tina dang aldana, m.a., o.d., f.a.a.o. 28 october …...tina dang aldana, m.a., o.d., f.a.a.o. 28...
TRANSCRIPT
Tina Dang Aldana, M.A., O.D., F.A.A.O.
28 October 2018
Aarhus, Denmark
COPE 53554-NO
Traumatic Brain Injury
A traumatically induced structural injury or physiological disruption of brain function as a result of an external force, that is indicated by newonset or worsening of at least one of the following clinical signs, immediately following the event:
• Any period of loss of or decrease of consciousness, observed orself-reported (LOC)
• Any alteration in mental status (confusion, slowed thinking, disorientation, “seeing stars”) (AOC)
• Any loss of memory for events immediately before or after the injury (PTA)
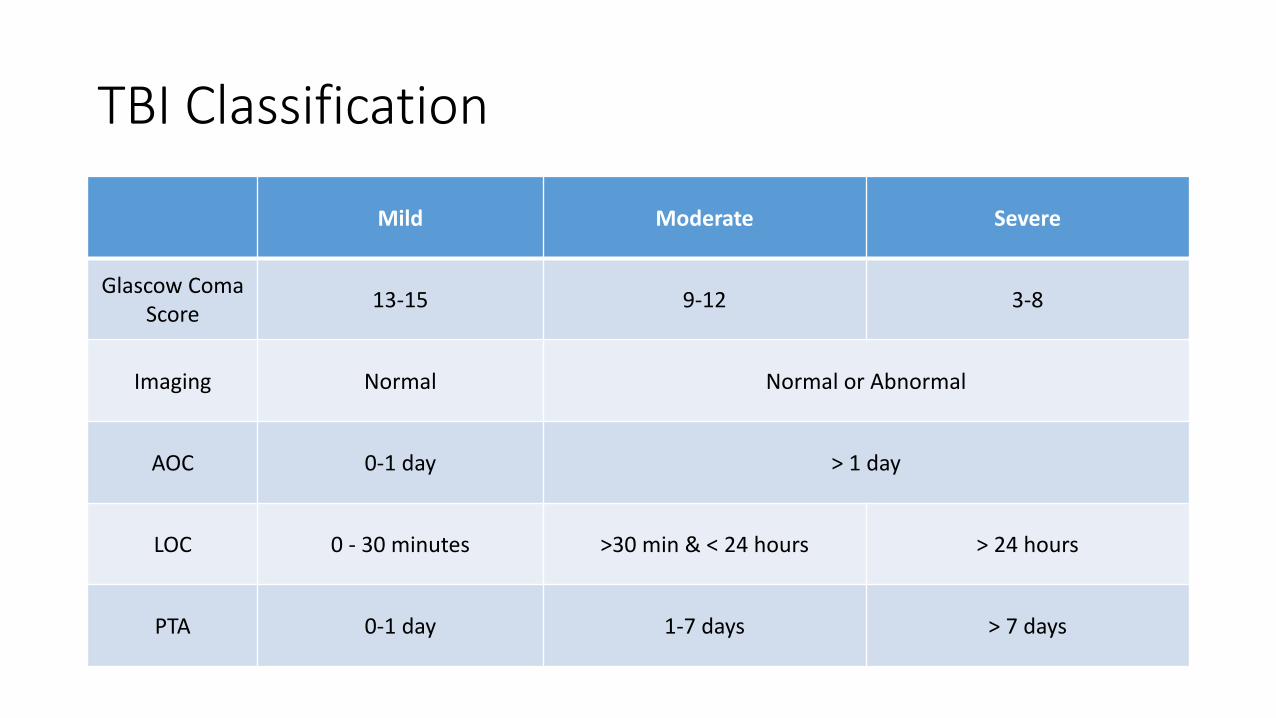
TBI Classification
Mild Moderate Severe
Glascow Coma Score
13-15 9-12 3-8
Imaging Normal Normal or Abnormal
AOC 0-1 day > 1 day
LOC 0 - 30 minutes >30 min & < 24 hours > 24 hours
PTA 0-1 day 1-7 days > 7 days
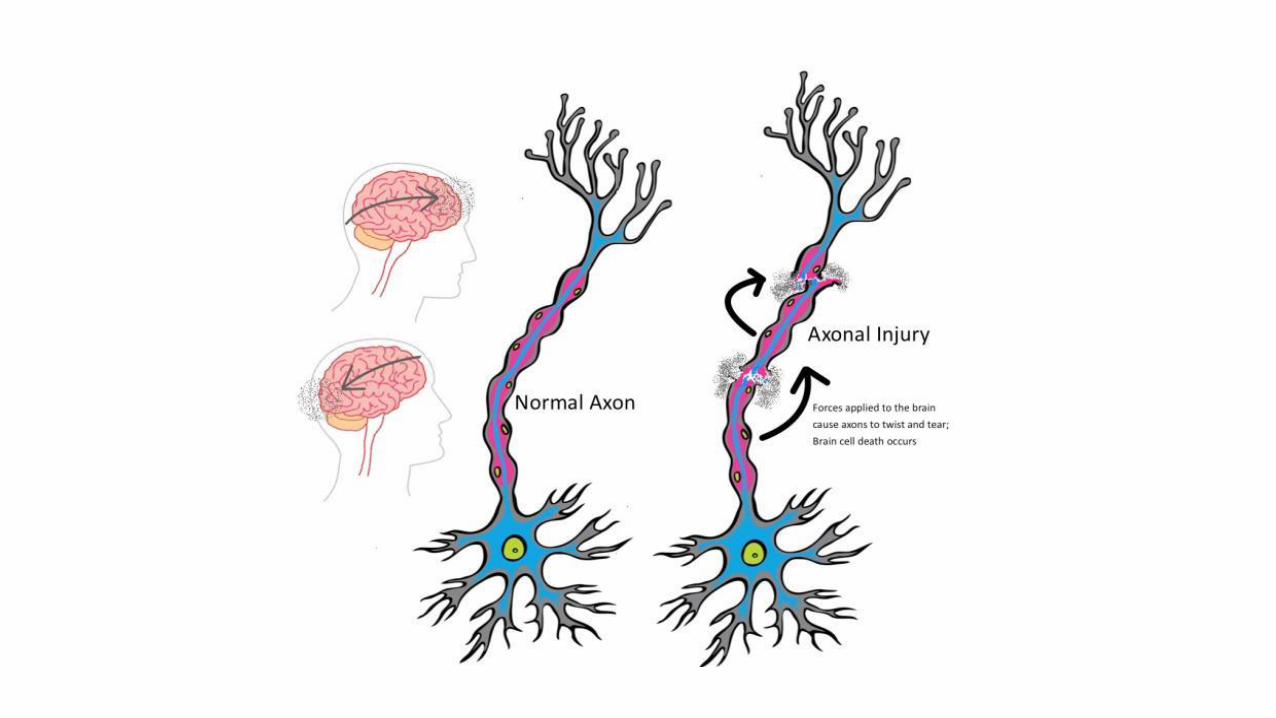
Diffuse Axonal Injury
• Sudden acceleration-deceleration of the head
• Gray matter density vs white matter density
• Shearing of neuronal axons which traverse the junction of gray and white matter
• Damage not visible on standard imaging CT/MRI
Diffuse Axonal Injury
• 2 Phases of Injury
• Primary injury: Axons undergoing shearing forces are stretched at the moment of impact
• Secondary (delayed) phase: Bulb formations Stretched axons undergo swelling and rupture
• Degeneration process and Clinical symptoms may take up to 2 years to fully develop
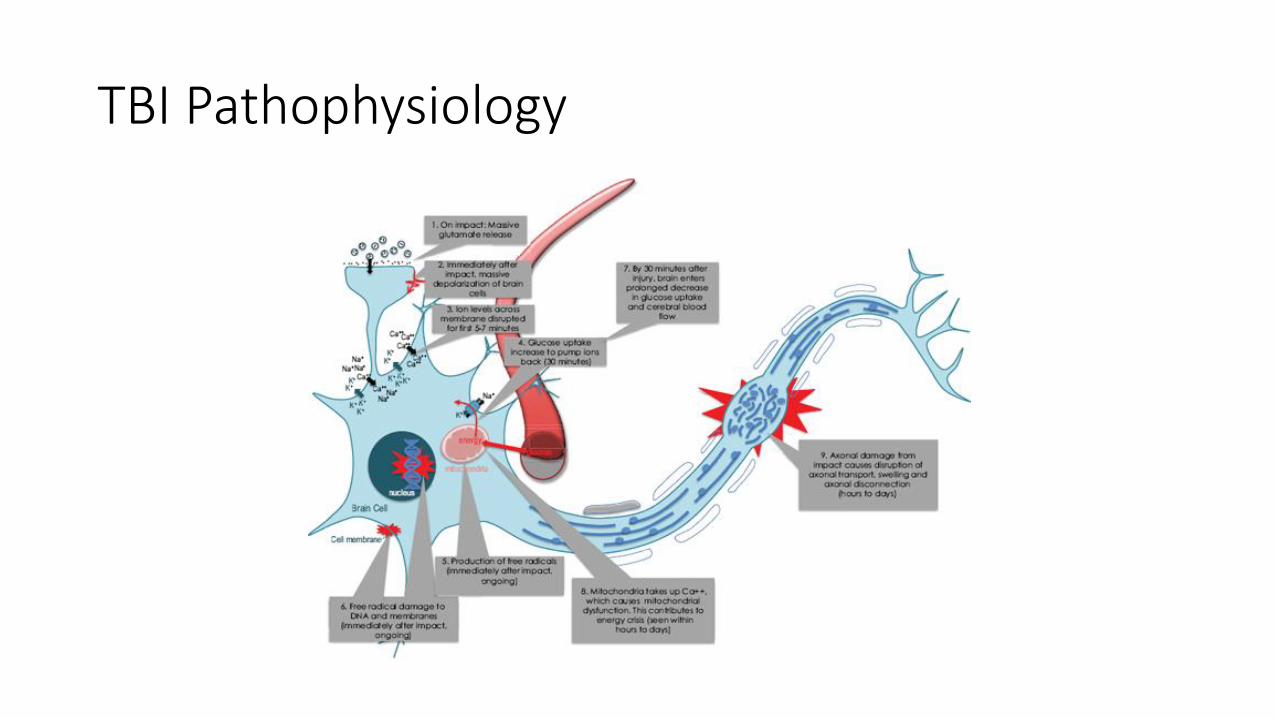
TBI Pathophysiology
Multiple mTBI
