the role of aromatase inhibitors in assisted reproductive technologies
TRANSCRIPT

The Role of Aromatase Inhibitors in Assisted
Reproductive Technologies
Ulun ULUG, M.D.
Bahceci IVF Centers, Istanbul

1. Does addition of AI increase pregnancy rates ?
2. Does addition of AI reduce cost ?
3. Does addition of AI augment ovarian response ?
4. Does addition of AI during luteal phase decrease OHSS risk
5. ART in breast ca survivors

Pharmacology
Inhibit or inactivate AROMATASEAromatase is the rate limiting step in the
conversion of androstenedione and testosterone to estrone and estradiol
Suppression of plasma estrogen levelsAromatase
– Cytochrome P-450 superfamily

Aromatase Enzyme
Sources:– Granulosa cells of Ovary– Endometrial cells– Placenta– Subcutaneous fat– Liver– Muscle– Brain– Normal breast – Breast cancer

Aromatase Enzyme
Premenopausal women– Ovarian source
Postmenopausal women– Adipose tissue
• Aromatase transcription regulated by:– Cytokines– Cyclic nucleotides– Gonadotropins– Glucocorticoids– Growth factors

Aromatase Inhibitors

3rd Generation Aromatase Inhibitors
Type 1: Exemestane– t½= 27h
Type 2: Anastrozole and Letrozole– t½= 48h, once daily dosing
99% inhibition of aromatase enzyme1000-10,000 fold more effectiveOral administrationMore selective for aromatase

Dosage
1. Letrozole 2.5mg/5mg daily from day 3 to day 7 of menses
2. Letrozole 20mg single dose on day 3

A Randomized Trial of Superovulation with Two Different Doses of Letrozole
Al-Fadhli et al 2006
Unexplained Infertility
Side effects of Letrozole usage:
Headache (6.9%)Nausea (6.3%)Peripheral eodema (6.2%)Fatigue (5.2%)Hot flushes (5.2%)Skin reactions (3.4%)

11
Hypothesis• Aromatase inhibition decreases estrogenic negative
feedback centrally• Increased FSH • Short half-life and no ER effects (no depletion)• Intact central feedback loop for estrogen & FSH (Normal
feedback mechanisms centrally)• Avoids the undesirable peripheral anti-estrogen effects of
CC = ( no –ve effect on endometrium)• Result in predominantly mono-ovulation when used alone• Ovarian intrinsic accumulation of A, increases GC-FSH
sensitivity

Androgens increase FSH receptor expression on granulosa cells (Weil et al. 1998)
Androgens increases ovarian paracrin factors such as IGF-1 and augments FSH activity (Vendola et al. 1999)

14
Clomiphene Citrate - ProblemsLong tissue half-life (2 weeks)
prolonged central ER depletionHigh multiple pregnancy rate Peripheral anti-estrogenic effects Thin endometrium (Gonen et al, 1990)Unfavorable cervical mucusReduced uterine blood flow Lower pregnancy rate than expected from
the high ovulatory rate

