the rights of psychiatric patients in china: a survey of medical staff and consumers' attitudes...
TRANSCRIPT

at SciVerse ScienceDirect
Social Science & Medicine 75 (2012) 823e827
Contents lists available
Social Science & Medicine
journal homepage: www.elsevier .com/locate/socscimed
The rights of psychiatric patients in China: A survey of medical staffand consumers’ attitudes toward patient participation in clinical trials
Liang Su a,b, Jingjing Huang a, David Mellor c, Weimin Yang a, Marita McCabe c, Yifeng Shen a,b,Huafang Li a, Weichun Wang d, Yifeng Xu a,*
a Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, No. 600 Wan Ping Nan Road, Shanghai 200030, People’s Republic of ChinabDepartment of Psychiatry, Huashan Hospital, Fudan University, School of Medicine, No. 12 Wulumuqi Road (middle), Shanghai 200040, People’s Republic of Chinac School of Psychology, Deakin University, 221 Burwood Highway, Burwood, Victoria 3125, Australiad School of Exercise and Nutrition Sciences, Deakin University, 221 Burwood Highway, Burwood, Victoria 3125, Australia
a r t i c l e i n f o
Article history:Available online 17 May 2012
Keywords:AttitudesPsychiatric hospitalsClinical trialGenderChinaPatient rights
* Corresponding author. Tel.: þ86 21 64387250; faxE-mail addresses: [email protected] (L. Su), jjhua
[email protected] (D. Mellor), [email protected] (M. McCabe), [email protected] (H. Li), [email protected] (Y. Xu).
0277-9536/$ e see front matter � 2012 Elsevier Ltd.doi:10.1016/j.socscimed.2012.03.056
a b s t r a c t
To explore and compare attitudes of consumers (patients and their family members) and medical stafftoward clinical trials related to mental health in China, we developed two questionnaires for medicalstaff and patients and their family members. Approximately 66.2% of medical staff who had no researchexperience believed that patients could be persuaded to participate in clinical trials, but the percentageof consumers who believed so was just 12.5%. Both groups agreed that written informed consent wasrequired; however, more medical staff than patients agreed that such consent could be provided bypatients or their guardian (88.4% vs. 71.4%). Only 9.5% of medical staff thought that patient treatmentwould be compromised by refusal to participate; the proportion of consumers who thought the samewas 29.4%. Great differences exist between medical staff and consumers’ attitudes and beliefs regardingclinical trials. Medical staff were more likely to have a favorable attitude toward their patients partici-pating in clinical trials and considered that informed consent could be provided by guardians rather thanthe patient.
� 2012 Elsevier Ltd. All rights reserved.
Introduction
Ongoing social changes in China have contributed to a highprevalence of mental illness (Demyttenaere et al., 2004), withestimates suggesting that more than 100 million people haveamental disorder and that 16million of these people have a seriousmental illness such as schizophrenia (Psychiatric institutions inChina, 2010). Despite the rapid and strong economic growth overthe past 25 years, China’s health care system is still underdeveloped(Blumenthal & Hsiao, 2005), and most psychiatric patients do notreceive adequate treatment and suffer continued stigmatization(Phillips et al., 2009).
High quality clinical trials often lead to improved treatmentregimes for mental illness. However, despite having 1/4 of theworld’s population, China has conducted only 3% of the world’s
: þ86 21 [email protected] (J. Huang),[email protected] (W. Yang),[email protected] (Y. Shen),au (W. Wang), hyyyyb@
All rights reserved.
pharmaceutical company-sponsored clinical trials (Research andethics in China, 2009), and few results from China can be foundin clinical practice guidelines and systematic reviews (Wang, 2010).However, as clinical trials are increasingly being conducted indeveloping countries, the proportion of clinical trials conducted inChina is growing steadily (Glickman et al., 2009). As more clinicaltrials are conducted in China, many observers are raising concernsabout the ethical issues that might complicate the findings ofresearch conducted in developing countries like China (Borry,Schotsmans, & Dierickx, 2005; Glickman et al., 2009). Of partic-ular concern is the lack of appropriate information related to ethicalaspects of clinical trials for both medical staff conducting researchand psychiatric patients who are particularly vulnerable potentialparticipants. In contrast to the United Kingdom, where the SpecialCommittee on Unethical Psychiatric Practices (SCOUPP) supportsthe rights of patients (Deahl, 2002), there is no such organization inChina. Parry and Cui (2010) even report the case of a dissidentwithout mental illness being sent to a psychiatric hospital.
