the wound care pathway
TRANSCRIPT
The Wound Care PathwayA practical and evidence-based approach towards wound healing

What is a chronic wound? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 04
STEP 1.
Assessing a person with a chronic wound . . . . . . . . . 06
STEP 2.
Developing a treatment plan . . . . . . . . . . . . . . . . . . . . . . . . . 08
STEP 3.
Managing & treating a chronic wound . . . . . . . . . . . . . 12
STEP 4.
Choosing a dressing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
STEP 5.
Monitoring patient & wound progression . . . . . . . . . . 22
When to refer or consult a specialist . . . . . . . . . . . 24
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Chronic wounds are a huge burden . They are challenging for patients to live with . Challenging for doctors and nurses to manage . And expensive for society to treat .
The Wound Care Pathway is an educational tool that offers solutions to these challenges and provides the guidance for healthcare professionals working with wounds to provide the right treatment for your patients .
Developed with feedback and input from over 2200 healthcare professionals working in the field of wound care, it offers a practical, evidence based approach to managing chronic wounds .
AUTHORS
Dr . David Keast, Canada | Mary Brennan, WOCN, USA | Dr . Marcelo Liberato, Brazil | Dr . Hubert Vuagnat, Switzerland | Dr . Caroline Dowsett, United Kingdom | Terry Swanson, Nurse practitioner, Australia | Dr . Tonny Karlsmark, Denmark | Dr . Alessandro Greco, Italy | Dr . Christian Münter, Germany | Dr . José Luis Lázaro-Martínez, Spain
Table of contentThe Wound Care Pathway – a step-by-step approach towards wound healing
Scan here to learn more
When to refer
3
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.

Chronic wounds are defined as wounds that have not healed in 30-days despite best practice intervention or are not expected to heal within 4 – 6 weeks, regardless of their aetiology .
While acute wounds are not the focus of these recommendations, always keep in mind that acute wounds can turn into chronic wounds if proper wound treatment is not followed .
Chronic wound care should focus on providing an optimal healing environment and managing the gap between the wound bed and the dressing, to prevent complications that could increase healing time and lead to loss of limb or death .
The goal of chronic wound care is to heal the wound and achieve fewer days with wounds
What is achronic wound?
4
Venous Leg Ulcer Diabetic Foot Ulcer Pressure Ulcer Surgical wound
Wound assessment should include both a holistic assessment of the patient and the wound . This should be repeated every 4 weeks to monitor healing progression or if a significant change in condition is present .
Holistic wound assessment considers a wide range of factors beyond simply the biology of the wound .
This requires coordination among multidisciplinary care providers and specialists .
STEP 1 .
Assessing a person with a chronic wound
Remember the wound is on a patient, the patient is in their environment and the environment is part of a health care system.
When to refer
5
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
The goal for chronic wounds, regardless of diagnosis or cause, should always be to heal the wound. In the case of non-healable wounds (i.e. inadequate vasculature) or palliative wounds, the treatment pathway recommendations still apply.
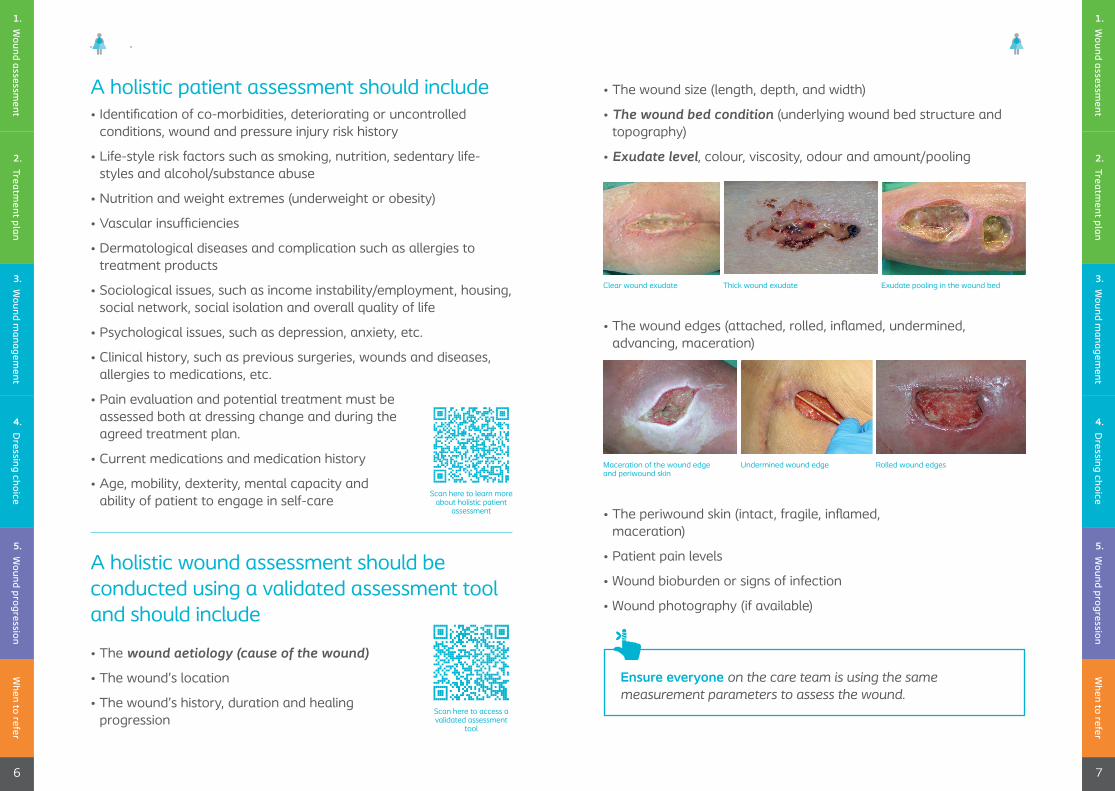
A holistic patient assessment should include • Identification of co-morbidities, deteriorating or uncontrolled
conditions, wound and pressure injury risk history
• Life-style risk factors such as smoking, nutrition, sedentary life-styles and alcohol/substance abuse
• Nutrition and weight extremes (underweight or obesity)
• Vascular insufficiencies
• Dermatological diseases and complication such as allergies to treatment products
• Sociological issues, such as income instability/employment, housing, social network, social isolation and overall quality of life
• Psychological issues, such as depression, anxiety, etc .
