1-treament of water imbalance.pdf
TRANSCRIPT
TREAMENT OF
WATER IMBALANCE
Hala Kilany, MD

TREATMENT OF WATER IMBALANCE
• Treatment of Hyponatremia – Revisiting hyponatremia classification, pathophysiology, and
symptoms
– Approach to hyponatremia treatment
– Systematic method of hyponatremia correction
– Special topic: Treatment of SIADH
• Treatment of Hypernatremia – Approach to hypernatremia treatment
– Systematic method of hypernatremia correction
– Special topics: Treatment of NDI and CDI
Lecture Outline

OVERVIEW
• [Na+]: 135 – 145 mEq/L
• Osmolality = 2 x (Na+) = 2 x (135 - 145 mEq/L)
– Normal (Isotonic) 280 – 300
– Low (Hypotonic) < 280
– High (Hypertonic) > 300

REVISITING
HYPONATREMIA

HYPONATREMIA
• Classify hyponatremia according to duration:
– Acute: onset < 48 hours
– Chronic: onset > 48 hours or unknown onset
• 48 hrs is the time that the brain cells take to generate
osmotically active particles in response to the cellular
swelling.
• As a general rule, if the patient is completely
asymptomatic, the hyponatremia is most likely a chronic
one.
Classification
HYPONATREMIA
• Water shift from the extracellular space into the cells.
• Brain swelling occurs in the confined space of the skull
• Signs will result in relation to 3 factors: – Severity of hyponatremia
– Rapidity of hyponatremia
– Risk factors
Pathophysiology
• In the setting of an acute drop in the serum osmolality, neuronal cell swelling occurs due to the water shift from the extracellular space to the intracellular space
• Swelling of the brain cells elicits the following 2 responses:
1-Inhibition of both arginine vasopressin secretion from neurons in the hypothalamus and hypothalamic thirst center causing excess water elimination as dilute urine.
2-Immediate cellular adaptation with loss of electrolytes, and over the next few days, there is a more gradual loss of organic intracellular osmolytes.
HYPONATREMIA Pathophysiology


Risk Factors Pathophysiologic Mechanism
Children < 16 • Higher brain-to-intracranial volume ratio
Premenopausal women • Sex steroids(estrogens) inhibit brain adaptation
• Increased vasopressin levels • Cerebral vasoconstriction and
hypoperfusion of brain
Hypoxemia • Impaired brain adaptation
Ecstasy use • Syndrome of Inappropriate ADH (SIADH)
HYPONATREMIA Risk Factors of Cerebral Edema

Plasma [Na+] (mEq/L) Symptoms Mortality
> 125 Alert -
120-125 Nausea, headache, altered cognition
23%
115-120 Confusion, stupor 30%
< 115 Seizures, coma 50%
HYPONATREMIA Clinical Features & Severity
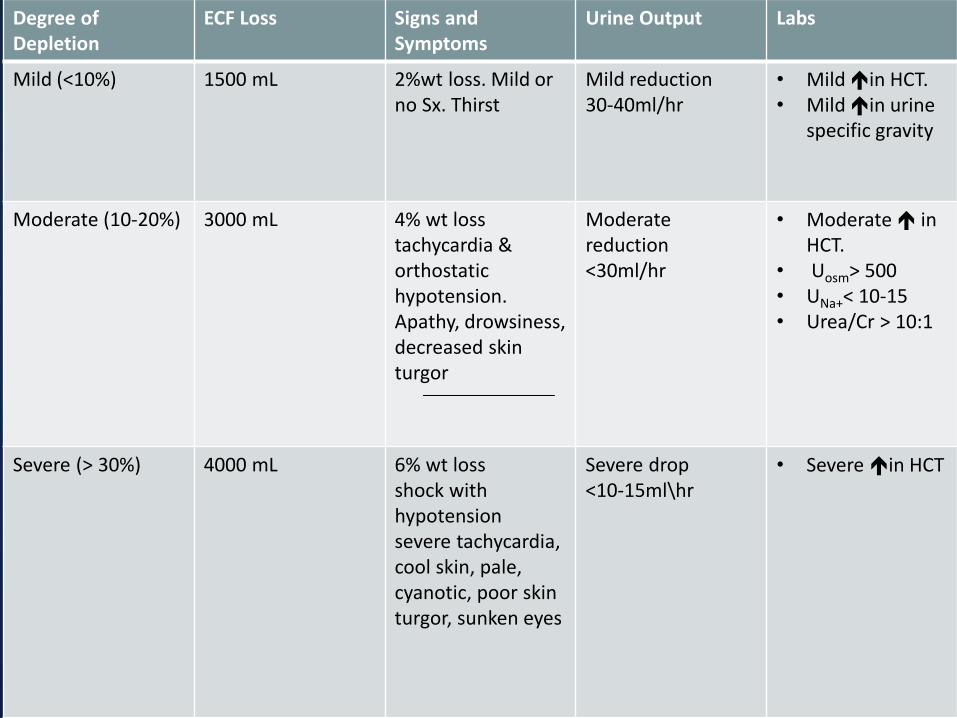
Signs and symptoms of ecf depletion according
to the degree of depletion
Degree of Depletion
ECF Loss Signs and Symptoms
Urine Output Labs
Mild (<10%) 1500 mL 2%wt loss. Mild or no Sx. Thirst
Mild reduction 30-40ml/hr
• Mild in HCT. • Mild in urine
specific gravity
Moderate (10-20%) 3000 mL 4% wt loss tachycardia & orthostatic hypotension. Apathy, drowsiness, decreased skin turgor
Moderate reduction <30ml/hr
• Moderate in HCT.
• Uosm> 500 • UNa+< 10-15 • Urea/Cr > 10:1
Severe (> 30%)
4000 mL 6% wt loss shock with hypotension severe tachycardia, cool skin, pale, cyanotic, poor skin turgor, sunken eyes
Severe drop <10-15ml\hr
• Severe in HCT

