the development of a norwegian pain questionnaire
TRANSCRIPT
Pain, 46 (1991) 61-66
0 1991 Elsevier Science Publishers B.V. 0304-3959/91/$03.50
ADONIS 0304395991001544
61
PAIN 01802
The development of a Norwegian pain questionnaire
Liv Inger Strand and Alex R. Wisnes College of Physiotherapy, 5009 Bergen (Norway)
(Received 9 February 1989, revision received 26 November 1990. accepted 17 December 1990)
Summary The study was undertaken to develop a multidimensional measuring instrument for pain in the Norwegian language. The McGill Pain Questionnaire (MPQ) was used as a model as it is a valid and reliable tool for pain measurement in English speaking countries.
A series of steps were taken to develop a Norwegian pain questionnaire: (1) words describing pain were derived from 95 subjects (patients, students and health personnel); (2) 10 subjects allocated pain descriptors into groups; (31 36 college student validated the word groupings; (4) 72 patients graded the words contained in each group according to intensity; and (5) the reliability of group items was tested.
The study demonstrated that there are many descriptors of pain in the Norwegian language. The final version of the Norwegian pain questionnaire consisted of 106 pain descriptors divided into 18 groups. Validity of the classifications as well as reliability of the words was demonstrated. The actual value of the Norwegian pain questionnaire as a measuring instrument has not yet been documented.
Key words: Pain questionnaire; Pain measurement; (Norwegian)
Introduction
Assessment of pain is a major concern for health personnel in clinical practice. However, since pain is a subjective experience, its measurement can be difficult. The development of a reliable, valid and sensitive instrument for pain measurement is, therefore, an im- portant step in the documentation of clinical pain as well as in the assessment of pain-relieving methods and strategies.
Pain is commonly measured using simple intensity scales such as the Visual Analogue Scale WAS) [2,9,29]. Pain is, however, a multidimensional experience that cannot be quantified easily [231; an adequate pain measuring instrument should, therefore, reflect the many different dimensions of pain [21,24].
To address these concerns, the McGill Pain Ques- tionnaire (MPQ) was developed in the 1970s [20,22]. The questionnaire was designed to measure sensory, affective and evaluative components of the pain experi-
Correspondence to: Liv Inger Strand, College of Physiotherapy. Mc?llendalsveien 6, 5009 Bergen, Norway.
ence. The MPQ is currently the most widely used multidimensional assessment device for studies of pain in English-speaking countries [30].
A measuring instrument designed for a specific pur- pose should meet the 4 necessary methodological crite- ria of being valid, reliable, precise and feasible [lo]. The fact that the MPQ meets these criteria has been documented [4,6-8,12,13,19,20,25,27,28,311.
Several attempts have been made to develop similar pain questionnaires in other languages: Finnish [ll], French [3], Slovak [l], Italian [181 and German [26]. Different patterns of behavioural and attitudinal re- sponses to pain have been found among different eth- nic groups [32]. Semantic differences have also been demonstrated in cross-cultural studies of pain terms. In some cultures a multitude of specific pain terms are commonly used, while in other cultures a single inclu- sive term is the norm. It is speculated that differences in pain reports may be an effect of culturally modu- lated differences in pain perception. Different cultures should, therefore, use their own pain terms as a basis for cross-cultural comparisons of pain [5].
A simplified and standardized Norwegian form of the MPQ for patients with lumbago/sciatica was pub-
lished in 1983 by Ljunggren [14] and used by Ljunggren et al. [IS] in a study of patients with lumbago/sciatica in 1985. We have used the MPQ ah a model for the
development of a comprehensive Norwegian pain ques- tionnaire. However, the validity of the MPQ is lost if it
is literally translated into Norwegian. Semantic difficul-
ties arise. as no dictionary contains precise Norwegian equivalents for the meaning and intensity of the Eng-
lish words. The possibility that ethnic differences bc-
tween the English- and Norwegian-speaking popula- tions cause variations in perception, and expression of pain may further impair the validity of a directly trans-
lated MPQ.
Methods and results
A series of discrete steps were taken to develop a
Norwegian Pain Questionnaire.
(1) Collection of words describing pain Method. In Norway there are 2 official written lan-
guages: Standard and New Norwegian. Standard Nor-
wegian is generally written and spoken in the cities, while New Norwegian is primarily used in the country districts. The main difference between the 2 languages lies in word endings; however. some words used to express the same phenomenon are completely differ- ent. Since the present study was conducted in a city, the questionnaire was formulated using Standard Nor-
wegian. However, when words describing pain were being collected, participants were free to use either Standard or New Norwegian.
