the vitreous and vitreoretinal interface || the vitreous in idiopathic giant retinal breaks
TRANSCRIPT
CHAPTER 15
THE VITREOUS IN IDIOPATHIC GIANT RETINAL BREAKS
H.M. FREEMAN
Outline
Vitreoretinal findings in idiopathic giant retinal breaks Ophthalmoscopic findings Vitreous fmdings
Vitrectomy in idiopathic giant retinal breaks Rationale Technique
Role of the vitreous in the pathogenesis of idiopathic giant retinal breaks Findings in fellow eyes Ophthalmoscopic and biomicroscopic findings in fellow eyes preceding development of a giant retinal break
Prophylactic scleral buckling in the management of fellow eyes Rationale Technique
Recognition and understanding of the vitreous pathology in giant retinal breaks are fundamentally important in their treatment and in the management of fellow eyes of nontraumatic cases.
Giant retinal breaks have been defined as retinal breaks extending 90° or more around the fundus circumference (1). They occur in approximately one in 2 million persons annually and in approximately one in 200 rhegmatogenous retinal detachments (2). Bilateral giant retinal breaks were observed in 13% of patients in a series of2l5 nontraumatic cases with a 19-year follow-up (3). Schepens described three types of giant retinal breaks: approximately 70 % were classified as idiopa-
C. L. Schepens et al. (eds.), The Vitreous and Vitreoretinal Interface© Springer Science+Business Media New York 1987

- 230 -
thic, 20% were traumatic, and 10% occurred either along the posterior edge of chorioretinal degeneration, or along the edge of excessive treatment(4).
This chapter deals with idiopathic giant retinal breaks: their ophthalmoscopic and biomicroscopic findings, and the technique of vitrectomy used in their management. In addition, vitreoretinal findings in fellow eyes that developed a giant retinal break during the follow-up are described. The pathogenesis and prevention of idiopathic giant retinal breaks are discussed.
Vitreoretinal findings in idiopathic giant retinal breaks
Ophthalmoscopic findings
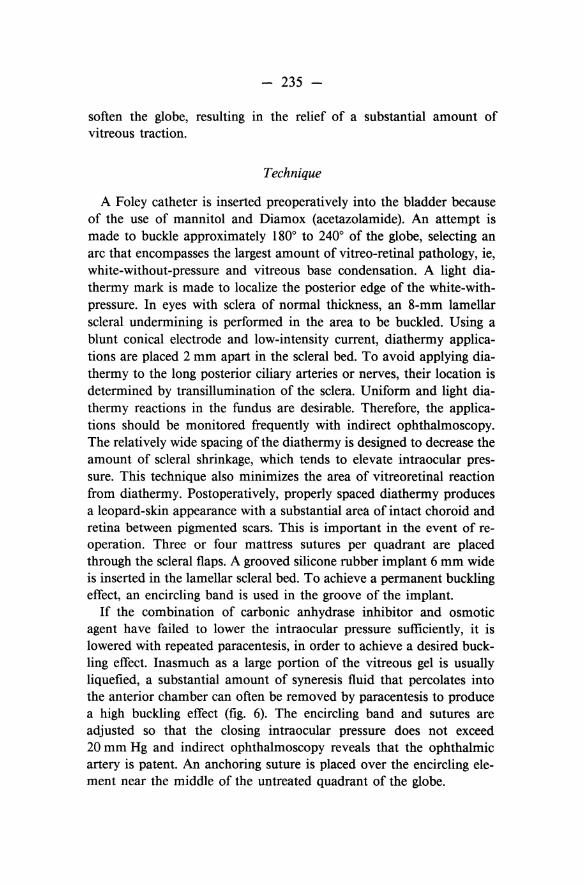
Idiopathic giant retinal breaks are usually located slightly posterior to the ora serrata or, less commonly, at the ora itself. The anterior flap of the retinal break includes the pars plana ciliaris, which is detached in 96 % of cases as a result of shrinkage and traction of the vitreous base (5) (fig. 1). The posterior flap of the giant retinal break often becomes partially or completely inverted over the optic disc. Untreated, the giant retinal break may extend posteriorly or 3600 around the fundus. Proliferative vitreoretinopathy in varying degrees of severity is very common.
