updated guideline of glycoprotein iib/iiiainhibitor for...
TRANSCRIPT

Updated Guideline of Glycoprotein IIb/IIIa Inhibitor
for Acute Coronary Syndrome
1
YoungYoung--Hak Kim, MD, PhDHak Kim, MD, PhD
Heart Institute, Heart Institute, AsanAsan Medical Center, Medical Center, University of Ulsan College of Medicine, Seoul, KoreaUniversity of Ulsan College of Medicine, Seoul, Korea

Disclosure InformationDisclosure Information
Honorarium from Handok Corp

Acute Coronary Syndrome
Clinical Classification of ACSClinical Classification of ACS
No ST Elevation
Unstable Angina
ST Elevation
STEMI
Hx
EKG
Cardiac Biomarker
Final Dx
Non-STEMI
3
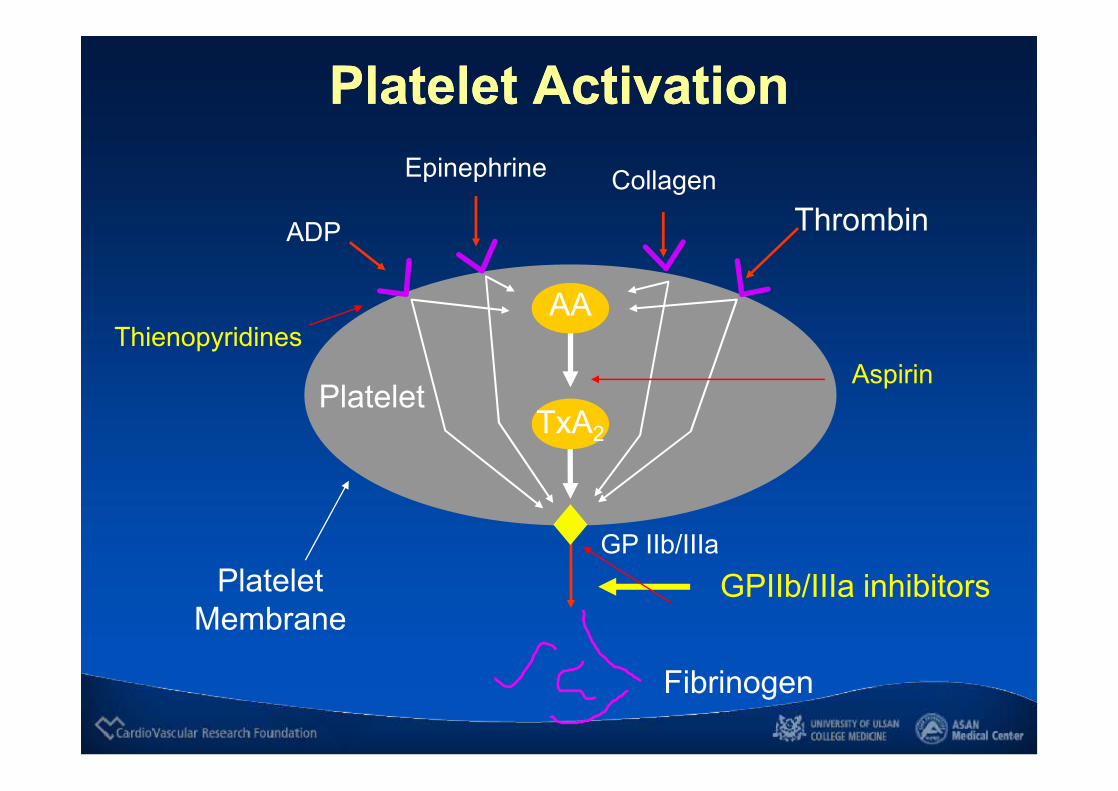
Platelet ActivationPlatelet Activation
PlateletAspirin
Epinephrine
ADP
CollagenThrombin
Platelet Membrane
GP IIb/IIIa
Fibrinogen
AA
TxA2
GPIIb/IIIa inhibitors
Thienopyridines

ll ThrombinThrombin
ll SerotoninSerotonin
ll ADPADP
ll TXATXA22
ll OthersOthers
Target Sites of Antiplatelet TherapyTarget Sites of Antiplatelet Therapy
DirectDirectAntithrombinsAntithrombins
Disruption ofDisruption ofEndotheliumEndothelium
PlateletPlateletAdhesionAdhesion
PlateletPlateletActivationActivation
PlateletPlateletReleaseRelease
PlateletPlateletAggregationAggregation
Prostaglandins Prostaglandins
GPlb/vWFGPlb/vWFAntagonists,Antagonists,DipyridamoleDipyridamole
Aspirin,Aspirin,TxS InhibitorsTxS Inhibitors
GPllb/lllaGPllb/lllaAntagonistsAntagonists
Shear Stress,Shear Stress,Binding of Agonists:Binding of Agonists:
Schafer AI. Am J Med. 1996;101:202.
SerotoninSerotoninAntagonistsAntagonists
ClopidogrelClopidogrelTiclopidineTiclopidine
TXATXA22 ReceptorReceptorAntagonistsAntagonists
GP = GlycoproteinvWF = von Willebrand factor TxS = Thromboxane synthaseTXA2 = Thromboxane A2

