tossicità renale da immune checkpoint inhibitors - · pdf filetossicità renale...
TRANSCRIPT

Patrizia GiannatempoFondazione IRCCS Istituto Nazionale
dei Tumori, Milano, Italy
Tossicità renaleda Immune checkpoint inhibitors

Co‐Investigator in IMvigor210, IMvigor211,
CA209‐275, MK‐3475‐045, DANUBE trials
Disclosures

Typical patient with bladder cancer
Typical clinical trial participant

Renal dysfunction is common in patients with urothelial cancer
Dash et al, Cancer, 2006
Proportion of patients deemed ineligible (i.e. creatine clarance< 60 min/ml) by the Cockroft‐Gault formula by age group

The burden of cancer is shifting to the elderly
Edwards BK et al. Cancer. 2002Slide used with courtesy of T. Cerny
3.0
2.5
2.0
1.5
0.5
0
85
75–84
65–74
50–64
<50
2030 2040 205020202000 2010Year

Immunotherapyand
kidney failure

Metabolism and Elimination ofTherapeutic Monoclonal Antibodies
• mAbs are metabolized to peptidesand amino acids in several tissues,by circulating reticuloendothelialsystem (RES=macrophages andmonocytes)
• Antibodies and endogenousimmunoglobulins are protectedfrom degradation by binding toprotective receptors (the neonatalFc‐receptor [FcRn]), which explainstheir long elimination half‐lives (upto 4 weeks).
Keizer RJ et al., Clin Pharma 2010Tabrizi MA et al., DDT 2006
Lammerts van Bueren JJ et a., Cancer Res 2006Duconge J et al., Drug Metab Pharmacokinet 2002
Pharmacokinetics of TherapeuticMonoclonal Antibodies
• intracellular metabolism and be reduced to small endogenous amino acids
• GFR 15 mL / min / 1.73 m (2) or higher has no effect on the clearance compared to normal renal function
Keizer RJ et al., Clin Pharma 2010Tabrizi MA et al., DDT 2006
Lammerts van Bueren JJ et a., Cancer Res 2006Duconge J et al., Drug Metab Pharmacokinet 2002

Quanto riportato in RCP
Nivolumab: • Non sono state riscontrate differenze clinicamenteimportanti nella clearance di nivolumab tra pazienticon compromissione renale lieve(GFR < 90 e ≥ 60mL/min/1,73 m2; n = 379) moderata (GFR < 60 e ≥30 mL/min/1,73 m2; n = 179) e pazienti confunzionalità renale normale.
• I dati su pazienti con compromissione renale severa(GFR < 30 e ≥ 15 mL/min/1,73 m2; n = 2) sonotroppo limitati per poter trarre delle conclusioni inquesta popolazione

Pembrolizumab“Non è necessario alcun aggiustamento della dose nei pazienti con danno renale lieve o moderato. KEYTRUDA non è stato studiato in pazienti con danno renale grave
Quanto riportato in RCP

Immunotherapy and renal impairment
• Ipilimumab/Nivolumab/Pembrolizumab :– Currently approved ICBs have not been evaluated in patients with severe renal impairment
– No dose adjustment is recommended for patients with mild or moderate renal impairment (i.e. ≥30 ml/min creatinine clearance)
• Clinical and pharmacokinetic data with pre‐existing severe renal impairment are limited

