ventilation in covid-19 respiratory failure: a (cpap) in
TRANSCRIPT

Page 1/20
The role of Continuous Positive Airway Pressure(CPAP) in Delaying or Avoiding MechanicalVentilation in COVID-19 Respiratory Failure: ARetrospective Cohort StudyAllan Cameron
Glasgow Royal In�rmarySharif Fattah ( [email protected] )
Glasgow Royal In�rmary https://orcid.org/0000-0002-1781-5746Laura Knox
Glasgow Royal In�rmaryPauline Grose
Glasgow Royal In�rmary
Research
Keywords: COVID-19, CPAP, Respiratory Failure
Posted Date: August 5th, 2021
DOI: https://doi.org/10.21203/rs.3.rs-722133/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 2/20
AbstractBackground - During the winter of 2020-2021, the second wave of the COVID19 pandemic in the UnitedKingdom caused increased demand for intensive care unit (ICU) beds, and in particular, for invasivemechanical ventilation (IMV). To alleviate some of this pressure, some centres offered non-invasivecontinuous positive airway pressure (CPAP), delivered on specialised COVID high dependency units(cHDUs). However, this practice was based largely on anecdotal reports, and it is not clear from theliterature how effective CPAP is at delaying or preventing IMV.
Methods - This was a retrospective observational cohort study of consecutive patients admitted to aspecialised cHDU at Glasgow Royal In�rmary between November 2020 and February 2021. Each patienthad a continuous record of the level of respiratory support required, and was followed up to hospitaldischarge or death. We examined patient outcomes according to age, sex and maximum level ofrespiratory support, using logistic regression and time-to-event analysis. The number of patients whocould not be oxygenated by standard oxygen facemask but could be oxygenated by CPAP was countedand compared to the number of patients admitted to ICU for IMV over the same period.
Results - There were 152 admissions to cHDU over the study period. Of these, 125 received CPAPtreatment. Of the patients who received support in cHDU, the overall mortality rate was 37.9% (95% CI30.3% - 46.1%)). Odds of mortality were closely correlated with increasing age and oxygen requirement.Of the 152 patients, 44 patients (28.8%, 95% CI 22.0 – 36.9%) went on to require IMV in ICU. Thisrepresents 77.2% of the 57 COVID-19 admissions to ICU during the same period. However, there were also41 patients who received levels of respiratory support on cHDU which would normally necessitate ICUadmission but who never went to ICU, potentially reducing ICU admissions by 41.8% (95% CI 32.1 –52.2%).
Conclusion - Providing respiratory support in cHDU reduced the number of potential ICU admissions by41.8%, as well as delaying IMV for over 75% of ICU admissions. This represents a signi�cant sparing ofICU capacity at a time when IMV beds were in high demand.
IntroductionThe SARS-Cov-2 pandemic has caused signi�cant morbidity and mortality worldwide, being responsiblefor more than 3 million deaths globally as of May 2021 [1]. Despite the recent development of therapiesshown to reduce mortality and the rollout of vaccination programmes against COVID-19, global casenumbers, hospitalisations and deaths remain high [1–3].
The large number of patients with COVID-19 has put pressure on many health services, and in particular ahigh demand for critical care beds; at the peak of the second COVID-19 wave in the UK in January 2021,there were over 4,000 patients on invasive mechanical ventilation (IMV) for COVID-19 across the country[4].

Page 3/20
Beginning in March 2020, some National Health Service (NHS) resources were diverted to help supportintensive care units (ICUs) in preparation for the anticipated demand. In several centres, this included thedevelopment of respiratory support units (RSUs) and COVID-19 high dependency units (cHDUs), as areaswhere patients could receive non-invasive respiratory support such as continuous positive airwaypressure (CPAP) and high �ow nasal oxygen (HFNO). Both of these modalities are considered aerosol-generating procedures (AGPs), and hence must be provided in speci�c facilities with stringent infectioncontrol procedures and specialized staff. CPAP and HFNO are used for a variety of reasons in COVID-19,but one rationale is to reduce the number of patients requiring IMV at any one time [5–7].
CPAP has been used previously in pneumonitis caused by other coronaviruses, playing a role in thetreatment of Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS)[8, 9]. Its utilization in COVID-19 was also described in hospitals in China and Italy at the start of thepandemic [10]. This led the British Thoracic Society to recommend CPAP as �rst-line respiratory support inpatients with COVID-19 pneumonitis who fail to oxygenate adequately on standard oxygen therapy [11].
CPAP typically uses less oxygen than high-�ow nasal oxygen therapy, and thus places less of a burdenon a hospital’s oxygen supply when the hospital has a high COVID-19 workload. Due to it being a non-invasive modality, CPAP has the potential to act as both a bridge to delay or avoid IMV, and as a ceiling ofcare for those unsuitable for IMV.