• Increased symptoms and lingering effects are reported from subsequent concussions when they occur close in time
• Blast concussions tend to be repeated and have more lingering effects
• Post trauma deficits often lead to subsequent concussions
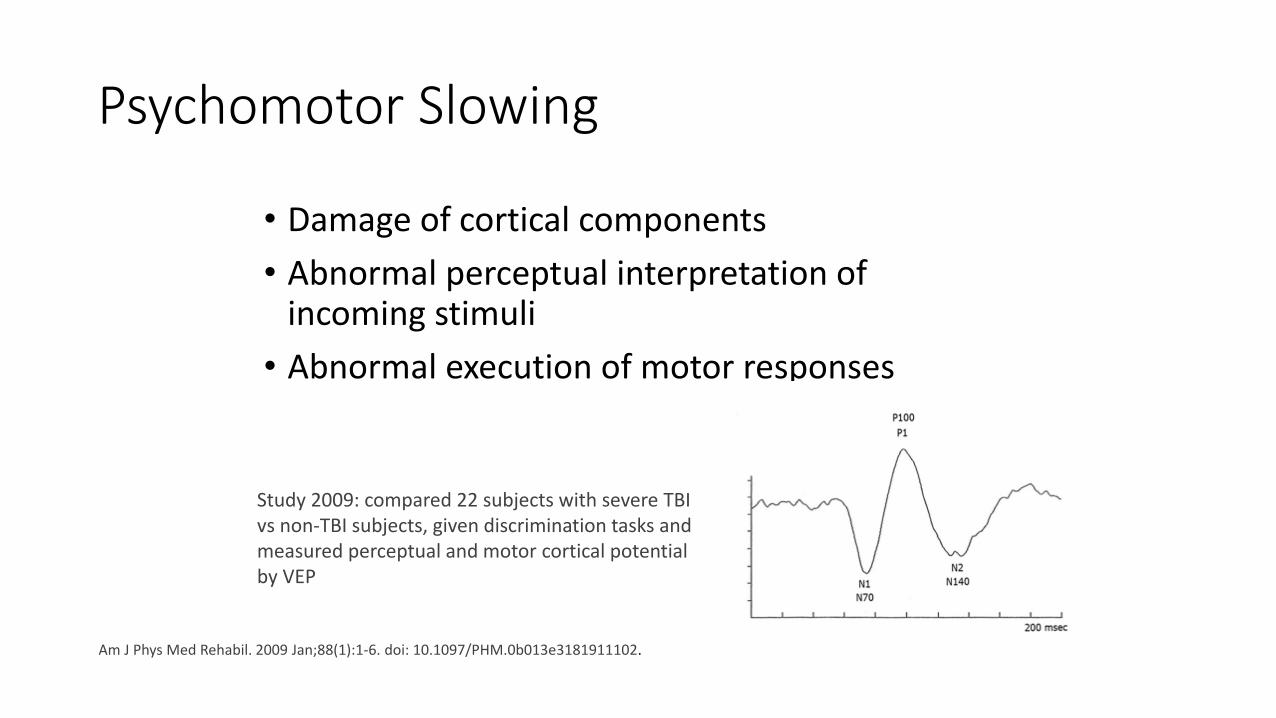
Psychomotor Slowing
• Damage of cortical components
• Abnormal perceptual interpretation of incoming stimuli
• Abnormal execution of motor responses
Study 2009: compared 22 subjects with severe TBI vs non-TBI subjects, given discrimination tasks and measured perceptual and motor cortical potential by VEP
Am J Phys Med Rehabil. 2009 Jan;88(1):1-6. doi: 10.1097/PHM.0b013e3181911102.
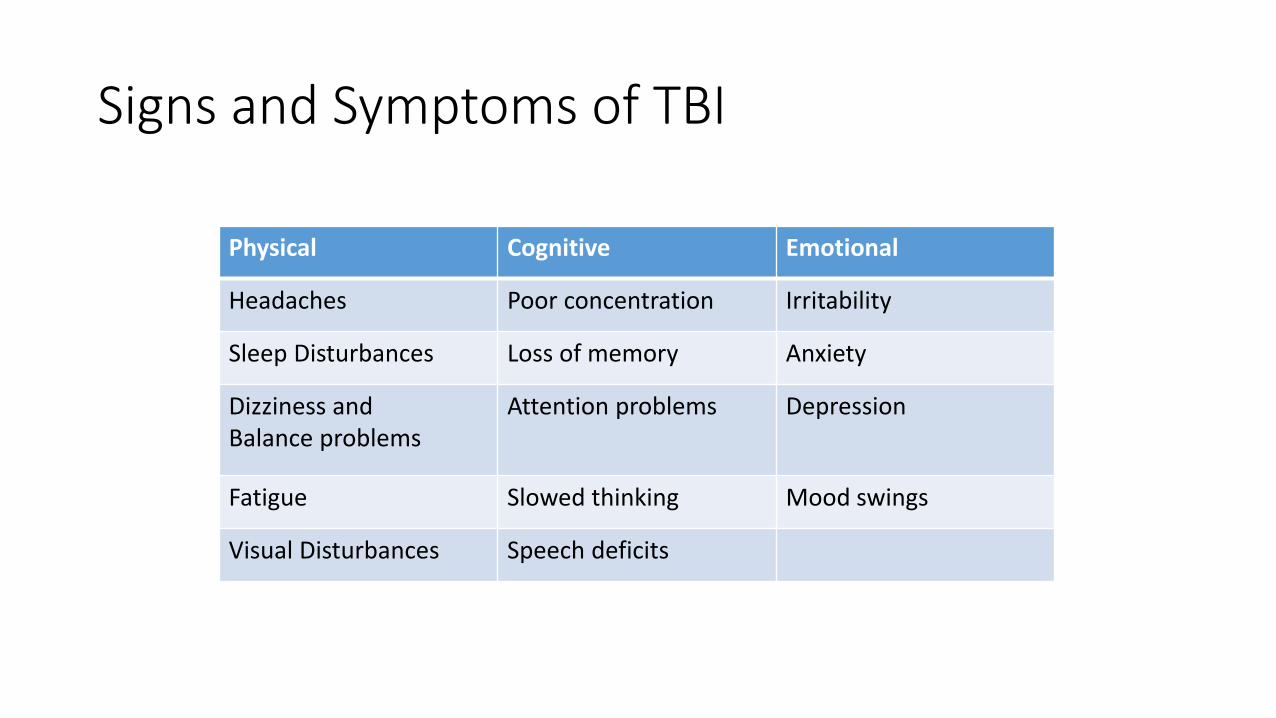
Signs and Symptoms of TBI
Physical Cognitive Emotional
Headaches Poor concentration Irritability
Sleep Disturbances Loss of memory Anxiety
Dizziness and Balance problems
Attention problems Depression
Fatigue Slowed thinking Mood swings
Visual Disturbances Speech deficits
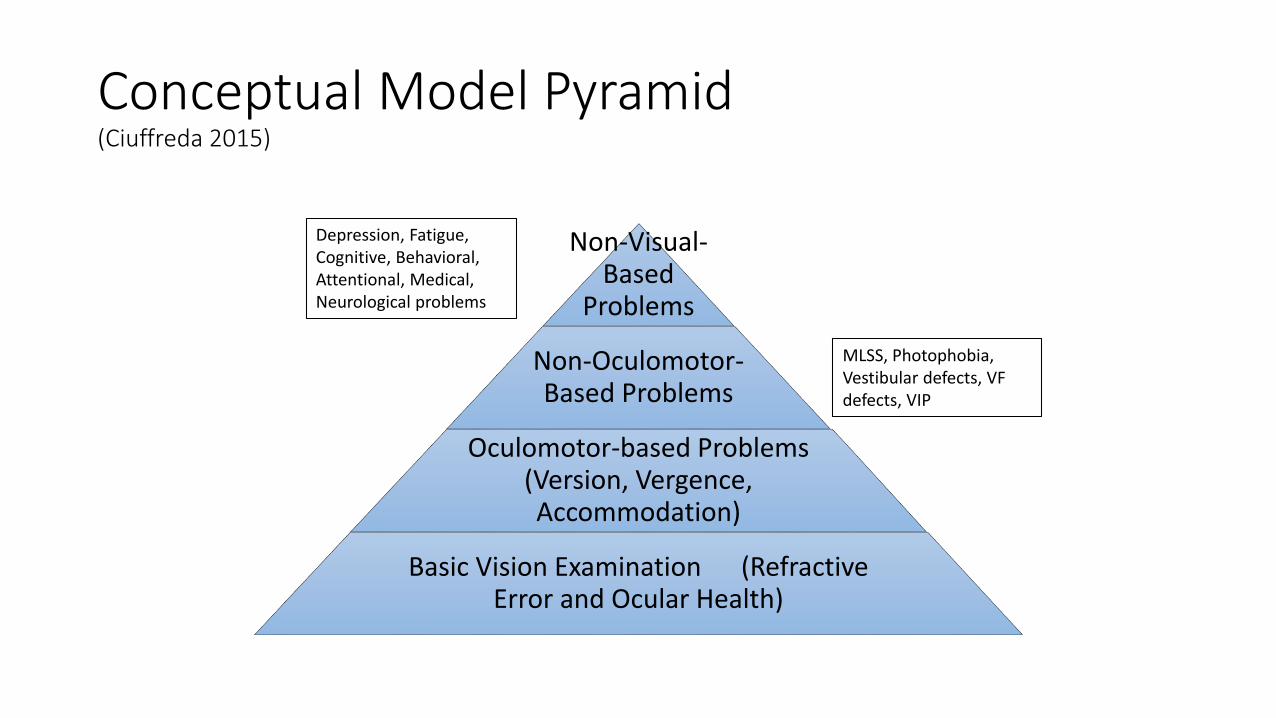
Conceptual Model Pyramid(Ciuffreda 2015)
Non-Visual-Based
Problems
Non-Oculomotor-Based Problems
Oculomotor-based Problems (Version, Vergence, Accommodation)
Basic Vision Examination (Refractive Error and Ocular Health)
MLSS, Photophobia, Vestibular defects, VF defects, VIP
Depression, Fatigue, Cognitive, Behavioral, Attentional, Medical, Neurological problems

Hierarchy of Vision
SubcorticalInformationprocessed First and faster
20%Peripheral Retinal
Unconscious Vision (non-planned reflexes)
Proprioception
Vestibular
CorticalInformationprocessed Secondary and Slower
80 %Central RetinalVisual Cortex
Subconscious Vision (learned reactions)