Parenteral GP IIb/IIIa inhibitors
Antibody• abciximab
(ReoProâ, Centocor/Lilly)
Cyclic peptide• eptifibatide
(INTEGRILIN®, COR/Key)
Nonpeptide• tirofiban HCI
(Aggrastatâ, Merck)

GP IIb/IIIa Receptor AntagonistsGP IIb/IIIa Receptor AntagonistsAbciximab (ReoPro®)
Tirofiban (Aggrastat®)
Eptifibatide (Integrilin®)
Pharma
Renal Adj.
Dosage
No
0.25 mcg/kg bolus followed by 0.125 mcg/kg/min drip (max 10 mcg/min) for 12-24 hours
Synthetic non-peptide
Yes
0.4 mcg/kg/min for 30 minutes followed by 0.1 mcg/kg/min drip for 48-96 hours
Cyclic heptapeptide
Yes
180 mcg/kg bolus (x2) followed by 2.0 mcg/kg/min drip for 18-24 hours
Fab portion of chimeric monoclonal antibody
Half-life 30 minutes 1.8 hours 2.5 hours

Early Abciximab PCI TrialsEarly Abciximab PCI Trials
NEJM 1997; 336:1689-96
Death, MI, Urgent Revascularization Death, MI, Urgent Revascularization –– 30 Days30 Days
DaysDays00
44
88
1212 BolusBolus
Bolus + InfusionBolus + Infusion
PlaceboPlacebo 12.812.8
8.38.3
EPICEPIC
Absolute Absolute -- 4.5%4.5%Relative Relative –– 35%35%
p = 0.008p = 0.008
DaysDays
PlaceboPlacebo 11.711.7
5.25.2AbciximabAbciximab
EPILOGEPILOG
Absolute Absolute -- 6.5%6.5%Relative Relative –– 55%55%
p < 0.001p < 0.001
10.810.8
6.96.9
Placebo + StentPlacebo + Stent
Abciximab + PTCAAbciximab + PTCA5.35.3Abciximab + StentAbciximab + Stent
00 3030DaysDays
EPISTENTEPISTENT
Absolute Absolute -- 5.5%5.5%Relative Relative –– 51%51%
p < 0.001p < 0.001
NEJM 1994; 330:956NEJM 1994; 330:956--6161 Lancet 1998; 352:87Lancet 1998; 352:87--9292
00 303000 3030

For STEMIFor STEMI

Primary PCI30 Day Death, MI or Urgent TVR
11.210.5
14.6
6.9
10.5
5.8 5.06.0
4.5 4.5
0
5
10
15
20
% o
f Pat
ient
s
Placebo Abciximab
¯ 48%p = 0.03
¯ 52%p = 0.04
¯ 52%p = 0.01
¯ 30%p = 0.02
JACC 2000;35:915-21.
NEJM 2001;41:1895-03.
Circ 1998;98:734-41.
n = 401 n = 300 n = 2082n = 483ISAR-2 ADMIRAL CADILLAC*RAPPORT
¯ 57%p = 0.02
n = 400ACE**
NEJM 2002;346:957-66

Ellis S. Ellis S. ESC ESC N Engl J Med 2008;358:2205
*All-cause mortality; rehosp or ED visit for CHF; VF >48 hours after randomization; cardiogenic shock. N=2452.
FINESSE – 90-Day Endpoints FINESSE – 90-Day Endpoints P
erce
ntP
erce
nt
4.5
8.9
2.2
10.5
5.5
7.5
2.9
9.8
5.2
7.4
1.9
10.7
0
2
4
6
8
10
12
Composite* Death MI Comp CHF
Primary PCI (806) PCI+Abcix (818) PCI+Abcix+Reteplase (828)
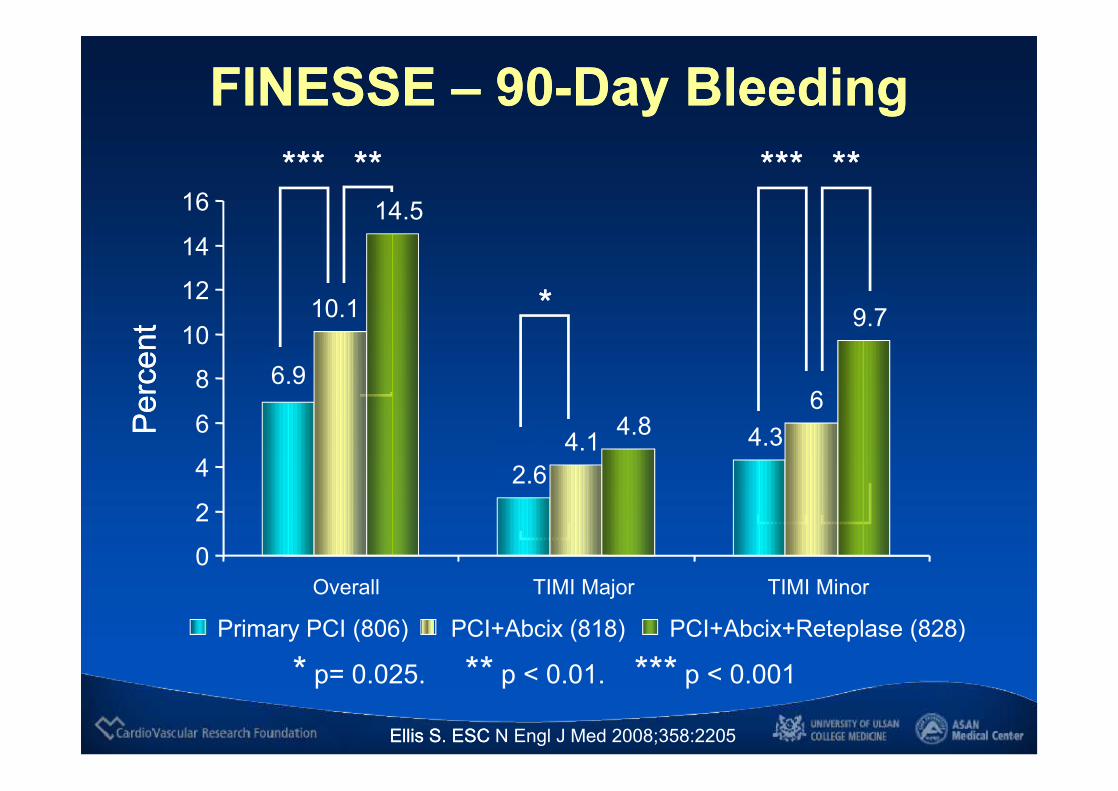
FINESSE – 90-Day Bleeding FINESSE – 90-Day Bleeding P
erce
ntP
erce
nt
**
******
* p= 0.025. ** p < 0.01. *** p < 0.001
********** ****
2.64.3
10.1
4.16
14.5
4.8
9.7
6.9
0
2
4
6
8
10
12
14
16
Overall TIMI Major TIMI Minor
Primary PCI (806) PCI+Abcix (818) PCI+Abcix+Reteplase (828)
Ellis S. Ellis S. ESC ESC N Engl J Med 2008;358:2205