To our knowledge, the extent to which a dedicated CPAP unit can relieve the demand for ICU beds has notbeen well described in the literature.
ObjectivesThe aim of this study is to describe the outcomes of a cohort of patients with COVID-19 pneumonitistreated in a dedicated COVID-19 high dependency unit. In particular, we examine whether use of CPAP orHFNO therapy could delay or avoid IMV.
Methods
Study DesignThis was a retrospective cohort study of consecutive patients admitted to the cHDU at Glasgow RoyalIn�rmary over a three-month period coinciding with the second wave of Coronavirus in the UK betweenNovember 2020 and February 2021.
SettingThe Glasgow Royal in�rmary (GRI) is a large 950-bedded city teaching hospital serving a population ofaround 320,000 people. The city as a whole had a high prevalence of COVID-19 during the study periodwith a peak 7-day rate of cases per 100,000 population of 402 at the beginning of January 2021 [12].

Page 4/20
During the �rst wave of the pandemic in March 2020, a 14-bedded COVID-19 high dependency unit(cHDU) was established at GRI. By the time this was reestablished for the second wave of COVID-19 inAutumn 2020, staff had already developed considerable experience in managing COVID-19 with CPAPand HFNO, and there were agreed referral and treatment pathways already in place. Dexamethasone hadbeen introduced as an evidence-based treatment, and there was emerging evidence for the use of othertherapeutics such as Remdesevir and Tocilizumab.
The unit’s facilities included a 2:1 patient-to-nurse ratio; the ability to provide continuous invasivemonitoring when indicated; 24-hour senior-level medical presence, and appropriate physical barriersaround the ward so that aerosol generating procedures (AGPs) could take place in a sealed environment.Staff wore full personal protective equipment including FFP3 respirator masks to minimise exposure.
CPAP was provided via face mask using ResMed Stellar™ machines with supplemental oxygenadministered via a wall-mounted �ow valve capable of 30L/min delivery. We used a standard PEEP of 10cmH2O for all patients on CPAP, and all patients treated with CPAP were given 5mg midzolam and 5mgmorphine over 24 hours by subcutaneous infusion to improve mask tolerance unless speci�cally contra-indicated.
In-house testing of the FiO2 achieved at various oxygen �ow rates was undertaken by our RespiratoryPhysiology Colleagues, this is summarised in Table 1.
Table 1Measured FiO2
achieved with variousoxygen �ow rates on
CPAP deviceOxygen FiO.2.
10 l/min 40–45%
15 l/min 50%
20 l/min 60–70%
25 l/min 80%
30 l/min 75–90%
NHFO was provided by the Fisher and Paykel AIRVO 2™, which on maximum settings provided 60 L/minof warmed, humidi�ed gas with an FiO2 of 95%.
Oxygenation was assessed by pulse oximetry, and the oxygenation target was 90–94% unless the patientwas known to have chronic hypoxia from a pre-existing condition, in which case the target was 88–92%.
Patients

Page 5/20
We examined records for all consecutive adult patients admitted to the cHDU at Glasgow Royal In�rmarybetween 15th November 2020 and 14th February 2021 inclusive. Admission to the unit was the soleeligibility criterion. The start date was chosen for convenience, as this was when daily electronicrecording of observations began on the unit, and the end date was chosen because the number of newadmissions had fallen to low levels.
VariablesThe data extracted from electronic records included each patient’s age, sex and NCoV-19 PCR status. Werecorded dates and times of admission to hospital, admission to cHDU, and where appropriate,admission to ICU. Each patient’s date of discharge from hospital (or date of death) was also obtained.For each patient, a daily record of various parameters measured during their time in cHDU was obtained.This included respiratory rate and SpO2, type of respiratory support, FiO2 and PEEP.
Our main outcome variables were the binary outcomes of ICU admission and of death. The explanatoryvariables were type of respiratory support, amount of supplemental oxygen, and duration of respiratorysupport. Age and sex were considered as important confounding variables.
Data sourcesPatients were identi�ed and cross-checked using the WardWatcher and TrakCare™ patient informationsystems, which also provided dates and times of admissions, discharges and deaths. The patientobservations and respiratory settings were extracted from the TURAS COVID-19 application, whichallowed electronic recording of each patient’s parameters throughout their cHDU stay. Each TURAS dailyreview (and initial TURAS assessment, where available) was obtained in Portable Document Format(PDF) from Orion Software’s Clinical Portal™ and the relevant data extracted from the PDF �le using thepdftools package in R [13]. Missing data was recti�ed by review of electronic scans of written clinicalnotes available as PDFs on Clinical Portal.
