uncg spartan g's tryout participants must have a minimum of a 2.3 semester gpa at the time of...
TRANSCRIPT
“We discover and develop champions in life.” -The Spartan Way
UNCG SPARTAN G'S2018 SPRING TRYOUTS
INFORMATION PACKET
“We discover and develop champions in life.” -The Spartan Way
2018 UNCG Dance TeamSpring Tryouts
Spring tryouts will be held Sunday, April 22nd Tryout Fee: $20/person Times and locations are as follows:
Sunday, April 22, 2018
Time: 9 am - 1 pmLocation: Fleming Gym - Coleman BuildingPlease arrive by 8:30 am
Fleming Gym is located in the Coleman Building on the campus of UNCG. Participants can park in the Walker Avenue Parking Deck (1408 Walker Avenue) at a rate of $1 per hour.
All Tryout Sessions for the UNCG Dance Team are closed, without exception.
Video Tryout Submission
Submission of a tryout video will be accepted. However, video submissions must be submitted by April 22nd, 2018 and must include all of the following material:1. Eight 8-counts of Pom work (cadences/sidelines/fight song)2. Any Extensions you can do (arabesque, tilt, needle, etc)3. Double Pirouette4. Triple Pirouette5. Turns in second (AT LEAST: 5 into a double pirouette, 3 coming out of a
double pirouette, 3+ with pirouettes before AND after)6. Splits (right, left, center)7. Leaps (right, left, center)8. Calypso (both sides)9. Turning disc (right) 10. Channe turns (both sides)11. Pique turns (both sides)12. High kicks (R/L in front, R/L to the side, arabesque back)13. Freestyle (Eight 8-counts each of jazz and hip-hop choreography)14. Any special tricks/tumbling you can do (arial, kip-up, headspring, freeze, etc-- this is the only thingNOT mandatory for the video audition)
All questions regarding the UNCG Dance Team tryouts may be directed in writing to the head coach, Megan Cunningham at

“We discover and develop champions in life.” -The Spartan Way
General Tryout Information
All tryout participants must be: Current, full-time UNCG students (enrolled in a minimum of 12 credit hours) College transfers, or incoming freshman with an acceptance letter. All tryout participants must have a minimum of a 2.3 semester GPA at the time of tryouts.
Tryout Attire
You must present a “clean cut” image to be selected as a Spartan G's dancer. All participantsare expected to wear ALL BLACK at tryouts. Remove all piercings and cover all tattoos prior toarrival at tryouts.
Expected attire for tryouts is as follows:
Sunday:
MUST WEAR ALL BLACK SPORTS BRA OR CROP TOP, DANCE SHORTS OR LEGGINGS DURING TRYOUTS (CLOTHES MUST BE FITTED TO BODY).All uniforms are sports bra or crop tops so we want all team members to be comfortable wearing these.
Dark colored jazz pants or boy shorts Jazz shoes No bright colors or excessive glitter. We are going for a clean
and mature look but bold enough to see from the court. Bold but neutral makeup Hair down and out of face Shoes must be worn at all times. ("Foot undies" or sandal soles may be worn)
All tryout participants must available for practices:
• Practices are held Monday/Tuesday/Thursday from 7 pm - 9:30 pm.*Sometimes earlier/laterTake this into consideration when scheduling classes and work.
• Mandatory practices will be held the week before classes start in August (2-a-days to goover material learned from videos over the summer)
“We discover and develop champions in life.” -The Spartan Way
CHECKLIST OF REQUIREMENTS: Tryout Registration Fee: $20, check made payable to UNCG Athletics UNCG Dance Team Tryout Application (Appendix A)
All questions on the application must be completed before the application will be processed. Headshot (both listed below)
Please submit a COLOR photo headshot of yourself and submit along with the other requiredpaper-work (no selfies!) —AND—
Photo copy of UNCG Student ID, if you are a current student Proof of full-time enrollment at UNCG
Documentation must be provided via a print-out from UNCGenie that must contain partici-pant’s name and current GPA (Appendix B)
Copy of 2017 Fall Class Schedule (Appendix C) Students are considered full-time only if they are enrolled in a minimum of 12 credit hours Acceptance letter to UNCG, if an incoming freshman or transfer student
Copy of current physical (conducted within the past 6 months) (Appendix D)**(Must be signed by a physician)
Health Insurance Information Form (Appendix E) A copy of the front and back of the participants insurance card must accompany this form
Consent to Disclose Protected Health Information Form (Appendix F) This form will only be kept on file should the participant be selected as a member of the squad This form requires the signature of a parent or legal guardian, regardless of participant’s
age ICA Agreement & Release Form (Indemnity Form) (Appendix G)
Participants must have a parent or legal guardian’s signature This form requires the signature of a parent or legal guardian, regardless of participant’s
age Insurance Information & Injury Release Forms (Appendix H & I)
Appendix H requires the signature of a parent or legal guardian, regardless of partici-
pant’s age. Appendix I only requires a signature of a parent or legal guardian if partici-
pant is less than 18 years of age.
