the contact lens industry: structure, competition, and
TRANSCRIPT
The Contact Lens Industry: Structure,Competition, and Public Policy
December 1984
NTIS order #PB85-204451
LIBRARYOF TECHNOLOGY ASSESSMENT
HEALTH TECHNOLOGY CASE STUDY 31
The Contact Lens IndustryStructure, Competition, and
Public Policy
This case study was
Federal Policies
DECEMBER 1984
performed
and the
as part of OTA’s Assessment of
Medical Devices Industry
Prepared for OTA by:Leonard G. Schifrin, Ph.D.
Department of Economics, College of William and Mary, Williamsburg, VAand
Department of Preventive Medicine, Medical College of VirginiaVirginia Commonwealth University, Richmond, VA
with
William J. Rich, A.B.Department of Economics, College of William and Mary, Williamsburg, VA
OTA Case Studies are documents containing information on a specific medical tech-nology or area of application that supplements formal OTA assessments. The materialis not normally of as immediate policy interest as that in an OTA Report, nor doesit present options for Congress to consider.
Recommended Citation:Schifrin, Leonard G., with Rich, William J., The Contact Lens Industry: Structure, Com-petition, and Public Policy (Health Technology Case Study 31), OTA-HCS-31, Washington,DC: U.S. Congress, Office of Technology Assessment, November 1984. This case studywas performed as part of OTA’s assessment of Federal Policies and the Medical DevicesIndustry.
Library of Congress Catalog Card Number 84-601157
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402

Preface
The Contact Lens Industry: Structure, Com-petition, and Public Policy is Case Study 31 inOTA’s Health Technology Case Study Series. Thiscase study has been prepared in connection withOTA’s project on Federal Policies and the MedicalDevices Industry, which was requested by theSenate Committee on Labor and Human Resourcesand endorsed by the Senate Committee on Veter-ans’ Affairs. A listing of other case studies in theseries is included at the end of this preface.
OTA case studies are designed to fulfill twofunctions. The primary purpose is to provideOTA with specific information that can be usedin forming general conclusions regarding broaderpolicy issues. The first 19 cases in the Health Tech-nology Case Study Series, for example, were con-ducted in conjunction with OTA’s overall projecton The Implications of Cost-Effectiveness Anal-ysis of Medical Technology. By examining the 19cases as a group and looking for common prob-ems or strengths in the techniques of cost-effec-tiveness or cost-benefit analysis, OTA was ableto better analyze the potential contribution thathose techniques might make to the managementof medical technology and health care costs andquality.
The second function of the case studies is toprovide useful information on the specific tech-nologies covered. The design and the funding lev-els of most of the case studies are such that theyshould be read primarily in the context of the as-sociated overall OTA projects. Nevertheless, inmany instances, the case studies do represent ex-pensive reviews of the literature on the efficacy,safety, and costs of the specific technologies ands such can stand on their own as a useful contri-bution to the field.
Case studies are prepared in some instances be-cause they have been specifically requested byCongressional committees and in others becausethey have been selected through an extensive re-view process involving OTA staff and consulta-tions with the congressional staffs, advisory panel the associated overall project, the Health Pro-gram Advisory Committee, and other experts invarious fields. Selection criteria were developedto ensure that case studies provide the following:
● examples of types of technologies by func-
●
●
●
●
●
●
●
tion (preventive, diagnostic, therapeutic, andrehabilitative);examples of types of technologies by physicalnature (drugs, devices, and procedures);examples of technologies in different stagesof development and diffusion (new, emerg-ing, and established);examples from different areas of medicine(e.g., general medical practice, pediatrics,radiology, and surgery);examples addressing medical problems thatare important because of their high frequen-cy or significant impacts (e.g., cost);examples of technologies with associated highcosts either because of high volume (for low-cost technologies) or high individual costs;examples that could provide information ma-terial relating to the broader policy and meth-odological issues being examined in theparticular overall project; andexamples with sufficient scientific literature.
Case studies are either prepared by OTA staff,commissioned by OTA and performed under con-tract by experts (generally in academia), or writ-ten by OTA staff on the basis of contractors’papers.
OTA subjects each case study to an extensivereview process. Initial drafts of cases are reviewedby OTA staff and by members of the advisorypanel to the associated project. For commissionedcases, comments are provided to authors, alongwith OTA’s suggestions for revisions. Subsequentdrafts are sent by OTA to numerous experts forreview and comment. Each case is seen by at least30 reviewers, and sometimes by 80 or more out-side reviewers. These individuals may be fromrelevant Government agencies, professional so-cieties, consumer and public interest groups, med-ical practice, and academic medicine. Academi-cians such as economists, sociologists, decisionanalysts, biologists, and so forth, as appropriate,also review the cases.