Peripheral Awareness
Organization
Conscious Vision “Eye Sight”Visual attention
Post Trauma Vision Syndrome
• PTVS sensory mismatch between subcortical and subconscious cortical levels
• Dysfunctional peripheral nonvisual pathways interfere with central cortical inputs
• Causing problems of central attention and spatial awareness
• Mal-adaptations can cause alterations in postural alignment and balance
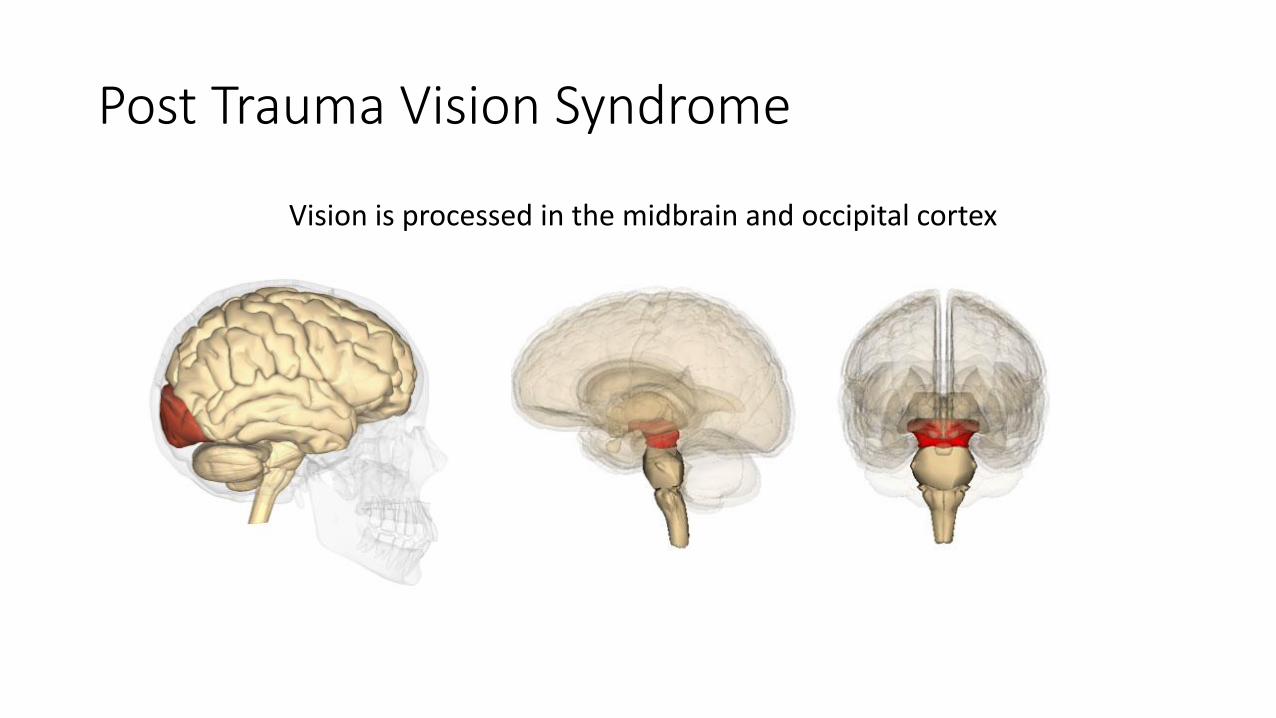
Post Trauma Vision Syndrome
Vision is processed in the midbrain and occipital cortex
Post Trauma Vision Syndrome
• Disruptions in nonvisual pathways have an impact on patients ADLs
• Perceived distortions affect the nervous system: concentration and performance
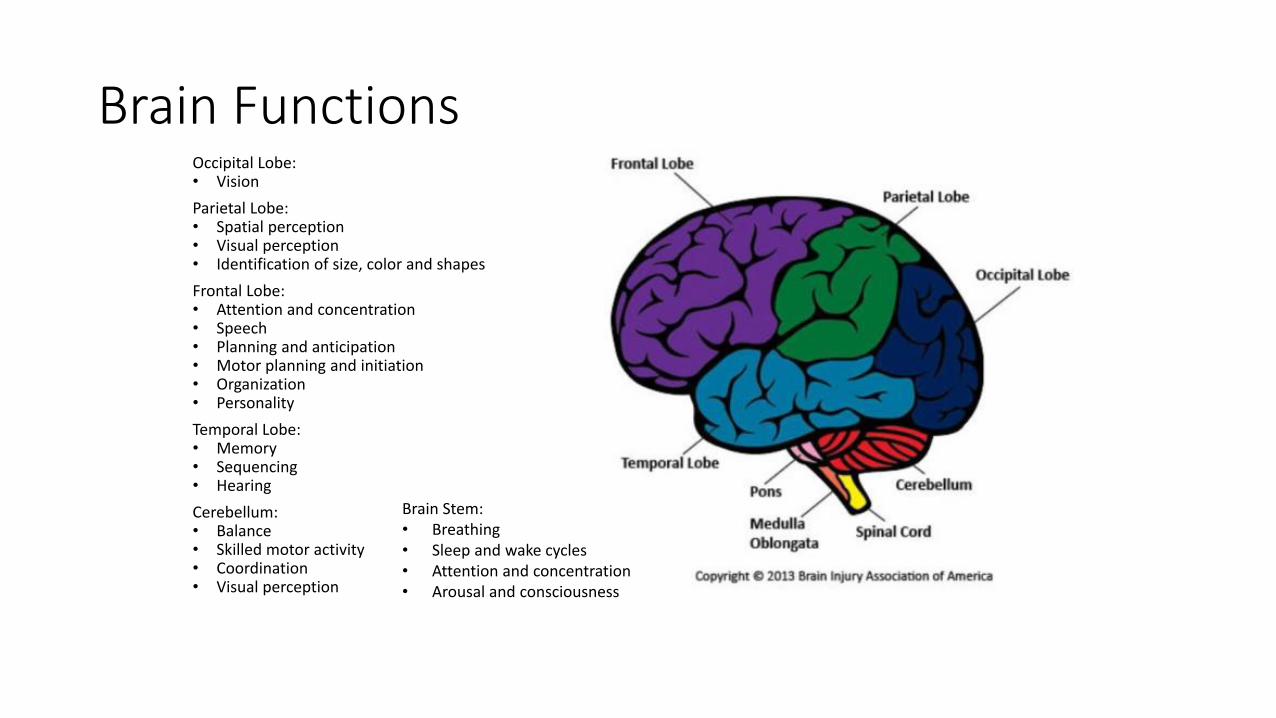
Brain FunctionsOccipital Lobe: • Vision
Parietal Lobe:• Spatial perception• Visual perception• Identification of size, color and shapes
Frontal Lobe: • Attention and concentration• Speech• Planning and anticipation• Motor planning and initiation• Organization• Personality
Temporal Lobe:• Memory• Sequencing• Hearing
Cerebellum:• Balance• Skilled motor activity• Coordination• Visual perception
Brain Stem:• Breathing • Sleep and wake cycles• Attention and concentration• Arousal and consciousness
Visual Processing
Focal Processing
• Occipital Cortex
• Fovea / Central Vision
• Details
• Concentration / Attention
Ambient Processing
• Midbrain
• Peripheral Vision
• Visual System coordinates with Kinesthetic, Proprioceptive, Tactile, Vestibular Systems
• Organizes Spatial Information

Vestibular Ocular Dysfunction
Radiology. 2014 Jul;272(1):224-32. doi: 10.1148/radiol.14132670. Epub 2014 Apr 15.
