025

Epic Module/Areas
Acute
26

Level Current State Workflow Future State Workflow Impacted Roles
High The EC does not utilize barcode scanning for blood or medication administration.
Barcode Scanning: Barcode scanning will be expanded to support positive patient identification for blood product transfusing as well as medication administration. One step medications will not be barcode scanned.
• EC Nurses• Respiratory Therapy
High Order sets are in multiple systems. A significant amount of the processes are conducted on paper.
Massive Transfusion Protocol: Physicians will need to place order set in Epic for Mass Transfusion. Nursing will document in the flowsheet for Mass Transfusion and will not be required to scan the blood unit or have dual sign-off. This is separate from the regular blood prepare and transfuse blood admin workflow.
• EC Nurses• Physicians
Medium Doctors are writing a wet signature on paper. They are able to do an interpretation without an order and the order can be vetted afterwards.
EKG Workflows: Providers are can do a wet read in Epic. When an order is placed, the physician must link it to an order to document the wet read. Scribes can pend orders but cannot sign the order. Epic generates a technical charge upon completion of task.
• Nurses• Scribes• Diagnostic Techs• Providers
Medium Acute resuscitation events are documented predominantly on paper and then scanned into the patient’s EMR. Medications are ordered after the event and the nurse back documents the administration.
Code Narrator: Nurses will document codes electronically in real-time in all acute areas using a tool within Epic known as the code narrator. At the end of the code, the physician who is leading the code is required to sign the document, which includes one-step medications administered during the code.
Two sign-off options are available: • Real-time sign off that occurs on the RN’s screen (preferred option)• From an InBasket message to sign off the code or code report
The recording RN will need to update any documentation prior to the physician sign off. The physician will not be able to edit any code documentation from the code report that they receive in their InBasket.
• Clinicians• Code Team• Training Team
Medium CCHC does not use signed and held orders. When a patient is in the EC, the admitting hospitalist can write STAT orders in Soarian that can be routed to PulseCheck for orders to be carried out in EC, otherwise there is an icon indicating that the patient has signed orders in Soarian, which requires the nurse to log into a separate system to see orders.
Signed and Held Orders: EC patients without a bed assignment two hours after the admit order is placed will in “Boarder” status. If there is no bed two hours after the bed request, all signed and held orders are to be manually released by the EC Nurse. EC Nurses may choose to release selected orders from the “signed/held” status, or all the orders, before the two hour cutoff. Nurses will release orders for any antibiotic orders immediately. On the EC trackboard there will be a “held orders” column which will turn red two hours after the bed request order, indicating they are now a “Boarder” and prompting the nurse to release all held orders. Orders that need immediate attention are not “signed/held” by the ordering provider, rather signed for immediate action.
• EC Nurses• PACU Nurses
Need-to-Know Epic Benefits, Change Impacts, and New FunctionalitiesASAP Emergency Center Snapshot (Page 1 of 2)
Epic Benefits
• Improve patient care and communications through improved digital documentation processes and patient identification
• Expand digital documentation process and integrate clinical documentation between EC and Inpatient Units
• Assign patients to emergency care providers electronically, track patient histories and allergies, and make notes about each patient’s visit
• Enable customizable ordering tools and documentation macros• Leverage decision-support from hundreds of Epic customers’ best
practices
In one glance…You can find key exciting changes to the Emergency Center (EC) workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/17/202027

Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Level Current State Workflow Future State Workflow Impacted Roles
Medium Providers and their scribes can concurrently document in a Provider note.
Scribe Documentation and Orders: EC Scribes can no longer place any active orders. All orders will pend and not be communicated until signed. Signatures can be done through iPads (Canto).
• Providers• Scribes
Medium EC Pyxis machines are not profiled.
EC Pyxis Are Profiled with the exception of trauma machines: Medication orders in ASAP will be auto-verified through Willow unless that medication order has a ‘High’ or ‘Very High’ warning, or if it is a medication that is prepared to dispense from Pharmacy. Pediatric Parenteral are also not auto verified. Nurses can override the warning and administer the medication in an emergency situation.
• Nursing• Pharmacy
Medium Physicians are using Picis (PulseCheck) in both the UC and EC settings.
Applications in Urgent Care and Emergency Center: Physicians practicing in both UC and EC will be using different modules within Epic in the respective settings.
• Physicians• APCs
Low EC provider performs a procedure on an inpatient floor (e.g. Intubation) and then communicates this procedure to the EC administrators to manually send the documentation to Logix.
Inpatient Consults/Procedures Billing: EC providers have a button available in a sidebar when writing their inpatient procedure note to automatically send the documentation to Logix.
• EC Physicians• Billing Staff
Low There is one shared note containing different elements of the record.
Physician Notes: In Epic, CCHC will use Shared Notes. There is a share button to share notes between physician and scribe. Notes can only be shared between physician and scribe, not physician to physician. Once an ER note is started for a patient and there is a physician hand off, the physician or scribe can write a progress note.
• Providers• APCs• Scribes
Need-to-Know Epic Benefits, Change Impacts, and New FunctionalitiesASAP Emergency Center Snapshot (Page 2 of 2)
In one glance…You can find key exciting changes to the Emergency Center (EC) workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
New Functionality brought on by Epic
Expected Patients: EC staff will have the ability to list expected patients on the EC track board prior to their arrival. This can be done for both EMS patients and transfers from other facilities.
Temporary Patients: In Epic, the Nurse will have the ability to arrive or expect a temporary patient with an anonymous namingconvention.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/17/2020 28

Level Current State Workflow Future State Workflow Impacted Roles
Medium TheraDoc pulls Lab and Radiology data from Soarian and provides a report. Then, the Infection Preventionist manually checks Soarian to verify the remaining criteria to confirm the infection.
Surgical Site Infection (SSI): Epic allows for automated tracking of surgical patients for SSI reporting in one location, without manual extractions. Manual verifications are only needed if someone in the OR does not document per the workflow.
• OR Nurses• Infection Preventionists
Medium In TheraDoc, if the Infection Preventionist opens a patient chart that had an MDRO in the past year, then they will either follow up manually with the patient care team for decolonization protocol to be ordered in Soarian, or manually order in Soarian Clinicals.
Infection Tracking: An “infection” smart text appears on a patient’s chart when they have a positive Multi-Drug Resistant Organisms (MDRO). There are default review dates for Physicians or Infection Preventionists to complete review. System automation can add infection on positive lab results.
Patient Care team is notified immediately to put on the decolonization protocol without Infection Preventionists needing to take manual action.
• Infection Preventionists• Attending Provider• Patient Care Team
(Nurses, etc.)
New Functionality brought on by Epic
Patient and Provider Contact Tracing Reports exist directly in Epic for Infection Preventionists to monitor potential outbreaks and alert affected personnel
Auto-Update Infection and Isolation/Infection Mismatch Rules are used to inform clinicians that a patient has an infection as soon as a lab is resulted and alert clinicians if they need to take more isolation precautions
Heads-Up Dashboard exists for Infection Prevention with daily counts of patients who have been identified by the lab as having a certain organism
Microbiology Data is categorized based on patient populations to investigate disease spread
COVID-19 Infection Status enables Providers to identify infected patients as soon as they express COVID symptoms, thus allowing them to enact the proper precautions as early as possible. Providers can use the infection status to both manage and rule-out confirmed COVID-19 cases in the clinic
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Bugsy (Infection Control) Snapshot
Epic Benefits
• Improve safety of patients and their communities as clinicians are alerted as soon as the lab is resulted to activate isolation precautions
• Receive prompt and accurate assessment of infection risk
• Monitor potential outbreaks and activate isolation precautions efficiently with contact tracing, infection tracking, and data trending dashboards
• Enhance interdisciplinary care with auto-update infection and isolation/infection mismatch rules
• Minimize manual review of surgical cases with automated tracking of surgical patients for surgical site infection (SSI) reporting
• Assist with reporting requirements to disease registries, government agencies, and other entities
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Infection Control & Prevention workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202029

Level Current State Workflow Future State Workflow Impacted Roles
High CCHC does not have a health information exchange capable of viewing, incorporating, or discretely reconciling any information from external records.
Care Everywhere Adoption: Care Everywhere will be used throughout CCHC for health information exchange. Upon a patient’s arrival to the Emergency Center (EC), there is a two-step process:1) Automatic query out of Care Everywhere to see if there are patient
matches. 2) If there is no match, staff can search for a patient and manually link.
Staff can look at clinical data in real time from other organizations. Depending on the organizations’ existing authorization requirements, CCHC staff may need to sign other organizations’ authorization forms to have data released to CCHC.
• All Ambulatory providers and Clinical support Staff
• All Acute Providers and Nursing
• All EC Providers and Nursing
• HIM Staff
High HIM is only involved when patients sign the form. They are not responsible for talking to physicians and updating links.
HIM Operational Group: If another organization links to CCHC or vice versa and there is a chart correction, HIM department is responsible for unlinking the patient. HIM needs to provide a Care Everywhere ID when another organization partner calls due to an inability to match.
• HIM Staff
Medium Allergies, meds, problem list, and immunizations are not reconciled.
Reconciling External Epic Organizations’ Patient Data into CCHC Patient Chart: Physicians will be able to: • Review and reconcile external patient data (i.e. discrete allergies,
medications, problems, and immunization history) and incorporate into the CCHC chart if desired.
• Once the data is reconciled, it becomes a permanent part of the patient’s chart and can be used to drive future clinical decisions.
• Patient can sign a form to opt out from Care Everywhere by contacting HIM medical records retroactively or signing a form upon arrival.
• Providers• Nurses• Medical Assistants on
ambulatory side
New Functionality brought on by Epic
Care Everywhere Queries:• When patients are arrived into EC, Urgent Care, inpatient, or any scheduled encounters, the patients’ demographic information will be
queried to Care Everywhere (and prior to their appointment for Ambulatory encounters)• Automatic queries are performed for any Epic organization that is near a patient's home or work address. If there is no match, a
manual query can be performed
Offers automatic event notifications to patients’ PCPs.
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Care Everywhere Snapshot
Epic Benefits
• Improve patient safety with secure patient record exchanges for planned and unplanned transitions of care
• Access accurate, consistent, and complete patient information quickly
• Enhance patient experience by minimizing duplicative tests, examinations, and procedures
• Save time by enabling real-time and secure exchange of accurate patient medical information between organizations
• Reduce costs by decreasing unnecessary tests• Allow clinicians to reconcile external data in patients’ local charts to
improve accuracy of medical histories• Monitor patient statuses with real-time notifications across organizations
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Health Information Exchange workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 30

Level Current State Workflow Future State Workflow Impacted Roles
High Allscripts is used for discharge planning, which includes manual documentation, faxing, and eReferrals.
Case Management Discharge Module: Epic’s Continued Care and Services Coordination (CCSC) module is used for discharge planning and placement. EpicCare Link will be used for 45 facilities, and facilities not using Link will use electronic faxing through Epic.
• Case Management / Social Work
• IT Staff
High DME orders for discharge are conducted on paper.
Electronic Durable Medical Equipment (DME) Orders: DME Orders are electronic, and staff are able to enter and pend DME orders for Provider signature. If a Provider does not sign the DME orders prior to discharge, a Best Practice Advisory (BPA) will display for Providers and Nurses letting them know there are pended orders.
• Case Management / Social Work
• Nurses• Therapists• Providers
High CCDAs are sent by unit clerks. Continuity of Care Documents (CCDA) Transmission: Case Manager sends CCDAs by choosing an appropriate destination under the placement header in the Case Manager Navigator.
• Case Management / Social Work
• Unit Coordinators
High EDD is not entered into the system during patient care visits.
Expected Discharge Date (EDD): Case Managers and Physicians enter and modify an expected discharge date.
• Case Management• Nurses• Physicians• Admin
Medium CCHC uses Nursing-only care plan documentation.
Elsevier Interdisciplinary Care Plan Documentation: Care Plans will be reviewed daily and during interdisciplinary rounds. Nurses, Therapists (PT, OT, SLP, RT), Nutritionists, Case Managers, Social Workers, Palliative Team, IV team, and Spiritual Care will contribute to and update the Inpatient Care Plan.
• Nursing / Nurse Managers• Allied Health• Case Management• Respiratory Therapists• Dietary
Medium Case Managers do not use workqueues.
Workqueues: In Epic, workqueues will be to identify patients needing various case management intervention.
• Case Management / Social Work
Low Paper-based/Soarian documentation. Forms are generated in Allscripts.
Case Management Forms: The top 5 most utilized paper forms will be fillable forms in Epic and can be completed electronically. Form Filler allows Case Managers to fill out and send PDF forms electronically to government agencies, payors, regulatory agencies, and more. Data is pulled in automatically from the patient’s chart, making it faster and easier to submit the necessary paperwork.
• Case Management / Social Work
Low Case Managers place some orders (including paper orders).
Order Mode and Signature (Case Management): Orders placed by Case Managers all require a Physician to co-sign and are all placed in Epic.
• Case Management / Social Work
• Physicians
New Functionality brought on by Epic
The ‘Risk of Unplanned Readmission’ Predictive Model is used for Case Management to identify patients at high risk for readmission with the goal of focusing on discharge planning and increasing transitional care.
Streamline patient transitions from hospital to continued care services by sending clinical information electronically to post discharge service providers, community resources, and social care providers.
Case Managers can use pre-built reports or pick and choose parts of a patient’s chart to build the best case for patients’ reimbursements
Dynamic patient lists provide the team with real time information rather than printed lists on paper.
Sort and identify patient information from Census List (e.g., demographics).
Social work referrals: Referral sources (including information and fax numbers) have been built in the system, decreasing the time consumed by staff needing to look up fax numbers as the whole record does not need to be printed.
Data integration flows into the GMLOS, limiting the manual entry requirement by staff.
New system views facilitate utilization review for Managers.
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Case Management Snapshot
Epic Benefits
• Improve transition of care after discharge by sharing accurate patient information across CCHC and outside organizations
• Focus on patient safety and experience with predictive modeling, order modes, and data integration
• Cut down on communication exchanges with payors that can slow down patients’ reimbursements
• Enhance interdisciplinary coordination and communication through electronic DME orders, streamlined responsibilities when sending CCDAs, and Elsevier Interdisciplinary Care Plan documentation
• Reduce manual processing with Continued Care and Services Coordination (CCSC), filling forms electronically, dynamic patient lists, and data integration
• Increase resource efficiency by assigning expected discharge dates
In one glance…You can find key exciting changes to the Case Management workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202031
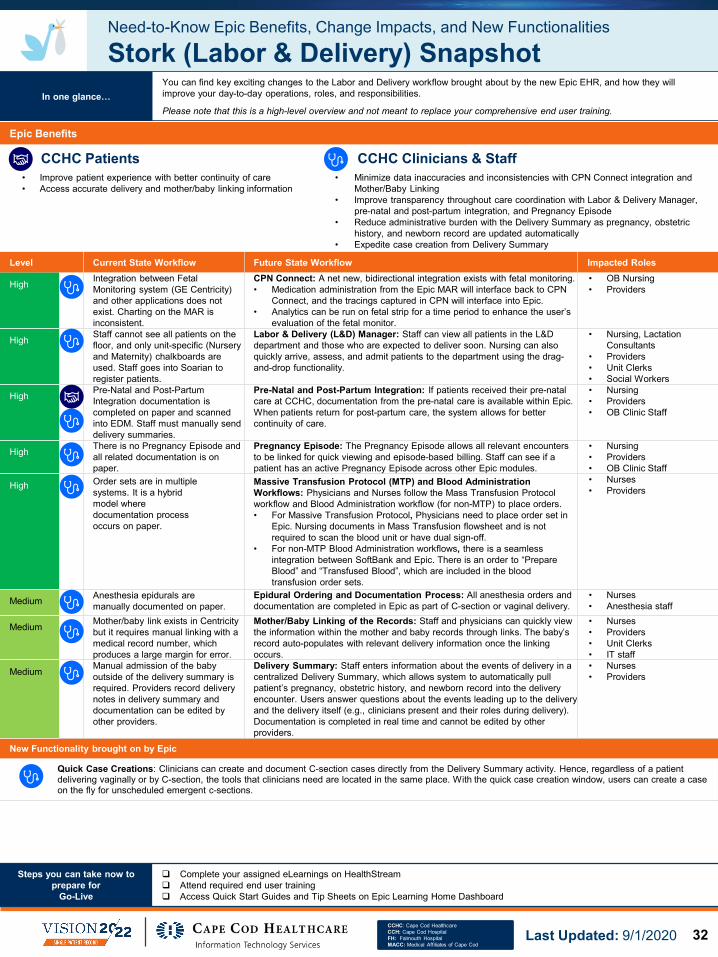
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
New Functionality brought on by Epic
Quick Case Creations: Clinicians can create and document C-section cases directly from the Delivery Summary activity. Hence, regardless of a patientdelivering vaginally or by C-section, the tools that clinicians need are located in the same place. With the quick case creation window, users can create a case on the fly for unscheduled emergent c-sections.
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Stork (Labor & Delivery) Snapshot
Epic Benefits
• Improve patient experience with better continuity of care• Access accurate delivery and mother/baby linking information
• Minimize data inaccuracies and inconsistencies with CPN Connect integration and Mother/Baby Linking
• Improve transparency throughout care coordination with Labor & Delivery Manager, pre-natal and post-partum integration, and Pregnancy Episode
• Reduce administrative burden with the Delivery Summary as pregnancy, obstetric history, and newborn record are updated automatically
• Expedite case creation from Delivery Summary
In one glance…You can find key exciting changes to the Labor and Delivery workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
Level Current State Workflow Future State Workflow Impacted Roles
High Integration between Fetal Monitoring system (GE Centricity) and other applications does not exist. Charting on the MAR is inconsistent.
CPN Connect: A net new, bidirectional integration exists with fetal monitoring.• Medication administration from the Epic MAR will interface back to CPN
Connect, and the tracings captured in CPN will interface into Epic.• Analytics can be run on fetal strip for a time period to enhance the user’s
evaluation of the fetal monitor.
• OB Nursing• Providers
High Staff cannot see all patients on the floor, and only unit-specific (Nursery and Maternity) chalkboards are used. Staff goes into Soarian to register patients.
Labor & Delivery (L&D) Manager: Staff can view all patients in the L&D department and those who are expected to deliver soon. Nursing can also quickly arrive, assess, and admit patients to the department using the drag-and-drop functionality.
• Nursing, Lactation Consultants
• Providers• Unit Clerks• Social Workers
High Pre-Natal and Post-Partum Integration documentation is completed on paper and scanned into EDM. Staff must manually send delivery summaries.
Pre-Natal and Post-Partum Integration: If patients received their pre-natal care at CCHC, documentation from the pre-natal care is available within Epic. When patients return for post-partum care, the system allows for better continuity of care.
• Nursing• Providers• OB Clinic Staff
High There is no Pregnancy Episode and all related documentation is on paper.
Pregnancy Episode: The Pregnancy Episode allows all relevant encounters to be linked for quick viewing and episode-based billing. Staff can see if a patient has an active Pregnancy Episode across other Epic modules.
• Nursing• Providers• OB Clinic Staff
High Order sets are in multiple systems. It is a hybrid model where documentation process occurs on paper.
Massive Transfusion Protocol (MTP) and Blood Administration Workflows: Physicians and Nurses follow the Mass Transfusion Protocol workflow and Blood Administration workflow (for non-MTP) to place orders.• For Massive Transfusion Protocol, Physicians need to place order set in
Epic. Nursing documents in Mass Transfusion flowsheet and is not required to scan the blood unit or have dual sign-off.
• For non-MTP Blood Administration workflows, there is a seamless integration between SoftBank and Epic. There is an order to “Prepare Blood” and “Transfused Blood”, which are included in the blood transfusion order sets.
• Nurses• Providers
Medium Anesthesia epidurals are manually documented on paper.
Epidural Ordering and Documentation Process: All anesthesia orders and documentation are completed in Epic as part of C-section or vaginal delivery.
• Nurses• Anesthesia staff
Medium Mother/baby link exists in Centricity but it requires manual linking with a medical record number, which produces a large margin for error.
Mother/Baby Linking of the Records: Staff and physicians can quickly view the information within the mother and baby records through links. The baby’s record auto-populates with relevant delivery information once the linking occurs.
• Nurses• Providers• Unit Clerks• IT staff
Medium Manual admission of the baby outside of the delivery summary is required. Providers record delivery notes in delivery summary and documentation can be edited by other providers.
Delivery Summary: Staff enters information about the events of delivery in a centralized Delivery Summary, which allows system to automatically pull patient’s pregnancy, obstetric history, and newborn record into the delivery encounter. Users answer questions about the events leading up to the delivery and the delivery itself (e.g., clinicians present and their roles during delivery). Documentation is completed in real time and cannot be edited by other providers.
• Nurses• Providers
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 32

