universal health coverage in latin american countries: how to improve solidarity-based schemes
TRANSCRIPT
Health Policy
www.thelancet.com Published online October 16, 2014 http://dx.doi.org/10.1016/S0140-6736(14)61780-3 1
Universal health coverage in Latin American countries: how to improve solidarity-based schemesDaniel Titelman, Oscar Cetrángolo, Olga Lucía Acosta
In this Health Policy we examine the association between the fi nancing structure of health systems and universal health coverage. Latin American health systems encompass a wide range of fi nancial sources, which translate into diff erent solidarity-based schemes that combine contributory (payroll taxes) and non-contributory (general taxes) sources of fi nancing. To move towards universal health coverage, solidarity-based schemes must heavily rely on countries’ capacity to increase public expenditure in health. Improvement of solidarity-based schemes will need the expansion of mandatory universal insurance systems and strengthening of the public sector including increased fi scal expenditure. These actions demand a new model to integrate diff erent sources of health-sector fi nancing, including general tax revenue, social security contributions, and private expenditure. The extent of integration achieved among these sources will be the main determinant of solidarity and universal health coverage. The basic challenges for improvement of universal health coverage are not only to spend more on health, but also to reduce the proportion of out-of-pocket spending, which will need increased fi scal resources.
IntroductionUniversal health coverage shows an uneven pattern in Latin American countries. Available data indicate that improvement of access and coverage, together with reduction of health inequalities, is a pending task in most Latin American countries, as stated by the Pan American Health Organization,1,2 WHO,3,4 and the Economic Commission for Latin America and the Caribbean.5,6
The fi nancing structure of health systems plays an important part in achievement of universal health coverage, particularly in the way that solidarity-based schemes are fi nanced and implemented. In most countries of the region, public spending on health is insuffi cient and inadequately assigned. When, as is the case in Latin America, there is an over-reliance on private spending for health services and medications, achievement of universal health coverage is largely constrained by the feasibility of introduction of solidarity-based schemes into health system fi nancing.7 A solidarity-based scheme is one in which participants have access to the benefi ts of the health-care system irrespective of the contribution they make to its fi nancing. Thus, participants contribute according to their means, but receive benefi ts according to need. As a result, high earners contribute proportionally more to fi nancing the system than do low earners or those without income, hence the concept of solidarity.
Latin American health systems are fi nanced from a wide range of sources, giving rise to various fi nancial arrangements, which translate into diff erent solidarity schemes. In this paper we identify the schemes used by some Latin American countries to achieve universal health coverage. In particular, we examine solidarity issues in the context of health systems that combine contributory (payroll taxes) and non-contributory (general taxes) sources of fi nancing. We argue that to move towards universal health coverage, solidarity schemes must be able to combine both types of fi nancing and that in the short to medium term the dynamics of universal health coverage are strongly correlated with the non-contributing
component of fi nancing. In this context, the basic challenges for improvement of universal health coverage are not only to spend more on health, but also to reduce the proportion of out-of-pocket spending.
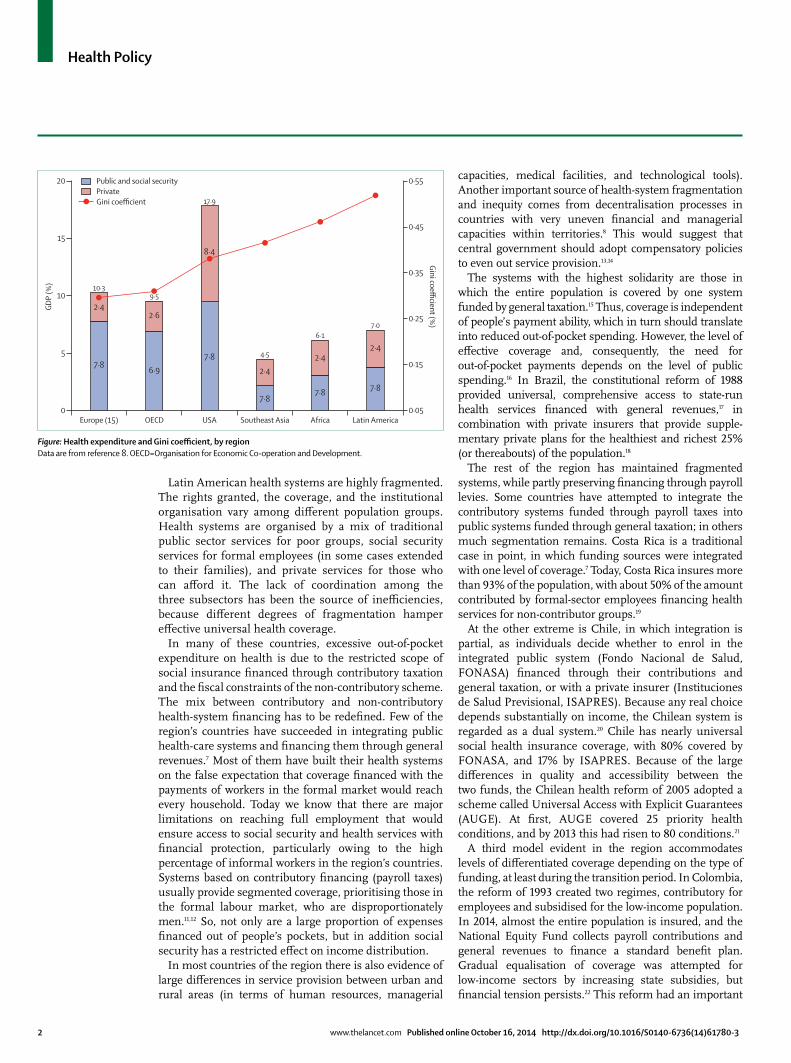
