thorax hut lung: domesticallyacquired pneumoconiosis ... · "anthracosis" in 12,...
TRANSCRIPT
Thorax 1991;46:334-340
Hut lung: a domestically acquiredpneumoconiosis of mixed aetiology in ruralwomen
J P Grobbelaar, E D Bateman
Respiratory Clinic,Department ofMedicine, Universityof Cape Town andGroote SchuurHospital, Observatory7925, Cape Town,South AfricaJ P GrobbelaarE D BatemanReprint requests to:Professor BatemanAccepted 15 February 1991
AbstractA form of pneumoconiosis in ruralAfrican women termed "Transkeisilicosis" has been thought to be due tosilica particles inhaled while they arehand grinding maize between rocks.Twenty five women were studied whowere considered to have this conditionaccording to the following criteria: ruraldomicile, radiographic and lung biopsyevidence of pneumoconiosis, no exposureto mining or industry and no evidence ofactive tuberculosis. They were assessedfor radiological, pathological,physiological and bronchoalveolarlavage fluid features. Potentialaetiological factors were assessed bydetermining levels of exposure torespirable quartz and non-quartz con-taining dusts and smoke in rural dwell-ings during maize grinding and cooking.Most of the women were symptomless.Radiological findings ranged from amiliary pattern to extensive fibrosisresembling progressive massive fibrosis.Histological features included simple"anthracosis" in 12, anthracosis withmacules in six, and mixed dust fibrosisin seven. Cell numbers and theirproportions in lavage fluid were normal.More than 60% of macrophages wereheavily laden with inorganic inclusions.Respirable quartz concentrations andcalculated cumulative time weightedexposures were below those recom-mended for industry during grindingwith sandstone (100% quartz) and theywere even lower during grinding withdolerite containing no quartz despite thepresence of an appreciable amount ofquartz in the ground maize. Totalrespirable dust and smoke con-centrations were greater than therecommended safe levels. Three womenhad no exposure to maize grinding. It isconcluded that the inhalation of non-quartz containing dust and smoke frombiomass fuelled fires is more importantin the aetiology of this condition thanexposure to quartz dust. The term "hutlung" may be more appropriate.
Domestically acquired pneumoconiosis hasbeen described in women from the Transkeidistrict of South Africa.' In their originalpaper Palmer and Daynes suggested that theterm Transkei silicosis should be used for this
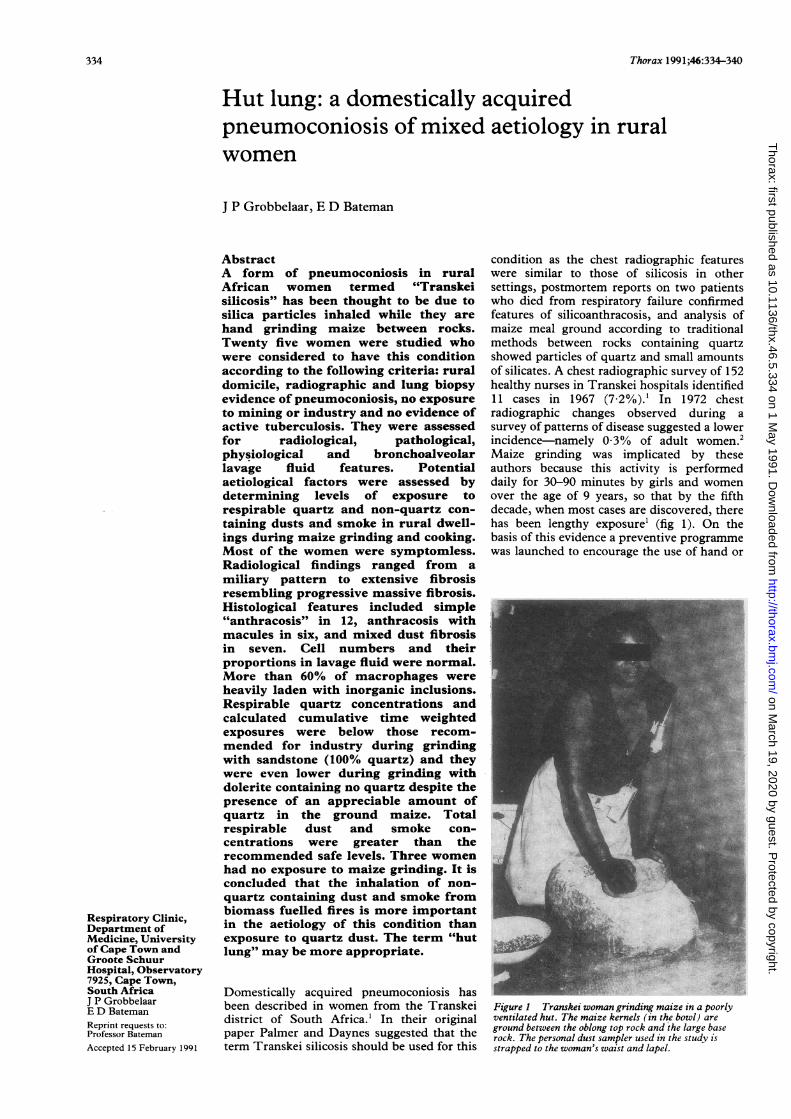
condition as the chest radiographic featureswere similar to those of silicosis in othersettings, postmortem reports on two patientswho died from respiratory failure confirmedfeatures of silicoanthracosis, and analysis ofmaize meal ground according to traditionalmethods between rocks containing quartzshowed particles of quartz and small amountsof silicates. A chest radiographic survey of 152healthy nurses in Transkei hospitals identified11 cases in 1967 (7 2%).' In 1972 chestradiographic changes observed during asurvey of patterns of disease suggested a lowerincidence-namely 0 3% of adult women.2Maize grinding was implicated by theseauthors because this activity is performeddaily for 30-90 minutes by girls and womenover the age of 9 years, so that by the fifthdecade, when most cases are discovered, therehas been lengthy exposure' (fig 1). On thebasis of this evidence a preventive programmewas launched to encourage the use of hand or
Figure 1 Transkei woman grinding maize in a poorlyventilated hut. The maize kernels (in the bowl) areground between the oblong top rock and the large baserock. The personal dust sampler used in the study isstrapped to the woman's waist and lapel.