Level Current State Workflow Future State Workflow Impacted Roles
High In Soarian, medication administration documentation can occur up to 8 hours after the scheduled administration time. After 8 hours, there is a hard stop and clinicians are not able to document the medication administration.
Medication Administration Documentation after Due Time: In Epic, medication administration documentation can occur up to 72 hours after the scheduled due time.
• Pharmacy• Nursing• Respiratory Therapist
High Nurses call and/or message pharmacy to change medication times. Nurses cannot change any scheduled doses independently.
Medication Administration Time Adjustments: Clinicians can adjust administration time for a single dose without contacting the pharmacy, but will need to supply a reason for this change in the MAR. If the clinician wants to adjust the entire medication schedule, they still have to contact the pharmacy via the Rx message link on MAR and select “Adjust Times” as the reason for the message.
FH will continue to use standard dosing windows per hospital policy whenever applicable.
• Pharmacy• Nursing• Respiratory Therapist
Medium Maintenance fluids are set to auto-discontinue today +1 at 1400 (CCH) or 1300 (FH) to prevent IV fluids from continuing to infuse for several days without being re-evaluated.
Discontinuation of Maintenance IV Fluids:1. Maintenance IV fluids are built with a default stop time of
48 hours from when the order is placed.2. At the 24th hour, the order will move into the “expiring
medications” section of the orders activity where Providers can renew or discontinue the order. If no action is taken, the order will auto-discontinue at 48 hours.
• Pharmacy• Nursing• Physicians
Medium All of a patient’s active medication orders display within the Pyxis with medications that are dispensed by the Pharmacy displaying as greyed out.
Medication Profile Display within Pyxis:1. Pyxis only displays orders for those medications that are
stocked within the cabinet on the Pyxis.2. The active orders report, medication orders report, and
Single Patient MAR will be the source of truth for a patient’s active medication orders.
• Pharmacy• Nursing• Respiratory Therapists
Medium EC Pyxis machines are not profiled. EC Pyxis: EC Pyxis machines are profiled, with the exception of trauma machines.
End users have their medication auto-verified unless:• the medication order has a ‘High’ or ‘Very High’ warning;• or if medication is prepared to dispense from Pharmacy. Pediatric Parenteral are not auto verified.
• Pharmacy• EC Nursing
Medium RhoGAM is dispensed by the Blood Bank.
RhoGAM Dispensing: RhoGAM is dispensed by the Pharmacy.
• Pharmacy• Nursing• Blood Bank
Medium Staff uses tablets to take pictures. All batch and patient specific are in Consortiex.
Dispense Prep: Hover cameras are used to take pictures and integrated into the EHR. Hover cameras are used for patient specific compounding, but batch compounding will continue to be in Consortiex.
• Pharmacy
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Willow Inpatient (Pharmacy) Snapshot (Page 1 of 2)
Epic Benefits
• Improve quality of care and save time as pharmacists have a centralized view of patient history and their contexts
• Enhance patient safety with efficient medication administration workflows
• Enhance interdisciplinary coordination and communication as data is integrated into Epic for EC and Pharmacy, antimicrobial tools, and new carousels
• Minimize unnecessary pharmacy manipulation with updated verification decision logic, auto-verification of specific medications, and enhanced medical profiling
• Save time with one-click verification, robust reporting capabilities, and enhanced medication administration workflows
• Improve quality of care as pharmacists can access patient history and dynamic system lists for clinical monitoring
In one glance…You can find key exciting changes to the Inpatient Pharmacy workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202033

Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Level Current State Workflow Future State Workflow Impacted Roles
Medium • CCHC charges for medications on administration in the inpatient units.
• EC and OR charge for medications on dispense.
• High-cost infusions are charged on administration when the medication is scanned.
• Inpatient Nurses do not indicate a stop time on the MAR. EC, IV Therapy and Outpatient Nurses indicate a “bag end time” on the MAR.
• Return credit process includes:o Return back to Pyxis (not a
MAR action).o Some pharmacists have access
to credit accounts.
Medication Charges: All medications are charged on administration except Cath Lab medication which will charge on dispense. A return credit process will remain in place for medications that are charged on dispense but not used.
• Pharmacy• Nursing
Medium RN conducts this process. Standardized Ortho Warfarin Protocol: In Epic, CCH Pharmacists will enter the order daily, similar to FH. Nomograms may be site specific, but easily implemented as long as the RN Manager and Pharmacists are aware.
• CCH Pharmacists• Nursing
Low Completed and updated for pending EC patients only in Soarian.
Adjusted Medication Reconciliation Tech Workflow: Pharmacy Techs use a score to determine the priority of patients already admitted that need historical home medications confirmed and updated. All EC patients being admitted will provide their medical histories, but if multiple patients were waiting, the tech would then use this score.
• Pharmacy• Medical Reconciliation
Techs
Low No carousels are used. New Carousel Install: Newly installed dispensing carousels are implemented in both main pharmacies. This equipment is integrated with Willow Pharmacy.
• Pharmacy
Low Antimicrobial tools are stored in Theradoc and the data is siloed.
Antimicrobial Tools: Pharmacy will no longer have to go outside of the EHR to locate the antimicrobial tools as they will be integrated into Willow, which integrates all data.
• Pharmacy• Infection Prevention
Low RX messages are received largely through phone calls.
RX Messages: RX messages are accessed through Epic InBasket.
• Pharmacy• Nursing• Respiratory Therapists
New Functionality brought on by Epic
“Smarter” decision support for pharmacists will point out important warnings
Updated dispense logic will prevent unnecessary manipulation of orders at the time of verification
Easy access to patient history (including outpatient notes and prescription history) can provide context for why a patient is on a specific medication
Additional robust reporting capability in Epic will provide flexibility for the management team. The current reporting is cumbersome and limited
One-click verification will enable verification efficiency
EC and Pharmacy are integrated in Epic and will be utilizing the same system, enabling have access to all patients
Pharmacy will use dynamic system lists in Willow for clinical monitoring
Willow will auto-verify specific medications therefore limiting pharmacists touch points. Medications will have enhanced profiling, leading to less pharmacy manipulation
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Willow Inpatient (Pharmacy) Snapshot (Page 2 of 2)
In one glance…You can find key exciting changes to the Inpatient Pharmacy workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 34

Epic Module/Areas
Ambulatory
35
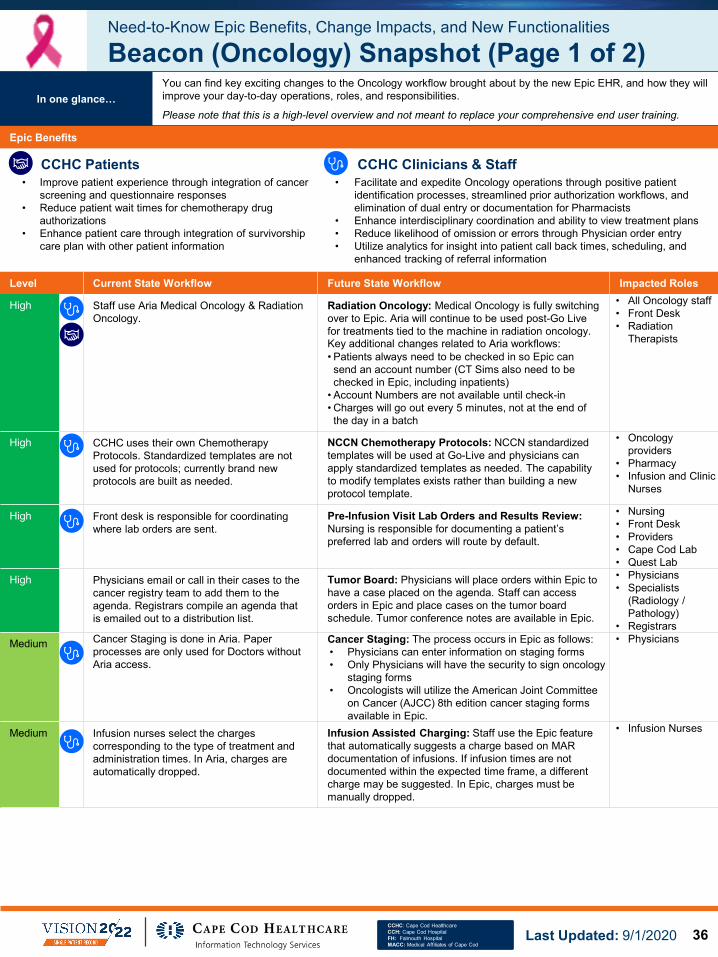
Level Current State Workflow Future State Workflow Impacted Roles
High Staff use Aria Medical Oncology & Radiation Oncology.
Radiation Oncology: Medical Oncology is fully switching over to Epic. Aria will continue to be used post-Go Live for treatments tied to the machine in radiation oncology. Key additional changes related to Aria workflows:• Patients always need to be checked in so Epic can send an account number (CT Sims also need to be checked in Epic, including inpatients)
• Account Numbers are not available until check-in• Charges will go out every 5 minutes, not at the end of the day in a batch
• All Oncology staff• Front Desk• Radiation
Therapists
High CCHC uses their own Chemotherapy Protocols. Standardized templates are not used for protocols; currently brand new protocols are built as needed.
NCCN Chemotherapy Protocols: NCCN standardized templates will be used at Go-Live and physicians can apply standardized templates as needed. The capability to modify templates exists rather than building a new protocol template.
• Oncology providers
• Pharmacy• Infusion and Clinic
Nurses
High Front desk is responsible for coordinating where lab orders are sent.
Pre-Infusion Visit Lab Orders and Results Review:Nursing is responsible for documenting a patient’s preferred lab and orders will route by default.
• Nursing • Front Desk• Providers• Cape Cod Lab• Quest Lab
High Physicians email or call in their cases to the cancer registry team to add them to the agenda. Registrars compile an agenda that is emailed out to a distribution list.
Tumor Board: Physicians will place orders within Epic to have a case placed on the agenda. Staff can access orders in Epic and place cases on the tumor board schedule. Tumor conference notes are available in Epic.
• Physicians• Specialists
(Radiology / Pathology)
• RegistrarsMedium Cancer Staging is done in Aria. Paper
processes are only used for Doctors without Aria access.
Cancer Staging: The process occurs in Epic as follows: • Physicians can enter information on staging forms• Only Physicians will have the security to sign oncology
staging forms• Oncologists will utilize the American Joint Committee
on Cancer (AJCC) 8th edition cancer staging forms available in Epic.
• Physicians
Medium Infusion nurses select the charges corresponding to the type of treatment and administration times. In Aria, charges are automatically dropped.
Infusion Assisted Charging: Staff use the Epic feature that automatically suggests a charge based on MAR documentation of infusions. If infusion times are not documented within the expected time frame, a different charge may be suggested. In Epic, charges must be manually dropped.
• Infusion Nurses
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Beacon (Oncology) Snapshot (Page 1 of 2)
Epic Benefits
• Improve patient experience through integration of cancer screening and questionnaire responses
• Reduce patient wait times for chemotherapy drug authorizations
• Enhance patient care through integration of survivorship care plan with other patient information
• Facilitate and expedite Oncology operations through positive patient identification processes, streamlined prior authorization workflows, and elimination of dual entry or documentation for Pharmacists
• Enhance interdisciplinary coordination and ability to view treatment plans• Reduce likelihood of omission or errors through Physician order entry• Utilize analytics for insight into patient call back times, scheduling, and
enhanced tracking of referral information
In one glance…You can find key exciting changes to the Oncology workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 36

Medium Barcode scanning for positive patient identification occurs in the following scenarios: • Medications and lab specimen collection,
including nurse collect specimens.• Medication barcode scanning is in place
for all Critical Care Units, Inpatient Care Units, IV Therapy (Oncology and Non-Oncology), and Labor and Delivery.
• Mobile phlebotomy scanning is in place for all of the above plus the Emergency Center, IR/Cath Lab, and Perioperative areas.
Barcode scanning for positive patient identification does not occur in the following scenarios: • Blood products and breast milk.• Medication Administration in the
Emergency Centers.
Barcode Scanning: Barcode scanning will be expanded to support positive patient identification for blood product transfusion. The areas that will implement bar code scanning for medication and/or blood product transfusions include:• Inpatient Units• Emergency Care• Perioperative Units• IV Therapy (Oncology and Non-Oncology)
Note: Ambulatory offices will be an exception for implementing barcode scanning for procedural time outs.
• Oncology staff• Nursing staff
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Beacon (Oncology) Snapshot (Page 2 of 2)In one glance…
You can find key exciting changes to the Oncology workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
New Functionality brought on by Epic
Visibility of patient treatment plan in any context on Storyboard
Implementation of positive patient identification processes
Cancer screening and questionnaires are available to patients at home on MyChart and in the clinic with iPads
Integration of Epic Modules for Oncology, Willow Inpatient Pharmacy, and Pathology
Streamlined prior authorization workflows for chemotherapy drugs will be more efficient for staff, reduce patient inconvenience, and reduce financial risk to the organization
Use of workqueues across multiple roles and functions
Physician order entry will reduce risk for omission or errors and increase efficiency
Population management functionality such as oral chemotherapy management tools
Integration of the survivorship care plan with the record instead of a separate stand alone document manually scanned in
Streamlined receipt, tracking of referrals from referring physicians utilizing Epic at CCH/FH
New analytics capabilities to take the place of manual dashboards
Access to tumor conference notes as part of the medical record at both facilities, with concurrent documentation during conference
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202037

Level Current State Workflow Future State Workflow Impacted Roles
High Staff document 15 Minute Safety Checks on paper.
15 Minute Safety Checks: Staff will document 15 Minute Safety Checks on a mobile device or on a workstation.
• Nursing
High Outpatient billing services are conducted within a third party system. Accounts Receivable and Payment Posting are managed by Advantage.
Behavioral Health – Billing: Outpatient billing services will be conducted within CCHC’s Epic system. Accounts Receivable and Payment Posting are managed in-house at CCHC, but submission of claims and coding will be managed by Advantage.
• Billing staff• 3rd Party Coders
High Treatment planning is conducted on paper (checkboxes) for Inpatient and Partial.
Treatment Planning: Staff will conduct treatment planning electronically. New reporting tools are available to track status of treatment plans. Staff can discretely update problem goals and interventions for patients on individual electronic care plans.
• All BH staff
Low Staff are not alerted or required to change a patient’s observation status.
Patient’s Observation Status – Ready for Discharge: For any patients in observation status, there will be a BPA that appears in the Discharge Navigator for Nursing to have them change the patient’s level of care from ‘Observation’ to ‘Ready for Discharge.’
• Primary RN
Low HIM staff can mark patient chart content as sensitive.Inpatient: No similar current state functionality for providers.Outpatient: All Physicians can mark patient charts and notes as sensitive, and the option exists to either mark the patient’s chart or a single note as confidential.
Sensitive Notes: Sensitive Notes can be viewed only by Behavioral Health Therapists and Counselors on patient’s care team. If a note is marked as “sensitive”, it will not be shared to the patient portal. Notes written by Behavioral Health therapists and counselors are sensitive by default, but the option is available to not mark the notes as sensitive.
• Therapists• Counselors
Low Outpatient staff can mark the patient’s chart or a single note as confidential.
Confidential Encounters: Providers have the ability to mark patient encounters as confidential. When an encounter is marked as confidential, it will trigger the break-the-glass functionality within Epic. This will prompt the Physician to enter a reason why they are viewing the record. Information about this “break-the-glass” encounter is then sent to the Health Information Management (HIM) team.
Patient encounters that will automatically be marked as confidential include: Behavioral Health Clinic*, IP Psych*, Partial Hospitalization*, Infectious Disease, Occupational Health*.* Registration can also mark an encounter as confidential for specific patients, e.g., VIPs & Legal Reasons.
• Providers• Patients• Registration staff• HIM staff
Low Partial department documents on paper.
Partial Department Documentation: Partial department will document electronically in Epic.
• All Partial Department users
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Behavioral Health Snapshot
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Behavioral Health workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/15/2020
Epic Benefits
• Improve patient experience through improved care and treatment planning capabilities, as well as quicker billing processes
• Enable quicker and more discrete documentation of patient information, such as 15 Minute Safety Checks and Patient Treatment Plans
• Leverage reporting capabilities to more efficiently track patient treatment plan information
• Create and update a patient’s care plan using Elsevier content• Facilitate patient billing services using system logic and workqueues
CCHC Patients CCHC Clinicians & Staff
38