Universal health coverage and the health fi nancing structureThe system’s fi nancing structure is not neutral from the viewpoint of equality. A key distinctive feature of the health fi nancing structure in Latin America is the relative importance of private expenditure. As shown in the fi gure,8 health spending in the region is not only lower measured as a proportion of GDP than in Organisation for Economic Co-operation and Development (OECD) countries, but it also shows a higher burden of private spending. On average, private spending in the region accounts for 45% of total health spending, which as a percentage of GDP is higher than in Europe and the OECD countries. This implies that families themselves largely fund the relatively low levels of health expenditure in Latin American countries, through out-of-pocket payments.
The need to incur out-of-pocket expenses to gain access to health services or consume medicines is a major source of inequity and limits countries’ capacity to move towards universal health coverage. The fi gure shows a negative correlation between private expenditure on health and income distribution. Countries in which private spending on health is proportionally lower have better Gini coeffi cients.
Expansion of coverage consistent with the principles of universality and solidarity depends on how health fi nancing is organised. Diff erent fi nancial arrangements determine diff erent results in income redistribution (between rich and poor people) and in risk sharing (between healthy and ill people).9 Here we concentrate on the fi rst of these. By income solidarity we mean that access to health services is independent of people’s contributions to the system or their actual capacity to make out-of-pocket payments.9,10
Published OnlineOctober 16, 2014http://dx.doi.org/10.1016/S0140-6736(14)61780-3
Economic Development Division, Economic Commission for Latin America and the Caribbean (ECLAC), Santiago, Chile (D Titelman PhD); Universidad Buenos Aires, Buenos Aires, Argentina (Prof O Cetrángolo MPhil); and ECLAC Bogotá, Bogotá, Colombia (O L Acosta PhDc)
Correspondence to:Dr Daniel Titelman, Economic Development Division, Economic Commission for Latin America and the Caribbean, Av. Dag Hammarskjold 3477, Vitacura, Santiago, [email protected]
Health Policy
2 www.thelancet.com Published online October 16, 2014 http://dx.doi.org/10.1016/S0140-6736(14)61780-3
Latin American health systems are highly fragmented. The rights granted, the coverage, and the institutional organisation vary among diff erent population groups. Health systems are organised by a mix of traditional public sector services for poor groups, social security services for formal employees (in some cases extended to their families), and private services for those who can aff ord it. The lack of coordination among the three subsectors has been the source of ineffi ciencies, because diff erent degrees of fragmentation hamper eff ective universal health coverage.
In many of these countries, excessive out-of-pocket expenditure on health is due to the restricted scope of social insurance fi nanced through contributory taxation and the fi scal constraints of the non-contributory scheme. The mix between contributory and non-contributory health-system fi nancing has to be redefi ned. Few of the region’s countries have succeeded in integrating public health-care systems and fi nancing them through general revenues.7 Most of them have built their health systems on the false expectation that coverage fi nanced with the payments of workers in the formal market would reach every household. Today we know that there are major limitations on reaching full employment that would ensure access to social security and health services with fi nancial protection, particularly owing to the high percentage of informal workers in the region’s countries. Systems based on contributory fi nancing (payroll taxes) usually provide segmented coverage, prioritising those in the formal labour market, who are disproportionately men.11,12 So, not only are a large proportion of expenses fi nanced out of people’s pockets, but in addition social security has a restricted eff ect on income distribution.