Although cases are not statements of officialOTA position, the review process is designed tosatisfy OTA’s concern with each case study’sscientific quality and objectivity. During the vari-ous stages of the review and revision process,therefore, OTA encourages, and to the extentpossible requires, authors to present balanced in-formation and recognize divergent points of view.
,..111

—
Health Technology Case Study Seriesa
Case Study Case study title; author(s); Case Study Case study title; author(s);Series No. OTA publication numberb Series No. OTA publication numberb
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
Formal Analysis, Policy Formulation, and End-Stage RenalDisease;
Richard A. Rettig (OTA-BP-H-9(1))C
The Feasibility of Economic Evaluation of Diagnostic Pro-cedures: The Case of CT Scanning;
Judith L, Wagner (OTA-BP-H-9(2))Screening for Colon Cancer: A Technology Assessment;
David M. Eddy (OTA-BP-H-9(3))Cost Effectiveness of Automated Multichannel ChemistryAnalyzers;
Milton C. Weinstein and Laurie A. Pearlman(OTA-BP-H-9(4))
Periodontal Disease: Assessing the Effectiveness and Costs ofthe Keyes Technique;
Richard M. Scheffler and Sheldon Rovin(OTA-BP-H-9(5))
The Cost Effectiveness of Bone Marrow Transplant Therapyand Its Policy Implications;
Stuart O. Schweitzer and C. C. Scalzi (OTA-BP-H-9(6))Allocating Costs and Benefits in Disease Prevention Programs:An Application to Cervical Cancer Screening;
Bryan R. Luce (Office of Technology Assessment)(OTA-BP-H-9(7))
The Cost Effectiveness of Upper Gastrointestinal Endoscopy;Jonathan A. Showstack and Steven A. Schroeder(OTA-BP-H-9(8))
The Artificial Heart: Cost, Risks, and Benefits;Deborah P. Lubeck and John P. Bunker(OTA-BP-H-9(9))
The Costs and Effectiveness of Neonatal Intensive Care;Peter Budetti, Peggy McManus, Nancy Barrand, andLu Ann Heinen (OTA-BP-H-9(10))
Benefit and Cost Analysis of Medical Interventions: The Caseof Cimetidine and Peptic Ulcer Disease;
Harvey V. Fineberg and Laurie A. Pearlman(OTA-BP-H-9(11))
Assessing Selected Respiratory Therapy Modalities: Trends andRelative Costs in the Washington, D.C. Area;
Richard M. Scheffler and Morgan Delaney(OTA-BP-H-9(12))
Cardiac Radionuclide Imaging and Cost Effectiveness;William B. Stason and Eric Fortess (OTA-BP-H-9(13))
Cost Benefit/Cost Effectiveness of Medical Technologies: ACase Study of Orthopedic Joint Implants;
Judith D. Bentkover and Philip G. Drew (OTA-BP-H-9(14))Elective Hysterectomy: Costs, Risks, and Benefits;
Carol Korenbrot, Ann B. Flood, Michael Higgins,Noralou Roos, and John P. Bunker (OTA-BP-H-9(15))
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
The Costs and Effectiveness of Nurse Practitioners;Lauren LeRoy and Sharon Solkowitz (OTA-BP-H-9(16))
Surgery for Breast Cancer;Karen Schachter Weingrod and Duncan Neuhauser(OTA-BP-H-9(17))
The Efficacy and Cost Effectiveness of Psychotherapy;Leonard Saxe (Office of Technology Assessment)(OTA-BP-H-9(18))d
Assessment of Four Common X-Ray Procedures;Judith L. Wagner (OTA-BP-H-9(19))e
Mandatory Passive Restraint Systems in Automobiles: Issuesand Evidence;
Kenneth E. Warner (OTA-BP-H-15(20))f
Selected Telecommunications Devices for Hearing-ImpairedPersons;
Virginia W. Stern and Martha Ross Redden(OTA-BP-H-16(21))g
The Effectiveness and Costs of Alcoholism Treatment;Leonard Saxe, Denise Dougherty, Katharine Esty,and Michelle Fine (OTA-HCS-22)
The Safety, Efficacy, and Cost Effectiveness of TherapeuticApheresis;
John C. Langenbrunner (Office of Technology Assessment
(OTA-HCS-23)Variation in Length of Hospital Stay: Their Relationship toHealth Outcomes;
Mark R. Chassin (OTA-HCS-24)Technology and Learning Disabilities;
Candis Cousins and Leonard Duhl (OTA-HCS-25)Assistive Devices for Severe Speech Impairments;
Judith Randal (Office of Technology Assessment)(OTA-HCS-26)
Nuclear Magnetic Resonance Imaging Technology: A ClinicalIndustrial, and Policy Analysis;
Earl P. Steinberg and Alan Cohen (OTA-HCS-27)Intensive Care Units (ICUs): Clinical Outcomes, Costs, anDecisionmaking;
Robert A. Berenson (OTA-HCS-28)The Boston Elbow;
Sandra J. Tanenbaum (OTA-HCS-29)The Market for Wheelchairs: Innovations and Federal Policy
Donald S. Shepard and Sarita L. Karen (OTA-HCS-30The Contact Lens Industry: Structure, Competition, and PublicPolicy
Leonard G. Schifrin with William J. Rich (OTA-HCS-3)
aAvailable for sale by the Superintendent of Documents, U.S. Government dBackground paper #3 to The Implications of Cost-Effectiveness AnalysisPrinting Office, Washington, DC, 20402, and by the National Technical Medical Technology.Information Service, 5285 Port Royal Rd., Springfield, VA, 22161. Call eBackground Paper #5 to The Implications of Cost-Effectiveness AnalysisOTA’s Publishing Office (224-8996) for availability and ordering infor- Medical Technology.
