the red eye - yorkgpvts.co.uk · questions • one eye or both • painful / itchy / scratchy •...
TRANSCRIPT

The red eye
Tim Manners MRCGP FRCOphthConsultant Ophthalmologist
equipment
• Snellen chart• Pinhole• Daylight• Fluorescein• Illuminated magnifier (auriscope head)• Paper clip• Proxymetacaine minims
What do you do?
What do you do?
• Ask a few questions• Have a look• Ask more if necessary• Find your eye things• Look again.

questions

questions
• One eye or both• Painful / itchy / scratchy• Trauma• How long• Contact lenses• Stuck together• History of same or same in others/family• Associated URTI• Any treatment
1st look
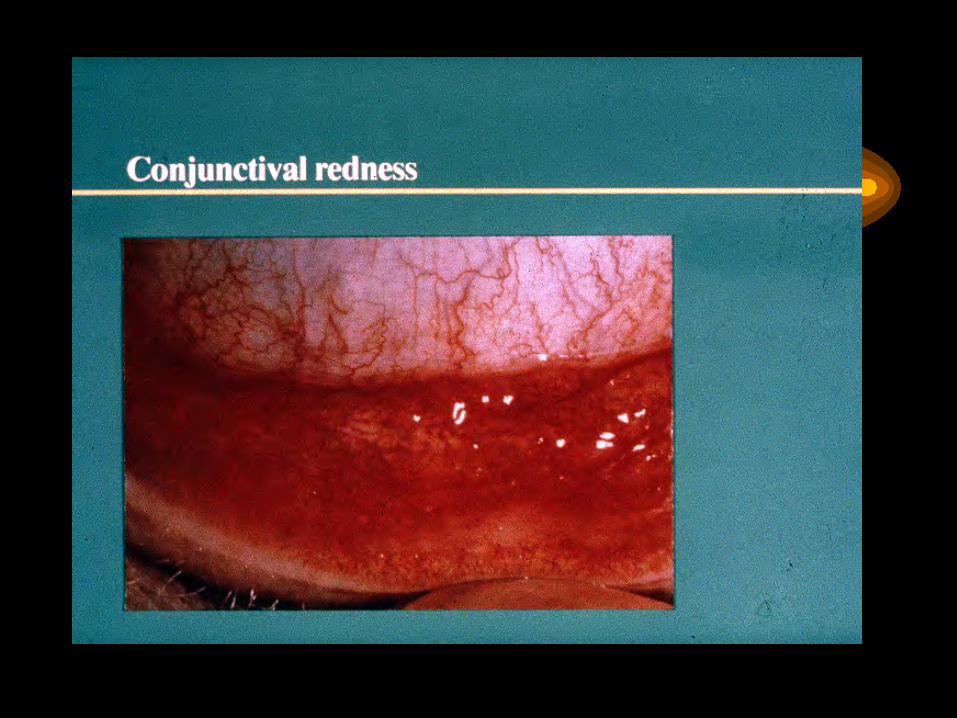
– How old– One or both– Acuity affected– Pattern of redness in daylight– Pupil-reactive? shape? – Cornea- bright or cloudy– Look for foreign body

2nd look
• Fluorescein-stains corneal injury(abrasion, fb, herpes. All unilateral)
• Local anaesthetic-is pain relieved?• Magnifier-lumps on palpebral conjunctiva and good
look at cornea• Evert lid if fb suspected (wipe)• Feel for pre auric lmyph nodes

conjunctivitis
• Viral• Bacterial• chlamydial• allergic

viral
– Watery– Unilateral then bilateral– Often with urti and preauric nodes– May be trivial to severe– May need referral if painful– May last weeks– sometimes epidemic

