treament of malaria
TRANSCRIPT

1
TREATMENT OF MALARIA
Dr Roto Robo
OBJECTIVES AND USE OF ANTIMALARIALS1. To prevent & treat clinical attack of malaria.
2. To completely eradicate the parasite from patient’s body.
3. To reduce the human reservoir of infection- to cut down transmission to mosquito.
4. To minimize risk of spread of drug resistant parasites by use of effective drugs in appropriate dosage by everyone.
2

CLASSIFICATION OF ANTIMALARIAL DRUGS1. Cinchona Alkaloid – Quinine, Quinidine
2. 4-Aminoquinolines – Chloroquine, Amodiaquine, Piperaquine
3. Diaminopyrimidines – Pyrimethamine
4. 8-Aminoquinoline – Primaquine, bulaquine
5. Sulfonamides & Sulfone – Sulfadoxine, sulfamethopyrazine, Dapsone
6. Sesquiterpine Lactones – Artesunate, artemeter, arteether
7. Quinoline -Methanol – Mefloquine
8. Tetracyclines – Tetracycline, Doxycycline
9. Amino Alcohols – Halofantrine, Lumefantrine
10. Mannich base – Pyronaridine
11. Naphthoquinone – Atorvaquone
12. Biguanides – Proguanil, chlorproguanil3
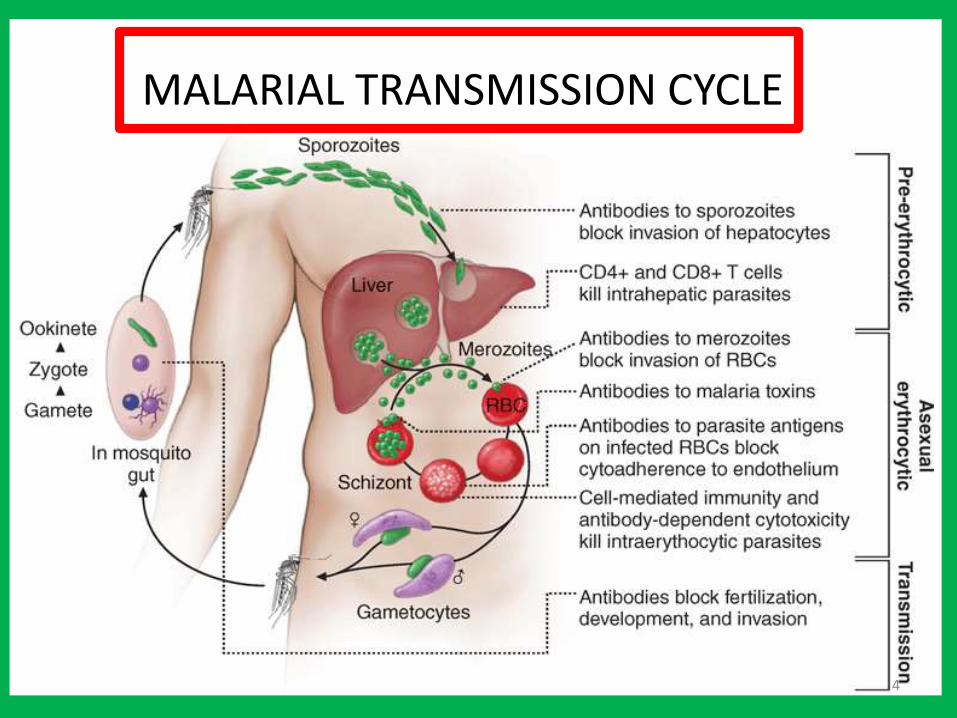
MALARIAL TRANSMISSION CYCLE
4