fBackground paper #1 to OTA’s May 1982 report Technology and Hanmation.bOriginal publication numbers appear in parentheses. capped People.cThe first 17 cases in the series were 17 separately issued cases in Background gBackground Paper #2 to Technology and Handicapped People.Paper #2: Case Studies of Medical Technologies, prepared in conjunctionwith OTA’s August 1980 report The Implications of Cost-Effectiveness Anal-ysis of Medical Technology.

OTA Project Staff for Case Study #31
Roger Herdman, Assistant Director, OTAHealth and Life Sciences Division
Clyde J. Behney, Health Program Manager
Jane E. Sisk, Project Director
Lawrence H. Miike, Senior Associate
Katherine E. Locke, Research Assistant
H. Christy Bergemann, Editor
Virginia Cwalina, Administrative Assistant
Rebecca I. Erickson, Secretary/Word Processor Specialist
Brenda Miller, Word Processor/P. C. Specialist
.-
Advisory Panel for Federal Policies andthe Medical Devices Industry
Richard R. Nelson, ChairInstitute for Social and Policy Studies, Yale University
New Haven, CT
William F. BallhausInternational Numatics, Inc.Beverly Hills, CA
Ruth FarriseyMassachusetts General HospitalBoston, MA
Peter Barton HuttCovington & BurlingWashington, DC
Alan R. KahnConsultantCincinnati, OH
Grace KraftKidney Foundation of the Upper MidwestCannon Falls, MN
Joyce LashofSchool of Public HealthUniversity of CaliforniaBerkeley, CA
Penn LupovichGroup Health AssociationWashington, DC
Victor McCoyParalyzed Veterans of AmericaWashington, DC
Robert M. MoliterMedical Systems DivisionGeneral Electric Co.Washington, DC
Louise B. RussellThe Brookings InstitutionWashington, DC
Earl J. SaltzgiverForemost Contact Lens Service, Inc.Salt Lake City, UT
Rosemary StevensDepartment of History and Sociology of ScienceUniversity of PennsylvaniaPhiladelphia, PA
Allan R. ThiemeAmigo Sales, Inc.Albuquerque, NM
Eric von HippelSloan SchoolMassachusetts Institute of TechnologyCambridge, MA
Edwin C. WhiteheadTechnicon Corp.Tarrytown, NY
Contents
PageCHAPTER 1: SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
CHAPTER 2: THE DEVELOPMENT OF CONTACT LENSES . . . . . . . . . . . . . . . . . . . . 9
CHAPTER 3: TYPES OF CONTACT LENSES AND THEIR CHARACTERISTICS . . 15Hard PMMA Lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Soft Lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Gas-Permeable Lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Present Usage and Future Trends... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
CHAPTER 4: WEARERS, PRICES, AND SOURCES OF PAYMENT . . . . . . . . . . . . . . 23Wearers of Contact Lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Prices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Sources of Payment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
CHAPTER 5: PRODUCERS OF CONTACT LENSES.. . . . . . . . . . . . . . . . . . . . . . . . . . . 31
CHAPTER 6: CONTACT LENS PRESCRIBERS AND DISPENSERS. . . . . . . . . . . . . . . 39Ophthalmologists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Optometrists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Opticianry: Independent Optical Outlets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Opticianry: Optical and Drug Chains . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41The Marketing of Contact Lenses to Dispensers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
CHAPTER 7: THE ROLE OF FEDERAL POLICY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47General Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Patents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47The Maintenance of Market Competition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
Mergers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48State Commercial Practice Restraints. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
FDA Regulatory Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51The Origins, Development, and Scope of FDA Authority Over Contact Lenses . . . 51The Effects of the Present System of Regulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
APPENDIX A.– FDA APPROVED CONTACT LENSES AND CURRENT PRICES.. 57
APPENDIX B.– MAJOR CONTACT LENS MANUFACTURERS, METHODS OFENTRY, AND ACQUISITIONS AND LICENSE AGREEMENTS . . . . . . . . . . . . . . . . 59
APPENDIX C.– GLOSSARY OF TERMS AND ACRONYMS . . . . . . . . . . . . . . . . . . . . 62
APPENDIX D.– ACKNOWLEDGMENTS AND HEALTH PROGRAMADVISORY COMMITTEE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
Tables
Table No. Pagel. Summary of the Historical Development of Contact Lenses . . . . . . . . . . . . . . . . . . . 92. Persons Wearing Corrective Lenses: 1966, 1971, and 1977. . . . . . . . . . . . . . . . . . . . . 173. Persons Wearing Corrective Lenses: 1970, 1975, 1978-82 . . . . . . . . . . . . . . . . . . . . . . 184. Share of U.S. Contact Lens Market by Lens Type, 1978-87. . . . . . . . . . . . . . . . . . . . 18
vii
—————
Contents—continuedTable No. Page5.
