tissue integration of one-stage implants - quintessence publishing!
TRANSCRIPT
Implant Dentistry
Tissue integration of one-stage implants: Three-year results of a prospec-tive longitudinal study with hollow cylinder and hollow screw implantsDaniel Bnser* / Hans-Peter Weber*'! / Urs Brägger*** / Christian Balsiger "
Tissue integration of one-stage, nonsubmerged ITJ implants over a 5-year period is docu-mented. Fifiy-four implants were placed in 38 partially edentulous patients. No implants haddetectable mobility afier a healing phase of at least 3 montlis, and there were no clinical signsof peri-implant infection. Radiographs revealed no peri-implant radiolucencies and all im-plants were in favorable positions for fixed prosthetic restorations. Following completion ofthe prosthetic treatment, all patients were placed in 3-month oral hygiene recall programs.Annual dental e.xamitiations included evaluation of each implant according to fixed criteria.Three years after implatit placement, 51 of 53 implants (96.2%) were evaluated as successful(one patient was lost to the study). Acute peri-implant infections were associated with twoimplants; both were classified as late failures. The results demonstrated that one-stage trans-gingivally healing ITl implants integrate dependably in the tissue and that successful tissueintegration can be maintained for at least 3 years. (Quintessence Int 1994;25;679-686.)
Introduction
Treatment of edentulous or partially edentulous pa-tients with implant-supported prostheses has taken onincreasing significance over the past 10 years. Endos-seous implants, which arc anchored in the maxilla ormandible through direct contact with bone, are pre-ferred today.'"' This phenomenon of direct bone an-chorage is widely known as osseointegraiion.^ Osseoin-tegration of an implant can be achieved dependably ifcertain prerequisites arc fnlfilled. Brânemark et al,'-'"'among others, require closed healing of an implant
Oral Surger>' Clinic, University oí Bern, Frei burgs tr a sse 7,CH-3010 Bern. Switzerland.Department of Periodontology, Harvard University, School ofDental Medicine. 188 Longwood Avenue. Boston. Massachu-setts 02115.Clinic for Crown and Bridge Prosthetics and SynopticDentistry. University of Bern.
under intact mucosa because that impedes epithehalingrowth, development of peri-implant infection, andthe risk of premature stress on the implant. In contrast,ITl (International Team for Oral Implantoiogy) im-plants are characterized, among other things, hy a sin-gle-phase surgical technique and transgingival heal-ing,' Experimental and clinical studies over the past 18years have demonstrated clearly that single-phase ITlimplants osseointegrate dependably in the bone of thejaw,^^
Tollowing clinical experience of tnore than 10 yearswith earlier forms of ITl implants, ITl decided, in 1985,to develop a new implant system. This developmentwas intended to achieve various goals;
1, Improvement of existing TTl implants and integra-tion into a single system
2, Complete standardization of the system as regardsimplant dimensions, instruments, and supplementalprosthetic components
3, Simplification of the clinical procedure4, An increased spectrum of indications for use as
broadly as possible
Quintessence International Volume 25, Number 10/1994 679
implant Dentistry
Table ¡ Implantation of 54 ITI hoiknv screw ( HS) and hollow cylinder (HC) implants in 38 patients
Indication
Mandibular free-end dentureSingle-tooth gaps in
the mandibleMaxillary free-end dentureSingle-tooth gaps in
the maxillaMultiple gaps in
the mandible
Total
No,ofPatienls
1910
52
2
38
No, of HS
300
92
3
44
No, of HC
010
00
0
¡0
Total
3010
92
3
54
Table 2 Prosthetic treatment of 38 patients with fixedsuperconstructions
Indication
Mandibular free-endSingle-tooth gaps iti
the mandibleMaxillary free-endSingle-tooth gaps in
the maxillaMultiple gaps in
the mandible
Total
No, ofC
010
12
0
13
No, ofI
80
3
n
1
¡2
No, ofI-T
150
60
1
JS
Total
2310
102
2
43
C = single crown: I = implant-borne prosthesis; I-T = implanl-loolh-supporied prosthesis.
Two-part hollow cylinder and hollow screw implantsare cnmponents of this new ll'I system, which wasplaced on the market in Europe in 1988 as the BonefitSystem, "' '
The purpose of the present study was to examine thetissue integration of 54 two-part hollow screw and hol-iow cylinder implants over a 3-year period.
