trauma tips and tricks pdf - ki...
TRANSCRIPT

TRAUMA Tips and Tricks for GPs
Christopher Dobbins MB.BS, MS, FRACS
Division of Surgery, Division of Trauma and Critical Care Royal Adelaide Hospital

Triad of death
• Cold
• Acidosis
• Coagulopathy

Damage control resuscitation
• Correct coagulopathy
• Warm patient
• Fill patient
• Damage Control Surgery
Damage Control Surgery• Non definitive surgery
• Patients unstable
• Aim is control of haemorrhage and control of sepsis
• Move patient to ICU to continue resuscitation
• Make patient metabolically and haemodynamically stable
• Return to theatre for definitive procedure
Damage control for GPs• ABCDE (CABCDE)
• Commence Resuscitation
• Warm patient
• Control of Haemorrhage
• Control of Sepsis
• Splint Fractures
• Move patient to major centre for definitive care

Airway• Cricothyroidotomy
• Indications
• Can’t get airway by conventional means
• Can’t ventilate by conventional means
• Severe facial trauma
• Most difficult aspect of cricothyroidotomy is making decision to do it

Breathing• Needle Thoracostomy • 2nd ICS mid-clavicular line • 14g jelco • 50% do not go in. Some go into lung • 50% fail • Easy to do !Not always useless but mostly !• Would I do it?

Breathing• Finger thoracostomy
• Patient must be intubated, ventilated-Positive Pressure Ventilation
• Make hole as per chest drain
• Look and Listen for GUSH
• Prelude to chest drain
• Placement of immediate drain not required

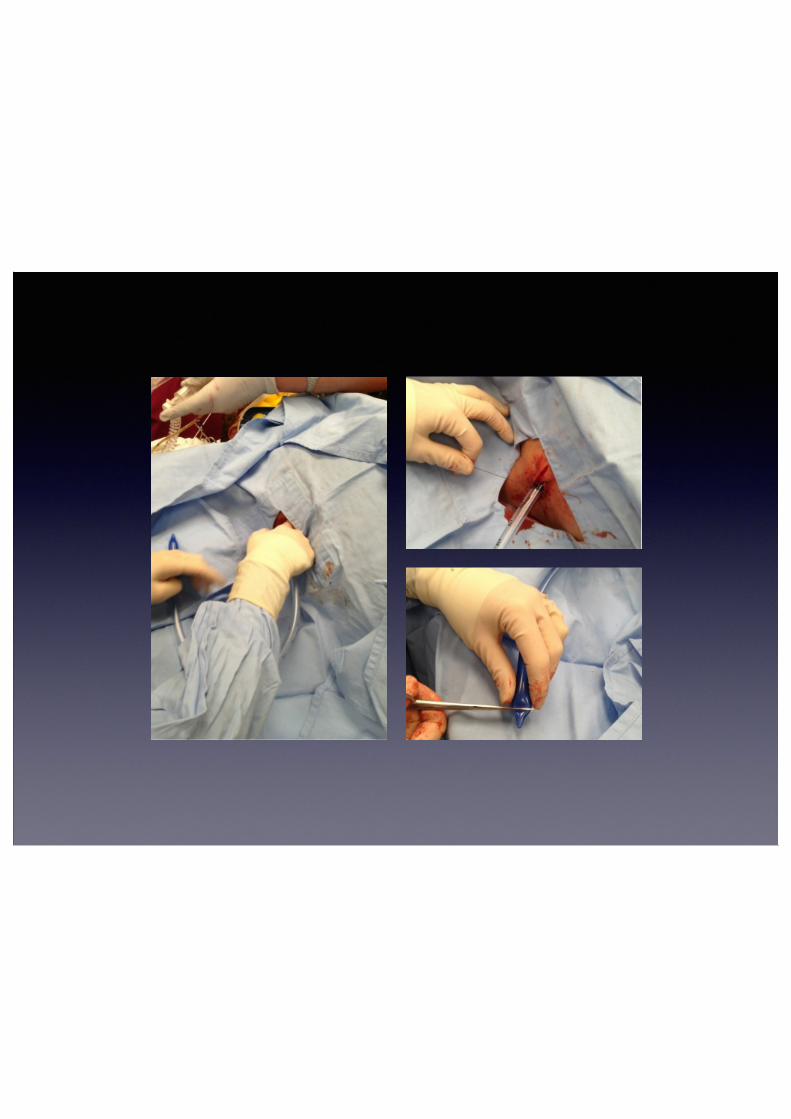
Chest Drain!
• Nipple level and above
• Big Drain (32Fr)
• 3cm incision
• Blunt dissection with artery clip

