thoracoscopic talc insufflation versus talc slurry for symptomatic malignant pleural effusion
TRANSCRIPT

Thoracoscopic Talc InsufflationVersus Talc Slurryfor Symptomatic Malignant Pleural EffusionAnthony P. C. Yim, MD, Anthony T. C. Chan, MB, BS, Tak Wai Lee, FRCS(E),Innes Y. P. Wan, MB, ChB, and Jonathan K. S. Ho, MDDivisionof CardiothoracicSurgery,Departmentof Surgery,andDepartmentof ClinicalOncology,The Chinese University ofHong Kong Prince of Wales Hospital, Shatin, Hong Kong
Background. Talc has been generally accepted to be themost effectivesclerosantfor chemicalpleurodesis,althoughthe optimal route of administration remains unclear.
Methods. We designed a prospective, randomizedstudy to compare video-assisted thoracoscopic talc insuf-flation with bedside talc slurry in the treatment of ma-lignant pleural effusion. From September 1993 to Novem-ber 1995, 57 patients were recruited and randomized toeither video-assisted thoracoscopic talc insufflation un-der general anesthesia (n = 28) or talc slurry by thebedside (n = 29). Patients with poor general condition(Karnofsky score less than 30~0), poor pulmonary func-tion (forced expiatory volume in 1 second less than 0.5L), or trapped lungs were excluded from this study. Fivegrams of purified talc was used for either video-assistedthoracoscopic talc insufflation or talc slurry.
Malignant pleural effusion is a common condition,which is often disabling and could be very difficult
to treat. It represents a terminal condition with shortmedian survival (in terms of months), and the goal oftreatment is palliation [1]. Systemic chemotherapy isoccasionally useful for breast and small cell lung carci-noma, but local therapy remains the mainstay of treat-ment. Talc has been identified as an effective sclerosantfor chemical pleurodesis [2], although the optimal routeof administration (dusting [3], “slurry” [4], “poudrage”[5]) remains unclear. More recently, video-assisted tho-racoscopic talc insufflation (VT) has been shown to be asafe and effective approach in controlling malignantpleural effusion [6, 7]. We designed a prospective, ran-domized study to compare this approach with conven-tional bedside talc slurry (TS). Our results from a singleinstitution form the basis of this article.
Material and Methods
From September 1993 to November 1995,79 patients withestablished, symptomatic malignant pleural effusionwere referred to us for treatment. Eleven patients, how-ever, were excluded from this study because of eitherpoor general condition (Karnofsky score less than 30%)
Accepted for publication July 22, 1996.
Address reprint requests to Dr Yim, Division of Cardiothoracic Surge~,Department of Surge~, Prince of Wales Hospital, Shatin, NT Hong Kong.
01996 by The Society of Thoracic SurgeonsPublished by Elsevier Science Inc
Results. There was no statistically significant differ-ence between the two groups of patients with respect toage, sex ratio, chest drainage duration, postproceduralhospital stay, parenteral narcotics requirement, compli-cations, or procedure failure (ie, recurrence).
Conclusions. Video-assisted thoracoscopic talc insuf-flation has not been shown to be a superior approachcompared with talc slurry in our study. Because theformer demands more resources, we advocate that talcslurry should be considered as the procedure of choice inthe treatment of symptomatic malignant pleural effusionin patients who do not have trapped lungs.
(Ann ThoracSurg1996;62:1655-8)
[8] or poor pulmonary function (forced expiatory volumein 1 second less than 0.5 L). Seven patients were furtherexcluded when trapped lung was revealed after eitherchest tube drainage or large-volume thoracocentesis. Inaddition, 4 patients who received chemotherapy or radi-ation therapy within 6 months before the diagnosis ofmalignant effusion were excluded from the study. Thisleft 57 patients (20 men and 37 women with age rangingfrom 50 to 86 years) to be randomized for VT undergeneral anesthesia (n= 28) or TS by the bedside (n = 29).We were careful in excluding patients whose dyspneawas due to tumor replacement of lung parenchymarather than to effusion. We only selected those patientswhose dyspnea improved after tube thoracostomy orlarge-volume thoracocentesis. Permission for the studywas obtained from the Hospital Review Board, and fullconsent was obtained from the patients. Our techniquesare briefly described below.
Video-AssistedThoracoscopicTalc InsulationWe modified the technique previously described usinglocal anesthesia by Hartman and associates [6]. Theprocedure was performed under general anesthesia withselective one-lung ventilation and the patient in thelateral decubitus position with the table flexed at 30degrees [9]. We routinely use a 10-mm operating tele-scope to minimize the number of ports made [10]. If thepatient already came with a chest drain, we would usethe drain site for the introduction of the telescope.
