using a brief solution focussed approach with children in care
TRANSCRIPT
Using a brief solution focussed
approach with children in care: An
evaluation of the NSPCC Face to
Face service
Prakash Fernandes and Louise Bazalgette
• 45% of children in care have a mental disorder (Meltzer et al, 2003); a rate that is four times higher than children in the general population (Ford et al, 2007)
• The mental health needs of children in care are frequently unmet due to:o A lack of routine assessmento Ineligibility for support (e.g. not meeting diagnostic criteria/ child is not in a
stable placement)o Waiting lists for CAMHS and inaccessible services.
• NSPCC research conducted by The Who Cares? Trust with children in care found they wanted:o Face to face support in a venue that was “not like an office”o An accessible locationo Support from a person who would “understand and not judge”o A confidential service that was “not a big heavy thing” and would make
them “feel happier”2
Why a new service for LAC
The Face to Face model
• Aimed at young people aged 5-18 (in care or on the edge of care)
• Solution Focused Brief Therapy as the method of intervention
• Supporting the child/young person to identify their skills and strengths
• Child/ young person-led approach (their issue)
• A timely and responsive service – aim to respond within 24 hours
• Brief intervention – up to 8 sessions.
• Flexibility: the child or young person decides frequency and location of sessions
Referral pathways:
• Referral by a professional or self-referral
Access and reach:
• The service has been offered in 18 locations in England, Wales and N. Ireland
• 1,543 young people accessed the service between September 2011 and February 2015.