BiasSince this was an observational study, there will be unmeasured confounding variables. The mostimportant are likely to be patient-level variables such as co-morbidities and frailty, which would affect thedecision to admit to ICU, and make adverse outcomes more likely. However, there may also be a time-dependent patient selection bias, as bed availability dropped during the peak of the wave in January,meaning that patients admitted during this time may well have been more unwell as the threshold foradmission to cHDU increased. For the same reason, there may have been a time-dependent changing ofthe threshold for admission to ICU. There is no straightforward way to measure or correct for thesepotential biases, and they simply need to be borne in mind when interpreting the results.
Study sizeOur study size was determined by the demand for and capacity of the unit during the study period. Thisallowed us to capture the majority of patients treated in the second wave of the coronavirus pandemic.
Page 6/20
Quantitative variablesThe daily data for each patient was summarized to give a duration of time spent on respiratory support,and a maximum FiO2 or oxygen �ow rate during their stay. To help give a more complete summary of therespiratory support on a per-patient basis, we also recorded the number of days spent on a high level ofnon-invasive respiratory support. This was de�ned as being on greater than 15L/min of oxygen whilst onCPAP or being on HFNO with an FiO2 of ≥ 0.9. These numbers were chosen because by consensus theyrepresented levels of support beyond that which could be achieved by standard oxygen therapy.
Statistical methodsData was manually tidied and veri�ed before being converted to comma separated variable format andimported into R version 4.1.0 [14]. Simple summary statistics including means, medians, ranges andhistogram plots were produced using base R functions. Con�dence intervals for simple proportions werecalculated using binomial con�dence intervals[15]. Comparison of proportions in two groups was doneusing Fisher’s exact test. Comparisons of medians between two groups was performed using the Mann-Whitney U test. Age density plots were created using normal kernel density estimates. The effect of binaryoutcomes according to continuous variables such as age or peak supplemental oxygen was carried outby logistic regression analysis. Kaplan-Meier curves were also constructed to perform survival analysisbetween men and women.
There was no missing data, as we were able to reconstruct missing data points from the written clinicalnotes.
To ensure reproducibility and transparency of the results, the statistical analysis code and methodssection of this paper were written in R Markdown prior to the �nal data set becoming available.
Results
ParticipantsThere were 1045 observations found for 153 episodes in 152 unique patients. The episodes comprised71 admissions of women and 82 admissions of men.
The median age was 60, with a range of 24–87, and an interquartile range of 53–68. The age distributionis shown more completely in the histogram in Fig. 1.
A total of 58 episodes ended in death, giving a crude mortality rate of 37.9% (95% con�dence interval30.3% − 46.1%) per admission.
The median length of stay in hospital was 11.8 days, with a range of 0.2–115 days and interquartilerange of 8–18.5 days.
Page 7/20
The mean age of those who survived was 55.7, whereas those who died had a mean age of 65.1 (p < 0.001 by Mann-Whitney). Survivors were therefore around 10 years younger than non-survivors onaverage. The relative age distribution of survivors and non-survivors is depicted in Fig. 2.
Association between age and mortalityAge had a signi�cant association with mortality. Logistic regression (Fig. 3) showed that the odds ofdeath approximately doubled for every extra 8.0 years of age, with the survival odds being 1 (i.e. 50%probability of survival) at an age of 66.5 years.
Association between sex and mortality31 out of the 71 women died (43.7%) versus 27 of the 82 men (32.9%). This difference was non-signi�cant by Chi Square test (p = 0.231).
A comparison of the Kaplan Meier survival curves for men and women is shown in Fig. 4, and doesappear to show a difference, with the hazard ratio for men being 0.606, but the effect size just missesstatistical signi�cance (CI 0.352–1.044, p = 0.071). This effect does not appear to be attributable to age,as there was less than 3 months’ difference between the mean age of men and women in the cohort.
ICU admission and mortalityOf the patients who died after admission to cHDU, 27 of these died in ICU. The other 31 died either incHDU or in a step down ward.
Use of CPAP and HFNO142 patients had either continuous positive airway pressure (CPAP) applied via a facemask, or had high�ow nasal oxygen (HFNO) for at least part of their time in cHDU.
The predominant modality was CPAP, with 95 (62.1%) patients receiving CPAP only as their mainmodality. Only 17 (11.1%) patients had HFNO only, with 30 (19.6%) switching between modalities forvarious reasons, and 11 (7.2%) not receiving either.
Of the 11 patients who did not receive an AGP, four patients were Covid positive with complex HDU needsother than respiratory support. Four patients had been stepped down from ICU, two were thought torequire an AGP but stabilized quickly on admission and never required one. There was also one patientwho turned out not to have Covid at all.
