update on emergency cardiac care guidelines mark l. greenberg, md associate professor of medicine...
TRANSCRIPT

UPDATE ON EMERGENCY CARDIAC CARE
GUIDELINES
Mark L. Greenberg, MDAssociate Professor of Medicine
Director, Clinical Electrophysiology and Pacing

1
BLS and ACLS--Historical Perspective
1956: External defibrillation (Zoll) 1958: Mouth-to-mouth ventilation (Safar,
Elam) 1960: Chest compressions (Kouwenhoven) 1979: Automatic External Defibrillator (AED)
(Diack) 1996: Biphasic waveform approved for AED
use in USA 2000: First international evidence-based
resuscitation guidelines

The Chain of Survival of Cardiopulmonary Resuscitation

Valenzuela, et al. Circulation. 1997;96:3308-13.
Interdependence of Early CPR and Early Defibrillation

The physiologic mechanism of chest compressions: cardiac pump (A) or
thoracic pump (B)?

What’s New in BLS
New Chest Compression Rate and Compression-Ventilation Ratio for Adults
Interposed Abdominal Compression CPR (IAC-CPR)

INTERRUPTIONS IN CHEST COMPRESSIONS ARE
DETRIMENTAL
Lay rescuers: 16 seconds to administer 2 breaths (cf 3-4 sec. for professionals).
Compression: ventilation ratio of 5:1 yields higher PaO2 but lower oxygen delivery than 15:2 (64 compressions, 8 ventilations per minute).
New Chest Compression Rate and Compression-Ventilation
Ratio for Adults
Compression rate approx. 100/min for adults and children over age one
Compression-ventilation ratio 15:2 for both one and two-rescuer CPR (5:1 after trachea intubated)
Interposed Abdominal Compression CPR (IAC-CPR)
An alternative for in-hospital resuscitation
Abdomen compressed between xiphoid and umbilicus during relaxation phase of chest compression
Increases forward blood flow during CPR and appears to improve survival

IAC-CPR

Seesaw-like Function of the Lifestick

ResQPump™
Metronome Force Gauge
Handle
Suction Cup

Inspiratory Impedance Threshold Valve (ITV)
Design: Each time the chest wall recoils following a compression, the ITV transiently blocks air/oxygen from entering the lungs, creating a small vacuum in the chest.
Concept: Lower intrathoracic pressure in the chest during the decompression phase of CPR enhances venous return to the thorax.

ResQValve (CPRx)
Disposable, one-way valve that fits into the respiratory circuit and impedes
inspiratory gas exchange during decompression

ResQValve Placement

BrainLeft Ventricle
STD CPR
STD CPR + ITV
ACD CPR
ACD CPR + ITV
0.0
0.2
0.4
0.6
0.8
1.0
Blood Flow During CPR
(Porcine VF Model) B
lood
Flo
w (
ml/m
in/g
m)
Lurie et al. Improving ACD CPR with an inspiratory impedance valve. Circulation 1995;91:1629-32.

Blood Pressure During CPR in Humans
0
20
40
60
80
100
120
mm
Hg
Systolic Diastolic
STD CPR
ACD + ITV
Cohen et al, JAMA 1992 and Plaisance et al, Circulation 2000
Baseline (Normal)

RCT of ACD/ITV CPR vs. STANDARD CPR
220 patients, 157 with witnessed events (Mainz, Germany)
24 hr. survival 37% with ACD/ITV CPR vs. 22% with standard CPR (p=0.03)
Wolcke et. al. Circulation.2002;106:II-538.

What’s New in External Defibrillation
More emphasis on early defibrillation
Automatic External Defibrillation (AED) and Public Access Defibrillation (PAD)
Defibrillation with a biphasic waveform

04/19/23
Defibrillation The Time Factor*
Survival rates after VF cardiac arrest decrease approximately 7% to 10% with every minute that defibrillation is delayed.
Guidelines 2000 for Cardiovascular Resuscitation and Emergency Cardiovascular Care.Circulation. 2000;102(suppl I)8. August 22,2000
Time (min)
100
80
90
70
60
50
40
30
20
10
01 2 3 4 5 6 7 8 9
Per
cen
t o
f S
urv
ival
10
* Non-linear

13 year old boy struck by a pitch
Commotio Cordis

Goals For Early Defibrillation
In hospital: defibrillation within 3 minutes
Out of hospital: defibrillation within 5 minutes of activation of the EMS (value of AED and PAD)


Unconscious patient, no pulse
Shock advised

Unconscious patient, no pulse
No shock advised?