3
Service Development

Evaluation
• The Outcome Rating Scale to measure change for young people• To measure ‘quality of life’ changes not change in just ‘symptoms’ • To give young people control in defining the changes experienced
• Follow up data after 3 months using the ORS and a questionnaire
• Questionnaires at the first and last session
• Interviews with children and foster carers at the end of the service
• Focus groups with practitioners
• Interviews with referrers
5
Evaluation Design
6* ( a change of 5 points or more is defined by the authors of the scale as reliable change)
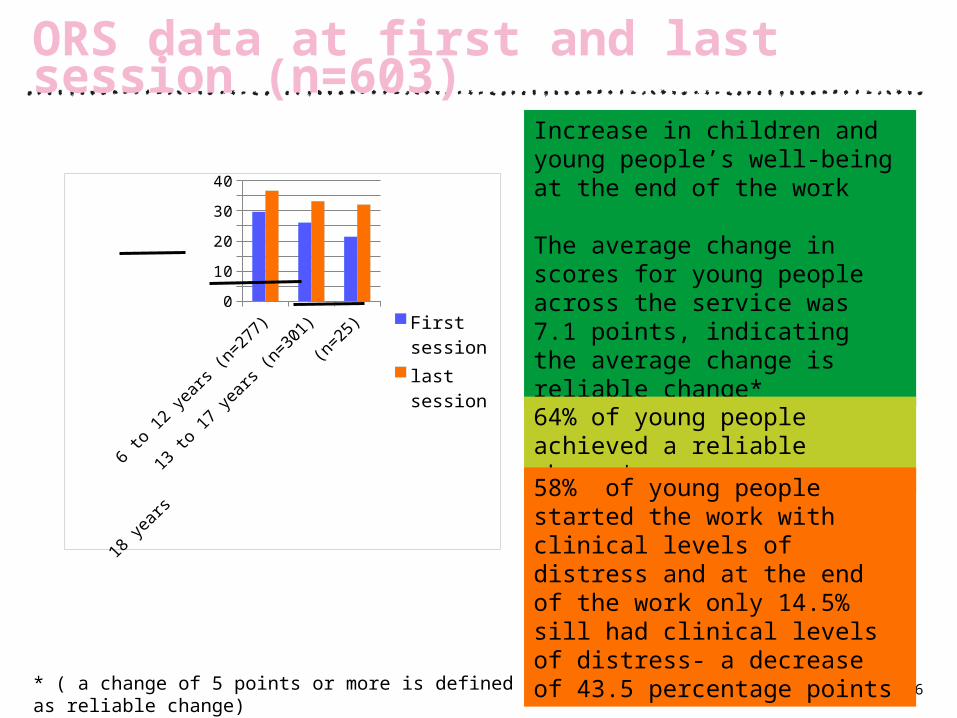
ORS data at first and last session (n=603)
6 to 12 years
(n=277)
13 to 17 years
(n=301)
18 years (n=25)
0
5
10
15
20
25
30
35
40
First sessionlast session
Increase in children and young people’s well-being at the end of the work
The average change in scores for young people across the service was 7.1 points, indicating the average change is reliable change*
64% of young people achieved a reliable change*
58% of young people started the work with clinical levels of distress and at the end of the work only 14.5% sill had clinical levels of distress- a decrease of 43.5 percentage points
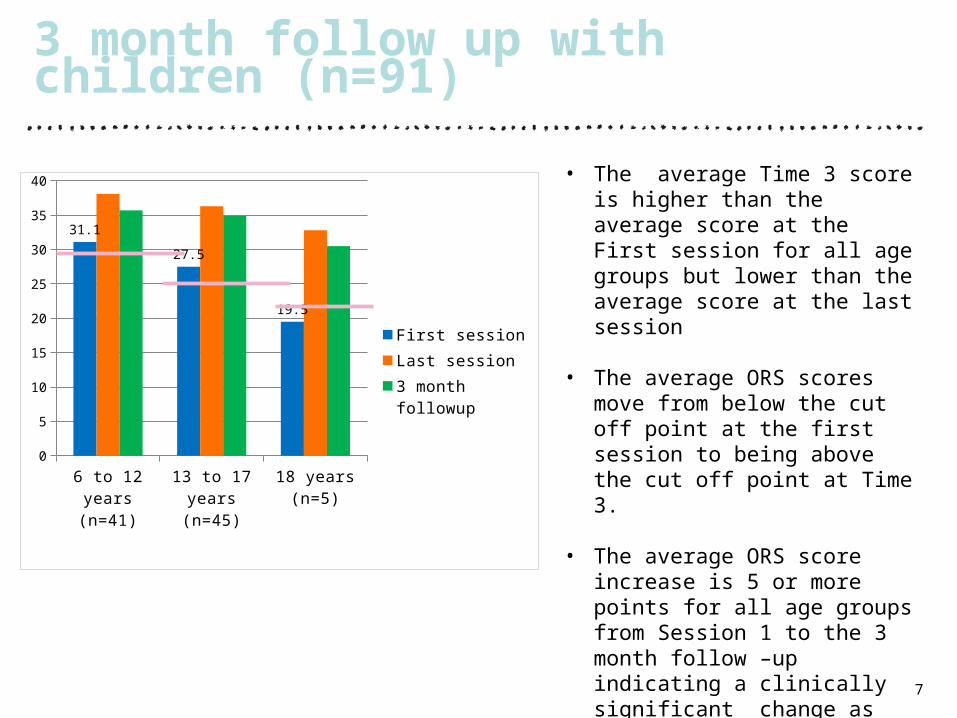
3 month follow up with children (n=91)
7
6 to 12 years (n=41)
13 to 17 years (n=45)
18 years (n=5)0
5
10
15
20
25
30
35
40
31.1
27.5
19.5 First sessionLast session3 month followup
• The average Time 3 score is higher than the average score at the First session for all age groups but lower than the average score at the last session
• The average ORS scores move from below the cut off point at the first session to being above the cut off point at Time 3.