DTI findings suggests central axonal injury underlies vestibulopathy and ocular convergence insufficiency after mild traumatic brain injury • Compared with control subjects, patients with mild TBI and vestibular symptoms had decreased
neurocognitive test scores and FA values in the cerebellum and fusiform gyri • Patients with ocular convergence insufficiency had diminished neurocognitive test scores and FA values in
the right anterior thalamic radiation and right geniculate nucleus optic tracts • Cerebellar injury showed an inverse correlation with recovery time • Anterior thalamic radiation injury showed correlation with decreased processing speed
Balance & Illusions of Movement
Dizziness and Balance Problems Related to Vision
• Vision plays a significant role in balance.
• Approximately 20% of the nerve fibers from the eyes interact with the vestibular system.
• There are a variety of visual dysfunctions that can cause, or associate with dizziness and balance problems. Sometimes these are purely visual problems, and sometimes they are caused from other disorders such as stroke, head injury, vestibular dysfunction, deconditioning, and decompensation.
Visual Dysfunctions Causing Dizziness and Balance Problems
• Aniseikonia
• Binocular Vision Dysfunction
• Double Vision
• Vertical Imbalance
• Ambient Visual Disorder
• Eye Movement Disorders
Visual Motion Sensitivity
• Visual motion sensitivity to peripheral movement• “Supermarket Syndrome”
• Bi-nasal Occlusion (BNO)• VEP documented improvement in Patients with TBI
• Decreased amplitudes in Patients w/o TBI
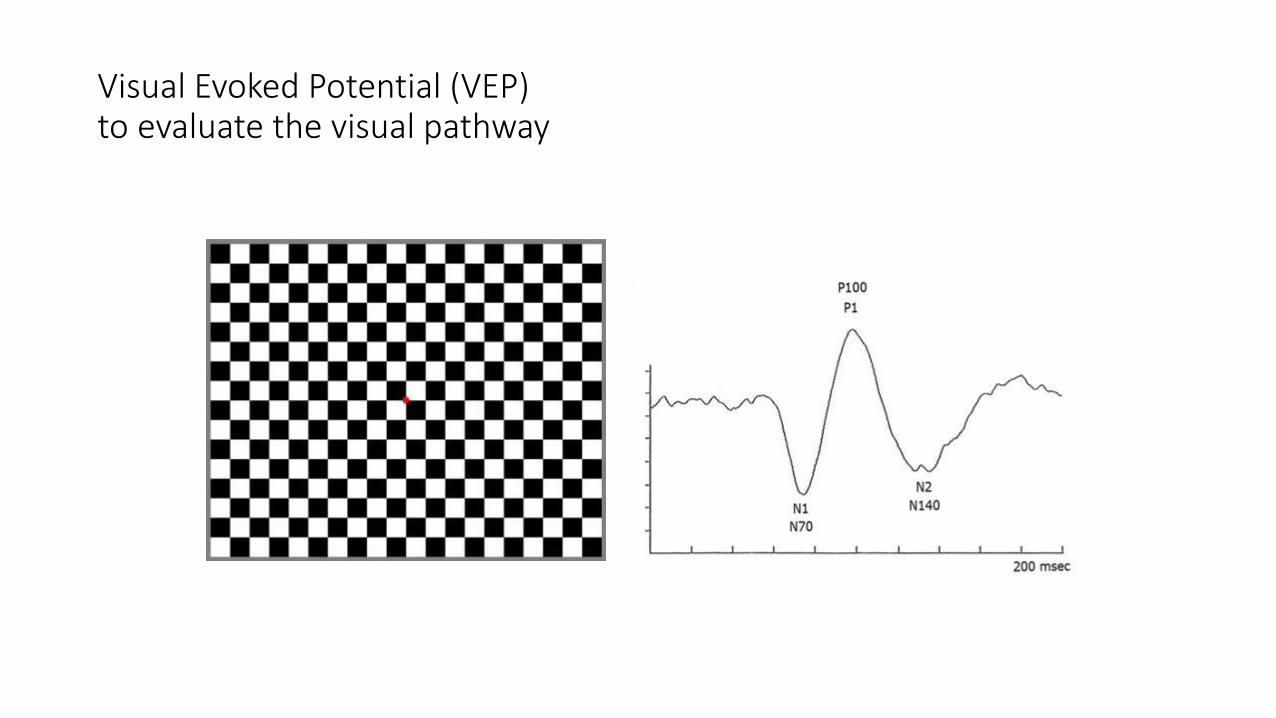
Visual Evoked Potential (VEP)to evaluate the visual pathway
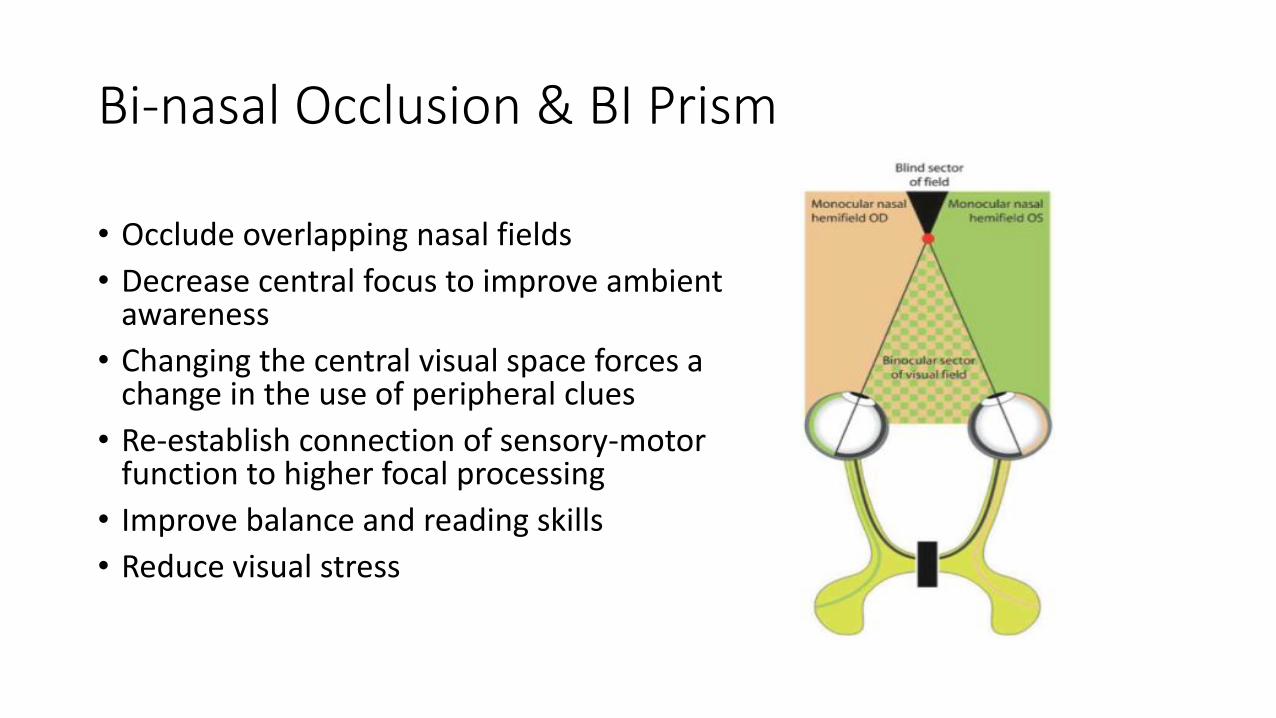
Bi-nasal Occlusion & BI Prism
• Occlude overlapping nasal fields
• Decrease central focus to improve ambient awareness
• Changing the central visual space forces a change in the use of peripheral clues
• Re-establish connection of sensory-motor function to higher focal processing
• Improve balance and reading skills
• Reduce visual stress
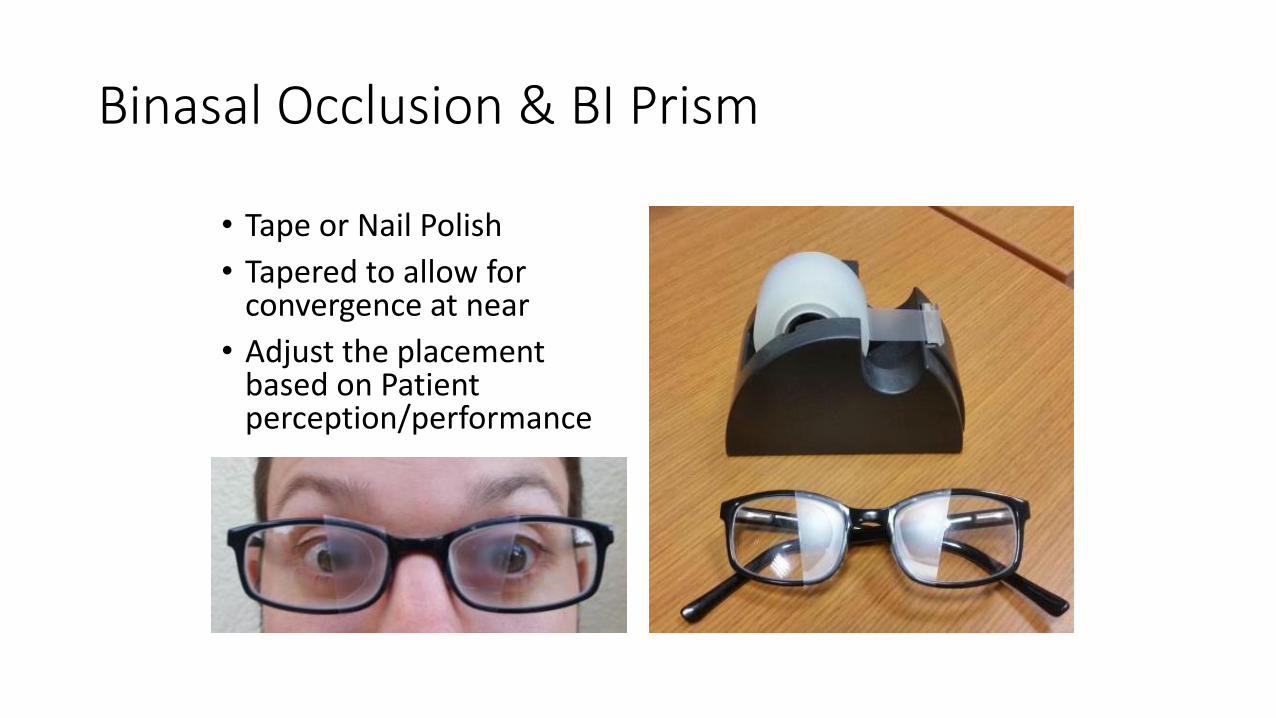
Binasal Occlusion & BI Prism
• Tape or Nail Polish
• Tapered to allow for convergence at near
• Adjust the placement based on Patient perception/performance
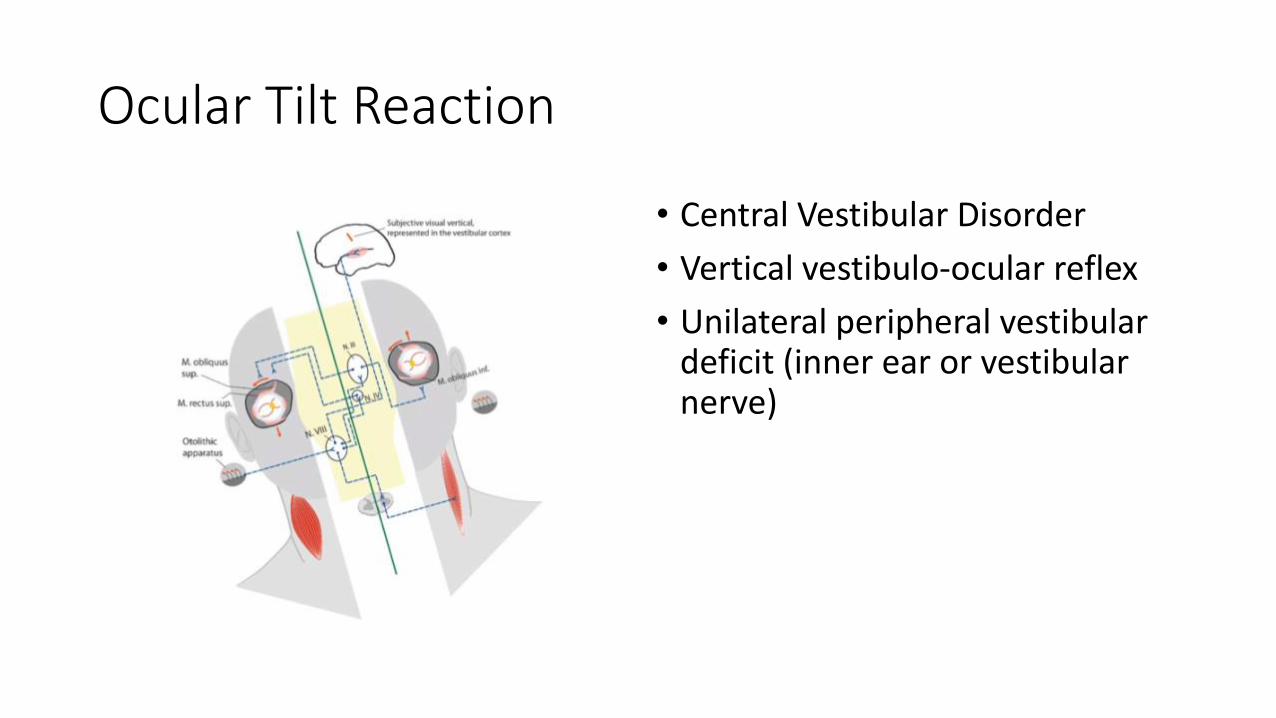
Ocular Tilt Reaction
• Central Vestibular Disorder