These �ndings are summarised in Table 2.
Page 8/20
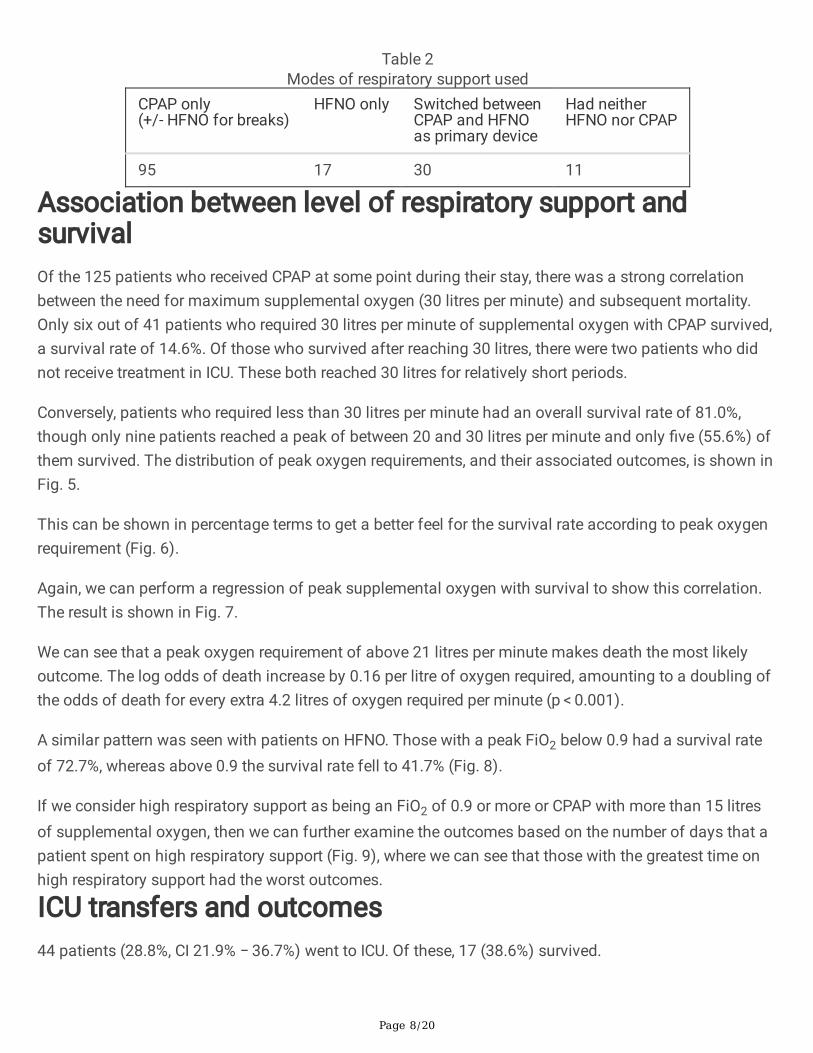
Table 2Modes of respiratory support used
CPAP only(+/- HFNO for breaks)
HFNO only Switched betweenCPAP and HFNOas primary device
Had neitherHFNO nor CPAP
95 17 30 11
Association between level of respiratory support andsurvivalOf the 125 patients who received CPAP at some point during their stay, there was a strong correlationbetween the need for maximum supplemental oxygen (30 litres per minute) and subsequent mortality.Only six out of 41 patients who required 30 litres per minute of supplemental oxygen with CPAP survived,a survival rate of 14.6%. Of those who survived after reaching 30 litres, there were two patients who didnot receive treatment in ICU. These both reached 30 litres for relatively short periods.
Conversely, patients who required less than 30 litres per minute had an overall survival rate of 81.0%,though only nine patients reached a peak of between 20 and 30 litres per minute and only �ve (55.6%) ofthem survived. The distribution of peak oxygen requirements, and their associated outcomes, is shown inFig. 5.
This can be shown in percentage terms to get a better feel for the survival rate according to peak oxygenrequirement (Fig. 6).