Sickle Cell Screening Results (Appendix J) **Returning members DO NOT have to complete thisrequirement. Prospective new members only! Lab Results AND Appendix J must be submitted before tryouts. No exceptions.
Please give 24 to 48 hours to receive your lab results. Appendix J requires the signature of a parent or legal guardian, regardless of participant’s
age.
By Mail: UNCG Athletics c/o Dacia Ijames 1408 Walker Ave, 101CC Coleman Bldg Greensboro, NC 27402
By Fax: To: Dacia Ijames Re: UNCG Dance
Tryouts Fax Number: 336.334.4063
By Drop-off: Room 101C, Coleman BuildingAttn: Dacia Ijames
General Tryout Information continued Tryout Paperwork Requirements All tryout participants must submit the following paperwork and bring their $20 tryout fee (checks made payable to UNCG Athletics) no later than Monday, April 16th at 5 pm NO EXCEPTIONS!The Tryout Application and the paperwork included in the UNCG Dance Team Tryout Packet must be submitted directly to the UNCG Dance Team Staff Advisor using one of the methods listed below. All tryout participants are encouraged to submit all paperwork as soon as possible so any issues that may arise can be addressed prior to the final deadline..
“We discover and develop champions in life.” -The Spartan Way
General Tryout Information continued
Candidates will be judged on, but are not limited to:
1. Eight 8-counts of Pom work (cadences/sidelines/fight song)2. Any Extensions you can do (arabesque, tilt, needle, etc)3. Double Pirouette4. Triple Pirouette5. Turns in second (AT LEAST: 5 into a double pirouette, 3 coming out of a double pirouette, 3+
with pirouettes before AND after)6. Splits (right, left, center)7. Leaps (right, left, center)8. Calypso (both sides)9. Turning disc (right)10. Channe turns (both sides)11. Pique turns (both sides)12. High kicks (R/L in front, R/L to the side, arabesque back)13. Freestyle (Eight 8-counts each of jazz and hip-hop choreography)14. Any special tricks/tumbling you can do (arial, kip-up, headspring, freeze, etc.
Do not assume that a weakness or lack of skill in any one area will automatically disqualify you as a team member. Display an eager and positive attitude at all times.
Candidates will tryout in groups of four and will be assigned by the coaching staff on Sunday.
The coaching staff will make all final decisions on team member selection. Any candidate that has questions after the team selections are announced may e-mail the UNCG Dance Team coach at [email protected] any time AFTER the weekend. Outbursts or questions from parents will not be accepted.
If you have ANY questions regarding paperwork or the general audition process, please con-tact the staff advisor in advance! Being proactive will insure you are prepared and cleared to participate in auditions.
Keep working on your skills! We look forward to meeting and working with you!
GO SPARTANS!
We are looking for well-rounded dancers with outstanding skills, technique and SCHOOL SPIRIT!
Results will be posted the next morning (Monday, April 23rd) and the head coach will send out an email to all participants. Please make sure the email you list is your PREFERRED email.
“We discover and develop champions in life.” -The Spartan Way
Q:
A:
Do you offer any partial or full scholarships for dancers?
No scholarships are currently provided to UNCG Dance Team members.
Q:
A:
Q:
A:
Q:
A:
Q:
A:
Q:
A:
What is the UNCG Dance Team squad size?
Our maximum squad size is 20 dancers.
When are tryouts?
The UNCG Dance Team holds tryouts in mid April.
What are the additional benefits of being a UNCG Dance Team member?
The UNCG Dance Team is sponsored by the UNCG Athletic Department. Team members are able to pre-register for classes, have access to the Athletic Training room and staff, study hall sessions, strength and conditioning coaches, uniforms, shoes, travel accommodations and meal stipend when traveling and tickets to UNCG’s home athletic events.
