the impact of nanoparticles on cellular functions
TRANSCRIPT

1
SCBM342-Cardiovascular Pathology
Associate Professor Dr. Wannee Jiraungkoorskul
Department of Pathobiology, Faculty of Science, Mahidol University
Tel: 02-201-5563, E-mail: [email protected]

2
• Mr. A is 55 years old, high 158 cm and weight 82 kg. He
works as the personal officer more than 30 years, smokes
cigarette 1 pack/day and drinks 2-3 times/week. What are
the risk factors of his disease or illness?
Problem

3
Cardiovascular Pathology
• Cardiac Failure
• Cardiac Adaptation
• Myocardial Infarction
• Endocarditis
• Myocarditis
• Pericarditis
• Cardiac tumor

4
• Heart failure is a clinical syndrome not a disease.
• The heart is unable to pump sufficient blood to the body
tissues to meet ordinary metabolic demands.
• HF is defined as “a complex clinical syndrome that an result
from any structural of functional cardiac disorder that
impairs the ability of the ventricle to eject blood (systolic
heart failure) or to fill with blood (diastolic heart failure) .”
(American Heart Association Guidelines 2013)
CARDIAC FAILURE: Definition

5
• Ischemic heart disease ~ 40 percent
• Dilated cardiomyopathy ~ 30 percent
• Primary valvular heart disease ~ 15 percent
• Hypertensive heart disease ~ 10 percent
• Other ~ 5 percent
CARDIAC FAILURE: Causes

6http://saypeople.com/wp-content/uploads/2011/05/Heart-failure-Symptoms.gif
Clinical Manifestations of CHF

7http://image.slidesharecdn.com/chf-140124151550-phpapp02/95/congestive-heart-failure-6-638.jpg?cb=1390576817

8
• Left heart failure
• Increase diastolic volume causes
– pulmonary congestion, edema, hemoptysis
• Decreased output causes
– renal ischemia, acute tubular necrosis, oliguria
– CNS ischemia, confusion
– bowel ischemia, GI bleeding, sepsis
– skeletal muscle ischemia, weakness, fatigue
CARDIAC FAILURE

9
Pulmonary edema and congestion

10
Pulmonary edema and congestion

11
Heart failure cells (Hemosiderin-laden macrophages)

12
“Heart failure cells” in lung

13
• Right heart failure
• Increase diastolic volume causes
– visceral congestion, edema and effusions
– pitting edema
• Usually caused by left heart failure
CARDIAC FAILURE

14

15
Nutmeg (ลกูจันทนเ์ทศ)Liver (passive congestion)
Myristica fragans

16
Liver, passive congestion

17
Pitting edema of leg in right heart failure

18
• What is not one of the main symptoms of heart failure?
A. Edema
B. Cool hands
C. Reduced urinary output
D. Shortness of breath
E. Stomach pain

19
• What is not a primary cause of heart failure?
A. Cardiomyopathy
B. Coronary artery disease
C. High blood pressure
D. Valvular disease
E. Polio

20
• What is the name for shortness of breath when lying
down?
A. Apnea
B. Orthopnea
C. Narcolepsy
D. Paroxysmal nocturnal dyspnea
E. Sleep apnea

21
• Right heart failure causes each of the following except:
A. Splenomegaly
B. Pulmonary edema
C. Ankle edema
D.Distended neck veins
E. Liver congestion

22
CARDIAC ADAPTATION
• CO = HR x SV (Male 5.6 L/min, Female 4.9 L/min)
• HR 60-180 beats per minute, SV 70-120 ml
Major cardiac adaptive changes to increased workload
• 1. Heart rate increases
• 2. Stroke volume increases
• 3. Hypertrophy

23

24

2525

2626

27
• Each of the following result in left ventricular hypertrophy
except:
A. Aortic stenosis
B. Coarctation of the aorta
C. Mitral stenosis
D.Severe prolonged anemia
E. Systemic hypertension

28
MYOCARDIAL INFARCTION
Etiology and pathogenesis
- Atherosclerosis of coronary arteries
- Decreased supply (atherosclerotic stenosis, coronary
thrombosis, vasospasm)
- Increased O2 demand (e.g., LVH due to hypertension or
aortic stenosis)
- Decreased pO2 with fixed stenosis (e.g., pulmonary
disease, anemia, high altitude, CO poisoning)
- M : F = 2-6 : 1