Uso compassionevole Atezolizumabinel carcinoma uroteliale (II linea)
• …..• …..• …..• Pazienti con adeguata funzionalità renale• …..GFR>15 mL/min/1,73 m2
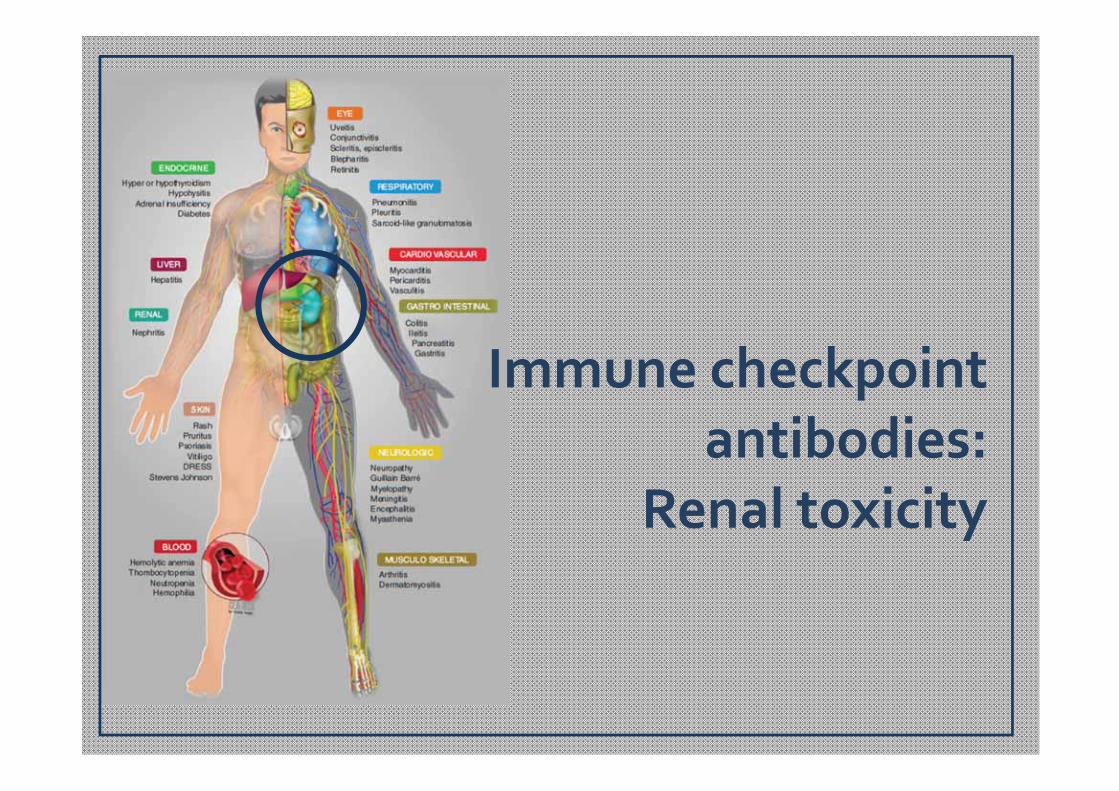
Immune checkpoint antibodies:
Renal toxicity

Case Report
• 78‐year‐old man was hospitalized for acute kidney injury• Metastatic (bone, lung and lymph nodes) melanoma was
diagnosed on February 2012• Ipilimumab 10 mg/Kg every 3 weeks RT (6 Gys in 3
fractions on one axillarymetastatic lymph node)• 5 days after the 2nd injection, the patient experienced
fatigue, anorexia, mild diarrhea and a grade 3 rashes. Ipilimumab was discontinued.
• Body temperature = 38.5 °C • blood pressure = 120/80 mm Hg
Izzedine H. et al.,Invest New Drugs 2014

• Progressive renal failure was observed 1 week• Blood examination:
– leucocytes 11,450/mm3 with eosinophils 2,300/mm3– urine proteins (0.3 g in a 24 h collection)– 35.5 leucocytes per high‐power field– negative urinary cultures
• Serum creatinine from 0.68 to 2.33 mg/dl (creatinineclearance 28 ml/min versus 84ml/min at baseline)
• Hepatitis B and C serology, anti‐nuclear antibody,antineutrophil cytplasmic antibodies (ANCAs) andantiglomerular basement antibodies were negative
Case Report

• Septic screening was negative, no volume depletion, hemodynamic stress, nor administration of nephrotoxicmedications neither radio contrast, urinary Bence Jones protein was negative.
• Renal ultrasound showed enlarged, swollen kidneys without dilated pyelocaliceal cavities.
• A percutaneous renal biopsy was performed.– Severe interstitial inflammation + edema + polynuclear
infiltration in glomerular
Case Report

• Oral prednisone at a dose of 1 mg/kg for 4 weeks, followed by fast tapering.
• Serum creatinine level fell to 1.0 mg/dl over the next 2 weeks without dialysis and urinary leucocytes disappeared.
• His rash had completely resolved and the rest of medical examination was within normal limits.
• Staging showed a 40 % tumor reduction
Case Report

• Mainly asymptomatic laboratory findings– Elevated creatinine and blood urea nitrogen (BUN)levels
• Change in urine output, proteinuria, flank pain,and edema may be symptoms of renal failure
• Fever may occur• In some case + other immune‐related AE• Appears much later, after 14–42 weeks onimmunotherapy Naidoo J,et al. AnnOncol.2015
Kodner CM el al. Am Fam Physician 2003Izzedine H et al. Invest New Drugs. 2014
Voskens CJ et al. PlosOne 2013
Immuno‐related nephritis: symptoms

Differential diagnosis of immuno‐related nephritis• Acute deydration from fluid loss (eg. Diarrhea, CT‐induced)
• Infection• Physical obstruction• Tumor progression in kidney and/or metastaticdisease
• Autoimmune disease (e.g LES, sarcoidosis)• Vascular etiologies• Metabolic abnormalities (e.g. diabetes)
Kodner CM et al.Am Fam Physician. 2003Rahman M, et al. Am Fam Physician. 2012