Method and materials
Thirty-eight consecutively treated partially edentulotispatients were included in the study. Only patientswhose treatment was initiated between April 1986 andJuly 1987 and who did not have systemic or local com-plications were provided with implants,'- In all, 54 im-
plants were placed, of which 44 were holluw screw typeand 10 were hollow cylinders (Table 1), Nineteen im-plants were placed in the maxilla and 35 in the man-dible: all were inserted by a single operator (DB), usinga technique that was standardized as much as possible.Details of preoperative patient education, the surgicaltechnique, and postoperative care have been publishedelsewhere,'-
Following a healing phase of at least 3 months with-out functional loading, the implants were checked clin-ically and radiographically. Given the existence of suc-cessful tissue integration, the secondary eomponentswere screwed into the implants and the appropriatecrown or fixed partial prostheses were fitted. Whenprosthetic treatment was completed, all patients wereplaced into a 3-month recall program with an oral hygi-enist.
Annual clinical and radiographie checkups were pro-vided by a dentist, during the same month as that oftheimplant procedure, whenever possible. The followinggingival parameters, deseribed previously,''' weremeasured on four surfaces per implant; plaque index(PI)'-*; sulcular bleeding index (SBI)'"*: probing depth(PD)^ ; distance between the implant border and themucosal margin (DIM)'-' : and clinical attachment level(AL),'' Implant mobility was evaluated twice, manual-ly and wilh the Periotest unit (Siemens),'^ Further-more, radiographs that were as standardized as pos-sible were prepared with the aid of the long-cone tech-nique and custom-made bite blocks. The radiographswere evaluated for possible alterations in the peri-im-plant hard tissue changes in the level of marginal bone.For this purpose, a computer-assisted measuring de-vice'^" was used to establish the distance between theimplant border and the first visible implant-bone con-
680 Quintessence International Volume 25, Number 10/1994
Implant Dentistry
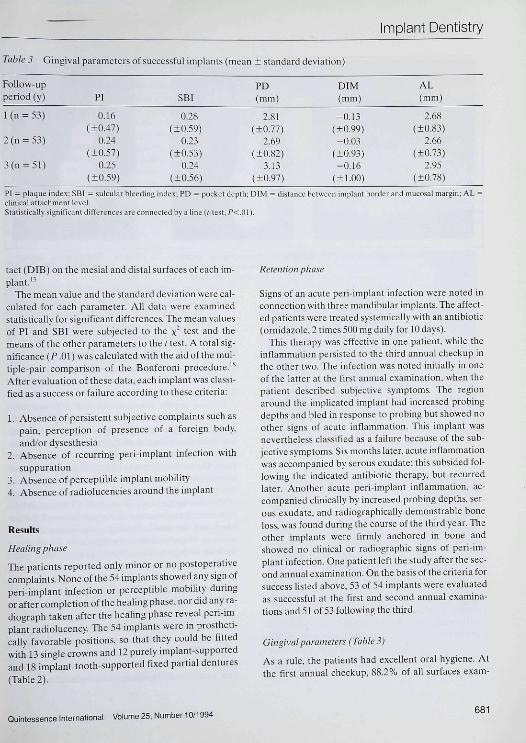
Table 3 Gingival parameters of successful implants (mean + standard deviation)
Follow-upperiod (y) PI SBI
PD( mm ]
DIM(mm)
AL(mm)
1 (n = 53)
2(n = 53)
3(n = 5 l )
0,16(+0,47)
0.24(±0,57)
0,25(±0.59)
0,28(±0,59)
0.23(±0,53)
0,24(±0.56)
2,81(±0,77)
2,69(±0,82)
3,13(±0.97)
-0 ,13(±0.99)-0,03
(±0,93)-0,16
(±1.00)
2.68(±0,83)
2,66(±0,73)
2,95(±0,78)
PI = plaque mdex: SBI = sulcular bleeding inde.x; PD = pocket depth; DIM = distance between implant border and mucosal margin; AL •chnical attachment level.Statistically significant differences are connected by a hne (i-test. /'<,01).