5
6

7

CHLOROQUINE
8

CHLOROQUINE RESISTANCE
• Slow in P. Vivax
• P. Falciparum acquired significant resistance(NE region).
MOR – Mutations in pfcrt > decreased ability of parasite to accumulate chloroquine > easy leak out of vacuole.
PHARMACOKINETICS
• Absorption – 1. orally - excellent
2. i.m. injection - good
• Large volume of distribution due to extensive tissue binding.
• Selective accumulation in retina > ocular toxicity in long use.
• Partly metabolized by liver & slowly excreted in urine.
• Early plasma t1/2 varies 3-10 days.
Terminal plasma t1/2 of 1-2 months.
9
SIDE EFFECTS
• GIT - nausea, vomiting, epigastric pain
• EYE - ↓ vision & difficulty in accomodation
• ENT - ↓ hearing
• CVS - hypotension, cardiac depression, arrythmias.
• CNS – convulsion, headache.
• Others - rashes, photo allergy, mental disturbances, myopathy , graying of hair.
CAUTIONS
• Liver damage, severe git, CNS & haematological diseases.
• Not to be co administered with mefloquine, amiodarone and other antiarrhythmics.
In pregnancy - no abortifacient or teratogenic.
10

QUININE
• Levorotatory alkaloid from cinchona bark.
• d-isomer quinidine used as an anti arrhythmic.
• Erythrocytic schizontocide for all the species of plasmodia.
• Less effective & more toxic than chloroquine.
• No pre- & exoerythrocytic action but kills vivax gametes.
• MOA ≈ chloroquine.
PHARMACOKINETICS
• Oral absorption – rapid & complete
• 90% plasma bound.
• Large fraction of dose metabolized in the liver.
• Plasma t1/2 (a) Malaria - 16hrs
(b) Healthy - 11hrs11

SIDE EFFECTS
• Hypoglycemia – common major toxicity.
• Cinchonism - tinnitus, difficulty in hearing, visual defects, nausea, vomiting, diarrhea, headache, vertigo, mental confusion, flushing, marked perspiration, postural hypotension, QTc interval prolongation.
• Other major rare s/e – hypotension, blindness, deafness, cardiac arrhythmias, thrombocytopenia, hemolysis, HUS, vasculitis, cholestatic hepatitis, neuromuscular paralysis.
• On rapid i.v. - hypotension, cardiac arrhythmias > die
12

Pyrimethamine• MOA – inhibitor of plasmodial DHFRase
• High selective affinity for plasmodial enzyme(≈2000 times > mammalian enzyme)
• Slow but long acting erythrocytic schizontocide
• No pre- & exoerythrocytic action
PHARMACOKINETICS
Good oral but variable i.m. absorption.
Plasma t1/2 of 4 days.
Prophylactic conc. remain in blood for 2 wks.
SIDE EFFECTS
Megaloblastic anemia, granulocytopenia
Folate deficiency rare13

SULFONAMIDE
• SULFADOXINE and SULFAMETHOPYRAZINE –
ultra long acting but attain low blood conc.
• They are able to synergise with pyrimethamine.
• Combination has potential to cause serious adverse effects –exfoliative dermatitis, SJS etc.
• Contraindicated – infant & patient allergic to sulfonamide.
14

PRIMAQUINE• Poor erythrocytic schizontocide – weak action on Pv and
blood form of Pf totally insensitive.
• Eradicates hepatic forms of Pv & P ovale.
• Kills all stages of gametocyte development of Pf.
MECHANISM OF ACTION
1. Generating reactive oxygen free radicals or
2. By interfering with the electron transport in the parasite.
PHARMACOKINETICS
• Complete oral absorption, Plasma t1/2 of 7 hrs
SIDE EFFECTS
• Most imprt toxic potential is dose related – hemolysis, methaemoglobinaemia, tachypnea & cyanosis(oxidant property)
• Normal individual doses < 60mg – little hemolysis but
pt with G-6-PD deficiency even 15-30 mg/day. 15

MEFLOQUINE
• Fast acting(relative) erythrocytic schizontocide against chloroquine sensitive as well as resistant plasmodia.
• Due to long t1/2 (14-20 days) chances of selection of resistant strains are high.
• Its resistance confer cross resistance to quinine & halofantrine.
• MOA ≈ quinine
PHARMACOKINETICS
• Oral absorption is good but slow.
• Metabolized in liver & secreted in bile.
16