Differential diagnosis of immuno‐related nephritis• Infectious etiologies
– fever, chilling, nausea, vomiting, pos urine cultures or viral serology
• ObstructionHydronephrosis• PD in kidneyCT scan• Autoimmune diseaseAb (ANAs…)• Vascular etiologies
– livedo reticularis, abdominal bruits, funduscopicabnormalities
• Immuno‐related asymptomatic, mild proteinuria, gradually increasing creatinine, rash

Diagnosis of immuno‐relatednephritis:• Clinical assessment (vital signs, hydratationstatus, hypotension …)
• Laboratory finding:– GFR– Urinalysis– Complete blood count– Urine colture and viral serology (e.g.CMV, EBV)
• Radiologic finding:– US and/or CT scans


Ipilimumab Tremelimumab Nivolumab Pembro Atezo Durvalumab
Mechanism CTLA‐4 inhibitor
CTLA‐4 inhibitor
PD‐1 inhibitor
PD‐L1 inhibitor
PD‐L1 inhibitor
PD‐L1 inhibitor
Status
FDA melanoma
FDAmesothelioma
FDA HL, H&N,
lung cancer,RCC,
melanoma
FDA H&N, NSCLC,
melanoma
FDA NSCLC, urothelialcarcinoma
Under trial
RenalfailureAll Grade(%)
1 None 1‐3 <1 None 1‐2
Kumar V. et al. Pharmac 2017, Hodi et al., 2010; Wolchok et al., 2010; Ibrahim et al., 2011; Eggermont et al., 2015, 2016; Horvat et al., 2015; Larkin etal., 2015; Postow et al., 2015; Robert et al., 2015, Tarhini et al., 2012; Ribas et al., 2013b; Calabro et al., 2015; Kindler et al., 2016, Topalian et al., 2012,2014; Weber J. S. et al., 2013; Borghaei et al., 2015; Brahmer et al., 2015; Larkin et al., 2015; Rizvi et al., 2015; Robert et al., 2015a; Ferris et al., 2016,Berger et al., 2008; Armand et al., 2013; Westin et al., 2014, Berger et al., 2008; Armand et al., 2013; Westin et al., 2014, Fehrenbacher et al., 2016;Rosenberg et al., 2016; Rittmeyer et al., 2017, Massard et al., 2016
Immuno checkpoint inhibitors and Renal Failure
Howmany patients?

CPS = combined positive score of tumor and immune cell PD‐L1 expression.
Pembrolizumab 200 mg Q3W
Pembrolizumab 200 mg Q3W
Primary Endpoints• ORR in all patients• ORR in patients with PD‐L1–positive tumors
Patients (N = 350)• Advanced urothelial
cancer• No prior chemotherapy
for metastatic disease• ECOG PS 0‐2• Ineligible for cisplatin
based on ≥ 1 of the following:– CrCl <60 mL/min– ECOG PS 2 – ≥ grade 2 neuropathy or
hearing loss– NYHA class III CHF
• Secondary Endpoints: DOR, PFS, OS, and ORR in all patients, PD‐L1 positive and PD‐L1–high expressing patients; safety and tolerability; establish an assay cut point for high PD‐L1 expression
Balar AV et al., Lancet 2016
CDDP UNFIT: KEYNOTE‐052

• Baseline characteristics: – 70% (n= 83) pts with renal impairment
• GFR less than 60 mL/min and more than 30 mL/min
– 7%(n=8) pts with renal impairment + ECOG PS2
Treatment‐related adverse events: Renal failure 2 (2%)

• Durvalumab + Tremelimumab 2%• Ipilumumab (lupus nephrititis or granulomatousnephritis
• Nivolumab + platinum‐doublet chemo in NSCLC phase I
Segal NH, et al. ESMO 2014.Antonia S, et al. LancetOncol 2016.
Izzedine H, et al. Invest New Drugs 2014.Thajudeen B, et al. AM J Ther 2015
Di Giacomo AM, et al. Cancer Immunol Immunother 2009.
Immune checkpoint inhibitors and RenalFailure
Howmany patients?

Treatment of immuno‐relatednephritis
• Steroids even for low‐grade events (Grade 2) in order to prevent potential progression tohigher‐grade event
• Monitor:– Routine urinalysis– Elevated serum BUN and creatinine, GFR, electrolyte imbalance, decrease in urine output, proteinuria

Immuno‐related NephritisTake home message• Most cases asymptomatically• Gradual increases in serum creatinine levels• Rule out other causes of elevated creatinineor acute failure
• An early intervention can prevent worse orirreversible renal injury ‐‐ Steroids
• Routine laboratory monitoring of kidneyfunction at baseline, prior to each treatment,after treatment cessation