In most countries of the region there is also evidence of large diff erences in service provision between urban and rural areas (in terms of human resources, managerial
capacities, medical facilities, and technological tools). Another important source of health-system fragmen tation and inequity comes from decentralisation processes in countries with very uneven fi nancial and managerial capacities within territories.8 This would suggest that central government should adopt compensatory policies to even out service provision.13,14
The systems with the highest solidarity are those in which the entire population is covered by one system funded by general taxation.15 Thus, coverage is independent of people’s payment ability, which in turn should translate into reduced out-of-pocket spending. However, the level of eff ective coverage and, consequently, the need for out-of-pocket payments depends on the level of public spending.16 In Brazil, the constitutional reform of 1988 provided universal, comprehensive access to state-run health services fi nanced with general revenues,17 in combination with private insurers that provide supple-mentary private plans for the healthiest and richest 25% (or thereabouts) of the population.18
The rest of the region has maintained fragmented systems, while partly preserving fi nancing through payroll levies. Some countries have attempted to integrate the contributory systems funded through payroll taxes into public systems funded through general taxation; in others much segmentation remains. Costa Rica is a traditional case in point, in which funding sources were integrated with one level of coverage.7 Today, Costa Rica insures more than 93% of the population, with about 50% of the amount contributed by formal-sector employees fi nancing health services for non-contributor groups.19
At the other extreme is Chile, in which integration is partial, as individuals decide whether to enrol in the integrated public system (Fondo Nacional de Salud, FONASA) fi nanced through their contributions and general taxation, or with a private insurer (Instituciones de Salud Previsional, ISAPRES). Because any real choice depends substantially on income, the Chilean system is regarded as a dual system.20 Chile has nearly universal social health insurance coverage, with 80% covered by FONASA, and 17% by ISAPRES. Because of the large diff erences in quality and accessibility between the two funds, the Chilean health reform of 2005 adopted a scheme called Universal Access with Explicit Guarantees (AUGE). At fi rst, AUGE covered 25 priority health conditions, and by 2013 this had risen to 80 conditions.21
A third model evident in the region accommodates levels of diff erentiated coverage depending on the type of funding, at least during the transition period. In Colombia, the reform of 1993 created two regimes, contributory for employees and subsidised for the low-income population. In 2014, almost the entire population is insured, and the National Equity Fund collects payroll contributions and general revenues to fi nance a standard benefi t plan. Gradual equalisation of coverage was attempted for low-income sectors by increasing state subsidies, but fi nancial tension persists.22 This reform had an important
Figure: Health expenditure and Gini coeffi cient, by regionData are from reference 8. OECD=Organisation for Economic Co-operation and Development.
Europe (15)
7·8
2·4
10·3
OECD USA Southeast Asia Africa Latin America0
5
10
15
20 0·55
0·45
0·35
0·25
0·15
0·05
GDP
(%)
Gini coefficient (%
)
Public and social securityPrivateGini coefficient
6·9
2·6
9·5
7·8
17·9
4·5
6·17·0
8·4
7·8
2·4
7·8
2·4
7·8
2·4

Health Policy
www.thelancet.com Published online October 16, 2014 http://dx.doi.org/10.1016/S0140-6736(14)61780-3 3
eff ect on income distribution and reduced private health expenditure.23 In Uruguay, the recent reforms constitute a new paradigm in which partial progress based on incremental budgetary increases is gradually leading to improved coverage and less heterogeneity.24
Beyond this classifi cation, the eff ects on effi ciency and equity resulting from each particular mode of fi nancing are far more complex. On one hand, systems are always in transition. As Kutzin pointed out, universal health coverage is “a set of objectives that health system pursues”, and is “a direction rather than a destination”.11 On the other hand, not only do the sources and level of funding have to be considered, but also the pooling mechanisms and prevailing purchasing arrangements in each system. Anyway, the likelihood of provision of suffi cient and homogeneous universal health coverage will depend in the fi rst instance on the fi scal resources that each country allocates to health.