Chest Tube• Once in, open clip up wide
• Rip out
• Finger in and sweep
• Insert tube with finger
• Tie in
• Local Anaesthetic-lots +/- fentanyl and midazolam



“Do not clamp chest tubes-it is dangerous!”

Circulation• EZ IO
• Rapid Infuser Catheter
• EJV cannulation
• Swan sheath into femoral vein
• Venous Cutdown

Haemorrhage Control
Limb Pressure Tourniquet !Torso Pressure Foleys catheter




Permissive Hypotension• If patient able to talk to you coherently
and making enough urine, can accept BP ~ 80 systolic
• Pushing fluid to aim for higher BPs thought to dilute clotting factors and dislodge clots
• In NON head injured patients

Abdominal Trauma
• Penetrating Trauma
• Blunt Trauma
• The 2 are different

Blunt Abdominal Trauma• Spleen
• Liver
• Bowel
• Mesentery
• Pelvis
• Retroperineum
Penetrating Abdominal Trauma
• Rule of Thumb
• They all go in
• Other Rule of Thumb
• They generally deserved it
• One medical condition where obesity is good

Penetrating Trauma
• If They're still in, Leave ‘em in

Penetrating Abdominal Trauma
• Local Wound Exploration
• Dipstick
• Finger
!ALL ARE NONSENSE!
• All should undergo surgical review
• Positive is positive but negative means nothing

Penetrating Abdominal Stabs• Isolated stab wounds can be managed conservatively:
• Patient haemodynamically stable
• Patient has minimal signs
• Patient alert and cooperative
• Only in a major trauma centre
• Multiple stab wounds probably need surgical exploration
• ALL SHOULD BE REFERRED FOR SURGICAL REVIEW

Gunshot Wounds
• All warrant a trip to the operating theatre

U/S• FAST scan
• Supplanted use of DPL
• Detects presence of fluid in abdominal cavity and pelvis
• Extended FAST
• Checks pericardium for fluid/tamponade
• Checks for Pneumothorax

CT scan• Gold standard investigation for blunt abdominal trauma
• Patient must be stable to perform
• Logistically at the RAH, scan takes 30 min to perform
• Directly impacts patient management
• Theatre vs interventional radiology vs conservative
• Dedicated contrast scans- combined arterial and venous phase

Pelvic Binder• Pelvic Binder for all
suspected pelvic injuries
• Position across greater trochanters-lower than you think
• Binder not available- use sheet and tie knees

Pelvic Spring
• If going to do it,do it only once
• If going to do Xray or CT- not necessary

Emergency Room Thoracotomy
• Indications
• Witnessed arrest within arrival in emergency room. Standard resuscitation efforts fail
• Penetrating trauma
• Blunt Trauma controversial
Aims of ED Thoracotomy
• Relieve cardiac tamponade
• Control bleeding
• Aortic compression

Risks of ED thoracotomy
• Potential for staff exposure
• Uncontrolled bleeding




Other Points• Blood taking-generally won’t be used
• CT scans-not necessary as often need repeating
• If scans are done, please get radiology to make them available to us, we will review them early. SEND HARD COPIES
• Liaise early

Summary• ?ABCDE (CABCDE)
• Warm patient
• Damage Control
• Package patient for transfer
• Do the Basics Well