Di Mario C. Lancet 2008; 371: 559–68
CARESS Abciximab with ½ Dose Reteplase
CARESS Abciximab with ½ Dose Reteplase
Composite = 30-day Death, Re-MI, Refractory ischemia. N=600
Per
cent
Per
cent
P=0.032P=0.032P=0.001P=0.001
3.1
0.3 0.7
12.2
3.7
11.1
4.4
1.7
5
7.4
2
4.1
0
2
4
6
8
10
12
14
Composite Death Re-MI Ischemia Bleed Transfuse
Immediate PCI (N=298) Rescue PCI (N=300)

On-TIME 2: Study DesignOn-TIME 2: Study Design
Angiogram
HDB Tirofiban*Placebo
Transportation
PCI centerAngiogram
ProvisionalHDB Tirofiban
Tirofibancont’d
N=984Jun 2006–Nov 2007
PCI
*Bolus: 25 µg/kg and 0.15 µg/kg/min infusion.
STEMIdiagnosed in ambulance or
referral centerASA + 600 mg clopidogrel + UFH
van ‘t Hof AWJ, et al. Lancet 2008;16;372(9638):537-46

BRAVE-3Abciximab before Primary PCI
30-day Death, MI, Revas, and Stroke
BRAVE-3Abciximab before Primary PCI
30-day Death, MI, Revas, and Stroke
Mehilli et al. Circulation. 2009;119

On-TIME 2Pre-hospital High Dose Tirofiban
ST-Resolution Time
Lancet. 2008;372:537
(Complete) post-PCI
P=0.033 P=0.020 P=NS P=NS P=NS
Bleeding
Pre-treated with aspirin, heparin & 600 mg clopidogrel
Composite: death, recurrent MI, urgent revascularization

IIB/IIIa Meta-regression30-Day Mortality
IIB/IIIa Meta-regression30-Day Mortality
De Luca G. et al. Eur Heart J 2009;30:2705

GP IIb/IIIa Guideline for STEMI2009
GP IIb/IIIa Guideline for STEMI2009
Early invasive / PCI Medical Management
ACC / AHA ESC ACC / AHA ESC
Class IIaAbciximab
Class IIbTirofiban,eptifibatide
Class IWithout stenting
Class IIaWith stenting
Class IIbAbciximab with half-dose lyticfor patients age < 75 years
Class III
GPI = glycoprotein IIb/IIIa inhibitor
For UA / NSTEMIFor UA / NSTEMI

15.6%
10.1%11.3%
8.0%
14.5%
7.8%
10.8%
8.7%
0%
5%
10%
15%
20%
PURSUIT PRISM PLUS PARAGON B GUSTO-IV ACS
Placebo2b3a Inhibitor
Medical vs Interventional Therapy30-day Death or MI – No Early PCI
P=NSp=NS
p=NS
p=NS

16.7%
10.2%
18.5%
9.0%
11.6%
5.9%
11.6%
4.8%
0%
5%
10%
15%
20%
PURSUIT PRISM PLUS PARAGON B CAPTURE
Placebo2b3a Inhibitor
Medical vs Interventional Therapy30-day Death or MI – Early PCI
P<0.05
p=NS
p=0.01
p=0.03

0.3%
3.8% 4.0%
0.6%0.3%
3.7% 4.0%
0.9%
0%
5%
10%
Death MI Death/MI Urg Revac
PlaceboAbciximab
ISAR-REACTPCI for Low-risk SA Patients – 30 Days
p=NSp=NSp=NS p=NS
NEJM 2004;350:232-8