29

3030

31
48-hour-myocardial infarct
4 to 7 days MI
2 months MI
MYOCARDIAL INFARCTION

32

33

34
One-day-old infarct 3 to 4 days' duration
7 to 10 days’ duration Granulation tissues

35Well-healed myocardial infarct
36
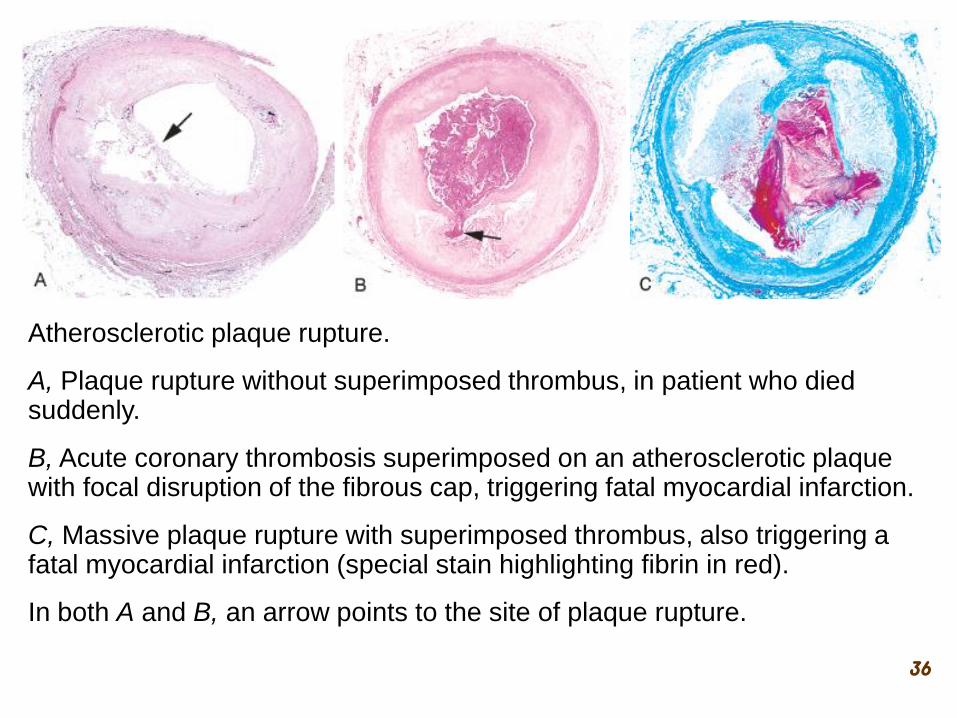
Atherosclerotic plaque rupture.
A, Plaque rupture without superimposed thrombus, in patient who died suddenly.
B, Acute coronary thrombosis superimposed on an atherosclerotic plaque with focal disruption of the fibrous cap, triggering fatal myocardial infarction.
C, Massive plaque rupture with superimposed thrombus, also triggering a fatal myocardial infarction (special stain highlighting fibrin in red).
In both A and B, an arrow points to the site of plaque rupture.

37
Schematic representation of
sequential progression of
coronary artery lesion
morphology, beginning with
stable chronic plaque
responsible for typical
angina and leading to the
various acute coronary
syndromes.

38

39

40

41

42

43

44

45

46
Acute myocardial infarct, predominantly of the posterolateral left ventricle,
demonstrated histochemically by a lack of staining by the
triphenyltetrazolium chloride (TTC) stain in areas of necrosis (arrow). The
staining defect is due to the enzyme leakage that follows cell death. Note
the myocardial hemorrhage at one edge of the infarct that was associated
with cardiac rupture, and the anterior scar (arrowhead), indicative of old
infarct. (Specimen the oriented with the posterior wall at the top.)

47
• What term refers to damage of the heart muscle due to
inadequate blood flow?
A. Non-ischemic cardiomyopathy
B. Dilated cardiomyopathy
C. Hypertrophic cardiomyopathy
D. Ischemic cardiomyopathy
E. Cardioplegia

48
• Myocardial infarction or heart attack occurs when there is
blood clotting in_____.
A. Aorta
B. Coronary artery
C. Hepatic artery
D.Mesenteric artery
E. Renal artery

49
I. Types of endocarditis
– Non-infective
• acute rheumatic fever
• systemic lupus
• Non-bacterial thrombotic
– Infective
• Mainly bacterial or fungal infections
• Destroy valve tissue (non-infective doesn't)
• Thrombus with microorganisms
ENDOCARDITIS

50

51
• Inflammation
– Resulting in injury to cardiac myocyte
– Cardiac allograft rejection
– Collagen vascular disease
– Drug hypersensitivity
• Infection
– Virus
• Coxsackievirus A & B and other enterovirus (most common)
• Cytomegalovirus
• Human immunodeficiency virus
MYOCARDITIS

52
– Parasites
• Chagas’ disease (Trypanosoma cruzi)
(most common cause in S. America)
• Toxoplasmosis
– Bacteria
• Lyme disease
• Diphtheria (injury from toxin of Corynebacterium
diphtheriae)
MYOCARDITIS