• Clinical history, such as previous surgeries, wounds and diseases, allergies to medications, etc .
• Pain evaluation and potential treatment must be assessed both at dressing change and during the agreed treatment plan .
• Current medications and medication history
• Age, mobility, dexterity, mental capacity and ability of patient to engage in self-care
A holistic wound assessment should be conducted using a validated assessment tool and should include
• The wound aetiology (cause of the wound)
• The wound’s location
• The wound’s history, duration and healing progression
• The wound edges (attached, rolled, inflamed, undermined, advancing, maceration)
• The periwound skin (intact, fragile, inflamed, maceration)
• Patient pain levels
• Wound bioburden or signs of infection
• Wound photography (if available)
Ensure everyone on the care team is using the same measurement parameters to assess the wound.
Clear wound exudate
Maceration of the wound edge and periwound skin
Scan here to access a validated assessment
tool
Scan here to learn more about holistic patient
assessment
Thick wound exudate
Undermined wound edge
Exudate pooling in the wound bed
Rolled wound edges
• The wound size (length, depth, and width)
• The wound bed condition (underlying wound bed structure and topography)
• Exudate level, colour, viscosity, odour and amount/pooling
When to refer
7
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
When to refer
6
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
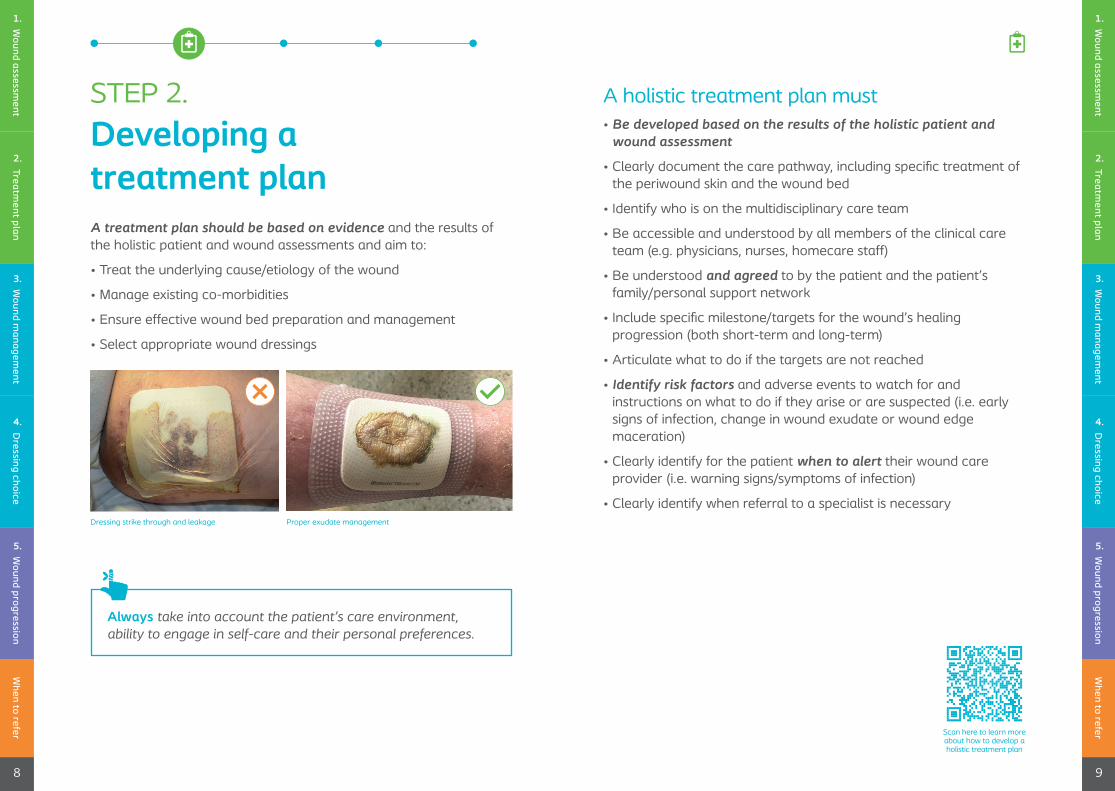
A treatment plan should be based on evidence and the results of the holistic patient and wound assessments and aim to:
• Treat the underlying cause/etiology of the wound
• Manage existing co-morbidities
• Ensure effective wound bed preparation and management
• Select appropriate wound dressings
A holistic treatment plan must• Be developed based on the results of the holistic patient and
wound assessment
• Clearly document the care pathway, including specific treatment of the periwound skin and the wound bed
• Identify who is on the multidisciplinary care team
• Be accessible and understood by all members of the clinical care team (e .g . physicians, nurses, homecare staff)
• Be understood and agreed to by the patient and the patient’s family/personal support network
• Include specific milestone/targets for the wound’s healing progression (both short-term and long-term)
• Articulate what to do if the targets are not reached
• Identify risk factors and adverse events to watch for and instructions on what to do if they arise or are suspected (i .e . early signs of infection, change in wound exudate or wound edge maceration)
• Clearly identify for the patient when to alert their wound care provider (i .e . warning signs/symptoms of infection)
• Clearly identify when referral to a specialist is necessaryDressing strike through and leakage Proper exudate management
Scan here to learn more about how to develop a holistic treatment plan
Always take into account the patient’s care environment, ability to engage in self-care and their personal preferences.
When to refer
9
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
When to refer
8
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
STEP 2 .