0003-4975/96/$15.00PII S0003-4975(96)00808-9
1656 YIM ET ALTALC INSUFFLATION VERSUS SLURRY
Ann Thorac Surg1996;62:1655-8
Otherwise, needle aspiration was undertaken to deter-mine the location of the fluid. We normally prefer tointroduce the telescope low down in the chest (usuallyover the sixth or seventh intercostal space unless thediaphragm was shown or suspected to be elevated). Anyresidual pleural fluid was aspirated. Loculations werebroken down. Fibrinous adhesions were taken down,whereas dense fibrous adhesions were selectively di-vided. Five grams of purified talc (Halewood Chemicals,Middlesex, UK) sterilized by dry heat was then insuf-flated into the chest to evenly cover the entire visceraland parietal surfaces. Initially we used a special talcatomizer (K. Storz, Culver City, CA), but we now preferusing a mucus extractor (UnoPlast, Hundested, Den-mark) connected to a 50-mL syringe, which we havefound to be simple, cheap, and reliable. A 28F chest drainwas left in situ (placement of which was visually guided)and connected to 15 cm H20 suction. The lung wasconfirmed to be fully reexpanded before withdrawal ofthe scope. The drain was connected to 15 cm H20 suctionand removed when the output was less than 50 mL in 24hours.
Talc SlurryOur technique was similar to that advocated by Webband colleagues [4]. Five grams of purified talc (HalewoodChemicals) was mixed with 50 mL of normal salinesolution and 10 mL of 2Y0lidocaine to form a suspension,which was then instilled through the chest drain. Thedrain was clamped for 2 hours and the patient turned indifferent positions. The drain was then reconnected to15 cm H20 suction and removed when the output wasless than 50 mL in 24 hours.
Follow-upAll the patients were prospectively followed up. Particu-lar attention was paid to the postprocedural chest drain-age duration, hospital stay, parenteral meperidine re-quirement, and periprocedural complications. Afterdischarge, the patients were regularly seen in the clinic at6-week intervals for the first 4% months and then every 3months. Any procedural failure in terms of radiologicevidence of fluid reaccumulation was noted. Telephoneinterviews with the patients were made as required torecord changes in symptoms. Differences between thetwo groups were analyzed using Mann-Whitney U tests.
Results
Our results are summarized in Table 1. There was nostatistical difference in the demographics of the patientsbetween the VT and TS groups in terms of age, sex ratio,and underlying pathology. There was no procedure-related mortality in either group. We found no differ-ences between the two groups in terms of chest drainagedurations, hospital stays, or parenteral meperidine re-quirement.
Three complications were encountered in the VTgroup: reexpansion pulmona~ edema, persistent airleak, and tumor recurrence at a port site. (1) Reexpansion
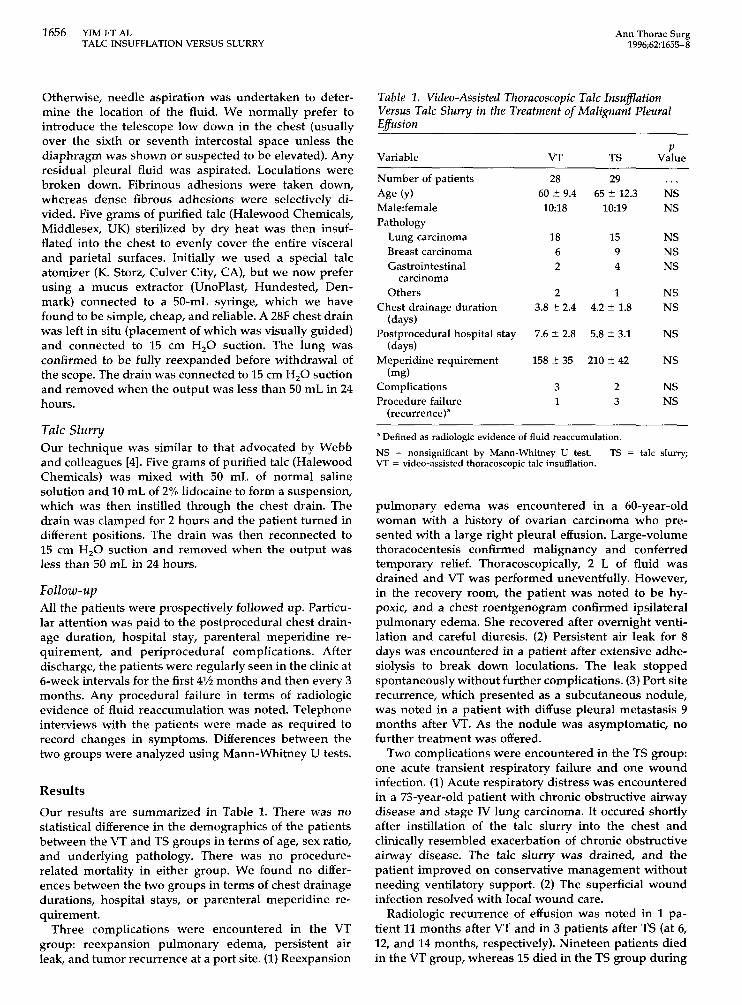
Table 1. Video-AssisfedThoracoscopicTalc Insuj7ationVersus Talc Slurry in the Treatmentof Malignanf PleuralEffusion
Variable VT TS Va?ue
Number of patientsAge (y)Male:femalePathology
Lung carcinomaBreast carcinomaGastrointestinal
carcinomaOthers
Chest drainage duration(days)
Postprocedural hospital stay(days)
Meperidine requirement(mg)
ComplicationsProcedure failure
(recurrence)’
28613~ 9,4
10:18
1862
7.6 ~ 2.8
158 z 35
31
2965 ~ 12,3
10:19
1594
23
. . .NSNS
NSNSNS
