tumours of the pleura - iarc.fr · spontaneous pneumothorax {943}, mass lesions and/or segmental or...
TRANSCRIPT
CHAPTER 2
Tumours of the Pleura
Mesothelioma is the most frequent neoplasm affecting the pleu-ra and remains a major health threat for many years to come.Although the causation by asbestos is firmly established sincemore than 50 years, in many world regions, the use of this dan-gerous carcinogen peaked between 1970 and 1990. Althoughnow banned in the USA and most European countries, inci-dence and mortality rates are still climbing. In Western Europealone, more than 200 000 mesothelioma deaths have been pre-dicted to occur during the next 25 years. Despite this grim out-look, the worldwide production of asbestos has not declinedsignificantly.Less is known about the cellular and molecular mechanismsoperative in the evolution of asbestos-induced mesothelioma.Clastogenic effects are well documented, but the sequentialacquisition of genetic alterations which typically form the basisof tumour development, are still poorly understood. During thepast decade, several studies have identified sequences of theoncogenic SV40 virus in human mesotheliomas, but it remainsto be shown whether or not SV40 is causally involved in theiretiology.

126 Tumours of the pleura
WHO histological classification of tumours of the pleura
__________1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {6} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
Mesothelial tumours Diffuse malignant mesothelioma 9050/3
Epithelioid mesothelioma 9052/3Sarcomatoid mesothelioma 9051/3Desmoplastic mesothelioma 9051/3Biphasic mesothelioma 9053/3
Localized malignant mesothelioma 9050/3Other tumours of mesothelial origin
Well differentiated papillary mesothelioma 9052/1Adenomatoid tumour 9054/0
Lymphoproliferative disordersPrimary effusion lymphoma 9678/3Pyothorax - associated lymphoma
Mesenchymal tumoursEpithelioid hemangioendothelioma 9133/1
Angiosarcoma 9120/3Synovial sarcoma 9040/3
Monophasic 9041/3Biphasic 9043/3
Solitary fibrous tumour 8815/0Calcifying tumour of the pleuraDesmoplastic round cell tumour 8806/3

127WHO and TNM classification
__________
1 {738,2045}.2 A help desk for specific questions about the TNM classification is available at http://www.uicc.org/tnm/.3 The regional lymph nodes are the intrathoracic, internal mammary, scalene and supraclavicular nodes.
TNM classification 1,2
T – Primary TumourTX Primary tumour cannot be assessedT0 No evidence of primary tumour
T1 Tumour involves ipsilateral parietal pleura, with or without focalinvolvement of visceral pleura
T1a Tumour involves ipsilateral parietal (mediastinal, diaphragmatic)pleura. No involvement of visceral pleura
T1b Tumour involves ipsilateral parietal (mediastinal, diaphragmatic)pleura, with focal involvement of the visceral pleura
T2 Tumour involves any ipsilateral pleural surfaces, with at least one ofthe following:– confluent visceral pleural tumour (including the fissure)– invasion of diaphragmatic muscle– invasion of lung parenchyma
T3* Tumour involves any ipsilateral pleural surfaces, with at least one ofthe following: – invasion of endothoracic fascia– invasion into mediastinal fat– solitary focus of tumour invading soft tissues of the chest wall– non-transmural involvement of the pericardium
T4**Tumour involves any ipsilateral pleural surfaces, with at least one ofthe following: – diffuse or multifocal invasion of soft tissues of chest wall– any involvement of rib– invasion through diaphragm to peritoneum– invasion of any mediastinal organ(s)– direct extension to contralateral pleura– invasion into the spine– extension to internal surface of pericardium– pericardial effusion with positive cytology– invasion of myocardium– invasion of brachial plexus
Notes: *T3 describes locally advanced, but potentially resectable tumour **T4 describes locally advanced, technically unresectable tumour
N – Regional Lymph Nodes3
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Metastasis in ipsilateral bronchopulmonary and/or hilar lymph
node(s) N2 Metastasis in subcarinal lymph node(s) and/or ipsilateral internal
mammary or mediastinal lymph node(s) N3 Metastasis in contralateral mediastinal, internal mammary, or hilar
node(s) and/or ipsilateral or contralateral supraclavicular or sca-lene lymph node(s)
M – Distant Metastasis
MX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping
Stage IA T1a N0 M0Stage IB T1b N0 M0Stage II T2 N0 M0Stage III T1, T2 N1 M0
T1, T2 N2 M0T3 N0, N1, N2 M0
Stage IV T4 Any N M0Any T N3 M0Any T Any N M1
TNM classification of pleural mesothelioma

