viral infections of the skin and mucus membranes
TRANSCRIPT
Viral Infections of the Skin and Mucus
Membranes

Maculopapular Rash Measles virus Rubella virus Parvovirus Human Herpes 6
Vesicular Rash Herpes simplex virus Varicella zoster virus Coxsakievirus
Measles Measles virus is a paramyxovirus
Paramyxoviruses : Enveloped virus, ssRNA genome as a single piece. The family includes parainfluenza virus, mumps virus, measles virus
and respiratory syncytial virus. Parainfluenza and mumps virus have a surface hemagglutinin and
neuraminidase, while measles have a hemagglutinin, but not neuraminidase.
The virion structure includes: Spikes F protein Matrix protein M, below the envelope
Only one serotype
Measles Disease
Acute febrile illness, mostly in childhood
Incubation period: 10 – 12 days
Onset is flu-like: high fever, cough, conjunctivitis
Koplik's spots: red spots with bluish-white centre on the buccal mucosa
1 – 2 days later, acute symptoms decline with appearance of a widespread maculopapular rash
Over 10 – 14 days, recovery is usually complete as the rash fades

Complications
Giant cell pneumonia, more common in adults
Otitis media
Post-measles encephalitis
Subacute sclerosing panencephalitis (SSPE): progressive and fatal degenerative disease within the infected cells, there is a defective form of the virus
which because it can not produce functional M protein, is not released as complete virus from the cells.
Laboratory Diagnosis
Most cases are diagnosed clinically
NPA, immunofluorescence

EpidemiologyEpidemiology
Transmission: person to person by respiratory droplets. Malnutrition contributes to high mortality.
ControlControl
Live attenuated vaccine, combined with mumps and rubella (MMR)
Administration: between 12 – 18 months.
Rubella (German Measles)
Rubella Virus Classified as togavirus ssRNA virus with an envelope pleomorphic in appearance, 50 – 60 nm in diameter nucleocapsid is icosahedral in symmetry ssRNA is infective and replication occurs in the
cytoplasm three major polypeptides: C and envelope
glycoproteins E1 and E2 single serotype

Postnatal Rubella
Incubation period: 12 – 21 days Macular rash, appears first on the face, then
spreads to the trunk and limbs Minor pyrexia, malaise and lymphadenopathy
with suboccipital nodes most commonly enlarged and tender
Arthralgia is uncommon in children, but may occur in up to 60% of adult females, involving the fingers, wrists, ankles and knees
Encephalitis and thrombocytopenia are rare complications
Pathogenesis
Virus is transmitted by air-borne route URT Viremia
Skin, joints, placenta cross the barrier
Infect fetal differentiating cells Early in pregnancy: this will cause congenital
abnormalities
Laboratory Diagnosis
Clinical diagnosis is unreliable Investigation by virus isolation is not indicated (unreliable
and time-consuming) Serological diagnosis is the method of choice, detecting
rubella specific IgG and rubella specific IgM. These tests are also used for screening to ascertain susceptibility and whether rubella immunization is indicated.
Congenital rubella syndrome: serological testing for specific IgM. Maternal IgM does not cross the placenta so detection of specific IgM is diagnostic of intrauterine infection
Control
Attenuated live vaccine (MMR) Seroconversion occurs in over 95% Protection persists for more than 20 years Administration in pregnancy is contra-indicated Pregnancy should be avoided for the month
following vaccination
Human Parvovirus
Only parvovirus B19 is the cause of diseases in humans
Genus: Erythrovirus
The Virus
20 – 25 nm in diameter icosahedral symmetry, no envelope the capsid consists of two proteins, VP1 and VP2 specific viral receptors such as blood group P
antigen; explains narrow host range infection is followed by life-long immunity Genome: ssDNA
Replication
Dependent on cellular factors expressed transiently in the cell during late S or early G2 phase of mitosis.
All parvoviruses require dividing cells for replication