tact (DIB) on the mesial and distal surfaces of each im-plant,'"^
The mean value and the standard devtatiou were cal-culated for each parameter. All data were examinedstatistically for significant differences. The mean valuesof PI and SBI were subjected to the x' test and themeans of the other parameters to the t test, A total sig-tiificance {P .01) was calculated with the aid ofthe mul-tiple-pair comparison of the Bonferoni procedure,'^After évaluation of these data, each implant was elassi-ficd as a success or failure according to these criteria:
1, Absence of persistent subjective complaints such aspain, perception of presence of a foreign body,and/or dysesthesia
2. Absence of recurring pert-implant infection with
suppuration3. Absence of perceptible implant mobility4, Absence of radiolucencies around the implant
Results
Healing phase
TTie patients reported only minor or no postoperativecomplaints. None of the 54 implants showed any sign ofperi-implant mfection or perceptible mobility duringor after completion ofthe healing phase, nor did any ra-diograph taken after the healing phase reveal peri-im-plant radiolucency, Tlie 54 implants were in prostheti-cally favorable positions, so that they could be fittedwith 13 single crowns and 12 purely implant-supportedand 18 implant-tooth-supported fixed partial dentures(Table 2),
Retention phase
Signs of an acute peri-implant infection were noted inconnection wilh three mandibular implants. The affect-ed patients were treated systemically with an antibiotic(ornidazole. 2 times 500 mg daily for 10 days).
This therapy was effective in one patient, while theinflammation persisted to the third annual checkup inthe other two, Tlie infection was noted initially in oneof the latter at the first annual examination, when thepatient described subjective symptoms. The regionaround the implicated implant had increased probingdepths and bled in response to probing but showed noother signs of acute inflammation. This implant wasnevertheless classified as a failure because of the sub-jective symptoms. Six months later, acute inflatnmationwas accompanied by serous exúdate; this subsided fol-lowing the indicated antibiotic therapy, but recurredlater. Another acute peri-implant inflammation, ac-companied clinically by increased probing depths, ser-ous exúdate, and radiographically demonstrable boneloss, was found during the course of the third year. Theother implants were firmly anchored in bone andshowed no clinical or radiographie signs of peri-im-plant infection. One patient left the study after the sec-ond annual examination. On the basis ofthe criteria forsuccess listed above, 53 of 54 implants were evaluatedas successful at the first and second annual examina-tions and 51 of 53 following the third.
Gingival parameters (Table 3)
As a rule, the patients had exeellent oral hygiene. Atthe first annual checkup, 88,2% of all surfaces exam-
Quintessence International Volume25, Number 10/1994681
Implant Dentistry
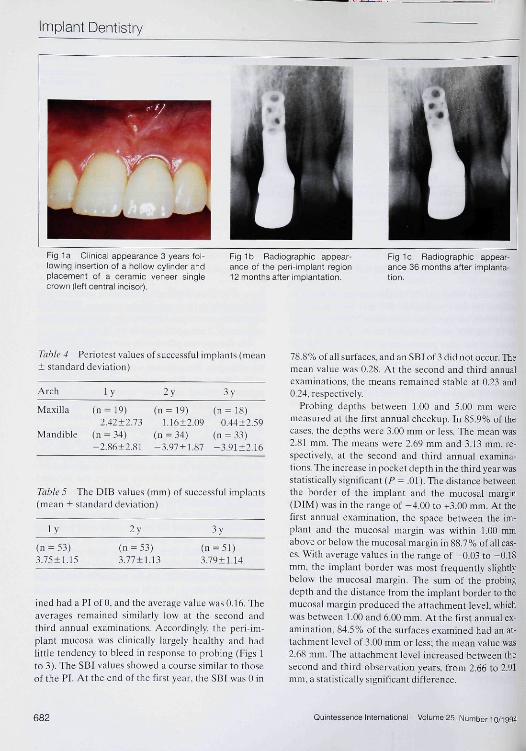
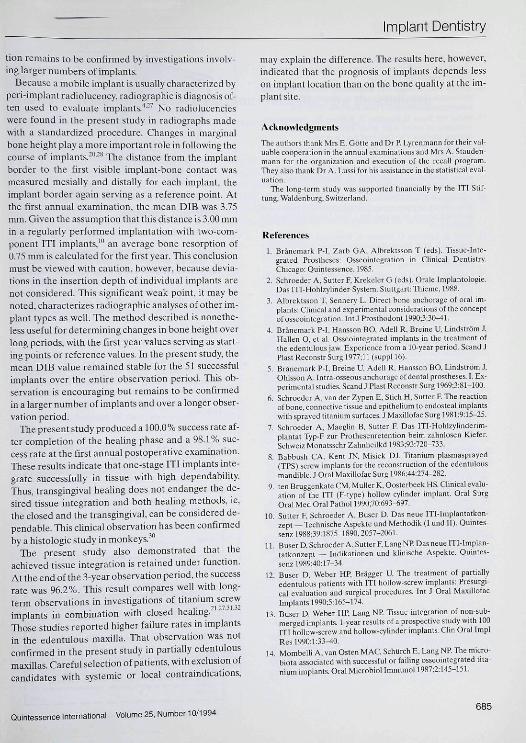
Fig la Clinical appearance 3 years fol-lowing insertion of a hollow cylinder andplacement of a ceramic veneer singiecrown (left central incisor].
