vats for thoracic diseases.ppt - bges€¦ · vats for thoracic diseases starters package ‐13 th...
TRANSCRIPT

Dr Sokolow Y.Dpt of Thoracic Surgery
Hôpital Académique ErasmeBruxelles
VATS for Thoracic Diseases
Starters Package ‐ 13 th edition ‐ Strasbourg18 th & 19 th February 2013

VATS INDICATIONS Mediastinal indications
Thymic Surgery Posterior neurogenic tumor Intra thoracic Parathyroid surgery VATS Staging in NSCLC (station L5 – L6)
Lung indications Wedge excision (biopsy, bullectomy, metastasectomy) VATS Lobectomy LVRS
Pleural indications Empyema Pleural biopsy
Others Thoracic Sympatectomy (palmar hyperhydrosis) Pectus excavatum (NUSS Technique) Diaphragmatic rupture
ADVANTAGES OF VATS
Reduction of chest wall trauma Reduction of post operative pain Reduction of impairment of pulmonary function Reduction of length of hospital stay Reduction of the time to return to work The overall cost of a VATS mediastinal mass
excision may be less than an open procedure(much of the expensive disposableinstrumentation is not needed for thesesoperations)
Lin, Surg Oncol. 2003; 12: 195-200Demmy, Ann Thorac Surg. 1998; 66: 187-92

VATS for Mediastinal Lesions
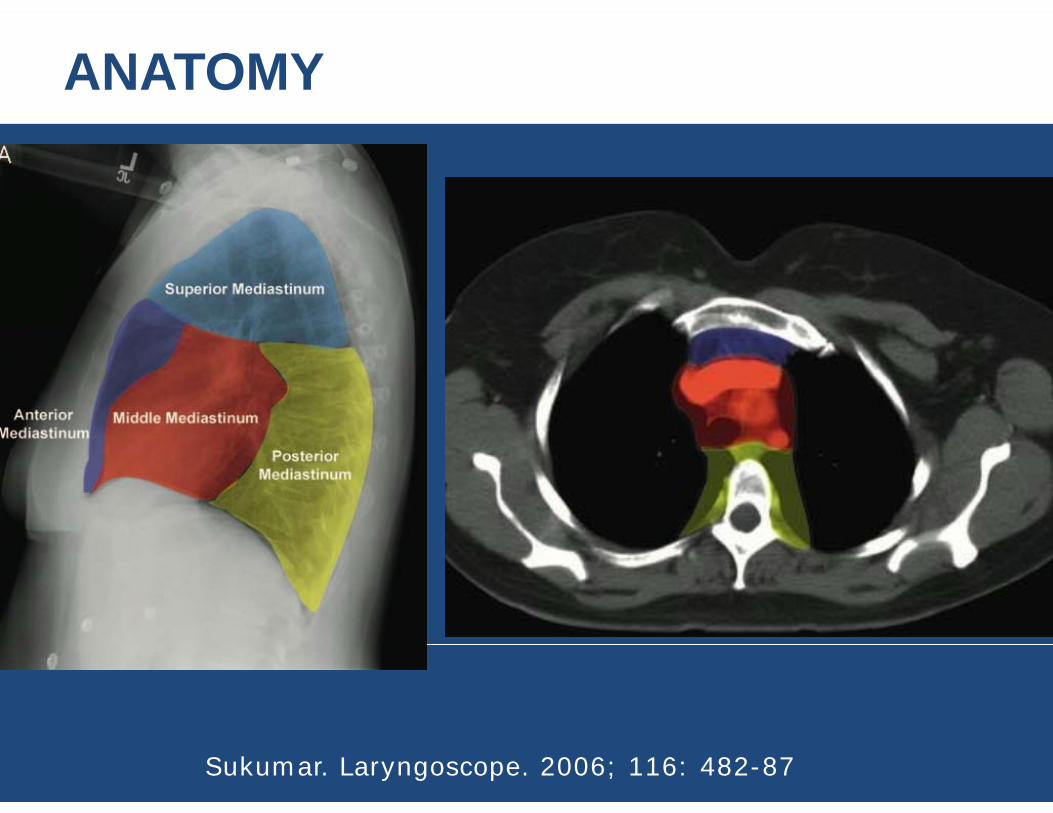
ANATOMY
Sukumar. Laryngoscope. 2006; 116: 482-87
VATS INDACTIONS
Posterior Neurogenic Tumors
Mediastinal cysts
Thymic hyperplasia
Thymoma
Intrathoracic parathyroid adenoma

