topic 3b: documentation prep for ncqa … 14, 2013 · topic 3b: documentation prep for ncqa...
TRANSCRIPT

Topic 3B: Documentation Prep for NCQA Recognition Focus on
Standards 3, 4, and 1F
Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant
January 2013

Welcome • Introductions and Housekeeping
http://www.ncqa.org/gri
Please visit the AIR FQHC Learning Portal for more information on upcoming events at http://fqhcportal.airprojects.org
Speaker introductions
2

PCMH Transformation Framework
3

Learning Objectives
4
• Understand documentation requirements for NCQA PCMHTM 2011 recognition by Standard, Element and Factor
• Understand formatting tips for outlining documentation in a clear and understandable manner
• Review documentation examples and tips for formatting documentation for submission

Session Road Map Documentation Tips
PCMH Standard 3 Plan and Manage Care:
Element A: Implement Evidence-Based Guidelines (4 points)
Element B: Identify High-Risk Patients (3 points)
Element C: Care Management (4 points) (Must Pass)
Element D: Medication Management (3 points)
Element E: Use Electronic Prescribing (3 points)
* This webinar covers element F of PCMH Standard 1. Elements A, B, C, D, E, and G of Standard 1 will be covered in other webinars.
PCMH Standard 4 Provide Self-Care Support and Community Resources:
Element A: Support Self-Care Process (6 points) (Must Pass)
Element B: Provide Referrals to Community Resources (3 points)
PCMH Standard 1 Enhance Access and Continuity: *
Element A: Access and Continuity (4 points) (Must Pass)
Element B: After-Hours Access (4 points)
Element C: Electronic Access (2 points)
Element D: Continuity (2 points)
Element E: Medical Home Responsibilities (2 points)
Element F: Culturally and Linguistically Appropriate Services (2 points)
Element G: The Practice Team (4 points)
5

General Tips on Documentation
6
• Accentuate information for the NCQA surveyor
• Format documentation in a clear and organized manner
• Include a ‘narrative description’ as a summary of information presented in the documentation
• Save documentation for a single element into one document, with sub-headers for each factor

General Tips on Documentation (Cont’d)
7
• Reports: Include the name of the report, reporting period, numeric values of the numerator and denominator
• Policies: Include date of most recent update
• Screen shots: use real patient data, de-identified
• Policies, procedures and job descriptions must not be younger than 3-months from date of submission. Data must not be older than 12-months.

Example of Documentation Formatting
8

PCMH 3: Plan and Manage Care The practice systematically identifies individual patients and plans, manages and coordinates their care, based on their condition and needs and on evidence-based guidelines.
Elements: A. Implement Evidence-Based Guidelines (4 points) B. Identify High-Risk Patients (3 points) C. Care Management (4 points) (Must Pass) D. Medication Management (3 points) E. Use Electronic Prescribing (3 points)
9

PCMH 3A: Implement Evidence-Based Guidelines Practice implements evidence-based guidelines through point-of-care reminders for patients with:
Factors:
1. The first important condition
2. The second important condition
3. The third condition, related to unhealthy behaviors or mental health or substance abuse (Critical Factor)
10
PCMH 3A Scoring 4 points for this element Scoring:
3 factors = 100% 2 factors (including factor 3 [critical factor]) = 50% 1 factor = 25% 0 factors = 0%
11

PCMH 3A Documentation Example
Example of format:
XXX Clinic’s Three Important Conditions: 1. Name First Condition Here (ex. Diabetes) – List name and
source of evidence-based guidelines for first condition
2. Name Second Condition Here – List name and source of evidence-based guideline for second condition
3. Name Third Condition Here – List name and source of evidence-based guideline for third condition, related to unhealthy behavior, mental health or substance abuse
12