Does your team compete?
UNCG has competed at Nationals in the past. A decision has not been made if we will compete in 2018-19.Does your team attend summer camp?
Yes, the UNCG Dance Team attends a summer camp.
UNCG Dance Team Q&A
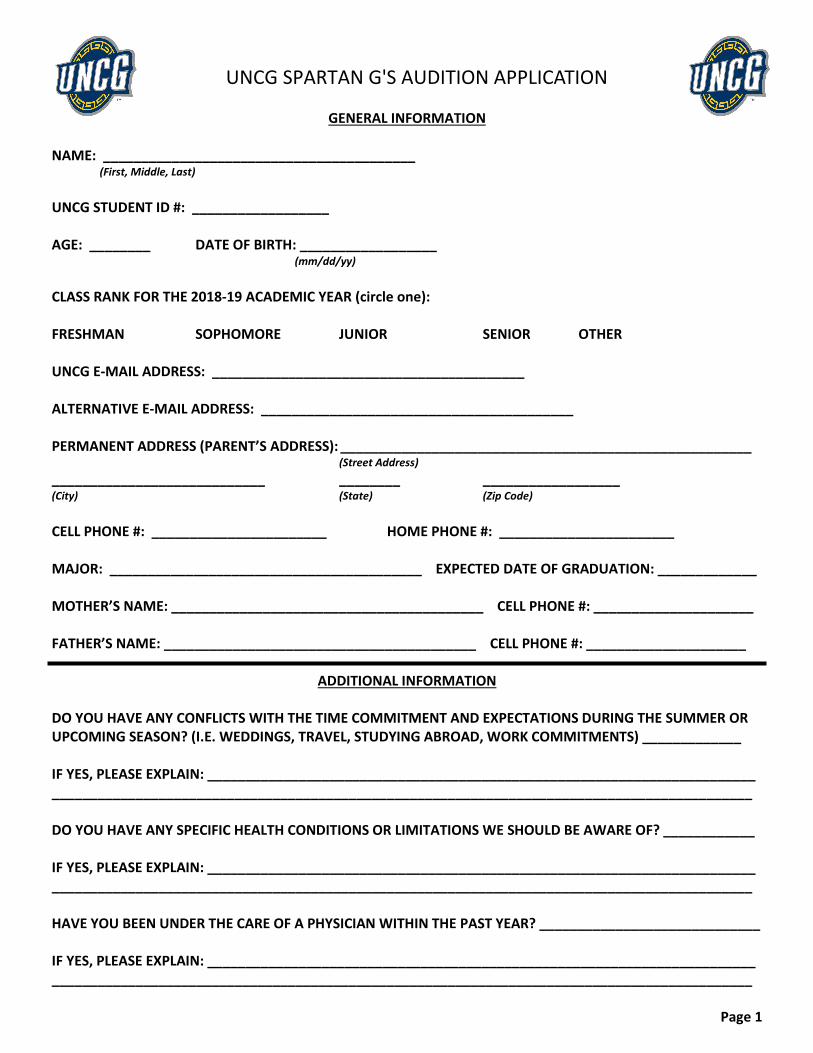
UNCG SPARTAN G'S AUDITION APPLICATION
GENERAL INFORMATION
NAME: _________________________________________ (First, Middle, Last)
UNCG STUDENT ID #: __________________
AGE: ________ DATE OF BIRTH: __________________ (mm/dd/yy)
CLASS RANK FOR THE 2018-19 ACADEMIC YEAR (circle one):
FRESHMAN SOPHOMORE JUNIOR SENIOR OTHER
UNCG E-MAIL ADDRESS: _________________________________________
ALTERNATIVE E-MAIL ADDRESS: _________________________________________
PERMANENT ADDRESS (PARENT’S ADDRESS): ______________________________________________________ (Street Address)
____________________________ ________ __________________ (City) (State) (Zip Code)
CELL PHONE #: _______________________ HOME PHONE #: _______________________
MAJOR: _________________________________________ EXPECTED DATE OF GRADUATION: _____________
MOTHER’S NAME: _________________________________________ CELL PHONE #: _____________________
FATHER’S NAME: _________________________________________ CELL PHONE #: _____________________
ADDITIONAL INFORMATION
DO YOU HAVE ANY CONFLICTS WITH THE TIME COMMITMENT AND EXPECTATIONS DURING THE SUMMER OR UPCOMING SEASON? (I.E. WEDDINGS, TRAVEL, STUDYING ABROAD, WORK COMMITMENTS) _____________
IF YES, PLEASE EXPLAIN: ________________________________________________________________________ ____________________________________________________________________________________________
DO YOU HAVE ANY SPECIFIC HEALTH CONDITIONS OR LIMITATIONS WE SHOULD BE AWARE OF? ____________
IF YES, PLEASE EXPLAIN: ________________________________________________________________________ ____________________________________________________________________________________________
HAVE YOU BEEN UNDER THE CARE OF A PHYSICIAN WITHIN THE PAST YEAR? _____________________________
IF YES, PLEASE EXPLAIN: ________________________________________________________________________ ____________________________________________________________________________________________
Page 1
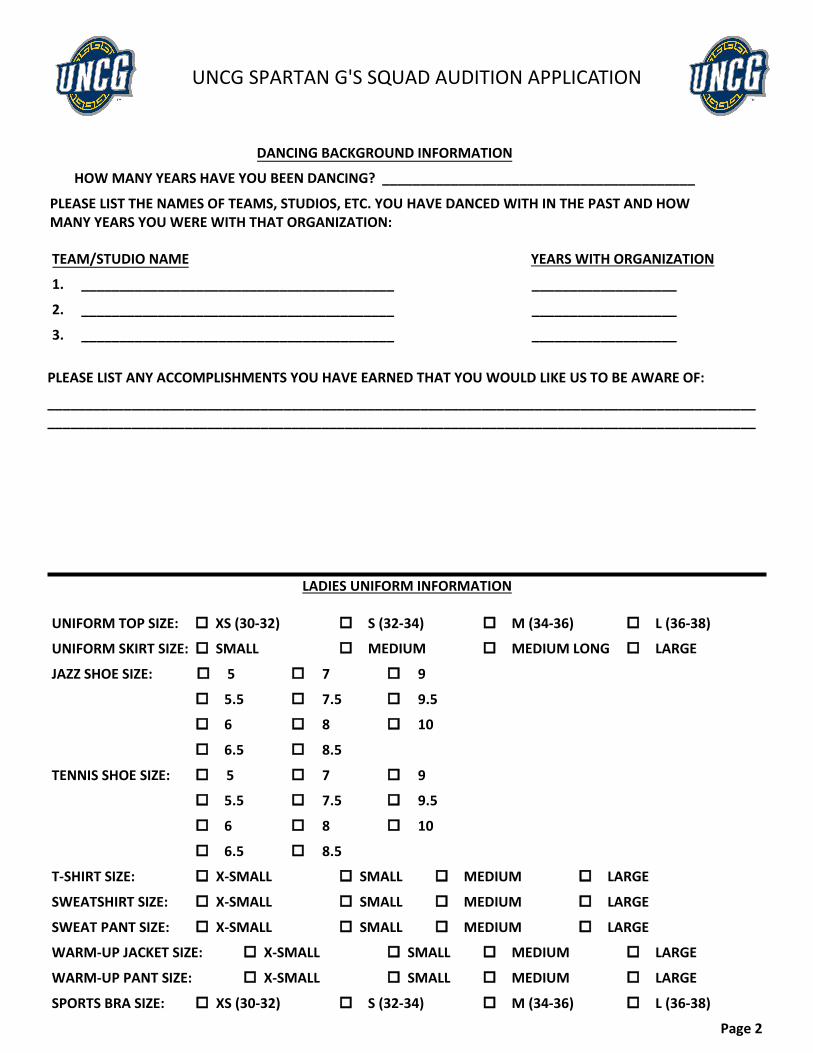
UNCG SPARTAN G'S SQUAD AUDITION APPLICATION
DANCING BACKGROUND INFORMATION
HOW MANY YEARS HAVE YOU BEEN DANCING? _________________________________________
PLEASE LIST THE NAMES OF TEAMS, STUDIOS, ETC. YOU HAVE DANCED WITH IN THE PAST AND HOWMANY YEARS YOU WERE WITH THAT ORGANIZATION:
TEAM/STUDIO NAME YEARS WITH ORGANIZATION
1. _________________________________________ ___________________
2. _________________________________________ ___________________
3. _________________________________________ ___________________
PLEASE LIST ANY ACCOMPLISHMENTS YOU HAVE EARNED THAT YOU WOULD LIKE US TO BE AWARE OF:
__________________________________________________________________________________________________________________________________________________________________________________________
LADIES UNIFORM INFORMATION
S (32-34) M (34-36) L (36-38)
MEDIUM MEDIUM LONG LARGE
UNIFORM TOP SIZE: o XS (30-32)
UNIFORM SKIRT SIZE: o SMALL
JAZZ SHOE SIZE: o 5 7 9
5.5 7.5 9.5
6 8 10
6.5 8.5
TENNIS SHOE SIZE: 5 7 9
5.5 7.5 9.5
6 8 10
6.5 8.5
T-SHIRT SIZE: X-SMALL SMALL MEDIUM LARGE
SWEATSHIRT SIZE: X-SMALL SMALL MEDIUM LARGE
SWEAT PANT SIZE: X-SMALL SMALL MEDIUM LARGE
WARM-UP JACKET SIZE: X-SMALL SMALL MEDIUM LARGE
WARM-UP PANT SIZE: X-SMALL SMALL MEDIUM LARGE
SPORTS BRA SIZE: XS (30-32) S (32-34) M (34-36) L (36-38)
Page 2
Appendix B
Sample print-out from UNCGenie:
Your Name Here
Appendix B
Sample print-out from UNCGenie:

UNCG CHEER AND DANCE PHYSICAL
Name: _________________________________________ Date: _____________ Sport: CHEER / DANCE
School Address: _______________________________________________________________________________
University ID: _______________ DOB: __________ Telephone Number: _______________________
Parents’ Name: _______________________________________________________________________________
Parents’ Address: ______________________________________________________________________________
List any allergies (including latex):___________________________ Last Tetanus: __________________
Medications currently taking (including birth control): ________________________________________________________________________________________________________________________________
*Please answer the questions below. Fill in details of “yes” answers in space provided.*
1. Have you ever been hospitalized? Yes No
2. Have you ever had surgery? Yes No
3. Have you ever passed out during exercise? Yes No
4. Have you ever been dizzy during exercise? Yes No
5. Have you ever had chest pain during exercise? Yes No
6. Have you ever had a head injury, seizure or unconscious? Yes No
7. Have you ever had heart trouble, or high blood pressure? Yes No
8. Has anyone in your family died suddenly before the age of 50 of heart problems? Yes No