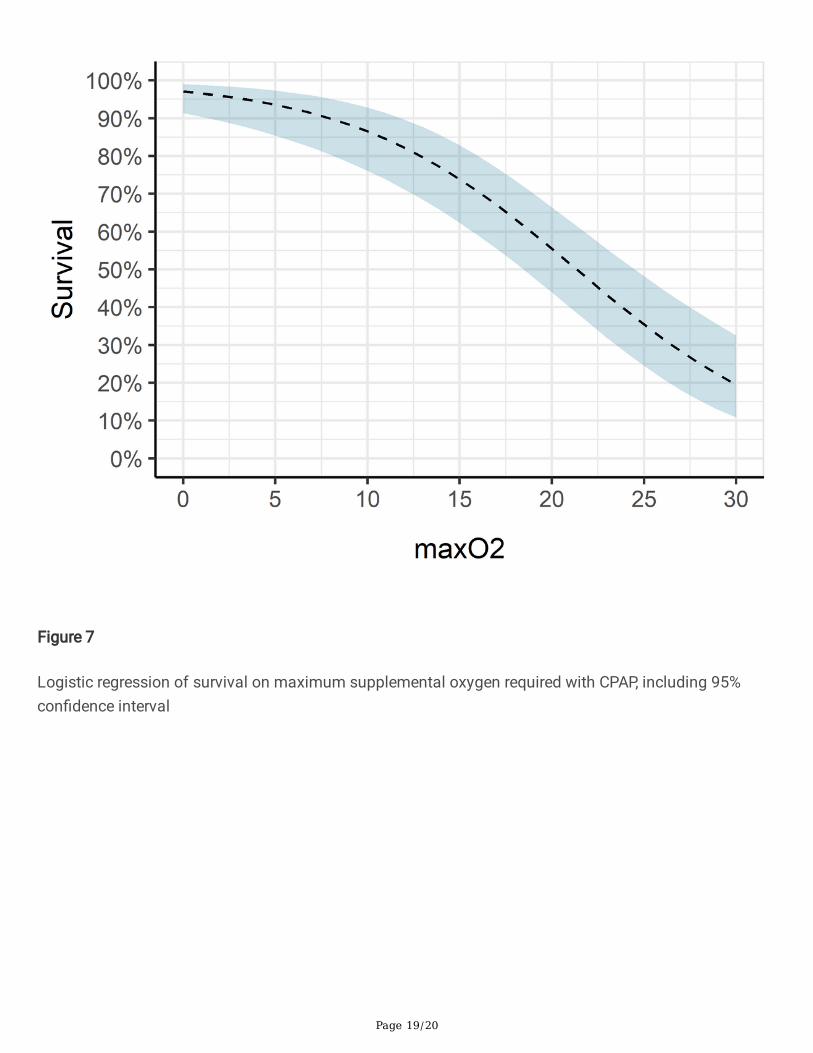
Again, we can perform a regression of peak supplemental oxygen with survival to show this correlation.The result is shown in Fig. 7.
We can see that a peak oxygen requirement of above 21 litres per minute makes death the most likelyoutcome. The log odds of death increase by 0.16 per litre of oxygen required, amounting to a doubling ofthe odds of death for every extra 4.2 litres of oxygen required per minute (p < 0.001).
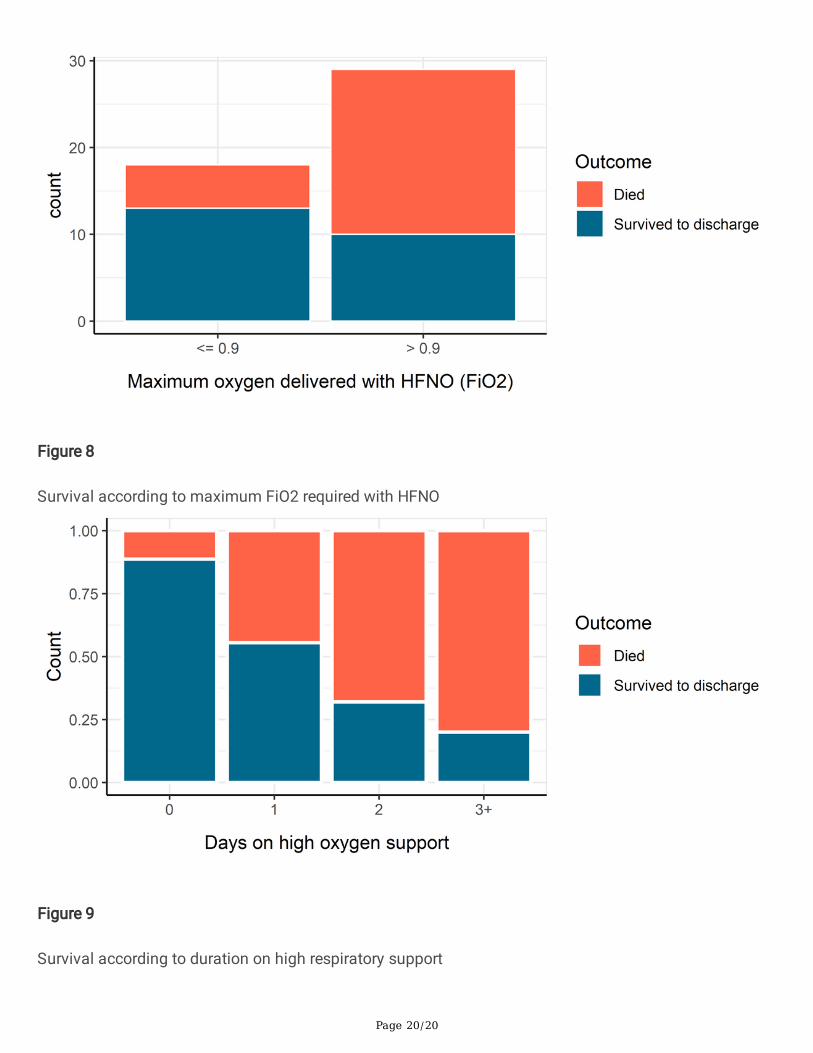
A similar pattern was seen with patients on HFNO. Those with a peak FiO2 below 0.9 had a survival rateof 72.7%, whereas above 0.9 the survival rate fell to 41.7% (Fig. 8).