To obtain descriptors of pain, 95 subjects were asked to write down adjectives which could be used to de- scribe pain. The pain they were describing consisted of
( 1) pain they were presently experiencing, (2) pain they had experienced in the past, or (3) pain they had heard of or read about. Twenty-nine of the subjects (14-74
years; mean age 48 years) were patients suffering from various conditions involving pain: 8 were inpatients at a
neurological unit, 10 were inpatients at a rheumatolog- ical unit and 11 were outpatients at a physiotherapy institute. Thirty-seven of the subjects (23-56 years; mean age 37 years) were health practitioners, including
(mostly) physiotherapists, physicians and nurses. This group was expected to be familiar with pain terminol- ogy through their professional work. An additional 20 subjects (21-41 years; mean age 24 years) were college physiotherapy students from different parts of Norway. All 95 subjects were asked to list as many pain descrip- tors as possible.
Result. A total of 333 different Norwegian adjectives describing pain were noted. Ten of the subjects listed New Norwegian words. However, all these words were synonymous to those in Standard Norwegian as only
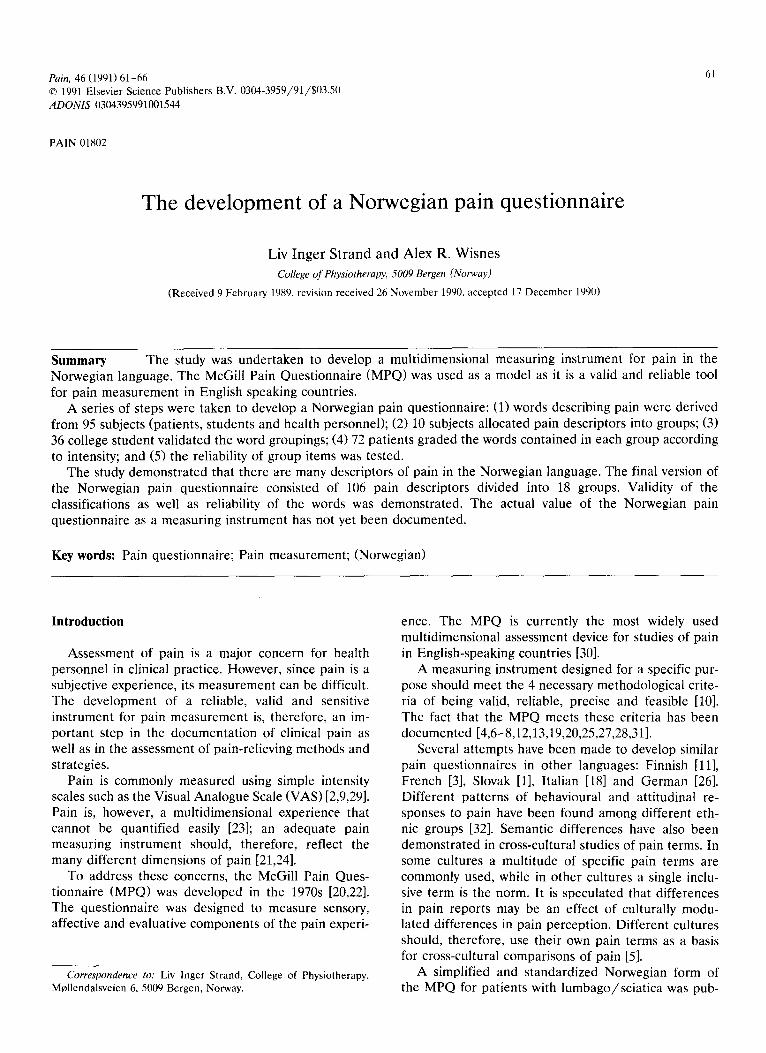
Fig. I. The number ot subject\ uho listed each pain descriptor. The
words were listed alphabetically. I’hc graph demonstrates the num-
her of subjects (N = Y.5) who listed each pain descriptor including the
words from ‘ahnorm’ to ‘klolignende.‘
their endings differed. The New Norwegian endings were changed into Standard Norwegian, and the words were included in the word list. The frequency of words listed is shown in Fig. 1.