Fig 1b Radiographic appear-ance of the peri-implant region12 months after implantation.
Fig lc Radiographic appear-anoe 36 months after implanta-tion.
Table 4 Periotest values of successful implants (mcLin± standard devialion )
Arch l v 3 y
Maxilla (n = 19) (n = 19) (n = 18)2,42+2,73 I.16±2,O9 0,44±2,59
Mandible (ti = 34) (n = 34) (ti = 33)-2.S612.S1 -3,97 + 1,87 -3,91±2,16
Table 5 The DIB values (mm) of successful implants(mean + standard deviation)
l v 2v 3v
{n = 53)3.75±1.15
(n = 53)3,77 + 1,13 3,79+1,14
inedhad a PI of Û. and the average value was 0,16, Theaverages remained similarly low at the second andthird annual examinations. Accordingly, the peri-im-plant mucosa was clinically largely healthy and hadlittle tendency to bleed in response to prohing (Figs 1to 3), The SBI values showed a course similar to thoseof the PI, At the end of the first year, the SBI was 0 in
7S,8% of all surfaces, and an SBI of 3 did not occur. Themean value was 0,28. At the second and third annualexaminations, the means remained stable at 0,23 and0.24, respectively.
Probing depths between 1,00 and 5,00 mtn weremeasured at ihe first annual checkup. In 85,9% of thecases, the depths were 3.00 mm or less. The mean was2,81 mm. The means were 2,69 mm and 3,13 mm, re-spectively, at the second and third annual examina-tions. The increase in pocket depth in the third year wasstatistically significant (P = ,01 ), The distance betweenthe border of the implant and the mueosal margin(DIM) was in the range of -4,00 to +3.00 mm. At thefirst annual examination, the space between the im-plant and the mueosal margin was within 1,00 mmabove or below the mueosal margin in 8S,7% of all cas-es. With average values in the range of -0.03 to -0,18mm, the implant border was most frequently slightlybelow the mucosa! margin. The sutii of the probingdepth and the distance from the implant border to themueosal margin produced the attachment level, whichwas between 1,00 and 6,00 mm. At the first annual ex-amination. 84,5% of the surfaces examined had an at-tachment level of 3,00 mm or less; the mean value was2,OS mm. The attachment level increased between thesecond and third observation years, from 2,66 to 2.91mm, a statistically significant difference.
682 Ouintessence International Volume 25, Number 10/t994
Implant Dentistry
Implant mobilily (Table 4)
All 54 implants, including the two failures, showed an-kylotic anchorage in bone, without perceptible mobil-ity on manual examination. The supplemental Perio-test measurements produced values in ihe range of-8.00 to +8.ÛU. The values for the 34 mandibula^ im-plants were predominantly negative, in the range of-8.00 to 0.00, with a mean of -2.2S at the first annualcheckup. The 19 tiiaxillary implants had significantlyhigher Petiotest values; ihe mean after 1 year was+2,42. The Periotest values tended lo decrease over thecourse of time, with mean reduetions after 3 years of—3.91 for mandibular implants and +0.44 for maxillaryimplants.
Radio graphic fm dings
Radiographs of each implant revealed no signs of peri-implant radiolucency over the entire 3-year period (seeFigs 1 to 3). The mean DIB was 3.73 mm in the 53 suc-cessfull implants at the end of the first year (Table 5).Mean DIB values of 3.75 (53 implants) and 3.79 mm (51implants) were calculated after years 2 and 3, respec-tively.
Discussion
Ciearly defined cnteria of success art.- demanded todayfor the evaluation of implants in long-term clinicalstudies. An initial attempt to define such criteria wasmade at the Harvard Consensus Conference in 1978.'''Later, Albrektsson et al.-** proposed even stricter crtte-ria for success. These served as the basis for the criteriafor success that have been established for long-termstudies wtth ITI implants.'-' The present report de-scribes 3-year results of a prospective long-term studyin partially edentulous patients. Detailed clinical andradiographie results obtained in the first 38 consecu-tively treated patients, in whom a total of 54 implantswere placed, are provided. Ali 54 implants (100%)showed successful tissue integration, with no early fail-ures. After a 3-year observation penod, two implantsshowed acute peri-implant infection and were classi-fied as late failures. One patient with a single implantdropped oui ofthe study after the second annual exam-ination. Tlie remaining implants fulfilled the criteria es-tablished for success.