9. Have you ever had a heat related illness?(cramps, dizzy or passed out) Yes No
10. Do you have any other medical problems?(ie asthma, diabetes, hepatitis,
Impaired function of any organ) Yes No
11. Do you have any menstrual irregularities or problems? Yes No
12. Do you wear glasses, contacts, braces of any kind, orthotics, hearing aid? Yes No
13. Have you ever injured (sprained, dislocated, fractured etc)? Circle all that apply.
Neck Chest Hip Thigh Knee Ankle Foot
Toes Lower Leg Elbow Arm Wrist Back Head
Fingers Shoulder
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Page 2
EXAMINATION
Height __________ Weight __________ RHR __________ BP __________
Heart ____________________ Lungs ____________________
Abdomen __________ General __________ Other __________
MUSCULOSKELETAL
Neck __________ Back __________ Shoulder __________ Knee __________
Elbow __________ Ankle __________ Wrist __________ Foot __________
Hip __________ Hand __________
ASSESMENT
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
RECOMMENDATION
_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
CLEARANCE
No Restrictions ____________________
Deferred Until ____________________
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
_________________________ _____________________________________ __________________ Name of Provider Signature of Provider Date
Appendix E
Health Insurance Information for 2018-19 Academic Year
Athlete’s Name__________________________________________________________ Date of Birth / /
Last First MI
Athlete’s Home Address___________________________________________________________________
___________________________________________________________________
City State Zip Code
Athlete’s University ID # Athlete’s SS#________________________
Sport _______________________________
Complete Name of Insurance Company ______________________________________________________
Address to Mail Claim ______________________________________________________
______________________________________________________
______________________________________________________
Policy Holder’s Name_________________________________________________________
Last First MI
Policy Holder’s Address __________________________________________________________________________
Number Street
__________________________________________________________________________
City State Zip Code
Policy Holder’s SS# - - Policy Holder’s DOB / /
Please copy the front and back of your insurance card and affix it below.
