uric acid and ckd - nyu langone health · pdf fileuric acid and ckd sonika puri . uric acid...
TRANSCRIPT

URIC ACID AND CKD SONIKA PURI

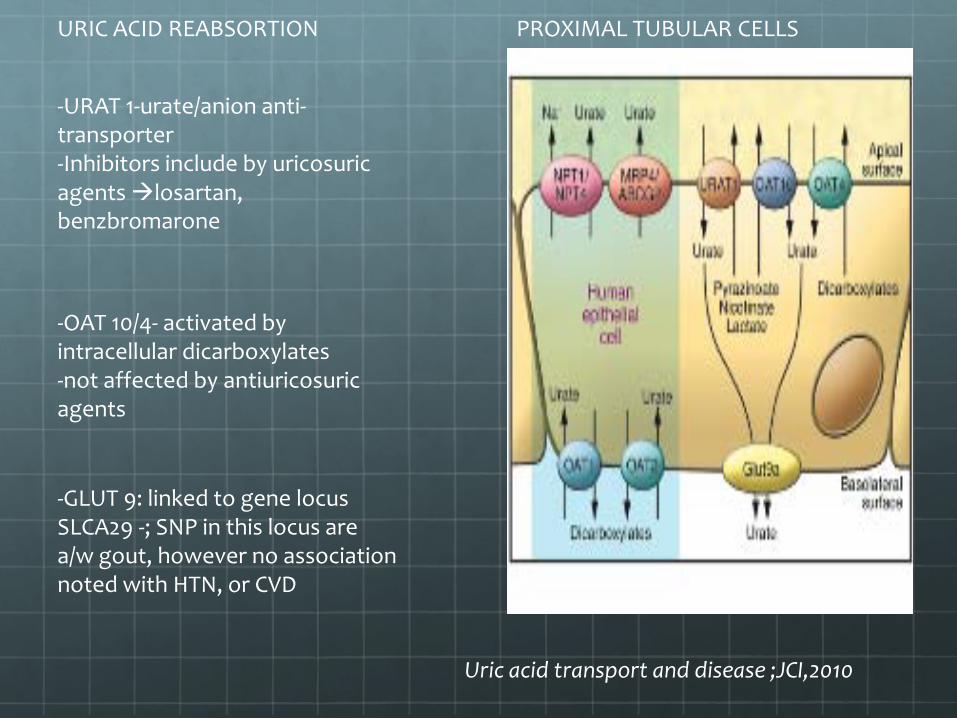
Uric acid transport and disease ;JCI,2010
Uric acid transport and disease ;JCI,2010
-URAT 1-urate/anion anti-transporter -Inhibitors include by uricosuric agents losartan, benzbromarone
PROXIMAL TUBULAR CELLS
-OAT 10/4- activated by intracellular dicarboxylates -not affected by antiuricosuric agents
-GLUT 9: linked to gene locus SLCA29 -; SNP in this locus are a/w gout, however no association noted with HTN, or CVD
URIC ACID REABSORTION

URIC ACID EXCRETION
-MRP4 and ABCG 2 –ATP dependant urate extrusion
-OAT1/3 –dicarboxylate/UA antitransporters

A: peroxinitrite can block tetrahydrobiopterin (HB4) which is a cofactor necessary for action of NOS. B:Uric acid prevents copper induced oxidation of LDL which may prevent against athersclerosis. C: Proinflammatory actions of UA- in vascular sm cells, adipocytes.
UA – PROINFLAMMATORY/ ANTI INFLAMMATORY

URIC ACID AND HTN Historically in 1800s Frederick Mohamed made an observation that many hypertensives came from gouty families .
1960s-1970s observations were made that hyperuricemia was present in 5%-6% of general population ; however elevated uric acid levels were seen in 40%-60% of hypertensive patients .
Debate : Hyperuricemia seen in hypertension is merely an association vs .causality
Hypertensive phenotype a/w other variables such as diuretics use, obesity, renal dysfunction which can independantly affect serum UA levels.
Johnson et al, Hypertension 2005


Elevated bp induces hypertension in rats , Mazzali et al, HYPERTENSION 2001


Sachez-Lozada et al; KI 2005


-125 patients age 6-18yrs referred for evaluation of HTN -40 normotensive controls who were referred for proteinuria, enuresis or hematuria

Feig ; Hypertension, 2003

Feig et al, NEJM 2008

Ua and CKD Conflicting data regarding role of hyperuricemia in progression of ckd .
Evidence that hyperuricemia affects progression of IgA nephropathy

ARIC study – 1987-1989
15,792 participants; age 45-65yrs
Mean follow up of 4-5yrs
Baseline S.cr measured for 99%pts
Outcome: Incident kidney disease- egfr decrease <15ml/min/1.73 m2/ final egfr <60ml/min
CHS study -1989-1990
5201 participants, age >65yrs
Additional 687 AA patients between 1992-1993; excluded d/t limited fup.
Baseline s.cr measured in 97% patients
Follow up for 5 years
Weiner et al, JASN 2008