Evaluation of the suceessfully integrated implantsrevealed clinically healthy peri-implant soft tissue with
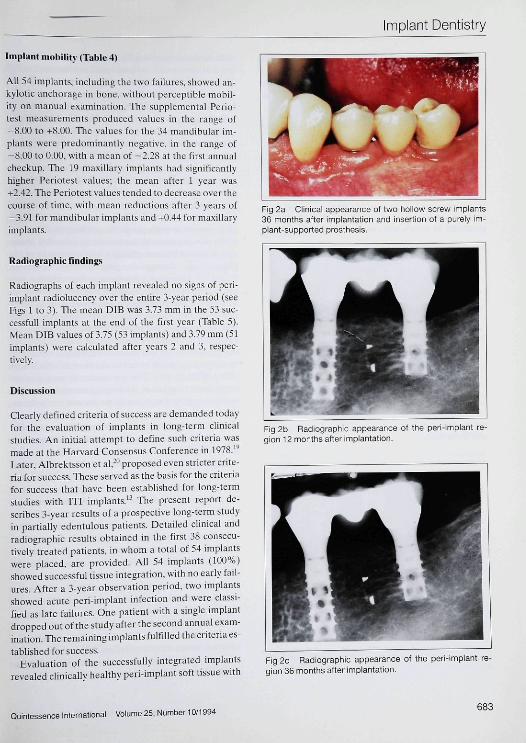
Fig 2a Clinical appearance of two hollow screw implants36 months after implantation and insertion of a purely im-plant-supported prosthesis.
Fig 2b Radiographie appearance of the peri-implant re-gion 12 months after implantation.
Fig 2c Radiographie appearance of the peri-implant re-gion 36 months after implantation.
Quintessence International Volume 25, Number 10/1994683
Implant Dentistry
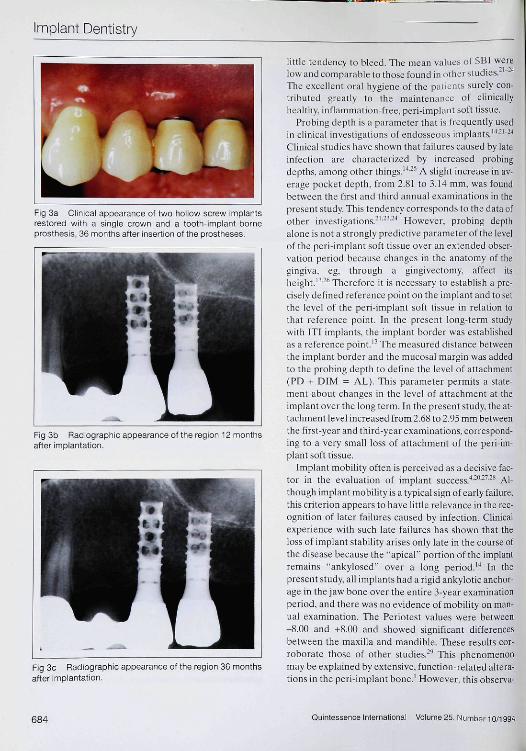
Fig 3a Clinical appearance of two tiollow screw implantsrestored with a single crown and a tooth-implant-borneprosthesis, 36 months after insertion ol the prcstheses.
Fig 3b Radiographic appearance of the region 12 monthsafter implantation.
Fig 3c Radiographic appearance of the region 36 monthsafter implantation.
little tendency to bleed. The mean values of SBI werelow and comparable to those found in other studies, '""Tlie excellent oral hygiene of the patients surely con-tributed greatly to the maintenance of clinicallyhealthy, inflammation-free, peri-implant soft tissue.