POSTERIOR NEUROGENIC TUMORS
The majority of posterior mediastinal neurogenic tumors are Schwannoma followed by ganglioneuroma and neurofibroma
The frequency of malignant lesions has been reported to be between 4 % and 13 %
VATS is recommended if the tumor is smaller than 7 cm and if there is no radiological signs of malignancy
Cansever. Thorac Cardiov Surg. 2010: 58; 473-5
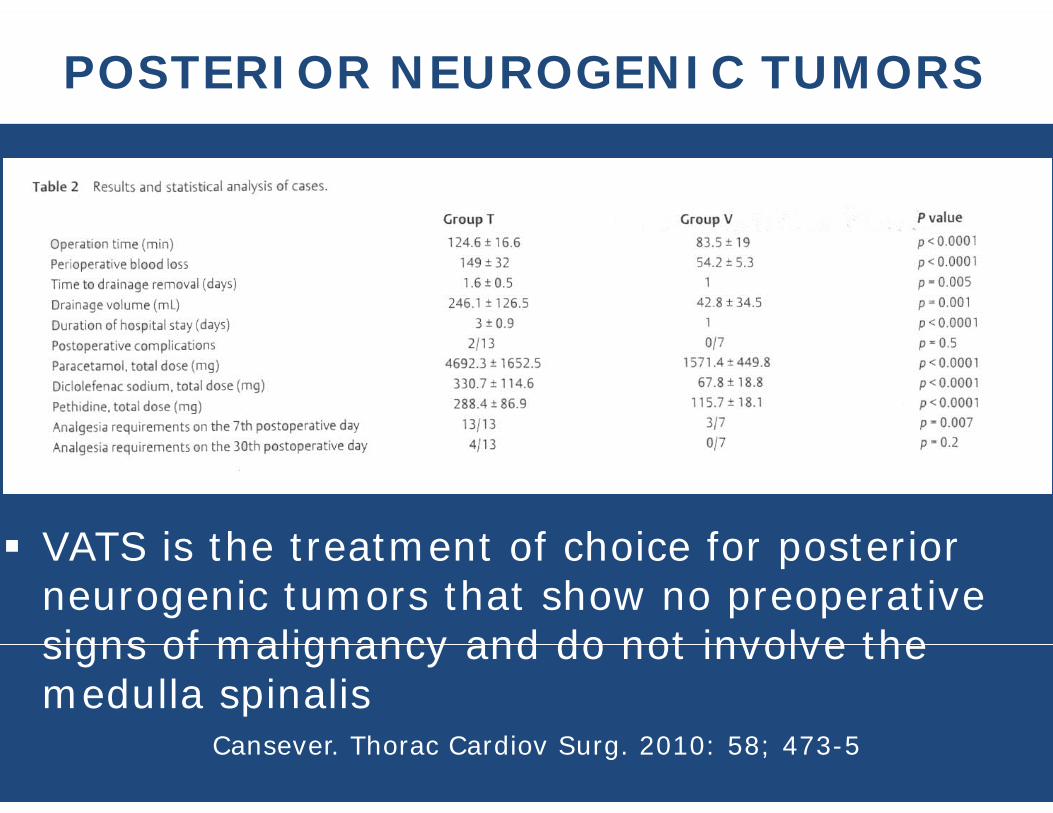
POSTERIOR NEUROGENIC TUMORS
VATS is the treatment of choice for posterior neurogenic tumors that show no preoperative signs of malignancy and do not involve the medulla spinalis
Cansever. Thorac Cardiov Surg. 2010: 58; 473-5

VATS RESECTIONOF POSTERIORNEUROGENIC
LESION


MEDIASTINAL CYSTS
Types Bronchogenic Cysts (50-60 % of mediastinal cysts)
Pericardic Cysts (30 % of mediastinal cysts)
Thymic Cysts (10-15 % of mediastinal cysts)
Resection is indicated for All symptomatic cysts
Large-sized even asymptomatic (excepted PC)
In case of non-formal diagnosis
Le Pimpec Barthes. Rev Pneumol Clin. 2010; 66:52-62
MEDIASTINAL CYSTS
The only radical and definitive treatment is complete surgical resection of the cyst
VATS is considered as the gold standard approach for mediastinal cysts but : VATS may not always be technically possible,
especially in case of dense pericystic adhesions of the cyst with adjacent structures
a bronchogenic cyst's central location, (ex: aortico pulmonary window) would have made VATS resection hazardous
Le Pimpec Barthes. Rev Pneumol Clin. 2010; 66:52-62Hazelrigg. Ann Thorac Surg. 1993; 56:659.
Ribet. Ann Thorac Surg. 1996; 61:1636