President Bill Clinton, 5/20/00 radio address.
“It is time for the national government to help bring AED’s to public places all over America. . . I am working with Congress to complete a vital piece of legislation that would not only encourage the installation of AED’s in federal buildings, but also grant legal immunity to good Samaritans who use them. .. It is now our responsibility to bring this technology , this modern miracle, to every community in America.”

Prevalence of AED’s
National Registry of CPR Hospitals: 31%
VA Hospitals: 14% Commerical Airliners: 100%

O’Hare International Airport: 60-90 Second Walk To An
AED
Caffrey et. al. N Engl J Med 2002;347:1242-7.

CHICAGO AIRPORT AED STUDY
Three airports, serving >100 million passengers/yr.
21 cardiac arrests over 2 yrs; 18 had VF, 11 of whom were resuscitated (10 alive & well one yr. later)
Caffrey et. al. N Engl J Med 2002;347:1242-7.

Incidence of Unexpected Cardiac Arrest


AEDs: UNANSWERED QUESTIONS
Does formal training improve performance?
How are they best deployed?
Are they cost effective?

DEFIBRILLATOR WAVEFORMS

04/19/23
Defibrillation
Current Flow
Biphasic defibrillation—current flows in two phases, first in one direction from one electrode, and then current flows the other way from the other electrode

04/19/23
Biphasic Defibrillation
Risk of Damage
Source: SL Higgins, Prehospital Emergency Care 2000; 4:305-313
Much less peak current and better efficacy than monophasic
Biphasic Peak Current
Monophasic Peak Current
40% Difference
-20
-10
0
10
20
30
40
0 5 10 15 20
Time (msec)
Cur
rent
(am
ps)

Transthoracic Impedance
Measured by the defibrillator
Higher impedance • Skin surface—especially dry• Hair• Fat• Bone• Air in chest

04/19/23
Impedance
The current a heart receives from a 200J shock depends on the patient’s impedance
0
10
20
30
40
50
60
25 50 75 100 125 150
Patient Impedance (ohms)
Pea
k C
urre
nt (
amps
)
Current variance due to impedance, energy held constant

04/19/23
Impedance Distribution
30 40 50 60 70 80 90 100 110 120 130 140 150 More0
2
4
6
8
10
12
14
16
Histogram of patient impedances
Impedance (ohms)
Per
cen
tag
e o
f P
atie
nts
Medtronic Physio-Control: Impedance data on 723 SCA patients.

Biphasic Defibrillators Are NOT All the Same
Waveforms vary (with regard to voltage or pulse duration) in their response to transthoracic impedance measurements.
Energy settings may be fixed, low-dose escalating, or “standard” dose escalating.
No clear superiority among manufacturers.

IMPEDANCE ADJUSTMENT WITH PHILIPS FR2
50
40
30
20
10
0
-10
-200 5 10 15 20 25 30 35 40
Current (A)
Time (msec)
SMART Biphasic 150-150-150 J Current adjusted for
impedance Customized
waveform shape for each patient and each shock
5050, 150 J, 150 J
7575, 150 J, 150 J
125125, 150 J, 150 J
Why Will Biphasic Defibrillators Replace Standard Monophasic
Models?
Impedance compensating, lower shock strength biphasic waveforms have less potential to damage cells.
Biphasic waveforms have superior efficacy for treating atrial fibrillation and ventricular fibrillation.

Randomized, controlled trial of 150 J biphasic shocks with 200-360 J monophasic shocks in 115
patients with out-of-hospital VF; time to first shock 8.9+/-3.0 min.
1st shock
%
Biphasic Monophasic
p <0.000196% (52/54)
59%(36/61)B
3 shocksBiphasic Monophasic
p < 0.000198% (53/54)
69% (42/61)
Schneider T, et al, Circulation 2000;102:1780-1787.
What’s New in ACLS?
Airway ManagementVasopressinIV amiodarone as a first-line drug

What’s New in Airway Management
Emphasis on skilled bag-mask ventilation with continuous cricoid pressure
Validation of airway adjuncts like the laryngeal mask and Combitube
Recommendation for secondary confirmation techniques to verify ETT placement (e.g.end-tidal CO2)

Cricoid Pressure Can Minimize Gastric Inflation
Advanced Airway Devices
Esophageal-tracheal combitube

Advanced Airway Devices
Laryngeal mask airway (LMA) Superior to ETT for BLS-level
personnel Equal to ETT for ACLS-level personnel

Laryngeal Mask

Confirming Tracheal Tube Placement
Esophageal detector devices

Vasopressin 40 U IV Before Epinephrine 1 mg IV?
Vasopressin appears at least as effective as epinephrine (large RCT underway in Europe).
Vasopressin is non-beta-adrenergic and does not increase myocardial 02 consumption.
Longer half-life (10-20 min. vs. 3-5 min.) simplifies administration.