SIDE EFFECTS
• nausea, vomiting, diarrhea, abdominal pain, sinus bradycardia.
• Dose related neuropsychiatric reactions – disturbed sense of balance, ataxia, errors in operating machinery, strange dreams, anxiety, hallucinations, rarely convulsion.
• It is safe during pregnancy but avoided in 1st trimester.
INTERACTIONS
• Co administration with halofantrine, quinidine/quinine > QTc prolongation > cardiac arrest.
• With β blockers, CCBs, digitalis and antidepressants –exaggerated bradycardia or arrythmias.
17
ARTEMISININ DERIVATIVES• Artemisinin is active principle of plant artemisia annua used
in chinese traditional medicine as “Quinghaosu”.
• Sesquiterpine lactone active against Pf resistant to all other antimalarial.
• Prodrug, active metabolite - dihydroartemisinin
• Potent & rapid blood schizontocide > quicker defervescence & parasitaemia clearance (< 48hr).
• Poor soluble in water & oil.
Artemether – soluble in oil
Artesunate – soluble in water.
arteether – soluble in chloroform.
• Don’t kill hypnozoites but have action on gametes.
• Fastest acting but short duration of action.18
• MOA –
functional group – endoperoxide bond > release of free radicals species > binds to membrane proteins > lipid peroxidation, damages ER > inhibit protein synthesis & ultimately lysis of parasite.
PHARMACOKINETICS
1. Artesunate – oral absorption is incomplete but fast reaching peak serum level within 1 hr & persist for upto 4 hrs.
Dihydroartemisinin t1/2 is < 2 hrs
2. Artemether – oral or i.m. only.
Slow oral absorption – 2-4 hrs
Plasma t1/2 is 3-10 hrs
3. Arteether - i.m. only
Plasma t1/2 23 hrs
19

SIDE EFFECTS
abnormal bleeding, dark urine,
S-T segment changes, QT prolongation, 1st degree A-V block,
transient reticulopenia & leucopenia.
Anaphylaxis, urticaria
INTERACTIONS
Co administration with terfenadine, astemizole, antiarrhythmics, TCA & phenothiazines - ↑ risk of cardiac conduction defects.
20

ARTEMISININ BASED COMBINATION THERAPY(ACT)
• WHO recommended ACT for acute uncomplicated resistant falciparum malaria.
• Artemisinin reduces parasite load rapidly & drastically killing >95% plasmodia.
• Leave only small biomass of parasites > eliminated by long t1/2
drug, reducing the chances of selecting resistant mutants.
ADVANTAGES OF ACT
1. Rapid clinical & parasitological cure.
2. High cure rates (>95%) and low relapse rate.
3. Absence of parasite resistance (components prevent development of resistance to each other).
4. Good tolerability profile.
21

VARIOUS ACT REGIMENS
1. Artesunate-Sulfadoxine + Pyrimethamine
2. Artesunate-Mefloquine
3. Artesunate-Lumefantrine
4. Artesunate-Amodiaquine
22

1. ARTESUNATE-SULFADOXINE + PYRIMETHAMINE (AS/S/P)
• 1st line drug for falciparum malaria in chloroquine resistant areas under the NAMP of india .
• But it is not effective against multidrug-resistant strains which are non responsive to S/P.
23

• Recommended dose of artesunate – 4mg/kg/bw once a day x 3 days
• Recommended dose of S/P – single dose of 25mg/Kg ofSulfadoxine and 1.25mg/Kg of pyrimethamine
• Dosage regimen recommended by NVBDCP for co-package is as follows
24