THYMUS – MYASTHENIA GRAVIS
Thymectomy is an effectivetreatment in patients withmyasthenia gravis withequivalent clinical outcomesobtained by VATS or openapproach.
Meyer. Ann Thorac Surg. 2009; 87: 385-91
Independently of the surgical approach,extracapsular resection of the thymus must beperformed, including the mediastinal fattytissue.

THYMUS – MYASTHENIA GRAVIS
VATS was found to be superior with regard to improvement ofmyasthenia gravis associated symptoms. The hospital stay wasshorter, and the patients felt less disturbed by direct effects ofthe operation. Therefore, VATS thymectomy can be regarded asthe treatment of choice for patients undergoing surgery formyasthenia gravis.
Bachmann. Surg Endosc. 2008; 22: 2470-77

THYMUS - THYMOMA
For early stage thymoma (stage I and II), the most significant prognostic factor is completeness of resection
VATS of early stage thymoma appears safe and feasible and is associated with a shorter hospital stay. The oncologic outcomes are comparable in the VATS and open surgery groups.
Davenport. Ann Thorac Surg. 2008; 86: 673-84Pennathur. J Thorac Cardiovasc Surg 2011; 141: 694-701
VATS THYMECTOMYFOR THYMIC HYPERPLASIA
IN CASE OF MYASTHENIA GRAVIS

VATS TECHNICAL ASPECTS
Position of trocars


ECTOPIC MEDIASTINAL PARATHYROID ADENOMAS
Ectopic mediastinal parathyroid adenomas can be found in up to 25 % of patients with primary hyperparathyroidism.
Most of these adenomas are located adjacent to the upper thymus and can be resected by cervical incision.
Less than 2% of these adenomas require a thoracic approach (12,5 % in case of re-operative cases)
Cupisti. Langenbeck’s Arch Surg. 2002; 386: 488-93

Russell. Ann Surg. 1981; 193: 805-9Callender. J Am Coll Surg. 2009; 208: 887-93
ECTOPIC MEDIASTINAL PARATHYROID ADENOMAS
Localisation

ECTOPIC MEDIASTINAL PARATHYROID ADENOMAS
Tcherveniakov. JCTS. 2007; 2: 41
Videomediastinoscopy

ECTOPIC MEDIASTINAL PARATHYROID ADENOMAS
Alesina. World J Surg. 2008;32: 224-31
ECTOPIC MEDIASTINAL PARATHYROID ADENOMAS
VATS is actually the gold standard approach for intrathoracic parathyroid adenoma.
(Sternotomy) and thoracotomy should only be used only in case of VATS failure.
VATS is should not be an exploratory procedure. Accurate preoperative anatomic localization of the parathyroid is essential (SPECT/Semstamibi)
Cupisti. Langenbeck’s Arch Surg. 2002; 386: 488-93Alesina. World J Surg. 2008; 32: 224-31
SUMMARY
VATS is considered as the gold standard approach for Mediastinal cysts excepted for some cases of
central or adherent bronchogenic cysts Intrathoracic parathyroid adenoma. Posterior neurogenic tumors that show no
preoperative signs of malignancy and do not involve the medulla spinalis
Thymectomy for Myasthenia Gravis Thymectomy for Stage I (and II) Thymoma

VATS LOBECTOMY

TYPE OF INCISIONS
Koizumi. Ann Thorac Cardiovasc Surg. 2007; 13: 228-35
VATS LOBECTOMY
Earliest reports of VATS lobectomy were
published in the early 1990
Definition of VATS lobectomy is ambiguous
The technique varies in the number of
incisions, degree of rib spreading, and type
of hilar dissection
Flores. Ann Thorac Surg. 2008; 85:S710-15
VATS LOBECTOMYINDICATIONS
Benign disease
Benign tumor
Bronchiectasis
Malignant disease
NSCLC Stage I or II (Intra Lobar)
Metastasis
Carcinoid Tumor

