treatment modality of non union fracture neck of femur
TRANSCRIPT

Treatment Modality of Non-Union in Fracture of Neck of Femur
Dr.Avik SarkarKB Bhabha Municipal General Hospital, Bandra (West), Mumbai

Causes of Non-Union in Fracture Neck of Femur
• FAILURE TO REDUCE OR MAINTAIN REDUCTION
• ABSENCE OF CAMBIUM LAYER OF PERIOSTEUM (CAMBIUM LAYER PRODUCES CALLUS)
• CUTTING OFF OF BLOOD SUPPLY OF HEAD
• DEVELOPMENT OF SHEERING FORCE AT FRACTURE SITE AFTER FRACTURE, CAUSING VERTICAL INCLINATION
• TAMPONADE EFFECT AT FRACTURE SITE DUE TO INTRACASPULAR NATURE OF FRACTURE
• SECRETION OF INHIBITORY SUBSTANCES AT FRACTURE SITE
INVESTIGATIONS• X-RAYS
AP
LATERAL
PBH
• CT SCAN
• MRI
• BONE SCAN WITH PIN COLOMETER (TO DIFFERENTIATE BETWEEN AVN AND NON-UNION)

Femoral neck non-union occurs in 20–30% of displaced femoral neck fractures.
Femoral neck fractures should unite by 6 months. If there is no evidence of healing, or the patient continued to have pain at 3 to 6 months after surgery, then a delayed union (3 months) or non-union (6 months) should be suspected.
TREATMENT Treatment modalities vary both in elderly and in young adults (less than 40 years)

IN THE ELDERLY Replacement Arthroplasty is the treatment
of choice for elderly patients in fracture of neck femur non-unions
Total Hip Replacement is the treatment of choice in a cooperative, independent individual with a normal life span.
Hemiarthroplasty may be done in a patient with much less demand and leading a sedentary lifestyle.
IN YOUNG ADULTS (BELOW 40
YEARS)
The type of femoral neck non-union determines the treatment needed.
Hence a classification of femoral neck non-unions was established to elucidate treatment protocols

Leighton's Classification of Femoral Neck Non-union [1]
TYPE I - INADEQUATE FIXATION OR NON-ANATOMIC REDUCTION
TYPE II - LOSS OF FIXATION WITH FRACTURE DISPLACEMENT
TYPE III - FIBROUS NON-UNION WITH NO DISPLACEMENT AND INTACT FIXATION
[1]CLASSIFICATION AND TREATMENT OF FEMORAL NECK NONUNIONS IN YOUNG PATIENTS. Leighton R. J Bone Joint Surg Br 2008 vol. 90-Bno. SUPP I 124

Type I (Inadequate fixation or non-anatomic reduction)
The surgical plan (a) removal of fixation (b) realignment of the femoral head on the neck
A Meyer's bone graft is used with a vascular Quadratus Femoris muscle pedicle. This muscle pedicle may be added to support the posterior comminution and provide a vascularized graft to ensure union.
Fixation is performed with multiple screws or a combination of sling hip screw with a superior de-rotation screw. Meyer’s Technique

a. Fracture neck femur non-union – AP viewb. 2 year follow-up – AP viewc. 2 year follow-up – Lateral view

TYPE II (Loss of fixation with fracture displacement)
The Surgical Plan
(a) removal of initial fixation
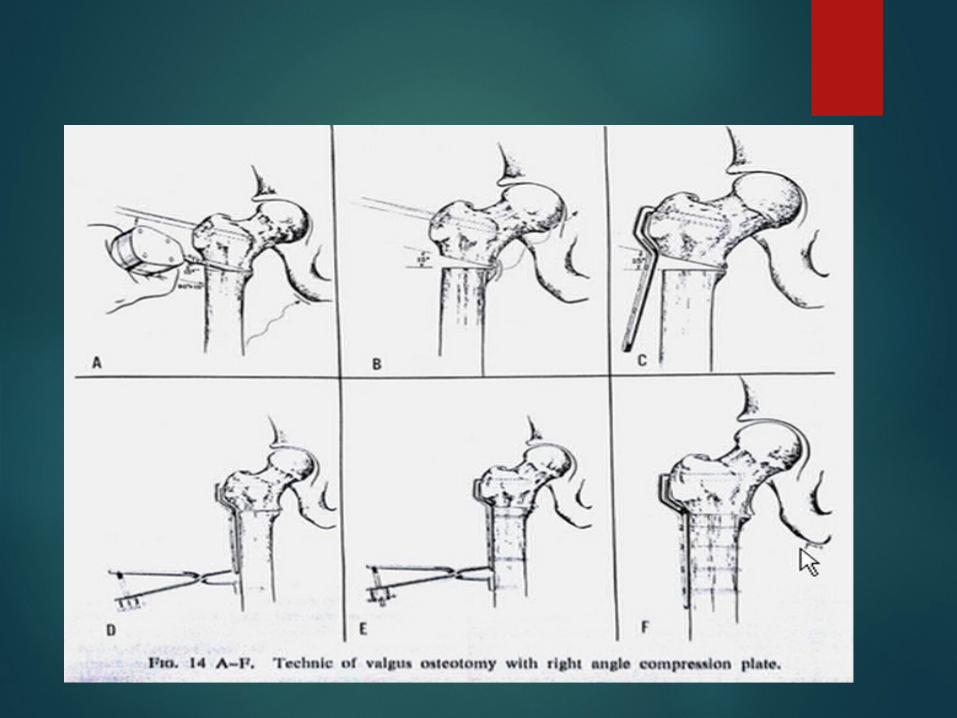
(b) deformity correction by osteotomy with an osteotomy plate using a compression device
GOALTo change a shear force on the neck fracture into a compression force.

