using emrs for pm, pi, pr, and p4p: opportunities and lessons we’re learning randall d. cebul,...
TRANSCRIPT

Using EMRs for PM, PI, PR, and P4P: Using EMRs for PM, PI, PR, and P4P: Opportunities and Lessons We’re LearningOpportunities and Lessons We’re Learning
Randall D. Cebul, M.D.Center for Health Care Research and Policy
Case Western Reserve University atMetroHealth Medical Center
Supported by grant R01-HS015123Agency for Healthcare Research and Quality
Center for
Health Care
Research &
Policywww.chrp.org

What We Thought We Knew
• Claims-based performance measurement (PM) is inadequate, lacking:– Accurate patient assignment for performance
reporting (PR) and P4P– Timeliness for clinical decision support and
performance improvement (PI)– Completeness and efficiency (sampling patients’
charts)– Granularity of measurement – few results– Ability to measure uninsured patients
• EMRs can solve all of these problems

We had friends who thought the same:Views on Accuracy of Performance Measures
Health Aff. 2007; 26: 492-97
30%
88%
85%
82%
38%
35%

There is evidence Re: unstable and untimely There is evidence Re: unstable and untimely assignment of patients using claimsassignment of patients using claims
• ~50% of patients change “assignments” over a 2-year period*.
* Pham etal. Care patterns in Medicare and their implications for Pay for Performance.
NEnglJMed. 2007;356:1130-9.

Some Limitations of Claims Some Limitations of Claims for PM, PR, and PIfor PM, PR, and PI
• PM/PR: Lack reliability of assignment of patient-physician links/related attribution
• Efficiency: Patient exclusions for specific measures/need for costly chart audits
• PI: Long intervals between audit & feedback
• No claims no performance measurement – 47,000,000 uninsured in the U.S.

“EMRs can solve all of these problems” Diabetes Improvement Group – Diabetes Improvement Group –
Intervention Trial (DIG-IT*): OverviewIntervention Trial (DIG-IT*): Overview
• Commercial EMR-facilitated: – study design– patient assignment/PCP attribution– PM: performance measurement– PI: real-time clinical decision support – PI: Nurse Case Management
*Funded, in part, by grant R01-HS015123Agency for Healthcare Research and Quality
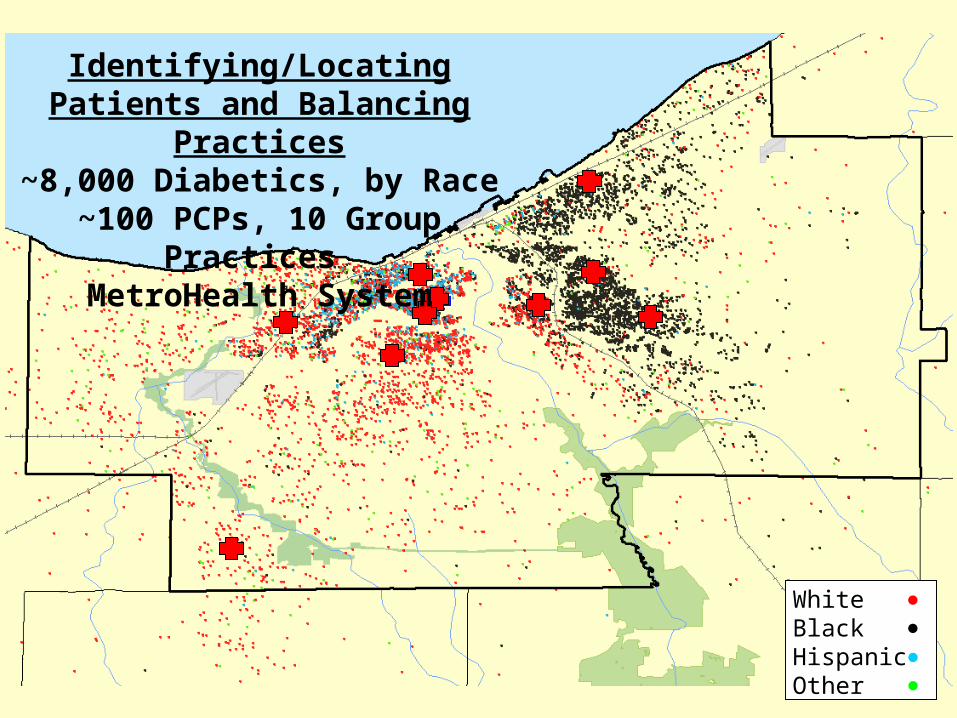
White BlackHispanicOther
Identifying/Locating Patients and Balancing Practices
~8,000 Diabetics, by Race~100 PCPs, 10 Group Practices
MetroHealth System