Universal health coverage and tax funding: can we change the fi nancing structure of solidarity?As we have discussed, health coverage in Latin America is insuffi cient. The fi nancial capacity to move towards universal health coverage rests, on one hand, on the need to increase the resources available to fi nance the health sector and, on the other, on the challenge to improve fi nancial solidarity schemes. At the same time, universal health coverage in Latin America is a powerful tool to improve the distribution of income and build a more equitable and cohesive society.1,7 Coverage secured by governments should be suffi cient and equal for all. To this end, governments should raise taxation, spend more on health care, improve the allocation and distribution of that spending, and, just as importantly, fund it equitably.
The region’s historical diffi culties in tax collection are well known: Latin America’s tax burden was 18·3% of GDP in 2010 (including social security payments), well below the averages of 35·2% in OECD countries and 39·2% in European countries. The average tax rate hides vastly diff erent situations. Only three countries in the region (Brazil, Argentina, and Uruguay) have attained tax burdens higher than 25% of GDP, but still far lower than European levels. At the other extreme, there are countries with tax burdens lower than 15% of GDP (Mexico, Venezuela, and Guatemala, among others). In view of the diffi culties in collecting taxes, in many Latin American countries’ eff orts to generate resources have concentrated on mechanisms with low redistributive potential.25 On average, more than half of tax revenue comes from VAT and other sales taxes on goods and services (indirect taxes). Only 30% comes from property, income, and other direct taxes, and the remaining 20% comes from social security contributions. By contrast, OECD countries obtain more than 40% of their tax revenue from direct taxes. With more developed social security systems, in these countries resources from social contributions represent almost 27% of the total.
We must acknowledge that contributory funding, although a hindrance to integration, is nevertheless a resource that is diffi cult for countries with funding problems to renounce. In most Latin American countries, funds raised from social security contributions, even if they do not represent a substantial volume as a percentage of GDP, are relatively important sources of health-care fi nancing.26,27 In these cases, it would be unwise (or unrealistic) to suggest replacing them in the near future with sources that are diffi cult to collect.
Additionally, governments have to prioritise health policies in their budget defi nitions. Although social spending has been rising in the region, this growth has not been uniform by sector. On average, we found that allocations had risen faster to social security, welfare, and education, and more slowly to health.28 During the past few decades, crises in pensions systems,30 the need for new social initiatives such as conditional transfer programmes,30 and diff erent pressures to increase expenditure on education31 have compressed the space available for boosting of public health expenditures.
Finally, the challenge of collecting more taxes is closely tied in with the insuffi ciency of social security systems. The countries with the highest tax burdens also have the lowest degrees of labour informality and, consequently, the highest health insurance coverage. As noted earlier, in view of the diffi culties in collection of taxes in some countries, the challenge for these societies is to fi nd a balanced combination of resources so that the level of payroll contributions does not create incentives for informality, evasion, or avoidance, but allows them to take advantage of the contributions made by the population participating in the formal labour market with high capacity to pay. Thus, achievement of universal coverage will need major eff orts in terms of labour market regulation, implementation of public policies to encourage formalisation, and the design of alternative contribution schemes, such as partly or fully subsidised contributions.32 Notably, many countries have incor-
porated simplifi ed schemes for small taxpayers that, in some cases (Argentina and Uruguay), include a contribution to ensure access to health insurance (unpublished data).
How much each country has to spend on health is therefore diffi cult to ascertain,33 since this depends on various factors. However, we have argued that making more effi cient and equitable use of funds in Latin America depends on the capacity to increase the publicly funded portion of expenditure on health. Countries will then be able to expand the tax base to obtain increased resources from general taxes.
ConclusionMany factors determine the potential to move towards universal health coverage, and many of them have political roots. In this paper we have focused on factors related to health fi nancing. To make headway towards

Health Policy
4 www.thelancet.com Published online October 16, 2014 http://dx.doi.org/10.1016/S0140-6736(14)61780-3
4 WHO. World health report 2010: health systems fi nancing—the path to universal coverage. Geneva: World Health Organization, 2010.
5 ECLAC. Social panorama of Latin America 2013. Santiago: Economic Commission for Latin America and the Caribbean, 2013.
6 ECLAC. Sustainable development in Latin America and the Caribbean: follow-up to the United Nations development agenda beyond 2015 and to Rio+20. Santiago: Economic Commission for Latin America and the Caribbean, 2013.