6.
7.
8.9.
10.
11.
12.13.14.15.16.17.
Contact Lens Wearers, Percent of Population, by Sex and Age,1965-66, 1971, and 1979-80. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Purchase or Repair of Contact Lenses per 1,000 Population at DifferentFamily Income Levels, 1977 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Average Soft Contact Lens List and Total Fitting Prices, per Pair, 1971-82,Selected Years . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Market Shares and Concentration Ratios, Soft Lenses, 1978-82 . . . . . . . . . . . . . . . . 31Market Shares and Concentration Ratios, Gas-Permeable Lenses, 1979-82 . . . . . . . 31Worldwide Sales, Profit, and R&D Data of the 17 Major Firms in theContact Lens Industry, 1982 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33U.S. Product Lines and List Prices Per Lens for the 15 Major Contact LensManufacturers, May 1983 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Contact Lens Fittingly Ophthalmologists, 1982 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Contact Lens Fitting by Optometrists, 1982 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Contact Lens Fitting by Independent Dispensing Opticians, 1982 .........,., . . . 41Contact Lens Fitting by Chain Outlets, 1982. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Major Optical Chains and Number of Outlets, 1982 . . . . . . . . . . . . . . . . . . . . . . . . . . 42Contact Lens Fitting by Opticians: Survey of State Limitations . . . . . . . . . . . . . . . . 49
. . .Viii
OTA Note
These case studies are authored works commissioned by OTA. Each authoris responsible for the conclusions of specific case studies. These cases are not state-ments of official OTA position. OTA does not make recommendations or endorseparticular technologies. During the various stages of review and revision, therefore,OTA encouraged the authors to present balanced information and to recognizedivergent points of view.
25-339 0 - 84 - 2 : QL 3

1
Summary
This study presents an analysis of the contactlens industry in the United States, emphasizingthe role of economics and public policy in shap-ing past and future development. The analysis fol-lows the general format usually employed in suchindustry studies: 1) the evolution and present con-figuration of the structural and institutional fea-tures, including public policy, that define the con-tact lens industry; 2) the corporate strategies andpolicies conditioned by this operational context;and 3) the end results of these strategies and pol-icies in terms of the technical improvement of con-tact lenses, the ways of making them, and theprices at which they are sold.
In following this general format, the study isboth descriptive and analytical. The descriptiveaspects include the historical evolution of contactlenses (ch. 2); the range of available lens types(ch. 3); the characteristics of wearers of contactlenses, how much they spend, and the sources ofpayment for these contact lenses expenditures (ch.4); the firms that make contact lenses (ch. 5); theeye-care professionals who represent the bridgebetween makers and users by prescribing and fit-ting contact lenses, and toward whom lens man-ufacturers direct most of their marketing efforts(ch. 6); and the regulatory context within whichthe entire manufacturing and selection processtakes place (ch. 7).
The first part of the analysis relates structureto behavior, or the influence that the number, size,market power, and policies of the makers of con-tact lenses have on their incentives and behaviorregarding competition in product developmentand price.
The second part of the analysis focuses on therole played by public policy in influencing thiscompetition, either directly or indirectly. Themore important elements of public policy affect:1) mergers, 2) market entry, 3) competition in theprofessional prescribing and fitting of contactlenses, and 4) the payment mechanism in the pur-chasing process.