Probing depth is a parameter that is frequently usedin clinical investigations of endosseous implants,'''' '" ''Clinical studies have shown that failures caused hy lateinfection are characterized by increased probingdepths, among other things,'''^'' A slight increase in av-erage pocket depth, from 2,81 lo 3,14 mm, was foundbetween ihe first and third annual examinations in thepresent study, Tliis tendency corresponds to the data ofother investigations,"'•"•'•"'' However, probing depthalone is not a strongly predictive parameter ofthe leveiof the peri-implant soft tissue over an extended obser-vation period beeause changes in the anatomy of thegingiva, eg, through a gingivectomy, affect itsheight,'-*-^ Therefore it is necessary to establish a pre-cisely defined reference point on the implant and to setthe level of the peri-implant soft tissue in relation tothat reference point. In the present long-term studywith ITl implants, the implant border was establishedas a reference point,'''The measured distance betweenthe implant border and the mucosal margin was addedto the prohing depth to define the level of attachment(PD -f DIM = AL). This parameter permits a state-ment about changes in the level of attachment at theimplant over the long term. In the present study, the at-tachment level increased from2,6ii to 2,95 mm betweenthe first-year and third-year examinations, correspond-ing to a very small loss of attachment of the peri-im-plant soft tissue.
Implant mobility often is pereeived as a decisive fac-tor in the evaluation of implant s ucee s s.""- "" - * Al-though implant mobility is a typical sign of early failure,this criterion appears to have little relevance in the rec-ognition of later failures caused by infeetion. Clinicalexperience with such late failures has shown that theloss of implant stability arises only late in the course ofthe disease because the '•apical" portion ofthe implantremains "ankylosed" over a long period,'"' In thepresent study, all implants had a rigid ankylotic anciior-age in the jaw bone over the entire 3-year examinationperiod, and there was no evidence of mobility on man-ual examination. The Periolest values were between-8.00 and 4-8,00 and showed significant differencesbetween the maxilla and mandible. These results cor-roborate those of other studies,'" This phenomenonmay be explained by extensive, function-related altera-tions in the peri-implant bone,' However, this observa-
684 Quintessence International Volume 25, Number 10/1994
Implant Dentistry
fion remains to be confirmed by investigations involv-ing larger numbers of implants.
Because a mobile implant is usually characterized byperi-implant radiolucency, radiographie is diagnosis of-ten used to evaluate implants,"'-'' No radiolucencieswere found in the present study in radiographs madewith a standardized procedure. Changes in marginalbone height play a more important role in following thecourse of implants, "•'•' The distance from the implantborder to the first visible implant-bone contact wasmeasured mesially and distally for each implant, theimplant bOTder again serving as a reference point. Atthe first annual e.xamination, the mean DIB was 3,75mm. Given the assumption that this distance is 3,00 mmin a regularly performed implantation with two-com-ponent ITI implants.'" an average bone résorption of0,75 mm is calculated for the first year. This conclusionmust be viewed with caution, however, because devia-tions in the insertion depth of individual implants arenot considered. This significant weak point, it may benoted, characterizes radiographie analyses of other im-plant types as well. The method described is nonethe-less useful for determining changes in bone height overlong periods, with the first-year values serving as start-ing points or reference values. In the present study, themean DIB value remained stable for the 31 successfulimplants over the entire observation period. This ob-servation is encouraging but remains to be confirmedin a larger number of implants and over a longer obser-vation period.
The present study produced a 100,0% success rate af-ter completion of the healing phase and a 98.1% suc-cess rate at the first annual postoperative examination.These results indicate that one-stage ITI implants inte-grate successfully in tissue with high dependability.Thus, transgingiva] healing does not endanger the de-sired tissue integration and both healing methods, ie,the closed and the transgingival, can be considered de-pendable. This clinical observation has been confirmedby a histologie study in monkeys.
The present study also demonstrated that theachieved tissue integration is retained under function.At the end of the 3-year observation period, the successrate was 96.2%, ITiis result compares well with long-term observations in investigations of titamum^ s cr ewimplants in combination with dosed heaUng, '-Those studies reported higher failure rates in implantsin the edentulous maxilla, ITiat observation was notconfirmed in the present study in partially edentulousmaxilias. Careful selection of patients, with exclusion ofcandidates with systemic or local contraindications,
may explain the difference. The results here, however,indicated that the prognosis of implants depends lesson implant location than on the bone quality at the im-plant site.
Acknowledgments
The authors Ihank Mrs E, Götle and Dr P, Lyrenmann for Iheir val-uable cooperation in Ihe annual examinations and Mrs A, Slauden-mann for the organization and execulion of the retail program.They aiso thank Dr A, Lussi for his assislanec in the stalistical eval-uation.