• Vertical vestibulo-ocular reflex
• Unilateral peripheral vestibular deficit (inner ear or vestibular nerve)
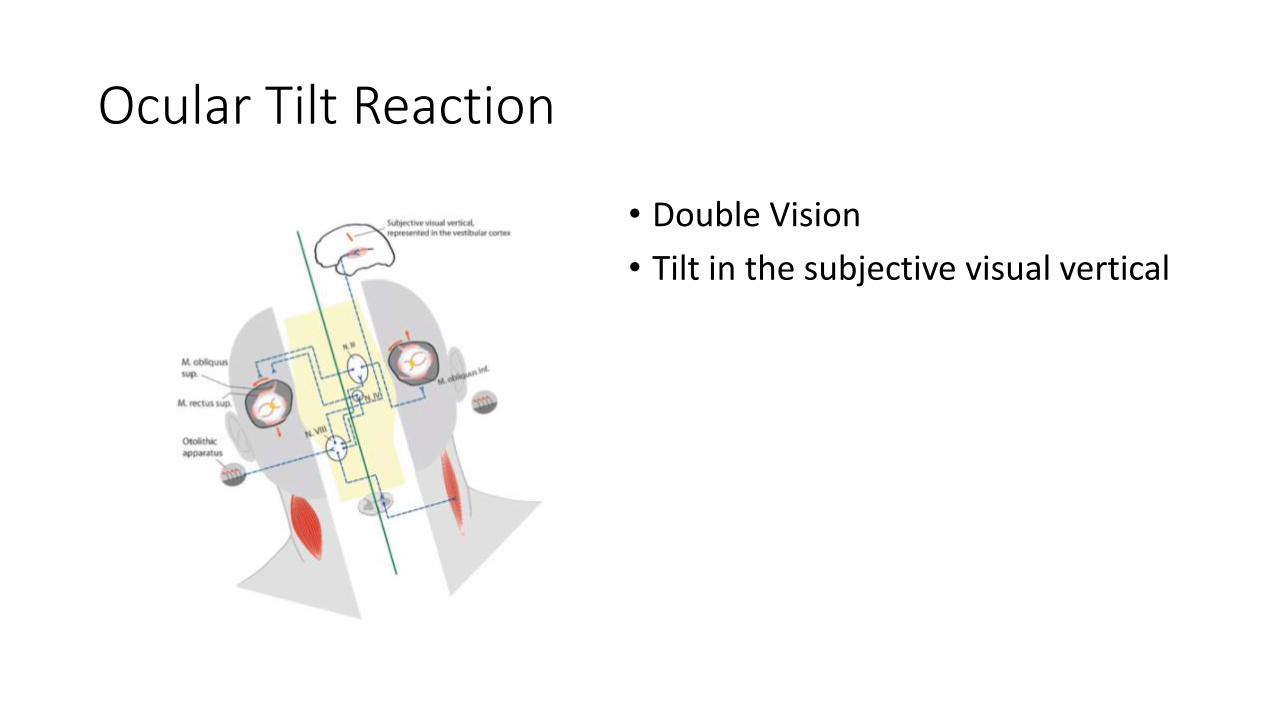
Ocular Tilt Reaction
• Double Vision
• Tilt in the subjective visual vertical
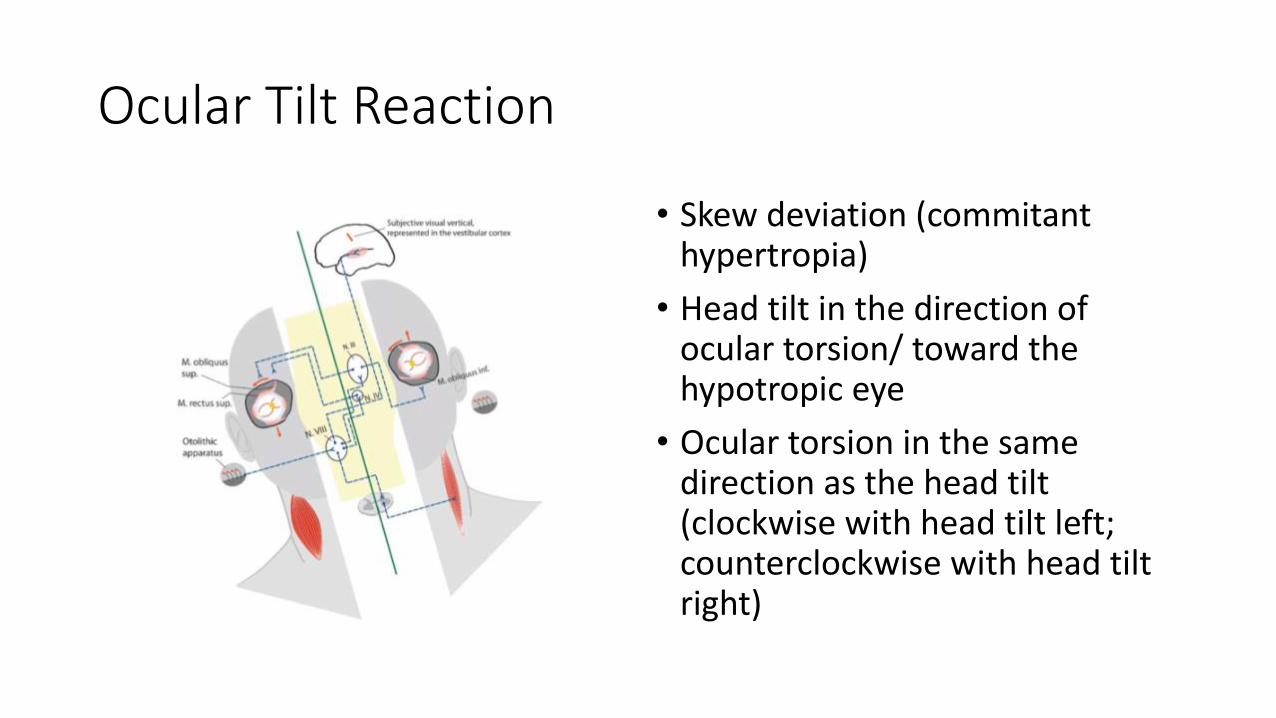
Ocular Tilt Reaction
• Skew deviation (commitanthypertropia)
• Head tilt in the direction of ocular torsion/ toward the hypotropic eye
• Ocular torsion in the same direction as the head tilt (clockwise with head tilt left; counterclockwise with head tilt right)
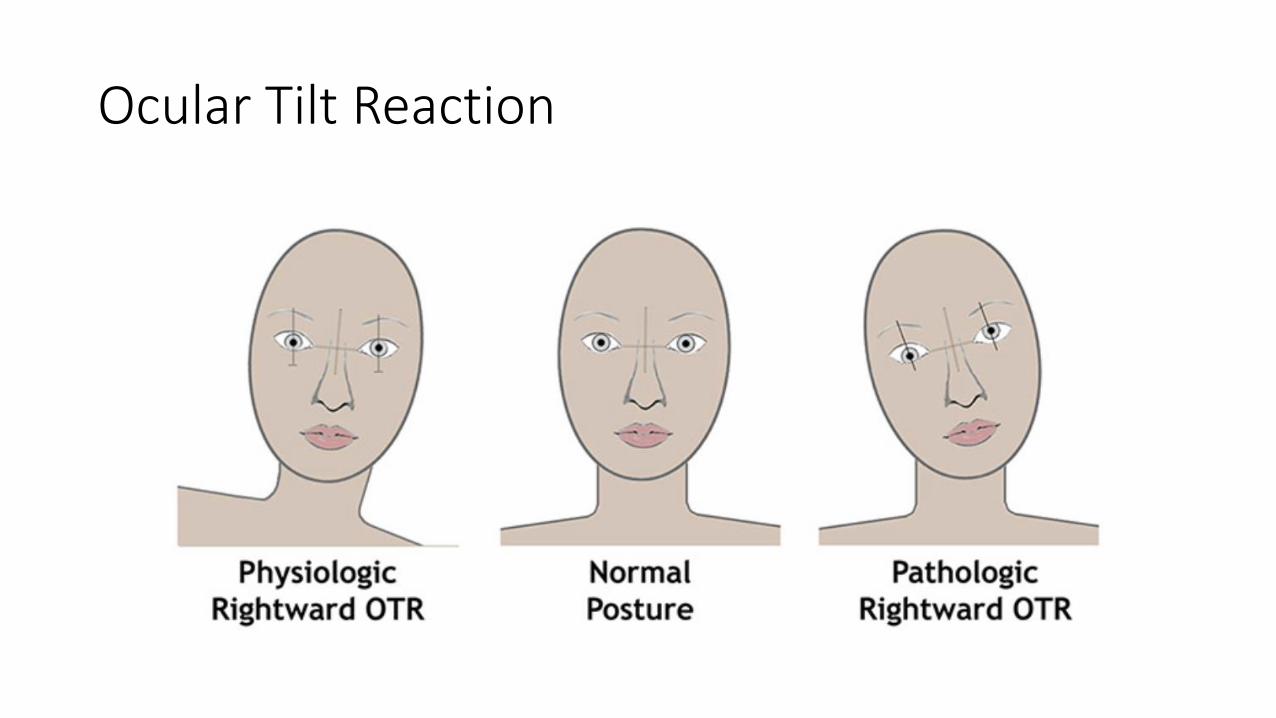
Ocular Tilt Reaction
Abnormal Egocentric Localization
• Mismatch between objective direction of straight ahead and subjective sense of direction
• May be present in up to 30% of mTBI patients
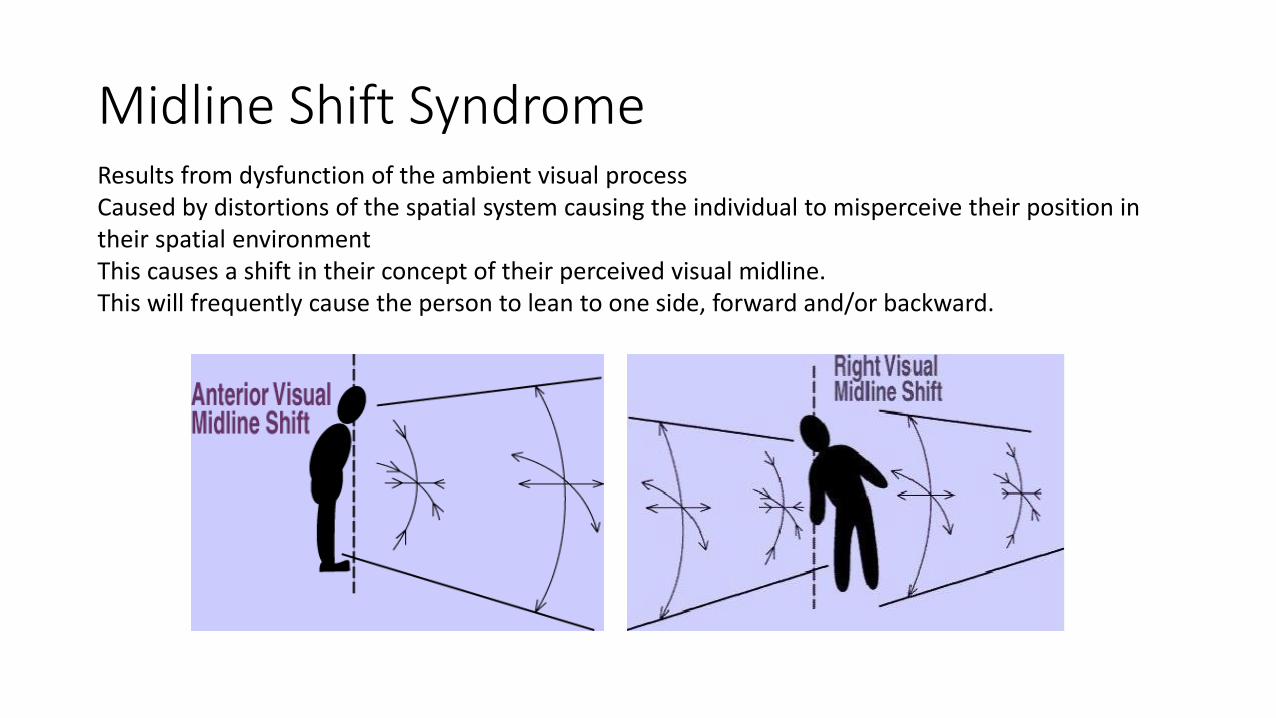
Midline Shift SyndromeResults from dysfunction of the ambient visual processCaused by distortions of the spatial system causing the individual to misperceive their position in their spatial environmentThis causes a shift in their concept of their perceived visual midline. This will frequently cause the person to lean to one side, forward and/or backward.