(Front) (Back)
Appendix F
Consent to Disclose Protected Health Information
I hereby consent to allow the UNCG Athletic Training Staff to disclose Protected Health Information
concerning any injury or athletically related illness to my coaching staff and the UNCG Athletics
Administration.
I hereby consent to allow UNCG Athletic Department Personnel to disclose Protected Health Information
concerning any injury or athletically related illness to my parents, legal guardians, or wards.
I authorize payment of medical benefits to all providers of services for all services and materials they
provide during the care of any injury/illness.
I agree to supply any and all information requested by my primary insurance, UNCG and the excess
insurance company, and the NCAA and their excess insurance company in a timely manner in order to
expedite the claim process.
I hereby authorize UNCG and their excess insurance company to secure and inspect copies of case history
records, lab reports, diagnoses, x-rays, and other data pertaining to the injury/illness I am receiving care for
or previous confinements, if disabilities relevant, to the care of the injury/illness.
I authorize the UNCG Athletic Training staff and/or my coach to hospitalize and secure treatment for me
for any athletic injury/illness. If the athlete is under 18 years of age, the undersigned parent/guardian grants
permission the UNCG Athletic Training staff and/or the coach to hospitalize and secure treatment for their
son/daughter/ward for any athletic injury/illness.
This consent is irrevocable for the duration of any executed disclosure due to an athletically related illness
or injury.
A photo static copy of this consent shall be deemed as effective and valid as the original.
I will notify the UNCG Athletic Training staff immediately upon any change in the above health insurance
information.
_____________________________________________________ ______________
Athlete’s Signature Date
_____________________________________________________ ______________
Parent/Guardian Signature Date
Parent/Guardian’s Name _________________________ Relationship______________________
Home Phone _________________________ Work Phone______________________
Parent/Guardian’s Name _________________________ Relationship______________________
Home Phone _________________________ Work Phone______________________
Alternate Person to Contact in Case of Emergency __________________________________
Relationship __________________________________
Home Phone __________________________________
Work Phone __________________________________
Appendix G
UNCG Athletics
Waiver, Release of Liability, & Indemnity Agreement
I am aware and understand that any physical activity, including (but not limited to) soccer, basketball, volleyball, tennis,
baseball, softball, cheerleading, weight lifting and conditioning, can be a dangerous activity, which may result in serious
personal injury. These injuries include, but are not limited to, serious neck and spinal injuries, complete or partial pa-
ralysis, brain damage, serious injuries to bones, joints, ligaments, and tendons; serious injury to other areas of the
body, general health and well-being, and even DEATH.
In consideration of the University of North Carolina Greensboro (UNCG) permitting me to use its Athletic Facilities, I agree to the following:
I will obey all rules established by UNCG Athletics for the use of its facilities.
I will obey any and all instructions or directions given to me by UNCG Athletic personnel concerning the use of its facili-ties.
I assume all financial responsibility for any injury or damage as a result of my use of UNCG Athletic Facilities.
To the fullest extent allowed by law, I hereby release and agree to hold harmless UNCG, its trustees, officers, agents, employees, coaches, professors, students, athletic trainers and other medical personnel from any and all liability arising out of any injuries to my person or property, or losses of any kind or nature whatsoever, which may result from, or which arise in connection with, my use of the UNCG Athletic Facilities, even to the extent that such injuries may arise from the negligence of those listed above.
To the fullest extent allowed by law, I will indemnify and hold harmless, including attorney’s fees and court costs, those
listed above for any injury to person or property that I may cause others in the course of my use of the UNCG Ath-
letics Facilities or due to my failure to obey any rules, directions, or instructions.
I acknowledge that I have read this agreement fully and that I understand the legal rights I waive by signing this agree-ment. I further acknowledge that I am aware of the potential hazards incident to engaging in physical activity.
_________________________________ ___________________________________ Signature of Participant Date Signature of UNCG Representative Date
_________________________________ ___________________________________ Printed Name of Participant Printed Name of UNCG Representative
______________________________________ __________________________________________
Printed Name of Parent/Guardian Date Signature of Parent/Guardian
Insurance Information
2018-2019
UNCG currently requires all students to have primary medical insurance. It is the responsibility of each student to prove that
he/she has medical insurance, and if not, the student account will be automatically billed per semester. The premium has not been finalized for the 2018-19 year but will be announced this summer. We strongly recommend that you research and
understand your insurance benefits prior to your arrival on campus. If the benefits are insufficient or non-existent in
NC(HMO), you may wish to call your carrier to inquire about alternatives. Another option would be to choose/default to the
school policy. Should the status of your insurance coverage change during the course of the school year, please be sure to
communicate this with the athletic training staff immediately. The UNCG Department of Intercollegiate Athletics carries an
excess insurance policy for each student-athlete to cover athletic related injuries. This policy carries a $0 deductible, per
injury.