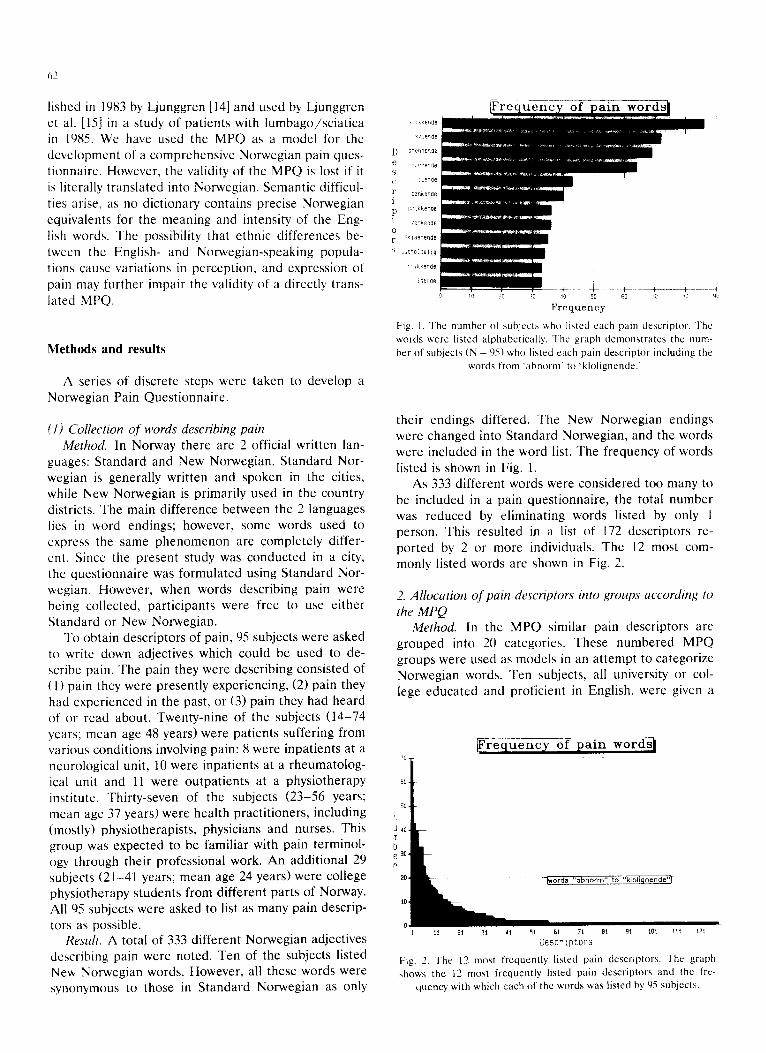
As 333 different words were considered too many to be included in a pain questionnaire, the total number was reduced by eliminating words listed by only 1 person. This resulted in a list of 172 descriptors re- ported by 2 or more individuals. The 12 most com- monly listed words are shown in Fig. 2.
2. Allocation of pain descriptors into groups according to the MPQ
Method. In the MPQ similar pain descriptors are grouped into 20 categories. These numbered MPQ groups were used as models in an attempt to categorize Norwegian words. Ten subjects, all university or col- lege educated and proficient in English. were given a
Wcrlptors
Fig. 2. The I2 most frequently l&led pain descriptors. The graph
shows the 12 most frequently listed pain descriptors and the fre-
quency with which each of the words was listed hy OS subjects.
63
copy of the MPQ categories as well as a list of Norwe- gian pain descriptors. The subjects were asked to allo- cate each Norwegian word on a content basis to the most appropriate MPQ group. The responses of the 10 subjects were analysed in the following way: (1) if at least 50% of the subjects assigned the same group number to a word, then the word was assigned to that category; (2) if less than 50% of the subjects assigned the same group number to a word, then the word was eliminated; and (3) if 50% or more of the subjects marked a word with a minus sign, then the word was eliminated.
Result. Using these criteria, 110 words were assigned to specific groups. Forty-four words, marked with mi- nus signs by at least 50% of the subjects, were elimi- nated from the list. Several of these words like mild, moderate and strong only expressed different intensity levels of pain; other words expressed a positive attitude towards the negative sensory pain experience and were therefore difficult to include in the MPQ groups. There were 4 MPQ categories (groups 10, 17, 18 and 20) to which no words were assigned. Norwegian words that appeared to correspond best to the English words in those groups were actually assigned by the subjects to one of the remaining groups. Following this initial screening, groups 1 and 2 were quite large. To facili- tate the next study, each group was subdivided into 2 other groups, each of which expressed somewhat dif- ferent aspects of temporal and spatial qualities of pain. The initial list of words was, therefore, divided into 18 separate groups: 12 sensory, 5 affective and 1 evalua- tive.