128 Tumours of the pleura - Mesothelioma
Definition
Diffuse malignant mesothelioma: a malig-nant tumour arising in the pleura frommesothelial cells, and showing a diffusepattern of growth over the pleural sur-faces.
ICD-O Codes
Epithelioid mesothelioma 9052/3Sarcomatoid mesothelioma 9051/3Desmoplastic mesothelioma 9051/3Biphasic mesothelioma 9053/3
Synonyms
This tumour is properly referred to as “dif-fuse malignant mesothelioma”, but isoften abbreviated as “malignant meso-thelioma” or just “mesothelioma.” Careneeds to be taken when using theseterms, since localized mesothelialtumours exist in the pleura and have dif-ferent behaviour.
Epidemiology
Pleural mesotheliomas are largely seenin patients over 60 years of age, but theage distribution is wide and occasionaltumours are observed in children. InNorth America tumours in males outnum-ber those in females by approximately
9:1, but in other countries such as theUK, France and Australia this ratio islower.In North America the incidence ofmesothelioma in females is about 2-3/million/yr and this number is essentiallyunchanged over the last 30 years {8}. Inmen the incidence is now about 20/mil-lion per year. The male incidenceincreased steadily until the early 1990’sbut appears to have peaked and there isa suggestion that the numbers aredecreasing. The experience in NorthAmerica is distinctly different from that inAustralia, France and the UK, where theincidence is considerably higher andnumber continue to increase. For exam-ple, in Australia, the current incidence in2000 was 60/million in men and 11/mil-lion in women {1156}. Within Europe, themesothelioma burden varies coniderably.For practical purposes the mortality ofpleural mesothelioma is 100%. It is pos-sible that some very early stage tumourshave been cured by so-called triplemodality therapy: extrapleural pneu-monectomy followed by chemotherapyand radiation therapy, but this remains tobe proven and would only apply to asmall number of cases.
Etiology
AsbestosIn most industrialized countries, greaterthan 90% of pleural mesotheliomas inmen are related to prior asbestos expo-sure. In women in North America onlyabout 20% of tumours are caused byasbestos {1862}. In other countries, par-ticularly the UK and Australia, whereextensive use was made of crocidolite,the proportion of mesotheliomas inwomen related to asbestos exposure ishigher. The latency period is typicallyvery long, with a mean of 30-40 years.Asbestos rarely if ever producesmesothelioma with a latency period lessthan 15 years. From past exposure,future mortality from mesothelioma hasbeen estimated. In the UK, the number ofdeath cases is expected to peak in 2015-2020, with more than 2000 per year{1588}. Another study postulated that inWestern Europe approximately a quarterof a miilon people will die from asbestos-induced mesothelioma over the next 35years, men born around 1945-1950being at highest risk {1587}.However, recent European incidencerates have already started to level off{1346,1347}.
Mesothelioma J.M. SametH. Weill
V. RuschT.V. Colby
P. VogtE. BrambillaW.D. Travis
A. Churg K. InaiV. Roggli M. PraetF. Galateau-Salle N.G. OrdonezPh.T. Cagle S.P. HammarA.R. Gibbs J.R. TestaPh.S. Hasleton A.F. GazdarD.W. Henderson R. SaracciJ.M. Vignaud R. Pugatch
Fig. 2.01 Asbestos imports into the United Kingdom and predicted mesotheliomadeaths. The mortality is expected to reach a maximum around the year 2020. From J. Peto et al. {1588}.
Fig. 2.02 European pleural mesothelioma incidence. Truncated (40-74) age-stan-dardized rates per 100,000 person-years. From F. Montanaro et al. {1347}.
129Mesothelioma
Fibre types. There are distinct differ-ences in the propensity of the differentasbestos fibre types to cause mesothe-lioma. Amphibole (amosite and crocido-lite) asbestos is considerably morepotent than chrysotile, and crocidolite ismore dangerous than amosite. The exactratio among these 3 fibres depends uponthe approach used to investigate theproblem: a recent report of estimates ofcohort, mean fibre exposure suggesteda ratio of 500:100:1 (crocidolite:amo-site:chrysotile) for relative risk {858}.
SV40Some polio vaccines used during 1955and 1962 were contaminated with theSimian monkey virus 40 (SV40) and thisinfection has since spread to millions ofpeople in several world regions, includ-ing North America and most Europeancountries Several studies have shown,that some human neoplasms, in particu-lar, mesothelioma, brain tumours, bonesarcomas and non-Hodgkin lymphomasfrequently contain sequences of SV40, ahighly oncogenic DNA virus in rodents{2085}. For mesotheliomas, this was firstreported in 1994 {283} and has beenconfirmed in subsequent analyses {668}.SV40 induces DNA strand breaks inhuman mesothelial cells {253} and caus-es pleural mesotheliomas in hamsters{374}. The viral large T-antigen (Tag)inactivates the function of the tumoursuppressor genes TP53 and retinoblas-toma (RB) and induces chromosomalaberrations {106,285}. The small t-anti-gen (tag) may contribute to transforma-tionby binding to the protein phos-phatase PP2A {106,668}.Whether a latent SV40 infection is acausal factor in the development ofmesothelioma, remains to be assessed.Epidemiological studies provided no evi-dence that populations which received
the contaminated polio vaccine have anelevated cancer risk {542}.
Other causesThese include the non-asbestos fibre,erionite (seen only in Cappadocia,Turkey), therapeutic radiation, and possi-bly processes that lead to intense pleuralscarring such as prior plombage therapyfor tuberculosis.
Pathogenesis
A considerable fraction of inhaledasbestos fibers remain permanentlyentrapped in lung tissue. The majority ofthese fibers remain naked, without caus-ing a tissue reaction: these are probablyresponsible for the clastogenic, and,eventually, carcinogenic effects. A minor-ity of asbestos fibers induce an accumu-lation of monocytes and become sur-rounded and encapsulated by multinu-cleated macrophages. This process isassociated with deposition of protein andof haemoglobin-derived iron, resulting inthe formation of ferruginous bodies.
Clinical features
Signs and symptoms The most common presenting symptomsin mesothelioma are dyspnoea, usuallydue to a large pleural effusion, and chest
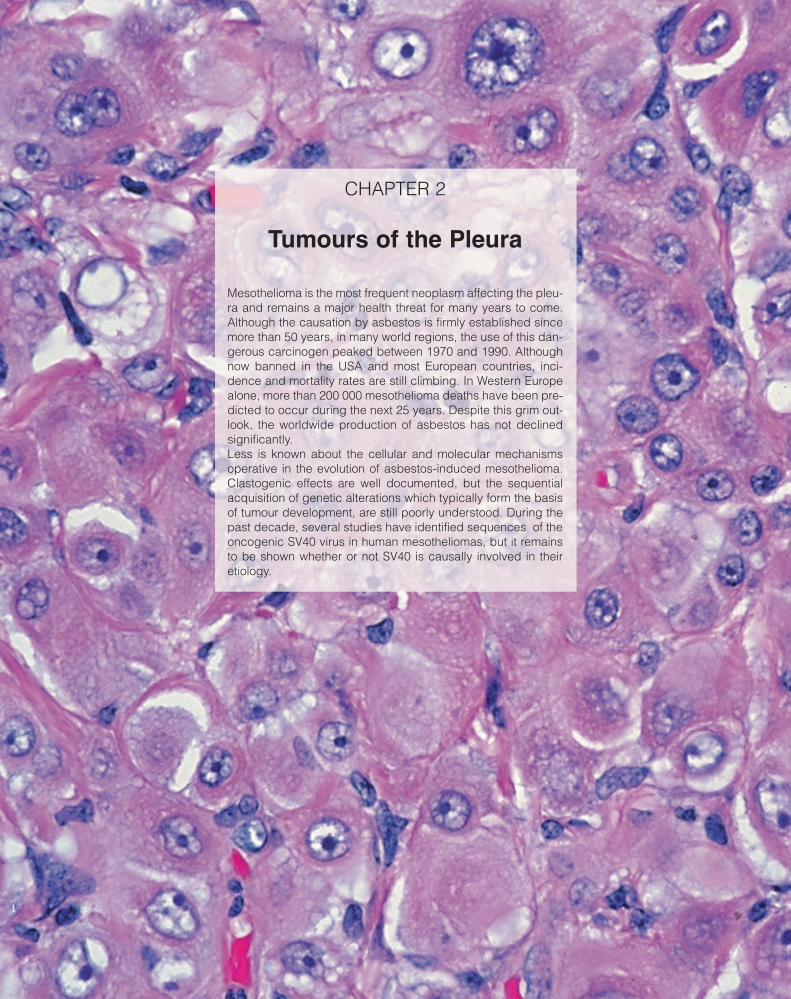
Fig. 2.05 Diffuse malignant mesothelioma. In this CTscan, the pleura shows marked diffuse thickeningby mesothelioma, with resulting encasement of thelung.
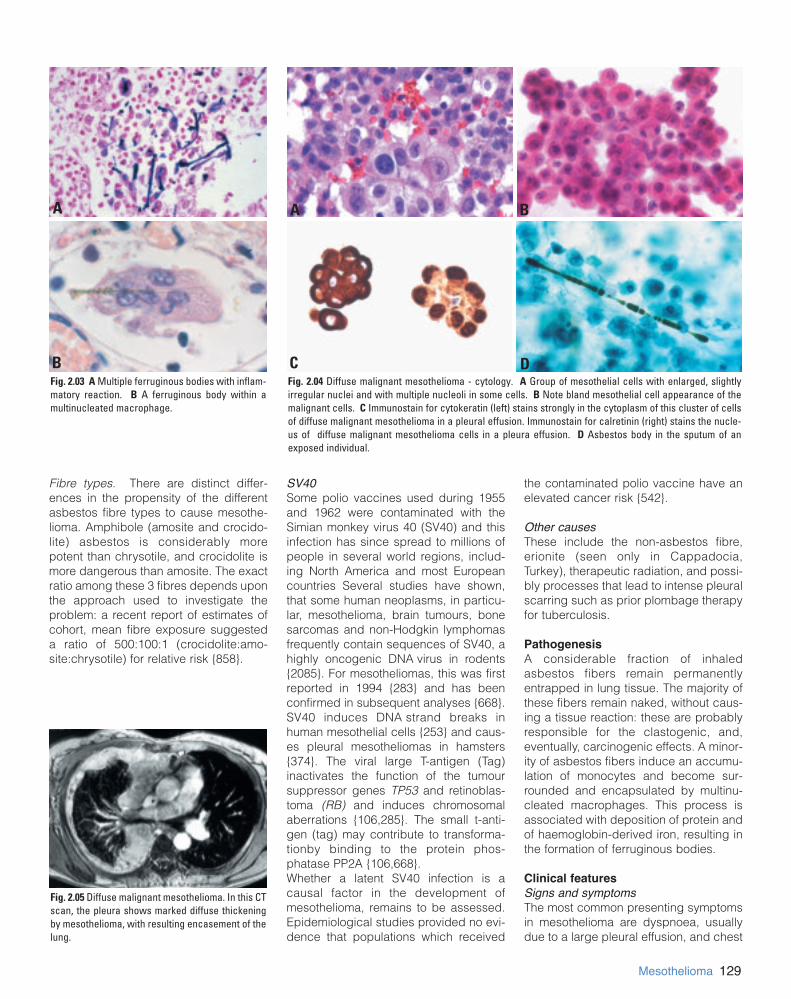
Fig. 2.03 A Multiple ferruginous bodies with inflam-matory reaction. B A ferruginous body within amultinucleated macrophage.
A
B CFig. 2.04 Diffuse malignant mesothelioma - cytology. A Group of mesothelial cells with enlarged, slightlyirregular nuclei and with multiple nucleoli in some cells. B Note bland mesothelial cell appearance of themalignant cells. C Immunostain for cytokeratin (left) stains strongly in the cytoplasm of this cluster of cellsof diffuse malignant mesothelioma in a pleural effusion. Immunostain for calretinin (right) stains the nucle-us of diffuse malignant mesothelioma cells in a pleura effusion. D Asbestos body in the sputum of anexposed individual.
A
D
B

130 Tumours of the pleura - Mesothelioma
wall pain {796}. These may be associat-ed with constitutional symptoms, espe-cially weight loss and malaise. Additionalclinical features include chills, sweats,weakness, fatigue, malaise and anorexia{18}. Unusual presentations includespontaneous pneumothorax {943}, masslesions and/or segmental or lobar pul-monary collapse, and mediastinal inva-sion with laryngeal nerve palsy or superi-or vena caval obstruction. Myalgias,aphonia, dysphagia, abdominal disten-sion, nausea and a bad taste in themouth have also been reported {1189}.
Imaging On a chest radiograph malignantmesothelioma often manifests as a largepleural effusion that may obscure anunderlying pleural mass or thickening. Itis not unusual to see associated pleuralplaques. The pleural disease may takeon a circumferential pattern of involve-ment with disease extending along thefissural, mediastinal and/or pericardialpleura. The ipsilateral hemithorax mayappear contracted. CT scanning andMRI better define the extent of pleuraldisease, in particular chest wall,diaphragmatic, pericardial, mediastinallymph node, or pulmonary involvement.
Relevant diagnostic procedures Malignant pleural mesothelioma (MPM)is usually diagnosed by pleural biopsiesobtained by videothoracoscopy (VATS).Occasionally, pleural fluid cytology willyield a sufficient sample for diagnosisalthough approximately 50% of patientswill have cytologically negative fluid. Inaddition, VATS pleural biopsy providessamples for immunohistochemistry,which is usually required to support adefinitive histological diagnosis.Thoracotomy is not required for diagno-sis and should be avoided because itincreases the risk of tumor implantationinto the chest wall and therefore, mayaffect the technical feasibility of subse-quent definitive resection. In patientswhose pleural space is fused by locallyadvanced tumor, tissue can be obtainedvia a 5cm incision with very limited ribresection and direct pleural biopsy.Computed tomography (CT) is the stan-dard imaging study for the initial stagingof MPM. However, it does not accuratelypredict the presence or absence ofsuperficial chest wall invasion (i.e.involvement of the endothoracic fasciaand intercostal muscles) or full thicknessinvolvement of the diaphragm. Magneticresonance imaging (MRI) may be slightly
more accurate than CT in these areas butnot consistently enough to be used as aroutine imaging modality. If transdi-aphragmatic tumor extension is suspect-ed on CT or MRI, this is best confirmed ordisproved by laparoscopy. Positronemission tomography (PET) detectsmetastatic disease in approximately 10%of patients in whom this is not suspectedclinically or seen by CT and is thereforeused in some insitutions as a routine partof the initial staging evaluation. The max-imum standard uptake value (SUVmax)on PET also appears to have prognosticsignificance. None of these imagingstudies accurately predicts the presenceor absence of mediastinal lymph nodemetastases, an important issue becausethese are known to have a prognosticimpact on survival. Mediastinoscopy canidentify some but not all lymph nodesmetastases because approximately 25%of these occur in areas that are notaccessible by mediastinoscopy (e.g.internal mammary lymph nodes).
Cytology In industrialized countries, about 1% ofmalignant pleural effusions are causedby diffuse malignant mesothelioma.Mesothelioma cells in effusions are virtu-
Fig. 2.06 Malignant mesothelioma. A Gross image of malignant mesothelioma at autopsy showing the typi-cal appearance of the tumor encasing the lung, and, in this example, the pericardium. B Extensive mesothe-lioma growth with compression of residual lung tissue.
BAFig. 2.07. Metastatic pleural adenocarcinoma(pseudomesothelioma). Note infiltration of lung tis-sue which is typically absent in mesothelioma.