When a student-athlete is injured during athletic participation, all medical insurance claims will be filed with your personal in-
surance company. Once your primary insurance company pays their portion of your bill, our excess policy will cover the
remain-ing balance. In order to help process payments you may be required to provide the following:
1) Itemized bills from all medical providers
2) Explanations of Benefits (EOB’s) from your medical insurance
company
All injuries must be reported to a staff athletic trainer. We will advise the student-athlete of the protocol that is recommended for
treatment and referral, and as appropriate, steps necessary to best insure proper payment by all insurance parties involved. Please
visit the student health center website to learn how to self-file charges incurred at the Student Health Center (SHC). The SHC
charges are eligible for insurance coverage, but are not submitted by the provider. Please note that charges incurred for services
at the SHC will be placed on the UNCG Student Account and lack of payment could affect future class registration, graduation
etc. At no time should the student-athlete seek medical treatment without the prior approval of the Athletic Trainer. This action
will jeopardize and/or remove responsibility from UNCG and its excess accident insurance company for payment of medical
bills.
Your signature on this letter indicates that you have read, understand and will comply with all that is stated above. Any false in-
formation will nullify UNCG from responsibility regarding any medical bills.
“I, _______________________________________ have read the above letter and understand that UNCG is responsible on a
secondary basis only for injuries which occur in an official UNCG athletic practice or competition. I also verify, that all of the
insurance information I have provided is correct and complete.”
_______________________________________ ______________________ _________________
Student-Athlete Signature UNCG Student ID # Date
_______________________________________________ _________________
Parent Signature Date
Appendix I
2018-2019 UNCG Intercollegiate Athletics Agreement,
Injury Release, Assumption of Risk, and Athlete Responsibility Form
UNCG Intercollegiate Athletic Sports:
Baseball, Basketball, Cheerleading, Cross Country, Dance, Golf, Soccer, Softball, Tennis, Track & Field, Volleyball
I am aware that trying out for, practicing or playing in any sport can be a dangerous activity involving MANY RISKS
OF INJURY. I understand the inherent potential dangers and risks of trying out for, playing and practicing in the above
intercollegiate sports may be catastrophic in nature and may include, but are not limited to, death; serious neck and spi-
nal injuries which may result in complete or partial paralysis or brain damage; serious injury to virtually all bones, joints,
ligaments, muscles, tendons and other elements of the muscular-skeletal system, including loss of limb; and serious inju-
ry or impairment to other parts of my body, general health and well-being.
Because of the dangers of participating in any of the above sports, I recognize the importance of following the coach’s
instructions regarding playing techniques, training, rules of the sport and other team rules, and of following such instruc-
tions. I also realize that during my entire athletic career at UNCG I have a responsibility to my own physical well being
and must accurately report any injury in a timely manner to the UNCG Sports Medicine Staff. I will follow the guide-
lines established by the UNCG Sports Medicine Staff for rehabilitation from any injury. If I have any questions regard-
ing my injury or care, I will ask the UNCG Sports Medicine Staff. I will also abide by the rules of the sport in which I
participate. I realize that adherence to these responsibilities in no way assures me of avoiding or lessening all injuries,
including those of catastrophic nature, but by following them, I may decrease the severity of some injuries.
In consideration of UNCG permitting me to try out for, practice, play or otherwise participate in the above listed inter-
collegiate sports and to engage in all activities related to the team, including, but not limited to practicing, playing and
traveling, I hereby voluntarily assume all risks associated with participation and agree to hold harmless The University
of North Carolina at Greensboro, its agents, officers and employees including, but not limited to, the UNCG Athletics
staff from any and all liability, claims, causes of action or demands of any kind and any nature whatsoever which may
arise by or in conjunction with my participation in any activities related to the UNCG Intercollegiate Athletics Program
except in the event of their gross negligence. The terms of this Agreement shall serve as a release and assumption of risk
for my heirs, estate, executor, administrators, assignees and all members of my family.