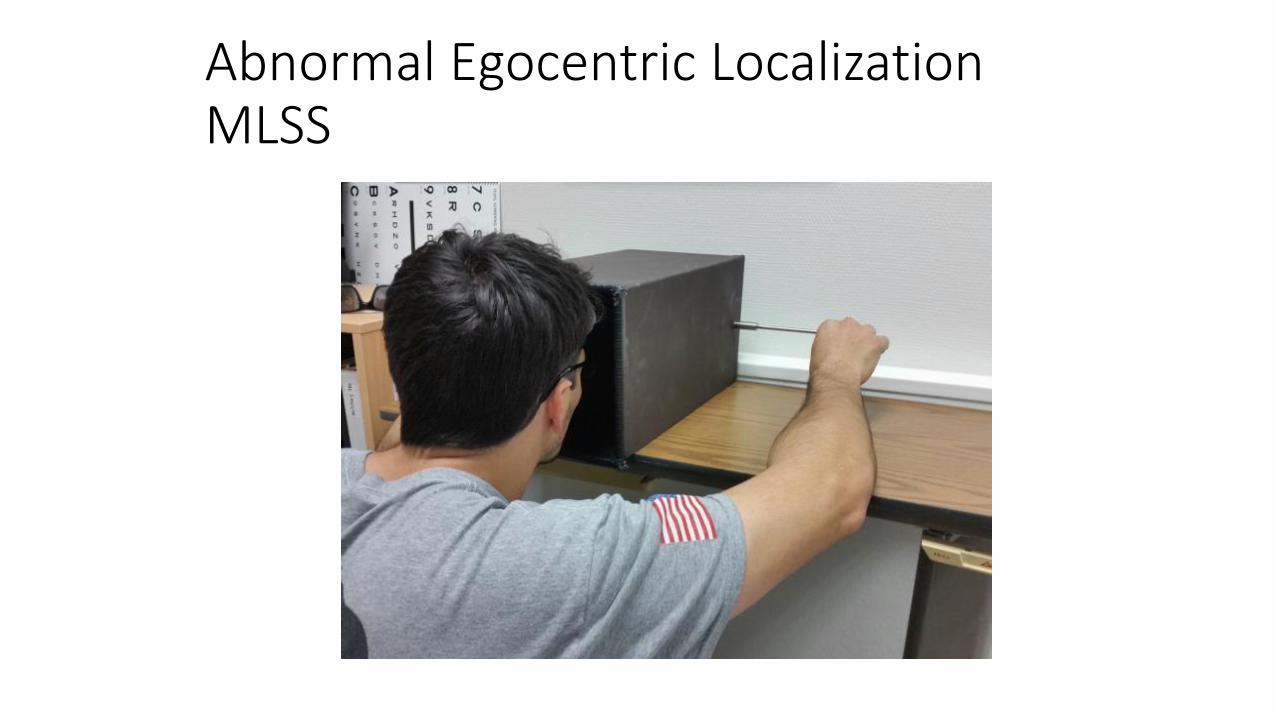
Abnormal Egocentric LocalizationMLSS

Prisms
• Yoked prisms• Light bends toward the base
• Yoked Prism Walk• Diagnostic vs Therapeutic
• Affected area of the brain
• Retinal Mapping• Inferior retina Temporal lobe (Base Down)
• Superior retina Parietal lobe (Base Up)
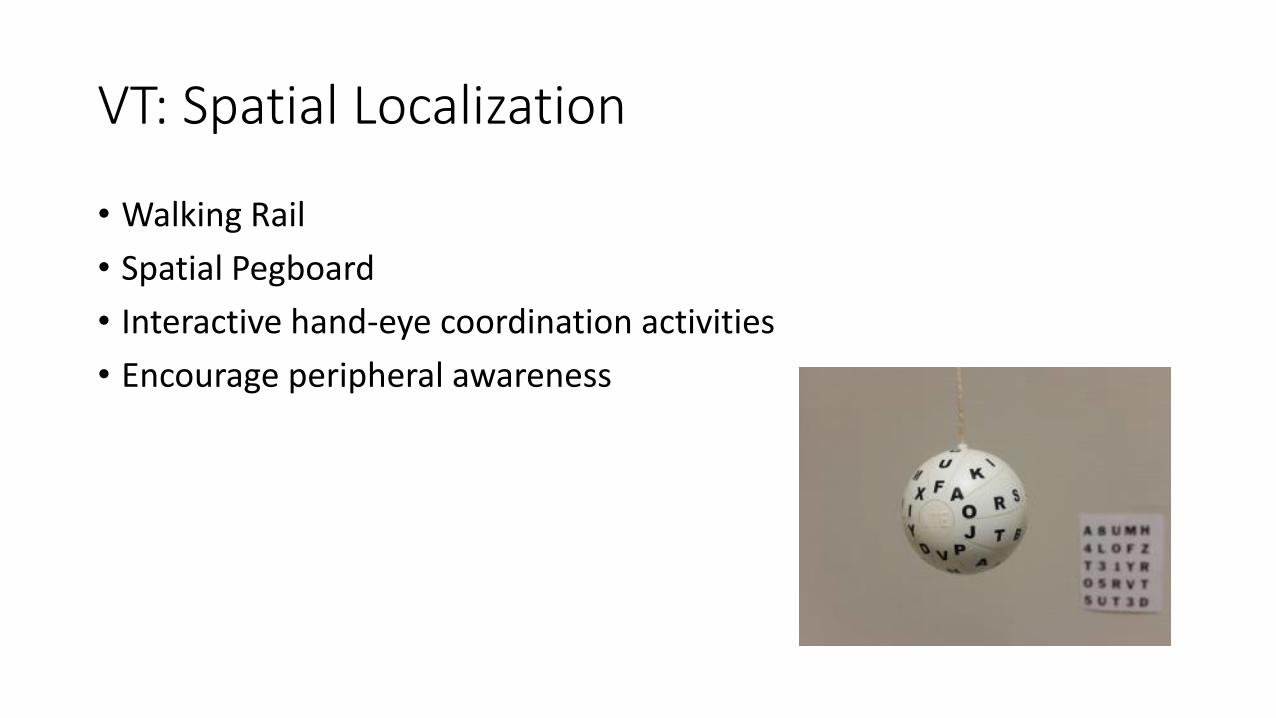
VT: Spatial Localization
• Walking Rail
• Spatial Pegboard
• Interactive hand-eye coordination activities
• Encourage peripheral awareness
Light Sensitivity
• Brain injury is often accompanied by increased light sensitivity and general inability to tolerate normal glare.
• Abnormal discomfort from normal light levels• up to 50% of patients
• The problem seems to be an inability of the brain to adjust to various levels of brightness. It is as if one had a radio and the volume control was broken and you could not make the adjustments you normally do to control loudness.

Photosensitivity
• Photosensitive retinal ganglion cells detect background illumination, projecting directly to the thalamus (regulates perceptual sensations)
• TBI can result in thalamic damage and dysregulation of incoming signals
• Poor regulation/suppression of back ground lighting intensity results in enhanced sensitivity to light
• Threshold of pain stimulus is reached
Photosensitivity
• Consider: • Pupillary basis
• Tinted lenses may promote visual adaptation over the long-term
• Avoid chronic dark adapted state
• Post Trauma Vision Syndrome patients may experience improvement in light tolerance when treated with neuro-rehabilitation
Tints
• Selective filters, particularly amber filters are often used by brain injury patients.
• FL41 50% filters 480nm wavelengths of light = peak activation range of retinal ganglion cells
• Migraine and Blepharospasm
Tints
• Blue spectrum filters: • Bend light more toward central retina
• Red spectrum filters:• Bend light toward peripheral retinal
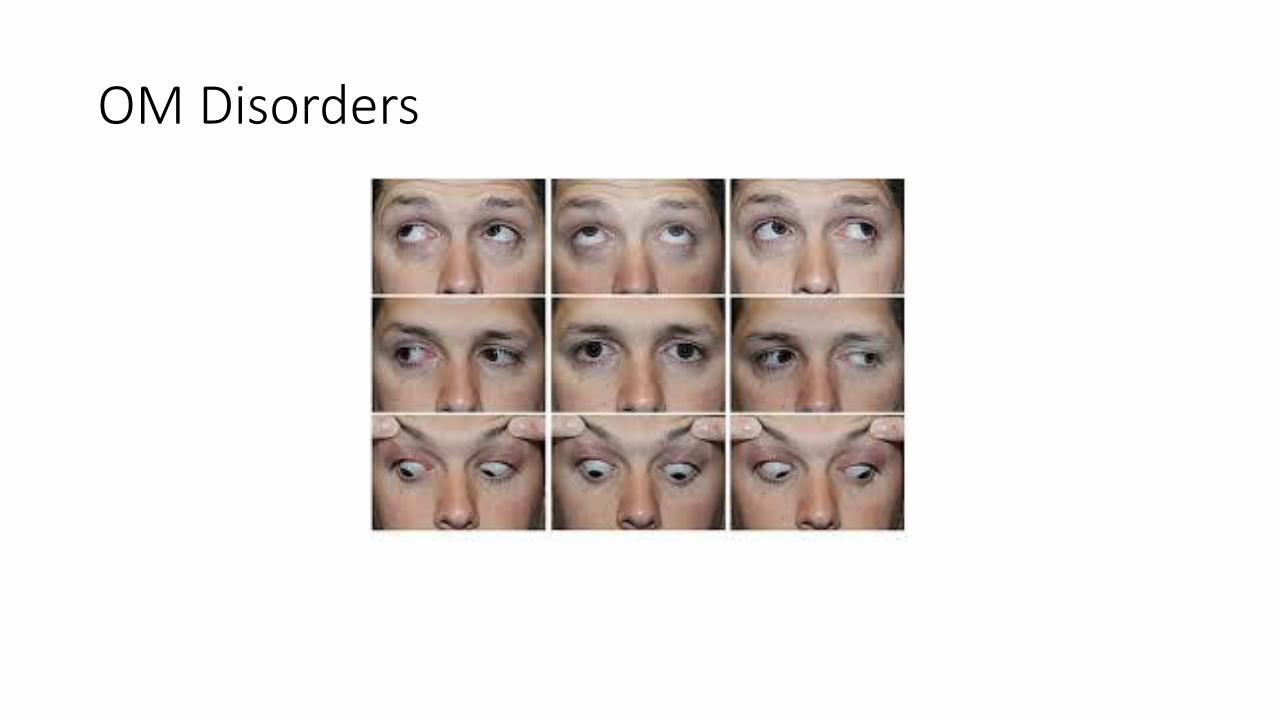
OM Disorders
OM Disorders
• Eye movements
• Saccades
• Pursuits
Reading Disorders
• Reading tasks require complex sensory motor cognitive functioning
• Can be damaged at many different levels
• Individuals with PTVS begin to look at paragraphs of print almost as isolated letters on a page and have great difficulty organizing their reading ability.