3. Validation of word groupings Method. Thirty-six college students were given copies
of the MPQ and the Norwegian word groups. They were asked to study the English MPQ categories care- fully and then agree or disagree with the allocation of each Norwegian word. If a word was perceived as belonging to another group, the number of that alter- native group was given. If a word was not found to fit into any of the categories, a minus sign was put behind the word. The minimum requirement for maintaining a word in a group was that 2/3 of the participants must be in agreement.
Result. This study validated the preliminary word groups; 88% of all the words were agreed upon by 90% of the participants, and only 4 words were not agreed upon by 2/3 of the participants. 106 pain descriptors remained in the Norwegian Pain Questionnaire after this initial validation.
4. Intensity grading of pain descriptors Method. Ninety-six patients with painful medical dis-
orders were asked to grade 106 pain descriptors ac- cording to intensity. The patients were selected by
their physiotherapist from rheumatological, or- thopaedic, surgical, neurological and rehabilitation hospital units, a pain clinic and 3 outpatient physio- therapy institutes. A lo-cm VAS was used to measure the relative intensity of each word; it was anchored on the left by ‘no pain’ and on the right by ‘unbearable pain.’ The words in each group were listed alphabeti- cally, and the VAS was placed to the right of each word.
Patients were asked to mark the VAS according to the perceived intensity of the pain described by the word. They were then asked to mark each word which was an adequate descriptor of the pain that they were presently experiencing. The subjects were allowed to choose as many words as they liked from each group to describe their pain. If, however, they chose more than one word from a group, they were asked to underline the word which best described their pain. To deter- mine whether 106 words were sufficient to describe clinical pain fully, the patients were also asked if any words were missing which they considered important to describe their pain adequately. They were asked to write these words down.
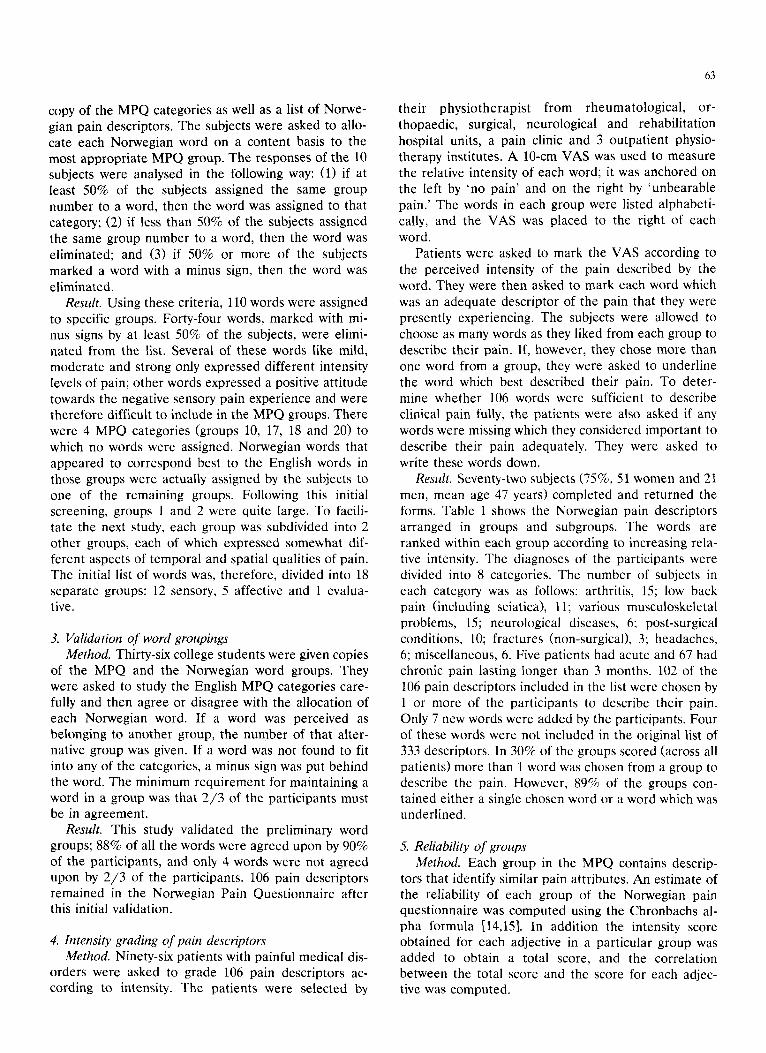
Result. Seventy-two subjects (75%, 51 women and 21 men, mean age 47 years) completed and returned the forms. Table I shows the Norwegian pain descriptors arranged in groups and subgroups. The words are ranked within each group according to increasing rela- tive intensity. The diagnoses of the participants were divided into 8 categories. The number of subjects in each category was as follows: arthritis, 15; low back pain (including sciatica), 11; various musculoskeletal problems, 15; neurological diseases, 6; post-surgical conditions, 10; fractures (non-surgical), 3; headaches, 6; miscellaneous, 6. Five patients had acute and 67 had chronic pain lasting longer than 3 months. 102 of the 106 pain descriptors included in the list were chosen by 1 or more of the participants to describe their pain. Only 7 new words were added by the participants. Four of these words were not included in the original list of 333 descriptors. In 30% of the groups scored (across all patients) more than 1 word was chosen from a group to describe the pain. However, 89% of the groups con- tained either a single chosen word or a word which was underlined.