NSNS
NS
NS
NSNS
a Defined as radiologic evidence of fluid reaccumulation.
NS = nonsignificant by Mann-Whitney U test. TS = talc slurry;VT = video-assisted thoracoscopic talc insufflation.
pulmonary edema was encountered in a 60-year-oldwoman with a history of ovarian carcinoma who pre-sented with a large right pleural effusion. Large-volumethoracocentesis confirmed malignancy and conferredtemporary relief. Thoracoscopically, 2 L of fluid wasdrained and VT was performed uneventfully. However,in the recovery room, the patient was noted to be hy-poxic, and a chest roentgenogram confirmed ipsilateralpulmona~ edema. She recovered after overnight venti-lation and careful diuresis. (2) Persistent air leak for 8days was encountered in a patient after extensive adhe-siolysis to break down loculations. The leak stoppedspontaneously without further complications. (3) Port siterecurrence, which presented as a subcutaneous noduIe,was noted in a patient with diffuse pleural metastasis 9months after VT. As the nodule was asymptomatic, nofurther treatment was offered.
Two complications were encountered in the TS group:one acute transient respiratory failure and one woundinfection. (1) Acute respiratory distress was encounteredin a 73-year-old patient with chronic obstructive airwaydisease and stage IV lung carcinoma. It occured shortlyafter instillation of the talc slurry into the chest andclinically resembled exacerbation of chronic obstructiveairway disease. The talc slurry was drained, and thepatient improved on conservative management withoutneeding ventilator support. (2) The superficial woundinfection resolved with local wound care.
Radiologic recurrence of effusion was noted in 1 pa-tient 11 months after VT and in 3 patients after TS (at 6,12, and 14 months, respectively). Nineteen patients diedin the VT group, whereas 15 died in the TS group during
———

AnnThoracSurg1996;62:1655–8
YIMETAL 1657TALCINSUFFLATIONVERSUSSLURRY
follow-up without evidence of fluid reaccumulation. Themean follow-up is 10 months among the survivors (range,4 to 16 months). Of the 4 patients with radiologic recur-rence of effusion,only 1 patient (in the TS group) had heractivity limited by dyspnea. She underwent repeat tubethoracostomy and TS treatment without further recur-rence, until her death 2 months later.
Comment
There is now a wealth of literature on the treatment ofsymptomatic malignant pleural effusion, although theoptimal therapy remains unclear [1]. Options includerepeated therapeutic thoracocentesis, tube thoracostomyand sclerotherapy, thoracoscopic talc insufflation, me-chanical pleurodesis, pleuroperitoneal shunt, and pleu-rectomy. We normally reserve repeated thoracocentesisto those who are severely disabled and require continu-ous hospitalization (Karnofsky score less than 307.) [8] asrapid reaccumulation, protein depletion, and risk ofempyema occur with this treatment. On the other hand,pleurectomy carries with it substantial morbidity andmortality [11] and is hard to justify for a palliativeprocedure. Pleuropentoneal shunt has been shown to beeffective [12], but it requires a very compliant patient whoneeds to manually pump 400 times a day. Moreover,there is a risk of shunt occlusion by blood clots or fibrindebris [13]. We therefore have reserved this approach topatients with severely (more than 25% fixed pneumotho-rax) trapped lung.