Amiodarone 300 mg IV Should Be Given Before Lidocaine
Advantage lidocaine: rapid onset of action, no hypotension
Game, set, and match amiodarone: minimal proarrhythmia, much stronger evidence for efficacy

Kudenchuk et. al. NEJM 1999;341:871-8.
Amiodarone vs. Placebo in 504 Pts. with Shock Refractory Out-of-
Hospital VT/VF
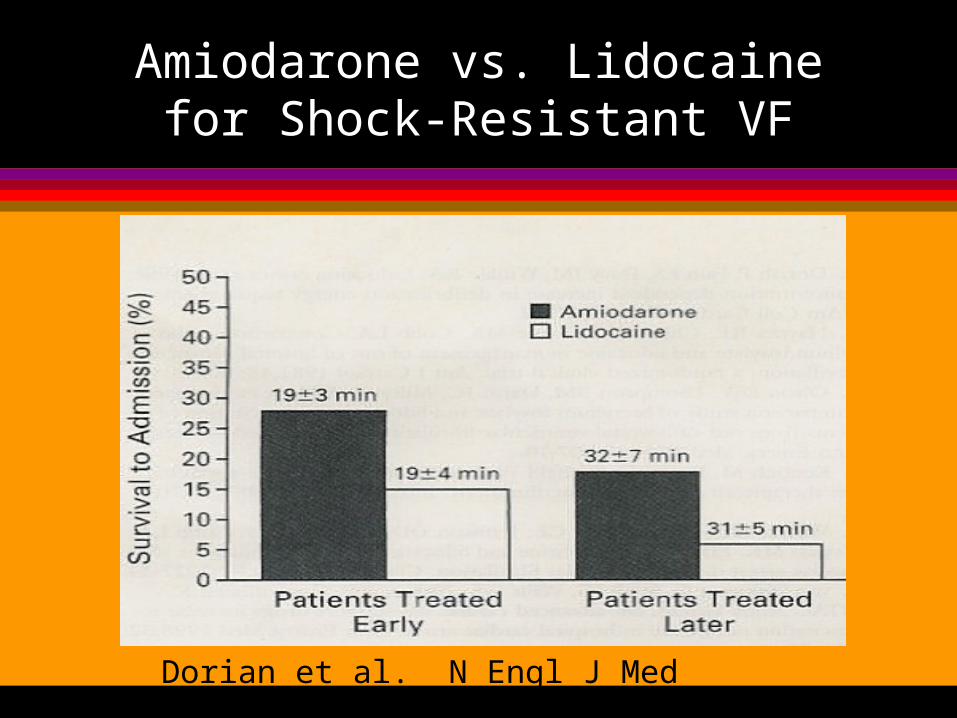
Amiodarone vs. Lidocaine for Shock-Resistant VF
Dorian et al. N Engl J Med 2002;346:884-90.

Stable Ventricular Tachycardia
A m io d aro ne* 1 50 m g IV ove r 1 0 m inu tes
orL ido caine
* 0 .5 to 0 .7 5 m g /kg IV pu shThen use
S ynch ro n ized card iovers ion
M edica tio n s: * Procainam ide
O th ers acceptab le * Am iodarone * Lidocaine
Reasonable LV function Poor LV function
M onom orphic VTIs ca rd ia c fu n ctio n im p a ire d?

Polymorphic Ventricular Tachycardia
L o n g b ase line Q TIn te rval* Correct abnorm alelectrolytes
Interventions: * Magnesium * Overdrive pacing * Isoproterenol * Lidocaine
N o rm a l b ase line Q TIn te rval * Treat ischem ia * Correct electrolytes
M edications: * Beta Blockers or * Lidocaine or * Am iodarone or * Procainam ide or * Sotalol
N o rm a l b ase lineQ T Inte rval
P ro lo n ged b ase lineQ T Inte rval
(su gg es ts T o rsades)
P o lym o rp hic VT* Is QT baseline interval prolonged?