7 ECLAC. Shaping the future of social protection: access, fi nancing and solidarity. Santiago: Economic Commission for Latin America and the Caribbean, 2006.
8 Cetrángolo O, Goldschmit A. Fiscal decentralization: increasing social cohesion among widely disparate territorial units. In: Decentralization and reform in Latin America. Improving intergovernmental relations (Chapter 3). Brosio G, Jiménez JP, eds. London: Edward Elgar Publishing, 2013: 38–69.
9 Wagstaff A. Social health insurance vs. tax-fi nanced health systems—evidence from the OECD. Policy Research Working Paper 4821. Washington, DC: The World Bank, 2009.
10 Titelman D. Reformas al sistema de salud en Chile: desafíos pendientes. Financiamiento del desarrollo series, No. 104 (LC/L.1425-P/E). UN publication, Sales No. S.00.II.G.99. Santiago: Economic Commission for Latin America and the Caribbean, 2000.
11 Kutzin J. Health fi nancing for universal coverage and health system performance: concepts and implications for policy. Bull World Health Organ 2013; 91: 602–11.
12 ECLAC. Observatorio de Igualdad de Género de América Latina y el Caribe. Informe anual 2012. Santiago: Economic Commission for Latin America and the Caribbean, 2013.
13 Musgrave R, Musgrave P. Public fi nance in theory and practice, New York: McGraw-Hill Inc, 1989.
14 Oates W. Fiscal federalism. New York: Harcourt-Bracem, 1972.15 Van Doorslaer E, Wagstaff A, Rutten F, eds. Equity in the fi nance
and delivery of health care: an international perspective. Oxford: Oxford University Press, 1992.
16 Medici AC. Seguros públicos de salud en América Latina: ¿Cuáles son las perspectivas?. In: Seguro público de salud. Aportes para un debate abierto. Compiled by Báscolo EP. Rosario: Instituto de la Salud “Juan Lazarte”, 2004: 7–21.
17 Afonso J. El fi nanciamiento bifurcado de la protección social y de la salud en Brasil. In: Cohesión social en América Latina y el Caribe: una revisión perentoria de algunas de sus dimensiones. Sojo A, Uthoff A, eds. Santiago: Economic Commission for Latin America and the Caribbean, 2007: 209–18.
18 Marten R, McIntyre D, Travassos C, et al. An assessment of progress towards universal health coverage in Brazil, Russia, India, China, and South Africa (BRICS). Lancet 2014; published online April 30. http://dx.doi.org/10.1016/S0140-6736(14)60075-1.
19 Cercone J, Pacheco J. Costa Rica: good practice in expanding health care coverage. Lessons from reforms in low and middle-income countries. In: Good practices in health fi nancing. Gottret P, Schieber J, Waters H, eds. Washington, DC: The World Bank, 2008: 182–226.
20 Titelman D, Uthoff A. El mercado de la salud y las reformas al fi nanciamiento de los sistemas de salud. In: Ensayos sobre el fi nanciamiento de la seguridad social en salud. Los casos de: Estados Unidos, Canadá, Argentina, Chile, Colombia. Compiled by Titelman D, Uthoff A. Santiago: Fondo de Cultura Económica, 2000.
21 Bitran R, Urcullo G. Good practice in expanding health coverage—lessons from reforms. In: Good practices in health fi nancing. Gottret P, Schieber J, Waters H, eds. Washington, DC: The World Bank, 2008: 89–136.
22 Giedion U, Acosta O. Sistema de salud y democracia, el caso de Colombia. In: La política fi scal para el afi anzamiento de las democracias en América Latina: refl exiones a partir de una serie de estudios de caso. Compiled by Bárcena A, Kacef O. Santiago: Economic Commission for Latin America and the Caribbean, 2011: 127–58.
23 Glassman A, Escobar ML, Giuff rida A, Giedion U. From few to many; ten years of health insurance expansion in Colombia. Washington, DC: Inter-American Development Bank and The Brookings Institution, 2009.
24 PAHO. Perfi l de sistemas de salud de la República Oriental del Uruguay: monitoreo y análisis de los procesos de cambio y reforma. Washington, DC: Pan American Health Organization, 2009.
universal health coverage, countries in the region must strengthen and universalise the fi nancial coverage of health risk, so that the need to make out-of-pocket payments ceases to be a barrier to access to health services. The two basic challenges for improvement of equity and achievement of universal health coverage are the need to increase the fi nancial resources fl owing into the health sector, and to improve solidarity-based schemes.