Of all the sclerosants available, talc is generally con-sidered the agent of choice because of its good trackrecord (more than 90Y0 success rate), wide availability,and low cost [2]. The possible harmful long-term effectsof talc [14] seem academic in this group of patients withlimited survival. Acute respiratory failure [15] and death[16] have been anecdotally reported with TS [15] orinsufllation [16]. We encountered 1 case of acute respira-tory failure with TS in this series. The exact underlyingmechanism remains unclear, even though it maybe doserelated. Kennedy and Sahn [2] recommended a 5-g dose,which is what we use. In the past we tried thoracoscopictalc insufllationunder local anesthesia [6] and found it tobe fairly uncomfortable for the patients. In addition, itwas difllcultto carry out interventions like adhesiolysis inpatients who were awake with ventilating lungs.
Patients with diffuse pleural metastasis are at risk oftumor seeding at thoracoscopy port sites. Fortunately,this is relatively uncommon: 6 of 215 patients reported byBoutin and associates [17], 2 of 30 patients reported byDavidson and colleagues [18], and 2 of our patients (1 isnot in this series [19]). We recommend observation if theport site recurrence is asymptomatic in view of thepatient’s short life expectancy; otherwise, local irradia-tion has been shown to provide good palliation [18].
Video-assisted thoracic surgery has provided an alter-native approach in the management of a variety ofthoracic conditions. Thoracoscopic talc insufflation formalignant effisions under local [6] or general anesthesia[71 has been shown to be safe and effective; here we
report a randomized, prospective comparison betweenthis approach and conventional TS.
We have not shown in our study any statisticallysignificant difference between TS and VT in terms ofhospital stay, analgesic requirement, complications, orprocedure failures. It is important to note that of the 4patients who had fluid reaccumulation, only 1 was symp-tomatic enough to require further treatment. We ac-knowledge that our sample size is small, but we empha-size that we are comparing two treatment modalities withthe goal of palliation for a condition with very limitedsurvival. A multicenter trial is underway, and it will beinteresting to see if the collective experience is in agree-ment with our own.
There are two further points of note. First, in this study,we are focusing only on those patients with no radiologicevidence of trapped lungs. For patients with a minordegree of trapped lungs (less than 25~0 fixed pneumo-thorax), thoracoscopic decortication has been shown tobe useful in achieving lung reexpansion [71. Second, weare aware of the weakness in our study in the lack ofdocumentation of patients’ quality of life after eitherprocedure. We have encountered problems in usingstandard questionnaires for our patients: they requiretranslation into Chinese; self evaluation and the visuallinear analogue scale pose difficultiesto those with a lowlevel of education or low performance status [20]; func-tional status is closely influenced by social and psycho-logical factors, which are difficult to quantify; and thequestionnaires have not been externally validated. Weare studying some of these problems.
We have changed our practice as a result of ourfindings. In view of VT demanding more resources(trained thoracoscopists, general anesthesia, operatingroom time), we now advocate TS to be considered as theprocedure of choice for patients with symptomatic ma-lignant effusionwithout trapped lungs. Pleuroperitonealshunt should be considered for those with severelytrapped lung who are likely to comply with handling thedevice. For those patients with minor degrees of trappedlungs (less than 25Y0fixed pneumothorax), the thoraco-scopic approach should be selectively considered [7].
We are grateful to Alex Fun% BA, for data collection andeditorial assistance. This study was supported by UniversityFunds (AIC 1635-23).
References
1. Hausheer FH, Yarbro JW. Diagnosis and treatment of ma-lignant pleural effusions. Semin Oncol 1985;12:54-75.
2. Kennedy L, Sahn SA. Talc pleurodesis for the treatment ofpneumothorax and pleural effusion.Chest 1994;106:1215-22.
3. Adler RH, Sayek I. Treatment of malignant pleural effusion:a method using tube thoracostomy and talc. Ann ThoracSurg 1976;22:8-15.
4. Webb WR, Ozmen V, Moulder PV, Shabahang B, Breaux J.Iodized talc pleurodesis for the treatment of pleural effu-sions. J Thorac Cardiovasc Surg 1992;103:881-6.
5. Nandi P. Recurrent spontaneous pneumothorax: an effectivemethod of talc poudrage. Chest 1980;77:493–5.
1658 YIM ET ALTALC INSUFFLATION VERSUS SLURRY
AnnThorac Surg1996;62:1655-8
6,
7.
8.
9.
10.
11.
12.
13.