Few studies have focused on the ethical attitudes towardpsychiatric clinical trials in China. To take the first steps to gain anunderstanding of the views about ethics in clinical trials in China,the current study was designed to explore and compare the

Agree Disagree Consideration
0
20
40
60
80 Medical staff Patients and family members
Pe
rc
en
ta
ge
(%
)
Fig. 1. Level of willingness between medical staff and consumers who had no expe-rience in clinical trials concerning patient participation in clinical trials.
L. Su et al. / Social Science & Medicine 75 (2012) 823e827824
attitudes of medical staff and patients and their family memberswho are consumers of mental health services in China. Wehypothesize that due to their different positions within thepsychiatric system, there will be some differences in the attitudestoward clinical trials between doctors and patients with mentalillness.
Methods
We developed and administered two self-report questionnaires,one for medical staff and one for consumers in 24 primary carepsychiatric hospitals. The data were collected from October toDecember 2010. This study was conducted with the approval of theMedical Ethics Committee of Shanghai Mental Health Center(No. 2010-29, IORG Number: IORG0002202; FWA Number:FWA00003065).
Questionnaire
The questionnaire for medical staff consisted of 80 questions,and that for patients consisted of 88 questions. The questionscovered general demographic information, such as age and gender,and attitudes relating to ethics in clinical trials. Respondents wereasked to indicate their level of agreement or disagreement withstatements such as “Do you agree that patients must give writteninformed consent before they participate in clinical trials?” A five-point response format was used, ranging from completely disagreeto completely agree, with a central neutral point.
Setting
We carried out the study in 24 primary care psychiatric hospi-tals in Beijing (one site), Shanghai (22 sites) and Guangzhou (onesite) as shown in Appendix A. These three cities are located innorthern, central and southern China and have higher than averagelevels of socioeconomic status and lower than average non-treatment rates than other parts of China. The ethnic mix issimilar to the China average.
Sampling and recruitment
Simple random selection methods were used to identify targetindividuals from the computerized registry of medical staff in thehospitals at each site. However, as China has no systematizedrecord of psychiatric patients, a convenience sample of individualpatients and family members was recruited from outpatientdepartments. Potential participants were generally approached bya member of the research team and, if interested, were invited toparticipate and given the self-report questionnaire. There was noeconomic incentive to complete the survey. The Medical EthicsCommittee of Shanghai Mental Health Center provided ethicsapproval for the study. Respondents provided oral informedconsent to participate in the study before they completed thequestionnaire. At each hospital, 50 staff and 150 patients and theirfamily members were selected. This resulted in a sample of 1200medical staff and 3600 consumers.
Statistical analysis
We used Epidata (version 3.1) for data entry and SPSS (version15.0) for analysis. We summarized medical staff and consumerdemographics using means (SD) and medians (inter quartile range)if the data were skewed. We calculated the proportion of respon-dents agreeing with the statements relating to attitudes in clinical
trials. To test differences in attitudes, we used the Pearson chisquared test. Significance levels were set at p < 0.01.
Role of the funding source
The sponsor had no role in the design, execution, data analysis,or writing of the study. The corresponding author had full access toall study data and has final responsibility for the content of thisarticle.
Results
Overall, 100% of medical staff (1200/1200) and 98.6% of patientsand their family members (3550/3600) responded to the survey.However, we excluded the questionnaires of 23 medical staff and94 consumers because more than 5% of the data were missing intheir questionnaire responses. The final analysis included 1177medical staff and 3456 consumers, as shown in Appendix A.
The 1177 medical staff included 569 (48.3%) doctors, 561 (47.7%)nurses and 37 (4%) other staff, with the mean length of servicebeing 12.2 years. The consumer sample included 1569 (45.4%)patients and 1885 (54.5%) family members (missing details ¼ 2).The median age of first onset of mental health problems forconsumer participants (i.e., the patient or the affected familymember) was 24 years (25e75 percentile ¼ 19.0e31.0, n ¼ 2567).There were 2653 (76.8% of 3456) patients (or the family member’scare recipient) with major psychosis or schizophrenia, 557 (16.1%)with organic mental disorders including alcohol dependence andepilepsy, 206 (6.0%) with mood disorders, and 40 (1.2%) withanxiety disorders and personality disorders. The characteristics ofthe respondents are shown in Appendix B. The results we presenthere are from unweighted analyses.