Why is it important to know these features ofthe contact lens industry and how public policyaffects the industry’s operation, when the indus-try is quite small, with annual domestic sales atthe manufacturers’ level currently running about$350 million? First, the analysis of any industry,however small, provides another economic casestudy that adds to our knowledge of how indus-try structure and public policy affect the competi-tive behavior of firms in the marketplace. Second,the contact lens industry gives every indicationof growing considerably in the relatively nearfuture; thus, its record in product improvementand pricing will be increasingly important rela-tive to the full range of goods and services pro-duced in the economy. Third, the study of the ef-fects of public policy regarding the contact lensindustry can provide guidelines for the formula-tion of sound policies in the future toward thisindustry, and, in turn, by serving as a case study,for the formulation of effective policies to influ-ence the activities and performance results of otherindustries, both inside and outside the medicalsector.
Contact lenses are of three types, although thedistinctions between the types could conceivablydisappear in the future. The first type of moderncontact lens was the hard “PMMA” (for “poly-methylmethacrylate”) lens, made of plexiglass-type plastics. The advantages of this type are rela-tive rigidity (where flexing may be a problem),smallness, lightness, safety (minimal risk to theeyes), ease of precision-machining, ease of main-tenance, and durability. Their major disadvan-tage is that they are impermeable to oxygen andinterfere with the flow of oxygen to the cornea.For a sizable proportion of potential wearers, thisproblem may actually deter the wearing of PMMAlenses; for others, wearing time becomes limitedto a usual daily maximum of 8 to 16 hours.PMMA lens wearers may also incur “spectacleblur” when switching from lenses to glasses.
The second type of contact lens is made fromwater-absorbing plastics caIled “hydrogels” (mostly
3

4 ● Health case study 31: The Contact Lens Industry : Structure, competition, and Public Policy
“HEMA’’-for “hydroxyethylmethacrylate’’—hy-drogels, but other hydrogel materials are alsopopular) or soft silicone. Their water absorbencyand resulting softness make them considerablymore easy to adapt to and more comfortable forlonger periods, but the same characteristics makethem fragile, provide less acute vision correction,and may increase the likelihood of eye infectionsfrom handling and wearing.
The third type of lenses is gas permeable. Theselenses have much of the superior optical and ease-of-care qualities of hard lenses because of theirrigidity, and the comfort of soft lenses becausethey are oxygen permeable.
About 120 million people in the United Stateswear corrective eyeglasses and another 16 millionto 18 million use contact lenses, either exclusivelyor interchangeably with eyeglasses. Among allU.S. contact lens wearers, the use of hard lensesis declining and the use of soft and gas permeablelenses is increasing. For new fittings, hard lensesrepresent a minor share, soft lenses predominate,and gas permeable are the fastest growing. Forboth new fittings and replacements together, softlenses represent upwards of 75 percent of the totalmarket, probably their peak figure. Hard lenseshave 15 percent or less of the market, and gaspermeable at least 10 percent.
In the future, soft and gas-permeable lenses willaccount for almost all lens sales, perhaps aboutequally. There are some signs that a hybrid typeof lens, combining the best qualities of each type,may be emerging. If so, then this fourth type willbe “the” contact lens of the future. Whether ornot this hybrid is developed, contact lenses maybecome as common or even more common amethod of vision correction than eyeglasses, astheir comfort, wearability, applications, and ef-fectiveness continue to increase.
At present, contact lenses are particularly usefulin the correction of single vision problems, essen-tially myopia (nearsightedness) and hypermetropia(farsightedness). They are also useful in the cor-rection of astigmatism (a vision defect usuallyresulting from an irregular, nonsymmetrical con-formation of the cornea, which results in a lackof sharpness or evenness of focus) and presbyopia(the loss of flexibility in refocusing from near to
far objects, and vice versa) for which bifocal ormultifocal corrective lenses or monovision cor-rection is employed. These “disorders of refrac-tion and accommodation” rank very high amongphysical problems, as evidenced by patient visitsto all eye-care professional practitioners.
Certain interesting features exist in the patternof contact lens wearers. Unlike eyeglasses, con-tact lenses have been a “younger person’s” prod-uct. The traditional wearer has been the youngadult female. However, as the therapeutic applica-tions of contact lenses expand and consumer tastesare altered (partly by increased direct advertis-ing by manufacturers), contact lens usage amongmales and among older persons is increasingrapidly and the traditional orientation toward theyoung adult female is disappearing.
The absolute price of contact lenses of all typeshas fallen significantly in the past decade, a timeof high general inflation. Soft lens wholesale pricesnow are about half their mid-1970s level, and totalfitting prices are half or less of their early 1970slevel. Lens price reductions have resulted fromlarge-scale entry, excess capacity, and vigorousprice competition among manufacturers, particu-larly in the soft lens group. Total-fitting price re-ductions reflect these cuts in lens prices and theexpanded competition among lens fitters, particu-larly the large chain optical houses. Continuedprice competition is likely, and further price de-clines, if less dramatic, may occur in the future.