PREPLANNING Identification and documentation of the
vascular status of the femoral head
A preoperative drawing to determine the change that will occur in leg lengths
A preoperative drawing to determine the position of the femoral head after the osteotomy (this drawing should be present in the OR while the surgery is performed)

TYPE III (Fibrous non-union with no displacement and intact
fixation) The Surgical Plan
(a) drill out the non-union
(b) fix the fracture with a fixed angled device (sliding hip screw or blade plate).
(c) add bone graft (optional)
The primary aim of this procedure is to drill out or open the endosteal canal to allow revascularization and endosteal healing in a previous fibrous non-union.
There is thick fibrous union between the two ends of the femoral neck and will prevent osseous union if canal is not freshened.

By placing numerous drill holes (4.5 to 8.0 mm in diameter) from the lateral cortex into the head, through the femoral neck, the canal is revascularized. These are inserted over guide pins, using cannulated drills.
A Meyer's vascularized graft should be added, to stimulate bone union of the femoral neck, posteriorly.
Application of a four-hole osteotomy plate, placed under compression. Subtrochanteric osteotomy was done and subsequently a secondary Meyer's graft was performed later to achieve fracture union.

REHABILITATION The patient is generally mobilized at 25%
weight-bearing over the first 6 weeks.
Once adequate healing is evident, full weight-bearing can be allowed, initially with crutches for 2 weeks, a single crutch for 2 weeks, and then weight-bearing with a cane.
PHYSIOTHERAPYAbductor strengthening should be initiated at week 6 to prevent development of Trendelenburg gait
OSTEOTOMYAn Osteotomy is a surgical corrective procedure used to obtain a correct biomechanical alignment of the extremity, so as to achieve equivocal load transmission, performed with or without removal of a portion of the bone.
PRINCIPLE
o Increases the contact areao Restores Biomechanical advantageo Moves normal articular cartilage into weight bearing zoneo Improves coverage of head

PROXIMAL FEMORAL OSTEOTOMYPROXIMAL FEMORAL OSTEOTOMIES can be classified according to
(A) Anatomic Location
High Cervical
Intertrochanteric
Subtrochanteric
Greater Trochanteric
(B) Displacement of Distal Fragment
Transpositional Osteotomy
Angulation Osteotomy
Sagittal Plane
Coronal Plane
Adduction Osteotomy (Varus)
Abduction Osteotomy (Valgus)

PRINCIPLES OF OSTEOTOMY IN NONUNION FRACTURE NECK FEMUR
Line of weight bearing is shifted medially.
Shearing force at the non-union is decreased, because the fracture surface has become more horizontal

Types of Osteotomies McMurray’s Displacement Osteotomy
Schanz Angulation Osteotomy
Dickson’s High Geometric Osteotomy
Pauwel’s Y Osteotomy
PAUWEL’S VALGUS OSTEOTOMY Valgus Intertrochanteric Femoral Osteotomies
transfer the centre of hip rotation medially from the superior aspect of the acetabulum to decrease the weight bearing area of femoral head.
Normally 15 o of correction is required
INDICATIONS Trendelenburg Limb Adduction Deformity Motion in adduction beyond adduction deformity Painful abduction
CONTRAINDICATIONS Flexion of less than 60 o
Knock Knees (It will increase the deformity)