Willingness to participate in clinical trials
Amongmedical staff, 245 (20.8%) had talkedwith patients aboutparticipating in clinical trials. About 2/3 (66.2%) of the remainingmedical staff who had no experience with clinical trials agreed thatthey would invite their patients to participate in clinical trials ifgiven the opportunity, with 231 (24.9%) indicating that the patientshould be allowed to engage in “consideration before makingdecision”. Only 82 (8.8%) thought that it was unnecessary to talkwith patients about clinical trials (see Fig. 1). Of patients and theirfamily members, 344 (10%) had participated in clinical trials. Ofthose who had not been involved in clinical trials (89.9%), 397(12.5%) indicated that they would agree to participate in clinicaltrials, 1689 (53.1%) said they would not, and 1090 (34.3%) indicatedthat they would like to engage in “consideration before making
Yes Not sure No Missing
0
20
40
60
Pe
rc
en
ta
ge
(%
)
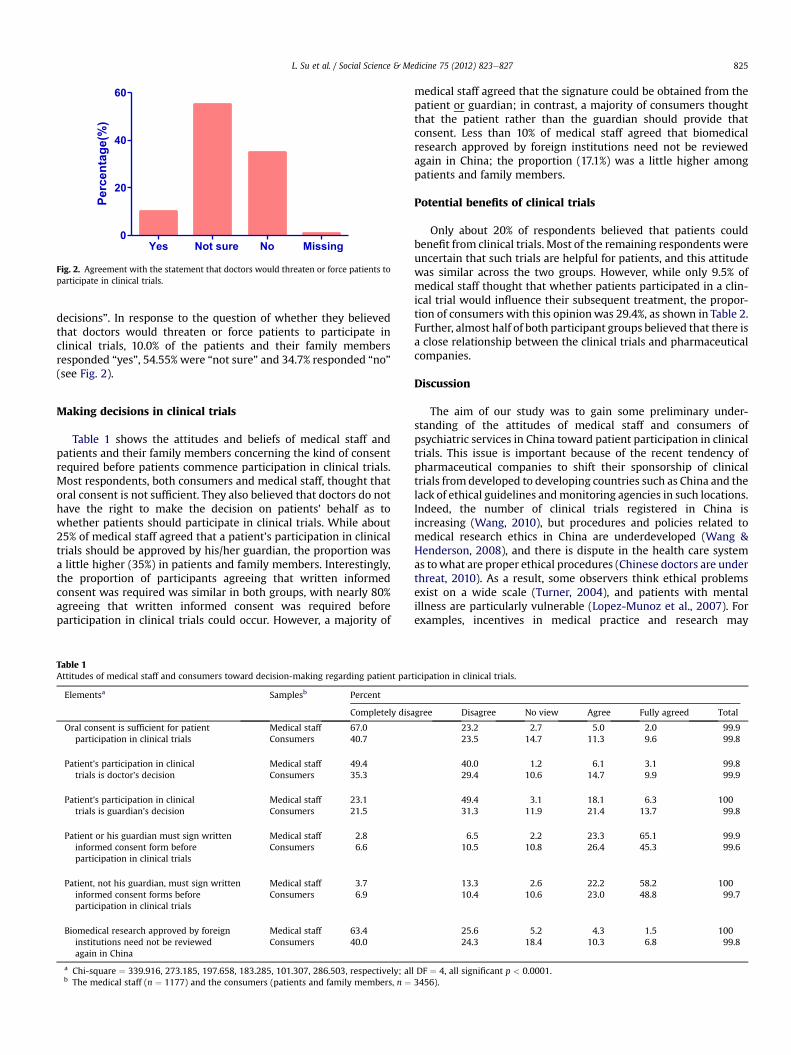
Fig. 2. Agreement with the statement that doctors would threaten or force patients toparticipate in clinical trials.
L. Su et al. / Social Science & Medicine 75 (2012) 823e827 825
decisions”. In response to the question of whether they believedthat doctors would threaten or force patients to participate inclinical trials, 10.0% of the patients and their family membersresponded “yes”, 54.55% were “not sure” and 34.7% responded “no”(see Fig. 2).