2. ARTESUNATE-MEFLOQUINE (AS/MQ)
• extensively used in Thailand, Myanmar
25
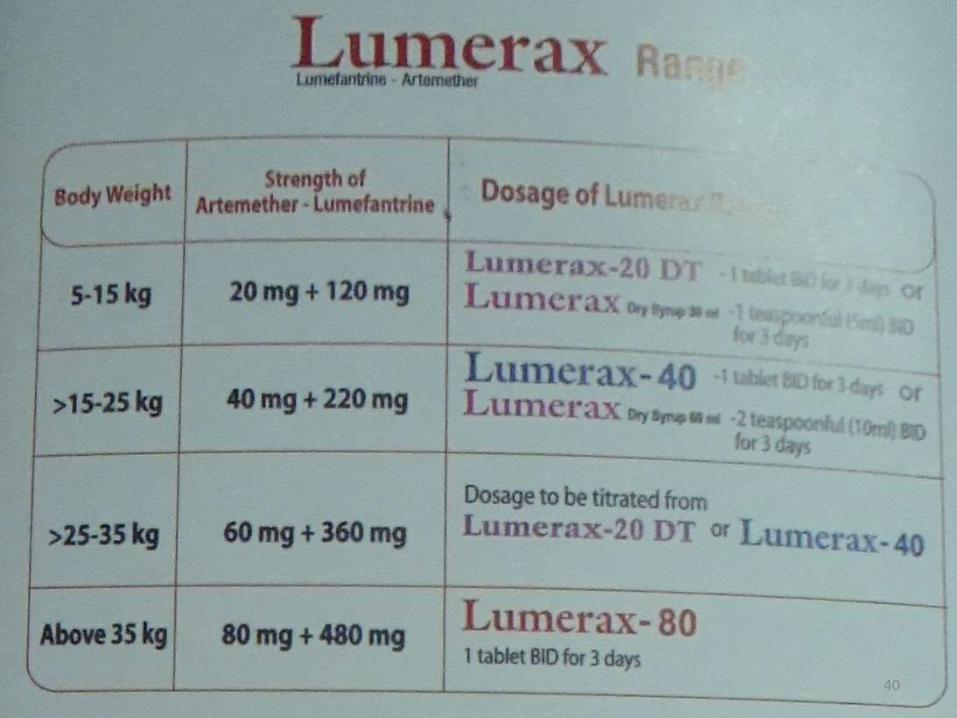
3. ARTEMETHER-LUMEFANTRINE
• LUMEFANTRINE – orally active, high efficacy, long acting erythrocytic schizontocide
• MOA ≈ Halofantrine and Mefloquine.
• No exoerythrocytic action
• Highly lipophilic – absorption starts after 2 hrs of ingestion and peaks at 6-8 hrs.
• Plasma protein binding – 99% & Metabolized by CYP3A4
• Terminal t1/2 of 2-3 days, prolonged to 4-6 days in malaria pt.
• Lumefantrine used only in combination with artemether & is only ACT available as fixed dose combination tablets.
• 80mg Artemeter BD with 480mg Lumefantrine BD for 3 days
• Two components protects each other from plasmodial resistance.
26