• The average ORS score increase is 5 or more points for all age groups from Session 1 to the 3 month follow –up indicating a clinically significant change as defined by the authors of the scale
Helped a lot (%)
Helped to some
extent (%)
No difference
(%)
Did not help
(%)
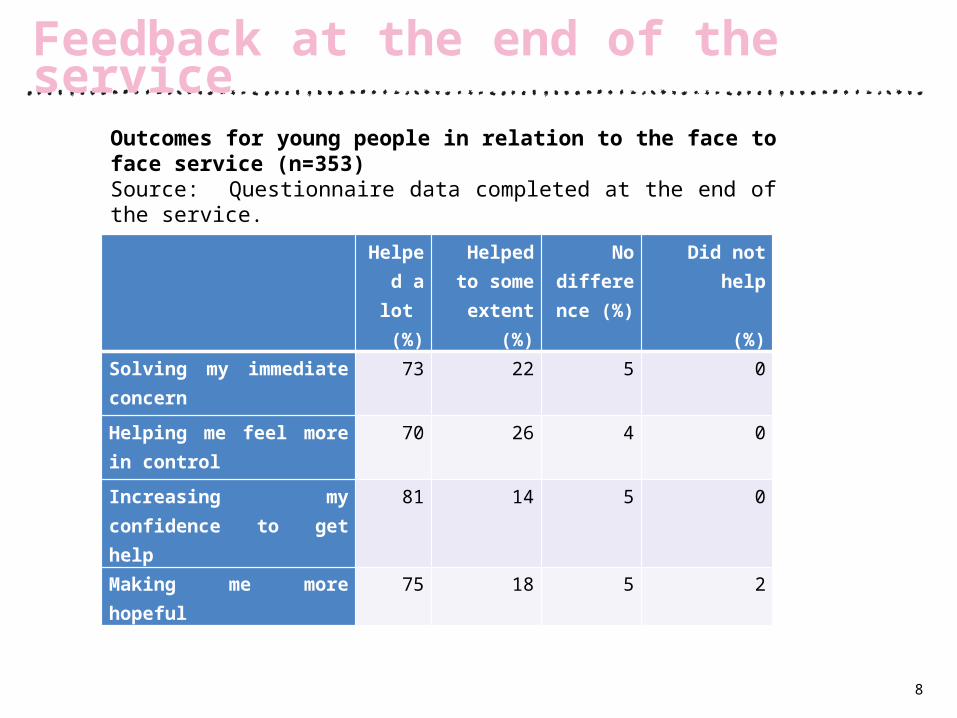
Solving my immediate concern 73 22 5 0
Helping me feel more in control
70 26 4 0
Increasing my confidence to get help
81 14 5 0
Making me more hopeful 75 18 5 2
8
Feedback at the end of the service
Outcomes for young people in relation to the face to face service (n=353)Source: Questionnaire data completed at the end of the service.
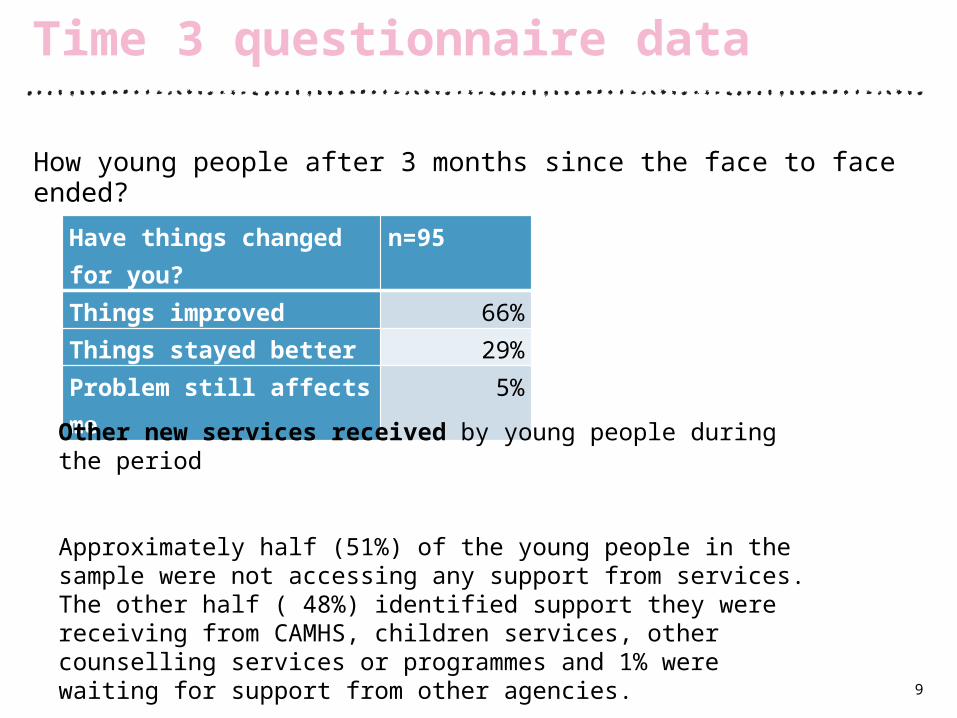
How young people after 3 months since the face to face ended?