Level Current State Workflow Future State Workflow Impacted Roles
Low Every exam room in the Ortho office has file folders with various instructions, forms, etc.
Reporting (Patient Questionnaires): Questionnaires and Questionnaire series can be manually assigned to patients by users or can be automatically assigned based on defined criteria.
• Rooming staff
Low CCHC uses a 3rd party referral process to charge for DMEs.
Durable Medical Equipment (DME) Ordering: The new process in Epic requires placing an electronic referral order but will still utilize 3rd party for DME.
• Rooming staff• Physicians• APCs
Low Each outpatient Ortho practice is using its own PACS system and some are integrated with their respective EMR.
PACS System: The PACS systems for all outpatient Ortho practices will be standalone and not integrated with their respective EMR. Staff will need to manually upload images, and staff will need to toggle between the two systems as needed until CCHC replaces their entire PACS system (date TBD).
• All Ortho staff
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Bones (Orthopedics) Snapshot
Epic Benefits
• Save time filling out questionnaire forms • Reduce staff time by automatically assigning patients’ questionnaires based on defined criteria
• Review pertinent information, document, order, and charge with minimal clicks
• Reduce time by physicians having quick access to accurate, consistent, and complete patient information through tailored Relevant Summaries
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…
You can find key exciting changes to the Orthopedics workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
New Functionality brought on by Epic
Ability to document, order and charge for joint injections with minimal clicks
Encounters can be concluded from a single screen
Images, injections, global period days, surgeries, therapy visits, and past encounters can be viewed for a particular body location at a glance. (This can only be done when the clinic’s PACS are integrated with the hospital)
Clinicians can have a tailored Relevant Summary where they can review pertinent information about body locations
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/16/202039

Level Current State Workflow Future State Workflow Impacted Roles
High eCS and Legacy systems are used. The AVS process is similar to Epic, but there is minimal Portal use.
After Visit Summary (AVS): Patients are able to schedule appointments and complete questionnaires in the MyChart portal.
• AVS will automatically print for patients who want to receive a printed copy
• Patients who do not want a printed copy can view their AVS in MyChart
• Patient • Ambulatory Clinic staff• Rooming staff
High Occupational Health workflow includes paper-based documentation.
Occupational Health: Ambulatory functionality in Epic is used for Occupational Health workflow. The workflows are transferring from paper charts to Epic documentation.
• Occupational Health Staff
High Emerald: Allows administration of Influenza immunizations by written protocol. MACC: Requires physician order to administer immunizations. Nurse can queue the order for physician to sign.
Immunizations Orders: Licensed Clinical Support Staff or Nurses can order and administer immunizations per protocol.
• Licensed Clinical Support Staff
• Nurses
High Primary Care and Specialty staff have to follow protocol in a hard copy book.
Nurse Triage: CCHC will implement Nurse Triage with Office Hours Schmitt-Thompson content for Nov. 1st go-live, to more efficiently provide consistent, standardized tools and documentation within Epic for seamless nurse triage workflows.
Nurse Triage is available to Clinic Nurses at go-live.
• Clinic Nurses
High Staff assist with home medication documentation in a limited capacity. There is a medical reconciliation manual process in eCW, and support staff can discontinue meds.
Ambulatory: Office clinical support staff record home medications, dose, and frequency with the patient and available tools, such as SureScripts.
Home Medications: Staff record home medications and utilize available tools, such as SureScripts.
• Ambulatory: Licensed Clinical Support Staff can remove medications and flag other medications for removal upon review by the Provider. Epic clearly indicates which medications are home/OTC medications.
• Medical Assistants are not able to remove a medication – however are able to flag for Providers.
• Physicians• APC’s• Nurses• Medical Assistants
Medium PCPs and Providers receive a patient’s discharge summary and emergency care information, but the information received is inconsistent.
Results Review: PCPs receive the correct information, faster, including emergency care tests, test results for patients that have been discharged, and results come back post-discharge.
• PCPs• Providers
Medium A diagnosis is required by Medicare for Ambulatory non-medication orders.
• Diagnoses are part of the Ambulatory encounter and inpatient diagnoses are used for professional billing, as well as, for the hospital bill
• Diagnoses are also used in determining the case mix index, which is used to adjust quality and mortality data that may affect reimbursement and may be reported publicly
Diagnosis Required on Physician Orders: The system requires diagnosis association for all Ambulatory (medication and non-medication) orders, but does not require diagnosis association for hospital encounters and emergency encounters. Providers can associate diagnosis and sign off within Epic.
• Physicians
Medium Preventative care needs and quality measures are documented in many different places in the patient record, which leads to duplication of effort in tracking down overdue care gaps.
Care Gaps: Epic provides one centralized place from which care gaps can be reviewed, postponed, discontinued, edited, satisfied, and/or ordered.
• Physicians • APC’s• Nurses• CMA’s
Medium There are no automated best practice alerts to flag providers.
Best Practice Advisory (BPA): Epic has several BPAs around immunizations, women's health, diabetes, cancer screening, control substance prescribing, and more. These alerts "pop up" when triggered by an action or data in the patient's chart to remind the provider that additional information may need to be considered.
• Physicians• APC's• Nurses
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
EpicCare Ambulatory Snapshot (Page 1 of 2)
Epic Benefits
• Enhance quality of care for patient through integrated patient data across all outpatient practices
• Improve patient experience through self-service appointment scheduling and questionnaire completion
• Standardize encounter types and documentation tools for Clinician-only visits across all specialties
• Collaborate cross-functionally on patient care through Integrated patient data across all outpatient practices
• Improve staff communication and efficiency through technology and modernized workflows
In one glance…You can find key exciting changes to the Ambulatory workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/2/2020 40

Level Current State Workflow Future State Workflow Impacted Roles
Medium There is no standardized workflow for how providers communicate with clinical support staff. Some providers send the information to the staff's inbox directly, other practices send the information to a "Team" or "Staff" inbox that the clinical support staff access.
Clinical Support Staff "Pools" by Department: Each department or office will have a Clinical Support Staff "Pool“, where communication to clinical support staff will be sent or routed. Staff can access these pools and have the ability to filter by provider. Epic's InBasket also has different folders for the various tasks (e.g., Rx refill, patient call message, etc) so not all communication to the clinical support staff is sent to one folder. Multiple folders exist, each designed for a specific task.
• Physicians• APC's• Nurses• CMA's
Medium Paper-based patient assessments are used.
Patient Questionnaires: Patient assessments are available via MyChartor mobile device (iPad/tablet).
For some questionnaires, may need to scan in results to have it be associated with Patient.
• Rooming Staff• Patients• Physicians• APCs
Medium CCHC has Clinician-only visits in select clinics. The type of visit determines whether a Clinician-only Visit is scheduled. The Clinician completes documentation and provides to the provider for sign off.
A Clinician-only visit refers to a clinic appointment where the patient does not see a Physician or Advanced Practice Provider. The most common Clinician only visits are Nurse only visits, Nutritionist Consults, and Medical Assistant visits.
Clinician-Only Visits: Clinician-only visits across CCHC and will be scheduled to the actual provider where known.
Nurse-Only Visits will be scheduled to generic nursing provider. Nurses should indicate themselves in Epic if they take the visit.
• Nurses• Providers• Clinicians
Low Integrated functionality exists within eCW. There are some practices that have integrated functionality, and some are paper-based.
ECG (Midmark): All practices have integrated functionality with Epic. • Physicians• Nurses• Medical Assistants
Low CCHC automatically routes all specialty notes, including consultation and follow-up notes to the PCP, which requires significant manual effort.
Sending Referral Notes to Referring Providers: Physicians can check a box in the note editor to have their note sent to the patient’s PCP and/or referring provider when the visit is signed. Epic automatically pulls in the correct recipient (referring provider and PCP). There is an option to send the note to the referring provider with changes in POC. If the provider does not check the box in note editor, then the note will not be sent to the referring provider.
• Primary Care Providers & Referring Provider
Low APCs must manually route notes to their supervising providers for review. Blue Cross requires that the supervising Provider be the billing provider for visits by APCs.
Routing Charts to Supervising Providers: APCs manually route charts to their supervising provider using Epic functionality (CC – Carbon Copy button) in order to meet the requirement for number of charts reviewed by the supervising physician per specified time period. The supervising provider can review the routed charts in their InBasket. Charts are routed automatically based on insurance. The routing of notes for review is not automated in Epic.
• APCs• Supervising Providers
Low There are no consistent standards or policies for result review timeframes or process to monitor compliance. There is limited information in the Provider & Clinic Manager dashboards. There is no system alert to reminds providers of result review.
Results Review Expectations: CCHC is implementing consistent standards for result review timeframes / process to monitor compliance. PCPs will receive more information than they did previously. For inpatient, providers will receive test results or patient results that have been discharged and those results are sent back to the PCP. Provider and Clinic Manager dashboards will be used to monitor results that have not been reviewed within the CCHC expected timeframe. Providers will receive a system reminder for result review.
• Providers
Low There is a telephone-process to input procedure orders. The Surgical Scheduler is responsible for submitting. Surgical scheduling is booked directly into OR Manager.
Prep for Procedure: There is new functionality for procedure orders in Epic (Case Request for Procedure). The process is standardized within EpicCare Ambulatory, which includes electronic ordering instead of by telephone. Providers and Surgical Schedulers are able to input procedure orders.
• Ambulatory staff
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
EpicCare Ambulatory Snapshot (Page 2 of 2)
Steps you can take now to prepare for Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Ambulatory workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
New Functionality brought on by Epic
A COVID-19 infection status column will be created for a patient during the scheduling process and will display the patient’s current infection status for CCHC staff. Providers can use the infection status to manage, rule out, and mitigate against confirmed COVID-19 cases in the clinic
Last Updated: 9/2/202041

Level Current State Workflow Future State Workflow Impacted Roles
Medium No clinical information is restricted for affiliate providers. All information is obtained through Soarian. Outpatient clinics do not have access to different practices’ EMRs.
Affiliate Provider Restriction: Affiliate providers use the portal to obtain referrals and place orders in a centralized location. Within Epic, physicians can navigate to “InBasket” to get the messages from outside affiliate providers. Outpatient clinics will have access to ambulatory information from different ambulatory practices.
Patient information will not be shared through EpicCare Link for the following:
• 42CFR (Behavioral Health encounters will be the umbrella to require consent)
• HIV/AIDS and other sensitive results• Information release regarding 42CFR and HIV/AIDS will follow the
process established by HIM
• Physicians• All EpicCare Link users• Skilled Nursing Facility
Clinicians
Low Allscripts is used for some referrals (post-Acute). Paper faxing is used in some instances (ex: CT).
Electronic Referrals Management: End users leverage electronic referral submission and/or allow affiliates to manage referral data between EpicCare Link sites and CCHC EHR.
• Scheduling staff• External Providers
Low Users access Soarian through Citrix.
Citrix Access: Users will not need Citrix to access EpicCare Link. The EpicCare Link website will be available to the public.
• All portal users
Low No restrictions exist in Soarian.
Patient Encounters: Cannot be accessed by External Providers until accepting the referral (post-Acute).
• External Providers
New Functionality brought on by Epic
Clinicians with access to EpicCare Link will be granted access to a patient’s chart based on existing clinician-patient relationship and knowledge of specific patient identifiers
E-mail notifications are available for InBasket messages on the patients’ major events such as test results, EC admissions, etc.
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
EpicCare Link Snapshot
Epic Benefits
• Improve patient experience through better care coordination with affiliate providers
• Streamline information and communication with affiliate providers by using a single portal to obtain referrals, add orders, and communicate with physicians
• Enhance patient care coordination between physicians and clinical team • Increase information accessibility by removing the need to utilize Citrix for
EpicCare Link• Create timely communication channels by sending e-mail notifications for
patients’ major events• Manage data electronically through online referral data and submissions
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the EpicCare Link workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 42

Level Current State Workflow Future State Workflow Impacted Roles
Medium Social Determinants of Health (SDOH) are not collected in a standardized way or displayed on a patient’s storyboard. SDOH are defined as social and environmental factors that affect patients' health status.
Display Social Determinants on Storyboard: Social Determinants of Health (SDOH) are available on a patient’s Storyboard, which provides quicker access to key details and common actions without switching screens. Key features of Storyboard include: • The SDOH in the Storyboard connects users with
assessments associated with the different domains• Screening may be opened from SDOH visible in the
Storyboard
• Clinicians (Outpatient Providers, Specialists, Nurses)
• Case Managers • Navigators• Diabetic Educators• Outpatient
Pharmacists
Medium Workflows for scheduling and appointments must be adjusted for Epic.
Scheduling/Referrals: There will be new workflows for handling referrals and appointments.
• Registered Dieticians• Pharmacists
Medium Patient’s care plan must be manually shared with PCP / Specialist.
Longitudinal Plan of Care (LPOC): Patient’s care plan and any interactions between the patient and case manager is viewable by the managing clinician.
• Clinicians (Outpatient Providers, Specialists, Nurses)
New Functionality brought on by Epic
Actionable work lists can be created for care managers through dashboards and reports
The Roster Management Engine can be utilized to drive the registry infrastructure to identify risk members across the health system
New Indicator on the Inpatient/Ambulatory Storyboard: CCHC staff are informed if a patient is part of a risk-based contract, which helps staff ensure post-acute resources are available
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Healthy Planet (Population Health) Snapshot
Epic Benefits
• Improve patient experience as clinicians have quicker access to patients’ social determinants and risk indicators
• Share electronic information through dashboards and reports• Improve continuity and transitions of care through LPOC• Maintain and improve support of current care management
programs and initiatives through visibility between case management and providers
• Inform staff of key patient information to ensure resources are available
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…
You can find key exciting changes to the Population Health workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202043

Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
MyChart (Patient Portal) Snapshot (Page 1 of 2)In one glance…
You can find key exciting changes to the patient portal workflow brought about by the new Epic EHR, and how they will improve the patient experience and your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/9/2020
Level Current State Workflow Future State Workflow Impacted Roles
Medium Providers must take manual action to share outpatient progress notes.
Confidential Encounters Triggering Break-the-Glass Functionality: Providers have the ability to mark patient encounters as confidential. When an encounter is marked as confidential, it will trigger the break-the-glass functionality within Epic. This will prompt the Physician to enter a reason why they are viewing the record. Information about this “break-the-glass” encounter is then sent to the Health Information Management (HIM) team.
Patient encounters that will automatically be marked as confidential include: Behavioral Health Clinic*, IP Psych*, Partial Hospitalization*, Infectious Disease, Occupational Health*.• * Registration can also mark an encounter as confidential for specific
patients, e.g., VIPs & Legal Reasons.• All patient encounters that are automatically marked as confidential
will have break-the-glass functionality except Occupational Health.
The patient’s treatment team and clinicians who log into these departments to complete their work will not have to break the glass to view the patient’s chart.
• Providers• Patients• Registration staff• HIM staff
Sensitive Notes: Sensitive Notes can be viewed only by Physicians on patient’s care team. If a note is marked as “sensitive”, it will not be shared to the patient portal.• CCHC will use Sensitive Notes, and will not default notes written in
specific areas as sensitive. Notes written by Behavioral Health therapists and counselors are sensitive by default. Psychiatry, Plastic Surgery, and Pediatrics can mark notes as sensitive on a case-by-case basis.
• Providers share all Outpatient Progress Notes via the patient’s MyChart account by default, and will have the ability to turn off sharing on a note-by-note basis.
• CCHC will consider giving all physicians the ability to mark notes as sensitive after assessing downstream effects post go-live.
• Patients • Physicians
Medium Patients cannot self-service schedule in the portal.
Patient Scheduling: New scheduling functionalities are available for patients, including: • Direct scheduling allows patients to schedule with Primary Care
practices • Ticket scheduling allows providers and clinical staff to send
appointment tickets for scheduling• Fast pass offers open slots to patient on the wait list automatically
• Patients • Providers• Scheduling staff
Epic Benefits
• Improve patient experience through self-service portal functionality that is user friendly and easy to use
• Enhance patient satisfaction through the ability to self-schedule and check-in to appointments online and reduce patient time spent in the waiting room
• Allow patients to invite family members or caregivers to have access to their MyChart accounts in order to help them schedule appointments and request medication refills
• Enable patients to receive non-sensitive test results automatically via the patient portal
• Enable comprehensive patient information to be available for providers and CCHC staff
• Reduce front desk staff and support staff workload
CCHC Patients CCHC Clinicians & Staff
44

Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
MyChart (Patient Portal) Snapshot (Page 2 of 2)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/9/2020
New Functionality brought on by Epic
MyChart COVID-19 Care Companion Care Plan: CCHC will utilize MyChart Care Companion - an interactive care plan in the MyChart mobile app, which delivers notifications, analyzes data provided by patients and connected devices, and orchestrates changes to the plan and escalations as needed to help patients, their caregivers, and care managers stay on top of a patient's care
MyChart Self-Triage: MyChart patient self-triage tools will direct patients to the right level of care for their symptoms and require limited intervention from Providers or staff. After the patient completes Self-Triage, actionable recommendations are presented to the patient (e.g. scheduling a visit). Physicians can review these recommendations in Chart Review
Paying Bills through MyChart: Patients can pay bills without having account by using ‘pay as guest’ feature
Patient Questionnaires: Patients can provide data about symptoms and history directly to the care team from the comfort of home/via personal device. Staff can also have instant access to this information either in the context of a visit or between visits in order to provide care and advice/education as needed
Personalized Messaging & Instructions: MyChart enables targeted population health messaging and instructions directly to patients via the portal (i.e. capture all patients at high risk criteria and send them a flu shot reminder)
Level Current State Workflow Future State Workflow Impacted Roles
Medium Patients are unable to make history updates via the legacy Patient Portal.
Patient Record Updates: Patients can make updates to their medical, social, surgical, and family history through on-line history questionnaires after they have been verified by a Nurse or Physician. This can be done prior to an appointment via MyChart or at a Welcome kiosk.
• Patients• Providers• Nurses
Low Patients call providers office directly and a Practice Manager has to field the call. Practice Managers must submit tickets.
Help Desk Support Model:• Help Desk Support for MyChart is being kept in-house at
CCHC• All Help Desk staff will be cross-trained in MyChart (handling
calls and MyChart app support)• Additional FTE resource for Help Desk• One portal for both inpatient and outpatient
• Help Desk staff• Patients
Low Patients must apply in person and bring documentation to Medical Records office.There is no proxy in place
Patient Proxy Access: Proxy requests are handled either by request submissions to HIM or a patient can invite another person to have proxy access to their account via MyChart.
• HIM staff• Patients
In one glance…You can find key exciting changes to the patient portal workflow brought about by the new Epic EHR, and how they will improve the patient experience and your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
45