5. Reliability of groups Method. Each group in the MPQ contains descrip-
tors that identify similar pain attributes. An estimate of the reliability of each group of the Norwegian pain questionnaire was computed using the Chronbachs al- pha formula [14,151. In addition the intensity score obtained for each adjective in a particular group was added to obtain a total score, and the correlation between the total score and the score for each adjec- tive was computed.
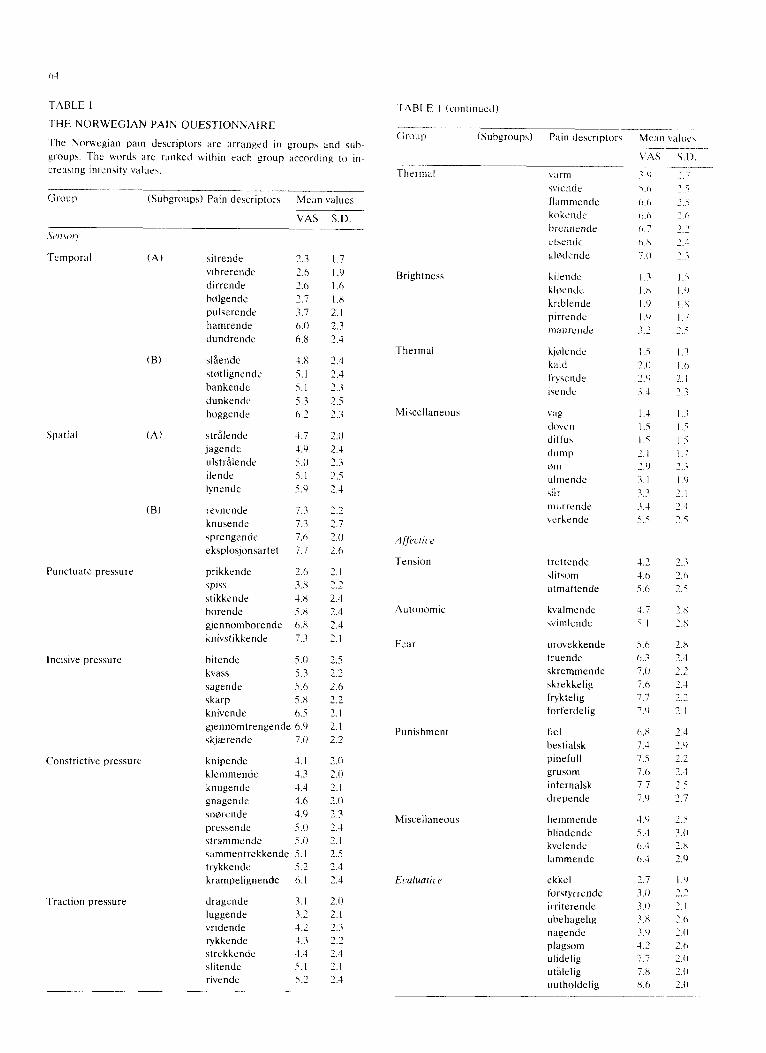
TABLE 1
THE NORWEGIAN PAIN QUESTIONNAIRE
The Norwegian pain descriptors are arranged in groups and suh-
groups. The words are ranked within each group according to in-
creasing intensity value\.
Group (Subgroups) Pain descriptor\ Mean values
VAS S.D.