1.6%
10.5%11.5%
1.2%1.1%
8.1%8.6%
1.0%
0%
5%
10%
Death MI Death/MI Urg Revac
Placebo (1012)Abciximab (1010)
ISAR-REACT 2PCI for Higher-risk ACS Patients – 30 Days
p=0.06p=0.03
p=0.34 p=0.64
JAMA 2006;295:1531-38

ISAR-REACT 2Higher-risk Patients (ACS) – 30 Days
JAMA 2006;295:1531-38
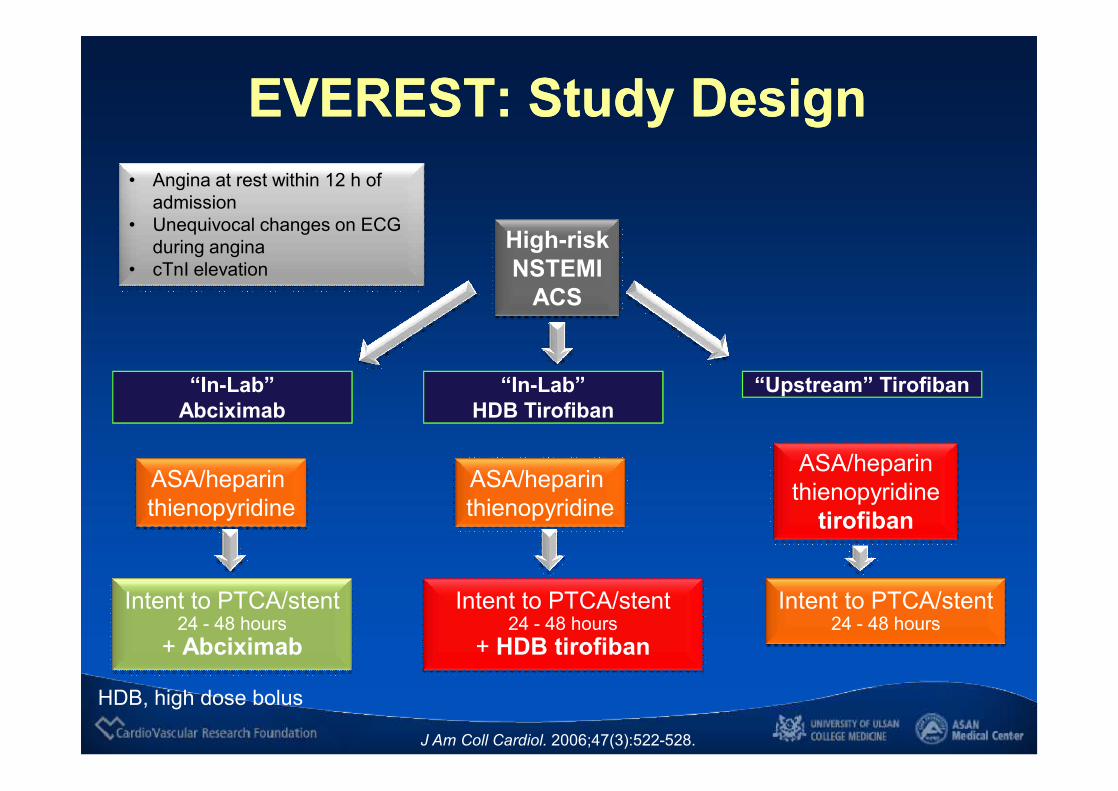
ASA/heparin thienopyridine
tirofiban
ASA/heparin thienopyridine
• Angina at rest within 12 h of admission
• Unequivocal changes on ECG during angina
• cTnI elevation
Intent to PTCA/stent24 - 48 hours
+ Abciximab
Intent to PTCA/stent24 - 48 hours
+ HDB tirofiban
J Am Coll Cardiol. 2006;47(3):522-528.
EVEREST: Study DesignEVEREST: Study Design
“In-Lab” Abciximab
“In-Lab” HDB Tirofiban
Intent to PTCA/stent24 - 48 hours
“Upstream” Tirofiban
ASA/heparin thienopyridine
High-riskNSTEMI