Clinical Diseases
Rash illness (Erythema infectiosum) Erythematous maculopapular rash Common in children aged 4 – 11 years Very similar to rubella
Joint disease 80% in adult females 10% in childhood cases arthritis involving small joints of the hands with wrists,
knees and ankles affected in some cases
Aplastic crisis A transient acute event which complicates chronic
hemolytic anemia Fall in hemoglobin Disappearance of reticulocytes from peripheral blood Erythropoiesis cessation lasts for 5 – 7 days Symptoms of worsening anemia B19 infection is responsible for 90% of the cases Occurs most commonly in children with sickle cell
anemic
B19 in the immunocompromized Persistent infection that leads to persistent anemia
Laboratory Diagnosis
Virus detection Serum,
detecting viral antigens using ELISA detecting viral genome using nucleic acid hybridization
and PCR
Antibody detection Recent infection can be diagnosed by detecting
B19-specific IgM or increasing amounts of specific IgG.

Epidemiology
Endemic throughout the year in temperate climates
Transmission occurs by respiratory route
High-titre viremia enables transmission by blood
Congenital transmission (vertical)
Treatment
Most cases are mild and self-limiting
Aplastic crisis: blood transfusion
Immunosuppressed: blood transfusion and human normal immunoglobulin
Intrauterine infection: intrauterine blood transfusion

Human Herpesvirus 6 (HHV 6)
Sequence analysis revealed two variants: HHV 6A: no clear disease association HHV 6B: exanthema subitum or roseola infantum
Roseola Infantum
The disease is common between 6 months and 3 years
Sudden onset of fever Throat congestion and cervical lymphadenopathy Widespread macular rash occurs in 10% of the
cases Some cases are associated with HHV-7 infection HHV-6 and -7, both infect T lymphocytes
Vesicular Rash
Herpes simplex virus
Varicella zoster virus
Coxsakievirus

Herpes Simplex Viruses Ubiquitous virus, infecting the majority of world’s
population
Two types: HSV-1 and HSV-2
Type 1 is associated primarily with mouth, eye and CNS
Type 2 is found mostly in the genital tract
Transmission: direct contact
Herpes Simplex Structure
Icosahedral virus
Lipoprotein envelope, derived from the nuclear membrane
Genome: linear, ds DNA
Replicate in the nucleus

HSV Glycoproteins At least 11 glycoproteins are known
Three are essential for production of infectious virus:
gB and gD : penetration into the cells
gH: release of the virus

Pathogenesis Primary Infection The typical lesion is the vesicle; ballooning degeneration of
intra-epithelial cells. The roof of the vesicle breaks down, forming ulcer
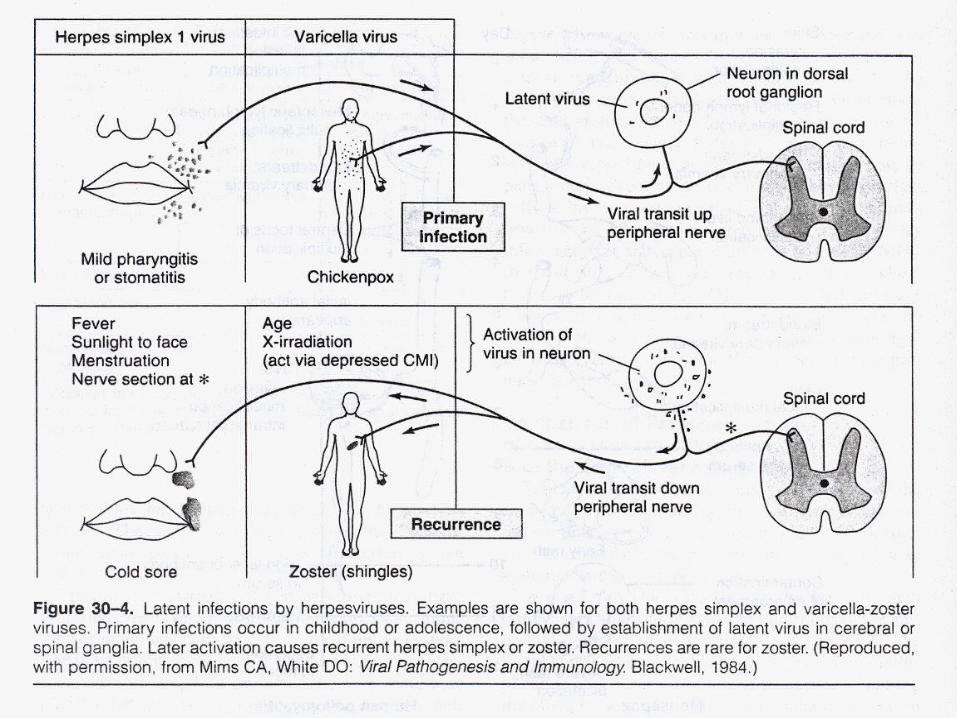
During the replication phase at the site of entery in the epithelium, virus particles enter through the sensory nerve endings and transported along the axon to the nerve body (neurone) in the sensory (dorsal root) ganglion by retrograde axonal flow. Latent infection occurs in the survived neurons that still harbor the viral genome
Antibodies reduce the severity of the infections, although it does not prevent recurrences.