Vitreous findings
Biomicroscopy of the vitreous cavity reveals extensive liquefaction of the vitreous gel. Liquefied vitreous offers no support to the posterior retinal flap of a superior giant break, and the flap tends to become inverted toward the optic disc. Extensive vitreous detachment is uncommon, so that a thin layer of vitreous cortex remains attached to the retina including the posterior retinal flap. This layer is not always visible because it is thin, transparent, and usually covered by an inverted retinal flap.
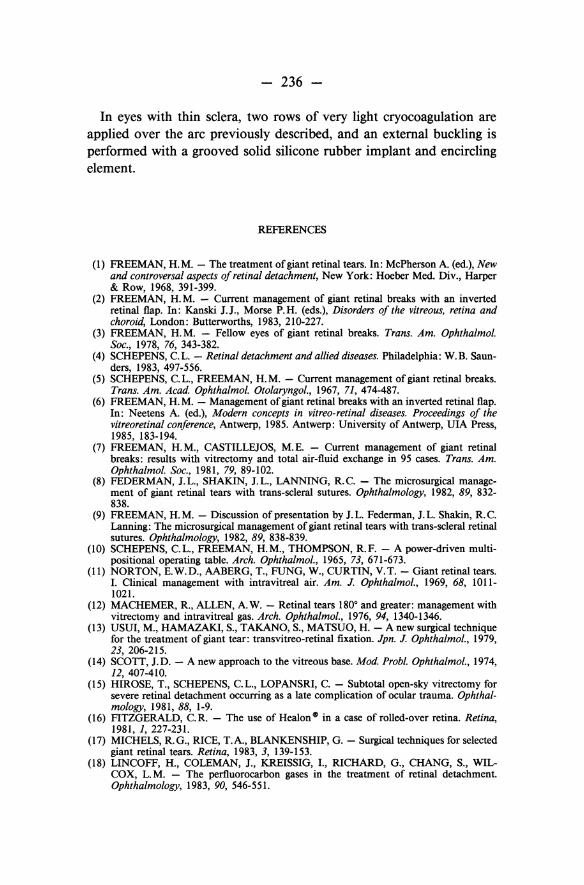
The vitreous base along the anterior margin of the giant retinal break is condensed and contracted, pulling the anterior flap toward the lens and resulting in detachment of the ora serrata and pars plana ciliaris (fig. 2). In many cases, detachment of the ora serrata and pars plana ciliaris extends beyond the ends of the giant break. In some instances,

- 231 -
condensation in the anterior portion of the vitreous gel produces a membrane extending like a trampoline parallel and anterior to the equator. This intravitreous membrane is inserted in the region of the posterior vitreous base and seems to coincide with the posterior surface of the condensed anterior vitreous gel.
A less common fmding is an extensive detachment of the cortical vitreous (fig. 3). Vitreous membranes that develop in planes parallel to the equator are separated by an optically empty space that may contain particles of blood. The anterior membrane is located in the equatorial region, whereas the posterior membrane is the detached posterior cortical vitreous that is adherent to the posterior edge of the giant retinal break.
Vitrectomy in idiopathic giant retinal breaks
Rationale
I perform a pars plana vitrectomy in all idiopathic giant retinal breaks with a partial or completely inverted posterior retinal flap (6). The rationale for vitrectomy is twofold. (1) Prone positioning of the patient and air injection into the vitreous cavity unfold and tamponade the posterior retinal flap. The larger the bubble of air that can be injected, the greater is the unfolding of the flap. Therefore, the aim is to inject as large a bubble of air as possible. Removal of the vitreous gel and the lens allows injection of a very large air bubble. (2) Removal of the vitreous gel and vitreous membranes interrupts vitreous traction that can result in the postoperative formation of additional retinal breaks or the extension of the existing giant break (7).
After the flap of the giant break is unfolded, transcleral sutures are used to anchor the posterior retinal flap in its anatomic position. The suture prevents unfolding or posterior slippage of the flap caused by globe manipulation during surgery. In addition, the retinal suture anchors the flap postoperatively during the formation of a chorioretinal adhesion (8, 9).