9
Time 3 questionnaire data
Have things changed for you? n=95Things improved 66%Things stayed better 29%Problem still affects me 5%
Other new services received by young people during the period
Approximately half (51%) of the young people in the sample were not accessing any support from services. The other half ( 48%) identified support they were receiving from CAMHS, children services, other counselling services or programmes and 1% were waiting for support from other agencies.

Interviews with children
• Increased confidence
• Managing anger
• Better relationships ( with family and peers)
• Better Learning at school
• More positive outlook to life
• Greater confidence to seek help
11
Types of changes for young people
Just I feel a better person just now I
can talk more to people. If I had
something bothering me I an go
and talk to them because before I
couldn’t have done that because I
would have felt nobody’s
listening, who cares? But now I
know there's people out there that
do care and do want to help me.
So I feel a better person for
managing to talk.

• Making them feel good about themselves
• Focussed on a key issue
• Rehearsing different ways of doing things
• Helping young people look ahead and ‘let the past go’
• Scaling questions to sustain change
• Relationship : made me laugh, persistence, just gets it, face to face
• Being in control
12
How Face to Face helped them achieve change
Because if someone else has
said, you know, “Right go and
do this. Go and talk to this
person.” Then you'll feel
pressurised and you don’t want
to, you’re scared, whereas if
you’re thinking and you’re
thinking to yourself, ‘I could do it
myself,’ then you find you make
it easier for yourself.

How face to face is different from other services
• Focused on strengths
• Practical
• Independent
• Helps ‘prevent, problems
13
Like sometimes we just do like he’ll become the social worker and I’ll try to talk to him and we do it like that. My feelings are never really changed but I think slowly – he gives me ways to talk to them, which makes me kind of get somewhere without getting angry . Before when I got angry, I would swear and just lose my temper but he’s given me like techniques to talk to them ( social workers) in like the appropriate way that makes them listen.
• Too much talking: would have liked more activities, drawing things
• More involvement from fostercarers /family would have been helpful for some sessions
• More information about the service at the beginning of the work
• Length of sessions could have been longer
• Meeting in different venues such as the park or café may help some children
14
Barriers to achieving change

Facilitators and Barriers:Practitioners and Referrer perspectives
• Child centred approach
• Child/young person defining the problem, separating the professional goals
• Listening- to use language of child
• Children in control
• ‘Time limited nature of the approach
• Beginning work with a clear outcome
• Lends itself to more focussed inter agency working
• Solution focussed approach
• Focus on the positives and their interests
• Techniques of best day, preferred future and scaling – powerful tools to think about change
16
Key aspects of the model that facilitated change
• Building rapport with the child to gain trust seems rushed to finish in eight session
• Younger children or children with learning difficulties struggle with some aspects of the model- scaling and preferred future
• Young people having ‘unachievable’ goals
• Unstable placements at time could limit engagement of the young person in the work
17
Barriers to helping children achieve change
• 64% of young people had experienced a reliable change of 5 points or more on the ORS
• Only 14.5% of young people were still experiencing clinical levels of distress by the end of the work
• 3 months after the work had ended, 95% of young people said things had continued to improve or had stayed better
• Young people and practitioners were able to articulate clear benefits of this way of working
18
Summary
Knowledge transfer strategy: Making Face to Face more widely available
• Final evaluation report will be published (June 2015)
• Practice toolkit and implementation pack for commissioners, to be made freely available (June 2015)
• Supporting the scale-up of this service with other providers (including statutory and voluntary sector)
For more information please contact:
Louise Bazalgette
Development Manager
020 3772 9030
19
Next steps
Fernandes, P. (April 2014), ‘Face to Face Service Impact and Evidence briefing: Interim Findings’, London: NSPCChttp://www.nspcc.org.uk/globalassets/documents/evaluation-of-services/face-to-face-interim-report.pdf
Ford, T., Vostanis, P., Meltzer, H., & Goodman, R. (2007). Psychiatric disorder among British children looked after by local authorities: Comparison with children living in private households. British Journal of Psychiatry, 190, 319-325.