Latent Infection About 1% of cells in the affected ganglion carry
the viral genome.
Viral DNA exists as free circular episomes (20 copies / cell).
Latency-associated transcripts (LAT) are present
HSV-1: causes latency in trigeminal ganglion HSV-2: causes latency in sacral ganglion
Reactivation Known triggers for recurrences are accompanied by
a local increase in prostaglandin levels and depression of cell-mediated immunity.
Reactivation can be induced by UV light Fever Trauma Stress
Interval between the stimulus and lesion appearance is 2 – 5 days.


Clinical Features Oral infectionOral infection Acute febrile gingivostomatitis in preschool children Vesicular lesions ulcerate rapidly
Skin infectionsSkin infections Herpetic whitlow: primary lesion on the fingers or
thumb of the toddler with herpetic stomatitis, due to autoinoculation. It also occurs as accidental inoculation in health care workers.
Eczema herpeticum: severe form of cutaneous herpes. It may occur in children with atopic eczema.

Clinical Features Eye infectionEye infection Conjunctivitis or keratoconjunctivitis associated with corneal
ulceration. This will result in corneal scarring and vision impairment.
The majority are caused by HSV-1 Most patients with recurring eye disease are aged over 50 years
CNS infectionCNS infection The most likely route of infection is central spread from
trigeminal ganglion HSV encephalitis
CSF collected in the acute stage should be used for PCR amplification of HSV DNA.
More commonly due to HSV-1
Clinical Features Genital tract infectionGenital tract infection
Both types can infect genital tract, but HSV-2 is more common. The lesions are vesicular at first but rapidly ulcerate
Male: affects the glans and shaft of the penis
Female: affects the labia and vagina or cervix Fever and malaise are accompanied by regional
lymphadenopathy, urethritis and vaginal discharge
Clinical Features Recurrent genital herpesRecurrent genital herpes
Can be as frequent as six or more episodes a year.
Attacks are milder and shorter than first episodes
HSV-1 genital infection recurs less often than HSV-2
Either type is capable of transmission from mother to infant. Transplacental passage has been recorded but is very rare. Ascending infection from the cervix is more significant especially when the membranes are ruptured prematurely.
Laboratory Diagnosis
Isolation of HSV in cultures of human diploid fibroblast cells. Growth is rapid. CPE includes rounded, ballooned cells in foci and giant cell formation
Detection of viral antigens in cell (by immunofluorescence), scraped from the base of lesions
Detection of amplified viral DNA by PCR in CSF
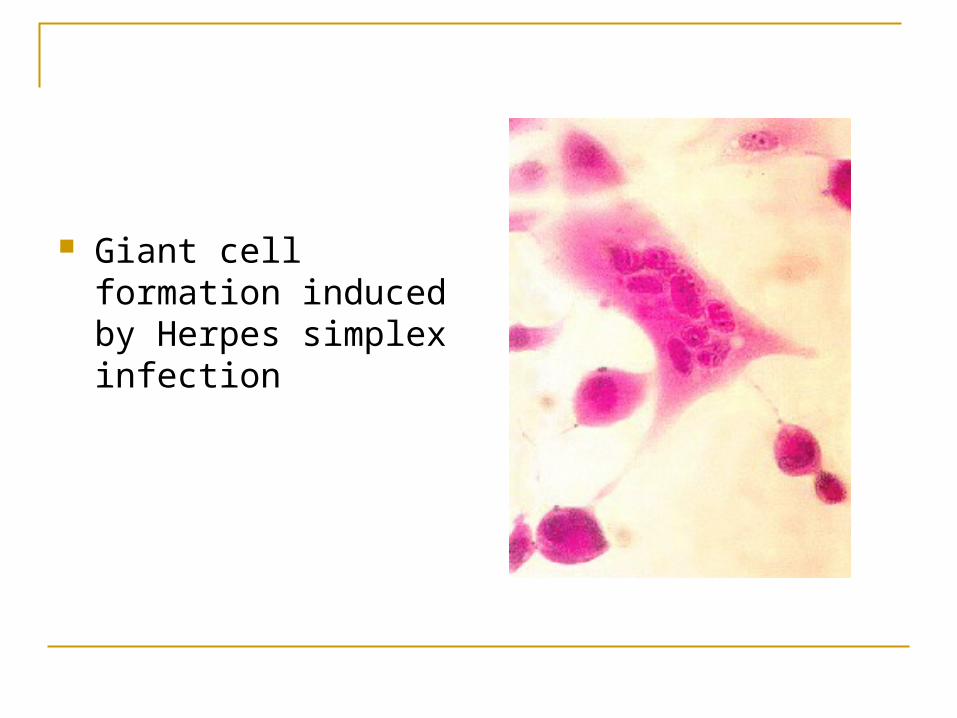
Giant cell formation induced by Herpes simplex infection
Treatment
Acyclovir: inhibits viral DNA synthesis
Acute HSV infections
Latency is not eradicated by this agent
Prophylactic to prevent reactivation in the immunocompromized (transplant recipients)
Available for topical, oral and intravenous route