Level Current State Workflow Future State Workflow Impacted Roles
High Inpatient: Documentation occurs in Soarian.
Outpatient: Documentation mostly occurs on paper. Therapists document via a Therapy Note.
Therapist Documentation Tools: Documentation occurs in Epic. Documentation status can be monitored by running reports. Therapist Documentation flowsheets will provide excellent trending opportunities.
Inpatient: will use flowsheet documentation in EpicOutpatient: will have some standardized flowsheet documentation and some free text.
• Therapists
High Visit count documentation occurs on paper.
Visit Counts: Based on referral and episodes, tracking is available for the following: • How many visits for an authorized referral• How many visits are left
• Therapists• Insurance Specialists• Front Desk staff• Patients
High Certification form must be faxed, which includes the most recent re-evaluation performed on the patient. Repeated every 30 days.
Plan of Care Certification: There is an automated tool that enables staff to view when a plan of care is coming due, awaiting signatures, and collecting signatures through InBasket. Medicare Plans of Care need to be recertified every 90 days.
• Physicians• Therapists• Front Office staff
High Staff documents how long they spent on each exercise and input total time. Staff manually enters charges and numbers.
8 Minute Charging Suggestions: Staff bills based on 15-minute increment time charge for therapeutic exercises. Epic provides suggestions on the appropriate type and number of charges, which is required by Medicare.
• Therapists
Medium Staff manually adds and removes patients to their rounding lists and also use coverage groups.
Patient Lists: Patient Lists are automatically created. Therapists are assigned based on incoming orders on Acute side. Therapists must acknowledge orders, which puts them on the patient’s treatment team. MyLists include patients where there is an established relationship.
• Therapists• Therapy Manager• Case Managers
New Functionality brought on by Epic
Leverage new, robust reporting capabilities (e.g., documentation status)
Rehab therapy minute tracking based on therapist documentation
Ability to automatically add the KX modifier on claims that need it
Utilize work queues to track billing edits, denials, insurance follow-up, and authorization
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Rehab Snapshot
Epic Benefits
• Improve patient experience by accurately tracking visit counts
• Standardize documentation tools through flowsheet templates • Reduce potential for inaccurate documentation by electronically tracking
visit counts • Reduce manual processes and time inefficiency through automated patient
lists, plan of care certification process, and KX modifier additions to relevant claims
• Track time accurately and quickly with 8-minute charging suggestions
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Rehab workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 46

Level Current State Workflow Future State Workflow Impacted Roles
High CCHC has four Urgent Care facilities that are staffed by EC physicians and Advanced Clinical Practice Nurses (APN), who mainly treat patients in Emergency Care and the Urgent Care clinics.
Urgent Care uses a subset of the Emergency Care content (assessment, documentation templates, order sets).
Urgent Care Application: The Epic Urgent Care Application is used across CCHC and involves the following features:
• Tools to enhance provider efficiency and streamline visits. Provides QPP/MIPS reporting functionality
• An Ambulatory/Urgent Care Module for urgent care facilities, which fits the Urgent Care patient population
• Urgent Care Providers
High Physicians are using Picis(PulseCheck) in both the UC and EC settings.
Applications in Urgent Care and Emergency Center: Physicians practicing in both UC and EC and will be using different modules within Epic in the respective settings.
• Physicians• APCs
Medium The Nurse order management system is in Picis (PulseCheck).
Nursing Workflows in Urgent Care: Nurse assessments are flow sheet-based. CCHC is moving away from a system of nursing assessments that were the same across EC and Urgent Care. Nursing will also be using the track board to monitor outstanding orders.
• Nurses• APCs• Urgent Care Techs
Low All results come in and are manually vetted by a nurse pool.
Results Routing: All results are being routed to pools instead of providers. A clinical pool will be receiving results from all labs ordered in the urgent care settings. PCPs are also being copied.
• Physicians• PCPs • Clinical Support
Low Staff indicate a discrete destination for a patient when they are discharged. Nurses discharge a patient from the current track board.
Disposition Workflow: Nurses will click “check out” instead of Discharge. Disposition will be completed in Navigator (Dispo and CC chart).
• All Urgent Care staff
Need-to-Know Epic Benefits and Change Impacts
Urgent Care Snapshot
Epic Benefits
• Improve patient care and communications through improved digital documentation processes and patient identification
• Enhance coordination and communication throughout continuum of care by enabling patient information to be viewed across separate Urgent Care centers
• Facilitate patient care through Express Lane functionality, which places all the tools that a provider needs to complete a specific visit into a single screen
• Leverage certification for the Quality Payment Program (QPP) and Merit-based Incentive Payment System (MIPS)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Urgent Care workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/22/202047

Level Current State Workflow Future State Workflow Impacted Roles
High Some CCHC Physicians use Tiger Text for Physician-to-Physician communication and Nurses use Ascom phones to communicate verbally.
Secure Chat: Secure Chat will be enabled for any member of the Care Team that can document in the patient’s chart. • Secure Chat allows users across roles to send secure text
messages to each other in Epic, and can be used via Haiku, Canto, Rover or from the workstation in HyperSpace.
• Content captured in Secure Chat will be discoverable and can become part of the patient’s medical record.
• Secure Chat promotes interdisciplinary communication for brief, non-emergent messages, but it should not be used to replace orders, e.g., request for a consult or communicate critical results.
• Nurses (Outpatient)
• Physicians (Outpatient)
Medium Anatomical images are not used in current state – only verbal descriptions and wound numbering.
Wound Location Documentation: CCHC has the ability to document the wound location using the human “avatar.”
• Nurses• UAPs• Physicians
Medium A different interface is used for charging for outpatient. Inpatient does not conduct charging. Hospital employed providers and private providers do not bill for private component.
Proc Doc Templates: Templates are used to facilitate documentation and charging for Wound Care visits. Only outpatient will be impacted from charging. Charge capture is a new interface for outpatient.Follow up with Bryan/Bart - determine if the Prof and Tech changes will be dropped by the Proc Doc or where these will be captured.
• Physicians and Nurses (Outpatient)
Medium Disparate systems are used:It is common to receive a patient that had an LDA placed in another area, e.g., procedure area, without associated documentation about its placement.
Lines, Drains, and Airways (LDA) Insertion Documentation: Epic allows for one patient record, which stays with the patient:• The clinician who places an LDA will be responsible to document
the associated LDA information in Epic. When the LDA is added to the patient record, the associated flowsheet rows are automatically added to support ongoing documentation.
• Wounds are also considered an LDA within Epic and clinicians can document wound associated information within the LDA activity.
• Physicians• Nurses
Low Nurses conduct screenings and patient instructions in Soarian.
Screenings and Patient Instructions: There will be a new way to document patient instructions. There will be an impact to the amount of time needed to complete the work and comfort level with the tool. Inpatient will have better documentation tools but Epic will be similar to what is done in current state.
• Nurses
New Functionality brought on by Epic
Rover provides Nurses and other clinicians the ability to complete select workflows using mobile devices.
Leverage cross-encounter documentation using LDAs and images to help wound care specialists and other clinicians contribute to care for the same wound over time.
Capture Wound Images: CCHC has the ability to capture digital images of the wound and incorporate it into the record via mobile devices. For outpatient, iPads will be used for image capture and documentation.
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Wound Care Snapshot
Epic Benefits
• Optimize patient experience by improving a patient’s ability to recover from wounds with strong cross-encounter workflows across both hospital and primary care settings
• Enhance staff collaboration workflows with cross-encounter documentation using LDAs and images to help wound care specialists and other clinicians contribute to care for the same wound over time
• Leverage additional technology for image capturing (Rover) and staff communication (Secure Chat)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Wound Care workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 48

Epic Module/Areas
Ancillary
49

Level Current State Workflow Future State Workflow Impacted Roles
High Anesthesia Providers manually capture vitals on paper.
Electronic Vitals Documentation: Anesthesia and Perfusion utilize device integration between anesthesia machines and ventilators to pull patient vitals data into anesthesia record electronically every minute.
• Anesthesia staff• Perfusion staff
High All documentation is done on paper.
E-Consents: Anesthesia Staff will use e-consents to perform documentation electronically.
• Anesthesia staff• Perfusion staff
Medium Anesthesia epidurals are manually documented on paper.
Epidural Ordering and Documentation Process: Anesthesia epidurals/medications are ordered using an Order Set prior to administration. If the drug is administered directly from the Anesthesia Medication Toolkit (One Step Meds), it will be read-only to the Nursing staff, and they will not be able to maintain the medication on the MAR. *CCH only: PCEA (Patient Controlled Epidural Analgesia) administration workflows require Anesthesia Providers to administer the medication on the MAR, but it will not appear on the Anesthesia record.
• Nurses • Anesthesia staff
Medium Surgical pre-procedure protocols are on paper.
Procedure Pass Protocols in Epic: Dynamic pre-procedure protocols track all required labs, tests, appointments, documents, etc. prior to the patient’s procedure. The process in Epic supplements existing paper protocols.
• Anesthesia staff• Periop staff• PAT staff• Surgeons• Surgical clinic staff
LowAnesthesia staff hang a sheet or leave a note on a whiteboard.
Post-Surgery Care: Anesthesia staff place follow up orders in Epic on patients needing ad-hoc post surgery rounding. This does not replace verbal communication if it is an urgent request.
• Anesthesia staff• Perfusion staff • Clinical care team
Low Document postoperative complications in postop note.
Complications: New section used to discretely document patient-experienced complications or incidents that occur during the procedure. Anesthesia Providers should not include education-based incident documentation as they should stay outside of the legal medical record.
• Anesthesia staff
New Functionality brought on by Epic
Only Anesthesiologists can mark the patient as “Ready for Procedure”, and this will notify all OR staff that the patient is ready for the procedure from an anesthesia perspective
Anesthesiologists and CRNAs can close encounters/signoff on patient’s chart
Touch-Enabled workstations in the OR help assist real-time documentation
Enhance intraoperative experience with notifications that recommend reducing fresh gas flow, which decreases the use of anesthetic agents, as well as intraprocedure blood documentation that includes electronic matching with the blood bank
Guardian helps Anesthesiologists see important procedure and patient details for all cases and appointments they’re responsible for
SlicerDicer provides clinicians with self-service reporting tools without having to work with IT
Share consistent and easily readable Anesthesia records across organizations with Care Everywhere
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Anesthesia Snapshot
Epic Benefits
• Improve patient safety and experience with e-consents, post-surgery care, and surgery complication documentation
• Access accurate, consistent, and complete patient information quickly with Care Everywhere
• Update patient records and document in real-time with automated device data capture
• Enhance interdisciplinary coordination and communication with “Ready for Procedure” notifications and Guardian
• Save time with e-consents, order sets, and procedure pass protocols• Share information across organizations securely through Care Everywhere• Update anesthesia records automatically and in-real time with automated
device data capture and touch-enabled workstations in OR• Save environment by transitioning from paper to electronic documentation
and intraoperative notifications
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Anesthesia workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
Last Updated: 9/1/2020CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
50

Level Current State Workflow Future State Workflow Impacted Roles
High Collection information is not enforced. Receiving Specimen: Specimens are not received in the lab until collection information and source is documented in Epic by the collector.
• Collecting Nurse• Lab staff
Medium Need to place separate (AOT) order for add-on tests.
Ordering Defaults to Add-Ons: Epic defaults to using an existing specimen if a viable specimen has already been collected. No specific add-on order is needed.
• Any clinicians placing lab orders
• Lab staffMedium Legacy version of troponin reference
range cannot distinguish specific characteristics.
New Lab Chemistry Analyzers: New lab chemistry analyzers will result in new troponin reference ranges.
• Clinicians
Medium AP Specimen collection is done on paper.
AP Specimen collection: AP Specimen collection and documentation is electronic.
• Lab staff• Nursing staff that
collect AP specimens
LowMobilab is used for specimen collection.
Rover: Rover is used for specimen collection. • Lab staff• Nursing staff at FH • EC nursing at CCH• IV Therapists at CCH
Low Lab staff needs to manually reorder. When a specimen is unfit for testing (IP only): Lab staff sends an order for a redraw and continues to call the Nursing unit for awareness. New orders are automated when existing specimen is marked as unfit.
• Lab staff• Nursing staff• Phlebotomists
Low No standardization of documentation of workups within LIS, and documentation is on paper.
Decision Trees in Micro: There is a standardized process and documentation of workups in Epic across three lab departments.
• Lab staff
Low No formalized bench process for Microplanting.
Microplanting: There is a formalized bench workflow process for Microplanting.
• Lab staff
Low Labels are developed by hand. Plate Labels: Micro generates plate labels using Epic. • Lab staff
Low Blood Bank receives their own specimens.
Central Processing Collects All Samples: Central processing collects all samples and Blood Bank does not need to go into Epic to receive specimens.
• Lab staff• Blood Bank staff
New Functionality brought on by Epic
Interfaced pathology system and blood bank results
Synoptic reporting will occur in Beaker
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Beaker (Laboratory) Snapshot
Epic Benefits
• Improve patient safety and experience with accurate reporting and efficient interdisciplinary coordination within patient’s care team
• Increase transparency of audits and quality control by requiring collection information and transitioning from paper to electronic documentation
• Save time with defaults to add-ons and generating plate labels in Epic• Improve quality, accuracy, and scalability of data with new chemistry
analyzers for troponin, standardized processes for workups and microplanting, and synoptic reporting
• Enhance interdisciplinary coordination through communication with Rover, the new workflow when specimens are unfit for testing, and streamlined central processing for all samples
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Laboratory workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202051

Level Current State Workflow Future State Workflow Impacted Roles
High Gastrointestinal (GI) consents are documented on paper.
GI E-consents: GI Staff use e-consents to perform documentation electronically. This ensures that consents are collected and attached to the patient's chart.
• GI Nurses• Endoscopists
High Information is tracked on paper. Procedure Pass and Dynamic Pre-Procedure Protocols: Real time checklist helps to track what pieces of required clinical documentation are obtained and/or missing for each patient prior to the procedure (including: consents, H&P, labs, tests, appointments, documents, anesthesia clearance, etc.)
• GI Nurses• Endoscopists
High Consents and History and Physical (H&P) are documented on paper.
Consents and H&Ps: Consents and H&Ps are conducted and documented electronically and viewable by all of the patient care team.
• GI Nurses• Endoscopists• Floor Nurses
Medium Endoscopy procedures are scheduled as cases in OR Manager.
Scheduling: Endoscopy procedures are scheduled as appointments.
Surgical offices request GI procedures as appointments while OR procedures are requested as cases.
• OR Schedulers• GI Physician Offices• GI Schedulers• Endoscopists
Low CCHC uses a modified version of the Main OR timeout.
Identical Timeouts: Endoscopy uses the same timeouts as Main OR for consistency. Identical Timeouts for both Endoscopy and OR areas will improve consistency in patient care.
• GI Nurses• Endoscopists
Low The result interface is indiscrete. It files as PDF with images in DMS.
Result Interface: The Provation and Pentax interfaces file the results into Epic discretely.
• Endoscopists• GI Nurses• Floor Nurses
New Functionality brought on by Epic
Room efficiency and tracking is improved by procedural core metric reporting and benchmarking, through input and utilization. Featured KPIs include volume, on-time starts, turnover, procedure length accuracy, cancellations, and utilization
Clinical documentation will automatically drive charging
Collect necessary information through pre-surgery questionnaires, and keep families up-to-date on a patient’s progress with Family Notifications
SlicerDicer provides clinicians with self-service reporting tools without IT intervention
Single Patient MAR allows GI Nurses and Physicians to view what medications were administered during a GI procedure to provide them with broader access to information, transparency and consistency of care
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Endoscopy Snapshot
Epic Benefits
• Enhance patient engagement with pre-surgery questionnaires and real-time ‘Family Notifications’ on patient’s progress
• Improve patient safety and experience with gastrointestinal (GI) e-consents as well as transparent and consistent patient care through single patient Medication Administration Record (MAR)
• Enhance interdisciplinary coordination and efficiency with procedure pass and dynamic pre-procedure protocols, clinical documentation-driven charging
• Increase transparency and consistency in patient care with identical timeouts for endoscopy and OR areas, as well as the single patient MAR
• Save time with GI e-consents and self-service reporting• Improve room efficiency and tracking with procedural core metric reporting
and benchmarking• Minimize data inconsistencies with discrete result interfaces
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Endoscopy workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 52

CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Level Current State Workflow Future State Workflow Impacted Roles
High Inpatient: Currently in Soarian.Outpatient: Currently on paper.
Invasive Cardiology Pre / Post Orders: Physicians enter pre / post orders in Epic.
• Invasive Cardiologists• Extenders • CVPA staff
High Booking requests are entered into OR Manager and confirmed by the OR schedulers. Inpatient: Currently in Soarian.Outpatient: Currently on paper.
Case Request Orders: Physicians, Extenders, PAs, and NPs enter case request orders in Epic.
• Physicians • Extenders• CVPA staff• CVPA Schedulers
High Resulting Workflows (Invasive Procedures): For several service lines, the Resulting System is changing as follows:
• Invasive Cardiologists
High Staff add on in OR Manager and schedule with specific surgeon. Add-on cases are communicated verbally.
Trauma Case / Emergent Procedures Scheduling: Specific buttons in Epic are used for scheduling cases.• Staff uses STEMI for CVPA, and ancillary orders
for emergent IR appointments. • Intraoperative Nurse needs to update Generic
procedure and provider.
• CVPA staff• Interventional MDs• Intraoperative Nurses
High Charges are manually uploaded in Xper via an Excel spreadsheet.
Document-based Charging: Select procedure charges, inventory, and contrast will generate a charge in Xper.
• CVPA staff• Revenue Integrity
Need-to-Know Epic Benefits and Change Impacts
Invasive Cardiology Snapshot (Page 1 of 2)
Epic Benefits
• Improve patient experience with efficient orders, resulting, and patient care workflows
• Streamline workflows between Cape Cod and Falmouth Hospital• Improve scheduling access as 3rd party Physicians can place case request
orders• Improve scheduling restrictions for available resources with case scheduling
blocks, limits on when outpatients can be scheduled, and user access• Enhance data consistency and efficiency with interfaces: Interface charging
from Peoplesoft to Xper. Sedation charging from Xper, and Supply interface directly from Peoplesoft to Xper
• Ensure efficiency, productivity, and flexibility as 3rd party resulting appears as discrete results and PDF, and automated result routing is based on results
• Improve transparency and consistency in patient care as patient chart will be accessible to all users
In one glance…You can find key exciting changes to the Cardiology workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
Service Line Current State Resulting System
Future State Resulting System
Cath/Cardiology Invasive Vascular
Xper Xper
EP – All EP Diagnostic, Ablations
EP Workmate EP Workmate
EP – Pacemakers, Biventricular
Pacemakers/ICDs
M*modal Dictation SmartText in Epic
Cardioversions M*modal Dictation SmartText in Epic
Last Updated: 9/23/202053