Making decisions in clinical trials
Table 1 shows the attitudes and beliefs of medical staff andpatients and their family members concerning the kind of consentrequired before patients commence participation in clinical trials.Most respondents, both consumers and medical staff, thought thatoral consent is not sufficient. They also believed that doctors do nothave the right to make the decision on patients’ behalf as towhether patients should participate in clinical trials. While about25% of medical staff agreed that a patient’s participation in clinicaltrials should be approved by his/her guardian, the proportion wasa little higher (35%) in patients and family members. Interestingly,the proportion of participants agreeing that written informedconsent was required was similar in both groups, with nearly 80%agreeing that written informed consent was required beforeparticipation in clinical trials could occur. However, a majority of
Table 1Attitudes of medical staff and consumers toward decision-making regarding patient par
Elementsa Samplesb Percent
Completely disa
Oral consent is sufficient for patientparticipation in clinical trials
Medical staff 67.0Consumers 40.7
Patient’s participation in clinicaltrials is doctor’s decision
Medical staff 49.4Consumers 35.3
Patient’s participation in clinicaltrials is guardian’s decision
Medical staff 23.1Consumers 21.5
Patient or his guardian must sign writteninformed consent form beforeparticipation in clinical trials
Medical staff 2.8Consumers 6.6
Patient, not his guardian, must sign writteninformed consent forms beforeparticipation in clinical trials
Medical staff 3.7Consumers 6.9
Biomedical research approved by foreigninstitutions need not be reviewedagain in China
Medical staff 63.4Consumers 40.0
a Chi-square ¼ 339.916, 273.185, 197.658, 183.285, 101.307, 286.503, respectively; alb The medical staff (n ¼ 1177) and the consumers (patients and family members, n ¼
medical staff agreed that the signature could be obtained from thepatient or guardian; in contrast, a majority of consumers thoughtthat the patient rather than the guardian should provide thatconsent. Less than 10% of medical staff agreed that biomedicalresearch approved by foreign institutions need not be reviewedagain in China; the proportion (17.1%) was a little higher amongpatients and family members.
Potential benefits of clinical trials
Only about 20% of respondents believed that patients couldbenefit from clinical trials. Most of the remaining respondents wereuncertain that such trials are helpful for patients, and this attitudewas similar across the two groups. However, while only 9.5% ofmedical staff thought that whether patients participated in a clin-ical trial would influence their subsequent treatment, the propor-tion of consumers with this opinionwas 29.4%, as shown in Table 2.Further, almost half of both participant groups believed that there isa close relationship between the clinical trials and pharmaceuticalcompanies.
Discussion
The aim of our study was to gain some preliminary under-standing of the attitudes of medical staff and consumers ofpsychiatric services in China toward patient participation in clinicaltrials. This issue is important because of the recent tendency ofpharmaceutical companies to shift their sponsorship of clinicaltrials from developed to developing countries such as China and thelack of ethical guidelines andmonitoring agencies in such locations.Indeed, the number of clinical trials registered in China isincreasing (Wang, 2010), but procedures and policies related tomedical research ethics in China are underdeveloped (Wang &Henderson, 2008), and there is dispute in the health care systemas towhat are proper ethical procedures (Chinese doctors are underthreat, 2010). As a result, some observers think ethical problemsexist on a wide scale (Turner, 2004), and patients with mentalillness are particularly vulnerable (Lopez-Munoz et al., 2007). Forexamples, incentives in medical practice and research may
ticipation in clinical trials.
gree Disagree No view Agree Fully agreed Total
23.2 2.7 5.0 2.0 99.923.5 14.7 11.3 9.6 99.8
40.0 1.2 6.1 3.1 99.829.4 10.6 14.7 9.9 99.9
49.4 3.1 18.1 6.3 10031.3 11.9 21.4 13.7 99.8
6.5 2.2 23.3 65.1 99.910.5 10.8 26.4 45.3 99.6
13.3 2.6 22.2 58.2 10010.4 10.6 23.0 48.8 99.7
25.6 5.2 4.3 1.5 10024.3 18.4 10.3 6.8 99.8
l DF ¼ 4, all significant p < 0.0001.3456).

Table 2Attitudes of medical staff and consumers toward potential benefits of participation in clinical trials.
Elementsa Medical staff (%) (n ¼ 1177) Patients and family member (%) (n ¼ 3456)
Yes Uncertain No Total Yes Uncertain No Total
Clinical trials are/can be beneficial topatients’ treatment
18.4 78.5 3.1 100 17.4 65.5 15.8 98.7
Treatment would be influenced if thepatients refused to participate in clinical trials
9.5 67.6 22.9 100 29.4 36.8 33.4 99.6
The relationship between the clinicaltrials and pharmaceutical companies is too close
40.6 54.9 4.4 99.9 45.1 49.2 5.5 99.8
a Chi-squared ¼ 133.010 (p < 0.0001), 360.988 (p < 0.0001), 11.611 (p ¼ 0.0030), respectively.