Developing a treatment plan
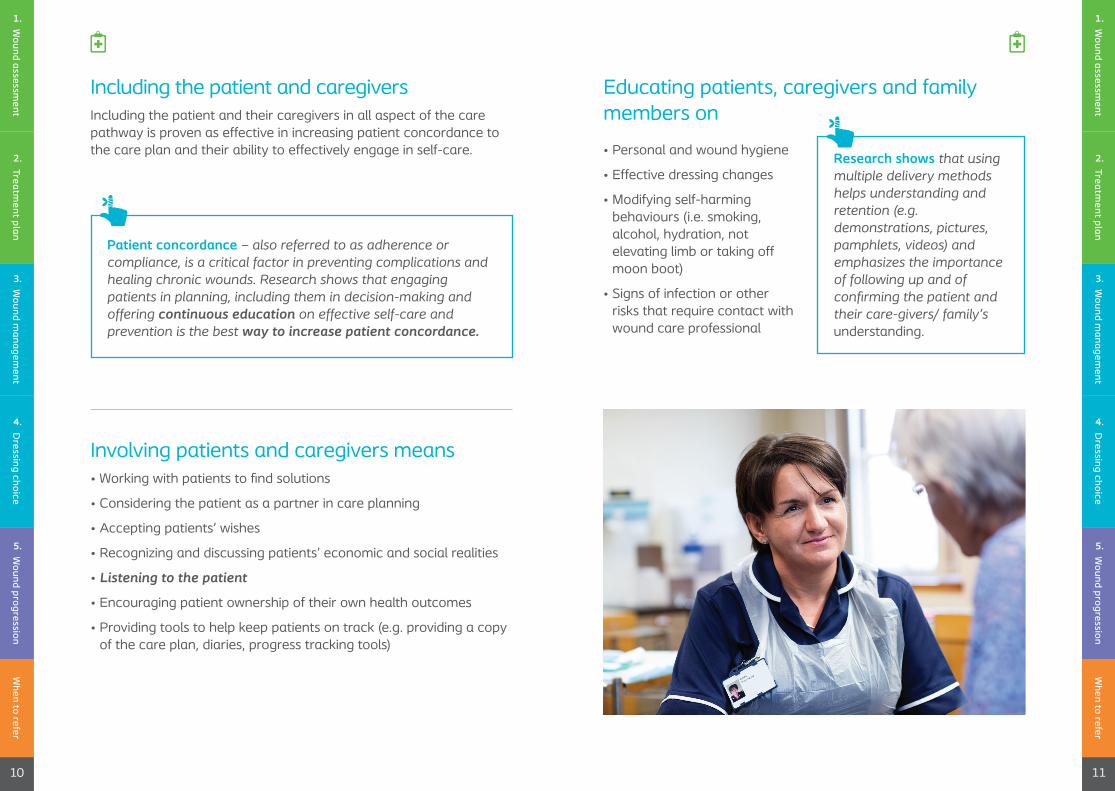
Involving patients and caregivers means• Working with patients to find solutions
• Considering the patient as a partner in care planning
• Accepting patients’ wishes
• Recognizing and discussing patients’ economic and social realities
• Listening to the patient
• Encouraging patient ownership of their own health outcomes
• Providing tools to help keep patients on track (e .g . providing a copy of the care plan, diaries, progress tracking tools)
• Personal and wound hygiene
• Effective dressing changes
• Modifying self-harming behaviours (i .e . smoking, alcohol, hydration, not elevating limb or taking off moon boot)
• Signs of infection or other risks that require contact with wound care professional
Including the patient and caregiversIncluding the patient and their caregivers in all aspect of the care pathway is proven as effective in increasing patient concordance to the care plan and their ability to effectively engage in self-care .
When to refer
11
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
When to refer
10
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
Educating patients, caregivers and family members on
Patient concordance – also referred to as adherence or compliance, is a critical factor in preventing complications and healing chronic wounds. Research shows that engaging patients in planning, including them in decision-making and offering continuous education on effective self-care and prevention is the best way to increase patient concordance.
Research shows that using multiple delivery methods helps understanding and retention (e.g. demonstrations, pictures, pamphlets, videos) and emphasizes the importance of following up and of confirming the patient and their care-givers/ family’s understanding .
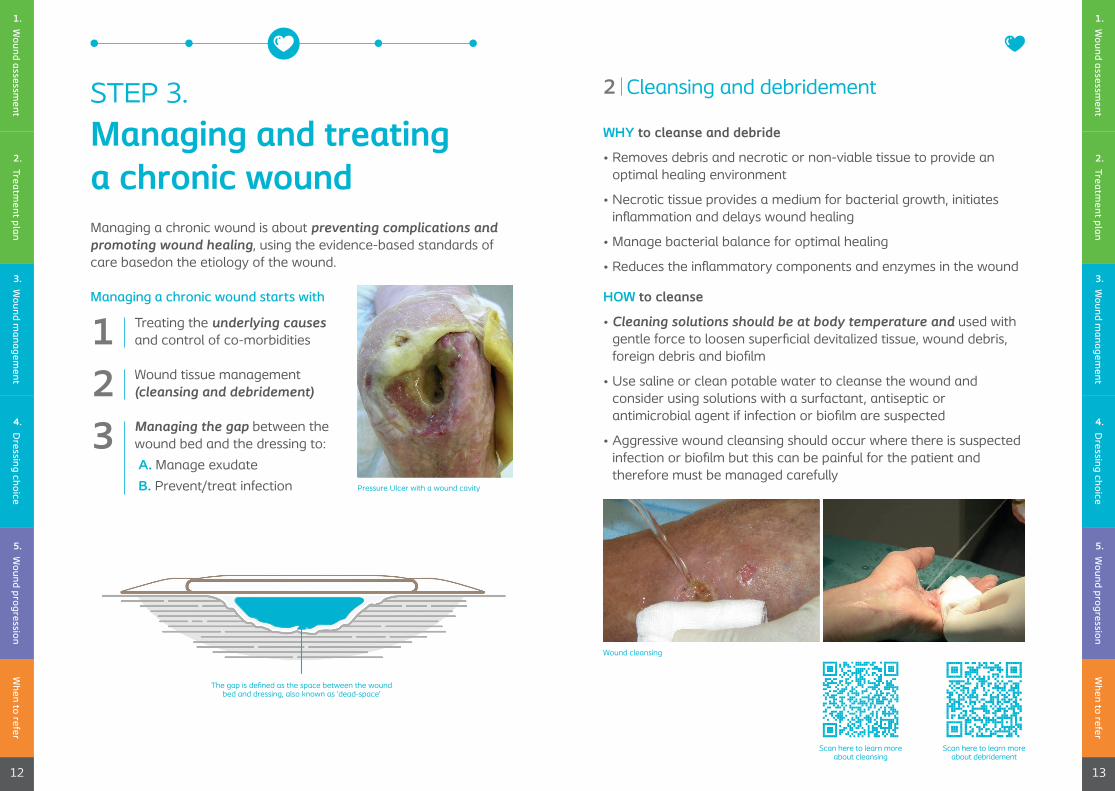
Managing a chronic wound is about preventing complications andpromoting wound healing, using the evidence-based standards of care basedon the etiology of the wound .