Level Current State Workflow Future State Workflow Impacted Roles
High Documentation Expectations in Xper and Epic: CVPA staff need to double document as follows: • CVPA staff
Medium Professional charges are captured on paper sheets, or coded in Zhealth on the backend (IR cases go to Zhealth).
Professional Charges: Professional Charges for all cases in CVPA, except for Transesophageal Echocardiography (TEEs) and cardioversions, are entered directly in Epic.
• All Cardiologists• Extenders
Medium Invasive and non-invasive patients follow the same discharging workflows.
Discharging workflows: Discharging workflows for invasive (case based) and non-invasive (appointment) are different:• Invasive cardiology patients need to be
discharged. • Non invasive cardiology patients need to be
checked out.
• IR staff• CVPA staff
Medium Invasive and non-invasive patients follow the same admission workflows.
Admission workflows: Admitting workflows for invasive (case based) and non-invasive (appointment) are different:• Invasive cardiology patients need to be
admitted. • Non-invasive cardiology patients will need to be
checked in.
• Registration/admitting staff
Medium Aborted procedures are documented in Xper. Aborted Procedures workflow: If CVPA procedure is aborted in the lab, CVPA staff updates performed procedure to “Aborted Procedure”, which auto-finalizes the study. This eliminates the need for the physician to result Invasive vs. Non-Invasive workflow.
• CVPA staff• Non-invasive
Physicians
Need-to-Know Epic Benefits and Change Impacts
Invasive Cardiology Snapshot (Page 2 of 2)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Cardiology workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
Workflow In Xper In EpicScheduling N/A • Schedule using Epic
Pre-call N/A • Document call was completed and print out prep sheet
Day of pre-procedure • General pre-procedure workflows
• Patient vitals• Pre-procedure meds
• Consents• Patient information
(allergies, home meds, patient history)
• LDAs (performed by Inpatient Nurse)
• Blood administration• Pre-procedure and
continuous medsIntra-procedure • Procedure log
documentation• Intra-procedure meds• Contrast
• Implants (ICD's IVC, Pacemaker, Leads)
Post-procedure • General post-procedure workflows
• Patient vitals• Post-procedure meds
• Post-procedure meds and continuous meds
• Printing out AVS
Charging • Procedure charges• Supply charges• Contrast charges• Pyxis meds will generate
from Pyxis
N/A
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/23/2020 54

Level Current State Workflow Future State Workflow Impacted Roles
High Resulting Workflows (Non-Invasive Procedures): For several service lines, the Resulting System is changing as follows:
• Non-Invasive Cardiologists
Medium Staff do not select specific procedure performed.
Diagnostic Imaging: Staff select the specific performed procedure at end of exam. The specific performed procedure selected will drop the correct charge for Revenue Integrity.
• Diagnostic Imaging Technicians
Low Stress data is documented on paper. Stress Data: All stress data is documented in Epic's flowsheet tables. Tracing is not interfaced and must be manually scanned in.
• Stress Technologists• Exercise
Physiologists• Cardiologists
Low There is no separate order for contrast from the procedure order.
Non-Invasive Cardiology Medications: A separate order is required for Non-Invasive Cardiology medications (including stress meds, contrast, radiopharmaceuticals), separate from procedure order. Techs can order per protocol.
• Diagnostic Imaging Technicians
Low Holter monitors are manually tracked. Holter Monitors: Staff will use the Monitor Status Report to track Holter monitors and event monitors. Tech fills out ID of monitor on worklist.
• Imaging staff• Stress Technologists
(Inpatient)
Need-to-Know Epic Benefits and Change Impacts
Non-Invasive Cardiology Snapshot
Epic Benefits
• Improve patient experience with efficient resulting and patient care workflows
• Streamline workflows between Cape Cod and Falmouth Hospital• Increase efficiency with automated charging for non-invasive procedures• Improve outpatient scheduling restrictions based on available resources• 3rd party resulting will appear as discrete results and PDF which will
ensure efficiency, productivity and flexibility • Improve transparency and consistency in patient care as patient chart will
be accessible to all users
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Non-Invasive Cardiology workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Service Line Current State Resulting System
Future State Resulting System
Echo, TEE, Echo Stress Xcelera XceleraNuclear Stress Cedars Cedars
Stress Print and Scan SmartText in EpicHolter/Events (CCH/25 Main) Preventice
(FH) BiotelSmartText in Epic
Vascular (CCH) Study Cast;(FH) PACS
Study Cast – Print and Scan
Cardioversions Dictation SmartText in EpicECGs Muse Muse
Last Updated: 9/1/202055

Level Current State Workflow Future State Workflow Impacted Roles
High Order sets are in multiple systems. It is a hybrid model where documentation process occurs on paper.
Massive Transfusion Protocol (MTP) and Blood Administration Workflows: Physicians and Nurses will follow the Mass Transfusion Protocol workflow and Blood Administration workflow (for non-MTP) to place orders.• For Massive Transfusion Protocol, Physicians will
need to place order set in Epic. Nursing will document in Mass Transfusion flowsheet and will not be required to scan the blood unit or have dual sign-off.
• For non-MTP Blood Adminstration workflows, there will be a seamless integration between SoftBank and Epic. There is an order to “Prepare Blood” and “Transfused Blood”, which are included in the blood transfusion order sets.
• Nurses• Physicians
High Clinical documentation for surgical clearance is tracked on paper.
Procedure Pass and Dynamic Pre-Procedure Protocols: Real time checklist helps to track what pieces of required clinical documentation are obtained and/or missing for each patient prior to the procedure (including consents, H&P, labs, tests, appointments, documents, anesthesia clearance, etc.).
• Perioperative Nurses• Surgeons• Floor Nurses• Anesthesia staff• PAT staff
High Paper consents are used for OR surgical consents.
E-Consents: E-Consents are used for OR surgical consents. Patients are able to sign consents with an iPad, and this ensures that consents are collected and attached to the patient's chart.
• Preoperative Nurses• Office staff• Surgeons
High Surgeons, Extenders, and Surgical Coordinators put booking requests in OR Manager.
Surgical Case Request: Surgeons, Extenders, PAs, NPs, and Surgical Coordinators utilizing Epic in their clinics, will use case request orders to generate procedural case requests electronically in Epic.
Surgeons not utilizing Epic in their clinics (or non-employed surgeons), will use Citrix to access Epic to place the case request order.
Surgical Coordinators can place the case request orders electronically in Epic but will still require cosign by the ordering physician.
• Surgeons• Surgeon offices• Physician Extenders,
PAs, NPs• Surgical Coordinators
High Surgical Coordinators can enter preoperative surgical orders in OR Manager.
Surgical Orders Placement: Only Surgeons, Extenders, PAs, and NPs are able to sign preoperative orders into Epic. Surgical Coordinators can pend preoperative orders in Epic for Surgeons, Extenders, PAs, and NPs to sign.
• Surgeons• Surgeon offices• Physician Extenders,
PAs, NPs• Surgical Coordinators
High PAT, Preoperative, PACU, Postoperative departments use paper for processes.
Integrated Electronic Medical Record System: PAT, Preoperative, PACU, Postoperative departments will move to one integrated system with intraoperative and the rest of the hospital.
• PAT staff• Preoperative Nurse• PACU Nurse• Postoperative Nurse
Need-to-Know Epic Benefits, Change Impacts, and New FunctionalitiesOpTime (Surgery) Snapshot (Page 1 of 2)
Epic Benefits
• Enhance patient engagement through reminders, questionnaires and real-time ‘Family Notifications’ on patient’s progress
• Improve patient safety and experience with e-consents
• Increase transparency and consistency in patient care with procedure pass and dynamic pre-procedure protocols
• Streamline disparate systems and processes with Epic’s Massive Transfusion Protocol, scheduling, and standardization of procedure lists
• Save time with e-consents, self-service reporting, and new processes in surgical case requests, orders placement, and specimen collection
• Track and improve OR efficiency, throughput, and utilization with perioperative core metric reporting and benchmarking
• Maximize resource efficiency with conflict checking capabilities
In one glance…You can find key exciting changes to the Surgery workflows brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 56

Level Current State Workflow Future State Workflow Impacted Roles
Medium Staff click “add on case” in OR Manager, print preference cards, and schedule directly with specific surgeon. Center Core then faxes alert to Preoperative, Postoperative, Sterile Processing Department (SPD), and Nursing Supervisor.
Trauma Case Scheduling: The Trauma Case button is used to schedule emergent cases, including emergency L&D, STEMI for CVPA and emergency procedures in the main OR. Intraoperative Nurse needs to retroactively update generic procedure and provider.
• OR Nursing• OR Scheduling
Medium Not using IMO. Procedures and Preference Cards: Procedure Lists are standardized through the third-party, IMO. More parameters are in place to ensure that procedures are booked with the correct patient class. Staff follow a new process in selecting from discrete procedure list.
• Schedulers• Preference card
builders• Surgeons, PA, NP
extenders who requests procedures
Medium Path specimens are on paper and entered into PowerPath. Double documentation is required in Soarian and on paper.
Specimen Collection Workflow: Intraoperative Nurse collects specimens and prints specimen labels and requisitions. Label printers will be available in each OR.
• Intraoperative Nurses• Lab staff
Low Scanning does not occur. Barcoding Supplies and Implants: Implants are scanned in with barcodes, but supplies are not.
• Intraoperative Nurses
Low No device integration in preoperative, PACU, and postoperative.
BMDI Vitals Monitors: There is device integration in preoperative and recovery departments.
• Recovery staff• Preoperative staff• Postoperative staff
Low Postoperative notes are written in Soarian and a few surgeons use dictation.
OpNotes: Surgeons use dictation (M*modal) and SmartTexts to write OpNotes.
• Surgeons
Need-to-Know Epic Benefits, Change Impacts, and New FunctionalitiesOpTime (Surgery) Snapshot (Page 2 of 2)
In one glance…You can find key exciting changes to the Surgery workflows brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
New Functionality brought on by Epic
OpTime Scheduling: For trauma and emergency cases (case classification A):• The surgical team will call the Center Core and Lead Anesthesiologist. • The Center Core or Nursing staff will use the ‘Trauma Case’ button to schedule the case on the Snapboard.
For add-on and urgent cases (case classifications B,C,D, and E):• Surgeons, Extenders, and PAs will electronically place the case request and verbally communicate to the Center Core and lead
anesthesiologist.• The Center Core or Nursing staff will schedule the case on the Snapboard.
Perioperative core metric reporting and benchmarking helps track and improve OR efficiency, throughput, and utilization. Featured KPIs include: volume, on-time starts, turnover, case length accuracy, cancellations, and utilization
SlicerDicer provides clinicians with self-service reporting tools without having to work with IT
Standardized CPT-based surgical procedure file automates Medicare Inpatient-only checks. Using IMO helps schedulers know which specific procedures will need to be scheduled as IP
Patients receive reminders of upcoming surgeries via text messages and submit electronic questionnaires. Family Notifications then keep the families up-to-date with patients’ progress updates. These keep patients engaged in their care from the day they find out they need surgery through their recovery period
Lab is able to see lab requisitions in Epic for pathology specimens coming from the ORs
Conflict checking capabilities allow users to understand the number of equipment, instruments and resources that are available at any given time to ensure smoother scheduling
Clinical documentation automatically drives charging
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
Last Updated: 9/1/202057

Level Current State Workflow Future State Workflow Impacted Roles
Medium Radiology RNs use paper for documentation.
Radiology Documentation: Radiology RNs use Radiant, Epic’s module for the Radiology department.
• Radiology Nurses
Low
Contracts and radiopharmaceutical administration information are documented on paper.
Contrasts and Radiopharmaceuticals: All contrasts and radiopharmaceutical administration information appear on the Medical Administration Record (MAR). Technologists administer contrast and document administration on the MAR. Technologists cannot end exams requiring contrast without documentation of the contrast medication on the MAR.
• Radiology Technologists
Low Protocolling occurs on paper. Protocolling: Technologists can protocol all CT exams and MRI exams without contrast in Epic. Radiologists can protocol MRI and CT. Nurses can protocol invasive exams (e.g., Guided Biopsies).
• Radiology Technologists• Radiologists • Radiology Nurses
Low • Contrasts are not ordered in an electronic system.
• If order changes, Techs need new order from the physician.
• Paper MRI screening form.• LDA/IV placement not documented.
Technologist Policy Changes: • Place an order for contrast per protocol in Epic.• Change an order within same procedure category without getting
a new order.• Use MRI-electronic screening form.• Document LDA/IV in Epic.
• Radiology Technologists
Low Need to reach out to PACS administrator to pull reports.
Reporting: Radiology staff are able to pull their own reports in Epic without outside assistance.
• Radiologists• Radiology Managers• Radiology Technologists• Radiology Nurses
Low Beginning and Ending Exams are not consistently documented in real time.
Beginning and Ending Exam: Beginning and Ending Exams are consistently practiced in real time.
• Radiology Technologists• Radiology Managers
Low CCHC documents radiation dose tracking in Radimetrics only.
Radiation Dose Tracking: CCHC double-documents radiation dose tracking in Radimetrics and Epic.
• Radiology Technologists
Low Both CCH and FH Radiologists perform wet reads in Primordial. However, FH Radiologists always perform wet reads on XR exams, and CCH EC doctors do not perform wet reads.
Discrepancy Tracking: Radiologists across CCHC will perform wet reads.FH: Radiologists perform wet reads in Epic.CCH: Radiologists perform wet reads in Primordial.
• Radiologists
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Radiant (Radiology) Snapshot
Epic Benefits
• Improve patient safety with consistent, accurate, and legible electronic documentation, medication allergy warnings, and contrast medication prompts
• Enhance patient experience by ensuring information is tied to the patient’s chart and carried forward to subsequent encounters
• Enhance interdisciplinary coordination and communication with “Needs Anesthesia” notifications, conflict checking for Physicians
• Save time with electronic documentation, new policies, and Radiology Decision Support with Appropriate Use Criteria (AUC) per regulations
• Track and report metrics easily with self-service reporting, radiation dose tracking, and discrepancy tracking with wet reads
• Ensure accurate and consistent information on patient’s chart with integrations
In one glance…You can find key exciting changes to the Radiology workflow brought about by the new Epic EHR, and how they will improve yourday-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
New Functionality brought on by Epic
Appropriate Use Criteria (AUC) per regulations: Cape Cod Healthcare has a contract with National Decision Support Company (NDSC) for their CareSelect product to provide decision support based on appropriate use criteria for Radiology OrdersRadiologists can use default SmartText to complete post-procedure notes in Epic as an option, but not as a requirement. Radiologists can also result studies in PowerscribeMarking the Radiology procedure as “needs anesthesia” will automatically notify the Anesthesia Team that the patient needs anesthesia for a procedure and will perform conflict checking
MRI Screening Form logs implants and checks for “MRI safety”. Implants stay with the patient and pull forward to subsequent encounters
Radiology exams that require contrast will prompt users to administer contrast, thereby ensuring all procedures with contrast have the appropriate contrast medication administered
Lab ordering and resulting will be integrated into the patient’s chart and Radiology staff’s workflows
Medication, allergies, history is consistent, no double documentation, and will integrate into patient’s chart
Conflict checking available for Physician resources in CVPA and Radiology
Medication warnings are available for patients with allergies
Improve legibility of documentation for workflows with transition from paper to electronic
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 58
Epic Module/Areas
Front End
59

Level Current State Workflow Future State Workflow Impacted Roles
High CCHC uses a mix of central and decentralized scheduling across the enterprise:• CCH and FH maintain independent central
scheduling teams for select services at each facility. Other services are scheduled by the departments.
• Centralized scheduling teams have separate collective bargaining agreements, but there is a clause that allows the redistribution of work across the teams, based on scheduling volumes and needs across facilities.
• MACC is decentralized and department owned.
Centralized Scheduling: All of CCHC has standardized Epic scheduling functionality and configuration options, but scheduling will remain decentralized in certain areas. • CCH, FH, and MACC Schedulers are
considered CCHC Central Schedulers, fully centralizing the scheduling of hospital-based services.
• This standardizes the CCH and FH workflows, allowing CCH and FH Central Schedulers to book appointments across facilities.
• Physician practice scheduling, Cuda, IVT (Falmouth only) remain decentralized.
• Scheduling Staff• Financial Clearance
Analysts
Medium National Provider Identifier (NPI) is an additional data field in Soarian - if a Provider is not in the system workflow, a ticket is submitted to IT who then creates a provider record.
Provider on the Fly: CCHC IT verifies that the National Provider Identifier (NPI) entered in Epic is not a duplicate or inaccurate.• End users can quickly create a shell provider
record to schedule with. Users can access Provider on the Fly and create an SER record directly in referral entry or registration.
• The unverified provider report is used to verify that SER records have correct information/NPI.
• NPI Record is a required field.
• Scheduling Staff• Referral Coordinators• Lab / Radiology• Front Desk• CCHC IT
Low Physicians do not schedule appointments. Schedulable Orders: Physicians use OrderUp to directly schedule an appointment for orders that do not require a prior authorization.
• Physicians• Any role responsible
for WQ monitoring
Low Interpreters are requested outside of system and a generic interpreter resource is scheduled.
Interpreter Scheduling: Patient is marked as needing an interpreter during registration. This request is automatically routed to a worklist for interpreters to be scheduled to the appointment.
If a request for an interpreter needs to be entered after the initial appointment scheduling, scheduler must call interpreter services.
• Interpreters• Scheduling Staff• Registration Staff
Low CCHC has many client accounts in Soarian that do not have unique service agreements and are billed at ~110% Medicare.
CCHC experiences instances where the patient’s client account is not already entered into the system. Thus, registration staff create new client accounts “on the fly” in order to have this entered into the system.
Client Billing: Registration users will leverage a prompt to add an activity (and client information) that will route encounters for billing review and client creation when new accounts are identified.
This allows CCHC to continue the practice of adding non-existing client accounts but will create guardrails to support back-end approval and streamline communication between registration and billing staff.
• Registration Staff • Billing staff
Need-to-Know Epic Benefits and Change Impacts
Cadence Scheduling Snapshot
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Cadence Scheduling workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Epic Benefits
• Improve patient experience when scheduling appointments
• Access accurate and complete scheduling information
• Streamline communication between registration and billing staff when adding non-existing client accounts
• Reduce administrative burden and inconsistencies by centralizing scheduling workflows across CCHC
• Minimize inefficiencies with Provider on the Fly and OrderUp scheduling functionality
• Seamless interpreter scheduling with automated worklist • Expedite new patient creation during scheduling
Last Updated: 9/1/2020 60