Technique
In order that the vitreous gel will not interfere with the unfolding of the retinal flap, an attempt is made to remove as much gel as possible overlying the bare pigment epithelium. The vitrectomy is made to
- 232 -
extend into the vitreous base along the anterior edge of the giant break in order to lessen the incidence of peripheral proliferative vitreoretinopathy in the region of the vitreous base (anterior loop traction). The vitreous is very firmly attached to the peripheral retina. Postoperative shrinkage of the vitreous base often results in an elevation of the ends of the giant retinal break, producing an anterior retinal detachment. For that reason, as much vitreous is removed in the region of the vitreous base as can be done without causing an extension of the giant retinal break. To avoid iatrogenic retinal breaks or extension ofthe giant break during vitrectomy, one must proceed very cautiously when extending the vitrectomy into the vitreous base overlying attached retina. The vitrectomy instrument is set at a low section pressure and a slow cutting speed. Scleral depression is used to enhance visualization of the peripheral retina during vitrectomy. It is important to examine the entire fundus periphery with indirect ophthalmoscopy and scleral depression after vitrectomy in order to determine whether the giant retinal break has extended circumferentially or radially and to detect retinal tears that may have been produced during surgery.
I recommend a 3600 scleral buckling in all giant breaks with an inverted retinal flap because postoperative shrinkage of the remaining vitreous overlying the vitreous base can cause an anterior retinal detachment. This detachment can extend posteriorly around the end of a scleral buckle that does not encompass the entire circumference of the fundus periphery.
Role of the vitreous in the pathogenesis of idiopathic giant retinal breaks
Findings in fellow eyes
In spite of advances in surgical techniques (10-21), a considerable number of eyes with giant retinal breaks continue to be lost. In addition, there is a high incidence of retinal breaks and retinal detachment in fellow eyes of nontraumatic cases. For these reasons the management offellow eyes of giant retinal breaks is important. We therefore studied fellow eyes of a series of nontraumatic giant retinal breaks in the hope of obtaining information concerning their pathogenesis and possibly their prevention. Follow-up included indirect ophthalmoscopy with scleral depression and biomicroscopy of the vitreous using the Gold-
- 233 -
mann three-mirror lens at least every six months for five years, and then at yearly intervals.
Retinal breaks with or without retinal detachment developed in 51 % of fellow eyes of nontraumatic giant breaks that were followed during a 19-year observation period. Retinal detachment caused by either retinal tears, holes, or dialyses occurred in 16 % of the fellow eyes. Retinal breaks without detachment consisted of giant breaks in 13 % of the fellow eyes, retinal tears in 12 %, retinal holes in 10%, and retinal dialyses in 0.4 %. The average latent period from the diagnosis of a nontraumatic giant retinal break to the development of a giant break in the fellow eye was 3! years.
Ophthalmoscopic and biomicroscopic findings in fellow eyes preceding development of a giant retinal break
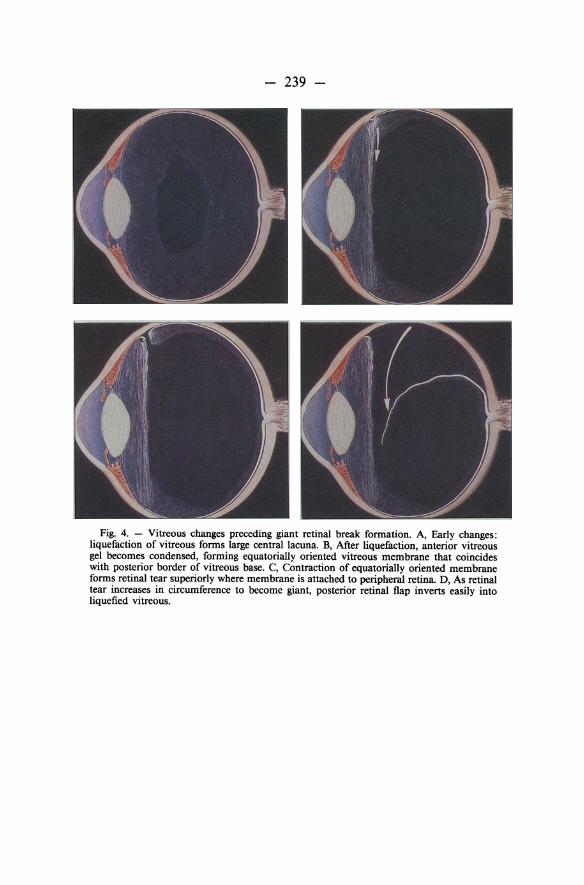
The majority of fellow eyes that developed a giant retinal break during the follow-up period were highly myopic, ie, over 10 diopters, and they developed increasing vitreous base condensation and increasing areas of white-with-pressure. The earliest biomicroscopic changes were syneresis and liquefaction of the vitreous gel, converting the posterior and central portions of the vitreous body into a large lacuna (fig. 4A). Later the anterior gel became condensed and its posterior border formed a membrane extending across the equatorial region and separating the anterior gel from liquefied vitreous (fig. 4B). This membrane seemed rigid and did not oscillate with ocular movements, suggesting it was under tension. Marked contraction of this membrane seems responsible for tearing the retina along the posterior border of the vitreous base (fig. 4C). This tense membrane attached to the anterior edge of the giant break is not infrequently encountered during vitrectomy. After the retinal break develops, the posterior retinal flap inverts easily into the liquefied vitreous (fig. 4D).