Managing a chronic wound starts with
Treating the underlying causes and control of co-morbidities
Wound tissue management (cleansing and debridement)
Managing the gap between the wound bed and the dressing to:
A. Manage exudate
B. Prevent/treat infection
WHY to cleanse and debride
• Removes debris and necrotic or non-viable tissue to provide an optimal healing environment
• Necrotic tissue provides a medium for bacterial growth, initiates inflammation and delays wound healing
• Manage bacterial balance for optimal healing
• Reduces the inflammatory components and enzymes in the wound
HOW to cleanse
• Cleaning solutions should be at body temperature and used with gentle force to loosen superficial devitalized tissue, wound debris, foreign debris and biofilm
• Use saline or clean potable water to cleanse the wound and consider using solutions with a surfactant, antiseptic or antimicrobial agent if infection or biofilm are suspected
• Aggressive wound cleansing should occur where there is suspected infection or biofilm but this can be painful for the patient and therefore must be managed carefully
Wound cleansing
Pressure Ulcer with a wound cavity
The gap is defined as the space between the wound bed and dressing, also known as ‘dead-space’
Scan here to learn more about debridement
Scan here to learn more about cleansing
When to refer
13
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
When to refer
12
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
STEP 3 .
Managing and treating a chronic wound
12
2
3
Cleansing and debridement
HOW to debride
• Mechanical debridement includes therapeutic irrigation with a force of 4-15psi . Debridement pads or wipes can also be used to debride
• Conservative sharp, surgical, low frequency ultrasound, chemical and autolytic debridement must be done by a qualified wound care specialist and is used to remove devitalized or non-viable tissue, bacteria and contaminants
• Debriding a wound that does not have adequate vascular supply is not recommended
• Aggressive debridement must be considered when there are signs of infection or biofilm, but can cause considerable pain for the patient . Refer to a wound care specialist if aggressive debridement is outside of your scope of practice
• Cleanse the wound again after debridement
WHY is managing exudate important
• Exudate is defined as the fluid that leaks from a wound and is the result of the inflammatory process . Exudate is usually clear or amber coloured
• Exudate production is a normal feature of healing wounds but over or under production of exudate or exudate pooling can delay healing
HOW to manage exudate
• Assessing systemic reasons for over or under production of exudate (e .g . inadequate compression therapy for lower extremity wounds, lower limb oedema, nutrition or dehydration)
• Effective wound bed preparation
• Use of appropriate dressings that fill the gap
• Adapt the frequency of dressing changes
WHAT is recommended
• Effective wound bed preparation (cleansing and debridement) are key strategies to optimize wound healing
• Cleanse the wound bed at every dressing change to remove devitalized tissue, debris and biofilm, with potable water, saline, surfactant, antiseptic or antimicrobial solution
• Cleanse the periwound skin at every dressing change to remove dead skin and to decontaminate the area around the wound, removing further sources of contamination
3A
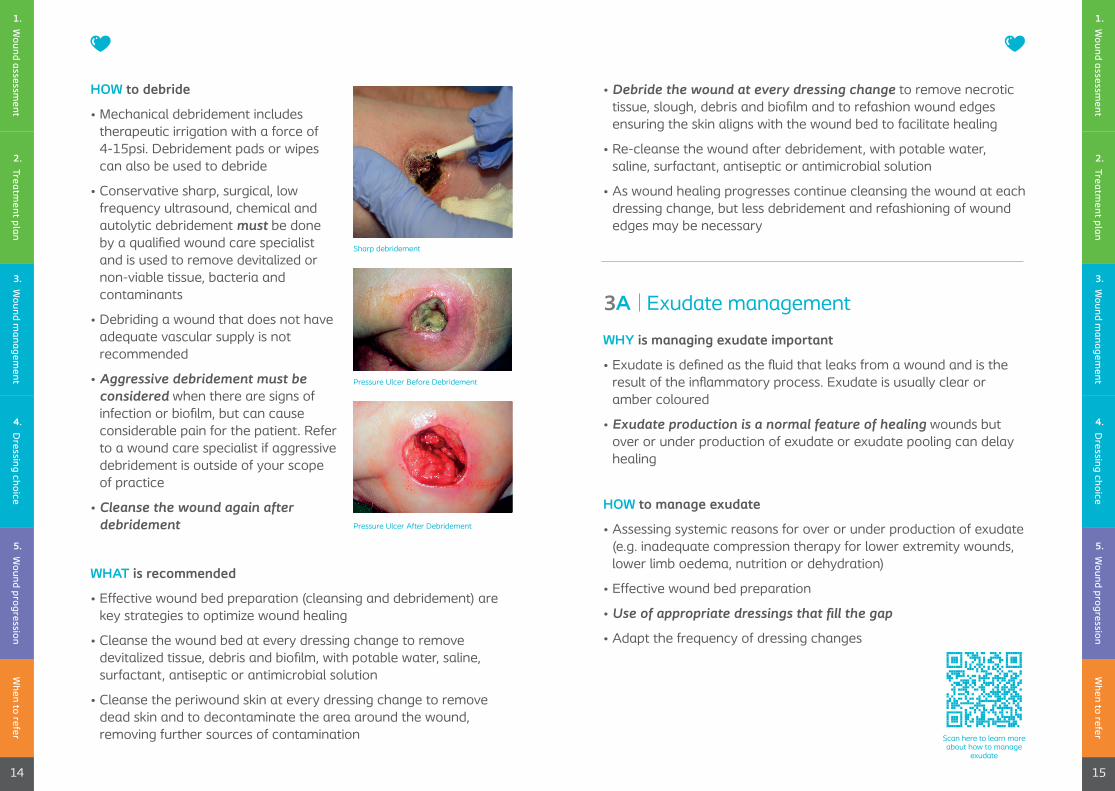
Sharp debridement
Pressure Ulcer Before Debridement
Pressure Ulcer After Debridement
• Debride the wound at every dressing change to remove necrotic tissue, slough, debris and biofilm and to refashion wound edges ensuring the skin aligns with the wound bed to facilitate healing
• Re-cleanse the wound after debridement, with potable water, saline, surfactant, antiseptic or antimicrobial solution
• As wound healing progresses continue cleansing the wound at each dressing change, but less debridement and refashioning of wound edges may be necessary
Scan here to learn more about how to manage
exudate
When to refer
15
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
When to refer
14
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
Exudate management
WHAT is recommended
When removing a wound dressing, always note when the dressing was last changed, inspect the dressing for any leakage, assess how full the dressing is and the type and amount of exudate that is in both the wound and dressing .