Level Current State Workflow Future State Workflow Impacted Roles
High • Patient Access is involved in the bed planning process.
• Tablets are not used. • After an admitting order prints,
staff call the Nurse Manager for bed planning.
Bed Planning in Epic: • Nursing oversees bed planning directly and Patient Access
will no longer be involved in the process. • Bed planners use tablets. • Orders are automated in Epic, which automatically generates
requests to Nurse Managers.
• Nurses (Manager, Supervisor)
• Patient Access (no longer involved)
Medium Hospital admitting staff directly admits patients.
Direct Admits: Hospital admitting staff are only responsible for completing the registration requirements at point of the patient's arrival. Nursing or Clerical Staff on the inpatient floors will complete the direct admit as part of the patient's arrival.
The admit time for a direct admit will reflect the instant that the Nursing or Clerical Staff on the floors takes the patient into their bed.
• Nurses (Manager, Supervisor)
• Clerical staff• Registration Staff
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Grand Central (ADT, Bed Planning) Snapshot
Epic Benefits
• Improve patient safety as patient movements and cleaning requests are promptly accounted for
• Enhance patients’ caregivers’ satisfaction as a result of accurate patient information
• Manage patient movements accurately and efficiently through automated tracking from arrival, to movements inside the hospital, to departure
• Organize EVS cleaning requests efficiently with EVS Manager, and new tracking and reporting capabilities displayed on monitors, tablets, and mobile devices
• Enhance care coordination and communication with system notifications, Unit Manager status updates, and notifications
• Save time with automatic bed charge drops and bed planning suggestions
In one glance…You can find key exciting changes to the Admission/Discharge/Transfer (ADT) and Bed Planning workflows brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
New Functionality brought on by Epic
Unit Managers provide an easy and integrated look at the system. Patient Location, Leave of Absence, Transfer/Discharge Orders, and EVS bed status are all visible for Nursing.
In the Unit Manager, if the patient is brought to another floor or unit, the system automatically updates their location. Upon return to the patient’s bed, the Nurse or Unit Clerk can mark them as "back in bed.”
Bed Planning automatically suggests beds for the patient based on their unique combination of patient class, level of care, and clinical service.
Automatic Bed Charges drop based on patient class, level of care, accommodation code.
EVS cleaning requests are automatically created for discharges and assigned to the next available housekeeper. EVS Manager makes it easy for supervisors to monitor, create, and reassign cleaning requests if needed.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/11/202061
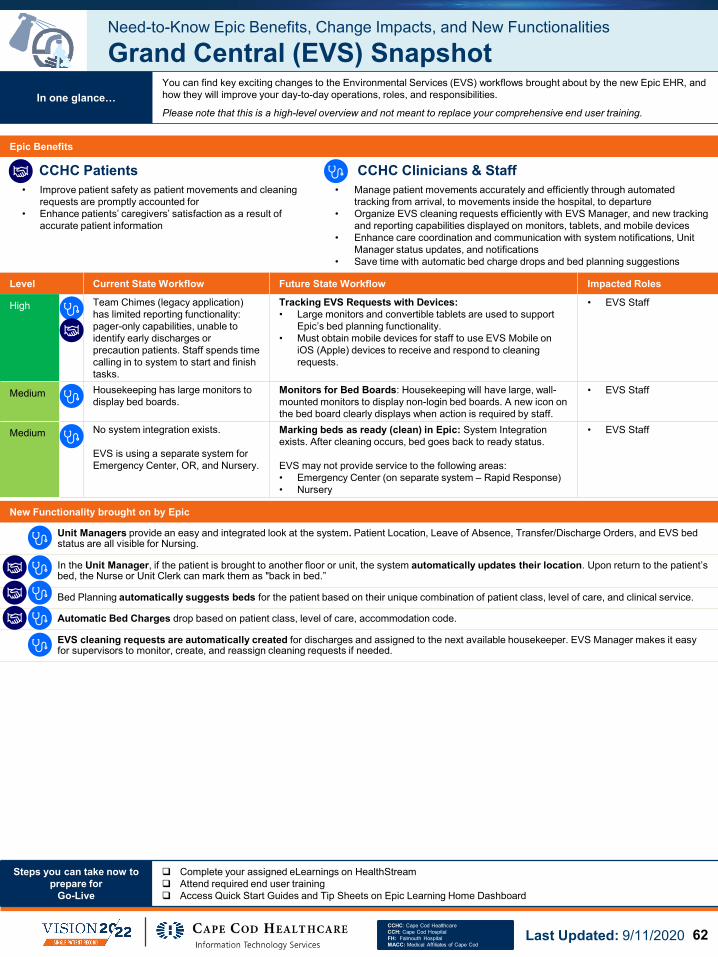
Level Current State Workflow Future State Workflow Impacted Roles
High Team Chimes (legacy application) has limited reporting functionality: pager-only capabilities, unable to identify early discharges or precaution patients. Staff spends time calling in to system to start and finish tasks.
Tracking EVS Requests with Devices:• Large monitors and convertible tablets are used to support
Epic’s bed planning functionality.• Must obtain mobile devices for staff to use EVS Mobile on
iOS (Apple) devices to receive and respond to cleaning requests.
• EVS Staff
Medium Housekeeping has large monitors to display bed boards.
Monitors for Bed Boards: Housekeeping will have large, wall-mounted monitors to display non-login bed boards. A new icon on the bed board clearly displays when action is required by staff.
• EVS Staff
Medium No system integration exists.
EVS is using a separate system for Emergency Center, OR, and Nursery.
Marking beds as ready (clean) in Epic: System Integration exists. After cleaning occurs, bed goes back to ready status.
EVS may not provide service to the following areas:• Emergency Center (on separate system – Rapid Response)• Nursery
• EVS Staff
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Grand Central (EVS) Snapshot
Epic Benefits
• Improve patient safety as patient movements and cleaning requests are promptly accounted for
• Enhance patients’ caregivers’ satisfaction as a result of accurate patient information
• Manage patient movements accurately and efficiently through automated tracking from arrival, to movements inside the hospital, to departure
• Organize EVS cleaning requests efficiently with EVS Manager, and new tracking and reporting capabilities displayed on monitors, tablets, and mobile devices
• Enhance care coordination and communication with system notifications, Unit Manager status updates, and notifications
• Save time with automatic bed charge drops and bed planning suggestions
In one glance…You can find key exciting changes to the Environmental Services (EVS) workflows brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
New Functionality brought on by Epic
Unit Managers provide an easy and integrated look at the system. Patient Location, Leave of Absence, Transfer/Discharge Orders, and EVS bed status are all visible for Nursing.
In the Unit Manager, if the patient is brought to another floor or unit, the system automatically updates their location. Upon return to the patient’s bed, the Nurse or Unit Clerk can mark them as "back in bed.”
Bed Planning automatically suggests beds for the patient based on their unique combination of patient class, level of care, and clinical service.
Automatic Bed Charges drop based on patient class, level of care, accommodation code.
EVS cleaning requests are automatically created for discharges and assigned to the next available housekeeper. EVS Manager makes it easy for supervisors to monitor, create, and reassign cleaning requests if needed.
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/11/2020 62

Level Current State Workflow Future State Workflow Impacted Roles
High Interventional Radiology/Cardiology outsources coding of charges to ZHealth.
A report with associated documentation is generated from Soarian and sent to ZHealth. ZHealth codes charges and returns the document to CCHC where it is uploaded into Soarian again.
ZHealth: Hospital charges are entered into Epic. Epic extracts and then sends accounts to ZHealth. HB charges are manually typed into the system by coders. Incoming professional charges are created through a charge interface.
• HIM Data Clerk
HighEC coding information is entered directly into 3M by Logix.
Logix: Logix will supply coding information via a file that will be interfaced into Epic to complete coding for EC accounts.
• HIM Director
HighInpatient and Ambulatory chart corrections and MPI management are performed by different owners in a decentralized process. • For inpatient, the HIM department currently
performs chart corrections. They receive approximately 65 correction requests in Soarian per week, resulting in an estimated work effort of 5 hours per week.
• The HIM department also processes approximately 50 inpatient Patient Portal sign-up requests per week, and an additional 10 emails or call from patients, resulting in an estimated effort of 8 hours per week.
• The HIM department does not handle ambulatory chart corrections.
Centralized Master Patient Index (MPI) Management: Chart correction and MPI management are centralized and are managed by HIM, including processing authorizations and maintenance for Care Everywhere.
There will be new responsibilities, such as:• Handling duplicates from the RME • Handling both inpatient and outpatient chart correction
• HIM Staff• MPI Staff
MediumLogix provides CCHC with Request for Additional Information (RAI) reports. Users work those reports to follow-up on EC documentation.
EC Follow-Up Process: Users following up on EC documentation will leverage Epic tools to track status and communicate with Physicians.
• Data Clerk• EC Physicians
MediumCDI staff does querying of Physicians and will alert coding staff when the appropriate response is received, which will allow the account to be coded.
Query Process: Post-discharge processes for physicians. CDI / Coding query processes are a change from current state. Physician process for interacting with the query will change in accordance with CCHC policy.
• Coders• CDI staff• Physicians
Low Coders and outside parties split responsibility for entering charges. Coders are working outside of the system to do this process in current state. Coders have ability to drop charges.
Missing Charge Workflow: Coders will now have a process to follow when sending accounts to Revenue Integrity if additional charges are needed. Coders will be sending information to Revenue Integrity to drop charges.
• HIM Coders
Low Soarian Financials calculates DRG during the billing process, and coders do not interact with DRG.
DRG Calculation: DRG flows into Epic from 3M, and the appropriate reimbursement data is applied at that time. The contract engine will calculate the reimbursement.
• Coders
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Health Information Management (HIM) Snapshot
Epic Benefits
• Improve patient experience by releasing patient records to MyChart
• Reduce administrative burden and inconsistencies via streamlined workqueues to help staff reconcile duplicate records based on upcoming visits and manage chart corrections
• Improve operational efficiency through integration between Deficiency Tracking and Hospital Coding
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Health Information Management workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020
New Functionality brought on by Epic
Integration between Deficiency Tracking and Hospital Coding to identify where dollars are being help up due to missing documentation
Ability to release patient records directly to a patient portal via MyChart
Streamlined workqueues to help staff reconcile duplicate records based on upcoming visits and manage chart corrections
63

Need-to-Know Epic Benefits and Change Impacts
Prelude (Registration) Snapshot (Page 1 of 2)
Epic Benefits
• Improve patient experience with expedited registration process, including electronic signatures and patient access photographs
• Reduce prior-authorization redundancies • Enhance and expedite provider registration via system workflow capabilities
allowing for “on the fly” provider registration• Leverage Epic as the sole source of truth for demographic data, guarantors,
authorization, and coverage creation
In one glance…You can find key exciting changes to the Registration workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
Level Current State Workflow Future State Workflow Impacted RolesHigh Financial clearance and insurance verification
responsibilities for the hospitals are performed by the FCC for centrally scheduled services.
The physician practices are only partially centralized within CCHC and have some duplicative professional service authorization processes with the FCC.
Centralized Financial Clearance and Insurance Verification Responsibilities: Transition centralized responsibilities to the hospital Financial Clearance Center (FCC). CCHC will maintain on-site registration staff, but:• Reduce financial clearance responsibility
overlaps with the FCC.• Perform verification for existing patients through
on-site staff via RTE as part of registration pathway.
• Transfer insurance verification for new patients to FCC.
• Standardize key processes/functions such as insurance verification, medical necessity checks, and authorizations.
• Hospital staff • Physicians
(involved in financial clearance)
• Financial Clearance Analyst
High Inpatient: e-sign pads in use in some areas,:• In the EC, registrars do not use e-sign pads and
must use paper copies of all forms.• In the EC triage area, e-sign pads are available but
not in use due to non-operable condition.• In CCH (Financial Counselors, SDC, PAT, Cashier
Coordinator, and Urgent Care) and FH (WI, Faxon, Rad, NF, Cardio), Topaz e-sign pads are in use.
Outpatient: e-sign pads are not in-use. Front desk staff have patients sign paper copies of all forms and manually scan them into the patient record in eCW.
Patient Access Electronic Signatures: • Use e-sign pads across CCHC (both Inpatient
and Outpatient) to capture signatures and enable electronic document types for registration.
• An electronic consent form is used with either Welcome Kiosks or iPads.
• Allows staff to leverage electronic document signature capabilities in Epic, while reducing paper and scanning costs.
• Reduces the likelihood of misplacing a signed document and gives all users defined areas within the chart where they can view signed documents.
• Registration staff• Admitting
High Inpatient: Photographs are only used in the CCH (EC) and FH (Faxon), but not in the rest of CCH and FH departments. CCH EC uses costly, outdated film camera. Photos are obtained when patient does not have any type of photo ID. Webcams are only in use at FH Faxon.Outpatient: Patient access photographs are used in the Emerald PCP practices. The rest of our Emerald and MACC PCP and Specialty practices do not use photographs. Emerald PCPs use Microsoft LifeCam HD and Logitech webcams to take patient photos at check-in and upload into eCW.
Patient Access Photographs: Expanded use of photos and update hardware across CCHC (both inpatient and outpatient).• Hardware to support registration photo workflows
in specified CCH and FH registration areas.• Devices at registration desks to take patient
photos have 1:1 PC to unit ratio.
• Registration staff • Front Desk
High Registration staff in the CCH and FH EC are printing facesheets and writing on hardcopy at bedside before going back to desk station to enter information into patient record. • Staff must return to desk station after gathering
registration information makes this an inefficient process
• To gain efficiency, staff are taking paper documentation from one patient and run it to another room before returning to desk station, which presents an opportunity to improve patient safety by collecting electronically
• CCH EC does not have WoWs. FH EC has one WoW that is not in use, and would need peripherals
Patient Access Emergency Department Registration: Use Workstation on Wheels (WoWs) to register patients electronically. • WoWs would be used at the CCH and FH EC.
Peripherals would include webcam, e-sign pad, credit card reader and scanner. Use 1:1 staff to WoW ratio.
• EC Registrar finish registrations face-to-face with patient when entering information into Epic.
• WoW hardware would improve patient safety by replacing inefficient process, and gets all patients registered who bypasses front desk with a more efficient workflow.
• EC Registration staff
• Front Desk
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 64

Need-to-Know Epic Benefits and Change Impacts
Prelude (Registration) Snapshot (Page 2 of 2)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Registration workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
Level Current State Workflow Future State Workflow Impacted Roles
High Some legacy system patient-guarantor relationships were not converted to Epic.
Guarantor Auto-Generator: The system will auto-generate guarantors for all patients over the age of 18 to “self” at the point of opening registration. Staff may need to verify or update guarantor for all patients upon first check in or registration.
• Patients• Registration Staff
High No unified policy for registration to work their own edits when claim fails. Managers export worklists and email them to staff. Some staff did work directly off EBEW (Encountered Billing Exception Worklists).
Edit Workqueues (WQs): Back-end edits are moved to front-end where registration areas are responsible for their own errors.All in Epic (no exporting).
• Registration
Medium “Worklist” verbiage is used. WQs are not a concept in legacy.
Referrals Workqueues (WQs): Workqueue verbiage is used. Referral coordination significantly changes expectation at go-live for some areas. One WQ for authorization and by department.
• Referral Coordinator• Ambulatory front desk
staff• Scheduling Analysts
Medium Payments not taken at POS for some areas. Payment Collection: Every department will be collecting front-end payments, including collecting any prior balances. Pre-payments are new in future state.
• Front-End/POS• Payment Coordinator
Low There is no verification within the system for past eligibility.
Coverage Changes: In instances where coverage changes on the guarantor account for users, there is a time period that the system will review scheduled patients with coverage changes every 30 days.
• Registration
Low Similar to Epic functionality. New Restrictions: Restricts users from being able to assign coverages that aren’t on the guarantor account.
• Registration
Low Compliance has no enterprise-wide standard for unknown demographic data.
New processes for unknown demographic data: • For unknown address:
Homeless123 No Name St.Homeless, MA.
• For unknown/no SSN, use 999-99-9999• For patients who refuse to give social, use 000-00-
0000• For unknown Phone #, use (000) 000-0000
• Registration
Low Confidential guarantor not used in legacy. Confidential Accounts: Patients are allowed to request separate accounts (and statements) for confidential visits, which will carve out charges to a separate guarantor and a separate statement processing.
• Patients• Registration• Schedulers• Admitting
Low Providers order without checking for medical necessity. In these situations, CCHC prepares ABN, drives it to a worklist for registration, then manually prints it, has patient sign, and then sends to next workqueue for coding to add a modifier.
Advanced Beneficiary Notices (ABNs) and Medical Necessity Checks: In any case where an order is placed for a procedure with a diagnosis combination that isn't defined as medically necessary, providers will see an ABN notification that they can review with the patient. The system prompts to check for medical necessity at the appropriate times. ABNs fire at order entry, check-in, and check-out. If the provider doesn't review, it will be flagged for follow up by front-end staff. At check-in, printing is required as e-sign will not be used.
• Providers• Front Desk
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202065

Level Current State Workflow Future State Workflow Impacted Roles
High Patient registration is completed at the front desk face-to-face with a CCHC staff member.
Welcome Kiosks: Patients can fully register for their encounter at self-service, electronic kiosks.
• Desk Staff• Cancer Center• Yarmouth Primary
Care• FH only – Volunteers• Patients
Low Consent for treatment forms are on paper. Welcome eConsent: An electronic consent form is used.
• Desk Staff• Patients
Need-to-Know Epic Benefits and Change Impacts
Welcome (Patient Kiosk) Snapshot
Epic Benefits
• Improve patient experience and efficiency by providing digital self-service options
• Reduce administrative burden by transitioning from paper consents to electronic for treatment forms
• Saves time by facilitating patient self-service
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the patient check-in workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 66