Ophthalmoscopy revealed increasing white-with-pressure in 90 % of fellow eyes that developed a giant retinal break. These eyes had marked white-with-pressure occurring in elongated patches anterior to the equator. In 60% of these eyes, adjacent areas of white-with-pressure increased in size circumferentially to become confluent. As the whitewith-pressure spread, it became more dense and developed a sharp posterior edge in contrast to the hazy, ill-defined posterior margin seen earlier. In some cases a sharp ridge developed in the retina at this
- 234 -
posterior edge. This was the location of the giant retinal break that subsequently developed (fig. SA, B).
On the basis of this study we concluded that fellow eyes at high risk for developing a giant retinal break are eyes that are highly myopic and that show increasing white-with-pressure and increasing condensation of the vitreous base. During the follow-up of nine such high-risk eyes, giant retinal breaks developed in six eyes and multiple retinal tears in three.
Prophylactic scleral buckling in the management of fellow eyes
Rationale
Eyes with myopia in excess of - 10.00 diopters, increasing whitewithout-pressure, and increasing condensation of the vitreous base show a high incidence of giant retinal breaks with unfavorable anatomic and visual results. This has prompted me to treat such eyes with a prophylactic slceral buckle. Results thus far have been encouraging in that no giant retinal breaks have developed in 24 eyes treated with a prophylactic scleral buckle and followed for a period of 3 to 19 years.
The study of fellow eyes indicates that vitreous traction plays a central role in the pathogenesis of giant retinal breaks. Therefore, the rationale for preventing giant retinal breaks should involve measures that relieve vitreous traction. I do not use prophylactic cryocoagulation or photocoagulation without scleral buckling because these modalities do not reduce vitreous traction. Quite the contrary, I have seen a significant number of cases where very difficult-to-treat, posteriorly located giant retinal breaks have developed along the posterior edge of photocoagulations or cryoapplications. In addition, these iatrogenic giant breaks were associated with a very high incidence of proliferative vitreoretinopathy.
I feel that the risks involved in prophylactic vitrectomy do not justify its use in the management of high-risk eyes, whereas the release of vitreous traction through scleral buckling is justified in high-risk eyes selected on the basis of detailed and repeated studies of the vitreous and retina. Although scleral buckling does not eliminate vitreous traction completely, a high buckling effect can be obtained with the help of carbonic anhydrase inhibitors, mannitol, and multiple paracenteses to
- 235 -
soften the globe, resulting in the relief of a substantial amount of vitreous traction.
Technique
A Foley catheter is inserted preoperatively into the bladder because of the use of mannitol and Diamox (acetazolamide). An attempt is made to buckle approximately 1800 to 2400 of the globe, selecting an arc that encompasses the largest amount of vitreo-retinal pathology, ie, white-without-pressure and vitreous base condensation. A light diathermy mark is made to localize the posterior edge of the white-withpressure. In eyes with sclera of normal thickness, an 8-mm lamellar scleral undermining is performed in the area to be buckled. Using a blunt conical electrode and low-intensity current, diathermy applications are placed 2 mm apart in the scleral bed. To avoid applying diathermy to the long posterior ciliary arteries or nerves, their location is determined by transillumination of the sclera. Uniform and light diathermy reactions in the fundus are desirable. Therefore, the applications should be monitored frequently with indirect ophthalmoscopy. The relatively wide spacing of the diathermy is designed to decrease the amount of scleral shrinkage, which tends to elevate intraocular pressure. This technique also minimizes the area of vitreoretinal reaction from diathermy. Postoperatively, properly spaced diathermy produces a leopard-skin appearance with a substantial area of intact choroid and retina between pigmented scars. This is important in the event of reoperation. Three or four mattress sutures per quadrant are placed through the scleral flaps. A grooved silicone rubber implant 6 mm wide is inserted in the lamellar scleral bed. To achieve a permanent buckling effect, an encircling band is used in the groove of the implant.