The long-lerm study was supported financially by the IT! Stit-lung, Waldenburg, Swit2erland,
References1, Bränemark P-l, Zarb GA, Albrektsson T (eds), Tisstie-Inie-
grated Proslheses; Osseointegralion in Qinical Dentislry.Chicago: Quintessence, 19S5.
2, Scbroeder A, Sutter F, Krekeler G (eds). Orale Implantologie,Das ITl-Hohlzyhnder-Syslem, Stuttgart: Tliieme, 19K8,
2. AlbreklEson T, Sennery L, Direct bone anchorage of oral im-plants: Clinical and experimental coiisideiationsof the conceptofosseointegration. Int JProsthodont I990-,3:30-41,
4, Bränemark P-I, Hansson BO, Adell R, Breine U, Lindström J,Hallen O, et al, Osseointegrated implanis in the treatment ofIhe edentulous jaw. Experience from a lÜ-year period. Scand JPlast Reconstr Surg 1977;11 (suppi 16),
5, Brânemark P-l, Breine U, Adcll R, Hansson BO, Lindström J,Ohlsson A. Intra-osseoui anchorage uf dental proslheses, 1, Ex-perimental studies, Scand J Plast Reconstr Surg l%9;3:St-10O,
6, Schroeder A, van der Zypen E, Stich H, Sutter F, The reactionof bone, connective tissue and cpithehum lo endosteal implantswith sprayed titanium surfaces, J Maxillofac Surg 1981:9:15-25.
7, Schroeder A, Maeglin B, Sutter F Das ITI-Hohlzylinderim-plantal Typ-F zur Pro thesenre ten tion beim zahnlosen Kiefer,Schwei?,MonatsschrZahnheilkd 1983:93:720-733.
8, Babbush CA, Kent JN, Misiek DJ, Titanium plasmasprayed(TPS) screw implanis for the reconstruction of the edentulousmandible, J Orai Maxillofac Surg 1986;44:274-2K2,
9, ten Bruggenkate CM, Müller K, Oosterbeek HS. Clinical evalu-ation ol the ITI (F-type) hollow cylinder implant. Oral SurgOral Med Oral Pathol 1990:70:693-697,
10, Sutter F Schroeder A, Buser D, Das neue ITI-Implaiitatkon-zept — Technische Aspekte und Methodik (I und II¡. Quintes-senz 1988,39:1875-1890,2057-2061,
11, Buser D, Schroeder A, Suiter F, Lang NP Das neue ITl-Implan-lalkonzept — Indikationen und klinische Aspekte, Ouintes-senzl989;40:17-34.
12, Buser D, Weber HP, Brägger U, The treatmeni of partiallyedentulous patients with ITI hollow-screw implants: Presurgi-cal evaluation and surgical procedures, Int J Oral MaxillofacImplants 1990;5:165-174,
13, Buser D, Weber HP. Lang NP Tissue integration of non-sub-merged implants, 1-year results of a prospective study with 100ITI hollow-screw and hollow-cylinder implants, Cliti Oral ImplRes 1990:1:33-40.
14, Mombelli A, van Osten MAC, Schurch F-, Lang NP. The micro-biota associated wilh successful or failing osseoinlegrated tila-nium implants. Oral Microbionmmunon987:2:145-151.
Quintessence International Volume 25, Number 10/1994685
Implant Dentistry
15, Schulte W. Messung des Da tnpfungs verhalten s cnossaler Im-plantate mit dem Periotestverfaliren, Vorläufige Mitteilung. ZZahnärztl Implantol 1986;2:22.
16, Jeffcoat MK, Wilhams RC, Relationship between linear andarea measurements of radiographie bone levels utilizing simplecomputerized techniques. J Dent Res 1984:19:191-1 W,
17, Weber HP, Buser D. Fiorellini JP, Williams RC, Radiographicevaluación ot crestal hone levels adjacent to non-submergedtitanium implants. Clin Oral Impl Res (in press),
18, Wilkinson L, SYSTAÏ: "ITie system for statistics, Evanston, IL:Systat,1989,
19, Schnitman PA, Sehulman LB. Recommendations of the Con-sensus Development Conferenee on Dental Implants, J AmDent Assoc 1979:98:373-377, .