Spatial
Punctuate pressure
Incisive pressure
Temporal (A) sitrende
vibrerende
dirrende
htilgende
pulserende
hamrende
dundrende
(B) slsende
sttitlignende
bankende
dunkende
hoygende
(A) strfilende
jagende
ul5trilende
ilende
lynende
(B) revnende
knusende
sprengende
eksplosjonsartet
prikkende
SPiSS
stikkende
horende
gjennomborende
knivstikkende
bitende
kvass
sagende
skarp
knivende
Constrictive pressure
Traction pressure
gjennomtrengende 6.9 2.1
skjrrtrende 7.1) 2.2
knipende 1.1 2.U
klemmende 4.3 2.0
knugende 1.4 7.1
gnagende 1.6 2.0
snfirende 4.9 2.3
pressende 5.0 2.4
\trammende 5.0 7.1
sammentrekkende 5. I 2.5
trykkende 5.2 2.4
krampelignende 0.1 2.4
dragende 3.1 2.0
luggende 3.7 2.1
vridende 4.2 2.3
rykkende 5.3 2.2
strekkende 4.3 I-1
slitende 5. I 2.1
rivende 5.7 2.3
1.7
I.9
I.6
1.x
2.1
2.3
2.1
2.4
2.4
2.3
2.5
2.3
2.0
7.4
1.3
2.5
2.4
2.2
2.1
2.0
2.6
?.I
2.2
7.-l
2.4
2.4
?.I
7.5
2.2
2.6
2.2
2.1
Brightness
Thermal
Tension
Autonomic
Fear
(;roup (Subgroups) Pain dtwriptor\ Mean v;~lue\
~______ Thermal \;trm
\\ iendc
l’l;m~mendc
hokende
bwnnende
Cl\Cll&
gll?dende
v/u 7.0
5.6
11.0
Il.0
Il.7 1).X
7.0
-
kilendc 1.3 klwnde I .H
krlblende I .Y
pirrende I .Y
maurcnde .%.2
kjtilencle
kald
iryszndr
Iwndc
\ ag
cloven
diffua
dump
+)rn
ulmende 0
s;,,
murrende
cerkende
trettende
4litsom
utmattende
kkalmende
wimlende
1.7
i I
urovekkende
truende
skremmende
skrekkelig
ftyktelig
forferdelig
Punishment fZl
hrstialsk
pinefull
grusom
infernalsk
drepende
Miscellaneous hcmmende
blindende
kvclende
lammende
ekkel
forstyrrende
irriterende
uhehagelig
nagende
plagsom
ulidelig
utHlelig
uutholdelig
5.6
0.3
7.0
7.0
7.7
7.‘)
6.X
1.4
7.5
7.0
7.7
7.0
4.9
5.4
h.4
0.4
2.7
2.1)
3.0
7.X
.:.o
1.2
7.7
7.x
X.6
63
Result. A high internal reliability (Kuder-Richard- son score) was indicated for all groups. They all ob- tained measures of reliability of at least 0.60; 11 of the 18 groups obtained scores of at least 0.80. As expected all adjectives showed a positive correlation with the corresponding total score of the actual group. Ninety- one words (total 106 words) had a correlation greater than 0.50. The scores indicate that all adjectives mea- sure pain along the same dimension as other adjectives in the same group. Of the adjectives with relatively low scores defined as less than 0.50, 7 words are in group 12, 4 words in group 18 and 1 word in each of the groups numbered 1, 7, 9 and 10. Seven out of 9 words in group 12 have relatively low correlation scores. This group might be considered a ‘miscellaneous’ sensory group.
Discussion
The present study revealed a remarkably long list of Norwegian pain descriptors. The original list of 333 Norwegian words had to be reduced to make a feasible questionnaire. However, it is important to note that about half of the 333 words were listed only once by the 96 subjects; these words were deleted from the questionnaire. The fact that the curve showing the distribution of word frequencies is hyperbolic gives evidence that a relatively small number of pain descrip- tors are most frequently used. This observation sup- ports the otherwise arbitrary decision to delete words chosen only once. The hyperbolic shape of the curve is also consistent with the very large number of infre- quently used pain descriptors. It is, therefore, not surprising that the final group of 72 pain patients listed 4 new words which were not even included in the original list of 333 pain descriptors. It is probably impossible to achieve a complete list of pain descrip- tors.
Ten of the subjects listed New Norwegian words. These were descriptors commonly listed by the subjects using Standard Norwegian, the only difference being the word endings used. It therefore seems reasonable to suggest that the questionnaire can be applied in both New Norwegian and Standard Norwegian.
Evidence of validity was demonstrated by the fact that the questionnaire contained pain descriptors com- monly used by Norwegians. Only 7 words had to be added to the questionnaire to describe the quality of pain of 72 subjects. Each of the 7 words was listed only once. This result indicates that the key descriptors of pain are contained within the word groups. Validity of word classification was demonstrated. There was con- siderable agreement as to the assigned grouping of most words as judged by 36 college students. This result supports the view that the words contained in
each group express related qualities of pain. Internal consistency for all groups was also demonstrated. The relatively high scores obtained indicate group reliabil- ity. All adjectives were found to give positive correla- tion, evidence that all words within a group can be used as part of the same measure of the actual quality of pain.