-MDRD study : 1989-1994;randomized- 840 individuals with ckd (s.cr 1.2-7 in women, 1.4-7 in men effect of strict bp control and effect of dietary protein restriction -All cause mortality, cv mortality and kidney failure (dialysis or transplant) Fup till Dec 2000.
Madero et al, AJKD 2010

-Model 1- adjusted for age -Model 2-age + cvd risk factors -Model 3 Model 2 + egfr+ proteinuria -Model 4 Allopurinol use

UA and Type 1 DM
-Single centre study of 263 patients with type 1 DM (1979-1984), median fup on 18years -data collected 3 yrs after onset of dm—normotensive (except 3- ace/diuretic); w/ normoalbuminuria -normal uric acid 200-450 micromol/l in mean, 130-350 micromol/l in women -72 patients developed microalbuminuria 23 progressed to macroalbuminuria (12%)

-normoalbuminuria vs microalbuminuria :no difference found in mean +/- standard deviation in uric acid levels -based on single measurement of uric acid levels Hovind et al, Diabetes 2009
Serum uric acid as a predictor of development of Diabetic nephropathy in Type 1 DM

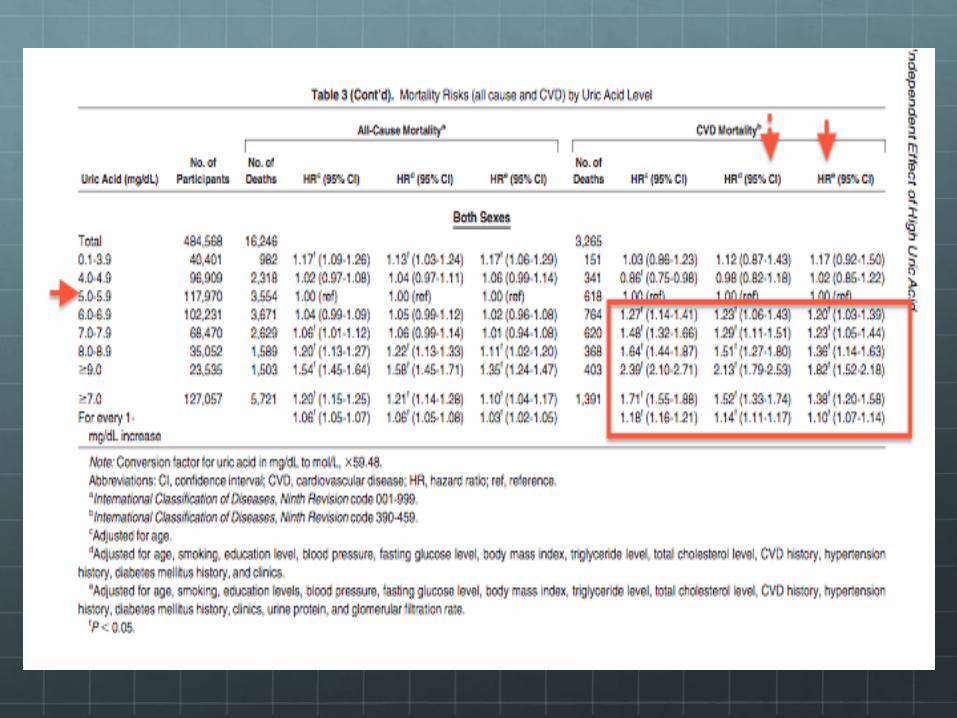
UA AND CVD Taiwanese study- 484,568 men and women , >20yrs age, followed since 1994
2 or more clinic visits
Questionnaire regarding medical history, lifestyle and demographics along with appropriate lab work.
Mean follow up of 8.5yrs.
OVERT CVD RISK FACTORS
-- 1 or more of the following
--DM/HTN/ obesity bmi>25, hyperTG
PRE-CVD RF
--preHTN (sbp 120-139), preDM or borderline high tg (150-199mg/dl)