Assess the wound bed, wound edges and periwound skin for improvement or complications .
To create an optimal moisture balance in chronic wounds, health care professionals must effectively analyze the wound and wound exudate and use thatinformation to determine the best dressing choice and frequency of dressing changes .
Educate patient on effective exudate management techniques (compression, elevation, hydration, frequency of dressing changes, etc .)
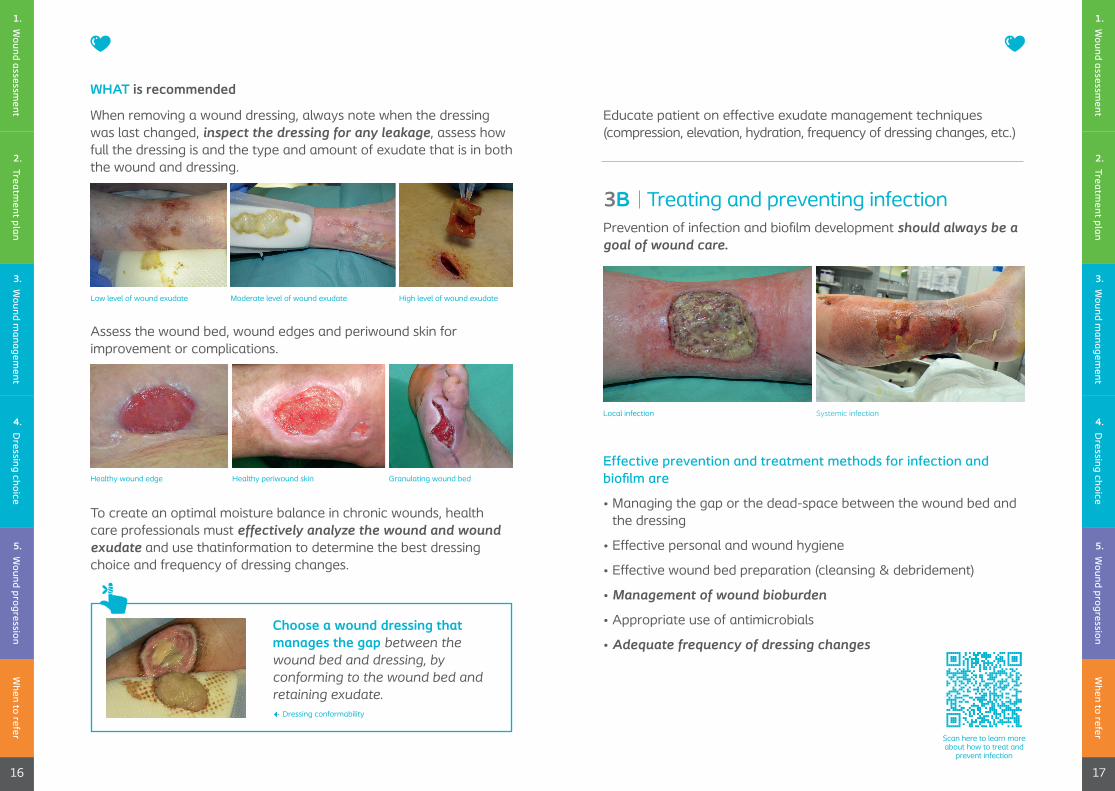
Low level of wound exudate Moderate level of wound exudate
Healthy wound edge Healthy periwound skin
High level of wound exudate
Granulating wound bed
3B
Choose a wound dressing that manages the gap between the wound bed and dressing, by conforming to the wound bed and retaining exudate.
Dressing conformability
Scan here to learn more about how to treat and
prevent infection
When to refer
17
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
When to refer
16
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
Prevention of infection and biofilm development should always be a goal of wound care.
Effective prevention and treatment methods for infection and biofilm are
• Managing the gap or the dead-space between the wound bed and the dressing
• Effective personal and wound hygiene
• Effective wound bed preparation (cleansing & debridement)
• Management of wound bioburden
• Appropriate use of antimicrobials
• Adequate frequency of dressing changes
Local infection Systemic infection
Treating and preventing infection

HOW to prevent and treat wound infection and biofilm development
• Educate and support the patient to ensure the promotion of a consistently clean environment through hand washing, antiseptic use, etc .
• Continuous appropriate use of antimicrobials (avoiding prescribing antibiotics when they are not indicated or when their intent is simply to prevent infection or improve wound healing) is also an important strategy in preventing wound infection and biofilm development
• Biofilm should be suspected if a local infection is non-responsive to topical antimicrobial treatment
WHAT is recommended
• Assessing wound bioburden at every dressing change using the Wound Infection Continuum (IWII, 2016)
• Therapeutic cleansing of the wound and periwound skin, using potable water, saline, surfactant, antiseptic or antimicrobial agent at every dressing change both before and after debridement
• Debridement at every dressing change to remove devitalized or non-viable tissue, bacteria and contaminants
• Managing exudate by managing the gap between the wound bed and the dressing
• Promoting a consistently clean environment through hand washing, antiseptic use, and ongoing patient education
• Use a dressing with antimicrobial properties for local, spreading, or systemic infections
• Use of systemic antibiotics appropriate for the type and level of spreading or systemic infections
Assess the wound for signs of infection and biofilm development at every dressing change . Warning signs include:
• A healable wound is not healing
• Exudate – increased amount, discoloration, odour
• Deterioration of wound edge or periwound skin
• Hyper-granulation – discolouration of the wound bed, granulation tissue, fragile wound bed tissue
• Changes to the patient’s overall health or wellbeing (fever, etc .)