• Gametocytes are rapidly killed, cutting down transmission.
• Oral – well tolerated.
SIDE EFFECTS
• Headache, dizziness, sleep disturbances, abdominal pain, arthralgia, pruritus and rash.
INTERACTIONS
• Not given with metoprolol, neuroleptics, TCA etc.
• Contraindicated in 1st trimester of pregnancy & during breast feeding.
27
TETRACYCLINES
• Slow acting, weak erythrocytic schizontocidal action against plasmodial species.
• Pre-erythrocytic stage of Pf is inhibited.
• Tetracycline 250 mg QID or Doxycycline 100mg OD.
• Doxycycline 200 mg/day combined with artesunate to treat mefloquine / chloroquine / S / P – resistant falciparum malaria in Thailand.
• Used as short term chemoprophylaxis for upto 6wks.
28
PROGUANIL• Slow acting erythrocytic schizontocide & also inhibit
preerythrocytic stage of Pf.
• Gametocytes exposed to proguanil are not killed but fail to develop properly in the mosquito.
• It is cyclized in body to triazine derivative (cycloguanil) which inhibits plasmodial DHFRase in preference to mammalian enzyme.
• PHARMACOKINETICS
• Slowly but adequate absorbed form gut.
• Partly metabolized & excreted in urine.
• Plasma t ½ of 16-20 hr
• SIDE EFFECT
• Mild abdomen upset, vomiting, haematuria, rashes and transient loss of hair.
29
ATOVAQUONE
• Synthetic naphthaquinone
• Rapidly acting erythrocytic schizontocide for Pf.
MOA
collapses plasmodial mitochondria membranes
interferes with ATP production.
• Proguanil potentiates antimalarial action and prevents emergence of resistance.
30
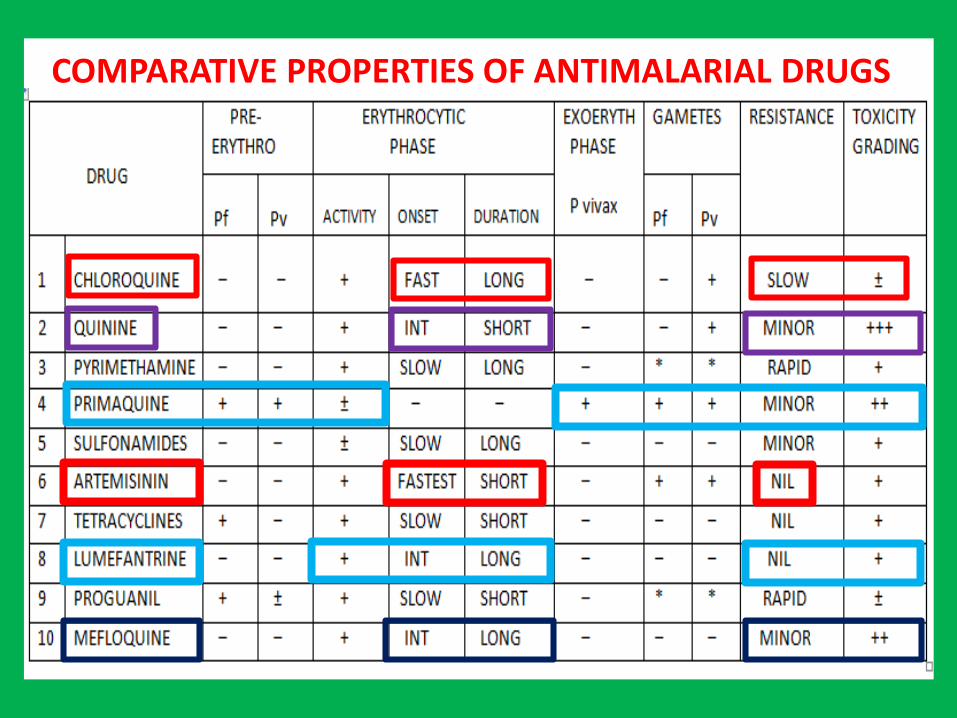
COMPARATIVE PROPERTIES OF ANTIMALARIAL DRUGS
31