334
on March 19, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.334 on 1 M
ay 1991. Dow
nloaded from
Hut lung: a domestically acquired pneumoconiosis of mixed aetiology in rural women
motor driven machinery to replace traditionalmethods.3
Patients with this condition are still seencommonly at Groote Schuur Hospital. Wereport the clinical, radiological, physiological,histological and bronchoalveolar lavage fluidabnormalities found in 25 women with thiscondition. As relatively few quartz particleswere identified in lung sections we studiedconcentrations of respirable quartz dust, non-quartz containing dust, and smoke in ruralTranskei houses during maize grinding andcooking.
MethodsPATIENTSAll patients entered into the study, who wereinvestigated at the Groote Schuur Hospitalrespiratory clinic over 12 years, satisfied fiveinclusion criteria. They had to (1) be ruralwomen (predominantly from the Transkei)who for most of their lives had been exposed tosmoke from cooking fires or who had groundmaize by traditional methods, or both; (2) haveno history of industrial or mining exposure;(3) have radiographic changes compatible withpneumoconiosis4; (4) have lung biopsy
MR-14. ~ ~N.fi'~
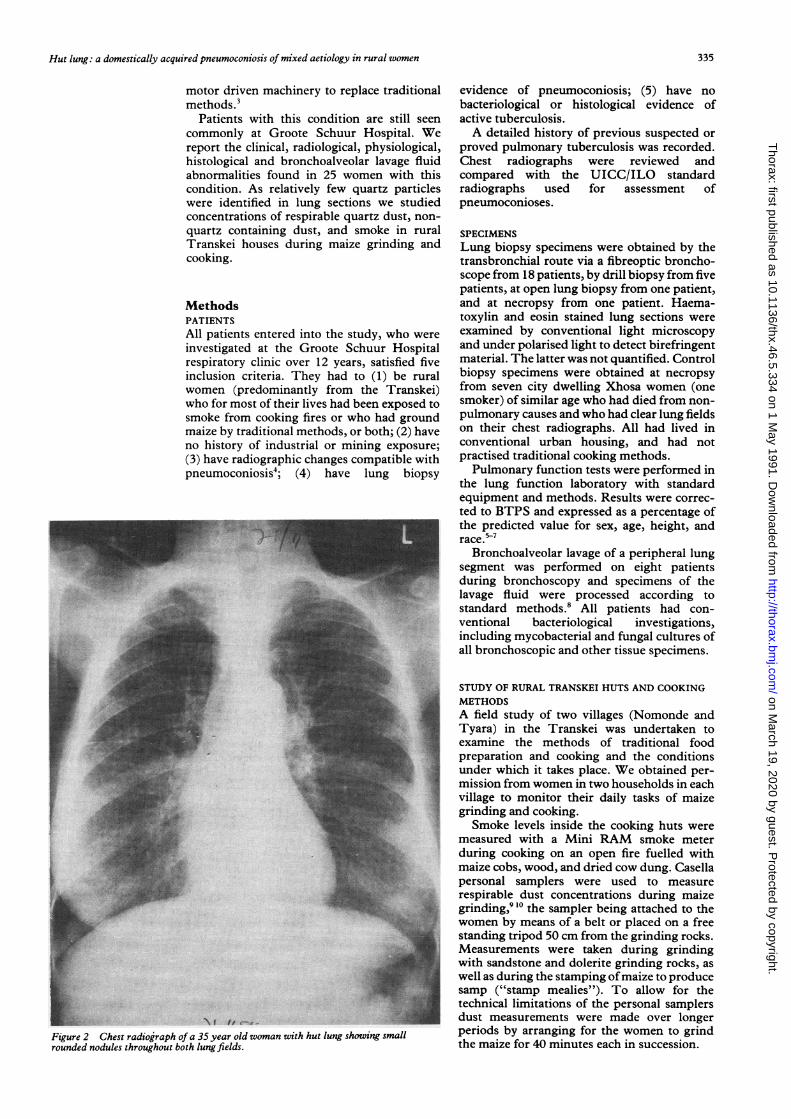
Figure 2 Chest radiograph of a 35 year old woman with hut lung showing smallrounded nodules throughout both lung fields.
evidence of pneumoconiosis; (5) have nobacteriological or histological evidence ofactive tuberculosis.A detailed history of previous suspected or
proved pulmonary tuberculosis was recorded.Chest radiographs were reviewed andcompared with the UICC/ILO standardradiographs used for assessment ofpneumoconioses.