Scan here to learn more about wound infection
When to refer
19
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
When to refer
18
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
Dressing with antimicrobial properties
Suspected biofilm
When to refer
20
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
WHAT is recommended
• Follow locally agreed dressing formularies and local protocols
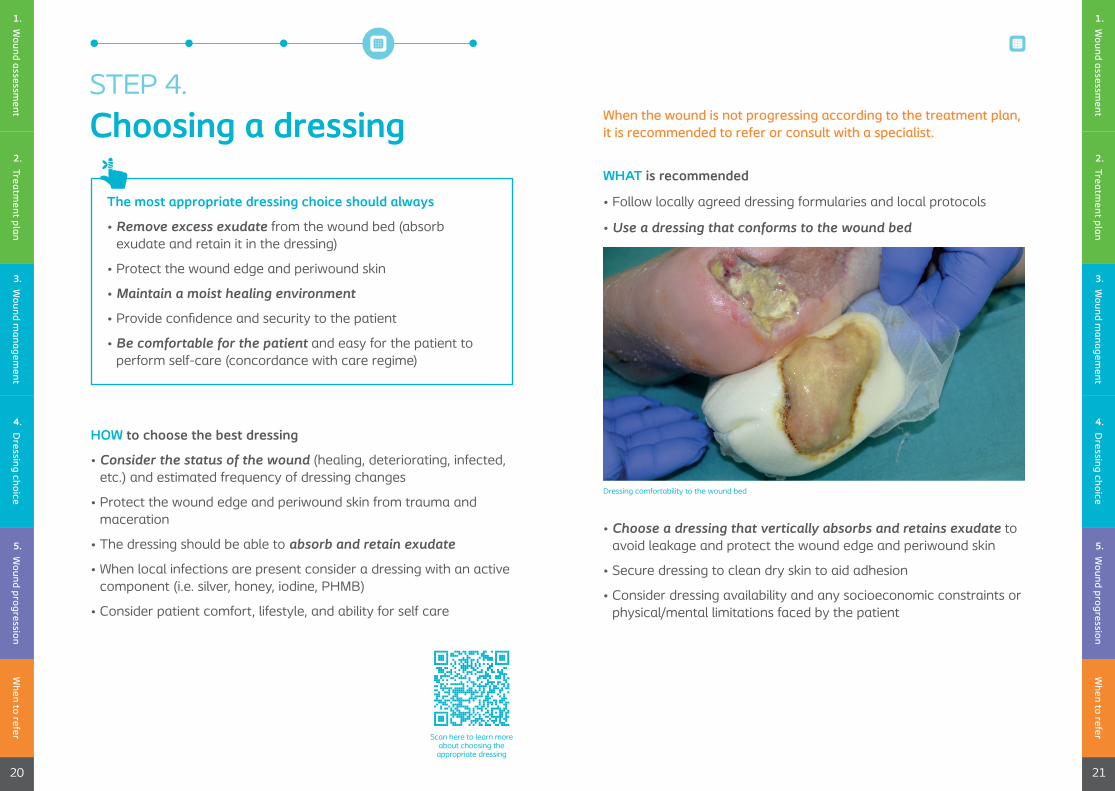
• Use a dressing that conforms to the wound bed
When the wound is not progressing according to the treatment plan, it is recommended to refer or consult with a specialist.
HOW to choose the best dressing
• Consider the status of the wound (healing, deteriorating, infected, etc .) and estimated frequency of dressing changes
• Protect the wound edge and periwound skin from trauma and maceration
• The dressing should be able to absorb and retain exudate
• When local infections are present consider a dressing with an active component (i .e . silver, honey, iodine, PHMB)
• Consider patient comfort, lifestyle, and ability for self care
The most appropriate dressing choice should always
• Remove excess exudate from the wound bed (absorb exudate and retain it in the dressing)
• Protect the wound edge and periwound skin
• Maintain a moist healing environment
• Provide confidence and security to the patient
• Be comfortable for the patient and easy for the patient to perform self-care (concordance with care regime)
Scan here to learn more about choosing the
appropriate dressing
STEP 4 .
Choosing a dressing
Dressing comfortability to the wound bed
• Choose a dressing that vertically absorbs and retains exudate to avoid leakage and protect the wound edge and periwound skin
• Secure dressing to clean dry skin to aid adhesion
• Consider dressing availability and any socioeconomic constraints or physical/mental limitations faced by the patient
When to refer
21
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.
When to refer
22
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
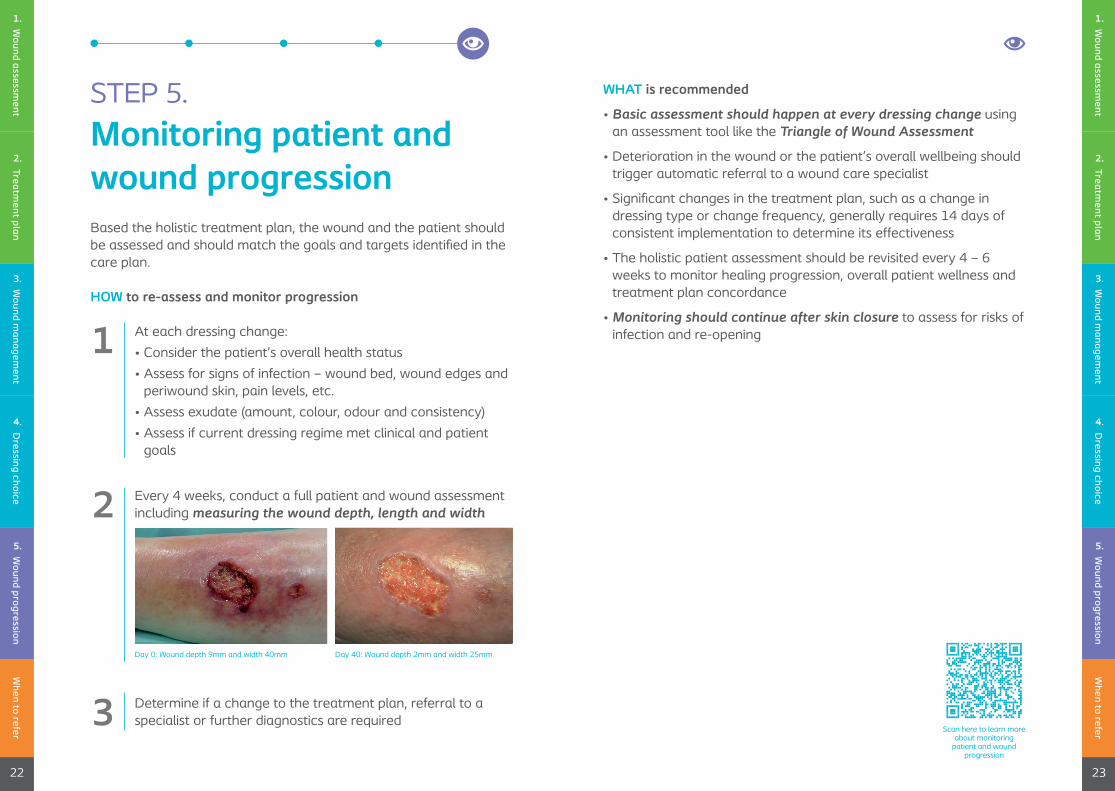
Based the holistic treatment plan, the wound and the patient should be assessed and should match the goals and targets identified in the care plan .