ACS
HDB, high dose bolus
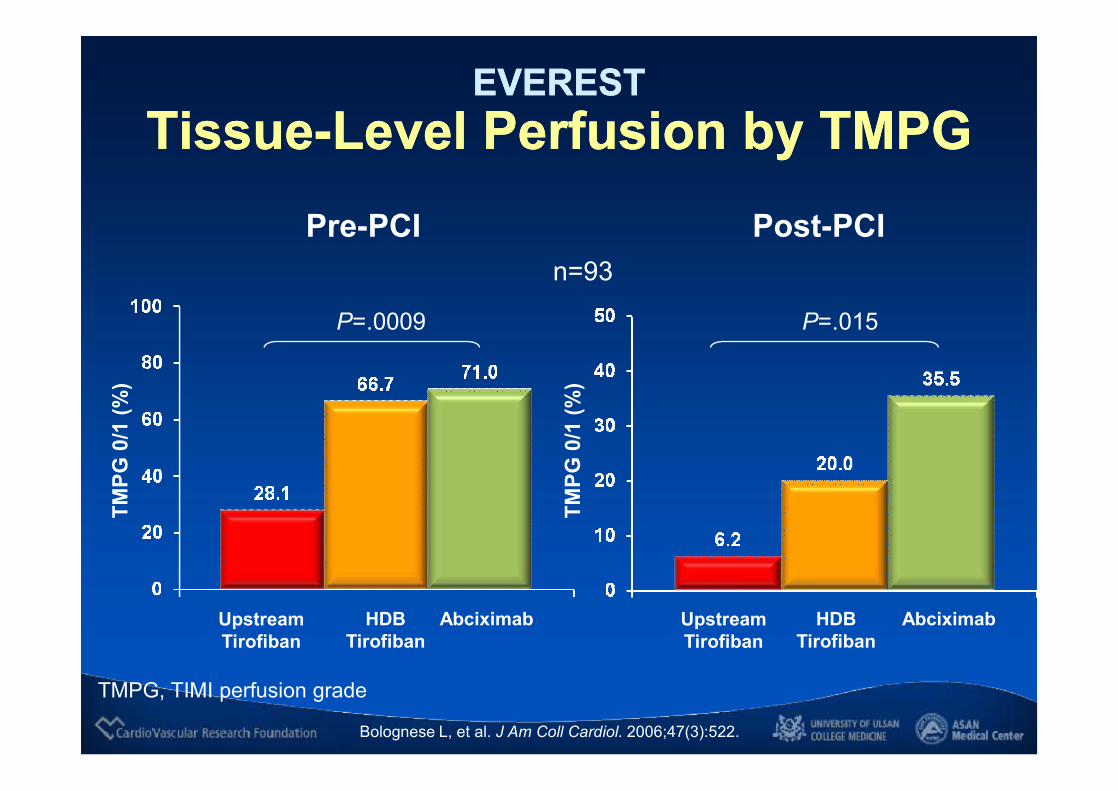
EVERESTTissue-Level Perfusion by TMPG
EVERESTTissue-Level Perfusion by TMPG
Pre-PCI Post-PCI
TMPG
0/1
(%)
UpstreamTirofiban
HDBTirofiban
Abciximab
P=.015
TMPG
0/1
(%)
UpstreamTirofiban
HDBTirofiban
Abciximab
P=.0009
n=93
Bolognese L, et al. J Am Coll Cardiol. 2006;47(3):522.
TMPG, TIMI perfusion grade
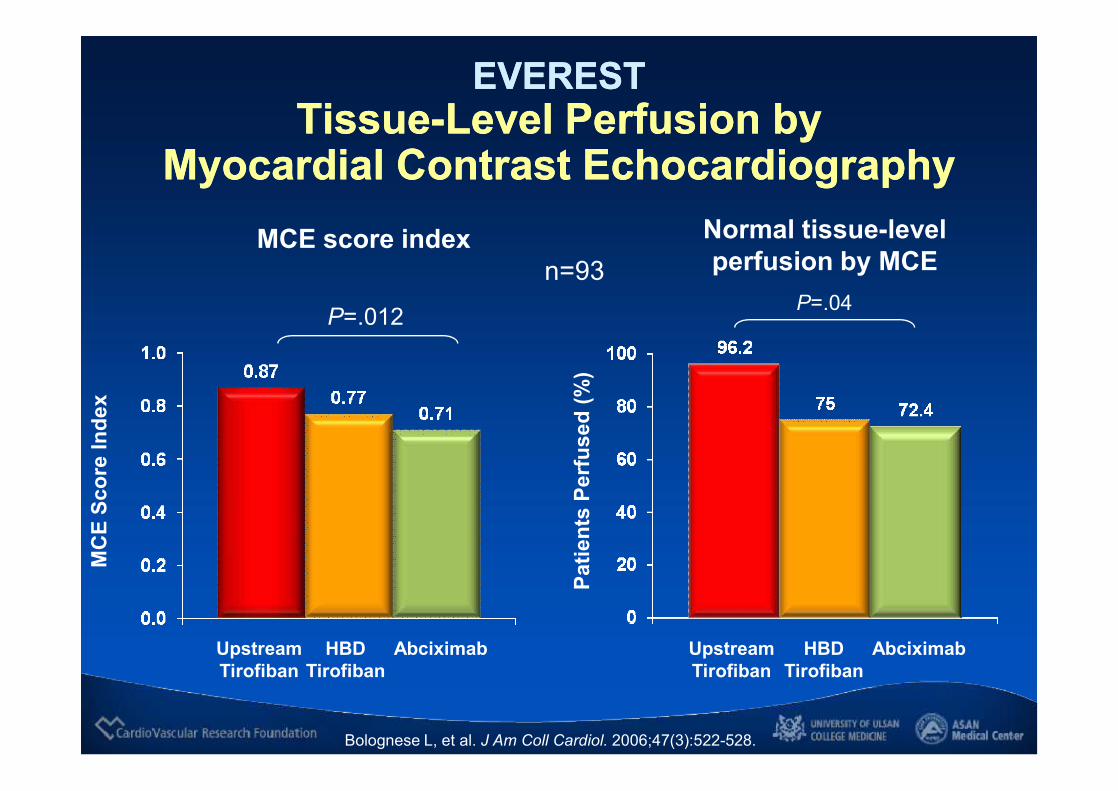
EVEREST Tissue-Level Perfusion by
Myocardial Contrast Echocardiography
EVEREST Tissue-Level Perfusion by
Myocardial Contrast Echocardiography
UpstreamTirofiban
HBDTirofiban
Normal tissue-level perfusion by MCE
UpstreamTirofiban
HBDTirofiban
Abciximab
P=.04
MCE score index
Abciximab
P=.012
Bolognese L, et al. J Am Coll Cardiol. 2006;47(3):522-528.
Patie
nts
Perf
used
(%)
MC
E Sc
ore
Inde
x
n=93