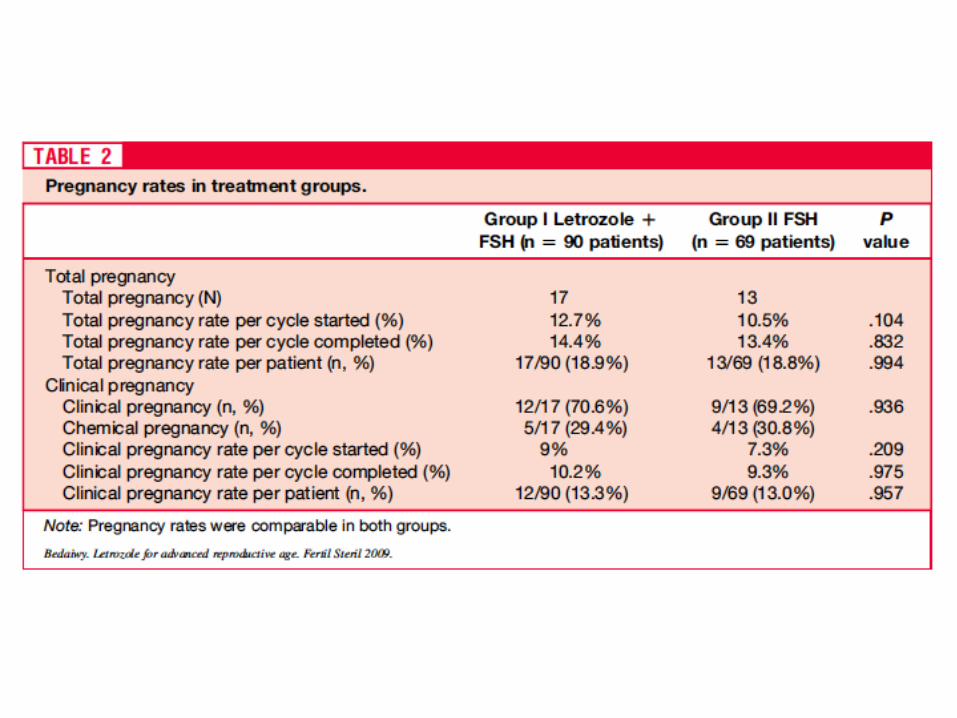
Letrozole co-treatment in infertile women 40 years oldand older receiving controlled ovarian stimulation and
intrauterine inseminationMohamed A. Bedaiwy, et al 2009


Management of Poor Responders: Can Outcomes Be Improved with a Novel Gonadotropin-Releasing Hormone Antagonist/Letrozole Protocol?
Schoolcraft et al. 2008


IVF/ICSI planlanan hastalarda 2. günden itibaren rFSH (150 IU/gün)rFSH (150 IU/gün) + ilk 5 günde letrozol (2.5 mg/gün) 6. günden itibaren ganireliks (0.25 mg/gün)
Aromatase Inhibitors in Ovarian Stimulation for IVF/ICSI: A Pilot Study
Verpoest et al. RBM Online 2006; 13: 16620 hasta


Daha önceden GnRH agonisti (uzun protokol) + 375 IU/gün gonadotropin tedavisi ile 4 folikül geliştirdikleri için siklusları iptal edilen IVF hastaları
¨ OK sonrası, 3. günden itibaren;¨ 375 IU/gün gonadotropin (n=76)¨ 375 IU/gün gonadotropin (n=76) + ilk 5 günde letrozol 2.5 mg/gün
(n=71)
¨ 14 mm’den itibaren GnRH antagonisti (ganireliks 0.25 mg/gün)
The Aromatase Inhibitor Letrozole Increases the Concentration of Intraovarian Androgens and Improves in Vitro Fertilization Outcome in Low Responders: A Pilot Study
Garcia-Velasco et al. Fertil Steril 2005; 84: 82



Use of aromatase inhibitors in poor-responder patients receiving GnRH antagonist protocolsOzmen et al, 2009RCT of 70 poor responder patients
FSH (450 IU) FSH (450IU)+ AI
Gonadotropin consumption (IU) 3850 2980 <0.05
Cancellation (%) 28.6 8.6 <0.05
Pregnancy rates (%) 20 25.8 NS
Cost (USD) 17584 11560 <0.05



Bahçeci Kliniği Letrozol Deneyimi
2009 yılıGnRH antagonist siklusları1328 siklusSeçilmemiş hasta grubu (infertilite
faktörü, yaş, ovaryen rezerv, sperm orijini-(TESE, MESA, Ejakülat))

Protokoller
Antagonist1. Siklusun 2. günü
2. Serbest başlangıç dozu (150 IU 450 IU)
3. Önde giden follikül >13mm veya 6.gün
4. Önde giden en az 2 adet >19mm: hCG enjeksiyonu
Letrozol1. Siklusun 2. günü
2. Letrozole 5 mg + 150 IU (5 gün)
3. Önde giden follikül >13mm veya 6.gün
4. Önde giden en az 2 adet >19mm: hCG enjeksiyonu