ally always of epithelioid type, since cellsof the sarcomatoid type are seldom shedinto the fluid.Mesothelioma cells in effusions may bearranged in sheets, clusters, morulae orpapillae, sometimes with psammomabodies. These cells show a range ofcytological appearances from pleomor-phic to bland, but frequently lack the sig-nificant atypia seen in carcinoma. On theother hand, benign mesothelial cells mayexhibit features usually associated withmalignancy, such as increased cellulari-ty, pleomorphism and mitotic activity.Therefore, differentiation of mesothe-lioma from benign mesothelial hyperpla-sia with reactive atypia may be very diffi-cult or impossible in cytologic speci-mens, since tissue invasion cannot beevaluated. Overall the accuracy of pure-ly cytologic diagnoses, as opposed totissue diagnoses, of malignant mesothe-lioma is fairly low. Immunostains of sec-tions from paraffin-embedded cell blocks
may help to confirm the lineage of thecells.
Macroscopy and localization
In its early stages, mesothelioma pres-ents as multiple small nodules on theparietal and sometimes visceral pleura.With progression the nodules becomeconfluent with resulting fusion of the vis-ceral and parietal pleurae and encase-ment and contraction of the lung. Thetumour may reach several centimetres inthickness and range from firm to gelati-nous in consistency. Loculated collec-tions of fluid may occur within the tumour.Spread frequently occurs along the inter-lobar fissures, into the underlying lung,through the diaphragm, and into thechest wall. Mediastinal involvement withinvasion of the pericardial sac and encir-clement of other midline structures isalso common, as is extension to theopposite pleural cavity. Mesotheliomasmay metastasize to the pulmonary
parenchyma and to hilar and mediastinallymph nodes. This appearance is notpathognomonic for mesothelioma, sincea variety of primary and secondary pleu-ral malignancies may spread in a similarfashion leading to the encasement of thelung.
Tumour spread and staging
Patterns of mesothelioma spreadInvasion of chest wall fat and muscle ischaracteristic, especially along needletracks or surgical biopsy sites.Substantial displacement of the medi-astinum to the contralateral hemithoraxmay occur. Spread through thediaphragm can result in seeding of theperitoneum and ascites, which is fre-quently found at autopsy and rarelycauses uncertainty regarding the pri-mary site.Infiltration into alveolar spaces may pro-duce a histologic pattern that resemblesorganising pneumonia, desquamative
131Mesothelioma
DC
BA
Fig. 2.08 Malignant mesothelioma, epithelioid type. A The tumour consists of a sheet of epithelioid cells with abundant eosinophilic cytoplasm and vesicular nuclearchromatin with prominent nucleoli. From Travis et al. {2024}. B Papillary proliferation of epithelioid cells. From Travis et al. {2024}. C Tubulopapillary pattern. FromTravis et al. {2024}. D Microcystic (adenomatoid pattern). From Travis et al. {2024}.

132 Tumours of the pleura - Mesothelioma
interstitial pneumonia, or bronchiolo-alveolar carcinoma {1476}. Peribronchiallymphovascular spread can occur,sometimes with miliary spread. Lymphnode metastasis rarely is a presentingmanifestation of mesothelioma {1906}. Atautopsy, haematogenous metastasesfrom pleural mesothelioma may be foundin lung, liver, adrenals, bone, brain or kid-ney {815}. It is rare for mesothelioma topresent clinically as metastatic disease{1415}. Staging is performed accordingto the TNM classification proposed bythe International Mesothelioma paneland the UICC {738,2045}.
Histopathology
While the term “desmoplastic mesothe-lioma” is universally accepted for a par-ticular subtype of highly aggressive sar-comatoid mesothelioma, there is noagreement on the nomenclature of other
subtypes, particularly the numerous mor-phologic variants of epithelioid malignantmesothelioma. Recognition of these vari-ants is important for diagnosis, butbecause they have no clear prognosticsignificance, we recommend that mostepithelioid and sarcomatoid mesothe-liomas be diagnosed with no further sub-classifiers beyond those shown at thebeginning of this chapter.
Epithelioid mesothelioma Epithelioid mesothelioma shows epithe-lioid cytomorphology. Most epithelioidmesotheliomas are remarkably bland,but more anaplastic forms are occasion-ally seen. Epithelioid mesotheliomasshow a wide range of morphologic pat-terns. Sometimes one pattern predomi-nates but several different patterns arecommonly seen in the same tumour. Inmost tumours the cells have eosinophilic
cytoplasm with bland relatively opennuclei. Mitoses are infrequent. In thepoorer differentiated forms, the nuclei arecoarser with prominent nucleoli, mitosesare frequent, and some multinucleatetumour giant cells occur; however, thesetumours are uncommon and often diffi-cult to separate from carcinomas.The most frequent patterns encounteredare tubulopapillary, adenomatoid(microglandular) and sheet-like. Lesscommon patterns include small cell,clear cell and deciduoid. The tubulopap-illary form exhibits varying combinationsof tubules, papillae with connective tis-sue cores, clefts and trabeculae. Thecells lining the tubules and papillae areflattened to low cuboidal and relativelybland. Psammoma bodies are occasion-ally observed. The adenomatoid formshows microcystic structures, with lace-like, adenoid cystic or signet ring
Fig. 2.09 Sarcomatoid mesothelioma. A Interlacing fascicles of spindle cells. From Travis et al., {2024}. BSarcomatoid pleural mesothelioma with bizarre anaplastic tumor giant cells. Such an appearance closelymimics that of malignant fibrous histiocytoma.
A
BFig. 2.10 Sarcomatoid mesothelioma with A osteo -sarcomatous differentiation. B Inflammatory lym-phohistiocytic pattern. From Travis et al. {2024}.
A
B

133Sarcomatoid mesothelioma
appearances, but does not stain for neu-tral mucin. Sheets and nests of cells arefrequently seen in association with otherpatterns. Uncommonly, solid, monoto-nous, relatively non-cohesive sheets ofpolygonal cells occur, simulating largecell carcinoma or lymphoma. Tumourswith anaplastic and/or tumour giant cellsmay be designated pleomorphic.Mesothelioma can mimic non-Hodgkinlymphoma (so-called lymphohistiocytoidmesothelioma, regarded by some as aform of sarcomatoid mesothelioma) andsmall cell carcinoma, but usually lackskaryorrhexis and haematoxyphylic stain-ing of blood vessels of the latter tumour.Rarely large cells with clear cytoplasmare prominent, mimicking metastaticrenal cell carcinoma. Small foci of cellswith plump eosinophilic cytoplasmresembling deciduoid cells of pregnancyare frequently present in epithelioidmesothelioma and uncommonly predom-inate (so-called deciduoid mesothe-lioma). The fibrous stroma of epitheloidmesotheliomas can vary from relativelyscanty to copious and can show varyingdegrees of cellularity from hyalinisedacellular to highly cellular, merging withsarcomatoid. These tumours may be dif-ficult to distinguish from a biphasicmesothelioma. Myxoid change may beconspicuous, with nests of epithelioidcells “floating” in the matrix; the matrix insuch tumours is hyaluronate, and showshyaluronidase-sensitive staining withAlcian blue.Immunohistochemistry is an importantadjunct to the diagnosis of malignant
mesothelioma, particularly in distinguish-ing it from pulmonary adenocarcinoma.A combination of two or more positivemesothelial with two or more negativeepithelial (carcinoma) markers is mostuseful, their choice to a large extentdepending upon the experience of thelaboratory. The most useful mesothelialmarkers appear to be cytokeratin 5/6,calretinin and Wilms tumour gene-1(WT1). N-cadherin is promising butneeds more study. The most usefulepithelial markers appear to be CEA(monoclonal), CD15, Ber EP4, B72.3,MOC 31 and thyroid transcription factor1 (TTF-1). The immunohistochemistrypanel will require amendment where thedifferential diagnosis includes tumoursother than pulmonary adenocarcinomas.A broad-spectrum keratin is useful toexclude rare cases of large cell lym-phoma, metastatic malignant melanomaand epithelioid haemangioendothelioma.The use of immunohistochemical mark-ers for the diagnosis of malignant versusreactive mesothelial lesions remains con-troversial.
Sarcomatoid mesothelioma The sarcomatoid variant of pleuralmesothelioma consists of spindle cellsarranged in fascicles or having a hap-hazard distribution. The pattern mostoften resembles fibrosarcoma, butmarked anaplasia and bizarre multinu-cleate tumour cells may result in a pic-ture closely mimicking that of malignantfibrous histiocytoma. In a small percent-age of cases, areas resembling
osteosarcoma, chondrosarcoma or othersarcomas may be present.Sarcomatoid mesotheliomas typicallystain positively for cytokeratins when abroadspectrum antibody cocktail isused, although an absence of stainingmay be seen in occasional cases. Areaswith chondrosarcomatous or osteosarco-matous differentiation often stain nega-tively for cytokeratins {2220}.Sarcomatoid mesotheliomas may stainpositively for vimentin, actin, desmin, orS-100. Some cases may also show stain-ing for calretinin {87}.The differentiation from sarcomatoid(pleomorphic) carcinoma of the lungsecondarily invading the pleura ormetastatic sarcomatoid renal cell carci-noma can be exceedingly difficult.Immunostains do not reliably differentiatebetween these possibilities {271}. Insuch cases, gross and clinical featuresmay be helpful.
Desmoplastic mesothelioma Desmoplastic mesothelioma is charac-terized by dense collagenized tissueseparated by atypical cells arranged in astoriform or “patternless” pattern, pres-ent in at least 50% of the tumour. Thesetumours can readily be confused withbenign organizing pleuritis, especially onsmall biopsy specimens. Certain diag-nostic criteria strongly suggest malignan-cy. These include frankly sarcomatoidareas, foci of bland collagen necrosis,invasion of adipose tissue, skeletal mus-cle, or lung, and distant metastases{1229}. Bone metastases from desmo-
Fig. 2.12 Malignant mesothelioma, biphasic type. A combination of sarcomatoid and epithelioid patterns.From Travis et al. {2024}.
Fig. 2.11 Malignant mesothelioma, desmoplastictype. Haphazard arrangement of slit-like spaces.From Travis et al. {2024}.