L. Su et al. / Social Science & Medicine 75 (2012) 823e827826
exacerbate the potential for conflicts of interest, which may violatepatients’ rights (Welsh & Deahl, 2002).
We found that in our large samples, about 20% of medical staffand 10% of consumers had experience relating to clinical trials.About 2/3 of the remaining medical staff who had no experiencewanted patients to participate in clinical trials; however, only 12%of the patients and family members had the motivation to do so.The difference in attitudes toward clinical trials between medicalstaff and patients may be due to their education and roles.However, it has the potential to influence doctorepatientrelationships.
Most of the patients and their family members did not believethat their doctors would threaten or force them to participate inclinical trials, and most were not worried that their subsequenttreatment would be influenced if they refused to participate. Thisconfidence may be due to the fact that laws and regulations havealready been set up in some large cities such as Beijing andShanghai or entered into the legislative process in other locations(e.g., Guangdong Province, where Guangzhou is located), and thus,patients feel that their rights are adequately protected. However,there is still no national mental health law in China, despite twodecades of effort (Phillips et al., 2009), and the BMJ recentlyreported a case of China’s psychiatric hospitals being used to stiflea dissident (Parry & Cui, 2010). This may be an extreme phenom-enon in western and central China, which are less developed.However, we think that the establishment of a national mentalhealth law would improve medical ethics and protect patients’rights.
Most of the consumers and medical staff in our study disagreedwith the statement that doctors should decide whether patientsshould participate in clinical trials. However, interestingly, medicalstaff disagreed more. This suggests that the medical professionalsmay be eager to stay out of this decision-making role, perhapsbecause such making such a decision is a risk factor that they wishto avoid. For example, for many Chinese doctors, personal safety isof great concern because Chinese doctors are often victims ofviolence (Chinese doctors are under threat, 2010). We suggest thatthis potential risk makes medical professionals more prudent andcareful in clinical practice, including being reluctant to makedecisions about their patients’ participation in clinical trials.
Only about 1/4 of medical staff and 1/3 of consumers acceptedthe rights of a guardian to make decisions pertaining to clinicaltrials on behalf of the patient. Nearly all of respondents agreed thatwritten informed consent was required before patients’ participa-tion in clinical trials could commence. Both groups preferredwritten informed consent from patients themselves; however,while most medical staff would accept written informed consentfrom the patient or guardian, consumers preferred that patientsrather than guardians provide this written consent. Patients withmental illness in China have no capacity for civil conduct duringtheir acute stage according to law. However, there is no temporarycourt to identify “mental illness” and “acute stage” in China’s
psychiatric hospitals, so the patients’ voices are seldom heard. Asa result, excessive powers of the guardian, such as the right to seekcompulsory admission of their family member, exist in China. Wethink it is necessary to try to avoid the participation in clinical trialsof patients with mental illness based on decisions made by doctorsand guardians. Ensuring that patients must give their owninformed consent to participate in a clinical trial could protectdoctors and hospitals avoiding judicial proceedings by patients andcould help protect patients (Munro, 2000).
Clinical trials provide scientific evidence for practice guidelines(Ulrich et al., 2010). It is of concern that most participants in bothgroups did not agree that clinical trials could lead to improvedtreatments for patients and believed that clinical trials werecompromised by sponsorship from pharmaceutical companies.This attitude, which may be due to China’s imperfect health caresystem and negative coverage by the popular media in recent years(Yang & Fan, 2012), may influence patients’ willingness to partici-pate in research. China could lead the world not only in researchquantity, but also in quality (Reforming research in China, 2007),but in the short term, at least in psychiatry, this is not the case.Slow-to-complete trials tend to lag behind changes in new tech-nology and therapies and so may provide obsolete results (Ulrichet al., 2010). Difficult and careful work needs to be undertakenbefore large sample psychiatric clinical trials such as CATIE can beexecuted (Stroup et al., 2005).
The findings of this study need to be considered in the context ofseveral limitations. First and foremost, the convenience sample ofpatients and their family members from 24 psychiatric sites wasnot representative of all consumers of mental health services inChina. However, these individuals, who sought professional help,were potential participants for clinical trials. Second, the sampleswere from developed regions of China. Developments in clinicaltrials and scientific evidence are not equally spread across allregions of China, so developed areas and large cities, such asShanghai, Beijing and Guangzhou are not representative of China’sscientific research situation. Lastly, we did not distinguish betweendoctors and nurses in medical staff or between patients and familymembers as consumers. Nevertheless, we think it is helpful todocument the differences between medical staff and consumerattitudes.