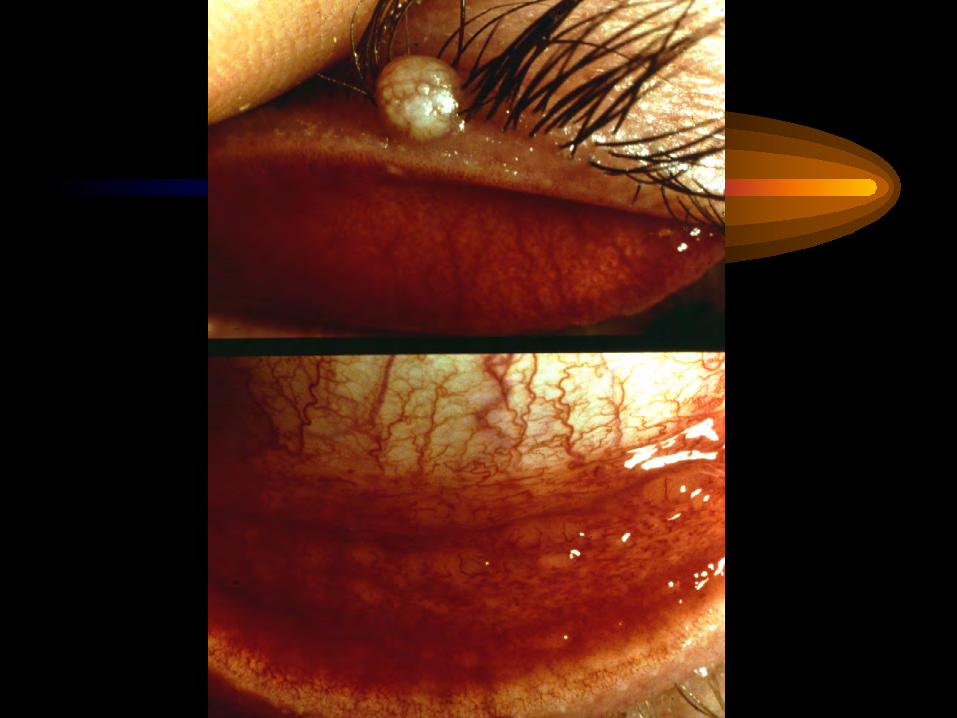

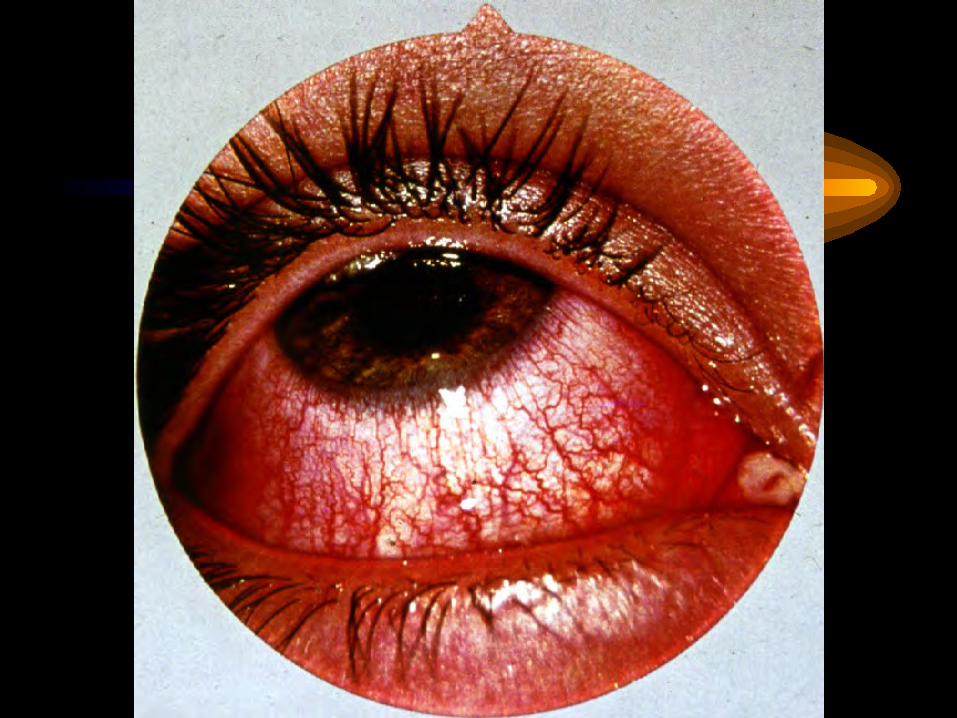
bacterial
– Usually bilateral– Sticky in am– Not usually painful– Self limiting, lasts days.– Treat with chloro, or fucidin in children
allergic
– Itchy– Seasonal or perennial– Hay fever– Chronic severe types may need steroids esp in
children/teenagers– sensitised to drops or preservatives





Corneal causes
• Abrasion• Foreign body• Corneal ulcer
• Contact lenses, herpetic
• Other rarer causes• Look for cloudy cornea• Any corneal cause needs slit lamp exam to confirm




herpetic
– Simplex usually corneal except as primary infection and commonly recurrent
– Zoster causes immune mediated intra ocular inflammation 2-any weeks after infection
– Signs of uveitis– Corneal denervation– Raised iop common


blepharitis
• Itching• burning• mild pain• fb sensation• tearing or dry• crusting• recurrent and variable