Varicella Zoster Virus
Two forms
Primary infection is a generalized eruption (chicken pox)
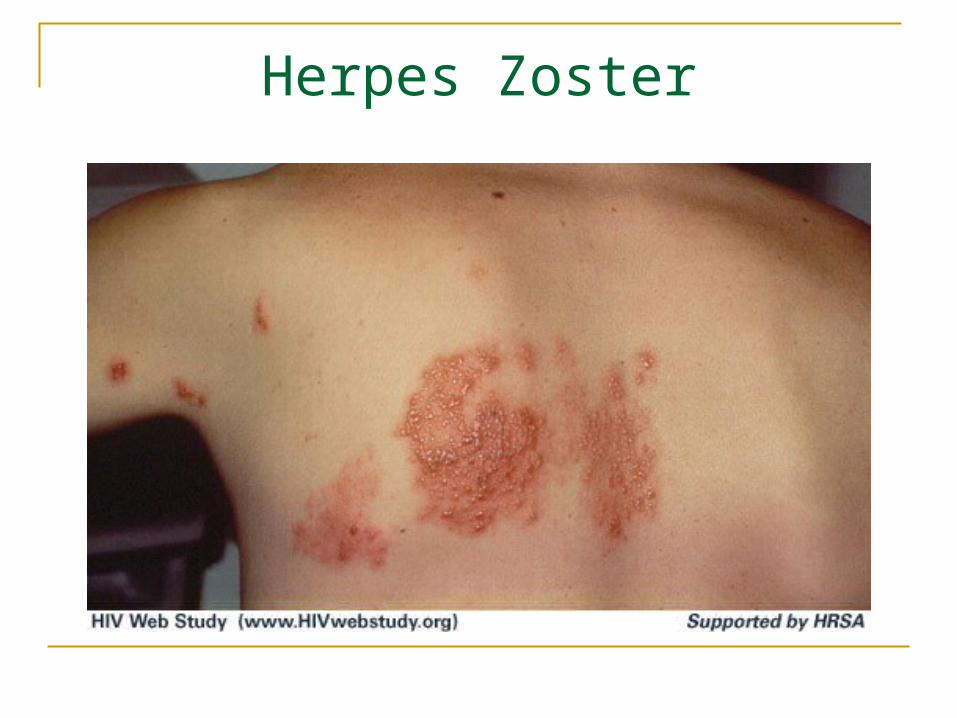
Reactivation is localized to one or few dermatomes (shingles, Varicella Zoster)
Only one antigenic type