PCMH 3A-1, 3A-2 or 3A-3 Documentation Example
13
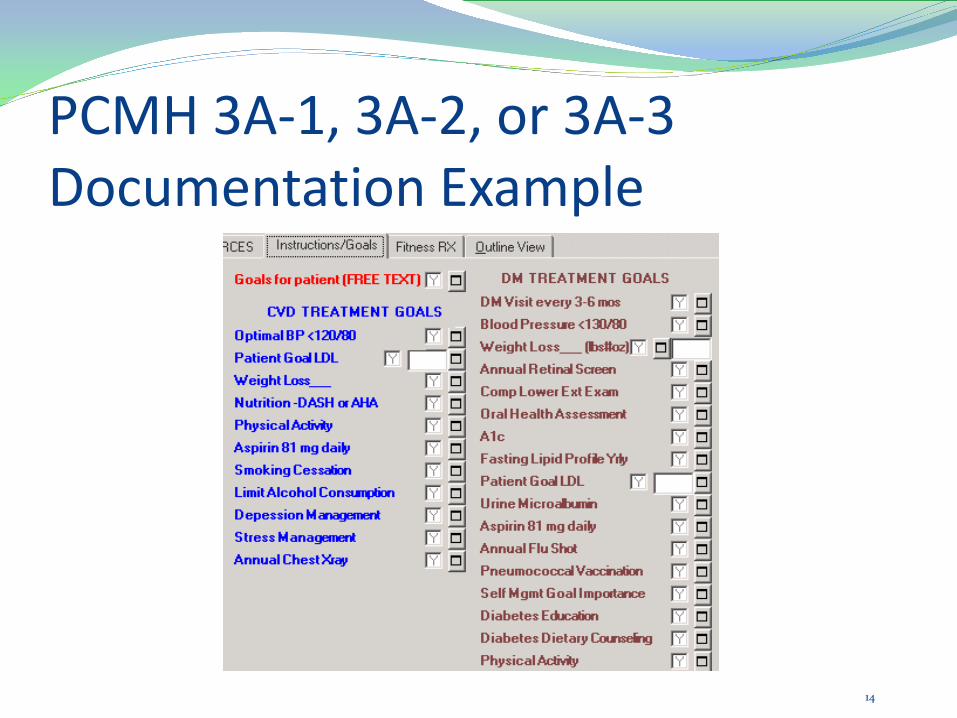
PCMH 3A-1, 3A-2, or 3A-3 Documentation Example
14
PCMH 3A-1, 3A-2, or 3A-3 Documentation Example
15

PCMH 3A-1, 3A-2, or 3A-3 Documentation Example
16

PCMH 3B: Identify High-Risk Patients To identify high-risk or complex patients, the practice:
Factors: 1. Establishes criteria and a systematic process to identify
high-risk or complex patients
2. Determines the percentage of high-risk patients in its population.
17

PCMH 3B Scoring 3 points for this element Scoring:
2 factors = 100% 1 factor = 25% 0 factors = 0%
18

PCMH 3B-1 Documentation Example
High-Risk Patient
Definition: Patients with co-morbidities of diabetes and hypertension Process for Identification: Patients diagnosed with diabetes and hypertension will receive a “high-risk” flag in the EHR. Once a month, the Nurse Manager will run a report to determine if there are any patients newly meeting this criteria. If so, the Nurse Manager will designate these patients within the EHR with a “high-risk” flag.
19

PCMH 3B-2 Documentation Example
20

PCMH 3C: Care Management (Must Pass)
The care team performs the following for at least 75 percent of the patients identified in Elements A and B.
Factors: 1. Conducts pre-visit preparations 2. Collaborates with the patient/family to develop an individual care plan,
including treatment goals that are reviewed and updated at each relevant visit 3. Gives the patient/family a written plan of care 4. Assesses and addresses barriers when the patient has not met treatment goals 5. Gives the patient/family a clinical summary at each relevant visit 6. Identifies patients/families who might benefit from additional care
management support 7. Follows up with patients/families who have not kept important appointments
21

PCMH 3C Scoring (Must Pass)
4 points for this element Scoring:
6-7 factors = 100% 5 factors = 75% 3-4 factors = 50% 1 factor = 25% 0 factors = 0%
22

Record Review Workbook 48 patient records
12 high-risk patient records 36 patient records of the
three important conditions (12 patient records x 3 separate conditions)
3C: Care Management (Must Pass)
3D: Medication Management
4A: Support Self-Care Process (Must Pass)
23