134 Tumours of the pleura - Mesothelioma
plastic mesothelioma {1219} are poten-tially liable to histological misdiagnosisas a primary benign fibrous tumour ofbone.Cytokeratin staining may be of greatestutility in highlighting invasion by keratinpositive spindle cells into adipose tissue,skeletal muscle, or lung. The mere pres-ence of keratin positive staining in thethickened pleura itself is of no particularbenefit, since reactive processes oftenhave keratin-positive spindle cells.
Biphasic mesothelioma Mesotheliomas contain both epithelioidand sarcomatoid patterns in about 30%of cases. Any combination of the pat-terns noted above may be present. Eachcomponent should represent at least10% of the tumour to warrant the termbiphasic. The percentage of cases clas-sified as biphasic will increase with morethorough tumour sampling.
Grading
Malignant mesotheliomas are not ordi-narily graded. Epithelioid forms are oftendeceptively monotonous and can beremarkably bland in appearance.Mitoses are scarce in most epithelioidmesotheliomas. Sarcomatoid forms maybe bland or fairly anaplastic. However,beyond the distinction between epithe-lioid and sarcomatoid forms, thesehistopathologic features do not correlatewell with prognosis.
Differential diagnosisThe differential diagnosis of diffusemalignant mesothelioma is shown inTable 2.01. The most important differen-tial is metastatic or locally invasive (fromlung or chest wall) tumour that covers thepleural surface. However, various local-ized tumours also exist in the pleura andsome mimic mesothelioma microscopi-cally. For this reason, knowledge of thegross distribution of tumour, whetherobtained from radiographic studies, theoperator’s description of the findings atthoracotomy or thoracoscopy, or from aresected or autopsy specimen, is crucialto making a proper diagnosis.
Postulated cell of origin
The exact cell of origin of malignantmesothelioma is unclear. Although thecommon belief is that these tumoursarise from surface mesothelial cells,some experimental data suggest thatthey may arise from submesothelial cellsthat differentiate in a variety of directions.
Precursor lesions
It is likely that malignant mesotheliomadevelops through an in-situ stage. Thereare at present no reliable histologic crite-ria for separating lesions that might be insitu mesothelioma from atypical benignreactions. The use of the term ‘atypicalmesothelial hyperplasia’ is recommend-ed for purely surface mesothelial prolifer-ations that might or might not be malig-nant.
Somatic genetics
Cytogenetics and CGH Most studied cases appear to be epithe-lioid mesotheliomas, although somereports do not distinguish cell type.Karyotypic and comparative genomichybridisation (CGH) analyses havedemonstrated that most mesotheliomashave multiple chromosomal alterations.
Although no single change is diagnostic,several recurrent sites of chromosomalloss have been identified. Deletions of1p21-22, 3p21, 4q, 6q, 9p21, 13q13-14,and 14q have been repeatedly observed{103,177,178,1075,1942}. Monosomy 22is the most frequent numerical change.Losses of 4p and proximal 15q havebeen reported in some CGH studies, andminimally deleted regions at 4p15 {1815}and 15q15 {457} have been document-ed. Recurrent losses of 17p12-pter,including the p53 locus, have beenobserved in some investigations {103,1075}. Loss of heterozygosity (LOH)analysis has confirmed that each of theabove sites is frequently deleted inmesothelioma and, for most of the affect-ed chromosomes, has defined a singleminimally deleted region (reviewed in{1997}). Allelic loss from chromosome 4has been reported to occur at multiplelocations, with the most frequent sitebeing 4q33-34 {1815}. LOH in 6q occursat several non-overlapping regionsbetween 6q14 and 6q25 {142}. Similarly,multiple non-overlapping regions of allel-ic loss have been reported for chromo-some 14, with 14q11.2-12 and 14q23-24each being observed in two independentstudies {179,458}. Chromosomal gainsare less common than losses in mesothe-lioma, although recurrent gains of 1q, 5p,7p, 8q22-24, and 15q22-25 have beendescribed. These abnormalities reflect
Fig. 2.13 A Well differentiated papillary mesothe-lioma. B Solitary papillary WDPM.
A
B
Table 2.01Differential diagnosis of diffuse malignantmesothelioma.
Metastases to the pleura*
- Carcinoma- Sarcoma- Lymphoma- Malignant Melanoma
Primary diffuse pleural sarcoma
- Angiosarcoma- Epithelioid haemangioendothelioma- Synovial sarcoma- Other sarcoma
Thymic tumours, primary or metastatic
Desmoplastic small round cell tumour and Ewing sarcoma family
Localized primary pleural tumours
- Localized malignant mesothelioma- Solitary fibrous tumour (benign and
malignant forms)- Sarcomas- Well-differentiated papillary mesothelioma- Adenomatoid tumour- Calcifying fibrous pseudotumour- Nodular pleural plaque
________*Metastasis to the pleura or reaching the pleura bydirect spread from the lung or chest wall.

similarities and differences with carcino-ma of the lung.
Molecular genetic alterations Inactivation of the CDKN2A/ARF locus at9p21 is a frequent finding in mesothe-lioma {345,2178}. CDKN2A/ARFencodes the tumour suppressor genesp16INK4a and p14ARF. Homozygous dele-tions of this locus are common, especial-ly in cell lines, and inactivation by pro-moter methylation is also a recurrent find-ing {1071}. Immunohistochemical analy-sis suggests that loss of p16INK4a expres-sion is a frequent finding {839}. Deletionsof p14ARF are frequently observed. Thismechanism of cell cycle control disrup-tion is also common in non-small cell car-cinomas. Unlike lung cancers, TP53mutations are relatively uncommon {417,1020,1302}, possibly because SV40 Tagis expressed in some mesotheliomasand retains its ability to bind to and inac-tivate p53 {284}. Also in contrast to lungcancer, mutations of the NF2 tumour sup-pressor gene, located at chromosome22q12, have been reported frequently inmesothelioma {165,1778}. Biallelic inacti-vation of NF2 occurs by combined pointmutation and LOH {346}. The previouslymentioned monosomy of chromosome22 may reflect these findings. Anothertumour suppressor gene, GPC3, is fre-quently down regulated due to aberrantpromoter methylation {1413}.Recurrent activation of oncogenes bypoint mutation or amplification has notbeen documented in mesothelioma{1020,1302}. However, asbestos inducesmRNA expression of the c-fos and c-junproto-oncogenes in mesothelial cells{810}, and asbestos-induced mesothelialcell transformation is linked to increasesin AP-1 DNA binding complexes and theAP-1 component, Fra-1 {810,1639}.Other experimental evidence indicatesthat when SV40 infects mesothelial cells,it causes activation of the Met and notch-1 proto-oncogene products {185,267}. Incontrast to lung cancers, relatively fewgenes are methylated in mesotheliomas.The gene most frequently methylated isthe RASSF1A tumour suppressor gene{2018}.
Genetic susceptibility (Familial cancer
syndromes)
Multiple cases of pleural mesotheliomahave been reported from families withdocumented exposure to asbestos or
other carcinogenic mineral fibres, suchas erionite {81,1175,1697}. While investi-gation of members of one family withfamilial mesothelioma failed to identifygermline mutations, the molecularchanges in the tumours were similar tothose found in sporadic mesothelioma{80}. One study {960} described an asso-ciation at population level with HLA anti-gens B41, B58 and DR16. Specificgenetic indicators of susceptibility tomesothelioma development have not yetbeen identified {1740}: currently avail-able observations may reflect differentiallevels and duration of exposure to car-cinogenic fibres among affected andnon-affected members of a family, ran-dom sequences of events, or genuinevariations in individual susceptibility.
Prognosis and predictive factors
Clinical criteria Chest pain, dyspnoea and weight loss aspresenting symptoms may be associatedwith a poorer prognosis {822,1708}.There was a trend towards pain beingrelated to sarcomatoid differentiation{1711}. Good prognostic indicators are ayoung age at presentation, epithelioidsubtype, stage of disease {1711} goodperformance status, lack of chest painand female sex below the age of 50years {1861}.
Histopathological criteria Most series show that patients whosetumours have a purely epithelioid histol-ogy have the longest survival, those witha purely sarcomatoid histology the worst,and those with mixed patterns an inter-mediate survival. The differences inmedian survivals as a function of histo-logic subtype are only however, a matterof a few months. In the future, therapymay be influenced by histologic subtype,since no patient with a sarcomatoid pat-tern treated with trimodality therapy sur-vived for 5 years {2235}.
Genetic predictive factors While there are many similarities in thefrequencies of various genomic imbal-ances between epithelioid and sarcoma-toid mesotheliomas, several chromoso-mal locations (3p, 7q, 15q, 17p) showsignificant variations {1075}. For exam-ple, deletion at 3p21 is common inepithelioid tumours but rare in sarcoma-toid and biphasic tumours. To date, cyto-genetic prognostic factors have not been
reported. Loss of 7q, which is associatedwith poor prognosis in other tumourtypes, was observed in ~20% of sarco-matoid tumours but was not observed inepithelioid cases {1075}. Moreover, theincidence of amplicons was 4-5-foldhigher in sarcomatoid than in epithelioidtumours. Gene expression profiles in asmall number of cases has been report-ed to predict outcome independent ofhistologic subtype {714}
Well differentiated papillarymesothelioma
Definition
Well differentiated papillary mesothe-lioma (WDPM) of the pleura represents adistinct tumour with a papillary architec-ture, bland cytologic features and a ten-dency toward superficial spread withoutinvasion.
ICD-O code 9052/1
Epidemiology
WDPM is a rare pleural tumour, withfewer than 50 cases reported in the worldliterature {261,864,2204}. These tumoursare considerably more common in theperitoneum, where they predominantlyoccur in women {444}. This sex predom-inance is not obvious in the pleuralcases. The reported age range in pleurallesions is 31-79 with a median of 63 forboth sexes {261,864,2204}.
Etiology
Asbestos exposure has been reported insome cases {261,656}, but this has notbeen established in epidemiologic stud-ies.
Localization
These lesions may be localized or multi-focal and widespread.
135Well differentiated papillary mesothelioma
Fig. 2.14 Localized malignant pleural mesothelioma.