TREATMENT OF HYPONATREMIA

HYPONATREMIA
• 3 issues must be addressed: – Asymptomatic vs. symptomatic – Acute (onset < 48 hrs) vs. chronic (onset > 48 hours or
unknown) – Volume status
• 2 basic principles for treatment:
– Raising plasma sodium at a safe rate – Treating the underlying cause
• Mainstay of treatment:
– Intravenous isotonic saline
– Need to discontinue diuretics
Approach


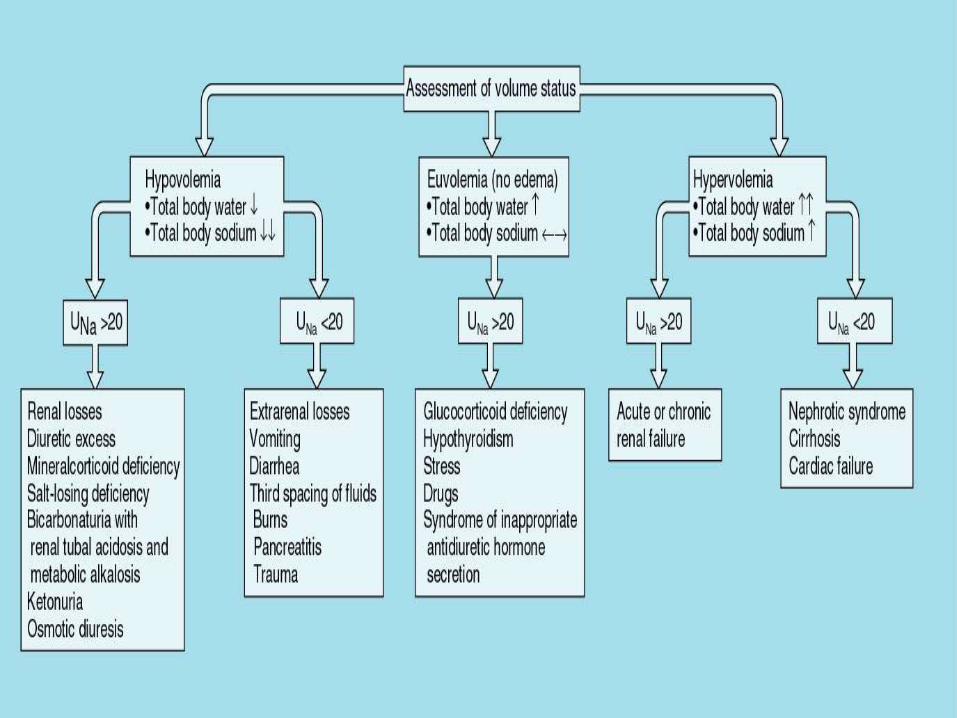
• Evaluate volume status by physical examination:
– HR and BP
• Supine and after 1 min of standing to assess
orthostatic hypotension, defined as any of the
following:
– Decrease of 20 mmHg or more of systolic pressure
– Decrease of 10 mmHg or more in diastolic pressure
– Increase in HR after rising > 15-30 bpm
– Skin turgor
– Lower extremity edema and sacral edema
HYPONATREMIA Evaluation of Volume Status