Unlike many categories of health care expend-itures, the largest proportion of payments for cor-rective lenses comes from patients, rather thanfrom private or public insurance. Although anumber of major collectively bargained employ-ment contracts provide vision-care benefits, suchcoverage applies only to a small proportion of allworkers, provides mainly for eyeglasses, and pro-vides only partial payment for contact lenseswhen they are covered. In the public sector, con-tact lenses are insured only for therapeutic, notcosmetic, use. (In a strict sense, all contact lensesthat offer vision correction or eye protection are“therapeutic” in use. However, contact lenses thatprovide correction or protection not achievablethrough the use of eyeglasses are commonly con-sidered “therapeutic” in use while those afford-

Ch. I—Summary ● 5
ing benefits also attainable through the wearingof eyeglasses are considered “cosmetic,” since, itis believed, the choice of contact lenses in the lattercases is made on the basis of appearance con-siderations. ) In practice, this means that contactlenses are provided under Medicare, Medicaid,and other public programs mainly in relation tocataract or other eye surgery. As a result of thisminimal role of third-party payment in the totalsource-of-payment pattern, insurance as a wholeand public programs in particular have little dis-cernible effect on contact lens usage, development,prices, or resource allocation patterns.
Although a large number of firms produce con-tact lenses, the manufacture of both soft and gaspermeable lenses is concentrated among a veryfew large firms. However, because of many fac-tors—e.g., the similarity of lenses within eachtype, the considerable substitutability and re-sulting competition among types, and excesscapacity—competition is active in both productdevelopment and price. Where market power ismost evenly distributed (hard lenses), price com-petition is greatest. Where large firms dominatebut are surrounded by a fringe of smaller firms(soft lenses), price competition is high. Where onlya few firms are in the market and one predomi-nates (gas permeable lenses), price competition,among groups if not within this group, is at leastobservable.
Yet public policy has not had benign effects onmarket competition. As a result, the degree ofcompetition is probably less than it otherwisewould be, and the gap between the actual and po-tential levels may widen in the future. To thepresent, the history of this industry shows theimportant role of small firms as generators of in-novational progress, service, and price rivalry.Yet the sector most open to small firms—hardroses - is becoming less important as time passes.n the soft-lens area, energetic small firms haveDifficulty entering the market, and mergers andacquisitions by large firms may eliminate manyof them. And small firms have the greatest diffi-culty in entering the fastest growing marketarea —gas-permeable lenses. The greatest poten-tial obstacle to the attainment of optimal prod-uct and price competition in the future is the U.S.Food and Drug Administration’s premarketing
approval policies, which have been especiallyburdensome to smaller firms. Restrictive marketapproval policies may be wise for significantlynew lens types, but once their effectiveness andsafety become established, more flexible approachestoward minor or closely similar new develop-ments seem warranted.
The study also examines the role of contact lensprescribers and dispensers (ophthalmologists, op-tometrists, and opticians) in the eye-care field.Ophthalmologists are medical doctors specializ-ing in eye care, and vision correction is a largepart of their activity. There are about 12,500ophthalmologists in the United States, of whom11,000 are involved in regular patient care. Op-tometrists, who are licensed to measure and fitcorrective lenses, outnumber ophthalmologists byroughly two-to-one, and fit proportionally morecorrective lenses. Opticians are usually limited tomaking contact lenses or to fitting them under thesupervision of an optometrist or ophthalmologist,but in some States they may measure for and fitcorrective lenses. There are an estimated 26,000dispensing opticians. Recent action by the U.S.Federal Trade Commission (FTC), however, hasexpanded the competitive roles of these dispens-ing opticians. The FTC requires all lens prescribersto provide copies of the prescription to the pa-tient, Thus, patients may take these prescriptionselsewhere, including to opticianries, for filling andfitting. State prohibitions against price competi-tion by corrective lens dispensers are also nolonger enforceable, and opticians have begun tocompete on the basis of price to fill corrective lensprescriptions written by others. Large chains, withinhouse optometrists and opticians, have been themost vigorously price competitive, both for fullprescribing and fitting, and for filling prescriptionsbrought in by patients. Accordingly, public pol-icy has been successful in providing strong com-petition in the fitting of contact lenses, which isdirectly advantageous to patients in the forms ofexpanded choices and lower prices, and indirectlyadvantageous by exerting a strong counteractingforce on any market power among lens manufac-turers.
Other Federal policies—tax, import, researchfunding, procurement—seem to have little, if any,effect on the contact lens industry. Patent policy

Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
is somewhat more important, but not critically approval requirements could suggest adjustmentsso. More importantly, the procompetitive effects in policies that would make mergers somewhatof enhancing competition among dispensers could more difficult to accomplish and market entrybe maximized subject, of course, to the mainte- considerably easier. Adoption of more flexiblenance of high-quality care. An assessment of the policies of premarket approval merits particulareffects of unhindered mergers and premarketing attention.