Clinical features
Patients present with dyspnoea andrecurrent pleural effusion or as an inci-dental finding. They rarely present withpneumothorax or chest pain. Unilateralfree-flowing pleural effusions may beseen, with or without nodular pleuralthickening or fibrous hyaline plaques.
Macroscopy
These tumours may appear as solitary ormultiple localized masses. The visceralor parietal pleura may be involved andmay have a velvety appearance.
Histopathology
WDPM is characterized by papillae, con-sisting of predominantly stout myxoidfibrovascular cores covered by a singlelayer of bland flattened to cuboidalmesothelial cells, exuding from the pleu-ral surface. Basal vacuoles may be pres-ent in the lining cells. Nucleoli are incon-spicuous and mitotic figures absent. Thesurface cells stain positively for mesothe-lial markers.In the strictest definition, invasion is notpresent in WDPM. However, some casesof otherwise typical WDPM may showlimited invasion. Nevertheless, diffusemalignant mesotheliomas may haveareas with a WDPM-like pattern andshould not be designated as WDPM.Consequently, great caution should beemployed in diagnosing WDPM in smallbiopsies.
Prognosis and predictive factors
These tumours are often indolent withprolonged survival. The development ofinvasion may herald a more aggressiveclinical course. The occurrence of rapid-ly progressive disease suggests that theunderlying disease is a diffuse malignantmesothelioma, a problem that may reflectsampling inadequacy.
Localized malignant mesothelioma
Definition
A rare tumour that grossly appears as adistinctly localized nodular lesion without
gross or microscopic evidence of diffusepleural spread, but with the microscopic,histochemical, immunohistochemicaland ultrastructural features of diffusemalignant mesothelioma.
ICD-O code: code according to the his-tologic subtype of mesothelioma.
Clinical features
Most reported cases have been inciden-tal findings on chest x-ray or CT scan.Occasionally they present with pleuraleffusions.
Macroscopy
Localized malignant mesotheliomas arecircumscribed nodular tumours thatmeasure up to 10cm in diameter. Theymay be attached to the visceral or pari-etal pleura, are pedunculated or sessile,and can extend into the subjacent lung.
Histopathology
These tumours are histologically identicalto diffuse malignant mesotheliomas andmay be epithelioid, sarcomatoid, orbiphasic (mixed). They show a pattern ofimmunohistochemical staining identicalto diffuse malignant mesothelioma {425}.
Prognosis
Some localized malignant mesothe-liomas are cured by surgical excision{425}. Recurrent tumours may metasta-size like sarcomas and usually do notspread along the pleural surface.
Adenomatoid tumour
Definition
A rare solitary small pleural tumour withhistological features identical to thoseseen in adenomatoid tumours in otherlocations.
ICD-O code 9054/0
Clinical features
The few reported cases have been inci-dental findings at gross examination ofthe pleura.
Macroscopy
The tumours appear as solitary distinctlynodular lesions.
Histopathology
The tumour cells are flattened tocuboidal and usually eosinophilic; theyform glands and tubules, often withmarked cytoplasmic vacuolisation {958}.They show a pattern of staining identicalto that seen in diffuse malignantmesothelioma. Adenomatoid tumourmust be separated from some diffuseepithelial mesotheliomas that may, inindividual microscopic fields, show asimilar pattern.
Prognosis and predictive factors
These neoplasms are identical to adeno-matoid tumours in other locations andare benign.
136 Tumours of the pleura - Mesothelioma
Fig. 2.15 Adenomatoid tumour. Irregularly shapedgland-like spaces are present within a fibrous stro-ma. From Travis et al. {2024}.

137Primary effusion lymphomas
Primary effusion lymphoma
Definition
A neoplasm of large B-cells presentingas serous effusions, usually withoutdetectable tumour masses, universallyassociated with human herpes virus 8(HHV8)/Kaposi sarcoma herpes virus(KSHV), and usually occurring in the set-ting of immunodeficiency.
ICD-O code 9678/3
Synonym
Body cavity-based lymphoma.
Epidemiology
The majority of cases arise in the settingof human immunodeficiency virus (HIV)infection {60,311,1421}. Most patientsare young to middle aged homosexualmales. This neoplasm is rare even in thesetting of HIV infection. Cases have beenreported in HIV negative allograft recipi-ents, particularly after cardiac transplan-tation {512,561,937}. The disease hasalso been reported in the absence ofimmunodeficiency especially in elderlyindividuals {282,380,821,1029,1422,1995}.
Localization
The most common sites of involvementare the pleural, pericardial and peritonealcavities. Typically only one body cavity isinvolved. One case has been reportedarising in the artificial cavity of a breastimplant {1721}. The most common extra-cavitary site of presentation is the gas-trointestinal tract; the GI tract, mediasti-nal and retroperitoneal soft tissue andother extranodal sites may also be sec-ondarily involved {130,209,415,479,877}.
Clinical features
Patients typically present with effusionsin the absence of lymphadenopathy ororganomegaly. Some patients, both HIV+and HIV-, have pre-existent Kaposi sar-coma {60,937,1721}. Rare cases areassociated with multicentric Castlemandisease {380,1995}.
Etiology
The consistent presence of HHV8 in theneoplastic cells in all cases suggests apathogenetic role for this virus in thedevelopment of the tumour {311}. Thereis consistent expression of viral IL-6 (vIL-6) in primary effusion lymphomas, sug-gesting that this and other cytokines mayplay a role in the pathogenesis of thetumours {62,514}. In one study of anEBV- HIV- case, HHV8 related transcriptsincluding viral G-coupled protein recep-tor, viral Bcl2, viral cyclin D1, viral IL6and viral MIP I and II were detected in tis-sue from a primary effusion lymphomaand an HHV8+ gastric lymphoma butonly vIL6 was detected in a multicentricCastleman disease lesion from the samepatient {1995}. Oncogenic genes encod-ing viral cyclin D, bcl2, G-protein cou-pled receptor IL-6, Flice inhibitory proteinand others were also shown to beexpressed in another EBV- PEL {379}. NFkappa-B is constitutively activated onHHV8+ PEL cell lines, and its inactivationleads to apoptosis, suggesting that, sim-ilarly to EBV, HHV8 may promote cell sur-vival through this pathway {989}.Although multicentric Castleman diseaseand primary effusion lymphoma maycoexist in some patients, a clonal rela-tionship between them has not beenestablished {82}.Most but not all cases are coinfected withEBV, but do not express the transformingproteins EBNA-2 and LMP1 and 2. Eachcase contains a single strain of clonalEBV, but there is considerable hetero-geneity among cases; thus no specificrole for EBV in the pathogenesis hasbeen found {561,868}.
Histopathology
With Wright or May Grunwald Giemsastaining performed on cytocentrifugepreparations, the cells exhibit a range ofappearances, from large immunoblasticor plasmablastic cells to cells with moreanaplastic morphology. Nuclei are large,round or irregular in shape, with promi-nent nucleoli. The cytoplasm is typicallyvery abundant and is deeply basophilic,
and vacuoles may be present in occa-sional cells. A paranuclear hole suggest-ing plasmacytoid differentiation may beseen. Binucleated or multinucleated cellsmay be present that can resemble Reed-Sternberg cells.The cells often appear more uniform inhistological sections than in cytospinpreparations. They are large, with somepleomorphism, ranging from large cellswith round or ovoid nuclei to very largecells with irregular nuclei and abundantcytoplasm; multinucleation can occur{60,311,1421}. Pleural biopsies showtumour cells adherent to the pleural sur-face, often embedded in fibrin and occa-sionally invading the pleura.This disease should be distinguishedfrom pyothorax-associated diffuse large
P.M. BanksN.L. HarrisR.A. WarnkePh. Gaulard
Lymphomas
Fig. 2.16 Diffuse lymphoma of the pleura in a patientwith AIDS.
Fig. 2.17 Primary effusion lyphoma of pleura.Discohesive atypical lymphoid tumour cells with afew pleomorphic cells.