VATS LOBECTOMYTECHNIQUES
Simultaneously stapled (SIS) Lobectomy Endoscopic procedure
Stapled division of fissures
Mass stapled division of lobar hilar structures
Lewis. Ann Thorac Surg. 1993; 56: 762-8
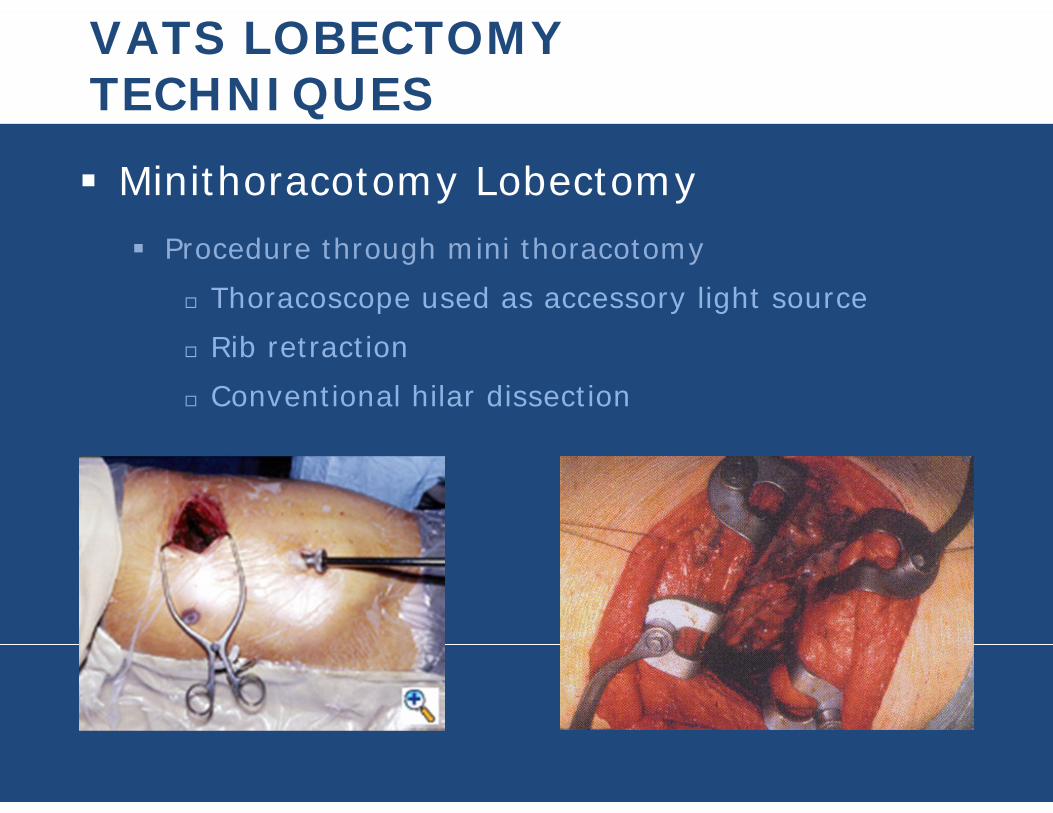
VATS LOBECTOMYTECHNIQUES
Minithoracotomy Lobectomy Procedure through mini thoracotomy
Thoracoscope used as accessory light source Rib retraction Conventional hilar dissection
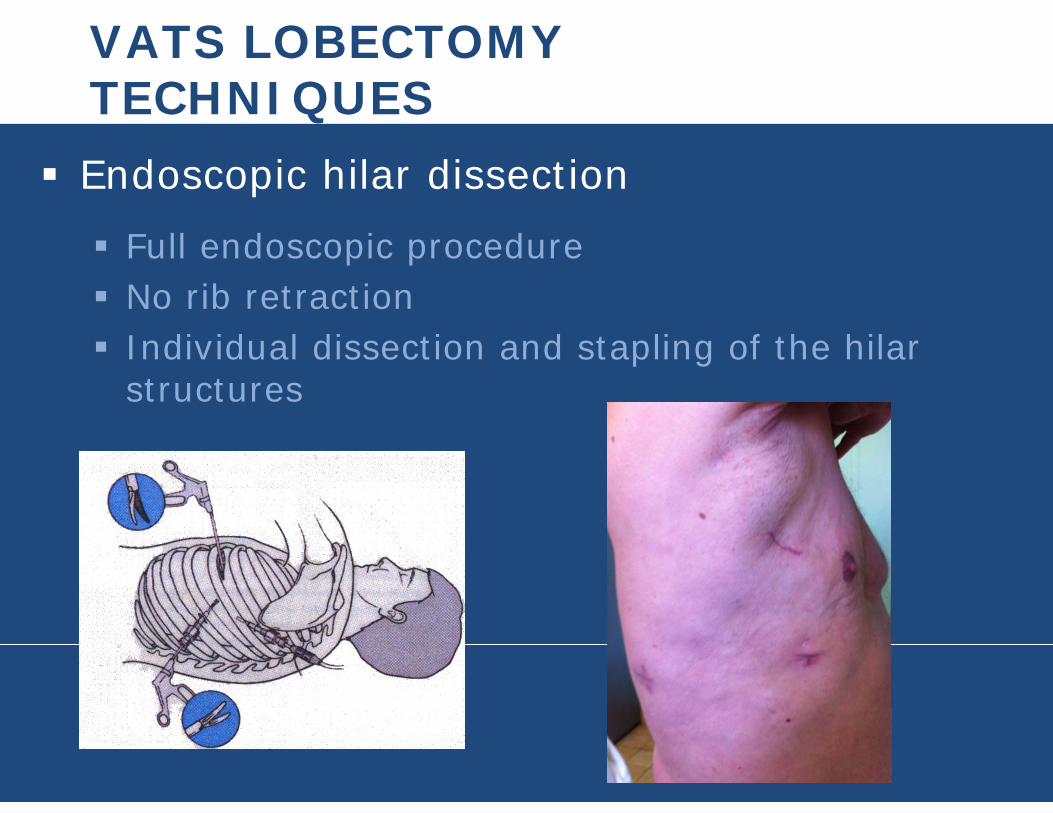
VATS LOBECTOMYTECHNIQUES
Endoscopic hilar dissection
Full endoscopic procedure No rib retraction Individual dissection and stapling of the hilar
structures