If the combination of carbonic anhydrase inhibitor and osmotic agent have failed to lower the intraocular pressure sufficiently, it is lowered with repeated paracentesis, in order to achieve a desired buckling effect. Inasmuch as a large portion of the vitreous gel is usually liquefied, a substantial amount of syneresis fluid that percolates into the anterior chamber can often be removed by paracentesis to produce a high buckling effect (fig. 6). The encircling band and sutures are adjusted so that the closing intraocular pressure does not exceed 20 mm Hg and indirect ophthalmoscopy reveals that the ophthalmic artery is patent. An anchoring suture is placed over the encircling element near the middle of the untreated quadrant of the globe.
- 236 -
In eyes with thin sclera, two rows of very light cryocoagulation are applied over the arc previously described, and an external buckling is performed with a grooved solid silicone rubber implant and encircling element.
REFERENCES
(1) FREEMAN, H.M. - The treatment of giant retinal tears. In: McPherson A. (ed.), New and controversal aspects of retinal detachment, New York: Hoeber Med. Div., Harper & Row, 1968, 391-399.
(2) FREEMAN, H.M. - Current management of giant retinal breaks with an inverted retinal flap. In: Kanski J.J., Morse P.H. (eds.), Disorders of the vitreous, retina and choroid, London: Butterworths, 1983, 210-227.
(3) FREEMAN, H.M. - Fellow eyes of giant retinal breaks. Trans. Am. Ophthalmol. Soc., 1978, 76, 343-382.
(4) SCHEPENS, C.L. - Retinal detachment and allied diseases. Philadelphia: W.B. Saunders, 1983, 497-556.
(5) SCHEPENS, C.L., FREEMAN, H.M. - Current management of giant retinal breaks. Trans. Am. Acad. Ophthalmol. Otolaryngol., 1967, 71, 474-487.
(6) FREEMAN, H.M. - Management of giant retinal breaks with an inverted retinal flap. In: Neetens A. (ed.), Modern concepts in vitreo-retinal diseases. Proceedings of the vitreoretinal conference, Antwerp, 1985. Antwerp: University of Antwerp, UIA Press, 1985, 183-194.
(7) FREEMAN, H. M., CASTILLEJOS, M. E. - Current management of giant retinal breaks: results with vitrectomy and total air-fluid exchange in 95 cases. Trans. Am. Ophthalmol. Soc., 1981, 79, 89-102.
(8) FEDERMAN, J.L., SHAKIN, J.L., LANNING, R.C. - The microsurgical management of giant retinal tears with trans-scleral sutures. Ophthalmology, 1982, 89, 832-838.
(9) FREEMAN, H.M. - Discussion of presentation by J.L. Federman, J.L. Shakin, RC. Lanning: The microsurgical management of giant retinal tears with trans-scleral retinal sutures. Ophthalmology, 1982, 89, 838-839.
(10) SCHEPENS, C.L., FREEMAN, H.M., THOMPSON, RF. - A power-driven multipositional operating table. Arch. Ophthalmol., 1965, 73, 671-673.
(11) NORTON, E. W.O., AABERG, T., FUNG, W., CURTIN, V. T. - Giant retinal tears. I. Clinical management with intravitreal air. Am. J. Ophtha/mol., 1969, 68, 1011-1021.
(12) MACHEMER, R, ALLEN, A. W. - Retinal tears 1800 and greater: management with vitrectomy and intravitreal gas. Arch. Ophthalmol., 1976, 94, 1340-1346.
(13) USUI, M., HAMAZAKI, S., TAKANO, S., MATSUO, H. - A new surgical technique for the treatment of giant tear: transvitreo-retinal fixation. Jpn. J. Ophthalmol., 1979, 23, 206-215.
(14) SCOTT, J.D. - A new approach to the vitreous base. Mod. Probl. Ophthalmol., 1974, 12, 407-410.
(15) HIROSE, T., SCHEPENS, C.L., LOPANSRI, C. - Subtotal open-sky vitrectomy for severe retinal detachment occurring as a late complication of ocular trauma. Ophthalmology, 1981, 88, 1-9.
(16) FITZGERALD, C. R. - The use of Healon GIl in a case of rolled-over retina. Retina, 1981, 1, 227-231.