138 Tumours of the pleura - Lymphomas
B-cell lymphoma, which usually presentswith a pleural mass lesion. The cells ofpyothorax-associated diffuse large B-celllymphoma have the appearance ofimmunoblasts, and are EBV positive andHHV8 negative {1972}.
ImmunoprofileThe neoplastic cells typically expressleukocyte common antigen (CD45) butare usually negative for the pan-B-cellmarkers CD19, CD20 and CD79a {60,1421}. Surface and cytoplasmic expres-sion of immunoglobulin is likewise oftenabsent. The B-cell specific transcription-al activator programme appears to bedisrupted in primary effusion lymphoma,with decreased or absent expression ofPU.1, Oct 2 and BOB.1, possiblyaccounting for the failure to produceimmunoglobulin {72}. CD30 is typicallypositive. The cells lack germinal centre-associated markers CD10 and Bcl-6 andexpress MUM1/IRF4, associated withlate germinal centre and post-germinalcentre B cells {281}. Plasma cell-relatedmarkers such as CD38, and CD138 aretypically expressed {650}. Aberrant cyto-plasmic CD3 expression has beenreported {130}, as well as CD7 and CD56{1608}. Because of the markedly aber-rant phenotype, it may be difficult toassign a lineage with immunophenotyp-ing. Rare cases of HHV8+ primary effu-sion lymphoma that express only T-cell-associated antigens have been reported{1146,1720}.The nuclei of the neoplastic cells arepositive by immunohistochemistry for theHHV8/KSHV-associated latent protein{522,1555}, and this staining can be use-ful in confirming the diagnosis. EBV-pos-itive cases have a Type I latency pheno-type, expressing only EBNA-1; EBNA-2and LMP-1 and 2 are not expressed atlevels detectable by immunohistochem-istry {278}.Cell lines from primary effusion lym-phomas have been shown to expressboth the Met tyrosine kinase receptorand its ligand, hepatocyte growth factor,similarly to myeloma cell lines {278}.
Histogenesis
Post-germinal center B-cell with differen-tiation towards plasma cells.
Somatic genetics
Immunoglobulin genes are rearrangedand are mutated consistent with a post-
germinal center B cell {1258}. The BCL6gene is somatically mutated in mostcases, consistent with a post-germinalcenter B cell {649}. Some cases alsohave rearrangement of T-cell receptorgenes {865}. Most cases have multiplebut non-recurring cytogenetic abnormal-ities {512}. Comparative genomic analy-sis has revealed gains in sequence ofchromosomes 12 and X {1401}. HHV8viral genomes are present in all cases.EBV is detected in most but not all casesby EBER in-situ hybridisation {60,209,561,1421}. Cases in HIV- non-immuno-suppressed patients appear to be moreoften EBV- {512}. Two cases with only T-cell antigen expression and rearrange-ment of the T-cell receptor gene havebeen reported {1146,1720}. The relation-ship of these cases to the more commonB-cell neoplasm is unclear.Gene expression analysis by DNAmicroarray technology has shown a dis-tinctive profile for the cells of primaryeffusion lymphoma, including genes indi-cating differentiation towards plasmacells and a set of genes unique to thistype of lymphoma {1027}.
Prognosis and predictive factors
The clinical behaviour is extremelyaggressive, with most reported patientsdead in less than one year. Recently afew cases have been reported torespond to antiviral therapy or combina-tion chemotherapy or both with pro-longed survival {209,1029}.
Pyothorax-associatedlymphoma
Definition
Pyothorax-associated lymphoma (PAL) isa neoplasm of large B cells, typically withimmunoblastic morphology, usually pre-senting as a pleural mass. It is stronglyassociated with Epstein-Barr virus (EBV).This rare type of primary pleural B-celllymphoma occurs in patients with a clini-cal history of longstanding pyothoraxresulting from pulmonary tuberculosis ortuberculous pleuritis.
Synonyms and historical annotation
Since its first recognition in 1987, it hasbeen established that PAL belongs to thediffuse large B-cell lymphoma (DLBCL)category {915}. Although the recentWHO classification of Tumours ofHaematopoietic and Lymphoid Tissues
describes different clinical subtypesamong DLBCL (i.e. mediastinal, intravas-cular, and primary effusion lymphoma){919}, PAL has not been included as adistinct clinico-pathologic entity in thisrecent classification, probably in view ofits rarity in most western countries. Weinclude it in this classification of pleuraltumours since it specifically occurs inthis location.
Epidemiology
Pyothorax-associated lymphoma (PAL)occurs in adults, usually in the 5-8thdecades with a median age around 65-70 years. It seems to affect males moreoften than females {1437,1586}. PALdevelops in patients without overt sys-temic immunosuppression, but consis-tently after a history of pyothorax result-ing from artificial pneumothorax for treat-ment of pulmonary tuberculosis or, morerarely, tuberculous pleuritis. The intervalbetween the onset of pleuritis and initialsymptoms of lymphoma ranges from20—67 -years, with a 37-48 years medi-an interval {1437,1586}. Most PALs havebeen reported in Japan, apart from sev-eral cases in France and Italy {63,79,1250,1339,1437,1503,1586}.
Etiology
Strong association with Epstein-Barrvirus (EBV) has been demonstrated {631,1503,1743}. Depending on the series,EBV DNA or EBV-encoded RNA (EBERs)are demonstrated in lymphoma cells of70-100% of cases. They also expresslatent infection genes, including EBVnuclear antigen 2 (EBNA-2) and latentmembrane protein 1 (LMP-l), resulting ina latency III pattern of EBV expression,similar to that observed in lymphoprolif-erative disorders occurring in immuno-compromised patients. Although thepathogenesis is not clearly understood,previous findings {954} suggest a role forchronic inflammation at the local site inthe proliferation of EBV-transformed B-cells by enabling them to escape thehost immune-surveillance system and/orby providing local production ofcytokines such as IL-6 and IL-10 {955,956}.There is no association with HIV, HTLV, orHHV8 infections.
Sites of involvement
In contrast to primary effusion lymphoma(PEL), PAL typically presents as a tumour

139Pyothorax-associated lymphomas
mass that involves the pleural cavity andshows direct invasion to adjacent struc-tures such as the chest wall, lung anddiaphragm in most cases, whereas pleu-ral effusion is rarely observed.Extrathoracic/metastatic dissemination(bone marrow, liver, abdominal lymphnodes, etc) is only rarely observed atpresentation {1437,1586}.
Clinical features
Patients typically present with symptomsrelated to a pleural tumour mass, withpains in the chest and/or back, or respi-ratory symptoms such as productivecough, often with haemoptysis or dysp-noea. Other common symptoms arefever and weight loss. A tumour swellingin the chest wall is present in 40% of thepatients. Chest radiography and com-puted tomography reveals a tumourmass in most patients, which is located inthe pleura (80%), pleura and lung (10%)and lung near pleura (7%) with a tenden-cy to invade adjacent structures, mainlythe chest wall, and is larger than 10 cmin about half of the patients {1437}.These features often suggest a diagnosisof lung cancer or pleural mesothelioma.About 70% of the patients have a AnnArbor stage I-II localized disease. Theserum lactate dehydrogenase (LDH)level is elevated in most patients {1437,1586}. Due to the presence of severalclinical prognostic factors (low perform-ance status, age, elevated LDH level),the majority of patients belong to theintermediate group of the InternationalPrognostic Index (IPI) score {2}.
Morphology
In tissue sections, there is a diffusedestructive proliferation of large cells.Despite a range of appearances, mostcases show a predominant population ofimmunoblasts with round nuclei showinglarge single or multiple nucleoli. Theymay have features of plasmacytoid dif-ferentiation. Some cases are consistentwith a centroblastic lymphoma and a fewhave been reported to have anaplasticfeatures. PAL is characterized by a highproliferative rate with numerous mitoticfigures and prominent apoptosis. Areasof necrosis and angiocentric or angioin-vasive features have been reported, thusresembling features of lymphoprolifera-tive disorders occurring in immunocom-promised patients. The disease shouldbe distinguished from primary effusion
lymphoma (PEL), which commonly pres-ents as serous effusions withoutdetectable tumour masses in patientswith a setting of immunodeficiency, ischaracterized by a proliferation of largeB-cells which are CD30, CD38 andCD138 positive but lack CD20 andCD79a B cell markers, and is constantlyassociated with HHV8 infection.
ImmunophenotypeTypically, lymphoma cells are positive forCD79a and CD20 B-cell antigens. Caseswith plasmacytoid differentiation, howev-er, have been reported to lack CD20 oreven CD79a. They may show weak het-erogeneous expression of plasma cellrelated markers such as CD138.Cytoplasmic expression of immunoglob-ulins can be detected. CD30 activationmarker can be expressed. Surprisingly, anumber of cases may express at leastone T-cell marker (CD2, CD3, CD4,and/or CD7), most frequently with a dualB/T phenotype {1380,1433,1437,1586,2010}. A similar observation has beenmade in PAL cell lines {36,433}. Thus, insome PALs, because of a markedly aber-rant phenotype – i.e., null-cell phenotypeor expression of some T-cell markers – itis difficult to assign a lineage.Based on CD20 negativity and expres-sion of T-cell antigens, rare cases of
pyothorax-associated T-cell lymphomahave even been reported. However, oneof these cases, investigated for genotyp-ic studies, was demonstrated to containa B-cell clone without clonal rearrange-ment of the T-cell receptor genes, thusindicating that such cases correspond toB-cell lymphomas with aberrant T-cellphenotype {2010}. Although the reasonfor such an aberrant phenotype in PAL isunknown, it is noteworthy that it has alsobeen described in B-cell lines infectedby EBV as well as in some EBV trans-formed B-cell lymphomas arising inimmunosuppressed patients, and it hasbeen suggested that EBV might promotethis dual phenotype.Recently, it has been shown that lym-phoma cells in PAL express a uniformCD10-, BCL-6-, MUM1/IRF-4+ phenotype,in agreement with derivation from a lategerminal centre/post-germinal centre B-cell {1586}.Lymphoma cells are positive byimmunohistochemistry for EBV in mostcases, showing an EBNA-2+/LMP-1-/+
phenotype consistent with a type IIIlatency. EBNA-2 is usually highlyexpressed in the nuclei of most tumourcells, whereas LMP-1 is found in a fewneoplastic cells {1339,1586}. Demon-stration of EBV is very useful in estab-lishing a diagnosis.
DCFig. 2.18 Pyothorax associated lymphoma. A At a higher magnification, the infiltrate consists of large neo-plastic cells, with immunoblasts and many cells showing a plasmacytoid differentiation with eccentricnuclei and abundant cytoplasm. B The neoplastic cells are strongly positive for CD79a. C However, in thiscase, they also show aberrant strong expression for CD2. D Immunostaining with the EBNA-2 antibodyshows that virtually all neoplasic cells disclosed strong nuclear staining for EBNA-2.
BA