VATS SURGERY LOBECTOMY REPORT OF CALGB 39802 : A PROSPECTIVE MULTI INSTITUTION FEASIBILITY STUDY
Swanson. J Clin Oncol. 2007; 25: 4993-7
Within 30 days, 3 (2,7%) of 111patients death occurred
7 (7,4 %) of 95 patients hadgrade 3 or greater complications,with only one case of bleeding
Conclusion : A standardizedapproach to VATS Lobectomywith avoidance of rib spreadingis feasible

NSCLCMANAGEMENT OF MEDIASTINAL LYMPH NODES
Mediastinal lymph node dissection shouldbe performed for all NSCLC patients
At Least 10 Mediastinal lymph nodes fromthree or more stations should be examined
Whitson. ATS. 2007; 84: 1059-65

A PROSPECTIVE TRIAL OF SYSTEMATIC NODAL DISSECTION FOR LUNG CANCER BY VATS: CAN IT BE PERFECT ?
Sagawa. Ann Thorac Surg. 2002; 73: 900-4
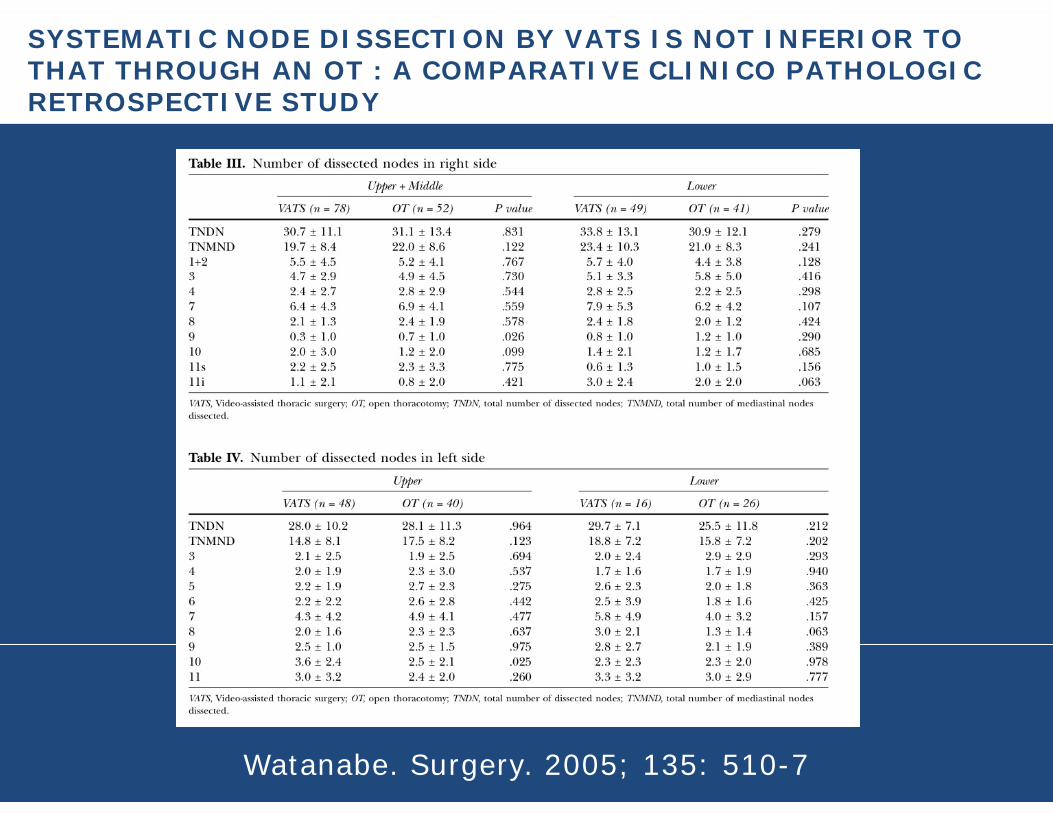
SYSTEMATIC NODE DISSECTION BY VATS IS NOT INFERIOR TO THAT THROUGH AN OT : A COMPARATIVE CLINICO PATHOLOGIC RETROSPECTIVE STUDY
Watanabe. Surgery. 2005; 135: 510-7