Random Assignment of Balanced Practices Random Assignment of Balanced Practices
5Groups
5GroupsDM2
Epic
Only
10 Practices, ~100 PCPs, ~8000 Patients
Primary Aims: Quality & Utilization (including sub-groups by insurance etc)
Secondary Aims: Adoption/Correlates; Unintended Consequences

““Table 1”. Pre-trial Characteristics of Table 1”. Pre-trial Characteristics of Practices after BalancingPractices after Balancing
0.228<0.001-0.57-0.66Slope A1c
0.392<0.00119.618.5% on Insulin
0.1380.00116.918.7% A1c>9
0.859<0.001136.2136.1Ave Syst BP
0.0490.00122.625.2% Smoker
0.830<0.00149.148.7% A-A
20252281# of Pts
55# of Practices
P-ValueICCGroup B Group AVariable

EMR-Based Patient Assignment EMR-Based Patient Assignment
• Patient Eligibility:– Diagnosis: ICD-9 codes or antidiabetic meds
• PCP Links/Attribution:– Two or more eligible patient visits with PCP– Initialization of Lists: PCP can report:
• “Not my patient” or “Not Diabetic”• Conflicts adjudicated (<.1%)
– Weekly Updating: • New patients• Transfers within or across practices• No complaints

PM/PI/PR - Clinical Decision PM/PI/PR - Clinical Decision Support (“DMSupport (“DM2”2”))
• Alerts and Linked Order Sets
• Patient and Physician Education
• Patient Lists/Registry, Current Status
• Practice panel performance feedback
Practice Panel Tools

PM/PI - encounter-based Alerts: PM/PI - encounter-based Alerts: Designed to Minimize FPsDesigned to Minimize FPs
What do we know about this patient?What do we know about this patient?• She has diabetes and is visiting her PCP• Her kidneys are leaking protein.• She is not on an ACE inhibitor or ARB
and has no documented allergies to them.
• She has no other contraindications (K, Cr)• There are several alternative drugs/doses
{Links to Automated Order Set}

PI - SmartSet PI - SmartSet Linked to ACE/ARB AlertLinked to ACE/ARB Alert
Patient name
Patient name
Re-cap of indications
Choice of Rxs/doses
Follow-up testing

PI/PR - Practice Panel: Comparative PerformancePI/PR - Practice Panel: Comparative Performance
“My panel” vs. Comparator
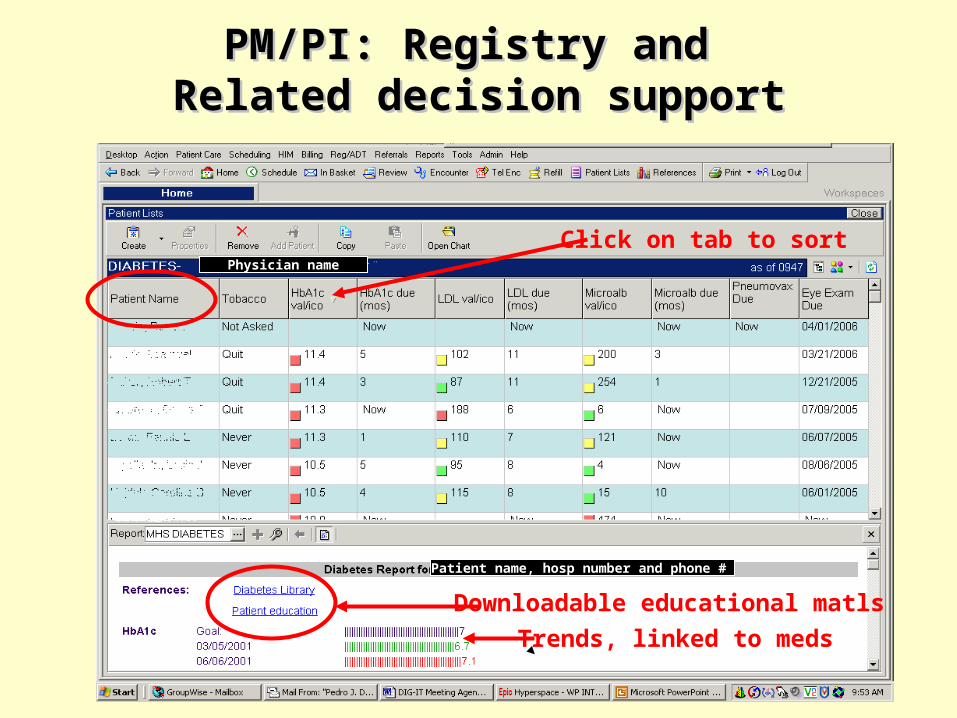
PM/PI: Registry and PM/PI: Registry and Related decision supportRelated decision support
Physician name
Patient name, hosp number and phone #
Click on tab to sort
Downloadable educational matls
Trends, linked to meds