140 Tumours of the pleura - Lymphomas
Genetic features
Immunoglobulin genes are rearrangedand are mutated {1333}. No characteris-tic chromosomal alterations have beenidentified. A high frequency of p53 muta-tions and of c-myc amplifications havebeen described {867,2191}. As seenabove, EBV genomes are detected in vir-tually all cases by in situ hybridizationwith EBERs probes and lymphoma cellsalso express EBNA-2 and LMP-l viral pro-teins. By Southern blot, they carry mono-clonal EBV genome {433,631} and chro-
mosomal integration of EBV has beenrecently demonstrated in one cell line{433}. A small percentage of PAL arereported to be EBV-negative. However,EBV genomes have been found by usingsensitive PCR techniques in at least afew cases that were scored as EBV-neg-ative on the results of in situ hybridizationand immunohistochemical studies {1503,1586}. In contrast to PEL, HHV8sequences and expression of HHV8/ORF73 antigens are absent in PAL{1496,1586}.
Postulated normal counterpart
EBV-transformed late germinal centre/post-germinal centre B-cell.
Prognostic features
Most series report a very poor prognosiswith a median survival of less than oneyear. However, in a recent series, morethan half of the patients showed aresponsiveness to chemotherapy and/orradiotherapy and the patients whoachieved complete remission after thera-py had a 50% 5-year survival rate {1437}.

141Epithelioid haemangioendothelioma / angiosarcoma
W.D. TravisA. ChurgM.C. AubryN.G. Ordonez
Mesenchymal tumours H. TazelaarR. PugatchT. Manabe
M. Miettinen
Epithelioid haemangio-endothelioma / angiosarcoma
Definition
Pleural epithelioid haemangioendothe-lioma (PEH) is a low to intermediategrade vascular tumour composed ofshort cords and nests of epithelioidendothelial cells embedded in a myxo-hyaline matrix. The tumours are distinc-tive for their epithelioid character, sharplydefined cytoplasmic vacuoles, intraalve-olar and intravascular growth and centralhyaline necrosis. High-grade epithelioidvascular tumours are called epithelioidangiosarcomas.
ICD-O code
Epithelioid haemangioendothelioma9133/1
Angiosarcoma 9120/3
Epidemiology
Most patients with PEH are Caucasian,65-85% are men and the mean age is 52years with a range of 34-85 years {424,435,533,1184,2120}.
Clinical features
Patients usually present with diffuse pleu-ral thickening, pleural effusion, and/orpleuritic chest pain. Some patients haveboth pulmonary as well as pleuralinvolvement. {424,1184,510,536,1184,1227,1453}.
Imaging
CT scans or chest x-rays characteristi-cally demonstrate pleural thickening andpleural effusions may represent the pri-mary manifestation {424,1184}, sometimesaccompanied by pulmonary nodules.
Macroscopy and localization
Epithelioid haemangioendotheliomasmay involve the pleura diffusely andmimic the gross appearance of diffusemalignant mesothelioma {424,1184,2222,2239}.
Histopathology
The tumours often show a biphasic pat-tern with nests of epithelioid cells within a
spindle cell stroma. The stroma is usualIyreactive, but may be neoplastic. It oftenshows a myxoid or chondroid appear-ance. A tubulopapillary pattern may beseen in about one third of cases. Theepithelioid tumour cells show large roundto oval nuclei with a vesicular chromatinpattern. Epithelioid angiosarcomas arehigh grade and typically show largenucleoli more frequent mitoses than thelow to intermediate grade epithelioidhaemangioendotheliomas. Intracytoplas-mic vacuoles are common.
Immunohistochemistry Most tumours stain with one or moreendothelial markers including CD31,CD34, Fli1, and factor VIII (von Wille -brand factor) {599,828,1184}. Cyto ke -ratin is expressed in up to 50% of cases,causing some difficulty in differentiating itfrom carcinoma {424,1184, 1308}.However, the staining is usually weak tomoderate and weaker than vimentinstaining {424,1184}.
Electron microscopyElectron microscopy reveals abundantintermediate filaments, micropinocytosisand Weibel- Palade bodies. An interrupt-ed basal lamina surrounding the tumourcells is present and cytoplasmic luminamay be seen {1184}.
Differential diagnosisThe differential diagnosis includes chron-ic fibrous pleuritis, malignant mesothe-lioma, metastatic carcinoma andmelanoma. Key to recognition of thistumour in the pleura is awareness of itsmorphologic and immunohistochemicalcharacteristics, particularly that it mayshow a biphasic and papillary appear-ance. If keratin staining in an epithelioidtumour in the pleura is weak or negative,an epithelioid vascular tumour should beconsidered and immunohistochemistryfor vascular markers should be per-formed.
Histogenesis
Epithelioid haemangioendotheliomas arederived from endothelial cells.
Prognostic factors
Epithelioid vascular tumours that presentin the pleura have an aggressive clinicalcourse. There is no known effective ther-apy for these patients.
Synovial sarcoma (SS)
Definition
Synovial sarcoma (SS) is a biphasic mes-enchymal neoplasm with epithelial andspindle-cell components, or a monopha-sic tumour which consists purely of aspindle cell component. Both biphasicand monophasic types can occur in thepleura and they can be easily confusedwith malignant mesothelioma or pul-monary sarcomatoid carcinoma.
ICD-O codes
Synovial sarcoma 9040/3Synovial sarcoma, spindle cell
9041/3Synovial sarcoma, biphasic
9043/3
Synonyms
Synovial cell sarcoma, malignant syn-ovioma, synovioblastic sarcoma
Etiology
There are no known etiological factors.
Clinical features
Patients with biphasic tumors may pres-ent at a younger age (mean 25 years,range 9-50 years) {644} than those withmonophasic tumours (mean of 47 years(range 33-69 years) {89}. SS shows nogender predilection {89,644,1463}. chestpain is the most common presentingmanifestation but pleural effusions, dysp-nea, dysphagia or pneumothorax canoccur {89,644}. Pleural SS can beaggressive with almost half of patientsdead of disease (with a mean of 18months).
Macroscopy and localisation
Pleural SS are usually localized, solidtumours, but they can present with dif-fuse pleural thickening like mesothelioma

{89,394,644,1463}. Some tumors have apseudocapsule, causing them to be welldemarcated from the surrounding tis-sues. The tumors may grow on a pedicle.They are usually large tumours with amean size of 13 cm (range 4-21 cm). Cutsurface of the tumour can show cysticdegenerative changes and necrosis.
Tumour spread and staging
Pleural SS typically recurs within thepleural cavity and may invade theinvolv-ing chest wall as well as adjacent struc-tures including the pericardium, anddiaphragm.
Histopathology
Histologic features of pleural SS areexactly the same as for those describedin the lung (see lung chapter). While themonophasic type is most common withinthe lung, a high percentage of pleuraltumors are biphasic {89,394,644,1463}.Mucin can be demonstrated in somebiphasic tumors. Immunohistochemistry of pleural SS typi-cally shows focal positive staining forkeratin and/or EMA with positive bcl-2,CD99 and vimentin. The glandular com-ponent of biphasic tumors may expressBER-EP4 and CEA. Calretinin and S-100may be focally positive, but desmin,smooth muscle actin and CD34 are usu-ally negative.
Differential diagnosis
In the pleura, the most important differ-ential diagnosis is malignant mesothe-
lioma, followed by sarcomatoid carcino-ma, solitary fibrous tumour and metasta-tic synovial sarcoma {89,394,644,1463}.Compared to mesothelioma, pleural SSoccur more often in younger patients,they are more likely to be localized, andtend to grow more rapidly. A pseudocap-sule may be present in pleural SS, butthis is typically absent in mesothelioma{644}. The spindle cells of SS tend togrow in long interweaving fascicles whilein mesothelioma the cells grow in bluntshort fascicles. Haemangioperi-cytoma-tous growth and hyaline fibrosis are com-mon in SS and uncommon in mesothe-lioma. The presence of mucin in glandsand expression of CEA and/or BER-EP4favors biphasic SS, although BER-EP4can be seen in some series in a high per-centage of mesotheliomasup to 20% ofmesotheliomas. Demonstration of theX:18 translocation is very helpful in con-firming the diagnosis of SS.
Histogenesis
Remains unknown. It is thought to be atotipotential mesenchymal cell and it hasnot been proven to arise or differentiatefrom synovium.
Somatic genetics
Synovial sarcoma has the distinctivetranslocation t (X; 18)(p11; q11) that isnot seen in the other tumors mentionedabove in the differential diagnosis, mostimportantly mesothelioma and sarcoma-toid carcinoma {89,694,850,957,1310,1992}. Fortunately this can readily be
demonstrated in formalin-fixed paraffin-embedded tissue. Other details aboutthis translocation are summarized in thelung chapter.
Solitary fibrous tumour (SFT)Definition
An uncommon spindle-cell mesenchy-mal tumour of probable fibroblastic deri-vation that often presents a prominenthaemangiopericytoma-like vascular pat-tern, but may exhibit other histologic pat-terns. A morphologically identical tumouroccurs in numerous other extrathoracicsites.
ICD-O code 8815/0
Synonyms
Also known as localized fibrous tumour,this lesion was once variously designat-ed benign mesothelioma, localizedfibrous mesothelioma, and submesothe-lial fibroma. The use of names thatinclude ‘mesothelioma’ for this tumour isdiscouraged because of potential confu-sion with diffuse malignant mesothe-lioma.
Etiology
No etiologic agent has been identified; inparticular there is no link with asbestosexposure.
Clinical features
Signs and symptomsThe most common symptoms at presen-tation are cough, chest pain, and dysp-noea. Some patients may present withhypertrophic osteoarthropathy and, onrare occasions, symptomatic hypo-glycemia as a result of the production ofan insulin-like growth factor {629}. Sometumours are incidental findings.
142 Tumours of the pleura - Mesenchymal tumours
Fig. 2.19 Malignant fibrous tumour of the pleura.
Fig. 2.20 Pleural synovial sarcoma. This biphasic tumour consists of glandular and spindle cells.

