uterine prolapse (clinical)
TRANSCRIPT

UTERINE PROLAPSE
-NITHIN NAIR

DEGREE OF UTERINE PROLAPSE (CLINICAL)
• FIRST DEGREE: The uterus descends down from its anatomical position (external os at the level of ischial spines) but the external os still remains inside vagina.
• SECOND DEGREE: The external os protrudes outside the vaginal introitus but the uterine body still remains inside the vagina

DEGREE OF UTERINE PROLAPSE (CLINICAL)• THIRD DEGREE: The uterine cervix and
body descends to lie outside the introitus. It is also known as Procidentia or complete prolapse.
Procidentia – Prolapse of the uterus with eversion of entire vagina. It is inevitably associated with cystocele and an enterocele

DEGREE OF UTERINE PROLAPSE (CLINICAL)
NORMAL ALIGNMENT DEGREE OF UTERINE PROLAPSE

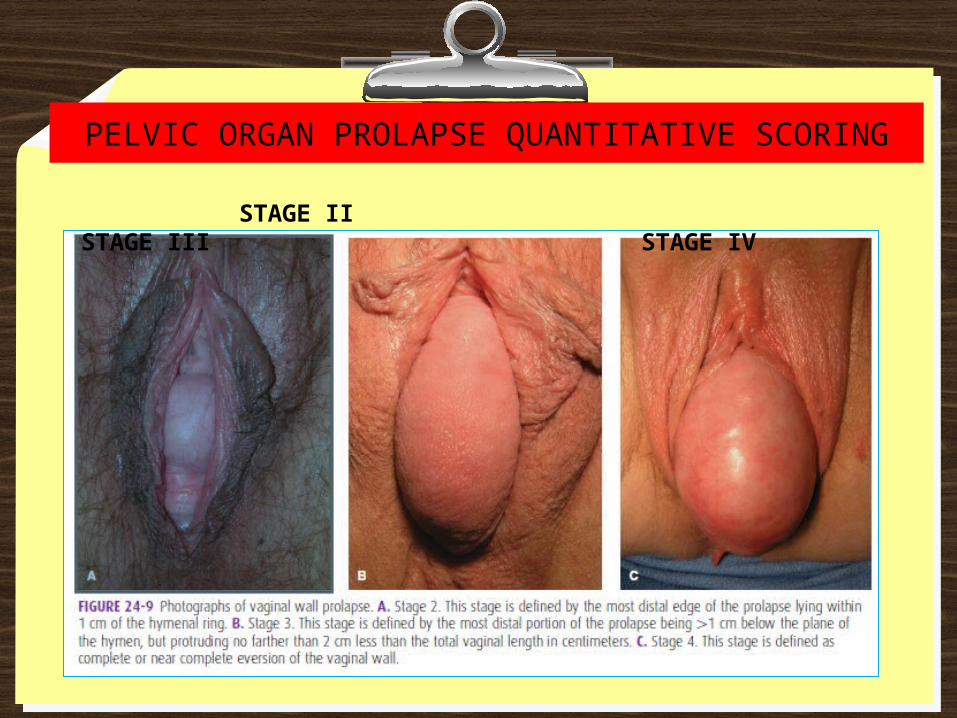
PELVIC ORGAN PROLAPSE QUANTITATIVE SCORING
STAGE
DESCRIPTION
0 No descent of pelvic organs.
I Leading edge of the prolapse remains 1cm or more above the hymenal ring (≤ 1cm.)
II Leading edge of the prolapse extends from 1cm above to 1cm below the hymenal ring.
III From 1cm beyond the hymenal ring but without complete vaginal eversion.
IV Essentially complete eversion of vagina.

PELVIC ORGAN PROLAPSE QUANTITATIVE SCORING
QUANTITATIVE GRADINGS OF PELVIC ORGAN PROLAPSE
PELVIC ORGAN PROLAPSE QUANTITATIVE SCORING
STAGE II STAGE III STAGE IV

SYMPTOMS• Symptoms are variable. Feeling of something coming down per vaginum ⇨
discomfort on walking. Backache or dragging pain in the pelvis Dyspareunia Urinary symptoms : (in presence of cystocele)• Difficulty in passing urine ⇨ elevate anterior vaginal
wall for bladder evacuation• Incomplete evacuation lead to frequent desire to pass
urine• Urgency and frequency of micturition may also be due
to cystitis• Painful micturition is due to infection• Stress incontinence is usually associated due to
urethrocele• Retention of urine

SYMPTOMS
Bowel symptom (in presence of rectocele)• Difficulty in passing stool. Patient has to push
back the posterior vaginal wall in position to complete the evacuation of faeces. Faecal incontinence may be associated.
Excessive white or blood stained discharge per vagina is due to associated vaginitis or decubitus ulcer.

CLINICAL EXAMINATION AND DIAGNOSIS• A composite examination – inspection and
palpation : Vaginal, rectal, rectovaginal

CLINICAL EXAMINATION AND DIAGNOSIS
SPECULUM EXAMINATION

CLINICAL EXAMINATION AND DIAGNOSIS• General examination – details including BMI,
signs of myopathy or neuropathy, features of chronic airway diseases or any abdominal mass.
• Pelvic organ prolapse is evaluated by pelvic examination in both dorsal (lithotomy) and standing positions. The patient is asked to strain as to perform a Valsalva maneuver during examination – helps to demonstrate a prolapse which may not be seen at rest.
• A negative finding on inspection in dorsal position should be reconfirmed by asking the patient to strain on squatting position

CLINICAL EXAMINATION AND DIAGNOSIS• Pelvic organ prolapse is evaluated by
pelvic examination in both dorsal (lithotomy) and standing positions. The patient is asked to strain as to perform a Valsalva maneuver during examination – helps to demonstrate a prolapse which may not be seen at rest.
• A negative finding on inspection in dorsal position should be reconfirmed by asking the patient to strain on squatting position

CLINICAL EXAMINATION AND DIAGNOSIS
STRAINING ON SQUATTING AND DORSAL POSITION

CLINICAL EXAMINATION AND DIAGNOSIS• Anterior and posterior vaginal walls and cervical
descend should be assessed with the patient straining in the left lateral position, using a Sim’s speculum.
• Combined rectal and vaginal digital examination can be an aid to differentiate rectocele from enterocele.

CLINICAL EXAMINATION AND DIAGNOSIS• Levator ani muscle tone is assessed by placing 2
fingers (index & niddle) inside the vagina and the thumb outside. The muscle (pubo-vaginalis) is palpated in lower third of vagina. Patient is asked to squeeze the anus and muscle tone is felt.

INVESTIGATIONS• No essential investigations.• If urinary symptoms persist – urine
microscopy, cystometry and cystoscopy should be considered.
• If renal failure suspected – serum urea, serum creatinine should be evaluated and renal ultrasound performed.