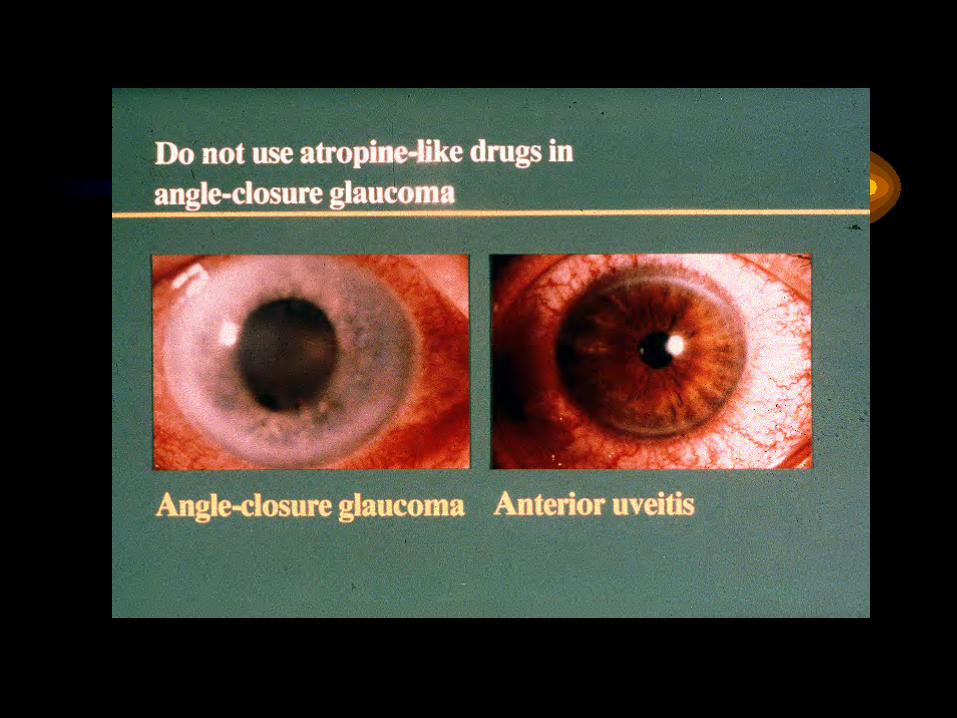
uveitis
– Usually unilateral or asymmetric– Painful, unrelieved by local– Circumcorneal injection– Recurrent– May be systemic associations
• HLA B27. Sarcoid etc– Needs referral
• Only indication in 1care for steroids if recurrent before slit lamp examination


episcleritis
• Sectorial or diffuse• Usually asymptomatic other than redness• Self limiting

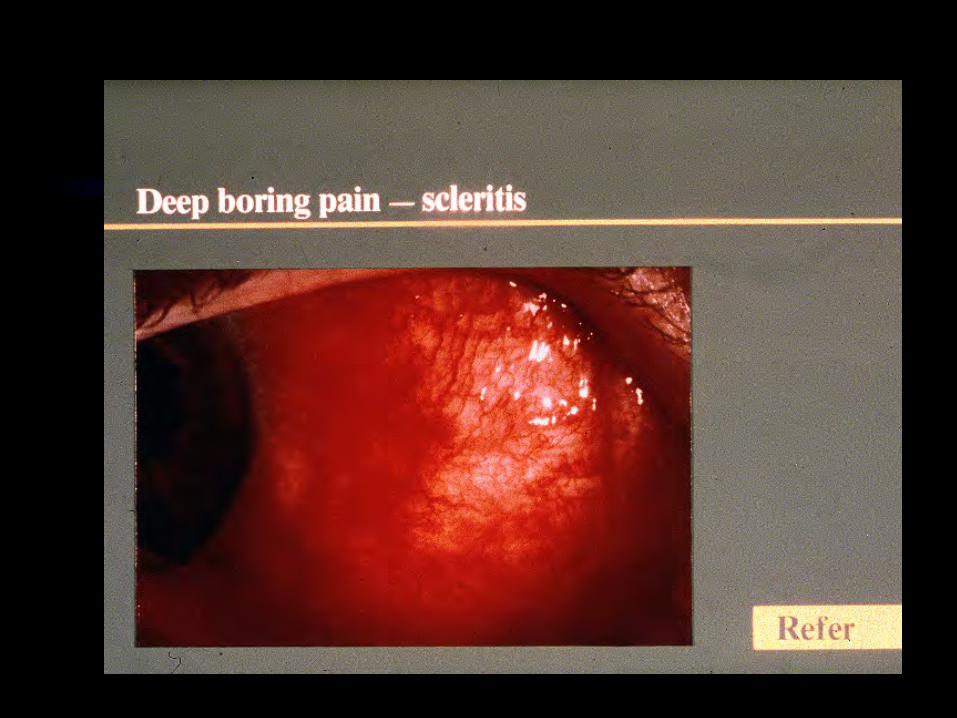
scleritis
– Immune mediated- complex deposition– Needs systemic Ix and Rx– Painful and usually bilateral– Try nsaids, then steroids then others

Acute glaucoma
• 60s-80s, in winter• Degree of pain• Fixed pupil, mid dilated• Variable injection


Before Rx any red eye
• Exclude foreign body• exclude corneal problem• exclude uveitis,scleritis, acute glaucoma
– history, degree of pain, lack of discharge,laterality, examination.
• NO OTHER PROBLEM WOULD SUFFER FROM A COURSE OF ANTIBIOTIC DROPS.