Antimalarial drugs exihibit considerable stage selectivity of action.
AMT is given in following forms
1. CAUSAL PROPHYLAXIS
Pre-erythrocytic phase in liver > cause of malarial infection & clinical attacks > target for this purpose.
Primaquine – causal prophylactic for all species of malaria.
2. SUPPRESSIVE PROPHYLAXIS
Schizontocides which suppress erythrocytic phase and thus attacks of malarial fever can be used as prophylactics.
Exoerythrocytic phase in vivax & other relapsing malarias continues, but clinical d/s does not appear.
32
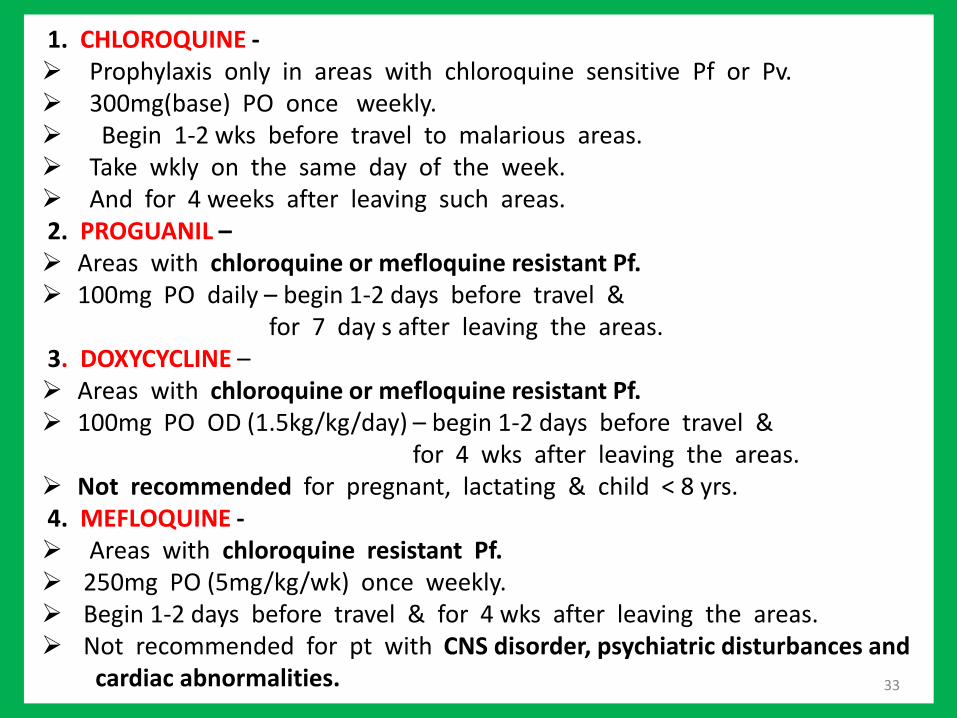
1. CHLOROQUINE - Prophylaxis only in areas with chloroquine sensitive Pf or Pv. 300mg(base) PO once weekly. Begin 1-2 wks before travel to malarious areas. Take wkly on the same day of the week. And for 4 weeks after leaving such areas.2. PROGUANIL – Areas with chloroquine or mefloquine resistant Pf. 100mg PO daily – begin 1-2 days before travel &
for 7 day s after leaving the areas.3. DOXYCYCLINE – Areas with chloroquine or mefloquine resistant Pf. 100mg PO OD (1.5kg/kg/day) – begin 1-2 days before travel &
for 4 wks after leaving the areas. Not recommended for pregnant, lactating & child < 8 yrs. 4. MEFLOQUINE - Areas with chloroquine resistant Pf. 250mg PO (5mg/kg/wk) once weekly. Begin 1-2 days before travel & for 4 wks after leaving the areas. Not recommended for pt with CNS disorder, psychiatric disturbances and
cardiac abnormalities. 33
3. CLINICAL CURE
• Erythrocytic schizontocides are used to terminate an episode of malarial fever.
1) FAST-ACTING HIGH EFFICACY DRUGS-
chloroquine, amodiaquine, quinine, mefloquine, halofantrine, lumefantrine, atovaquone, artemisinin.
2) SLOW-ACTING LOW-EFFICACY DRUGS-
proguanil, pyrimethamine, sulfonamides, tetracyclines.
4. RADICAL CURE
Drugs which attacks the exoerythrocytic stage, given together with clinical curative, achieve total eradication of parasite from patient’s body.
DOC for radical cure of vivax & ovale malaria - PRIMAQUINE 15mg daily for 14 days.
34

No point in antirelapse treatment in highly endemic areas → subsequent attack → erroneously labelled as failure of radical cure.
Antirelapse treatment of vivax malaria -
i. Areas with very low level of transmission
ii. During epidemic along with effective vector control measures to cut down transmission.
5. GAMETOCIDAL
refer to elimination of male & female gametes of plasmodia formed in pt’s blood → reducing transmission to mosquito.
PRIMAQUINE & ARTEMISININS CHLOROQUINE & QUININE
gametocidal to all species of plasmodia
active against vivax gametes
35

36

37

38

In North-Eastern states (ACT-AL)
39
40

In other states (ACT-SP)
41

42

43


45
48

SOME DON’TS IN SEVERE MALARIA CASE MANAGEMENT
DO NOT
1) Use corticosteroids
2) Give iv mannitol
3) Use heparin as anticoagulant
4) Administer adrenaline
5) overhydrate
46

47

VACCINE FOR MALARIA
RTS, S/ASO1 VACCINE
Hybrid construct of the hepatitis B surface antigen fused with a recombinant antigen derived from part of circum sporozoiteprotein.
Primarily for use in infants and young children in sub saharaAfrica.
First malaria vaccine for use in some african countries as early as 2015.
48

TREATMENT OF MALARIA - AIMS OF TREATMENT
49

50
THANK YOU