Record Review Workbook
24

Record Review Workbook
25

Record Review Workbook
26

Record Review Workbook
27
Record Review Workbook
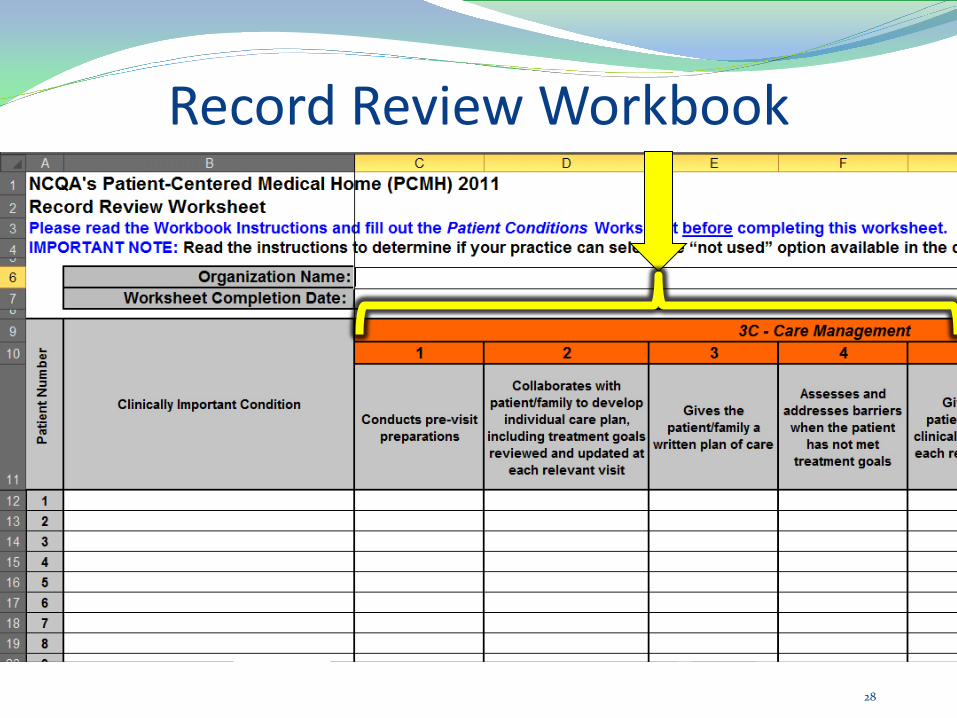
28

Record Review Workbook
29

PCMH 3C: Care Management (Must Pass) The care team performs the following for at least 75 percent of the patients identified in Elements A and B. Factors: 1. Conducts pre-visit preparations 2. Collaborates with the patient/family to develop an individual care plan,
including treatment goals that are reviewed and updated at each relevant visit 3. Gives the patient/family a written plan of care 4. Assesses and addresses barriers when the patient has not met treatment goals 5. Gives the patient/family a clinical summary at each relevant visit 6. Identifies patients/families who might benefit from additional care
management support 7. Follows up with patients/families who have not kept important appointments
30
PCMH 3D: Medication Management The practice manages medications in the following ways: Factors:
1. Reviews and reconciles medications with patients/families for more than 50% of care transitions (Critical Factor)
2. Reviews and reconciles medications with patients/families for more than 80% of care transitions
3. Provides information about new prescriptions to more than 80% of patients/families
4. Assesses patient/family understanding of medications for more than 50% of patients with date of assessment
5. Assesses patient response to medications and barriers to adherence for more than 50% of patients with date of assessment
6. Documents over-the-counter medications, herbal therapies and supplements for more than 50% of patients/families, with the date of updates
31

PCMH 3D Scoring 3 points for this element Scoring:
5-6 factors (including factor 1 [critical factor]) = 100% 3-4 factors (including factor 1) = 75% 2 factors (including factor 1) = 50% Only factor 1 = 25% 0 factors or does not meet factor 1 = 0%
32

Record Review Workbook
33

PCMH 3D: Medication Management The practice manages medications in the following ways: Factors: 1. Reviews and reconciles medications with patients/families for more than 50% of
care transitions (Critical Factor)
2. Reviews and reconciles medications with patients/families for more than 80% of care transitions
3. Provides information about new prescriptions to more than 80% of patients/families
4. Assesses patient/family understanding of medications for more than 50% of patients with date of assessment
5. Assesses patient response to medications and barriers to adherence for more than 50% of patients with date of assessment
6. Documents over-the-counter medications, herbal therapies and supplements for more than 50% of patients/families, with the date of updates
34

PCMH 3E: Use Electronic Prescribing The practice uses e-prescribing system with the following capabilities: Factors:
1. Generates and transmits at least 40% of eligible prescriptions to pharmacies
2. Generates at least 75% of eligible prescriptions (Critical Factor)
3. Enters electronic medication orders into the medical record for more than 30% of patients with at least one medication in their medication list
4. Performs patient-specific checks for drug-drug and drug-allergy interactions
5. Alerts prescribers to generic alternatives
6. Alerts prescribers to formulary status 35

PCMH 3E Scoring 3 points for this element Scoring:
5-6 factors (including factor 2 [critical factor]) = 100% 4 factors (including factor 2) = 75% 2-3 factors (including factor 2) = 50% 1 factor or 2-5 (but not factor 2)= 25% 0 factors = 0%
36