HOW to re-assess and monitor progression
Every 4 weeks, conduct a full patient and wound assessment including measuring the wound depth, length and width
Determine if a change to the treatment plan, referral to a specialist or further diagnostics are required
WHAT is recommended
• Basic assessment should happen at every dressing change using an assessment tool like the Triangle of Wound Assessment
• Deterioration in the wound or the patient’s overall wellbeing should trigger automatic referral to a wound care specialist
• Significant changes in the treatment plan, such as a change in dressing type or change frequency, generally requires 14 days of consistent implementation to determine its effectiveness
• The holistic patient assessment should be revisited every 4 – 6 weeks to monitor healing progression, overall patient wellness and treatment plan concordance
• Monitoring should continue after skin closure to assess for risks of infection and re-openingAt each dressing change:
• Consider the patient’s overall health status
• Assess for signs of infection – wound bed, wound edges and periwound skin, pain levels, etc .
• Assess exudate (amount, colour, odour and consistency)
• Assess if current dressing regime met clinical and patient goals
1
2
3Scan here to learn more
about monitoring patient and wound
progression
STEP 5 .
Monitoring patient and wound progression
Day 0: Wound depth 9mm and width 40mm Day 40: Wound depth 2mm and width 25mm
When to refer
23
Wound assessm
ent1.
Treatment plan
2.
Wound m
anagement
3.
Wound progression
5.
Dressing choice
4.
Wound progression
5.
Dressing choice
4.

WHAT is recommended
Referral or consultation with a wound care specialist is advised if:
• The treatment plan was established and followed but the wound shows no signs of healing progression within 14 days
• The wound area has decreased less than 20% within 4 weeks
• Worsening of wound condition observed by increases in wound size, odour, pain or exudate
• Deterioration of wound edge (e .g . advancing, rolling, undermining, maceration) or periwound skin (advancing maceration, etc .)
• Comorbidity complications (i .e . uncontrolled diabetes, increased BGL, elevated C-Reactive Proteins, vascular status)
• There are underlying structures in the wound like exposed bone or tendons
• The etiology of the wound is unknown
• There is suspicion or signs of systemic infection
• Where detrimental biofilm or local infection is suspected, and aggressive cleansing or debridement are indicated, but are outside of your scope of practice
• There is an overall decline in the patient’s health and wellbeing
When to refer
24
Wound assessm
ent
1.
Treatment plan
2.
Wound m
anagement
3.
Acute woundAn acute wound is a wound that progresses through the phases of normal healing resulting in closure of the wound, without complications .
Antimicrobial dressing propertiesAntimicrobial dressings can be divided into simple and composite dressings . Simple antimicrobial dressings exert only antimicrobial activity, whereas composite dressings exerts, not only the main antimicrobial action also other functions, including exudate normalization, debridement or bioactivity .
BiofilmBiofilms are microorganisms embedded in a thick, slimy barrier of sugars and proteins that acts as a barrier that shields microorganisms from the patient’s natural immune system and from many antimicrobial agents . Biofilms are a structured community of microbes with genetic diversity and variable gene expression (phenotype) that creates behaviours and defences used to produce unique infections (chronic infection) . Biofilms are characterised by significant tolerance to antibiotics and biocides while remaining protected from host immunity . Biofilm can develop within 2–4 days of initial colonisation, and become very tightly attached to extracellular matrix components or the wound bed, making them difficult to remove by surface irrigation or superficial debridement .
Wound infection in clinical practice, IWII 2016
Preventing and treating infection in wounds: translating evidence and recommendations into practice, WINT 2020
25
Wound progression
5.
Dressing choice
4.
Scan here to learn more about when to refer or
consult a specialist
When to refer or consult a specialist
Glossary
Chronic woundWounds with delayed healing of any etiology .Hard to heal wounds that have not healed or progressed, or are not expected to heal, within 4–6 weeks of proper wound care . Chronic wounds do not follow normal healing process, usually remain stuck in inflammatory stage which results in clinical challenges that these recommendation address . Chronic wounds are greater than 30 days despite best practice intervention . Wounds in the course of diabetes mellitus, chronic venous insufficiency, peripheral arterial disease and pressure injuries are regarded as chronic from their very beginning .
Co-morbiditiesPresence of additional diseases in relation to an index disease in one individual . Comorbidity technically indicates a condition or conditions that coexist in the context of an index disease .
ConformabilityIn the context of a wound dressing, conformability means that the dressing should closely follow the contours of the wound bed, to eliminate the gap between the wound bed and the dressing . Close conformability enables effective exudate management, protects the wound edges and periwound skin from maceration and reduces the risk of infection .
DebridementThe European Wound Management Association defines debridement as the “act of removing necrotic material, eschar, devitalized tissue, serocrusts, infected tissue, hyperkeratosis, slough, pus, hematomas, foreign bodies, debris, bone fragments, or
any other type of bioburden from a wound with the objective to promote wound healing .