Pathogenesis of Chicken Pox Children, vesicular skin eruption
Virus enters through URT or conjunctiva
The virus causes viremia
The vesicles lie in the middle of the epidermis. The fluid becomes cloudy with the influx of leucocytes. These pustules dry up, scabs form and desquamate.
Lesions in all stages are present at any time while new ones are appearing.

Pathogenesis of Varicella Zoster
VZV stays latent in the sensory ganglia
Reactivation can occur at any age but the rate is much increased in persons aged 60 years or over.
Zoster is usually limited to one dermatome; in adults most commonly in the thoracic or upper lumbar region.

Clinical FeaturesChicken Pox
Incubation period: 14 – 15 days
The patient is infectious for 2 days before and up to 5 days after onset
The rash is most dense on the trunk and head
Macules ---- Papules ---- Vesicles ---- Pustules
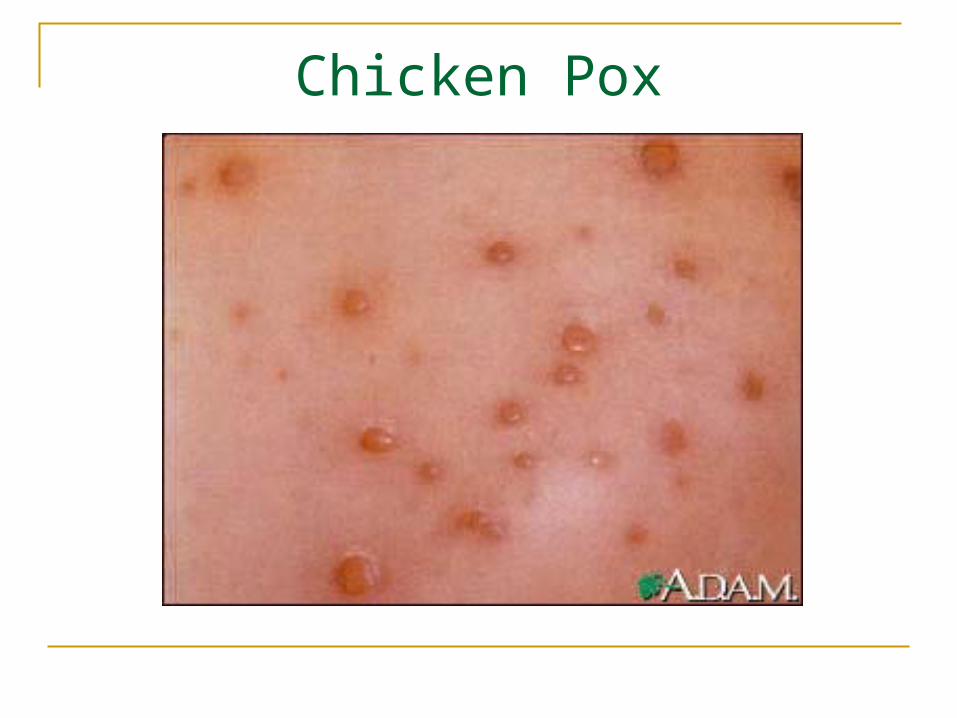
Chicken Pox

Complications
Secondary bacterial infection (commonest)
Pneumonia
CNS cerebellar ataxia syndrome acute encephalitits

Herpes Zoster
Reactivated VZV infection
Localized eruption, unilateral, typically confined to one dermatome
Prodromal paraesthesia and pain in the area supplied by affected nerve are common before skin lesions develop
Postherpetic neuralgia Most common complication of zoster 50% risk in patients aged over 60 years pain persisting for 1 month or more after the rash
Herpes Zoster
Ophthalmic zoster Involvement of ophthalmic division of the trigeminal
nerve corneal ulceration, stromal keratitis permanent scarring and loss of sight