Epic Module/Areas
Billing
67

Level Current State Workflow Future State Workflow Impacted Roles
Medium Legacy financial class definitions are in need of improvement.
Financial Class Changes (Reporting): Staff will utilize new financial classes and payer / plan mappings. Refer to the Payer Plan Crosswalkfor specifics. The new-to-Epic Benefit Plan groups that align with CCHC legacy system's categorizations will be available in both the Transactions and Accounts data models in SlicerDicer to assist with reporting questions.
• Reimbursement• Physician group• Human Services• Revenue Cycle
(Optum)
Medium For joint venture accounts (Radiation Therapy / MRI), manual reports are run to identify the data.
General Ledger (GL) Structure Changes: Joint Venture accounts no longer require separate manual reports. New Epic GL accounts are being created and will need to be managed concurrently as legacy accounts are worked down.
• Reimbursement
Medium Finance Reporting processes exist that require significant manual manipulation and setup.
Automated Finance Reporting Changes: Reports will be written and automated in Epic. A small degree of manual report manipulation is required, such as looking up patient accounts. Note: Some areas are not going live with Epic and therefore will follow current state processes for reporting:• Nauset Family Practice• Orleans Medical• Cape Cod Dermatology• Southeastern Surgical Associates
• Reimbursement• Physician group• Human Services• Revenue Cycle
(Optum)
Low AR codes are not standardized and some duplication exists.
Accounts Receivable (AR) Code Changes: AR Codes have been cleaned up and standardized to more efficiently and accurately manage outstanding AR (click here to access the file).
• Reimbursement• Physician group• Human Services• Revenue Cycle
(Optum)
New Functionality brought on by Epic
Reduce one-off manual reporting process for Optum based on Current Procedural Terminology (CPT) and through the introduction of new visit classifications and reporting structure and processes in Epic. This will enable for PB Finance to report on net-per-visit and RVU
Leverage the largely automated PB General Ledger (GL) Integration for eCW (Reporting Software)
Gain access to immense reporting capabilities through a self-service module linked to MS Excel
Remove the need for monthly journal entries from eCW to PeopleSoft with the new Epic GL interface
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Finance Snapshot
Epic Benefits
• Streamline the patient registration process by capturing accurate insurance plan information with new financial classes and payer/plan mappings
• Automate financial reporting through the PB General Ledger (GL) Integration for eCW (Reporting Software)
• Streamline new financial classes and payer/plan mappings for reporting purposes
• Minimize manual report manipulation and creation by automating financial reporting changes, including GL structure reporting and visit classifications
• Remove duplication and data inconsistencies with AR code clean-up• Leverage new reporting capabilities with self-service module linked to MS
Excel
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Finance workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 68

Level Current State Workflow Future State Workflow Impacted Roles
High Users are manually reviewing claims attachments.
Manual Review of Claims Attachments (Temporary): For the first two weeks after Go-Live, there will be a manual review of the claim attachments. The claims attachments will route to a workqueue. After the first two weeks of Go-Live, review of claim attachments will become automated, where appropraite
• AR Follow up Supervisors
• Hospital Billers
Medium Pending follow up. RMC Updates Thread: The CCHC IT team monitors the RMC Updates thread on the Epic UserWeb for updates to Claim Adjustment Reason Codes (CARC) and Remittance Advice Remark Codes (RARC), and will build these out in the system as they are released.Once IT makes an adjustment or creates a new code, they ensure that it is mapped and notification is sent to the HB and PB operations groups.
• CCHC IT• Rev Cycle Operations
Medium Paper claims are printed overnight out of the clearing house for payers that do not accept electronic claims.
Paper Claims Printing: Billing staff will print the paper claims directly from Epic in the workqueue the morning after. During the day, staff manually print out demands, appeals, and attachments.
Note: Claims with attachments will go to a workqueue for the first few weeks so they can be manually reviewed. Non-attachment paper claims should print automatically overnight.
• Billing staff
Medium Exceptions are not contained within the system.
Claims Eligibility Table: Users will need to maintain the Claims Eligibility Table in Epic to manage exceptions for Provider Credentialing and Enrollment.
• Optum• Rev Cycle Operations
Low • There is a hard stop associated with Appeal, Normal Claim Pay, and Claim Max Days.
• The system is not reporting on lowest amount of time to file.
• HB/PB utilizes Timely Filing workqueues and own policy document.
Appeals, Normal Claims Pay, and Claims Max Days: • For the Appeals, Normal Claim Pay, and Claim Max Days, there
will be max days for each payer that will need to be communicated to users who are filing the appeals. There will be standardized language and a lower limit of changes.
• New synonyms have been added to the current list of payers within Epic.
• Insurance follow-up will have a max day to appeal.• Normal Claim Pay and Claim Max Days for users will route to a
workqueue.• Supervisors and Managers can leverage a workqueue column to
determine the Max Days (Days / Time to file).
• HB and PB Billing staff• Follow-up staff
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Resolute Claims / Remittance (Page 1 of 2)
Epic Benefits
• Improve patient experience through more seamless, accurate, and error free claims processes
• Leverage Epic workqueue functionality to integrate automation into claims review process, including the automatic generation of claims attachments
• Remove the need to wait a full day for nightly processing and more quickly determine whether external claim errors have been resolved
In one glance…You can find key exciting changes to the Claims / Remittance workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202069
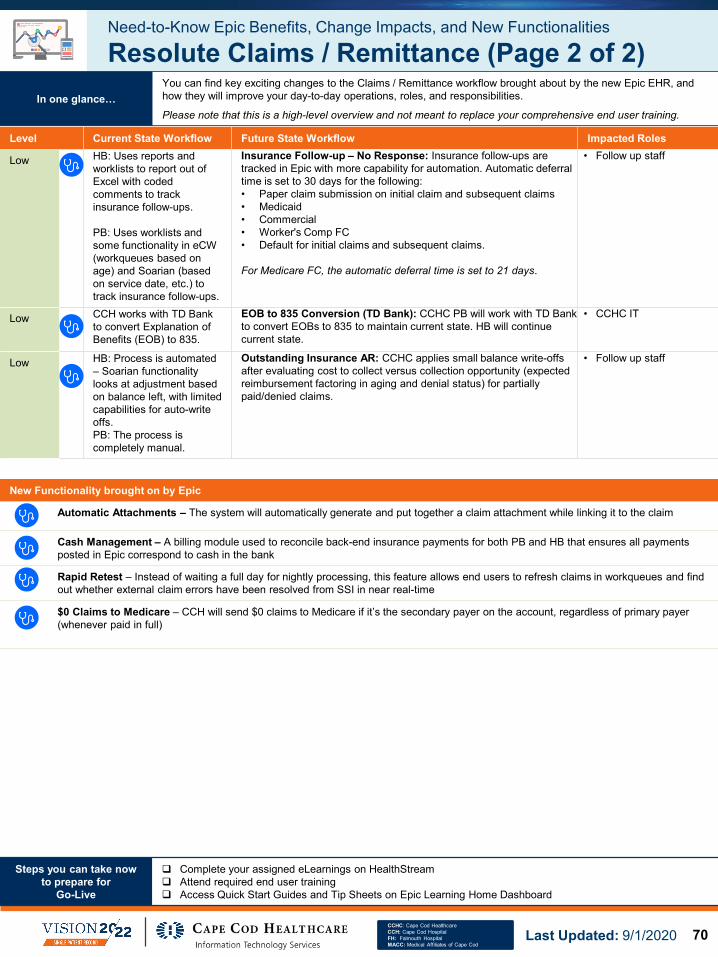
Level Current State Workflow Future State Workflow Impacted Roles
Low HB: Uses reports and worklists to report out of Excel with coded comments to track insurance follow-ups.
PB: Uses worklists and some functionality in eCW (workqueues based on age) and Soarian (based on service date, etc.) to track insurance follow-ups.
Insurance Follow-up – No Response: Insurance follow-ups are tracked in Epic with more capability for automation. Automatic deferral time is set to 30 days for the following:• Paper claim submission on initial claim and subsequent claims• Medicaid• Commercial• Worker's Comp FC• Default for initial claims and subsequent claims.
For Medicare FC, the automatic deferral time is set to 21 days.
• Follow up staff
Low CCH works with TD Bank to convert Explanation of Benefits (EOB) to 835.
EOB to 835 Conversion (TD Bank): CCHC PB will work with TD Bank to convert EOBs to 835 to maintain current state. HB will continue current state.
• CCHC IT
Low HB: Process is automated – Soarian functionality looks at adjustment based on balance left, with limited capabilities for auto-write offs.PB: The process is completely manual.
Outstanding Insurance AR: CCHC applies small balance write-offs after evaluating cost to collect versus collection opportunity (expected reimbursement factoring in aging and denial status) for partially paid/denied claims.
• Follow up staff
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Resolute Claims / Remittance (Page 2 of 2)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Claims / Remittance workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
New Functionality brought on by Epic
Automatic Attachments – The system will automatically generate and put together a claim attachment while linking it to the claim
Cash Management – A billing module used to reconcile back-end insurance payments for both PB and HB that ensures all payments posted in Epic correspond to cash in the bank
Rapid Retest – Instead of waiting a full day for nightly processing, this feature allows end users to refresh claims in workqueues and find out whether external claim errors have been resolved from SSI in near real-time
$0 Claims to Medicare – CCH will send $0 claims to Medicare if it’s the secondary payer on the account, regardless of primary payer (whenever paid in full)
Last Updated: 9/1/2020 70
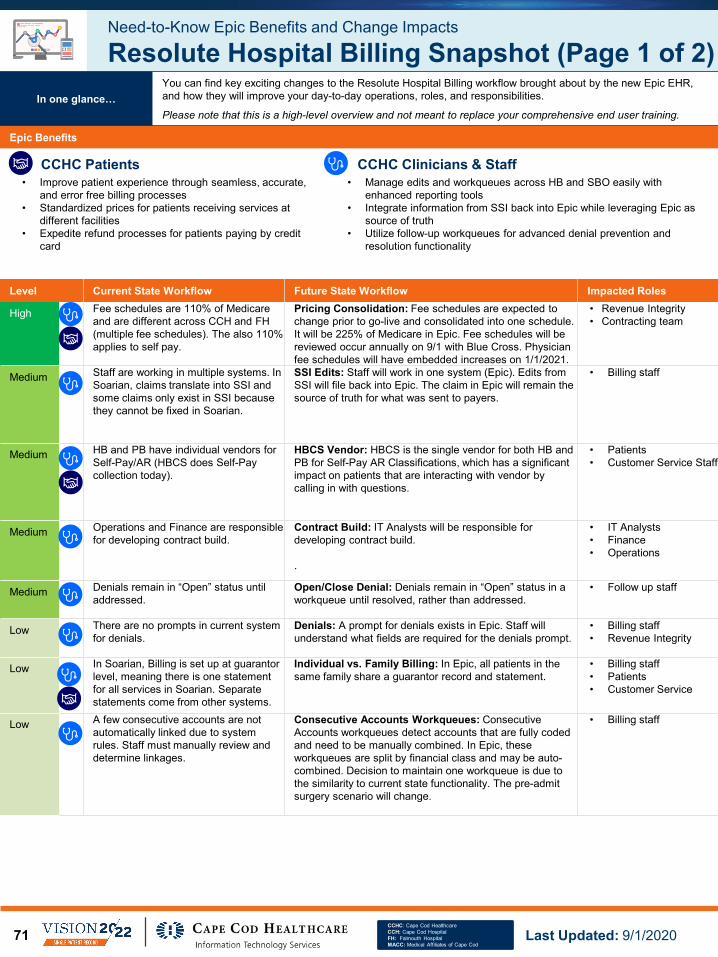
Level Current State Workflow Future State Workflow Impacted Roles
High Fee schedules are 110% of Medicare and are different across CCH and FH (multiple fee schedules). The also 110% applies to self pay.
Pricing Consolidation: Fee schedules are expected to change prior to go-live and consolidated into one schedule. It will be 225% of Medicare in Epic. Fee schedules will be reviewed occur annually on 9/1 with Blue Cross. Physician fee schedules will have embedded increases on 1/1/2021.
• Revenue Integrity• Contracting team
Medium Staff are working in multiple systems. In Soarian, claims translate into SSI and some claims only exist in SSI because they cannot be fixed in Soarian.
SSI Edits: Staff will work in one system (Epic). Edits from SSI will file back into Epic. The claim in Epic will remain the source of truth for what was sent to payers.
• Billing staff
Medium HB and PB have individual vendors for Self-Pay/AR (HBCS does Self-Pay collection today).
HBCS Vendor: HBCS is the single vendor for both HB and PB for Self-Pay AR Classifications, which has a significant impact on patients that are interacting with vendor by calling in with questions.
• Patients• Customer Service Staff
Medium Operations and Finance are responsible for developing contract build.
Contract Build: IT Analysts will be responsible for developing contract build.
.
• IT Analysts• Finance• Operations
Medium Denials remain in “Open” status until addressed.
Open/Close Denial: Denials remain in “Open” status in a workqueue until resolved, rather than addressed.
• Follow up staff
Low There are no prompts in current system for denials.
Denials: A prompt for denials exists in Epic. Staff will understand what fields are required for the denials prompt.
• Billing staff• Revenue Integrity
Low In Soarian, Billing is set up at guarantor level, meaning there is one statement for all services in Soarian. Separate statements come from other systems.
Individual vs. Family Billing: In Epic, all patients in the same family share a guarantor record and statement.
• Billing staff• Patients• Customer Service
Low A few consecutive accounts are not automatically linked due to system rules. Staff must manually review and determine linkages.
Consecutive Accounts Workqueues: Consecutive Accounts workqueues detect accounts that are fully coded and need to be manually combined. In Epic, these workqueues are split by financial class and may be auto-combined. Decision to maintain one workqueue is due to the similarity to current state functionality. The pre-admit surgery scenario will change.
• Billing staff
Need-to-Know Epic Benefits and Change Impacts
Resolute Hospital Billing Snapshot (Page 1 of 2)
Epic Benefits
• Improve patient experience through seamless, accurate, and error free billing processes
• Standardized prices for patients receiving services at different facilities
• Expedite refund processes for patients paying by credit card
• Manage edits and workqueues across HB and SBO easily with enhanced reporting tools
• Integrate information from SSI back into Epic while leveraging Epic as source of truth
• Utilize follow-up workqueues for advanced denial prevention and resolution functionality
In one glance…You can find key exciting changes to the Resolute Hospital Billing workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202071

Level Current State Workflow Future State Workflow Impacted Roles
Low Manual follow up is required for AR workqueues and denial workqueues.
Follow-up Workqueues: Epic follow-up workqueues provide advanced, automated denial prevention and resolution functionality.
• Billing staff• Follow up staff
Low Third party billing is set up byRegistration / Revenue Cycle to add parties on the fly.
Third Party Billing: There are three primary types of third-party billing in Epic, each with its own unique setup: corporate, client, and institutional. The appropriate category for each third party billed will be according to the Third Party Billing Matrix. Registration can add specialty billing accounts by submitting new ticket to IT to add new client third party.
Note: Registration will no longer be able to add parties; a representative from operations will be able to review client accounts. Add/modify actions will be conducted by IT.
• Registration• IT• Revenue Cycle
Analysts
Low Both Soarian and HBCS are utilized
Self-Pay Follow-Up: HBCS will be working in Epic/own system in order to properly accommodate workflow, but similar to what is being done today.
• HBCS staff
Low There is no process to maintain payment and adjustment code list across PB and HB.
Payment Adjustment Code Master List: Legacy payment adjustment codes have been mapped to Epic codes. There will be a change control process to maintain payment and adjustment code list across PB and HB. (click here to access the file).
• Denials• IT• Finance• Rev Cycle
Need-to-Know Epic Benefits and Change Impacts
Resolute Hospital Billing Snapshot (Page 2 of 2)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Resolute Hospital Billing workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/2020 72

Level Current State Workflow Future State Workflow Impacted Roles
High Fee schedules are 110% of Medicare and are different across CCH and FH (multiple fee schedules). The also 110% applies to self pay.
Pricing Consolidation: Fee schedules are expected to change prior to go-live and consolidated into one schedule. It will be 225% of Medicare in Epic. Fee schedules will be reviewed annually on 9/1 with Blue Cross. Physician fee schedules will have embedded increases on 1/1/2021.
• Revenue Integrity• Contracting team
Medium CCHC only bills for employed providers. Optum team must manipulate claims for certain payers in a highly manual process that often involves losing information in translation.
OR Charging - Mashpee ASC: CCHC will also bill for non-employed providers in addition to employed providers. There will be new coders, a new process, and changes to format / requirement of claims.
• Coding• PB Billing
Low Optum manages customer service for MACC and CCHC Physicians. In Soarian, HBCS manages patient balances and does not manage PB customer service.
Credit breakouts between Optum and HBCS: HBCS will be responsible for both HB and PB self-pay AR. Optum will continue to manage PB insurance credits.
• Patients• Call Center Staff• Optum
New Functionality brought on by Epic
Reference detailed plans, goals, and metrics for legacy AR reduction for both Pre- and Post-Live AR (Soarian, CCHP/MACC eCW) will be leveraged so AR follow-up staff can more quickly transition to Epic accounts. Four systems will be used at time of 11/1 Go-Live
Process for collecting ABNs requires workflow changes from legacy for both billing and clinical workflows; in addition to fee schedule, charge/modifier, claims, and reporting build
New field requirements for the denials prompt as there are three different screens. In the Appeal section, there will be training to understand which fields are required
Enhance denial prevention and resolution functionality through Epic follow-up workqueues
Save costs on refunds processing and credit card fees when refunding patients through credit card integration
Epic charge review workqueues will provide the physician’s note and documentation in line with the charge view for coding and charge error resolution
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Resolute Professional Billing Snapshot
Epic Benefits
• Improve patient experience through seamless, accurate, and error free billing processes
• Standardized prices for patients receiving services at different facilities
• Expedite refund processes for patients paying by credit card
• Leverage Epic Charge Review workqueues to integrate billing processes and collaborate with other staff, such as seeing a physician’s note and documentation
• Utilize follow-up workqueues for advanced denial prevention and resolution functionality
• Minimize refund processing costs in the event of charge error
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Resolute Professional Billing workflow brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202073