SPECIMENSLung biopsy specimens were obtained by thetransbronchial route via a fibreoptic broncho-scope from 18 patients, by drill biopsy from fivepatients, at open lung biopsy from one patient,and at necropsy from one patient. Haema-toxylin and eosin stained lung sections wereexamined by conventional light microscopyand under polarised light to detect birefringentmaterial. The latter was not quantified. Controlbiopsy specimens were obtained at necropsyfrom seven city dwelling Xhosa women (onesmoker) of similar age who had died from non-pulmonary causes and who had clear lung fieldson their chest radiographs. All had lived inconventional urban housing, and had notpractised traditional cooking methods.Pulmonary function tests were performed in
the lung function laboratory with standardequipment and methods. Results were correc-ted to BTPS and expressed as a percentage ofthe predicted value for sex, age, height, andrace.57
Bronchoalveolar lavage of a peripheral lungsegment was performed on eight patientsduring bronchoscopy and specimens of thelavage fluid were processed according tostandard methods.8 All patients had con-ventional bacteriological investigations,including mycobacterial and fungal cultures ofall bronchoscopic and other tissue specimens.
STUDY OF RURAL TRANSKEI HUTS AND COOKINGMETHODSA field study of two villages (Nomonde andTyara) in the Transkei was undertaken toexamine the methods of traditional foodpreparation and cooking and the conditionsunder which it takes place. We obtained per-mission from women in two households in eachvillage to monitor their daily tasks of maizegrinding and cooking.Smoke levels inside the cooking huts were
measured with a Mini RAM smoke meterduring cooking on an open fire fuelled withmaize cobs, wood, and dried cow dung. Casellapersonal samplers were used to measurerespirable dust concentrations during maizegrinding,9 lo the sampler being attached to thewomen by means of a belt or placed on a freestanding tripod 50 cm from the grinding rocks.Measurements were taken during grindingwith sandstone and dolerite grinding rocks, aswell as during the stamping ofmaize to producesamp ("stamp mealies"). To allow for thetechnical limitations of the personal samplersdust measurements were made over longerperiods by arranging for the women to grindthe maize for 40 minutes each in succession.
335
on March 19, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.334 on 1 M
ay 1991. Dow
nloaded from

Grobbelaar, Bateman
Figure 3 Chest radiograph of a 54 year old patient in this series showing progressivemassive fibrosis, coalescent nodules and hyperinflation of lower lobes with bullaformation.
Respirable dust concentrations were cal-culated by dividing the weight of the dust bythe volume of the air filtered. Quartz estima-tions were made by ashing the dust from thesampler filters and then determining the weightof the residual inorganic matter, shown to bequartz by x ray diffraction. The percentage ofquartz was calculated by dividing the weight ofthe quartz by the weight of the total respirable
Figure 4 Photomicrograph of a section of a lung biopsy specimen takenfrom a patientin this series, showing anthracosis with macule formation surrounding bronchi and in theperibronchiolar interstitium. (Haematoxylin and eosin.)
dust collected. The respirable quartz concen-trations were then calculated by multiplyingthe percentage ofquartz and the total respirabledust concentrations. The dust collected wasalso analysed by electron microscopy and x rayenergy spectrometry. To permit comparisonwith industry, the respirable dust and quartzconcentrations were converted to equivalenttime weighted average values of exposure for a40 hour working week" by dividing the valuesby 7-5 (calculated from a grinding time of 5-25hours per week).Crushed samples of two types of grinding
rock were analysed by x ray diffraction with aPhilips goniometer. Thin sections of the samerocks were examined microscopically fortexture. A sample of known pure quartz wasused as a control. X ray diffraction of unashedspecimens of maize ground with sandstone,dolerite rock, and "stamp mealies" was per-formed to determine their quartz content.
ResultsDEMOGRAPHYTwenty five patients met the inclusion criteria.Twenty two were Xhosas from the Transkei.The remaining three were of mixed race fromNamaqualand (on the west coast of southernAfrica) and did not grind maize but wereheavily exposed to domestic smoke from cook-ing on iron stoves fuelled by smoky wood fires inpoorly ventilated huts. They met all the otherinclusion criteria. The mean age of the wholegroup was 43 (range 20-84) years. Seventeenwere non-smokers, five were tobacco pipesmokers, and three (all from Namaqualand)had smoked under 11 cigarettes a day. Sevenhad evidence of previous tuberculosis. Four-teen were symptomless and had been referredfor investigation of abnormal chestradiographs, 13 had mild acute respiratorytract symptoms suggesting acute infectivebronchitis. Only four had presented because ofchronic respiratory symptoms (chronicproductive cough and mild dyspnoea on effort).