EVERESTPeak cTnI Levels Post-PCI
EVERESTPeak cTnI Levels Post-PCI
UpstreamTirofiban
HBDTirofiban
Abciximab
ng/m
L
Bolognese L, et al. J Am Coll Cardiol. 2006;47(3):522-528.
n=93P=.0002
P=.015
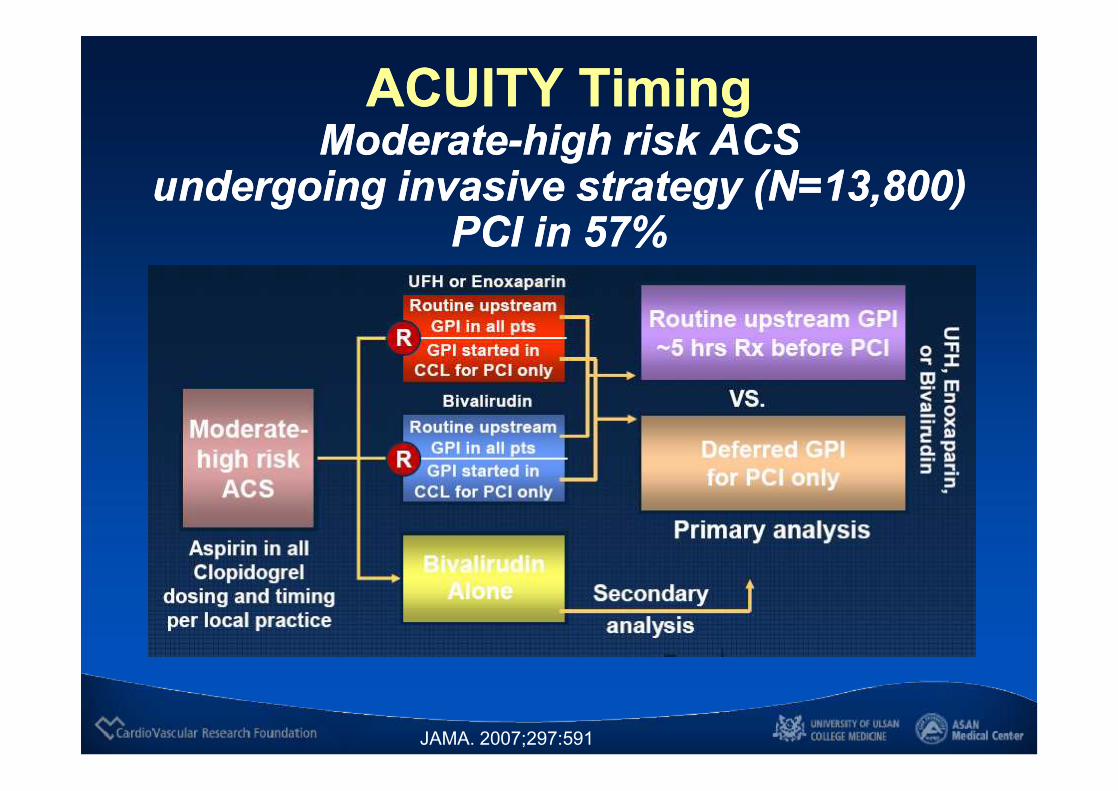
ACUITY TimingModerate-high risk ACS
undergoing invasive strategy (N=13,800)PCI in 57%
ACUITY TimingModerate-high risk ACS
undergoing invasive strategy (N=13,800)PCI in 57%
JAMA. 2007;297:591
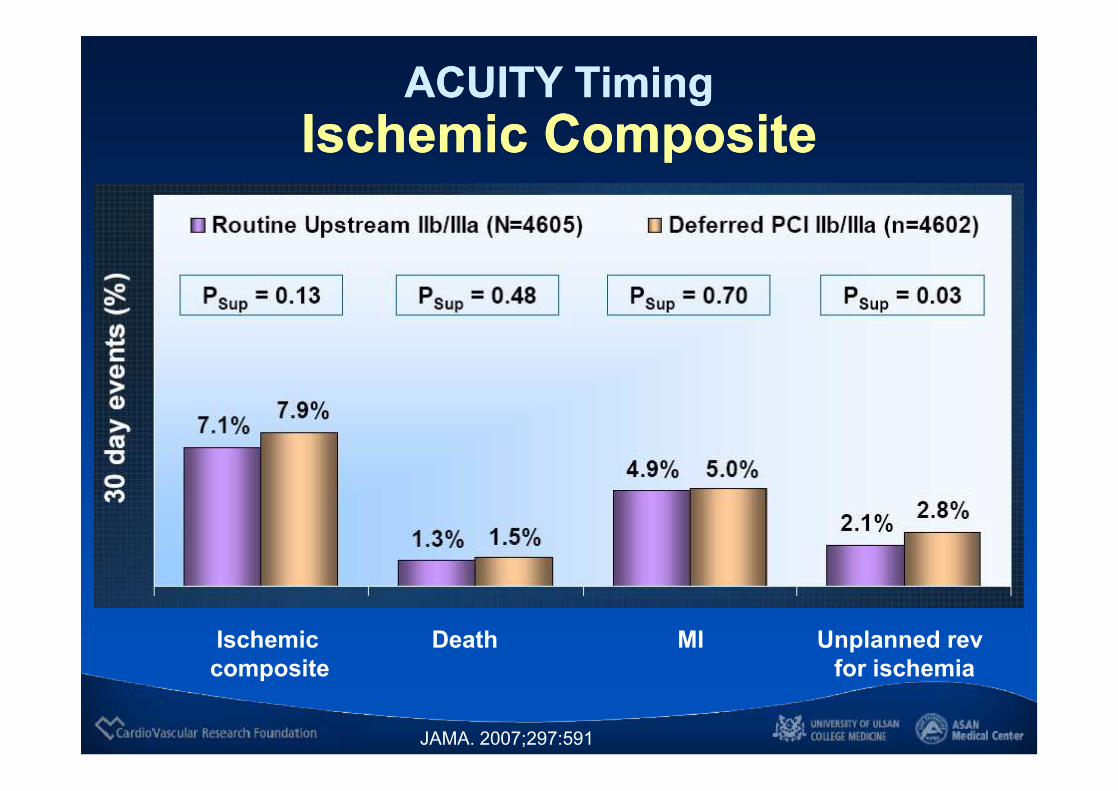
ACUITY TimingIschemic Composite
ACUITY TimingIschemic Composite
Ischemic Death MI Unplanned revcomposite for ischemia
JAMA. 2007;297:591