• Raise plasma sodium at a safe rate:
– Raise Na by <10 meq/L in the 1st 24 hours
– Raise Na by <18 meq/L in the 1st 48 hours
• Rapid correction may cause pontine myelinolysis:
– Paraparesis, dysarthria, dysphagia,coma seizures
– May not be detectable until 4 weeks.
HYPONATREMIA Principles of Treatment

©2010 by Cleveland Clinic

HYPONATREMIA
• Raising Na > Than 12 mEq/L elevation in the 1st day
• Overcorrection to > 140 mEq/L within the 1st 2 days
• Hypoxic or anoxic episode prior to therapy
• Hypercatabolism or malnutrition due to burns or chronic alcoholism
Risk Factors of Pontine Myelinolysis

1. Calculate Total Body Water (TBW)
1. Decide the desired correction rate based on
pt’s symptoms and onset of hyponatremia
1. Estimate serum Na+ change on the basis of
Na+ in the infusate
HYPONATREMIA Systematic Method of Correction

HYPONATREMIA
Calculate total body water (TBW)
TBW = 0.60 × Patient Weight (kg)
• Total body water: – Nonelderly male: 0.60 × patient weight (kg)
– Nonelderly female: 0.50 × patient weight (kg)
– Elderly male: 0.50 × patient weight in (kg)
– Elderly female: 0.45 × patient weight (kg)
Systematic Method of Correction

Decide the desired correction rate based on pt’s symptoms and onset of hyponatremia
• Symptomatic:
– Immediate increase in serum Na+ by 8-10mEq/L in 4-8 hrs with hypertonic saline.
• Acute:
– More rapid correction is possible, 8-10mEq/L in 4-6 hrs.
• Chronic:
– Slower rate of correction: < 10 mEq/L in the 1st 24hrs.
HYPONATREMIA Systematic Method of Correction
• If a patient is symptomatic due to rapid
decline in [Na+], hypertonic (3%) saline
should be considered:
– A simple rule of thumb: Correction of 1 mEq/Lhr
using 3% saline by infusing the body weight as
mL/hr
– Example: a man with a body weight of 70 kg
will increase by almost 1meq/l/hr when infused
with 3% saline at a rate of 70ml/hr
HYPONATREMIA Systematic Method of Correction

FIRST HOUR MANAGEMENT IN SEVERE
SYMPTOMATIC HYPONATREMIA

FOLLOW-UP MANAGEMENT IN CASE OF
IMPROVEMENT OF SYMPTOMS AFTER A 5
MEQ/L INCREASE IN SERUM Na+

Estimate serum Na+ change on the basis of Na+ in the infusate:
∆SNa+ = {[Na+ + K+]inf – SNa+} ÷ (TBW+1)
* ∆SNa+=change in serum sodium
* [Na+ + K+]inf = [Na+] and [K+] in 1 L of solution
HYPONATREMIA Systematic Method of Correction
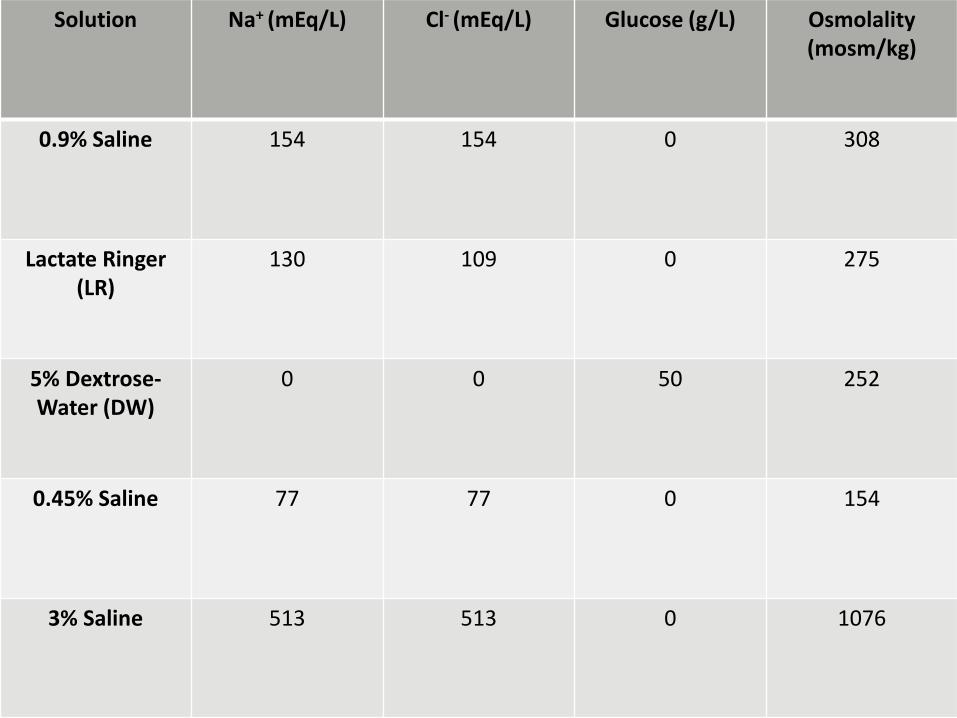
Solution Na+ (mEq/L) Cl- (mEq/L) Glucose (g/L) Osmolality (mosm/kg)
0.9% Saline 154 154 0 308
Lactate Ringer (LR)
130 109 0 275
5% Dextrose-Water (DW)
0 0 50 252
0.45% Saline 77 77 0 154
3% Saline 513 513 0 1076