RADIOLOGYThe radiological features were compatible withpneumoconiosis. They ranged from diffuse finerounded regular nodulation resembling miliarytuberculosis (fig 2) through coarser irregularnodules to extensive fibrosis resemblingprogressive massive fibrosis (fig 3). The lattershadows were ragged and not lobulated, andresulted in shrinkage of the affected areas andhyperinflation of the remaining lung. Theprofusion ranged from 1/1 to 3/3 changes' allzones were usually affected. One patient had corpulmonale. No eggshell calcification of hilarglands was noted, and none showed theappearance of Caplan's nodules. Six of 25patients showed additional radiologicalchanges compatible with healed tuberculosis.
HISTOLOGYThree histological patterns were observed.1 Simple anthracosis was found in 12 patients(defined as carbon pigment deposited within theseptal and perivascular areas and surrounding
336
Ahkoh-te..-4W* .1 1-
-
I
Y%l_ ...
'k 4'
f.,
on March 19, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.334 on 1 M
ay 1991. Dow
nloaded from

Hut lung: a domestically acquired pneumoconiosis of mixed aetiology in rural women
F mB f ;'S S~~~~~~~~~~~~-- -r - ,- ." AS,
-1
Figure 5 Photomicrograph of a section of a lung biopsy specimen taken from a patientin this series with mixed dustfibrosis. Features of a silicotic nodule are the amorphouscentral hyalinised tissue (on left) surrounded by a pallisade offibroblasts.(Haematoxylin and eosin.)
terminal respiratory bronchioles, but withoutmacule formation'2).2 Anthracosis with macule formation was
found in six patients (defined as carbonpigmentation with focal collections of dustladen macrophages occurring at-the division ofrespiratory bronchioles and within alveoli as
well as extending into the peribronchiolarinterstitium, with associated reticulin deposits)(fig 4). The small transbronchial biopsyspecimens did not permit a full assessment forareas of focal emphysema, but in all otherrespects the lesions were similar to those ofsimple coalworkers' pneumoconiosis. "3 Mixed dust fibrosis was found in biopsyspecimens from seven patients, of which twohad silicotic nodules (fig 5) and one progressivemassive fibrosis. Mixed dust fibrosis is seen as an
irregular or stellate interstitial fibrous lesionwith variable pigmentation from the inert dust,occurring predominantly in the area of therespiratory bronchiole and adjacent to smallarteries. The fibrotic response ranged fromsmall increases in reticulin to extensivecollagenisation; the fibrosis extended intosurrounding parenchyma in both a linear and a
radial fashion in areas containing quartz." "
Doubly refractile particles were seen underpolarised light, in specimens from 18patients." None of these features was seen inthe control lung biopsy specimens.
LUNG FUNCTION TESTSLung function measurements from 22 subjectsare shown in table 1. Airflow limitation (definedas forced expiratory volume in one second(FEV,)/forced vital capacity (FVC) below 70%or residual volume over 140% of the predictedvalue) was observed in 16 of the 22 patients anda restrictive pattern in one; in the remaining fivepatients the values were within normal limits.Carbon monoxide transfer factor (TLCO) was
less than 80% of predicted in 13 of the 17subjects tested. The mean percentage TLCOwas 65% (range 38-94%). The Kco was lessthan 80% of the predicted value in twopatients. Of the 16 patients with airflow limita-tion two were smokers and five had radiologicalevidence suggesting previous tuberculosis.None had evidence of reversible airflow limita-tion.