Reading
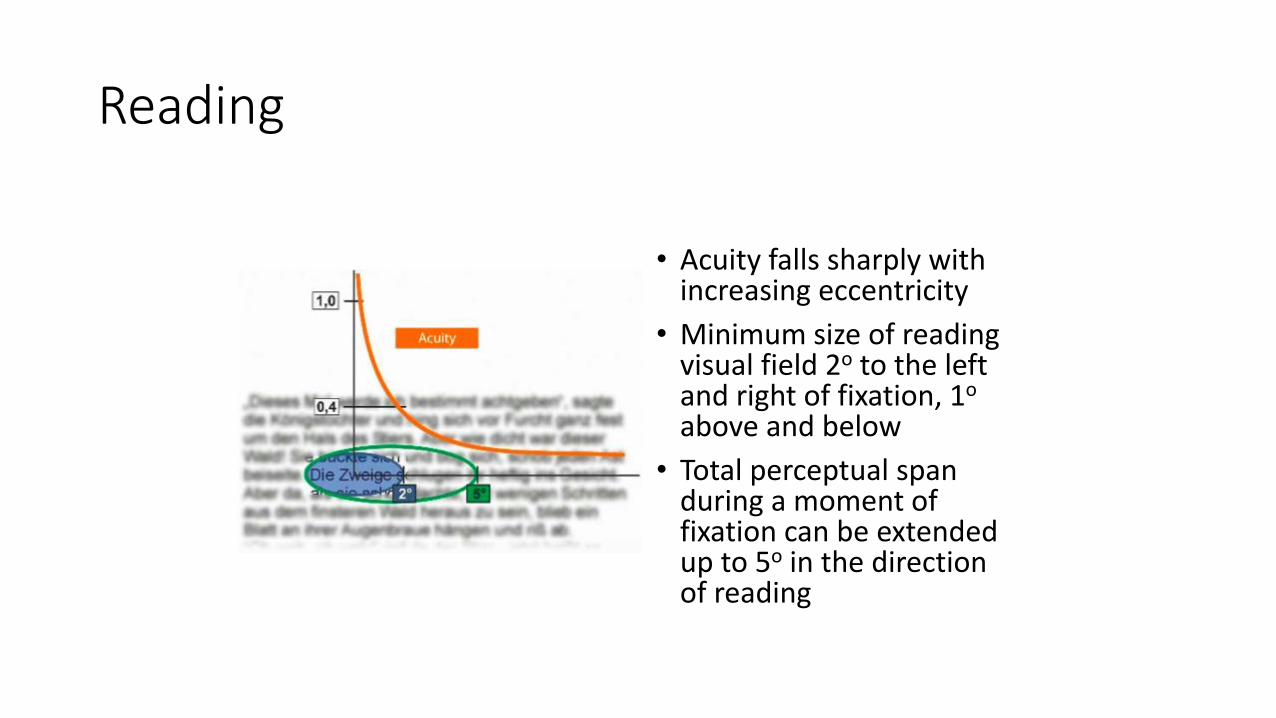
• Acuity falls sharply with increasing eccentricity
• Minimum size of reading visual field 2o to the left and right of fixation, 1o
above and below
• Total perceptual span during a moment of fixation can be extended up to 5o in the direction of reading
Reading Disorders Considerations
• Refractive error
• Poor accommodation
• Poor binocularity: Convergence Insufficiency
• Visual Field Defects within 5o eccentricity
• Motor disturbances: Ocular Motility / Gaze Control
• Developmental Dyslexia
Visual Perception• Visual-Motor Integration - Eye-hand, eye-foot, and eye-body coordination
• Visual-Auditory Integration - The ability to relate and associate what is seen and heard
• Visual Memory - The ability to remember and recall information that is seen
• Visual Closure - The ability "to fill in the gaps", or complete a visual picture based on seeing only some of the parts
• Spatial Relationships - The ability to know "where I am" in relation to objects and space around me and to know where objects are in relation to one another
• Figure-Ground Discrimination - The ability to discern form and object from background
Visual Information Processing Dysfunction
Vision Rehabilitation
• TBI effects are complex and vary from person to person, no two brain injuries are the same
• Patient education and Feedback is key!
• Emphasize awareness and attention
• Survey Symptoms
• Discuss clear goals
• Rehab goal is to correct maladaptive behaviors, habits and patterns
Vision Rehabilitation
• Correct refractive error
• Added lens power
• Prism: horizontal then vertical
• VT
• Tints, Yoked prism, BNO
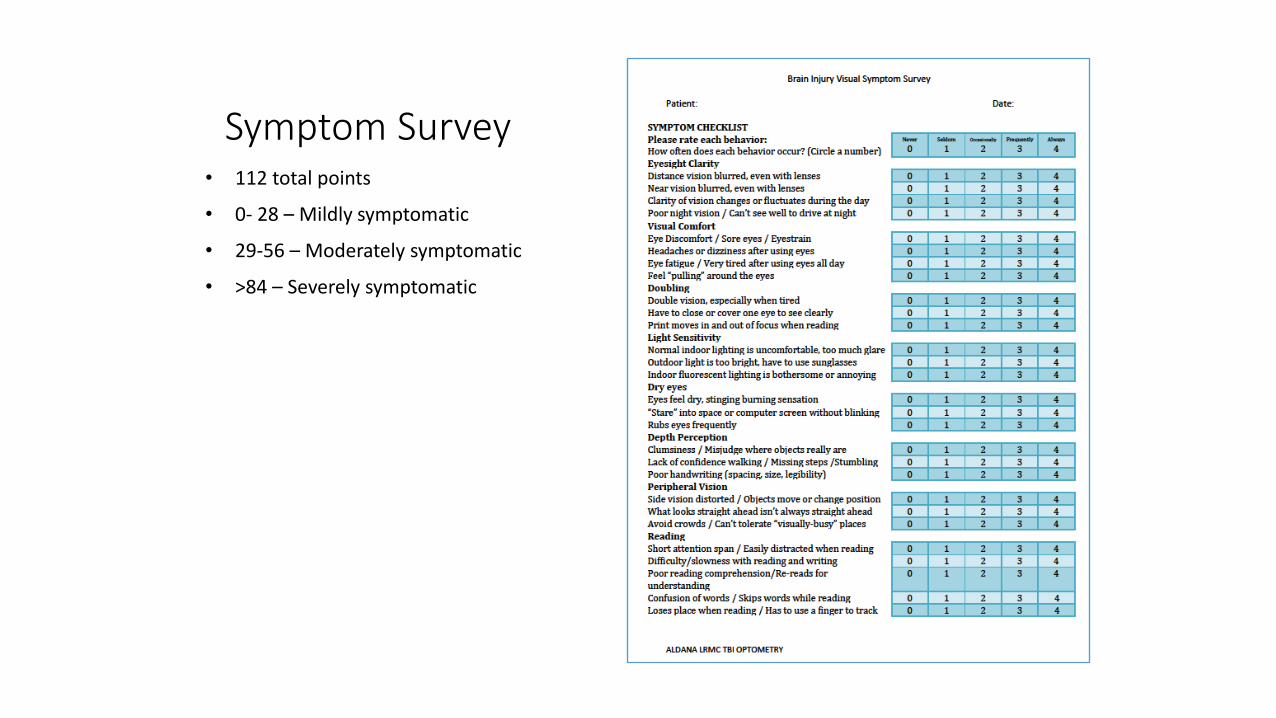
Symptom Survey• 112 total points
• 0- 28 – Mildly symptomatic
• 29-56 – Moderately symptomatic
• >84 – Severely symptomatic
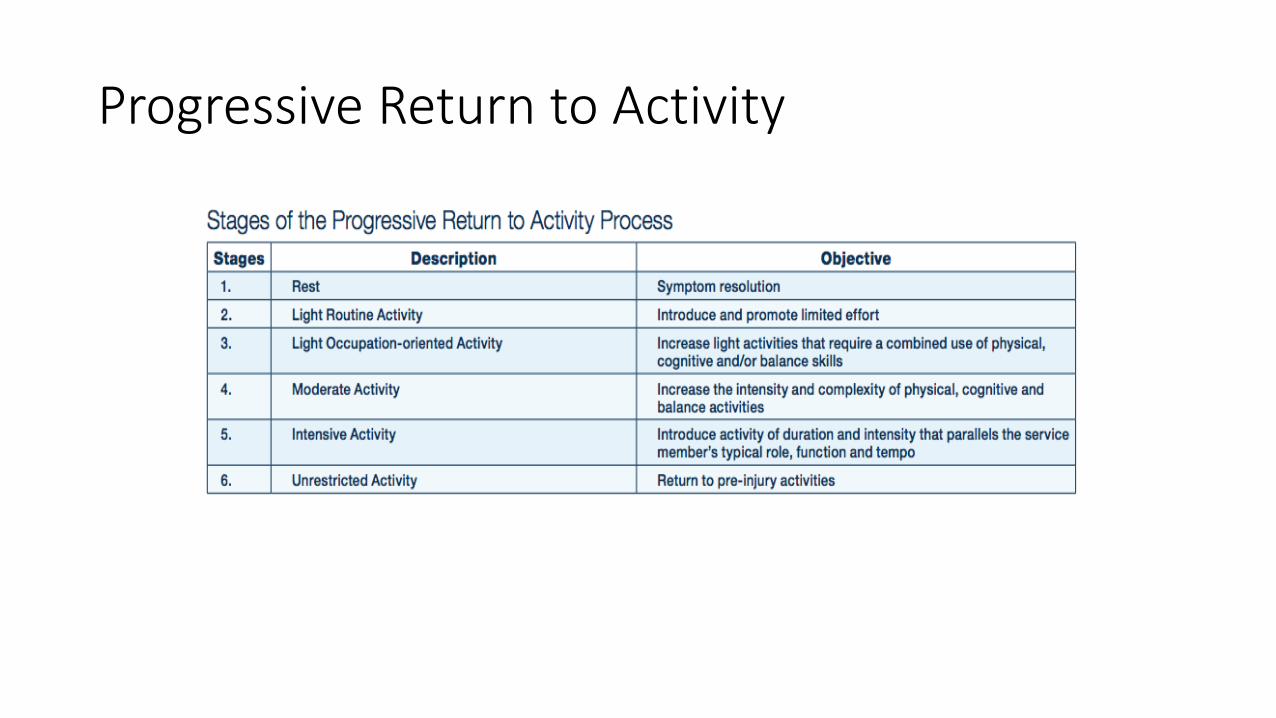
Progressive Return to Activity
https://youtu.be/ELpfYCZa87g