Antagonist Letrozole
OPU Siklus (n) 727 601
Embiryo Transfer (n) 526 465
Yaş 32.7 33.8 0.002
İptal Oranı (%) 27.6 22.6 0.03

ET İptal Nedenleri:
1. Başarısız OPU
2. Total fertilizasyon
3. Bölünmeme
4. Kötü embiryo kalitesi
5. OHSS önlemi için total freezing
6. TESE’de sperm bulunmaması
7. Endometrial faktörler (polip, septum)

Antagonist Letrozole
Gonadotropin (IU) 2618.4 1639.3 0.0001
Peak Estradiol (pg/ml) 2081.9 1298.5 0.0001
Endometrium kalınlık (mm)
9.8 8.6 0.001
Total Oosit 15.4 9.7 0.0001
ET 2.7 2.4 0.0001

P:0.09 P: 0.0002

P: 0.05 P:0.1

Biyokimyasal Gebelik
P:0,1

Pregnancy Outcome After the Use of an Aromatase Inhibitor for Ovarian Stimulation Mitwally et al.2005

Congenital Malformations Among 911 Newborns Conceived After Infertility Treatment with Letrozole or Clomiphene Citrate
Tulandi et al. 2006

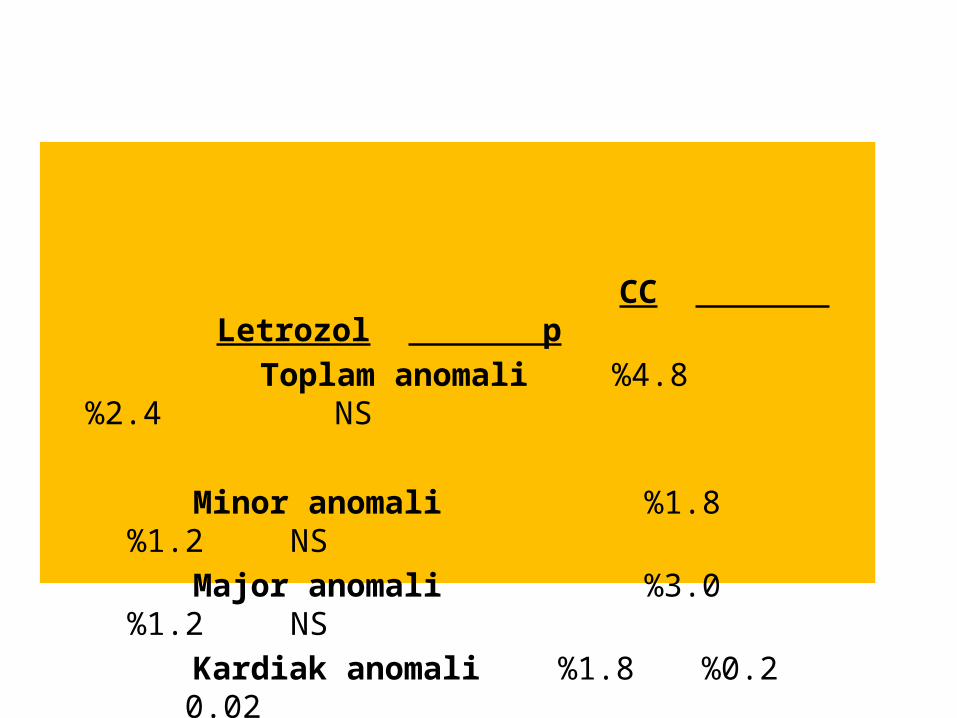
CC Letrozol p
Toplam anomali %4.8 %2.4 NS
Minor anomali %1.8 %1.2 NS
Major anomali %3.0 %1.2 NS
Kardiak anomali %1.8 %0.2 0.02
Does addition of AI increase pregnancy rates ?
Needs further evidence

Does addition of AI reduce cost ?
yes

Does addition of AI augment ovarian response ?
Needs further evidence