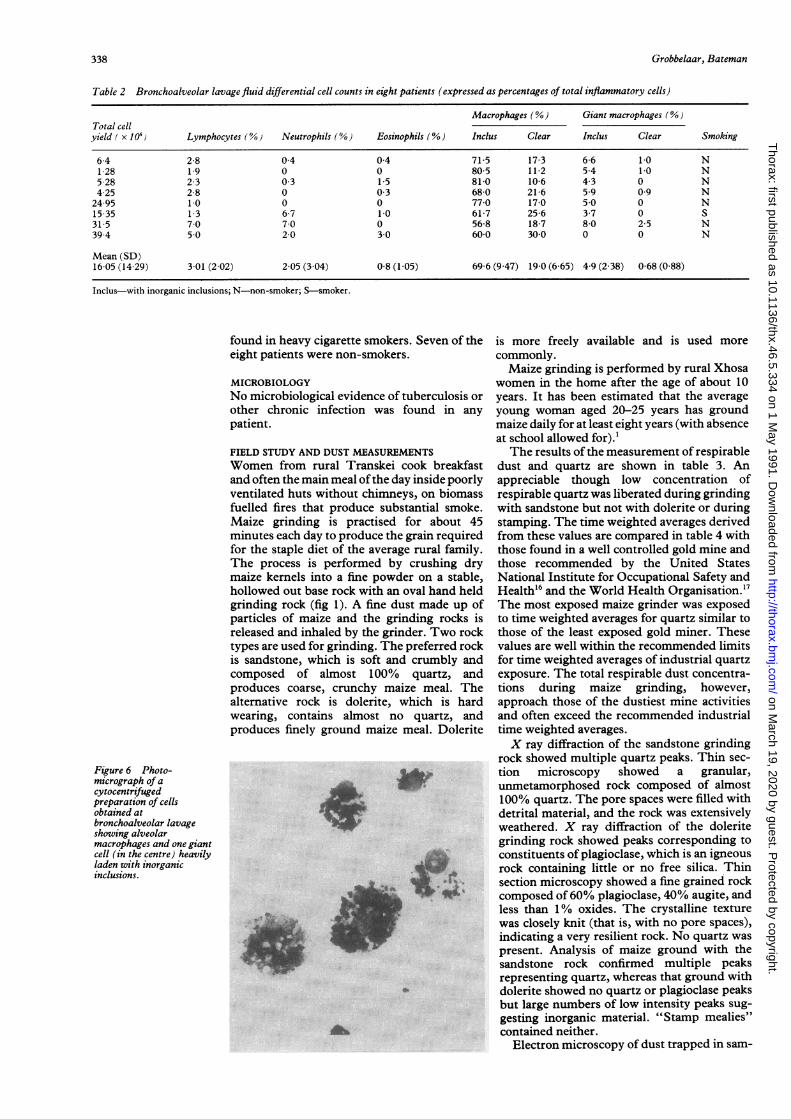
BRONCHOALVEOLAR LAVAGE FLUID FEATURESThe total cell yield was normal or mildlyincreased in the eight patients studied (table 2).The proportions of lymphocytes, neutrophils,and eosinophils were normal, but a largeproportion of the alveolar macrophages wereheavily laden with inorganic inclusions (fig 6).These were larger and more dense than those
Table I Results of lungfunction tests on 22 patients with hut lung, expressed as percentages ofpredicted values*
Patient no FEV, FVC FEV,/FVC TLCO Kco TLC RV Smoker or PPTB
1 57 113 43 64 90 172 2962 66 119 47 54 68 S3 52 61 76 38 88 105 273 PPTB4 59 104 48 50 82 PPTB5 69 105 63 PPTB6 111 143 67 94 121 159 244 PPTB7 99 97 86 69 96 121 1638 105 97 919 105 109 79 58 75lot 112 111 79 72 88 Slit 89 97 69 64 80 116 155 S12 65 61 89 80 117 S/PPTB13 83 115 61 65 84 123 15514 107 125 74 81 100 150 21015 114 115 83 92 11716 146 147 82 64 83 151 17517 33 56 48 43 89 PPTB18 55 64 74 53 115 95 14919 93 110 70 87 92 124 14520 62 75 6121 82 110 61 169 275 S/PPTB22 87 134 63 66 91 188 218
FEV,-Forced expiratory volume in one second; FVC-forced vital capacity; TLcO-carbon monoxide transfer factor; Kco-TLco/litre lung volume; TLC-total lung capacity; RV-residual volume; S-smoker; PPTB-probable previous tuberculosis.*For predicted values see ref 5 for FEV, and FVC, ref 6 for TLco and Kco, and ref 7 for TLC and RV. There are no lungfunction values for three of the 25 patients.tFrom Namaqualand.
337
on March 19, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.334 on 1 M
ay 1991. Dow
nloaded from
Grobbelaar, Bateman
Table 2 Bronchoalveolar lavagefluid differential cell counts in eight patients (expressed as percentages of total inflammatory cells)
Macrophages (%) Giant macrophages (00)Total cellyield ( x 106) Lymphocytes (0) Neutrophils (%) Eosinophils (%) Inclus Clear Inclus Clear Smoking
64 28 04 04 715 17-3 66 1 0 N1 28 1.9 0 0 805 112 54 1.0 N528 23 03 15 810 106 43 0 N425 28 0 03 680 216 59 09 N2495 1.0 0 0 770 170 50 0 N1535 13 67 10 617 256 37 0 S315 70 70 0 568 187 80 25 N394 50 20 30 60-0 300 0 0 N
Mean (SD)16 05 (14 29) 3 01 (2 02) 2 05 (3 04) 0-8 (1 05) 69-6 (9 47) 19-0 (6-65) 4-9 (2 38) 0-68 (0-88)
Inclus-with inorganic inclusions; N-non-smoker; S-smoker.
found in heavy cigarette smokers. Seven of theeight patients were non-smokers.
MICROBIOLOGYNo microbiological evidence of tuberculosis orother chronic infection was found in anypatient.