Meltzer, H., Gatward, R., Corbin, T., Goodman, R., Ford, T. (2003) ‘The mental health of young people looked after by local authorities in England’, The Office for National Statistics, London: The Stationary Office.
20
References
21
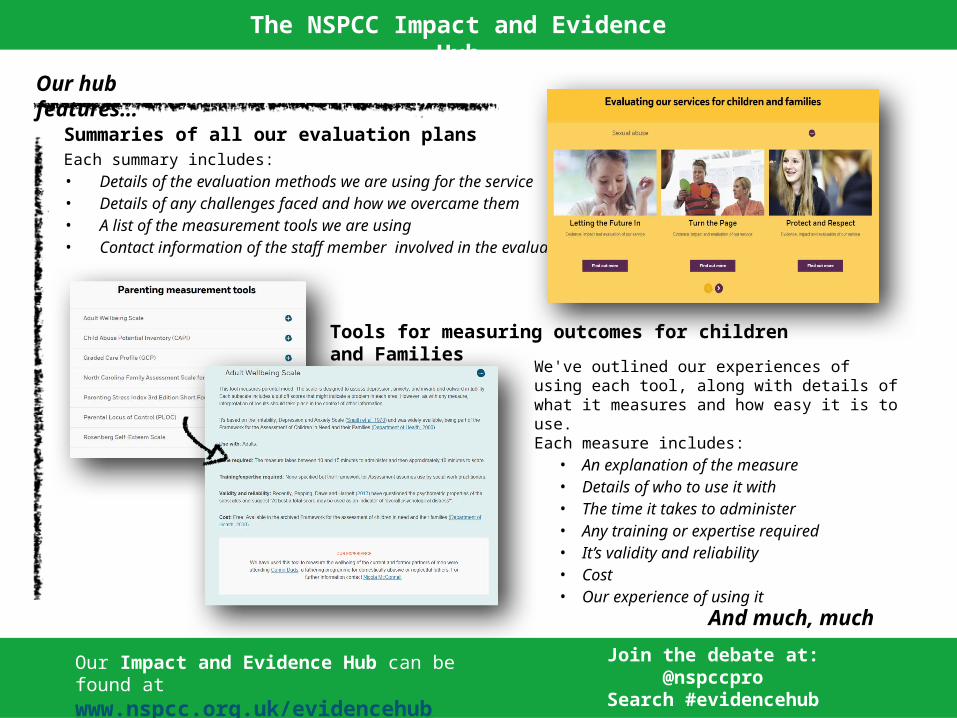
Summaries of all our evaluation plansEach summary includes:• Details of the evaluation methods we are using for the service• Details of any challenges faced and how we overcame them• A list of the measurement tools we are using • Contact information of the staff member involved in the evaluation
Tools for measuring outcomes for children and Families We've outlined our experiences of using each tool, along
with details of what it measures and how easy it is to use.Each measure includes:
• An explanation of the measure• Details of who to use it with• The time it takes to administer • Any training or expertise required • It’s validity and reliability • Cost• Our experience of using it
And much, much more….
Our Impact and Evidence Hub can be found at www.nspcc.org.uk/evidencehub
Join the debate at:@nspccpro
Search #evidencehub
Our hub features…
The NSPCC Impact and Evidence Hub