ACUITY TimingMajor Bleeding
ACUITY TimingMajor Bleeding
JAMA. 2007;297:591
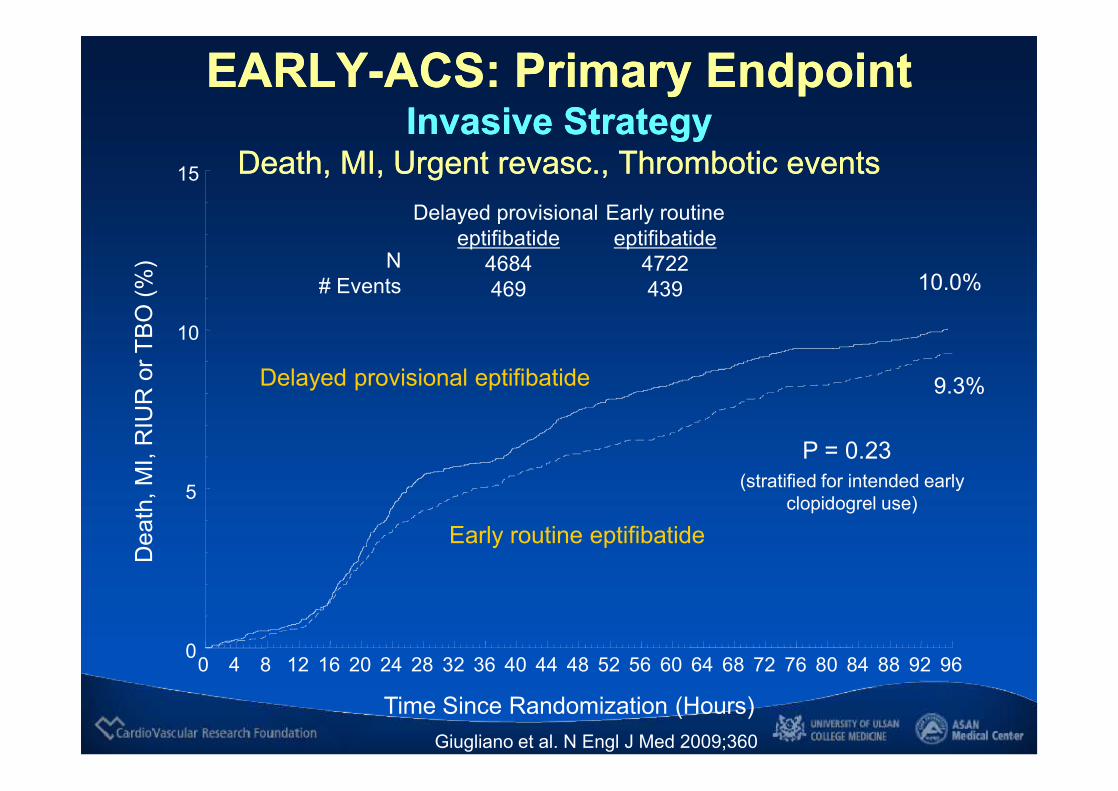
EARLY-ACS: Primary EndpointInvasive Strategy
Death, MI, Urgent revasc., Thrombotic events
EARLY-ACS: Primary EndpointInvasive Strategy
Death, MI, Urgent revasc., Thrombotic events
Giugliano et al. N Engl J Med 2009;360
Dea
th, M
I, R
IUR
or T
BO
(%)
0
5
10
15
Time Since Randomization (Hours)
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96
10.0%
9.3%
Delayed provisional eptifibatide
4684469
Early routineeptifibatide
4722439
P = 0.23(stratified for intended early
clopidogrel use)
N# Events
Delayed provisional eptifibatide
Early routine eptifibatide