FIELD STUDY AND DUST MEASUREMENTSWomen from rural Transkei cook breakfastand often the main meal ofthe day inside poorlyventilated huts without chirnneys, on biomassfuelled fires that produce substantial smoke.Maize grinding is practised for about 45minutes each day to produce the grain requiredfor the staple diet of the average rural family.The process is performed by crushing drymaize kernels into a fine powder on a stable,hollowed out base rock with an oval hand heldgrinding rock (fig 1). A fine dust made up ofparticles of maize and the grinding rocks isreleased and inhaled by the grinder. Two rocktypes are used for grinding. The preferred rockis sandstone, which is soft and crumbly andcomposed of almost 100% quartz, andproduces coarse, crunchy maize meal. Thealternative rock is dolerite, which is hardwearing, contains almost no quartz, andproduces finely ground maize meal. Dolerite
Figure 6 Photo-micrograph of acytocentrifugedpreparation of cellsobtained atbronchoalveolar lavageshowing alveolarmacrophages and one giantcell (in the centre) heavilyladen with inorganicinclusions.
is more freely available and is used morecommonly.Maize grinding is performed by rural Xhosa
women in the home after the age of about 10years. It has been estimated that the averageyoung woman aged 20-25 years has groundmaize daily for at least eight years (with absenceat school allowed for).'The results of the measurement of respirable
dust and quartz are shown in table 3. Anappreciable though low concentration ofrespirable quartz was liberated during grindingwith sandstone but not with dolerite or duringstamping. The time weighted averages derivedfrom these values are compared in table 4 withthose found in a well controlled gold mine andthose recommended by the United StatesNational Institute for Occupational Safety andHealth'6 and the World Health Organisation."7The most exposed maize grinder was exposedto time weighted averages for quartz similar tothose of the least exposed gold miner. Thesevalues are well within the recommended limitsfor time weighted averages of industrial quartzexposure. The total respirable dust concentra-tions during maize grinding, however,approach those of the dustiest mine activitiesand often exceed the recommended industrialtime weighted averages.X ray diffraction of the sandstone grinding
rock showed multiple quartz peaks. Thin sec-tion microscopy showed a granular,unmetamorphosed rock composed of almost100% quartz. The pore spaces were filled withdetrital material, and the rock was extensivelyweathered. X ray diffraction of the doleritegrinding rock showed peaks corresponding toconstituents of plagioclase, which is an igneousrock containing little or no free silica. Thinsection microscopy showed a fine grained rockcomposed of60% plagioclase, 40% augite, andless than 1% oxides. The crystalline texturewas closely knit (that is, with no pore spaces),indicating a very resilient rock. No quartz waspresent. Analysis of maize ground with thesandstone rock confirmed multiple peaksrepresenting quartz, whereas that ground withdolerite showed no quartz or plagioclase peaksbut large numbers of low intensity peaks sug-gesting inorganic material. "Stamp mealies"contained neither.
Electron microscopy of dust trapped in sam-
338
06I* 'S 1: ".
04 t
on March 19, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.334 on 1 M
ay 1991. Dow
nloaded from

Hut lung: a domestically acquired pneumoconiosis of mixed aetiology in rural women
Table 3 Domestic respirable dust and quartz concentrations
Grinding Air volume Dust weight Respirable dust % Respirabletime (min) (m3) (mg) (mg/m3) quartz quartz (mg/rm3)
SandstonePS 40 0-076 023 303 32 0097SS60 0-122 071 582 32 0-186
DoleritePS 158 0324 085 262 09 0024SS 160 0-288 0-98 3 40 0-7 0-024
Stamping* 50 0-098 0-43 4-39 <0 01 <0 004
*Crushing of maize kernals with a pestle and mortar usually made of wood.PS-personal sampler (attached to grinder); SS-standing sampler (placed on tripod).
Table 4 Equivalent time weighted average respirable dust and quartz concentrations inmaize grinders and South African gold miners, with recommended concentrations
Respirable % Respirabledust (mg/m3) quartz quartz (mg/m3)
MAIZE GRINDERS
Sandstone grinderPS 0404 30 0-013SS 0-776 3-0 0-023
Dolerite grinderPS 0-349 0 9 0 0032SS 0-453 0-7 0 0032
GOLD MINERS*Rock driller 0-844 19 0 0-160Blaster 0-649 20-0 0-130Team leader 0-649 13-0 0-032Locomotive driver 0-363 6-0 0-022
RECOMMENDED CONCENTRATIONStNIOSH" (1975): TLV-TWA 0 3 0 10WHO" (1986): TLV-TWA 0-5 0-04
PS, SS-see table 3.TLV-TWA-threshold limit value, time weighted average; NIOSH-National Institute ofOccupational Safety and Health (USA); WHO-World Health Organisation.*From unpublished work by J H Quilliam, Chamber of Mines, Johannesburg, 1978.
plers during grinding with sandstone confirmedquartz particles, dolomite (CaMg (CO3)2), andcomplex particles consisting of aluminium,calcium, chloride, iron, magnesium, potas-sium, and silicone.The average smoke concentration during
cooking (table 5) far exceeded that permitted inindustry.