VATS LOBECTOMYINTRAOPERATIVE COMPLICATIONS
Koizumi. Ann Thorac Cardiovasc Surg. 2007; 13: 228-35

VATS LOBECTOMYCONVERSION TO OPEN THORACOTOMY
Conversion is not a failure Conversion rate = 1-21 % Conversion Criteria
Inability to find lesion Loss of view
Inability to achieve good lung deflation
Inflammatory disease loss of pulmonary arterial sheath
Uncertain anatomy Major bleeding Unexpected advanced oncologic status

LONG TERM SURVIVAL AFTER VATS VS OPEN THORACOTOMY LOBECTOMY FOR STAGE I NSCLC
Koizumi. Ann Thorac Cardiovasc Surg. 2007; 13: 228-35

VATS VS OPEN THORACOTOMYADVANTAGES OF VATS
Whitson. Ann Thorac Surg. 2008; 86: 2008-18
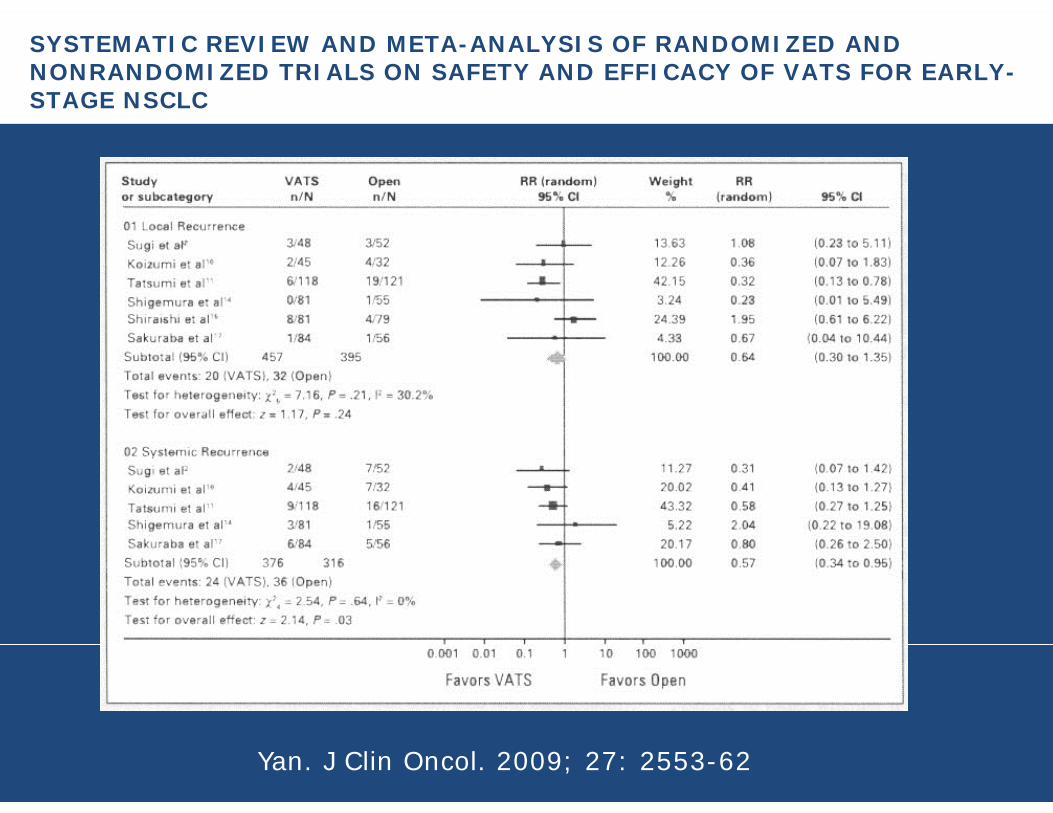
SYSTEMATIC REVIEW AND META-ANALYSIS OF RANDOMIZED AND NONRANDOMIZED TRIALS ON SAFETY AND EFFICACY OF VATS FOR EARLY-STAGE NSCLC
Yan. J Clin Oncol. 2009; 27: 2553-62
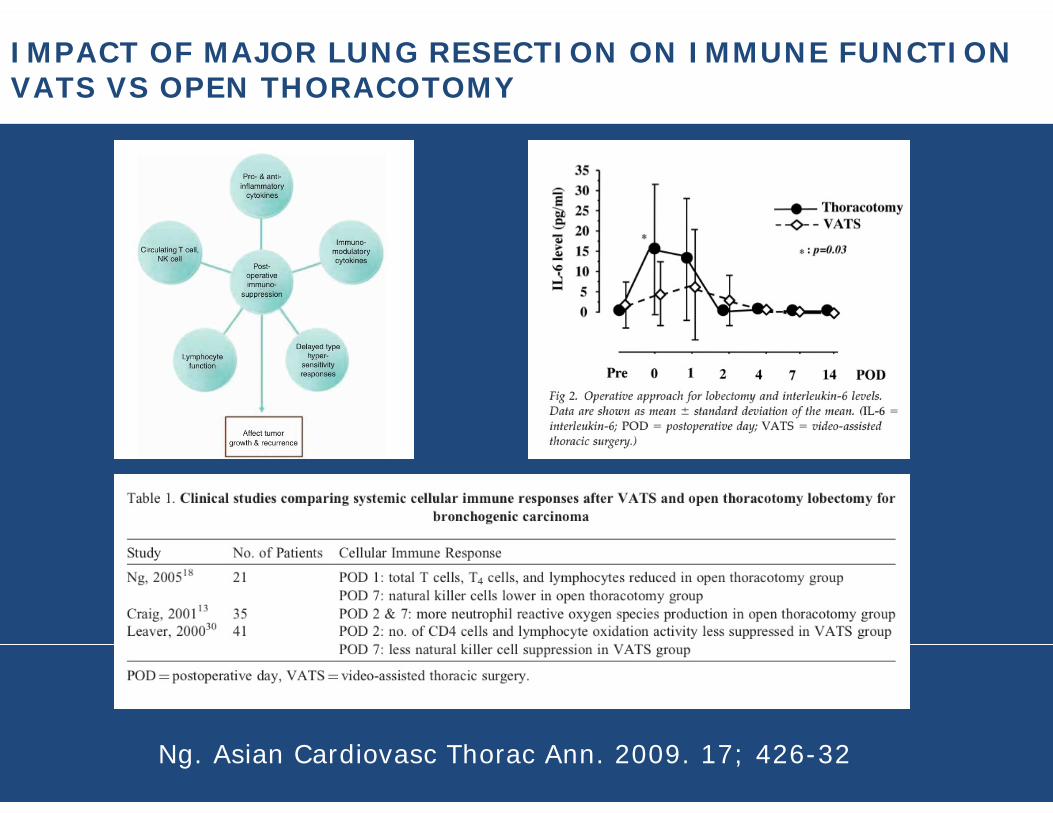
IMPACT OF MAJOR LUNG RESECTION ON IMMUNE FUNCTIONVATS VS OPEN THORACOTOMY
Ng. Asian Cardiovasc Thorac Ann. 2009. 17; 426-32