Early-ACS: 30-day Death or MIEarly-ACS: 30-day Death or MID
eath
or M
I (%
)
0
5
10
15
Time Since Randomization (Days)
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
12.4%
11.2%
P = 0.079(stratified for intended early
clopidogrel use)
Delayed provisional eptifibatide
4684578
2.1 (1.0, 5.8)
Early routineeptifibatide
4722528
2.7 (1.0, 4.9)
N# Events
Days to Event
Delayed provisional eptifibatide
Early routine eptifibatide
39% use of eptifibatide
Giugliano et al. N Engl J Med 2009;360

GP IIb/IIIa Guideline for UA / NSTEMI2009
GP IIb/IIIa Guideline for UA / NSTEMI2009
Early invasive / PCI Medical Management
ACC / AHA ESC ACC / AHA ESC
Class IEither GPI or clopidogrel in addition to aspirin should be initiated before angiography
Class IIaReasonable to initiate antiplatelet therapy with both GPI and clopidogrel
Class I (high risk)
Class IIf subsequent recurrent symptom/ischemia, heart failure, or serious arrhythmia occur, angiography should be performed with upstream use of either clopidogrel or GPI
Class IIaIf recurrent ischemic discomfort with clopidogrel, it is reasonable to add a GPI before angiography
Class IIbMay be reasonable to add GPI to oral antiplatelet and anticoagulant therapy
Class II (high risk)
GPI = glycoprotein IIb/IIIa inhibitor
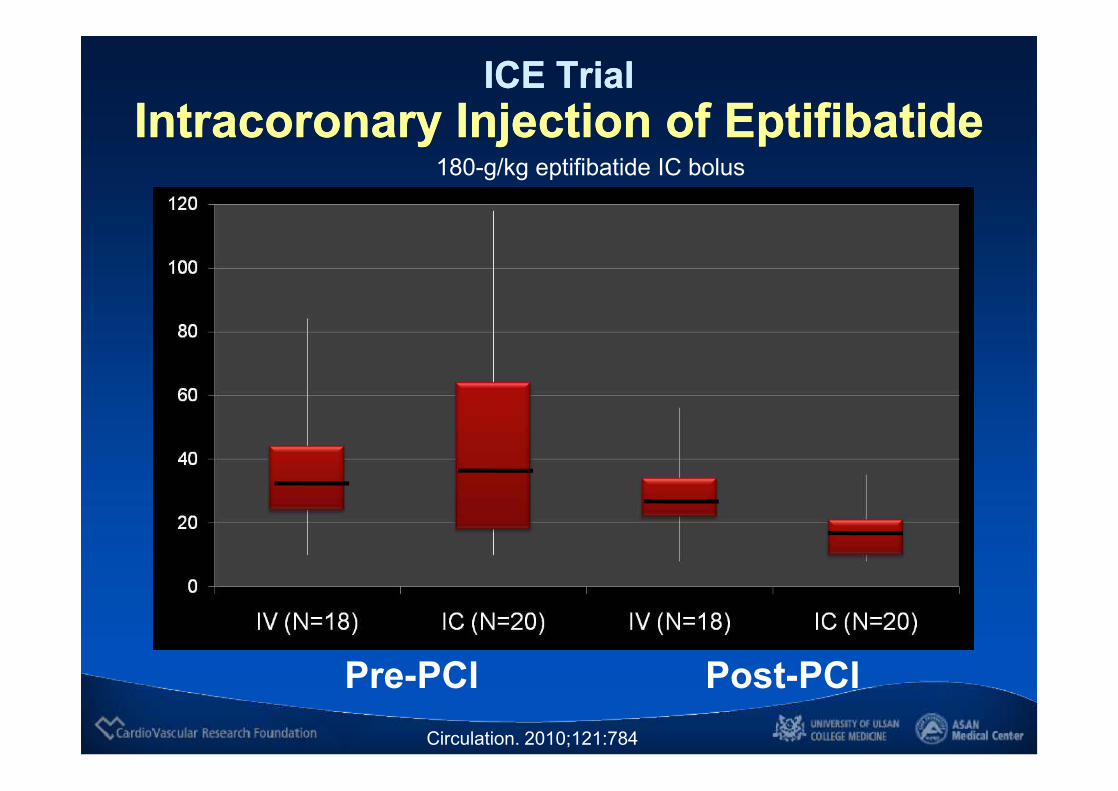
ICE TrialIntracoronary Injection of Eptifibatide
ICE TrialIntracoronary Injection of Eptifibatide
Pre-PCI Post-PCICirculation. 2010;121:784
180-g/kg eptifibatide IC bolus

ConclusionConclusion• Extensive data support the use of IV GPIs in the setting of
moderate- or high-risk NSTE-ACS, particularly if an early invasive strategy is planned.
• Patients who present with STEMI who are undergoing primary PCI also appear to benefit; however, the benefit is less evident.
• In the setting of low-risk ACS, GPIs may not be useful.• In spite of extensive studies, open questions remain,
including the timing of initiation, their clinical utility in combination with and compared with newer antithrombotics, and optimal dosing in certain patient populations (i.e., the elderly, patients with renal insufficiency).

Reimbursement Policy in KoreaReimbursement Policy in Korea
Abciximab Tirofiban
o High risk PCI
o PCI for high risk AMI
o Acute closure due to thrombus
o No reflow after stenting
o Threatening of acute closure due
to no reflow, new thrombus,
intramural hazziness during PCI
o High risk ACS with elevated
troponin or change of EKG