DiscussionThis study provides additional informationabout the nature of the domestic pneumo-coniosis originally called Transkei silicosis.'Although the typical patient is a rural Transkeiwoman exposed to domestic smoke duringcooking and maize grinding, we found a similarcondition in three rural Namaqua women who
Table 5 Smoke concentrations in a cooking hut at various stages offood preparation*
Average smoke Sampling timeconcentration (mg/rn3) (mm)
do not grind maize but have similar exposure tosmoky wood fuelled stoves in poorly ventilateddwellings. We have confirmed the presence ofrespirable quartz in relation to maize grindingand in the ground maize ofTranskeian women,but the concentrations of atmospheric respir-able quartz were well below the recommendedsafe time weighted averages for quartzexposure. Time weighted averages are con-
sidered to be exposure levels below whichdisease is unlikely to occur over 35 years ofwork." 16 Although sandstone grinding rocksare preferred, they are used less than dolerite,which is more widely available; grinding withdolerite liberates much less quartz. These datasuggest that domestic smoke may be more
important than maize grinding in causing thepneumoconiosis. Our series includes patientsin their 20s, which suggests heavy dustexposure from an early age.
Histological examination of lung tissueconfirmed that there were relatively fewbirefringent particles but many heavilyanthracotic macules similar to those seen insimple coalworkers' pneumoconiosis. Birefrin-gence is not specific and is a feature ofmore than200 types of particles, of which quartz is one.Alveolar macrophages contained dense blackinclusions compatible with carbon and othercomponents of smoke.
Total respirable dust concentrations,approached those seen in the most heavilyexposed gold miners, and smoke concentra-tions were unacceptably high. Women are
exposed to smoke for longer each day than tothe dust of grinding, particularly in coldweather. Airflow limitation is not a feature ofearly simple nodular silicosis and our finding ofairflow obstruction suggests that our patientshad airway disease. This is likely to be theresult of smoke inhalation as it could not beattributed to tobacco smoking or previoustuberculosis. Taken together this evidencesuggests that "Transkei silicosis" is apneumoconiosis ofmixed aetiology, with majorcontributions from "nuisance dust" of in-organic origin and smoke from biomass fuelledfires. Quartz dust appears to contribute in somepatients but probably to a minor degree. Possi-bly certain components of the organic maizedust inhaled contribute by causing extrinsicallergic alveolitis. We therefore propose thatthe term "hut lung" should be used for thiscondition, in recognition of its mixed aetiologyand occurrence in other areas of southernAfrica where similar domestic conditionsprevail.The contribution of small amounts of quartz
to mixed dust fibrosis caused by relatively non-fibrogenic inorganic dusts, such as carbon, iron,kaolinite, and feldspar, is well known." 18 Inthis setting the fibrogenesis relates to the quartzcontent of the mixed dust. More detailedstudies will be required to establish whetherwomen with more severe forms of hut lunghave been more exposed to respirable quartz.Another variable might be the young age atwhich thesewomen are first exposed to the dust.Infants secured on the mother's back are inclose proximity to the source of dust during
Cooking on fire made from maize cobs, wood,and cow dung 30 0 20
Dry maize grinding with fire low 7-8 40Fire smouldering with no domestic activity 0 6 32
*Huts poorly ventilated but door open; smoke concentration measured at one minute intervals.
339
on March 19, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.334 on 1 M
ay 1991. Dow
nloaded from

Grobbelaar, Bateman
grinding and food preparation. The role ofprevious tuberculosis also remains to bedefined; several patients in this series hadevidence of previous tuberculous disease. Wemay also speculate whether hut lung predis-poses to the development of tuberculosis, asoccurs with occupational silicosis."The range of clinical manifestations of hut
lung is well illustrated by this study. Mostpatients have a benign form that appears toprogress very slowly over many years ofexposure without causing illness or disability.Most patients had no respiratory symptomsand only mild radiological and physiologicalabnormalities. Attention is usually drawn totheir radiograph when they present withincidental acute bronchitis. Progressivemassive fibrosis develops in a minority and mayprogress to respiratory failure with cor pul-monale and death. The degree of histologicalabnormality noted in this study is almostcertainly an underestimate due to the limitedsize of the transbronchial biopsy specimensobtained at fibreoptic bronchoscopy, themethod used in most of our patients. Thoseobtained at open lung biopsy and at necropsywere the only ones showing silicotic nodules.Given the nature of the radiological changes,larger specimens would be likely to showadvanced histological changes in many morepatients.The bronchoalveolar lavage findings in hut
lung have not been previously described andare of some value in distinguishing this condi-tion from miliary tuberculosis, in which anexcess of lavage fluid lymphocytes is oftenfound.'9 In hut lung a high proportion ofalveolar macrophages are heavily laden withdense inorganic inclusions. Although heavycigarette smokers have similar proportions ofalveolar macrophages containing inclusions,these particles are finer than those found in hutlung.A major clinical dilemma is distinguishing
this disease from miliary tuberculosis, par-ticularly as some patients have both conditions.Palmer and Daynes recommended that allpatients with any possibility of miliarytuberculosis should be given a diagnosis oftuberculosis in the first instance and receivetreatment.' Our study suggests that fibreopticbronchoscopy and bronchoalveolar lavageshould facilitate accurate diagnosis and obviatethe need for a therapeutic trial of antituber-culous treatment. In a rural setting, wherethese patients are most commonly encounteredand where facilities for fibreoptic bronchoscopyare usually not available, recognising that hutlung often presents as acute bronchitis thatsettles rapidly with antibiotics should helpmanagement. Inpatient assessment is essentialuntil the results of sputum and other tests areknown. Empirical treatment with antituber-culous drugs is nevertheless often necessarybecause of the serious consequences of nottreating miliary tuberculosis.We conclude that hut lung occurs as a result
of exposure to both non-quartz and quartz
containing dusts as well as smoke from biomassfuelled fires. The radiological appearance is thatof pneumoconiosis and histologically it rangesfrom simple anthracosis to progressive massivefibrosis. Airflow limitation and reduced carbonmonoxide transfer factor are common andappear to be independent of the effects ofsmoking and previous tuberculosis. Patientsare generally symptom free. A few casesprogress to cor pulmonale and death. Bron-choalveolar lavage fluid, bronchial brushings,and transbronchial lung biopsy specimens mayhelp to distinguish hut lung from miliarytuberculosis. Preventive campaigns in ruralareas are needed, focusing on improved ven-tilation of cooking huts through the use ofchimneys, general reduction of nuisance dustand exposure, and grinding with quartz freerock or preferably mechanised grinders. Suchmeasures need to be applied in all rural com-munities practising similar traditional cookingmethods.