143Calcifying tumours of the pleura
ImagingSolitary fibrous tumours of the pleurapresent on chest radiographs as pleural-based soft tissue masses. The marginsare well defined and there is no associat-ed rib destruction or chest wall abnor-mality. A pleural effusion may be present.Tumours can vary in size from smalllesions to very large masses that occupymost of the hemithorax. When large, theyrequire CT or MR scanning to differenti-ate them from lung masses. The marginat which the lesion meets the chest wallis smooth. On CT scanning, they show apattern of heterogeneous contrast en-hancement and compress but do notinvade the contiguous lung. Rarely, theirattachment to the chest wall by a pediclecan be seen.
Macroscopy
Most tumours arise in the visceral pleura,but they may also originate in the lungparenchyma and mediastinum. They arewell circumscribed and often peduncu-lated {544}. Rarely they may be multiple.The cut surface is usually firm andwhitish, often with a whorled appear-ance. Myxoid change, haemorrhage,and necrosis may occasionally be seenand suggest that the tumour is malig-nant; large size also suggests malignan-cy. These features mandate extensivesampling.
Histopathology
SFT typically exhibits a patternless archi-tecture characterized by the coexistenceof hypo- and hypercellular areas sepa-rated by fibrous stroma having haeman-giopericytoma-like branching blood ves-sels. The hypercellular areas are com-posed of bland spindle cells arranged inshort intersecting fascicles, creating her-ringbone or storiform arrays. The hypo-cellular areas may be highly collage-
nized or, less frequently, present myxoidchanges. Malignant SFTs (ICD-O 8815/3)are characterized by greater cellularitywith an infiltrative growth pattern, moder-ate to marked cellular atypia and highmitotic activity (> 4 mitoses per 10 high-power fields) {544}.Immunohistochemical studies are helpfulin confirming the diagnosis of SFT. Incontrast with sarcomatoid mesothelioma,these lesions tend to be positive forCD34, and bcl-2, and are always nega-tive for cytokeratin {1519}. However,malignant SFT may not always expressCD34 and bcl-2. The differential diagno-sis of SFT in the pleura includes sarco-matoid mesothelioma, and a variety ofbenign and malignant soft tissuetumours, such as haemangiopericytoma,malignant fibrous histiocytoma, mono-phasic synovial sarcoma, thymoma, andperipheral nerve sheath tumours.
Somatic genetics
Only a few studies have reported cyto-genetic findings in SFT. Reported abnor-malities include: t(4;15)(q13;q26){436};46,XY,t(6;17) (p11.2;q23), ins (9;12)(q22;q15q24.1), inv (16) (p13.1q24){508}. In the latter case the rearrange-ment of 12q13-15 is similar to thatdescribed in a subset of haemangioperi-cytomas of soft tissue and meninges{508}.In one malignant SFT of the pleura suc-cessful karyotyping was obtained fromthe primary and recurrent tumours. Theinitial karyotype showed two abnormalclones: 48, XY; +8; +8; del(9)(q22; q32)[19] and 46, XY, t(1;16)(q25;p12) [7].Culture of the recurrent tumour yieldedone clone identical to the dominant cloneof the initial karyotype {447}.Comparative genomic hybridisation(CGH) of 12 SFT of pleura showed nochromosomal imbalances in 58 percent
of cases. Losses on chromosome arms13q (33%), 4q and 21q (17% each) werethe most frequent abnormality. Signifi-cant gains were seen at chromosome 8and at 15q in two cases each. There wasno correlation between tumour size andmolecular pathology findings {1073}.Another CGH study of one SFT revealedlosses of 1p33—>pter, 17pter q21, entirecopies of chromosomes 19 and 22, andgains of 1p21-p22, 2q23-q32.3, 3pl2-q13.2, 4p14-q28, 6p12-q21, 9p21—>pter and 13q21-q31. Further-more,there was loss of 20q, as was previouslyreported elsewhere in a case of benignand a case of malignant SFT {48}.
Calcifying tumour of the pleura
Definition
A rare slow growing plaque-like lesionoccurring in the visceral pleura, com-posed of nearly acellular fibrous tissue,and associated with extensive dystroph-ic calcification (which may be psammo-matous).
B CAFig. 2.21 Solitary fibrous tumour. A Spindle cells with ropy collagen stroma. B Diffuse strong positivity for CD34. C Malignant SFT showing hypercellularity, markedcellular atypia and high mitotic activity.
Fig. 2.22 Calcifying tumour. Psammoma-like calcifi-cations within a dense fibrous stroma. From {2024}.

144 Tumours of the pleura - Mesenchymal tumours
Synonyms and historical annotation
Calcifying fibrous pseudotumour, child-hood fibrous tumour with psammomabodies
Clinical features
Signs and symptomsRare examples of calcifying tumour ofthe pleura (CTP) are reported in the pleu-ra {1599}, or mediastinum {929}, butthese tumours more often occur in thesoft tissues of the extremities, trunk, scro-tum, groin, neck, or axilla {575}. Mostcases occur in children and young adultswith no sex predilection. Patients maypresent with chest pain or they may beasymptomatic.
ImagingChest radiographs or CT scans show asingle pleural mass or multiple pleural-based nodular masses with central areasof increased attenuation due to calcifica-tion, which may be extensive.
Macroscopy and histopathology
The lesions consist of circumscribed, butunencapsulated masses of hyalinizedcollagenous fibrotic tissue interspersedwith lymphoplasmacytic infiltrates andcalcifications, often with psammomatousfeatures The lesions are limited to thepleura and typically do not involve theunderlying lung parenchyma. Multiplelesions may be seen {758}. The fibrouscells may be positive for vimentin andFactor XIIIa and CD68 {830}, but nega-tive for actin, desmin, S100 protein,CD31, and usually, CD34 {2128}.
Differential diagnosisThe differential diagnosis includes otherpleural lesions such as solitary fibroustumour of pleura, calcified granulomas,calcified pleural plaques, and chronicfibrous pleuritis as well as intrapulmonarylesions such as hyalinizing granuloma,inflammatory pseudotumour, and amy-loid.
Prognosis and predictive factors
As in the soft tissues, local excisionappears adequate therapy for CFT of thepleura. If these lesions behave in a simi-lar fashion to CFT of soft tissues, onemight expect a low frequency of localrecurrence.
Desmoplastic small round cell tumour of the pleura
Definition
DRCT is a primitive polyphenotypic neo-plasm typically occurring on the seroussurfaces in the abdominal cavity andrarely in the pleura of young adult males.It possibly represents a primitive meso-thelial-related lesion.
ICD-O code 8806/3
Clinical features
The reported six cases involving pleura{164,1524,1551,1739,1936} occurred in4 men and 2 women aged 17-29 years(median age 23 years) and usually pre-sented with chest pain and pleural effu-sion. Although this pleural tumour usual-ly is fatal within 2 years, one patient livedover 5 years {1524}. DRCT can also pres-ent with an intrapulmonary mass {1936}.
Histopathology
Grossly the tumour typically forms multi-ple pleural-based nodular masses andcan produce pulmonary encasement
resembling that of malignant mesothe-lioma. Mediastinal involvement is typicalof pleural-based tumours; bilateral pleu-ral involvement and pulmonary paren-chymal metastases may also occur.Histologically the tumour is composed ofirregularly shaped islands or largersheets of small round tumour cells in cel-lular desmoplastic stroma. Focal nuclearatypia can occur in the tumour cells, andthe stroma may contain vascular prolifer-ation.
Immunohistochemical profileThe typical features include expressionof keratins, EMA, desmin (often in a per-inuclear dot-like pattern), vimentin andWilms tumour protein WT1 {677}. Sincetranslocation splits the latter gene, anti-bodies to WT1 should be used that rec-ognize the preserved carboxyterminus ofthe protein. NSE-positivity and expres-sion of CD15 are also common.
Genetics
The presence of WT1-EWS gene fusionwith the t(11;22) translocation are the keydiagnostic features of this tumour {677}.
BFig. 2.23 Desmoplastic round cell tumour. A Cellular round cell component within a dense fibrous stromaFrom {2024}. The tumour cells stain positively for B keratin and, for C desmin with a dot-like pattern.
A
C