To the best of my knowledge, I am in good health and suffer no disability or condition which renders my participation in
the sport(s) or other athletics activity medically inadvisable, or otherwise limits my ability to participate in such sport(s)
or athletics activity without restriction.
I hereby authorize the coach or other appropriate UNCG personnel to obtain in my behalf first aid, emergency medical
care, or if necessary admission to an accredited hospital, when such care is necessary for the treatment of any injuries I
may sustain while participating in any activity associated with UNCG intercollegiate sports, including practices, compe-
tition and travel. I also hereby consent to the administration of emergency medical treatment in the event I am unable
subsequent to such injury to give such consent as otherwise necessary.
Name_________________________________________________ Date of Birth _________________
Signature_______________________________________________ Date ________________________
Parent/Guardian Signature _________________________________ Date_________________________
(if student-athlete is less than 18 years of age)
Appendix J
UNIVERSITY OF NORTH CAROLINA at GREENSBORO SPORTS MEDICINE
Sickle Cell Trait Screening Declination and Release of Claims
**Must submit this form along with Sickle Cell Results
(signing this form is NOT a replacement for testing, still must have Sickle Cell trait screening)
About Sickle Cell Trait: Sickle cell trait is an inherited condition of the oxygen-carrying protein, hemoglobin, in the red blood cells.
Sickle cell trait is a common condition (> three million Americans).
Although Sickle cell trait is most predominant in African-Americans and those of Mediterranean, Middle Eastern, India, Caribbean, and
South and Central American ancestry, persons of all races and ancestry may test positive for sickle cell trait.
Sickle cell trait is usually benign, but during or after exercise, hypoxia(lack of oxygen) in the muscles may cause sickling of red blood cells
(red blood cells changing from a normal disc shape to a crescent or “sickle” shape), which can accumulate in the bloodstream and
“logjam” blood vessels, leading to collapse, personal injury and/or DEATH from the rapid breakdown of muscles starved of blood.
If the UNCG Sports Medicine Staff and the student-athlete’s coaches are made aware that a student-athlete has sickle cell trait, then col-
lapse, personal injury and/or DEATH from exercise may be avoided or decreased if the student-athlete follows the directives of the
Staff and his/her medical professionals. Such directives may include, but not be limited to, reduced or modified activity during prac-
tice and/or games.
Sickle Cell Screening: If the student-athlete does not have knowledge of their sickle cell trait status, the NCAA recommends that screening is performed. In order
to decrease the risk of collapse, personal injury and/or DEATH to its student-athletes, the University of North Carolina Greensboro
requires that all student-athletes who do not know their sickle cell status undergo the screening.
I ,______________________________, (parent or guardian name here if student-athlete is under 18)understand and
acknowledge that, in order to decrease the risk of collapse, personal injury and/or DEATH to its student-athletes the
University of North Carolina at Greensboro recommends that all student-athletes have knowledge of their sickle cell trait
status. Additionally, I have read and fully understand the aforementioned facts about sickle cell trait and sickle cell trait
testing. I understand that exercising without knowledge of sickle cell trait status can increase the risk of collapse, personal
injury and/or DEATH during or after exercise.
I hereby affirm that I have fully and accurately disclosed in writing any prior medical history and/or knowledge of sickle
cell trait status to UNCG Athletic Training staff.
I do not wish to undergo sickle cell trait testing (in the case of a minor, the parent or guardian does not wish the minor to
undergo sickle cell trait testing) through UNCG, as I (or my dependent) has been screened previously and I am able to pro-
vide these results. I (or in the case of a minor the parent or guardian) voluntarily agree to release, indemnify and hold harm-
less, regardless of their negligence, the State of North Carolina, the University of North Carolina at Greensboro, its officers,
employees, agents and volunteers from any and all costs, liabilities, expenses, claims, demands, or causes of action on ac-
count of any loss, personal injury or DEATH that might result from this decision to not be screened for sickle cell trait and/
or from any incorrect information that I or any person on my behalf provided to UNCG Athletic Training staff about sickle
cell trait status.
I have read and signed this document with full knowledge that I may be giving up rights that I may otherwise be entitled to
if I had not signed it. I am at least 18 years of age and competent to sign this waiver.
_________________________________________ ____________________________________
Student-Athlete Signature Date
_________________________________________ ____________________________________
Sport University ID#
_________________________________________ ____________________________________
Parent/Guardian Signature Date
_________________________________________ ____________________________________