PCMH 3E-1 Documentation Example
37
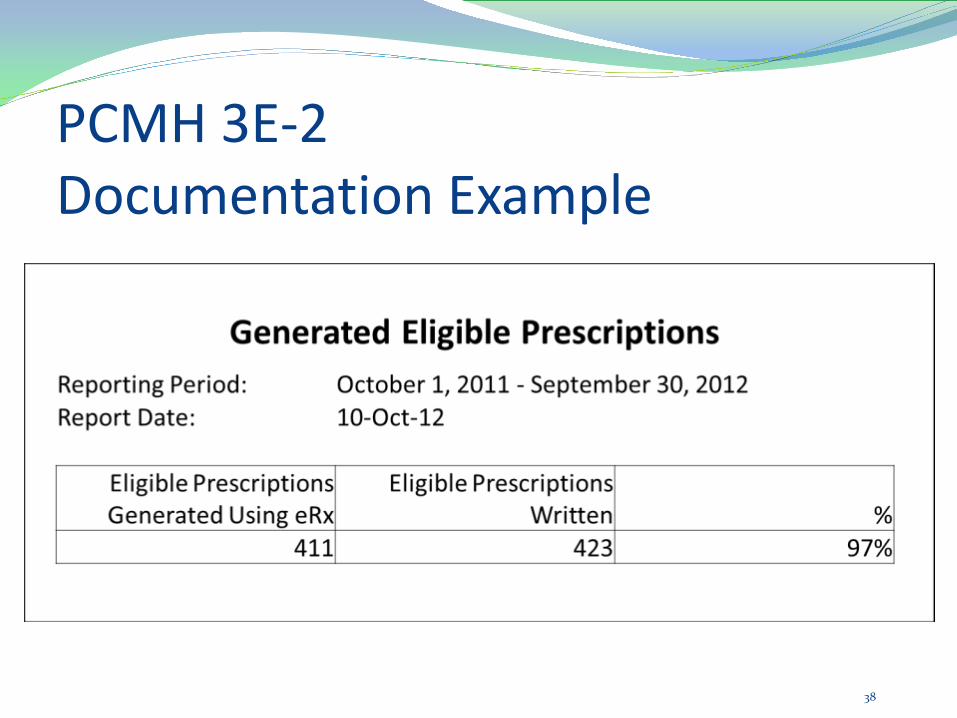
PCMH 3E-2 Documentation Example
38

PCMH 3E-3 Documentation Example
39

PCMH 3E-4 Documentation Example
40

PCMH 3E-5 Documentation Example
41

PCMH 3E-6 Documentation Example
42

PCMH 4: Provide Self-Care Support and Community Resources The practice acts to improve patients’ ability to manage their health by providing a self-care plan, tools, educational resources and ongoing support.
Elements: A. Support Self-Care Process (6 points) (Must Pass) B. Provide Referrals to Community Resources (3 points)
43

The practice conducts activities to support patients/families in self-management:
PCMH 4A: Support Self-Care Process (Must Pass)
Factors:
1. Provides educational resources or refers at least 50% of patients/families to educational resources to assist in self-management
2. Uses an EHR to identify patient-specific education resources and provide them to more than 10% of patients, if appropriate
3. Develops and documents self-management plans and goals in collaboration with at least 50% of patients/families (Critical Factor)
4. Documents self-managements abilities for at least 50% of patients/families
5. Provides self-management tools to record self-care results for at least 50% of patients/families
6. Counsels at least 50% of patients/families to adopt healthy behaviors 44

PCMH 4A Scoring (Must Pass) 6 points for this element Scoring:
5-6 factors (including factor 3 [critical factor]) = 100% 4 factors (including factor 3) = 75% 3 factors (including factor 3) = 50% 1-2 factors or 3-5 (but not factor 3)= 25% 0 factors = 0%
45

Record Review Workbook
46

PCMH 4A: Support Self-Care Process (Must Pass) The practice conducts activities to support patients/families in self-management: Factors:
1. Provides educational resources or refers at least 50% of patients/families to educational resources to assist in self-management
2. Uses an EHR to identify patient-specific education resources and provide them to more than 10% of patients, if appropriate
3. Develops and documents self-management plans and goals in collaboration with at least 50% of patients/families (Critical Factor)
4. Documents self-managements abilities for at least 50% of patients/families
5. Provides self-management tools to record self-care results for at least 50% of patients/families
6. Counsels at least 50% of patients/families to adopt healthy behaviors 47

Practice support patients who need access to community resources:
PCMH 4B: Provide Referrals to Community Resources
Factors:
1. Maintains current resource list covering five (5) community service areas.
2. Tracks referrals provided to patients
3. Arranges for or provides treatment for mental health/substance abuse disorders
4. Offers opportunities for health education and peer support
48