Improvement of solidarity schemes will need the expansion of mandatory universal insurance systems and strengthening of the public sector. The fi rst demands a new model to integrate the health sector’s diff erent sources of fi nancing: general tax revenue, social security contributions, and private expenditure. The extent to which integration is achieved will chiefl y determine solidarity and universal health coverage.
In view of the labour market dynamics in Latin American countries and their uneven income distribution, eff orts to achieve universal health coverage will need large increases in public expenditure, which are constrained by fi scal restrictions. Accordingly, eff orts to increase eff ective health coverage will need to be accompanied by tax reforms geared to increasing the availability of public resources and to improving the eff ects of tax structures on income distribution.
Building capacity to move towards universal health coverage in Latin America needs action in four areas: (1) increased tax revenue and a balanced combination of resources from general taxation and payroll taxes that does not create incentives for informality, evasion, or avoidance; (2) eff orts by governments to increase the share of public expenditure in health, so that ability to make out-of-pocket payments is not an access barrier to health services; (3) improved allocation and distribution of that spending, by means of a new model to integrate diff erent sources, able to secure funds for subnational governments; and (4) equitable funding to increase the redistribution capacity of tax systems.ContributorsAll authors contributed equally.
Declaration of interestsWe declare no competing interests.
AcknowledgmentsThis paper accompanies a Series funded by the Rockefeller Foundation through a grant to ECLAC. We thank the commission and the foundation for convening various author meetings, and their participants for very helpful suggestions.
References1 Pan American Health Organization. Championing health:
sustainable development and equity. Strategic plan of the Pan American Health Organization 2014–2019. http://www.paho.org/hq/index.php?option=com_docman&task=doc_download&gid=22850&Itemid=270&lang=en (accessed June 1, 2014).
2 Pan American Health Organization. Strategy for universal health coverage. 154th Session of the Executive Committee. 2013. http://www.paho.org/hq/index.php?option=com_docman&task=doc_download&gid=25710&Itemid=270&lang=es (accessed June 1, 2014).
3 WHO. World health report 2013: research for universal health coverage. Geneva: World Health Organization, 2013.

Health Policy
www.thelancet.com Published online October 16, 2014 http://dx.doi.org/10.1016/S0140-6736(14)61780-3 5
25 Gómez J. El rol de la política tributaria para el fortalecimiento del Estado en América Latina. In: La política fi scal para el afi anzamiento de las democracias en América Latina: refl exiones a partir de una serie de estudios de caso. Compiled by Bárcena A, Kacef O. Santiago: Economic Commission for Latin America and the Caribbean, 2011: 71–94.
26 PAHO. Health in the Americas. Washington, DC: Pan American Health Organization, 2002.
27 Cetrángolo O, Gómez J. La tributación directa en América Latina y los desafíos a la imposición sobre la renta, Serie Macroeconomía del Desarrollo No. 60. Santiago: Economic Commission for Latin America and the Caribbean, 2007.
28 ECLAC. Social panorama of Latin America 2012. Santiago: Economic Commission for Latin America and the Caribbean, 2012.
29 Mesa-Lago C. Las reformas de pensiones en América Latina y su impacto en los principios de la seguridad social. Serie Financiamiento del Desarrollo No.144. Santiago: Economic Commission for Latin America and the Caribbean, 2004.
30 Bastagli F. From social safety net to social policy? The role of conditional cash transfers in welfare state development in Latin America. Working Paper No.60, December 2009. Brasilia: Centre for Analysis of Social Exclusion (CASE), London School of Economics and Political Science, 2009.
31 Romaguera P, Gallegos S. Financiamiento de la educación en Chile: desafíos de calidad y equidad”. In: La política fi scal para el afi anzamiento de las democracias en América Latina: refl exiones a partir de una serie de estudios de caso. Compiled by Bárcena A, Kacef O. Santiago: Economic Commission for Latin America and the Caribbean, 2011: 159–84.
32 Gómez J, Morán D. Informalidad y tributación en América Latina. Explorando los nexos para mejorar la equidad. Serie Macroeconomía del Desarrollo No. 124. Santiago: Economic Commission for Latin America and the Caribbean, 2012.
33 Savedoff W. How much should countries spend on health? Discussion paper 2–2003. Geneva: World Health Organization, 2003.