Illustrative PM:Illustrative PM:“ADA Scores” Measured Every Week“ADA Scores” Measured Every Week
Clinical Outcome: Change in ScoresAce/ARB* 1Pnvx* 1Eye Exam* 1LDL<100* 1
A1C<7% 1BMI<30 1Non-Smker 1SBP<130 1
0-8 points
“MD-Centric”Measures

Changes in Scores, Exptl Pts (n=5288)Some Measures are Easier To Change than Others
Percent ADA Score by Patient Week
Overall ADA MD-Centric ADA
40
45
50
55
60
65
70
75
80
Patient Week0 10 20 30 40 50 60 70 80 90 100
% of All ADA Measures Met% of All ADA Measures Met
% of 4 MD-Centric Measures Met% of 4 MD-Centric Measures Met

EMRs can Measure Performance in All Patients
• Baseline Trial Data by:– RACE– Insurance

PM/PR/P4P: Poor Glucose Control by Race/ethnicity in One System
• Poor glucose control is strongly associated with diabetic complications– Eyes, kidneys,
amputations, admissions • P4P programs reward
practices with lower than 20% “poor values”
• More than half of our diabetic patients are Black or Hispanic
15.7%
21.9%23.3%
White Black Hispanic 1 '0
5
10
15
20
25
Perce
nt wi
th Po
or Gl
ycem
ic Co
ntrol
15.7%
21.9%23.3%

Poor Glucose Control by Insurance
At baseline:• 25% of our Medicaid
pts were in poor control.
• Almost 30% of our uninsured pts were in poor control.
• About 40% of our patients are uninsured or covered by Medicaid
25.0%
20.2%
11.2%
29.2%
11.2
20.2
25.0
29.2

EMRs for PM, PR, PI, P4P:Some Summary Thoughts
• Using EMR-centered data, we can:– Identify and link patients satisfactorily– Identify patients pretty well for whom measures are
appropriate (eg, no c/I to ACE/ARBs)– Measure performance at a granular level (eg, BMI, A1c)– Measure performance on all eligible patients, regardless
of race or insurance status– Monitor and provide meaningful feedback in a timely way– Measure improvement in process and outcomes
• Some measures are harder to improve than others• P4P systems should consider stratifying by
insurance, at least.
Additional Questions About PM/PR/P4P
• Are Our Data Complete?– NO
• Are There Biases in Our Data?– Probably, yes– Mostly Under-ascertainment (of good performance as
well as undesirable outcomes)
• Absent full regional HIE, are EMR-based system-level data Fair for P4P?– For within system PI and P4P, probably– For cross-system comparisons, it depends

Incomplete PM with EMRs alone: Depends on size, financing, functions
“HMO” or Very LgIntegrated System:Not missing much
Lg System butNo eRx Fncs:
Missing Filled Rxs,Out of system use
Small practice:Missing alot

HMO vs. Large System with Itinerant Patients
- Who’s missing data?
36.437.697.9Eye Exam, Last Yr
74.279.786.5Non-Smokers
92.096.969.7ACE/ARB if alb’inuria
84.886.156.4Pneumovax, ever
49.451.248.5LDL < 100 mg/dl
45.645.336.1Systolic BP < 130
56.1%59.9%44.2%A1c < 7%
8,0905,00211,849# of Patients
MHS Total
MHS Comm’cial + MedicareHMOStandard
All outside eye exams are billed

HMO vs. Large System without eRx Functions- Who’s missing data?
36.437.697.9Eye Exam, Last Yr
74.279.786.5Non-Smokers
92.096.969.7ACE/ARB if alb’inuria
84.886.156.4Pneumovax, ever
49.451.248.5LDL < 100 mg/dl
45.645.336.1Systolic BP < 130
56.1%59.9%44.2%A1c < 7%
8,0905,00211,849# of Patients
MHS Total
MHS Comm’cial + MedicareHMOStandard
Filled Prescribed

Where are the needed performance data?
• Outside the System (benefit from claims)– Eye Exams, Labs, Pharmacies, ED Visits/admissions
• In the System, but relatively inaccessible– Text portions of record
• Performance completed outside, noted• Patient exclusion for measure, but not in “check box”
– Unlinked computerized systems; e.g.• Echo lab – HF• ETTs – CAD• PFTs – asthma
• Or, they don’t exist…

Closing Thoughts: Measurement Challenges Closing Thoughts: Measurement Challenges Using EMRs for P4P (before HIE…)Using EMRs for P4P (before HIE…)
• We need to better capture exclusions: eg terminal patient, refusal, relative C/I, etc
• We need to better capture necessary ancillary data: e.g., echo’s, PFTs, etc
• We need simpler means to identify [necessary measures] obtained out-of-system– Insured patients’ claims? – What about Uninsured patients?