We acknowledge financial assistance from the South AfricanMedical Research Council and the University ofCapeTown staffresearch fund. We are indebted to staff nurses P Mdlatu and NNongowuza, who acted as interpreter and guide respectively;Mr R E G Rendall of the National Centre for OccupationalHealth, Johannesburg, for assistance with the atmosphericsampling and analysis; Dr D J G Harloe (department ofpathology, University of Cape Town) for reviewing the patho-logical specimens; and Mr C Skinner and Professor A M Read ofthe department of geology, University of Cape Town, foranalysing the rock and maize samples.
I Palmer PES, Daynes WG. Transkei silicosis. S Afr Med J1967;41:1 182-8.
2 Van der Walt E, Kloppers PJ, Solleder G. Disease patternsin Transkei and Ciskei. S Afr Med J 1983;63:568-70.
3 Daynes WG. The prevention of Transkei silicosis. S AfrMed J 1973;47:352-3.
4 International Labour Office. Guidelinesfor the use of the ILOinternational classification ofradiography ofpneumoconiosis.Geneva: ILO, 1980. (Occupational Safety and HealthSeries, No 80.)
5 Schoenberg JB, Beck GJ, Bouhuys A. Growth and decay ofpulmonary function in healthy blacks and whites. RespirPhysiol 1978;33:367-93.
6 Cotes JE. Lung function: assessment and application inmedicine. 4th ed. Oxford: Blackwell, 1979:329-97.
7 Grimby G, Soderholm B. Static lung volumes and maximumvoluntary ventilation in adults with a note on physicalfitness. Acta Med Scand 1963;173:199-206.
8 Turner-Warwick ME, Haslam PL. Clinical applications ofbronchoalveolar lavage: an interim view. Br J Dis Chest1986;80:105-21.
9 Hamilton RJ, Walton WH. The selective sampling ofrespirable dusts. In: Davies CN, ed. Inhaled particles andvapours. Oxford: Pergamon, 1961:465.
10 Orenstein AJ, ed. Proceedings of the Pneumoconiosis Con-ference in Johannesburg, 1959. London: Churchill, 1960:1-29.
11 Parkes WR. Occupational lung disorders. 2nd ed. London:Butterworths, 1982:31-88, 134-232.
12 Mark EJ. Lung biopsy interpretation. Baltimore: Williamsand Wilkins, 1984:14, 78-85.
13 Kleinerman J, Green F, Harley RA. Pathology standards forcoal workers' pneumoconiosis. Arch Pathol Lab Med1979;103:375-85.
14 Katzenstein AA, Askin FB. Surgical pathology of non-neoplastic lung disease. Philadelphia: Saunders, 1982:84-5.
15 Wolman M. On the use of polarised light in pathology.Pathol Annu 1970;5:381-416.
16 National Institute for Occupational Safety and Health.Criteria for a recommended standard occupational exposureto crystalline silica. Washington DC: Department ofHealth, Education and Welfare, 1975:75-120.
17 World Health Organisation. Recommended Health-BasedLimits in Occupational Exposure to Selected Mineral Dusts(silica, coal). Geneva: WHO, 1986:734.
18 Martin JC, Daniel-Moussard H, Le Bouffant L, Policard A.The role of quartz in the development of coal worker'spneumoconiosis. Ann NY Acad Sci 1972;200:127-41.
19 Bateman ED, Ainslie GM. Bronchoalveolar lavage-awindow to the lung. S Afr Med J 1990;77:550-2.
340
on March 19, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.334 on 1 M
ay 1991. Dow
nloaded from