Conclusion
This preliminary study provides the first data investigating theattitudes of medical staff at psychiatric hospitals and mental healthservice consumers in China. The results suggest that there isa significant difference in the attitudes of doctors and patientstoward clinical trials. Medical professionals were more positive intheir attitude toward their patients participating in clinical trials,and they were accepting of informed consent being provided byguardians. The ability of guardians to provide consent mightpotentially impair patients’ rights. Better education of staff and

L. Su et al. / Social Science & Medicine 75 (2012) 823e827 827
patients may encourage both to change their attitudes. Organiza-tions such as the Special Committee on Unethical PsychiatricPractices (SCOUPP) could be set up in China to raise awareness andavoid abuses of human rights. Finally, efforts should be made topromote the trust of the public in medical research.
Funding
The study was made possible by the research funding providedby the Major National Special Fund of China (2008ZX09312-003)and Shanghai Medical Ethics Society Fund (2011-002).
Competing interests
None declared.
Acknowledgments
We thank all the participants in our survey, and staff for makingconditions convenient for us to perform this research and forassisting us in completing this study.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.socscimed.2012.03.056.
References
Blumenthal, D., & Hsiao, W. (2005). Privatization and its discontents e the evolvingChinese health care system. New England Journal of Medicine, 353, 1165e1170.
Borry, P., Schotsmans, P., & Dierickx, K. (2005). Developing countries and bioethicalresearch. New England Journal of Medicine, 353, 852e853.
Chinese doctors are under threat. (2010). Lancet, 376, 657.Deahl, M. (2002). Commentary: the alleged abuses of human rights in Chinese
psychiatry. Psychiatric Bulletin, 26, 445.Demyttenaere, K., Bruffaerts, R., Posada-Villa, J., Gasquet, I., Kovess, V., Lepine, J. P.,
et al. (2004). Prevalence, severity, and unmet need for treatment of mentaldisorders in the world health organization world mental health surveys. JAMA,291, 2581e2590.
Glickman, S. W., McHutchison, J. G., Peterson, E. D., Cairns, C. B., Harrington, R. A.,Califf, R. M., et al. (2009). Ethical and scientific implications of the globalizationof clinical research. New England Journal of Medicine, 360, 816e823.
Lopez-Munoz, F., Alamo, C., Dudley, M., Rubio, G., Garcia-Garcia, P., Molina, J. D.,et al. (2007). Psychiatry and political-institutional abuse from the historicalperspective: the ethical lessons of the Nuremberg trial on their 60th anniver-sary. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 31, 791e806.
Munro, R. (2000). Judicial psychiatry in China and its political abuses. ColumbiaJournal of Asian Law, 14, 1e125.
Parry, J., & Cui, W. (2010). China’s psychiatric hospitals collude with officials to stifledissent, say civil rights’ groups. BMJ, 340.
Phillips, M. R., Zhang, J., Shi, Q., Song, Z., Ding, Z., Pang, S., et al. (2009). Prevalence,treatment, and associated disability of mental disorders in four provinces inChina during 2001e05: an epidemiological survey. Lancet, 373, 2041e2053.
Psychiatric institutions in China. (2010). Lancet, 376, 2.Reforming research in China. (2007). Lancet, 369, 880.Research and ethics in China. (2009). Lancet, 374, 502.Stroup, S., Appelbaum, P., Swartz, M., Patel, M., Davis, S., Jeste, D., et al. (2005).
Decision-making capacity for research participation among individuals in theCATIE schizophrenia trial. Schizophrenia Research, 80, 1e8.
Turner, L. (2004). Bioethics needs to rethink its agenda. BMJ, 328, 175.Ulrich, C. M., James, J. L., Walker, E. M., Stine, S. H., Gore, E., Prestidge, B., et al.
(2010). RTOG physician and research associate attitudes, beliefs and practicesregarding clinical trials: implications for improving patient recruitment.Contemporary Clinical Trials, 31, 221e228.
Wang, J. (2010). Evidence-based medicine in China. Lancet, 375, 532e533.Wang, R., & Henderson, G. E. (2008). Medical research ethics in China. Lancet, 372,
1867e1868.Welsh, S., & Deahl, M. P. (2002). Modern psychiatric ethics. Lancet, 359, 253e255.Yang, Z., & Fan, D. (2012). How to solve the crisis behind Bribegate for Chinese
doctors. Lancet, 379, e12ee15.