As in the MPQ, Norwegian pain descriptors are listed according to increasing intensity within each group, In the MPQ the first word in a group is given the value 1, the second word the value 2, et cetera. Accordingly, each move to the next word in a MPQ group represents an increase in intensity of 1. In order to provide a measuring instrument using a graded ratio scale, the VAS was applied to obtain relative intensity values for Norwegian words. Several words within Nor- wegian pain groups have almost the same intensity scores. A future study should determine whether groups contain synonyms; if found, a further reduction in the total number of words contained in the questionnaire would be possible. However, if words within one group with similar intensities are not synonymous, they should be retained in the questionnaire to offer the users the possibility of finding words which exactly describe their pain. The large number of words in the Norwegian pain questionnaire may, however, affect its feasibility for clinical use.
A comparison between the MPQ and the Norwegian pain questionnaire shows that there are 78 pain de- scriptors in the MPQ. The words are allocated in 20 groups: 13 sensory, 5 affective, 1 evaluative and 1 miscellaneous. The Norwegian pain questionnaire con- sists of 106 pain descriptors allocated in 18 groups: 12 sensory, 5 affective and 1 evaluative. Table I shows the Norwegian pain words contained in groups and sub- groups.
It is recommended that patients should be free to choose as many descriptors from each group as neces- sary to give a proper description of their pain. Seventy- two patients chose more than 1 word in 30% of the groups scored to describe the actual quality of their pain. However, in 89% of the groups scored, patients either chose a single word or underlined a word. A key descriptor is thus likely to be derived for each scored group. Accordingly, the same scoring system can be used for both the MPQ and the Norwegian pain ques- tionnaire.
The present study has hopefully provided a useful multidimensional measuring instrument for pain in the Norwegian language. However, the actual value of the Norwegian pain questionnaire as a measuring instru- ment of pain has not yet been documented. Further studies are necessary to investigate the reliability, valid- ity, sensitivity and feasibility of this tool in order to determine if it is in fact useful for clinical and research purposes.

hh
Acknowledgements 13
We wish to thank Prof. Dr. Nancy Watts for her help with the study, Assist. Prof. Dr. Raymond Ma- ciewicz for his advice and participation, and lecturer Tom Backer Johnson for his help with the statistical analysis. We would also like to thank the physiothera- pists, students, patients and other participants for their time and effort.
The study was supported by grants from the College of Physiotherapy, Bergen, Norway, and from the Nor- wegian Physiotherapy Educational Foundation.
References
I
2
3
4
5 h
7
8
Y
IO
11
I2
Bartko. D.. Kondas, M. and Jancso, S.. Quantification of pain in
neurology. Slovak version of the McGill-Melzack’s Question-
naire on Pain, desk. Neural. Neurochir.. 47 (1984) 113-121.
Bond. M.R., The measurement of pain. In: M.R. Bond (Ed.).
Pain. Its Nature. Analysis and Treatment, Churchill Livingstone.
Edinburgh, 1979, pp. 26-34.
Boureau. F.. Luu, M.. Doubr&re. J.F. and Gay. C‘., Elaboration
d‘un questionnaire d’auto&aluation de la douleur par liste de
qualicatifs, Th&apie. 39 (1984) 119-129.
Crockett. D.J.. Prkachin. K.M. and Craig, K., Factors of the
language of pain in patient and volunteer groups. Pain, 4 (1977)
175-1X2.
Dillcr. I\.. Cross-cultural pain semantics, Pain, Y (19X(I) Y-26.
Dubuihson. D. and Melzack, R., Classification of clinical pain
descriptions by multiple group discriminant analysis, Exp. Neurol..
51 (1976) 4X0-487.
Graham. C.. Bond, S.S.. Gerkovich, M.M. and Cook. M.R.. Use
of the McGill Pain Questionnaire in the assessment o! cancer
pain: replicability and consistency, Pain. X (1980) 377-3X7.
Grushka, M. and Sessle, B.J.. Applicability of the McGill Pain
Questionnaire to differentiation of ‘toothache‘ pain, Pain. 1Y
(1983) 4Y-57.
Iluskisson, E.C.. Visual analoyue scales. In: R. Melzack (Ed.).
Pain Measurement and Assessment. Raven Pres<. New York,
19X3, pp. 33-37.