20, Alhrektsson T, Zarb G, Worthington P, Eriksson AR, The long-term efficacy of currently used dental implants, A review andproposed criteria of success, lut J Oral Maxillotae Implants1986;l:ll-25,
21, Adetl R. Lekholm U, Rockier B, Brânemark P-l. Lindhc J,Eriksson B, et al. Marginal tissue reactions at osseointegratedtitanium fixtures. I. A 3-year longitudinal prospective study, IntJ Oral Maxillofac Surg 19S6;15:39-52.
22, Lekholm U, Adell R, Lindhe J, Brânemark P-I, Eriksson R.Rockier B, et al. Marginal tissue reactions at osseointegrated ti-tanium fixtures, I I , A eros5-sectional retrospective study, Int JOral Maxillofac Surg 1986;15:53-6I.
23, Cox JE Zarb G A, The longitudinal clinical efficacy of osseoin-tegrated implants: A 3-year report, Int J Ora! Maxillofac Im-plants ]9S7;2:91-1ÜO.
24, Strub JR. Rohner D, Schärer P Die Versorgung desLüekengebisses mit implantatzahn getragen en Brücken, ZZahnärztl Implantol 19K7;3:242-254,
25, Becker W, Becker BE, Newman MGT. Nyman S, Clinical andmicrobiological findings that may contribute to dental implantfailure. Int J Oral Maxillofac Implants 1990:5:31-38,
26, Orton GS, Steele DL, Wolinsky LE, The dental professional'srole in monitoring and maintenance of tissue-in te grated pros-theses, J Oral Maxillofac Implants 1989;4:305-31U,
27, Adell R, Lekholm U. Rockier B, Brânemark P-I, A 15-yearstudy of osseointegrated implants in the treatment of the eden-tulous jaw, Int J Oral Surg 1981:10:387^16.
28, Smith DE, Zarb G A. Criteria for success of osseointegrated en-dosseous implants, J Prosthet Dent 1989;62:567-572.
29, d'Hoedt B, Schramm-Scherrcr B, Der Periotestwert bei enos-salen Implantaten. Z Zahnärztl Implantol 19aS:4:89-95.
30, Gotfredsen K. Rostrnp E, Hjorting-Hansen E, Stoltze K,Budtz-Jorgensen E, Histological and histomorphometricalevaltiation of tissue reaetions adjacent to endosteal implants inmonkeys. Clin Orai Impl Res 199l;2:31)-37,
31, Albrektsson T, Dahl E, Enhom K, et al, Osseointegrated oralimplants, A Swedish multicenter study of 8139 consecutively in-serted Nobelpharma implants. J Periodontol 1988;59:287-2%,
32, Jaffin RA, Berman CL, The excessive loss of Brânemark fix-tures in type IV bone: A 5-year analysis. J Periodontol1991;62:24, D
ISBN 1-B5097-026-295pp;172illus(13Bincolor):
US ses
Aesthetic Dentistry WithIndirect ResinsHoward Stean
Drawing upon his vast experience in restorative dentistry,Dr Stean has developed techniques using SR Isosit/Con-cept materials to treat a wide range of patients. Detailedin this textbook are his case reports, techniques, atidresults—all profusely illustrated with a ward-winning pho-tographs. His techniques apply to not only the Isosit/Concept system hut also to other indirect resin systems.
Valuable both as an ititroduction to the indirect resinsystem and as a source for additional techniques.
Contents include: Indirect Resins and Inlays, AestheticColour Rendering, Onlay Modifications, Intra-coronalModifications, Crown and Bridgework, Laminate Ve-neers, Restoration of Endodonticaliy Treated Teeth, Indi-rect Resin Materials in Adhesive Bridgework, and ImplantDentistry,
CALL OR FAX TO ORDER: Tel: mm 621-0387 or(708) 682-3223; Fan: (7081 6S2-328H
or fill out :hc order form iiDd send to Quintessence Publishing Co,Inc, 551 N, Kimberly Drive, Carol Stream, I L 6D1SS-IN81
I Send me copies of (8802) Aesthelic Denlislry 'with Indireel Resins at tIS 168/copy,
686
City
Telephone.
. Z i p .
i I General Practitioner I 1 Specialist[ ] Bill me, including shipping & handling[ ] Charge to my credit card plus shipping & handlingI I Visa/MasterCard [ ] American Express
Carxl no.
Signature
Esp,
Pncci bubjccc 10 chjni^c wiUiuul niiLce, Al l sales are finiil, Shipping andhandling ehaiges will be added » all uriluri. For tllitwis and Canadianr ^ idcnrs, s les lii> will he adiLcd if applicable, Pnyntcni niu.ivi bñ inwk in