Level Current State Workflow Future State Workflow Impacted Roles
Medium Existing charge reconciliation reports and processes (CC/R policies) are specific to performing reconciliation for charges in Soarian.
Charge Reconciliation: Current policies will be updated to reflect new Epic processes and functionalities. Source departments are now responsible for the accuracy and the comprehensiveness of their charge capture in Epic.
Department managers and CC/R personnel should fully understand processes by demonstrating adherence to CC/R policies, entering charges in a timely manner, resolving accounts in workqueues, and running reports to reconcile charges daily.
• Revenue Integrity Staff• Clinical Department
Managers • Charge Capture
Personnel
Low CCHC uses Soarian Charge Capture Mechanisms and Charge Capture / Reconciliation (CC/R) policies.
Charge Capture Methods: CCHC will align to future state Epic processes, functionalities, and tools. Departments are primarily responsible for their charge capture.
Department managers and charge capture personnel should fully understand processes by demonstrating adherence to CC/R policies, entering charges in a timely manner, resolved accounts in workqueues and running reports to reconcile charges daily.
• Revenue Integrity Staff• Clinical Department
Managers • Charge Capture
Personnel
Low Revenue Integrity calls Payment Posting staff to move the prepayment for partial cosmetic accounts to the appropriate HAR.
Partial Elective and Cosmetic Surgery (Payment Posting): System functionality (account activity) will be used by Revenue Integrity staff to transfer partial cosmetic accounts to a workqueue. Then the Payment Posting staff will move the prepayment amount to the appropriate Hospital Account Record (HAR).
• Revenue Integrity Staff –Cosmetic/Elective
• Payment Posting Staff
New Functionality brought on by Epic
Coordination between Craneware and Epic: Both Craneware and Epic offer revenue tracking tools and end user charging workshops to assist RI team at Go-Live and to identify lost revenue at conversion. • Clearly established CCHC, Epic, and Craneware charge capture / reconciliation responsibilities• Clear understanding of CC/R processes and expectations by clinical staff• Maintenance of gross revenue neutrality at Go-Live and return to revenue baselines Post-Live
Revenue Guardian checks allow you to leverage Best Practice Advisories from patient’s charts to ensure accurate charge capture
Decentralized charge review ownership allows for more efficient distribution of charge editing
Epic Revenue Integrity Dashboards offer new insight into several key metrics for revenue reconciliation and charge review across all clinical departments
Need-to-Know Epic Benefits, Change Impacts, and New Functionalities
Revenue Integrity & Payment Posting Snapshot
Epic Benefits
• Improve patient experience through more seamless, accurate, and error free charging and billing processes
• Ensure accurate charge capture by leveraging Best Practice Advisories from patient’s Revenue Guardian checks
• Decentralize charge review ownership to staff who are familiar with the charge and responsible for edits
• Utilize Epic Revenue Integrity Dashboards for new insight into several key metrics for revenue reconciliation and charge review across all clinical departments
• Review all observation charges and automated functionality for observation carve-outs
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Revenue Integrity and Payment Posting workflows brought about by the new Epic EHR, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
CCHC Patients
Last Updated: 9/1/2020 74

Epic Module/Areas
New 3rd Party
75
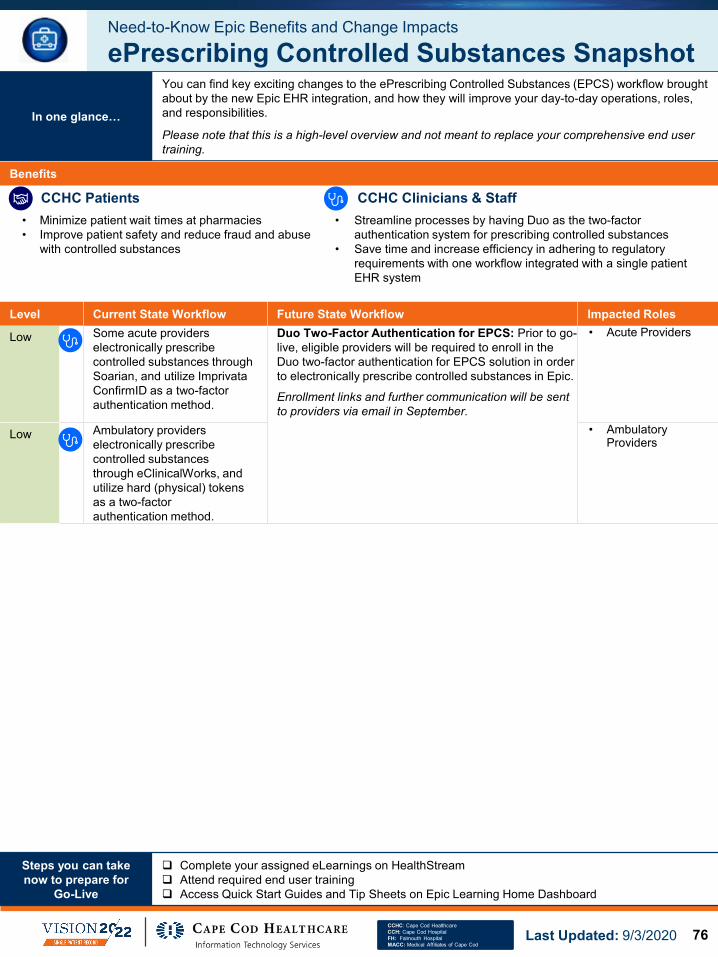
Level Current State Workflow Future State Workflow Impacted Roles
Low Some acute providers electronically prescribe controlled substances through Soarian, and utilize Imprivata ConfirmID as a two-factor authentication method.
Duo Two-Factor Authentication for EPCS: Prior to go-live, eligible providers will be required to enroll in the Duo two-factor authentication for EPCS solution in order to electronically prescribe controlled substances in Epic.
Enrollment links and further communication will be sent to providers via email in September.
• Acute Providers
Low Ambulatory providers electronically prescribe controlled substances through eClinicalWorks, and utilize hard (physical) tokens as a two-factor authentication method.
• Ambulatory Providers
Need-to-Know Epic Benefits and Change Impacts
ePrescribing Controlled Substances Snapshot
Benefits
• Minimize patient wait times at pharmacies• Improve patient safety and reduce fraud and abuse
with controlled substances
• Streamline processes by having Duo as the two-factor authentication system for prescribing controlled substances
• Save time and increase efficiency in adhering to regulatory requirements with one workflow integrated with a single patient EHR system
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…
You can find key exciting changes to the ePrescribing Controlled Substances (EPCS) workflow brought about by the new Epic EHR integration, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/3/2020 76
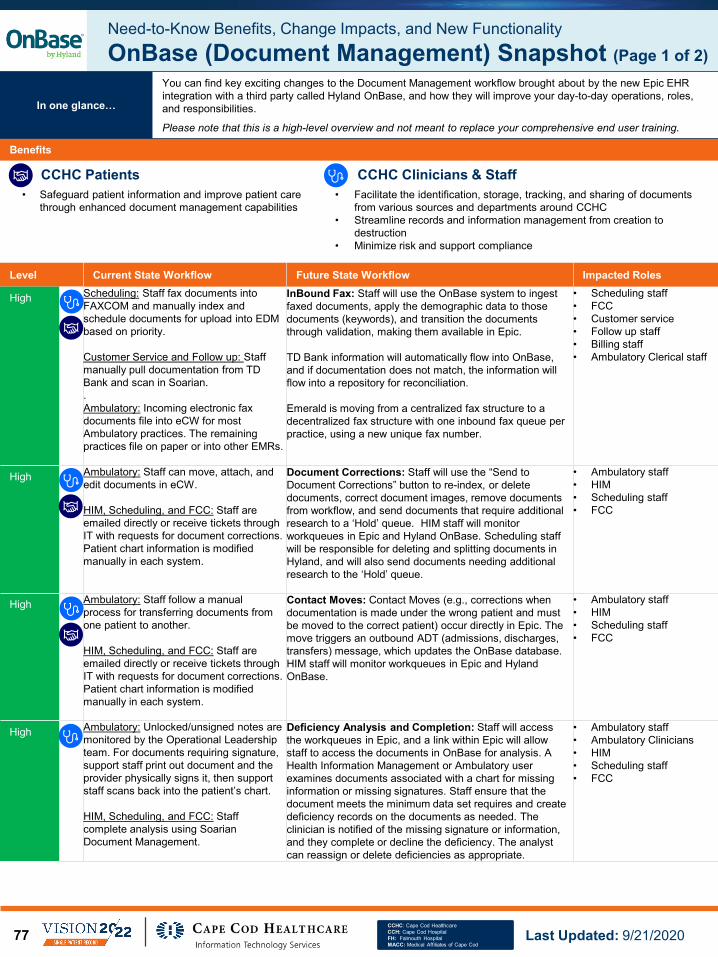
Level Current State Workflow Future State Workflow Impacted Roles
High Scheduling: Staff fax documents into FAXCOM and manually index and schedule documents for upload into EDM based on priority.
Customer Service and Follow up: Staff manually pull documentation from TD Bank and scan in Soarian.. Ambulatory: Incoming electronic fax documents file into eCW for most Ambulatory practices. The remaining practices file on paper or into other EMRs.
InBound Fax: Staff will use the OnBase system to ingest faxed documents, apply the demographic data to those documents (keywords), and transition the documents through validation, making them available in Epic.
TD Bank information will automatically flow into OnBase, and if documentation does not match, the information will flow into a repository for reconciliation.
Emerald is moving from a centralized fax structure to a decentralized fax structure with one inbound fax queue per practice, using a new unique fax number.
• Scheduling staff• FCC• Customer service• Follow up staff• Billing staff• Ambulatory Clerical staff
High Ambulatory: Staff can move, attach, and edit documents in eCW.
HIM, Scheduling, and FCC: Staff are emailed directly or receive tickets through IT with requests for document corrections. Patient chart information is modified manually in each system.
Document Corrections: Staff will use the “Send to Document Corrections” button to re-index, or delete documents, correct document images, remove documents from workflow, and send documents that require additional research to a ‘Hold’ queue. HIM staff will monitor workqueues in Epic and Hyland OnBase. Scheduling staff will be responsible for deleting and splitting documents in Hyland, and will also send documents needing additional research to the ‘Hold’ queue.
• Ambulatory staff• HIM• Scheduling staff• FCC
High Ambulatory: Staff follow a manual process for transferring documents from one patient to another.
HIM, Scheduling, and FCC: Staff are emailed directly or receive tickets through IT with requests for document corrections. Patient chart information is modified manually in each system.
Contact Moves: Contact Moves (e.g., corrections when documentation is made under the wrong patient and must be moved to the correct patient) occur directly in Epic. The move triggers an outbound ADT (admissions, discharges, transfers) message, which updates the OnBase database. HIM staff will monitor workqueues in Epic and Hyland OnBase.
• Ambulatory staff• HIM• Scheduling staff• FCC
High Ambulatory: Unlocked/unsigned notes are monitored by the Operational Leadership team. For documents requiring signature, support staff print out document and the provider physically signs it, then support staff scans back into the patient’s chart.
HIM, Scheduling, and FCC: Staff complete analysis using Soarian Document Management.
Deficiency Analysis and Completion: Staff will access the workqueues in Epic, and a link within Epic will allow staff to access the documents in OnBase for analysis. A Health Information Management or Ambulatory user examines documents associated with a chart for missing information or missing signatures. Staff ensure that the document meets the minimum data set requires and create deficiency records on the documents as needed. The clinician is notified of the missing signature or information, and they complete or decline the deficiency. The analyst can reassign or delete deficiencies as appropriate.
• Ambulatory staff• Ambulatory Clinicians• HIM• Scheduling staff• FCC
Need-to-Know Benefits, Change Impacts, and New FunctionalityOnBase (Document Management) Snapshot (Page 1 of 2)
Benefits
• Safeguard patient information and improve patient care through enhanced document management capabilities
• Facilitate the identification, storage, tracking, and sharing of documents from various sources and departments around CCHC
• Streamline records and information management from creation to destruction
• Minimize risk and support compliance
In one glance…
You can find key exciting changes to the Document Management workflow brought about by the new Epic EHR integration with a third party called Hyland OnBase, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/21/202077

Level Current State Workflow Future State Workflow Impacted Roles
Medium Staff access multiple systems to gather documents for ROI. Business Office staff handle ROI requests and ask HIM for assistance as necessary.
Ambulatory: Specialty office staff process their own ROI requests at the practice level. HIM processes ROI requests for primary care only.
Integrated Release of Information (ROI): Staff create and complete Release of Information requests directly in OnBase. When printed, the ROI contains OnBase documents that were attached to the chart and selected for printing by the user. They create a package in OnBase and send it over to Epic. Then, Epic adds in discrete or additional data, and then they send out to the requestor.
Specialty office staff will continue to process their own ROI requests at the practice level.
• HIM• Customer service• Follow up • Billing• Ambulatory Clerical staff
Low Staff log into EDM or Soarian Financials and use patient-specific links to review and print patient documentation. If specific information cannot be located, staff must go into Soarian Clinical (HIM/Business Office) or FAXCOM (Scheduling).
Ambulatory: Staff review patient documents within document the folder structure in eCW or Soarian.
OnBase Patient Window (OPW): Staff will review patient documentation through the OnBase Patient Window, which launches from Epic Chart Review and contains needed documents on the chart tabs. Filters are used to show results to staff as needed.
• HIM• Scheduling staff• FCC• Customer service• Follow up • Billing• Ambulatory staff• Clinicians
Low Staff scan documents into Soarian document management.
Ambulatory: Staff scan documents into eCW.
Batch Scanning and Processing: Staff will use the OnBase system to ingest scanned documents via batch scan, apply patient demographic data to those documents (keywords), and transition those documents through validation, making those documents available in Epic.
• HIM• Scheduling staff• FCC• Customer service• Follow up • Billing• Ambulatory staff
Low Merging occurs in Soarian Financials and staff check EDM if documents are not moved over automatically. Staff call or email HIM to report a potential merge.
Ambulatory (IT Team): Staff conducts merging processes in eCW (Emerald and MACC).
Master Record Number (MRN) Merge: Staff use Epic to report a potential merge which sends it to a Workqueue for HIM to review. HIM will own this process moving forward.
When MRN equals MPI, merges are initiated at the MRN level. When MRN does not equal MPI, MRNs can be merged if the assigning authority matches on both source and target MRN. The workflow is triggered by a merge in Epic and the user must verify that patients, charts, and documents are properly updated in OnBase.
• HIM• Ambulatory IT team
Need-to-Know Benefits, Change Impacts, and New FunctionalityOnBase (Document Management) Snapshot (Page 2 of 2)
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/21/2020
New Functionality
Integration with Other Applications: Hyland OnBase Document Management will store signed documentation from integrated Epic and Ancillary systems.
Streamlined workqueues in Epic will help staff reconcile duplicate records based on upcoming visits and manage chart corrections
In one glance…
You can find key exciting changes to the Document Management workflow brought about by the new Epic EHR integration with a third party called Hyland OnBase, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
78

Level Current State Workflow Future State Workflow Impacted Roles
High CCHC uses some paper forms for documentation, and also documents clinical data in Haemonetics applications (SafeTrace, El Dorado).
SCC Soft Transition: CCHC is moving to the SCC Soft suite of applications for the clinical documentation of Blood Bank and Donor services. This is inclusive of new applications, interfaces, and peripheral devices (barcode scanners, label printers). Within SCC Soft, Blood Donor staff will document electronically in Soft Donor, moving away from paper forms.
• Blood Bank staff• Blood Donor staff
High Order sets exist in multiple systems, but CCHC also completes documentation on paper.
Massive Transfusion Protocol: Physicians will need to place order sets in Epic for Mass Transfusion. Nursing will document in the Mass Transfusion flowsheet. This process will be different than the regular ‘blood prepare and transfuse blood admin’ workflow. In the flowsheet, staff will scan the unit number in and document the volume transfused.
• Physicians• Nurses• Blood Bank
High Staff place orders in Soarian Clinical which interfaces with SafeTrace.
Blood Administration Workflows: For non-MTP Blood Administration workflows, there will be a seamless integration between SoftBank and Epic. There is an order to “Prepare Blood” and “Transfused Blood”, which are included in the blood transfusion order sets.
• Physicians• Nurses• Blood Bank
Low Blood Bank receives own specimens.
Central Processing Collects All Samples: Central Processing collects all samples in Beaker which integrates into SoftBank. Blood Bank will not need to go into Epic to receive specimens.
• Lab staff• Blood Bank staff
Low There are a limited number of useful reports in SafeTrace.
SCC Soft Reporting: More robust reporting features are available to staff. SoftBI (Business Intelligence module) includes developed analytics reports for management tracking and statistics. Some examples of the analytics reports are included below:• Tests Collected for RIBC• Units Received by Week• Transfused Units by Blood Type• Percent of Transfusions• Average Units per Transfusion by Order Doctor• Total Units by MTP
• Blood Bank staff
Low SafeTrace is interfaced with Soarian Clinical.
Interfaced Blood Bank Results: Integration exists between SoftBank and Epic.
• Blood Bank staff
Low Test results from Vision Instruments are entered into the system manually.
Vision Instruments: Test results will be automatically entered into the system via interface with SoftBank.
• Blood Bank staff
Low Staff use paper orders and document on paper charts. Orders are manually faxed to the Blood Donor Center.
Therapeutic Phlebotomy: Therapeutic Phlebotomy Therapy Plan is built in Epic. Staff will manage Therapy Plans by using EpicCare Ambulatory and Beaker applications.
• Blood Bank staff
Need-to-Know Benefits and Change Impacts
SoftBank Snapshot
Benefits
• Eliminate errors through positive patient identification to ensure blood products are linked to the correct patient
• Interface seamlessly with CCHC Epic applications• Track blood products accurately from a centralized inventory with dynamic
features that include outstanding management reports, daily trace, and audit trail
• Improve documentation through usage of barcode scanners and label printers and ensure positive patient identification
Steps you can take now to prepare for
Go-Live
Complete your assigned eLearnings on HealthStream Attend required end user training Access Quick Start Guides and Tip Sheets on Epic Learning Home Dashboard
In one glance…You can find key exciting changes to the Blood Bank workflow brought about by the new Epic EHR integration with Soft Bank, and how they will improve your day-to-day operations, roles, and responsibilities.
Please note that this is a high-level overview and not meant to replace your comprehensive end user training.
CCHC Patients CCHC Clinicians & Staff
CCHC: Cape Cod HealthcareCCH: Cape Cod HospitalFH: Falmouth HospitalMACC: Medical Affiliates of Cape Cod
Last Updated: 9/1/202079