Jettc. A.M.. Concepts of health and methodological issues in
functional Assessment. In: C.V. Grangcr and G.E. Gresham
(Eds.). Functional Assessment in Rehabilitation Medicine,
Williams and Wilkins, Baltimore, MD. 1984.
Ketovuori. II. and Pgntinen. P.J., A pain vocabulary in Finnish
--- the Finnish Pain Questionnaire, Pain. 11 (1981) 237-75.3.
Klepac, R.K.. Dowling, J. and Hauge. G.. Sensitivity of the
McGill Pain Questionnaire to intensity and quality of laboratory
pain. Pain. 10 (1981) lYY-207.
I4
IS
I h
17
IX
I 0
70
‘I
‘2
73
73
75
26
‘7
7X
3
30
31
37
Kremer. E. and Hampton Atkinson, J.. Pain mcasurcment: i~)~,
\truct validity ot the a ffectivc dimension of the Mc(iill Pain
Ouestlonnairr with chronic benign pain pa~ienl\. Pain. I 1 c I%iI I 07.. 100.
Ljunggreli. A.E.. Dcscription5 ol pain and other sensory modali-
tics in palien& with lumbago-sciatica and hernlatecl intervertebral
discs. Inten’& adtnmi\tration ol an adapted McGill Pain Que\-
tionnaire. Pain. 16 (1983) 36276.
Ljunggren. A.E.. Jucob\cn. 7. ,~nd Osvih. r\.. l’,lin de\crlption\
,~nd surgical finding5 in patients with herniatecl lumbar intctvel tc-
bra1 d&c\. Pain, ii ( IS-%) 3%40. Lord, F. and Novik. hl.. Statistical Theor& (It Mental ‘I‘c\t
Scorch. Addison-We\lq. Reading. MA. IYhX, Ch. 1.
Magnusson. D.. Testteori. Almquiat and Wiksell. Stockholm, IY)hl.
Maiani. G. and Sanavio. I.. Scmanticj of pain in Italy: the Italian
version (11 the McGill Pain Quc\tionnaire. Pain. 23 C IWi.Z;) 390 -10.7. McGuire. D.B.. Assessment ot pain in cancer Inpatients using the
McGill Pain Qur$tlonnairc, Oncol. Nurs. Forum. I I (19X-l) 32-37.
Mclzack, R.. The McGill Pain Que6)nnaire: lmaior propcrtie<
and scoring methods. Pain. I ( 1075) 177-29’).
MelLack. R.. <‘oncept\ 01 pain mca\urement. In: R. MelLack
(Ild.). Pain Measurement and ,\\se$hment. R;t\cn Pres\. New
\‘ork. lYX3, pp. I 5. Melzack, R. and Torgcrcon. W.S.. On the language ol pain.
Anesthesiology. 34 (1Y7 I) 50-50.
Mclzack, R. and Wall. P.D.. The Challenge of Pain, Penguin
Books, London, I YR7.
Michel. T.H.. Introduction and atate of the at-t. In: T tIosklns
Michel (Ed.), Pain. Churchill Livingstone, Ncu York. IYXS, pp.
3 -17.
Philips, <‘.. Chronic headache experience. In: R. Melzack (Ed.).
Pain Measurement and Ahqessment. Raven Prc\a. N~M York.
IYXi. pp. Y7- 103.
Radvila. A.. Adler, R.tI.. Galeazzi. R.L. and Vorkauf. II., The
dc\elopmrnt ol a German language (Berne) pain questionnaire
and its application in it situation causing acute pain. Pain. 3X
(1Y87) IX5-lY5.
Reading. A.E.. The internal structure of the McGill Pain Vuea-
tionnaire in dysmenorrhoea patients, Pain, 7 (lY7Y) 353-35X.
Reading, A.E.. ,\ comparison of the McGill Pain Questionnaire
in chronic and acute pain. Pain. I3 (1982) IXS-lYl.
Scudds. R.A.. Pain assessment. Aust. J. Physiother.. 2Y (IYX.3)
Yh IOI.
Tul-k, D.C‘.. Rudy. T.E. and Salovey. P.. The McGill Pain Qucx-
ticmnaire reconsidered: confirming the factor \tructurc and exam-
ining appropriate uses. Pain. 71 (IYX5) 3X5-347.
Van Buren. J. and Kleinknecht. R.A., An evaluation ol the
McGill Pain Questionnaire for use in dental pain asse\smcnt.
Pain. h (lY7Y) Z-33.
Zhoromski. M.. People in Pain. Jossey-Bass. San Francisco. <‘A.
I ‘W.