Laboratory Diagnosis
Early vesicular lesions are the best diagnostic material
Virus isolation takes from 5 days to 3 weeks
More rapid detection is possible with centrifugation-enhanced cultures (shell vials)
Direct immunofluorescence
VZV DNA amplification by PCR

Treatment
Acyclovir
Given to high-risk of complication Neonates (first 3 weeks of life) Ophthalmic zoster Immunocompromized
Epidemiology Spread: respiratory route, in winter and early spring
Varicella is highly infectious to susceptible close contacts
Mortality is high in normal adults, particularly smokers who develop pneumonia
Zoster is associated with decreased T cell function: Old age Pre-AIDS phase Organ transplant recipients
Control
Passive immunization: varicella zoster immunoglobulin (VZIG): Neonates Non-immune pregnant contacts Immunocompromized contacts
A live attenuated vaccine, IM injection

Coxsackieviruses Picornavirus
Icosahedral, positive sense, linear, ssRNA
Two groups: A and B
Group A: Herpangina (vesicular pharyngitis) Hand – Foot – and – Mouth disease Acute hemorrhagic conjunctivitis
Group B: Pleurodynia (epidemic myalgia) Myocarditis Meningoencephalitis
Herpangina Severe febrile pharyngitis The pharynx is usually hyperemic and discrete
vesicles occur on the posterior half of the palate, pharynx, tonsils or tongue
Self-limited and most frequent in small children Hand – Foot – and – Mouth disease
Oral and pharyngeal ulcerations Vesicular rash on the palm and soles
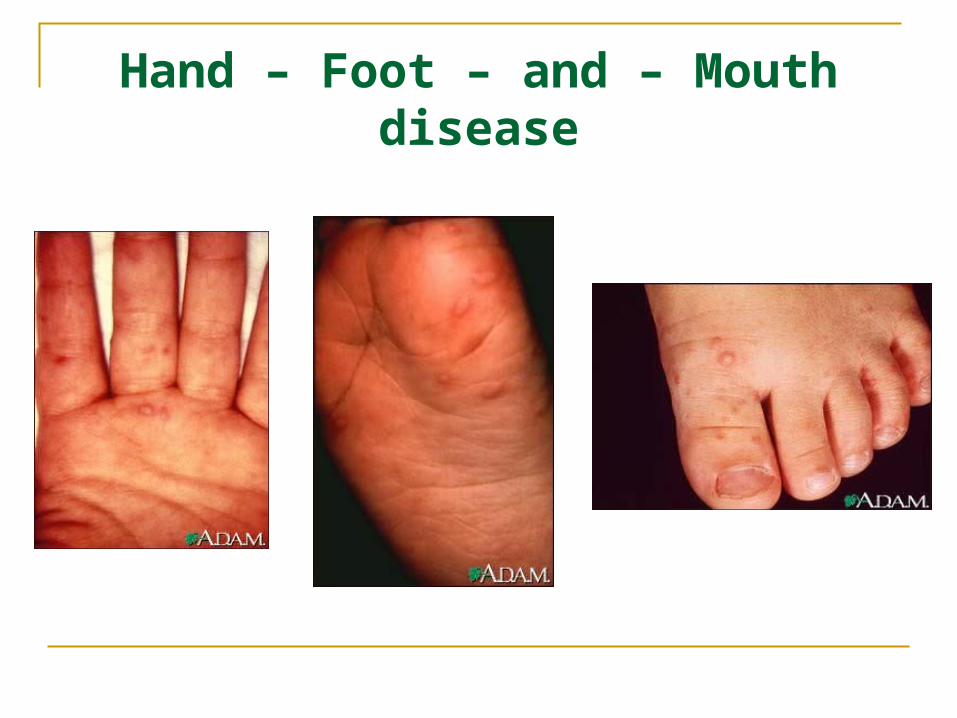
Hand – Foot – and – Mouth disease