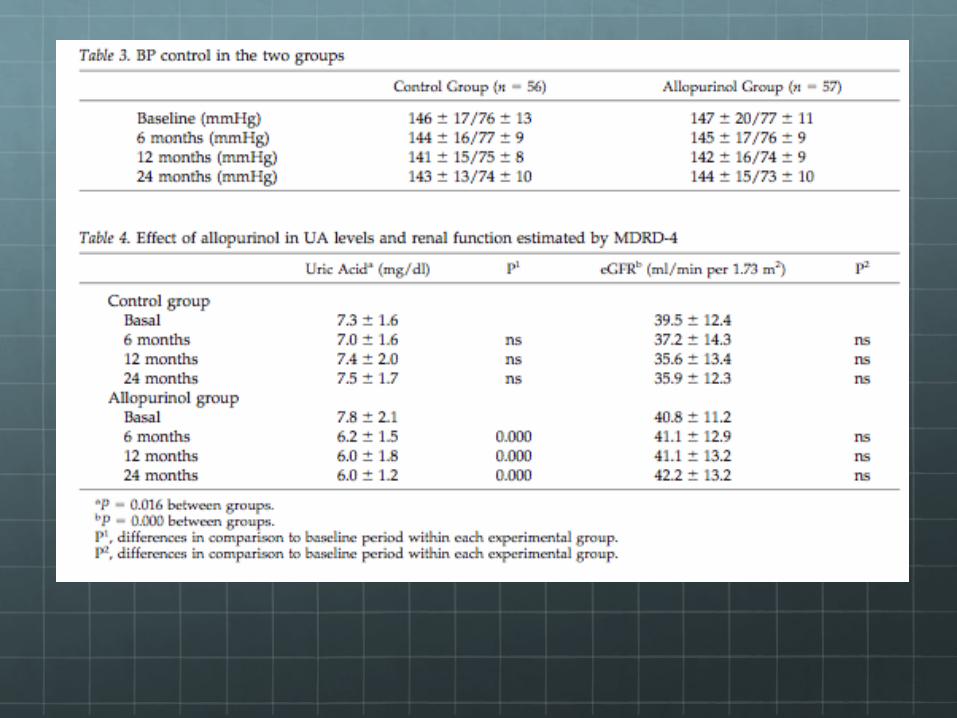
112 eligible patients w/ egfr <60cc/min-Randomization allopurinol : 57 ( 51)patients Control group: 56 (47) patients
Goicoechea et al, CJASN 2010
Renal function measured at baseline, 6,12 and 24 months
Mean time to followup 23.4 +/- 7.8 months
OUTCOMES
1) HOSPITALIZATIONS 2)CV EVENTS 3) ESRD requiring HD
4) MORTALITY
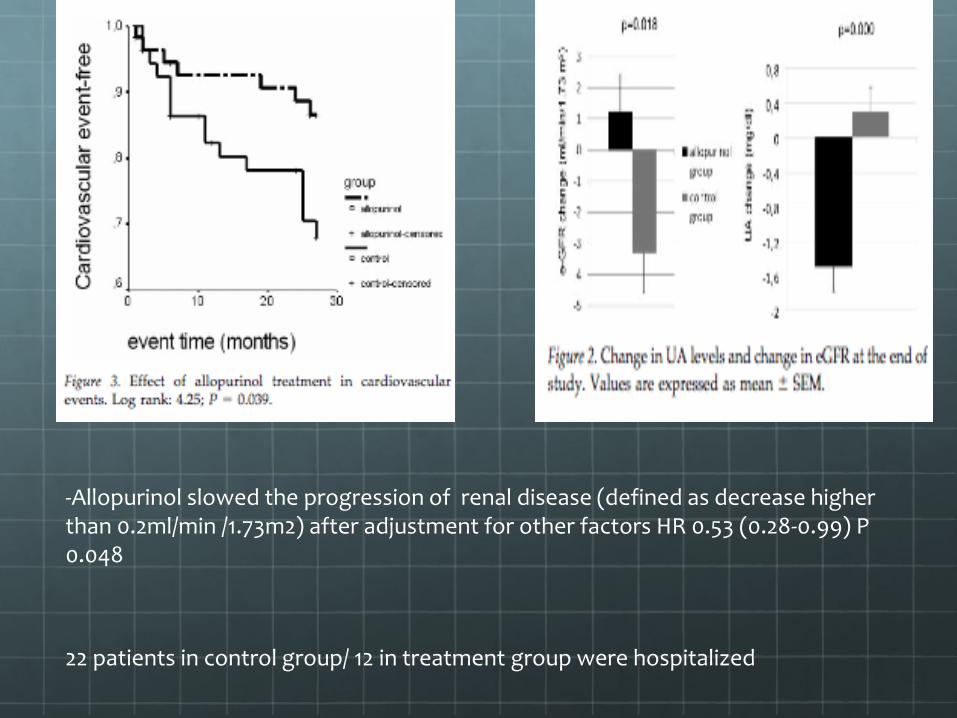
-Allopurinol slowed the progression of renal disease (defined as decrease higher than 0.2ml/min /1.73m2) after adjustment for other factors HR 0.53 (0.28-0.99) P 0.048
22 patients in control group/ 12 in treatment group were hospitalized


Feig et al ,JAMA 2008
-30 ADOLESCENTS AGE 11-17YRS , new diagnosed essential htn, no prior treatment -randomized,double blinded ,placebo controlled. -use ambul/office bp monitoring - cross over study 15 each received 200mg bid x 4 weeks, washout period of 2 weeks , cut off uric acid >6.0
Effect of allopurinol in bp of adolescents
2 randomized , double blinded ,placebo-controlled crossover studies performed for one month on pts with NYHA 2/3 comparing placebo, allopurinol 300mg daily and 600mg daily; 2nd study placebo vs probenecid 1000mg
Endothelial function as measured by venous forearm blood flow plethysmography- sodium nitroprusside, acetycholine and acetylcholine with vitamin c (25mg/ml)
30 patients were given medication/placebox 4 weeks, fasting samples
Similar uric acid reduction was achieved with probenecid and