If we consider high respiratory support as being an FiO2 of 0.9 or more or CPAP with more than 15 litresof supplemental oxygen, then we can further examine the outcomes based on the number of days that apatient spent on high respiratory support (Fig. 9), where we can see that those with the greatest time onhigh respiratory support had the worst outcomes.
ICU transfers and outcomes44 patients (28.8%, CI 21.9% − 36.7%) went to ICU. Of these, 17 (38.6%) survived.

Page 9/20
Of these 17 ICU survivors, in two cases, the Covid swab was negative and the �nal diagnosis was notCovid pneumonitis. A further three patients had radiological evidence of bacterial pneumonia in additionto Covid at the time of their admission to ICU.
This means that 12 patients out of the 39 (30.8%) patients with uncomplicated severe Covid pneumonitissurvived their ICU admission. Even among this group, there is signi�cant residual morbidity. One patientwent home on domicillary oxygen; another with a Zimmer frame for mobility. One patient has since beenreadmitted with right heart failure due to post-Covid pulmonary �brosis. Most have community rehabneeds and some require ongoing community mental health input.
Total ICU admissions during the study period and ICUavoidanceThere were 57 admissions in total to our ICU during the study period. These comprised 53 newadmissions and four re-admissions. Our ICU were heavily pressured during the majority of this period,with full occupancy plus expansion beds opened elsewhere in the hospital. During this time, there were 41patients treated in cHDU with levels of respiratory support exceeding the threshold that would normallymandate a transfer to ICU for IMV - that is, being on CPAP plus more than 15 litres per minute of oxygen,or being on HFNO with greater than 90% FiO2. These are patients who typically could not be oxygenatedon a ward without NIV or IMV. Although some of these patients may not have been deemed appropriatefor IMV in ICU, this sets an upper limit of a 42% reduction in ICU admissions during the study period as aresult of the facilities available in cHDU.
Although these patients are likely to have had a shorter length of stay in ICU than those who were actuallytaken for IMV, this still represents a large reduction in the burden placed on ICU resources.
ICU admissions and maximal CPAPNone of the 22 patients who were on the maximal 30 litres per minute of oxygen for more than 24 hourssurvived without going to ICU. Of the 14 patients on maximum CPAP for more than 24 hours who weretaken to ICU, none who were on maximum CPAP for more than 3 days survived. There is likely an elementof selection bias here, and the numbers are small, but in our cohort it seems that if a patient was onmaximum CPAP for more than 24 hours, the prognosis was grim.
ComplicationsSix of the patients treated with CPAP (5%) developed a pneumomediastinum, and one of these cases wasassociated with a small pneumothorax. Although two of these patients subsequently died, thepneumomediastinum was not thought to be a contributory cause. However, when pneumomediastinumor pneumothorax was identi�ed in any of these patients, CPAP was discontinued and HNFO was used asan alternative. The increased incidence of pneumomediastinum in mechanically ventilated patients hasalready been discussed in the literature, and there are case reports of patients with COVID-19 pneumonitis

Page 10/20
developing pneumomediastinum even without IMV or NIV, so it is not clear that CPAP was the directcause of these complications [16, 17].
Discussion
Key resultsAdmissions to cHDU in this cohort were almost all appropriate candidates, meaning that the majorityrequired some form of respiratory support beyond standard oxygen therapy. Predominantly these patientswere brought for CPAP to treat COVID pneumonitis. Out of 153 patients, only two did not have adiagnosis of COVID pneumonitis.
Over 80% of patients received CPAP during their time in cHDU and less than 10% did not require an AGP.Only seven patients brought for respiratory support did not require an AGP. Four other patients werebrought appropriately for complex care needs and did not receive an AGP. This suggests an appropriateuse of the facility during the second wave of the pandemic.