Composition of GI Fluids (mEq/L)
Source Daily Loss Na+ K+ Cl- HCO3-
Saliva 1000 30-80 20 70 30
Gastric 1000-2000 60-80 15 100 0
Panc 1000 140 5-10 60-90 40-100
Bile 1000 140 5-10 100 40
SB 2000-5000 140 20 100 25-50
LB 200-1500 75 30 30 0
Sweat 200-1000 20-70 5-10 40-60 0

EXAMPLE: ONE
A 60 kg woman with a plasma [Na+] =110 mEq/L:
– What is her total body water (TBW)?
– How high will 1 liter of NS raise the plasma Na+?
– If 40meq/l of K+ to the liter of NS are added, how
much will the plasma Na+ rise?
∆SNa+ = {[Na+ + K+]inf – SNa+} ÷ (TBW+1)

EXAMPLE: TWO
A 90 kg man with a plasma [Na+] of 110mEq/L:
– What is the TBW?
– How much 1 liter of 3% saline will raise the plasma
Na+?
∆SNa+ = {[Na+ + K+]inf – SNa+} ÷ (TBW+1)

EXAMPLE: THREE
A 60 kg woman with a plasma sodium concentration of
120mEq/ L:
• Correction of sodium deficit?
– Sodium deficit = TBW x (130 – [Na+]p) = 0.5 x 60 x (130-
120) = 300mEq
– 3% NaCl contains 513 mEq sodium/L: Volume of 3% NaCl
needed = 300/513 = 585 mL
– At 0.5 mEq/L/hr a correction of 10 mEq should be done
over 20 hours: 585 mL/20 hours = 29 mL/hour of 3% NaCl

HYPONATREMIA
• SIADH is a cause of hyponatremia that cannot be
treated conventionally:
– In hypovolemia, both Na+ and water are retained.
– In SIADH, Na+ handling is intact
• Administered Na+ will be excreted in the urine. Some water will be
retained leading to worsening of hyponatremia
• Instead, water restriction is mainstay of therapy in SIADH
Exception to the Rule: Treatment of SIADH
Treatment of SIADH
Acute Chronic
• Water restriction • Hypertonic saline • NaCl tablets • Loop diuretics
• Water restriction
• High salt, high protein diet • Loop diuretic • Other: demecleocycline,
lithium, or urea.

EXAMPLE: FOUR
• 85 year old male with weakness and headache:
– Serum [Na+ ] = 118meq/l
– Plasma Osmolality = 236mosm/kg
– Urine Osmolality = 450mosm/kg
– Urine Na+ = 54meq/l
– Uric acid = 3mg/dl
1. What is the cause of hyponatremia?
2. How to correct hyponatremia?

TREATMENT OF HYPERNATREMIA

HYPERNATREMIA
• General principles:
– Rapid correction can induce cerebral edema,
seizures, permanent neurologic damage, and
death.
– Correct slowly, not exceeding 12mEq/L per day
Approach

HYPERNATREMIA
• Most cases of hypernatremia are due to
water deficit
Water deficit
=
0.4 x lean body weight x (plasma Na+/[140 – 1])
Systematic Method of Correction
HYPERNATREMIA
• Thiazide diuretics
• Amiloride in lithium-induced NDI
– Amiloride inhibits entry of lithium to collecting
tubules through Na+ channels
– Increased Li+ absorption proximally
• Low protein and low sodium diet
Treatment of Nephrogenic Diabetes Insipidus (NDI)

HYPERNATREMIA
• Vasopressin by nasal insufflation or oral form
• Thiazide diuretic: Less helpful than in NDI
• Loop diuretics should not be used
Treatment of Central Diabetes Insipidus (CDI)