53
• Morphology (Gross)
– Cardiac dilation
– Myocardium flabby,
pale, with
hemorrhage
MYOCARDITIS

54
Morphology (Microscopic):-
Acute virus infection
• Edema
• Inflammatory infiltrate of lymphocyte and other
mononuclear cell
• Myocyte degeneration and/or necrosis
• Viral inclusion may be present
MYOCARDITIS

55

56
Inflammation of the pericardium
Types and (in parentheses: causes)
- Fibrinous (MI, uremia)
- Purulent (Staphylococcus)
- Granulomatous (TB)
- Hemorrhagic (tumor, TB, uremia)
- Fibrous (constrictive)
PERICARDITIS

57
• Causes
– Infection
• virus (most common)
• pyogenic bacteria
• mycobacteria
• fungi
– Secondary
• acute myocardial infarction
• cardiac surgery
• radiation to mediastinum
PERICARDITIS
• Causes
– Systemic disorder
• uremia
• acute rheumatic fever
• systemic lupus
erythematosus
• metastatic malignancy

58

59

60
I. Most common are metastatic: lung, breast, melanoma
II. Primary tumor
Rare, but most common is left atrial myxoma
- arise from interatrial septum, on a stalk , mostly in LA
- can prolapse through MV into LV, cause CHF
- can embolize, cause stroke, etc.
CARDIAC TUMOR

61
MYXOMA
Pedunculated mass is
attached to the left arterial
endocardium.
(left -external surface, right
- cut surface)
Vascular showing basophilic myxoid stroma and stellate cells

62
Atrial myxoma
Minimal cellularity, only scattered spindle cells with scant pink cytoplasm are present in a loose myxoid stroma.

63
METASTATIC TUMOR
• Metastatic cardiac
tumors are 20X more
common than primary
tumors arising in the
heart
• Commonly from lung,
breast, lymphoma.

64
• What is the most common tumor of cardiac?
A. Cardiac squamous cell carcinoma
B. Cardiac metastasis
C. Cardiac adenocarcinoma
D.Cardiac small cell cancer
E. Cardiac large cell cancer

65
• What is the most common primary originating site of
cardiac metastases?
A. Breast cancer
B. Pancreas cancer
C. Testes cancer
D.Uterus cancer
E. Stomach cancer

66
• Atrial myxoma commonly arises from____.
A. Left atrium
B. Left ventricle
C. Right atrium
D.Right ventricle
E. Heart wall

67
• Narrowing or completely obstructing the lumina
– Atherosclerosis (thrombosis, embolism)
• Weakening of the wall.
– Dilatation or rupture
DISEASES OF ARTERIES

68
Degenerative arterial disease, segmental and
multifocal
• Characterized by intimal deposition of lipids,
which results in intimal thickening (atheroma)
and scarring
• Causes stenosis, predisposes to thrombosis
• Results in ischemia and infarction
ATHEROSCLEROSIS

69
Three types of lesions
• 1. Atheroma (raised, lipid center, dangerous)
• 2. Fatty streak (small, intracellular fat, innocuous)
• 3. Fibrous plaque (intimal scar, innocuous)
ATHEROSCLEROSIS

70
ATHEROMA LESION
Sites:
-Intimal, may involve media
- Aorta and its major branches
(coronaries, cerebrals,
peripheral, etc.)

71
ATHEROMA LESION
• Three major elements
– Necrotic center of extracellular lipid
– Fibrous cap
– Proliferating cells (myofibroblasts)

72
Mechanism for intimal thickening

73
Major components of well-developed atheromatous plaque

74
Schematic diagram of sequence of cellular events and cellular interaction in atherosclerosis

75
Summary of the pathology, pathogenesis, complications and natural history of atherosclerosis

76
Mild Severe
Fibrous plaque
Atherosclerosis, aorta

77

78

79

80

81

82

83
Atherosclerotic plaque with needles and clot

84
RISK FACTORS FOR ATHEROSCLEROSIS

85
Sites of atherosclerosis

86
Complication of
atherosclerosis

87
References
Illustrated Textbook
of Cardiovascular
Pathology.
by
P. Chopra
R. Ray
A. Saxena
2004
Practical
Cardiovascular
Pathology.
by
Allen Burke
Fabio Tavora
2010
Braunwald's Heart
Disease. 10th ed. by
Douglas Mann
Douglas Zipes
Peter Libby
Robert Bonow
2014
Practical
Cardiovascular
Pathology.
2nd ed. By
Mary Sheppard
2011

88
SCBM342
Cardiovascular Pathology