The strongest clinical predictor of death was age, with the odds of a patient dying approximatelydoubling for every eight years of age. There was also a non-signi�cant trend for women to have worseoutcomes than men in our cohort.
The overall mortality rate appeared to be high, at 37.9%. This was despite the introduction of evidence-based therapeutics such as Dexamethasone, Tocilizumab and Remdesevir. A possible explanation forthis is that we had a high threshold for admission during the second wave.
There were 41 patients who did not go to ICU despite being on levels of respiratory support that wouldnormally mandate an ICU admission. If one posits that the main value of CPAP is in preventing intubationand protecting ICU capacity, then cHDU has been successful in achieving this goal during wave two,reducing ICU admissions by up to 42%.
High levels of respiratory support, particularly patients receiving the maximum of 30 litres ofsupplemental oxygen with CPAP, was found to be a very poor prognostic marker. Indeed after 24 hours ofsuch treatment, the only survivors in this group were those who went to ICU. Even of those that went on toinvasive ventilation the survivor numbers were still small.
InterpretationThere is currently no evidence of a survival bene�t from CPAP or HFNO in the context of Covidpneumonitis. However, it is thought that non-invasive CPAP may prevent the need for intubation andventilation in cases where the patient cannot be adequately oxygenated by simple supplemental oxygen.
In our experience, patients with Covid pneumonitis whose gas exchange is su�ciently impaired to requireCPAP plus 15 litres of oxygen per minute could not be adequately oxygenated with a standard oxygen
Page 11/20
mask. In some other units, patients reaching this level of support would be considered for ICU admission.
In contrast, our practice has been to provide up to 30 litres of oxygen with CPAP and up to 0.95 FiO2 withHFNO. In fact, of our 153 admissions, close to half of our patients (73 or 47.7%) were treated with highlevels of respiratory support at some point during their stay in cHDU. Of these, 32 ended up going to ICUanyway, but 41 did not. Of the 41 who did not go to ICU, we had only 14 survivors (34.1%), though thepatients who were this unwell and were taken to ICU had similar mortality rates. This certainly suggests arole for high-level respiratory support in an HDU setting as an alternative to invasive ventilation in ICU forsome patients.
LimitationsWe need to be cautious in interpreting these �ndings, since it is likely that there are clinical differencesbetween the ICU and non-ICU groups that are not apparent in the data. It may be that the cohort taken toICU were at the more severely unwell end of this range, or had level 3 care needs other than respiratorysupport. However, there does not seem to have been a clear disadvantage in terms of mortality to thecohort treated within cHDU as opposed to ICU, and this suggests that CPAP with high levels ofsupplemental oxygen may be a reasonable alternative to invasive ventilation in selected patients withCovid pneumonitis.
Although our 153 patients allow us to make some very clear inferences about outcomes based on ageand level of respiratory support, this is observational data and there will certainly be confoundingvariables and selection biases that are not recorded in the data. We should therefore be careful not toover-interpret apparent patterns in the data.
Finally, the design of this study does not allow any de�nite conclusions to be drawn about the optimalmode of respiratory support in patients with Covid-19 pneumonitis.
GeneralisabilityOur results suggest that for patients with severe COVID-19 pneumonitis, CPAP with up to 30 litres perminute of supplemental oxygen is a reasonable alternative to IMV and can protect ICU capacity. Forpatients who fail to oxygenate at 30 litres per minute, the prognosis is very poor whether they areintubated or not, but at this level we would consider that a trial of CPAP has failed. There is no reason tosuspect that these �ndings would be substantially different in other populations.
ConclusionOur data suggests CPAP has a clear role in preventing or delaying ICU admission in patients with severerespiratory failure due to COVID-19. It can be safely delivered with up to 30 litres per minute ofsupplemental oxygen in a non-ICU setting. Prognosis is poor for those who require high levels ofsupplemental oxygen with CPAP for a prolonged period of time, with or without subsequent IMV. CPAPshould be considered a key tool in alleviating pressure on IMV beds due to COVID-19.

Page 12/20
AbbreviationsCPAP Continuous Positive Airway Pressure
ICU Intensive Care Unit
IMV Invasive Mechanical Ventilation
cHDU COVID High Dependency Unit
NHS National Health Service
RSU Respiratory Support Unit
HFNO High Flow Nasal Oxygen
AGP Aerosol Generating Procedure
GRI Glasgow Royal In�rmary
DeclarationsEthics Approval
This study was approved by the chair of our Regional Ethics Committee (Ref GSH/21/ME/001), and theuse of anonymised patient data was granted by the local Caldicott Guardian.