2.The Development of Contact Lenses1
The oft-told history of the development of con-tact lenses is an interesting one, and its highlightsare presented in table 1. The history usually beginswith the theories of Leonardo da Vinci that awater-filled glass “half circle” could neutralize therefractive (light bending) power of the cornea andsubstitute the refractive power of the curved glassto improve the clarity of the image received bythe retina. Leonardo suggested at least two dem-onstrations of his theory: 1) a water-filled glassbowl in which the person placed his or her face(presumably for brief periods) and looked throughthe bottom, and 2) a water-filled glass hemisphereactually worn over the eye and remarkably likea contact lens. His ideas far exceeded the abilityof his times to actually implement them. How-ever, he had correctly identified several key prin-ciples of contact lenses; neutralizing the refrac-tion of the natural cornea by means of an artificialsurface; substituting the refractive powers of a
1Except as noted, this discussion was drawn from: Graham, 1981(15); Lowther, 1982 (21); and Ruben, 1976 (30).
curved, clear lens in its place; and positioning thatlens directly on the eye.
Almost a century and a half later, the philos-opher-mathematician René Descartes suggestedplacing a lens at the end of a water-filled tube,the other end of which was placed on the corneaof the eye. His concept was not really practicalas such tubes would require external support, buttime has shown that his idea of placing the lensonly over the cornea instead of including the sclera(white portion of the eye), as Leonardo had pro-posed, was most perceptive.
In 1801, Thomas Young, an English scientist,actually made a rudimentary set of contact lenseson the model of Descartes. Using wax, he affixedwater-filled lenses to his eyes, neutralizing his ownrefractive power, then corrected for it with anotherpair of lenses. His optic device affirmed the prin-ciples formulated by both Leonardo and Descartes.
Next in the progression of the science of con-tact lenses was Sir John Herschel, an English
Table 1 .—Summary of the Historical Development of Contact Lenses
Year Individual(s) Development
1508163618011827
188718881888
1936
1938194719471950
196019681971
Leonardo da Vinci . . . . . . .René Descartes . . . . . . . . .Thomas Young . . . . . . . . . .John Herschel . . . . . . . . . .
F. A. Muller. . . . . . . . . . . . .A. E. Fick . . . . . . . . . . . . . .E. Kalt . . . . . . . . . . . . . . . . .
W. Feinbloom . . . . . . . . . . .
Mullen and Obrig . . . . . . . .N. Bier . . . . . . . . . . . . . . . . .K. Tuohy . . . . . . . . . . . . . . .Butterfield . . . . . . . . . . . . . .
Wichterle and Lim . . . . . . .
Bausch & Lomb . . . . . . . . .1970s J. DeCarle . . . . . . . . . . . . . .1970s Rynco Scientific . . . . . . . .1970s1978 Danker Laboratories . . . . .1979 Syntex Ophthalmic . . . . .
Described glass contact lensTube of water used to neutralize the corneaUsed Descartes’ principle to study the eyeDescribed how a contact lens could be ground; concept
of molding the eyeFitted a glass blown lens for a patient to protect the eyeDescribed first glass lens to be worn to correct visionDesigned and fitted glass corneal lenses; Used
ophthalmometer to fit lensesMade lens with glass central optic and plastic surround
(first plastic used in contact lens)First all-plastic (PMMA) contact lensFenestrated minimum-clearance haptic lensAll-plastic corneal lensDesigned corneal lens to parallel the cornea; used
peripheral curvesHydrogel polymers for contact lensesU.S. FDA became involved in regulating contact lensesFirst hydrogel lens approved in United StatesExtended wear with high water content hydrogel lensesUse of CAB polymer for contact lensesFirst clinical marketing of soft silicone lensesU.S. FDA approval of CAB lensesU.S. FDA approval of a PMMA-silicone copolymer lens
SOURCE: G. E. Lowther, Contact Lenses: Procedures and Techniques (Boston, MA: Butterworths, 1982)
9

10 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
—
astronomer, who in the 1820s suggested principlesfor accurate lens grinding and fitting. His first con-tribution was to suggest grinding the inside cur-vature of a glass lens to conform as closely as pos-sible to an irregularly surfaced cornea, and theoutside curvature of the same lens to duplicatea normal cornea. He also proposed taking an ac-tual mold of the eye to use in rendering an ac-curate interior curvature fit and using a gel-likefilling for the cavity between the cornea and in-terior curve.