(17) MICHELS, R.G., RICE, T.A., BLANKENSHIP, G. - Surgical techniques for selected giant retinal tears. Retina, 1983, 3, 139-153.
(18) LINCOFF, H., COLEMAN, J., KREISSIG, I., RICHARD, G., CHANG, S., WILCOX, L. M. - The perfluorocarbon gases in the treatment of retinal detachment. Ophthalmology, 1983, 90, 546-551.

- 237 -
(19) PEYMAN, G.A., REDMAN, K.R. V., SEETNER, A. A. - Retinal microincarceration with penetrating diathermy in the management of giant retinal tears. Arch. Ophthalmol., 1984, 102, 562-565.
(20) LEAVER, P.K., COOLING, R.J., FERETIS, E.B., LEAN, J.S., McLEOD, D. -Vitrectomy and fluid/silicone-oil exchange for giant retinal tears: results at six months. Br. J. Ophthalmol, 1984, 68, 432-438.
(21) GLASER, B.M. - Treatment of giant retinal tears combined with proliferative vitreoretinopathy. Ophthalmology, 1986, 93, 1193-1197.
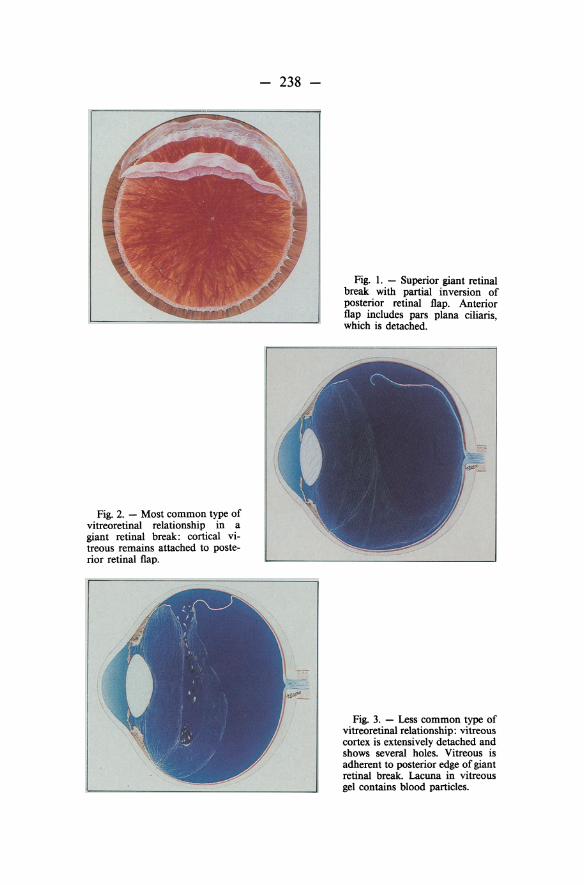
Fig. 2. - Most common type of vitreoretinal relationship in a giant retinal break: cortical vitreous remains attached to posterior retinal flap.
- 238 -
Fig. I. - Superior giant retinal break with partial inversion of posterior retinal flap. Anterior flap includes pars plana ciliaris, which is detached.
Fig. 3. - Less common type of vitreoretinal relationship: vitreous cortex is extensively detached and shows several holes. Vitreous is adherent to posterior edge of giant retinal break. Lacuna in vitreous gel contains blood particles.
- 239 -
Fig. 4. - Vitreous changes preceding giant retinal break formation. A, Early changes: liquefaction of vitreous forms large central lacuna. B, After liquefaction, anterior vitreous gel becomes condensed, forming equatorially oriented vitreous membrane that coincides with posterior border of vitreous base. C, Contraction of equatorially oriented membrane forms retinal tear superiorly where membrane is attached to peripheral retina. D, As retinal tear increases in circumference to become giant, posterior retinal flap inverts easily into liquefied vitreous.

- 240 -
Fig. 5. - Retinal changes before development of giant retinal break. A, Shrinkage of membrane on posterior face of shrunken vitreous gel (arrows) produces retinal ridge at posterior border of vitreous base. B, Continuing shrinkage of vitreous base and membrane has produced a superior giant retinal break with detachment of ora serrata and pars plana.
Fig. 6. - Drainage of aqueous and liquefied vitreous that percolates into anterior chamber helps to lower intraocular pressure so that desired buckling effect can be obtained.