VATS LOBECTOMY FACILITATES THE DELIVERY OF CHEMOTHERAPY AFTER RESECTION FOR LUNG CANCER
Petersen. Ann Thorac Surg. 2007. 83; 1245-50

VATS VS OPEN THORACOTOMYCOSTS
Nakajima. Cancer. 2000; 89: 2498-2501Casali. EJCTS. 2009; 35: 423-8
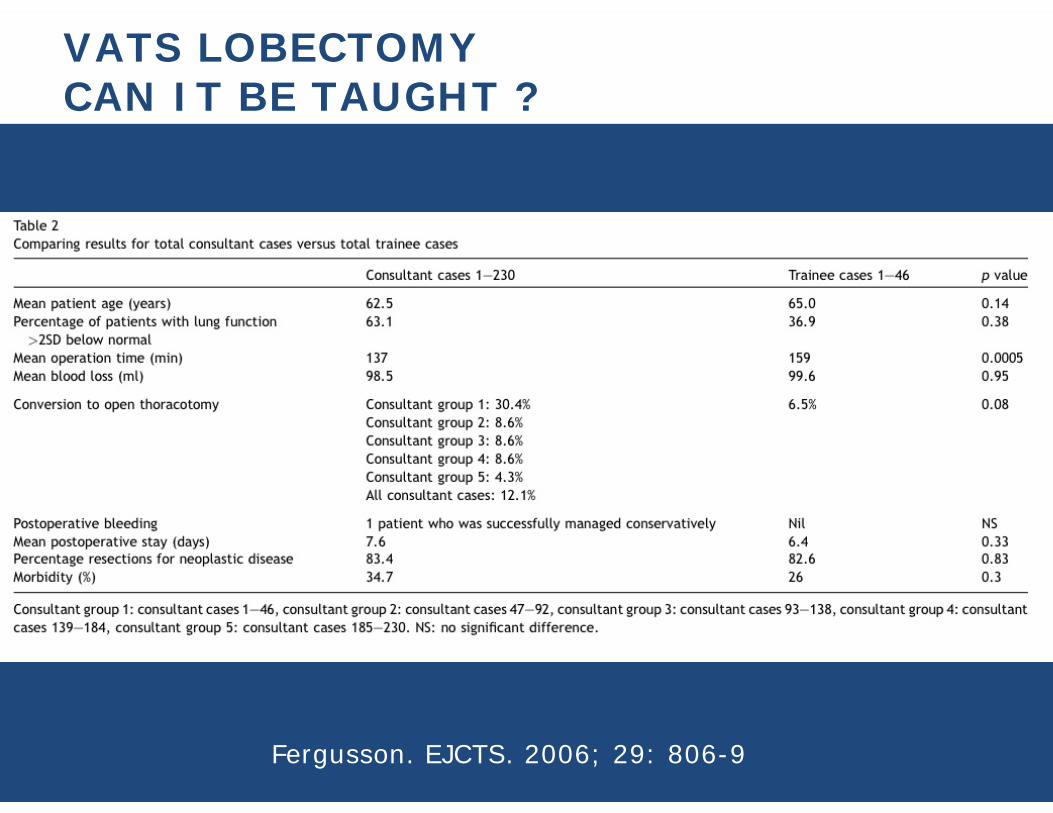
VATS LOBECTOMYCAN IT BE TAUGHT ?
Fergusson. EJCTS. 2006; 29: 806-9
VATS LOBECTOMY - WHO WILL DO IT ?
Major Thoracic interest
Good open thoracic surgical experience High volume thoracic surgeons (>20 resections/year)
Familiarity with hilum dissection
Familiarity with endoscopic surgery
Aptitude (spatial awareness)
Patience
Walker. 2005. 13th meeting of ESTS. Barcelona.
VATSLEFT UPPER LOBECTOMY


VATS LEFTRADICAL
LYMPHADENECTOMY
CONCLUSIONS
VATS Lobectomy is safe and feasible in themanagement of Stage I and II NSCLC
VATS Lymphadenectomy is feasible and aseffective as OT Lymphadenectomy in term of Number of lymph nodes retrieved Number of stations assessed Therefore, concerns about the efficacy of VATS
Lymphadenectomy should not limit the adoptionof VATS Lobectomy
CONCLUSIONS
Oncological principles are preserved Complete lymph nodes dissection could be
achieved There is no difference in term of local
reccurence VATS lobectomy seems to have a beneficial
impact in term of systemic reccurence and long term survival