ExudateExudate is the fluid that leaks from a wound and is the result of the inflammatory process . Exudate is usually clear or amber coloured and contains proteins, enzymes (especially matrix metallopeptidases /metalloproteinases or MMPs), leucocytes (granulocytes, macrophages), sugar, tissue cells, bacteria, and fungi . While exudate production is a normal feature of healing wounds, over or under production of exudate or exudate of the wrong composition can delay healing . In chronic wounds, exudate slows down or even blocks cell proliferation, interferes with growth factor availability and contains elevated levels of inflammatory mediators and activated MMPs8-10 . Effective exudate management allows moist wound healing and prevents maceration of the wound edge and periwound skin .
Exudate poolingThe accumulation of exudate in the gap between the wound bed and the wound dressing . Exudate pooling is likely in wounds with irregular topographies, pockets, or cavities and this can impact negatively on wound healing by causing maceration and potential infection . Exudate pooling can also occur when the exudate is not absorbed by the wound dressing or the volume of fluid exceeds the dressing’s absorptive capacity . Choosing an appropriate dressing can help manage exudate and avoid exudate pooling .
2726
Defining Comorbidity, ANNFAMMED 2009
Debridement, EWMA 2013
An investigation into the conformability of wound dressings, WUK 2011
Dressing conformability and silver-containing wound dressings, WUK 2010
Closing the gap between the evidence and clinical practice – a consensus report on exudate management, WINT 2020
Closing the gap between the evidence and clinical practice – a consensus report on exudate management, WINT 2020
Glossary Glossary
28
Healable woundsWounds that physiologically have the potential to heal in a timely fashion .
Local infectionAn infection that only affects the wound . Local infection is contained in one location, system or structure . Microbes are replicating at a rate that invokes a host response .
MacerationMaceration occurs when skin has been exposed to moisture for too long . A telltale sign of maceration is skin that looks soggy, feels soft, or appears whiter than usual . There may be a white ring around the wound in wounds that are too moist or have exposure to too much drainage .
MMPsMatrix metalloproteinases (MMPs), also known as matrix metallopeptidases or matrixins, are metalloproteinases that are calcium-dependent zinc-containing endopeptidases; other family members are adamalysins, serralysins, and astacins . The MMPs belong to a larger family of proteases known as the metzincin superfamily .
Non-healable woundsDoes not have the potential to heal without surgical intervention, due to factors such as vascular supply or malignancy .
Non-healing woundsNon-healing – has the potential to heal but is not healing due to patient or system factors . For example, a venous leg ulcer is not healing because the patient is unwilling or unable to use compression therapy or compression therapy is not available .
Patient concordanceAlso referred to as patient adherence, or patient acceptance, and means how a patient is following the treatment plan . Patient compliance is a term used in the same context, however there is a move away from the term compliance due to its negative connotations .
Periwound skinTissue surrounding a wound . Periwound area is traditionally limited to 4cm outside the wound’s edge but can extend beyond this limit if outward damage to the skin is present .
PHMBPolyhexamethylene Biguanide / Polyhexanide is an active component used to treat local wound infections .
Patient-Centred Clinical Method, 2013
Preventing and treating infection in wounds: translating evidence and recommendations into practice, WINT 2020
29
Wound infection in clinical practice, IWII 2016
Preventing and treating infection in wounds: translating evidence and recommendations into practice, WINT 2020
Glossary Glossary
30
PSIThe force, or pounds, per square inch that will adequately disengage bacteria detritus from the wound surface . A range of 4-15 psi has been determined to be the safest and most effective range depending on the perceived need to clean . As a general rule, lower pressures are adequate for cleansing clean granulating wounds with higher pressures reserved for those wounds requiring deeper cleansing .
Spreading infectionThe invasion of surrounding tissue by infective organisms that have spread from a wound . Microorganisms proliferate and spread, to a degree that signs and symptoms extend beyond the wound boarder . Spreading infection may involve deep tissue, muscles, fascia, organs or body cavities .
Systemic infectionMicroorganisms spreading throughout the body via the vascular or lymphatic systems invoking responses in the person and/or metabolically .
The gapThe space between the dressing and the wound bed . A gap between the wound bed and the wound dressing, or dead space, should be avoided as it negatively influences would healing . Increased bacterial invasion and impaired healing results from unfilled dead-space between the wound bed and the wound dressing .
UnderminingUndermining is caused by erosion under the wound edges . Wound undermining occurs when the tissue under the wound edges becomes eroded, resulting in a pocket beneath the skin at the wound’s edge . Undermining is measured by inserting a probe under the wound edge directed almost parallel to the wound surface until resistance is felt .
Undermining with depth or tunnelingSerration of tissue at deeper levels in the wound bed or where the edge of the wound is not attached and a probe will extend into the underlying space .
Vertical absorptionWhen referring to dressing properties, vertical absorption means the fluid or exudate is taken upward or wicked from the wound bed into the dressing . The dressing then holds the exudate meaning it doesn’t spread laterally or to the sides to leak onto the wound edges or periwound skin . Vertical wicking decreases the chance of maceration of the wound edges and periwound skin .
Wound etiologyWound etiology refers to the cause of the wound and includes co-morbidities .
Wound progressionProgression, or lack thereof, is improved, unchanged or deteriorated .
Wound infection in clinical practice, IWII 2016
Wound infection in clinical practice, IWII 2016
Managing the gap to promote healing in chronic wounds - an international consensus, WINT 2020
Quality of wound dressings, JOWC 2016
Ten top tips: wound cleansing, WINT 2019
31
Glossary Glossary
Coloplast A/S Holtedam 1
3050 Humlebaek Denmark
Coloplast develops products and services that make life easier for people with very personal and private medical conditions . Working closely with the people who use our products, we create solutions that are sensitive to their special needs . We call this intimate healthcare . Our business includes Ostomy Care, Continence Care, Wound and Skin Care and Interventional Urology . We operate globally and employ about 12,500 employees .
The Coloplast logo is a registered trademark of Coloplast A/S . © 2021-07 .
All rights reserved Coloplast A/S, 3050 Humlebaek, Denmark .