Hartman DL, Gaither JM, Kesler KA, Mylet DM, Brown JW,Mathur PN. Comparison of insutllated talc under thoraco-scopic guidance with standard tetracycline and bleomycinpleurodesis for control of malignant pleural ethrsions.J Tho-rac Cardiovasc Surg 1993;105:743-8.Yim APC, Chung SS, Lee TW, Lam C~ Ho JKS. Thoraco-scopic management of malignant pleural effusions. Chest1996;109:1234-8.Karnofsky DA, Burchenal VH. The clinical evaluation ofchemotherapeutic agents in cancer. In: MacLeodCM, ed.Evaluationof chemotherapeuticagents. New York: Colum-bia University Press, 1949:191-205.Yim APC. Minimizing chest wall trauma in video assistedthoracic surgery. J Thorac Cardiovasc Surg 1995;109:1255-6.Yim APC, Ho JKS, Lee TW, Chung SS. Thoracoscopicmanagement of pleural efusions revisited. Aust N Z J Surg1995;65:308-11.Martini N, Bains MS, Beattie EJ. Indications for pleurectomyin malignant etfusion. Cancer 1975;35:734-8.Little AG, Kadowaki MH, Ferguson MK Staszek VM, Skin-ner DB. Pleuroperitoneal shunting: alternative therapy forpleural effusions.Ann Surg 1988;208:443-50.Tsang V, Fernando AC, Goldstraw P. Pleuroperitonealshuntfor recurrent malignantpleuraletfusion.Thorax 1990;45:369-72.
14. Lange P, Mortensen J, Groth S. Lung function 22-35 yearsafter treatment of idiopathic spontaneous pneumothoraxwith talc poudrage or simple drainage. Thorax 1988;43:559-61.
15. Bouchama A, Chastre J, Gandichet A, Soler P, Gibert C.Acute pneumonitis with bilateral pleural effusion after talcpleurodesis. Chest 1984;86:795-7.
16. Todd TRJ, Delarue NC, Ilves ~ Pearson FG, Cooper JD. Talcpoudrage for malignant pleural effusion [Abstract]. Chest1980;78:542-3.
17. Boutin C, Viallat JR, Cargnino P, Farisse P. Thoracoscopy inmalignant pleural etfi.rsions.Ann Rev Respir Dis 1981;124:588-92.
18. Davidson AC, George RJ, Sheldon CD, Sinha G, Corrin B,Geddes DM. Thoracoscopy: assessment of a physician ser-vice and comparison of a flexible bronchoscope used as athoracoscope with a rigid thoracoscope. Thorax 1988;43:327-32.
19. Yim APC. Port site recurrence following video assistedthoracoscopic surgery. Surg Endosc 1995;9:1133-5.
20. Ballatori E, Roila F, Basurto C, et al. Reliabilityandvalidityofa quality of life questionnaire in cancer patients. Eur JCancer 1993;29A(Suppl):S63-9.
INVITED COMMENTARY
The very nice study by Dr Yim and his associates at-tempts to evaluate the optimal route of administration oftalc for pleurodesis. Talc has been demonstrated bynumerous studies to be effective in 907. or better ofmalignant effusions whether given by insufllation or byinjection through a chest tube. With this high degree ofeffectiveness, a very large number of cases would berequired to demonstrate any significant difference. Thus,it is not surprising that in this relatively small number ofpatients (57) no differences would be demonstrated. Yimand associates found the hospital stay to be the same inboth groups and were not able to evaluate costs in theirstate hospital system.
My colleagues and I use both methods, and in morethan 110 cases of slurry injection for both malignant andbenign effusions, the very few failures have usually beenbecause we used the slurry before adequate drainagehad been achieved (less than 100 mL/day) or there wereundetected loculations. We have modified our formerinstillation technique by increasing the volume of theslurry with the same 5 g of purified talc to more than
200 mL to assure rapid coating of all pleural surfaces. Wehave used thoracoscopic talc insutllation in all caseswhere thoracoscopic visualization was needed for biopsy,adhesiolysis, or some other interventional procedure.Here again our results with achieving pleurodesis withtalc insufflationhave been close to 100Yo.
We continue to use tube instillation in general becauseit is a much simpler bedside technique that does notrequire anesthesia and is tremendously cheaper in ourhospitals than video thoracoscopy. We believe videothoracoscopy should be used only for requisite diagnos-tic or therapeutic procedures rather than just instillationof the talc.
WatisR. Webb, MD
Departmentof SurgeryLouisianaState UniversitySchoolof Medicine1542 TulaneAveNew Orleans,LA 70112
. —.