Consent for Publication
Not applicable.
Availability of Data and Materials
Datasets used and analysed during this study are available from the corresponding author on request.
Funding
There was no external funding used.
Competing Interests
None of the authors have any competing interests to declare.
Author Contributions
AC collected and analysed the data, and wrote the methods and results sections. SF and LK researchedthe existing literature and wrote the introduction and discussion sections. PG helped with study design

Page 13/20
and interpretation of results, as well as having editorial input to writing the paper. The authors followedthe STROBE checklist for reporting cohort studies when writing this paper.
Acknowledgements
Not applicable.
References1. Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID-19 in real time. The
Lancet Infectious Diseases 2020;20:533–4.
2. The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with Covid-19. NewEngland Journal of Medicine 2021;384:693–704.
3. The REMAP-CAP Investigators. Interleukin-6 Receptor Antagonists in Critically Ill Patients with Covid-19. New England Journal of Medicine 2021;384:1491–502.
4. Government U. Coronavirus (COVID-19) in the UK. 2021.
5. Franco C, Facciolongo N, Tonelli R, Dongilli R, Vianello A, Pisani L, et al. Feasibility and clinicalimpact of out-of-ICU noninvasive respiratory support in patients with COVID-19-related pneumonia.European Respiratory Journal 2020;56:2002130.
�. Walker J, Dolly S, Ng L, Prior-Ong M, Sabapathy K. The role of CPAP as a potential bridge to invasiveventilation and as a ceiling-of-care for patients hospitalized with Covid-19—An observational study.PLOS ONE 2020;15:e0244857.
7. Nightingale R, Nwosu N, Kutubudin F, Fletcher T, Lewis J, Frost F, et al. Is continuous positive airwaypressure (CPAP) a new standard of care for type 1 respiratory failure in COVID-19 patients? Aretrospective observational study of a dedicated COVID-19 CPAP service. BMJ Open RespiratoryResearch 2020;7:e000639.
�. Cheung TMT, Yam LYC, So LKY, Lau ACW, Poon E, Kong BMH, et al. Effectiveness of NoninvasivePositive Pressure Ventilation in the Treatment of Acute Respiratory Failure in Severe AcuteRespiratory Syndrome. Chest 2004;126:845–50.
9. Alraddadi BM, Qushmaq I, Al-Hameed FM, Mandourah Y, Almekhla� GA, Jose J, et al. Noninvasiveventilation in critically ill patients with the Middle East respiratory syndrome. In�uenza and OtherRespiratory Viruses 2019;13:382–90.
10. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adultinpatients with COVID-19 in Wuhan, China: A retrospective cohort study. The Lancet 2020;395:1054–62.
11. Dr Ben Messer MAB Ms Pearlene Antoine-Pitterson. BTS/ICS guidance: Respiratory care in patientswith acute hypoxaemic respiratory failure associated with COVID-19. 2021.
12. Public Health Scotland. COVID-19 in Scotland. 2021.

Page 14/20
13. Ooms J. Pdftools: Text extraction, rendering and converting of PDF documents. 2021.https://CRAN.R-project.org/package=pdftools.
14. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: RFoundation for Statistical Computing 2021. https://www.R-project.org/.
15. CLOPPER CJ, PEARSON ES. THE USE OF CONFIDENCE OR FIDUCIAL LIMITS ILLUSTRATED IN THECASE OF THE BINOMIAL. Biometrika 1934;26:404–13.
1�. Lemmers DHL, Abu Hilal M, Bnà C, Prezioso C, Cavallo E, Nencini N, et al. Pneumomediastinum andsubcutaneous emphysema in COVID-19: Barotrauma or lung frailty? ERJ Open Research 2020;6.doi:10.1183/23120541.00385-2020
17. Goldman N, Ketheeswaran B, Wilson H. COVID-19-associated pneumomediastinum. ClinicalMedicine 2020;20:e91–2.
Figures
Figure 1

Page 15/20
Age Distribution
Figure 2
Age density of survivors and non-survivors

Page 16/20
Figure 3
Logistic regression model of association between age and survival with 95% con�dence interval

Page 17/20
Figure 4
Kaplan-Meier survival curves for men and women
Figure 5
Survival according to maximum supplemental oxygen required with CPAP (absolute numbers)

Page 18/20
Figure 6
Survival according to maximum supplemental oxygen required with CPAP (as proportion)
Page 19/20
Figure 7
Logistic regression of survival on maximum supplemental oxygen required with CPAP, including 95%con�dence interval
Page 20/20
Figure 8
Survival according to maximum FiO2 required with HFNO
Figure 9
Survival according to duration on high respiratory support