PCMH 4B Scoring 3 points for this element Scoring:
4 factors = 100% 3 factors = 75% 2 factors = 50% 1 factor = 25% 0 factors = 0%
49

PCMH 4B-1 Documentation Example
50

PCMH 4B-2 Documentation Example
51

PCMH 4B-3 Documentation Example Example Policy Excerpt– Behavioral Health Referral Procedures Effective 12/10/2011
1. Evaluation Outpatient: Patients who are assessed by their provider to be in need of Behavioral Health
care will be evaluated by the Behavioral Health Consultant. Based on the outcome of that assessment, the Behavioral Health consultant will either resolve or agree to manage the patient within the clinic or arrange for or refer care to one of the resources listed below.
Inpatient: Following assessment by either their provider or the Behavioral Health Consultant, patients in need of voluntary psychiatric care will have their care coordinated by the care team. Refer to Inpatient Admission procedures for inpatient care coordination. If involuntary psychiatric admission is determined to be necessary, refer to the Involuntary Admission policy and procedure.
2. Referrals Adults and adolescents who are experiencing psychiatric, emotional, behavioral and/or
addictive disorders should be referred to the services provided by ABCD Hospital Center, unless the provider has identified another facility to meet the immediate needs of the patient.
52

PCMH 4B-4 Documentation Example XYZ Community Health Center
Asthma Health Education Program for Adults For 2012, this program is scheduled the first Tuesday of the month,
7-8:30pm
If you have asthma, you may breathe easier when you join our innovative program, which complements your doctor's care. All participants, ages five and older, have access to professional care specialists and educational materials to help them better understand and manage their asthma.
If you participate in the program, we can help you understand:
Your asthma medications How to properly use an inhaler device and peak flow meter How to develop an action plan Understand the danger signs when you have symptoms
For more information, please call 1-888-xxx-9006,
53
PCMH 1: Enhance Access and Continuity The practice has a written process and defined standards, and demonstrates that it monitors performance against the standards for: Elements: *
A. Access During Office Hours (4 points) (Must Pass) B. After-Hours Access (4 points) C. Electronic Access (2 points) D. Continuity (2 points) E. Medical Home Responsibilities (2 points) F. Culturally and Linguistically Appropriate Services (2 points) G. The Practice Team (4 points)
* This webinar focuses only element F. 54

PCMH 1F: Culturally and Linguistically Appropriate Services The practice engages in activities to understand and meet the cultural and linguistic needs of its patients/families by: Factors:
1. Assessing the racial and ethnic diversity of its population
2. Assessing the language needs of its population
3. Providing interpretation or bilingual services to meet the language needs of its population
4. Providing printed materials in the languages of its population
55
PCMH 1F Scoring 2 points for this element Scoring:
4 factors = 100% 3 factors = 75% 2 factors = 50% 1 factor = 25% 0 factors = 0%
56

PCMH 1F-1 Documentation Example
Patients By Ethnicity 1/1/2012 – 12/31/2012
Refused to Report
Hispanic/Latino
Non-Hispanic/Latino
Total Unique Patients
# 124 198 523 845 % 15% 23% 62% 100%
Patients By Race 1/1/2012 – 12/31/2012
Refused to Report White
African American
American Indian or Alaska Native Asian
Hawaiian or Pacific Islander Other
Total Unique Patients
# 56 423 267 45 29 2 23 845 % 7% 50% 32% 5% 3% 0% 3% 100%
57

PCMH 1F-2 Documentation Example
Patients By Language
English Spanish Other Total
# 667 155 23 845
% 79% 18% 3% 100%
58

PCMH 1F-3 Documentation Example
59

PCMH 1F-4 Documentation Example
60

Review of Session Utilize NCQA Standards, Policies and Procedures as a
resource
Ensure the information presented in your documentation is clear and easy to understand
Create and modify documentation for your practice, not for NCQA
Create a plan for completing documentation, prioritize Must Pass Elements
Stay focused on the purpose: to enhance patient care
61

Acknowledgment
This presentation was produced by Qualis Health under a contract with the American Institutes for Research (AIR), with funding from the Center for Medicare & Medicaid Innovation, as part of the Federally Qualified Health Center (FQHC) Advanced Primary Car Practice Demonstration (contract no. GS-10F-0112J, order no. HHSM-500-2011-00147G). AIR would like to thank its partners—the National Association of Community Health Centers, Inc.; Qualis Health; and the MacColl Center for Health Care Innovation at Group Health Research Institute –for assisting with this endeavor.
62