The actual making of contact lenses becamepossible as the necessary technological capabil-ities slowly emerged. The development of anes-thesia in 1884 allowed for making a mold of theshape of the eye, as proposed by Herschel. Ad-vances in optics, particularly precision glass blow-ing and lens grinding, made possible the accurateduplication in glass of the curvatures of the eye.Usable lenses thus were developed, but their firstapplications were for pathological conditions ofthe eye (as opposed to correcting a refraction er-ror), since only the correction of severe problemsjustified the wearing of these large, heavy, anduncomfortable devices, which were tolerable onlyfor brief periods. In Germany, F. A. Muller, amaker of artificial glass eyes, made a transparentlens in 1887 to protect a diseased eye that seemsto have worked for many years.
The following year, two important develop-ments occurred. A. E. Fick, a Swiss physician,employed a small glass bowl—more accurately,a segment of a glass sphere “bounded by concen-tric and parallel sphere segments’’—to correctrefractive errors. These appear to be the first truecontact lenses, and Fick went on to design anduse both corneal and scleral lenses. Concomitantadvances in lens making, led by the Zeiss enter-prise in Germany, made Fick’s work possible andallowed for further experimentation with contactlenses in Germany, Switzerland, and France. Forthe most part, however, such lenses were notcomfortable enough for much use in other thanpathological conditions such as keratoconus,where the pressure of the lens might help suppressthe conical distention of the cornea and protectit; other severe distortions of the cornea in whichcorrection by the use of spectacles was not possi-
ble; and in cases where the cornea needed pro-tection from infections and encrustations of theeyelids.
By the end of the 19th century, then, a plateauhad been reached in the progress of contact lenses.Fairly well-fitting and carefully made glass con-tact lenses were available but were used on alimited scale only for occasional therapeutic pur-poses. Glass, even thin-blown or finely ground,is relatively heavy. Thus, small lenses would notadhere reliably to the surface of the eye, and largelenses which extended under the eyelids impededthe lubrication of the cornea and the flow of ox-ygen (and carbon dioxide) because they wereessentially impermeable. The results of wearingthese large, scleral lenses were: discomfort, irrita-tion, swelling, and perhaps infection or otherdamage; the need for continuous and usually notsuccessful artificial lubrication of the eye; and/ora cycle of short-term wearing and longer rest peri-ods. Additionally, wearing highly fragile lensesin the eye was considerably dangerous, and theglass material itself was affected by tears. Theregular use of contact lenses for simple vision cor-rection, although nearer to reality than before,was not yet feasible. The development of contactlenses thus remained static at this point, waitingfor supporting technology to catch up.
This catchup took another half-century and ap-peared in the form of plastics, which overcamesome of the more serious limitations of glasslenses. Feinbloom, in the United States, was thefirst to use plastic in contact lenses. In 1936, heproduced a scleral lens by bonding the glass cor-neal portion to an opaque, molded resin scleralband. Obrig and Mullen, also working in theUnited States, made the first all-plastic sclerallenses in 1938, using a new material, polymethyl-methacrylate (PMMA), which was particularlyeasy to shape to ultra-thin dimensions and greatlysuperior to glass in safety, lightness, and work-ability. The step from plastic scleral to plastic cor-neal lenses was a short but difficult and impor-tant one and was accomplished by Tuohy in 1947,and the modern era of contact lenses had begun.
Tuohy and others, including Butterfield, madegreat progress in both the construction and de-sign of corneal plastic contact lenses. The results

Ch. 2—The Development of Contact Lenses ● 11
were a small, light lens of high optical quality anda design that conformed very closely to the shapeof the central cornea, but with a slight “stand off”at the edges for better tear spreading for greaterlubrication and oxygen delivery to the cornea. Asa result, PMMA or “hard” corneal contact lensesfor correcting refractive errors became commer-cially practical in the early 1950s, and for the nexttwo decades, they were virtually the only typeof lenses used.
The search for new lens materials and designswas partly spurred by the wide range of correc-tive and therapeutic requirements that one mate-rial and a few design configurations were unlikelyto serve, but more so by the limitations of PMMAfor routine refractive corrections. A serious limita-tion of PMMA is that because it is nonpermeable,oxygen-bearing tears may not be able to diffusethrough the lens to reach the cornea in sufficientquantity. Without oxygen, the cornea swells andmakes lens-wearing difficult. For many people,natural blinking and movement of the lens allowfor an oxygen supply adequate for upwards of 16hours of wear, so-called “daily” wear. But formany others, shorter wearing times and higherlevels of discomfort can be expected, perhaps tothe point of their forgoing lenses totally, especiallysince many wearers of contact lenses choose themover glasses essentially for cosmetic reasons.
If PMMA lenses represent the first generationof modern contact lenses, “soft” lenses, designedlargely to overcome the limitations of hard PMMAlenses, represent the second generation. For themost part, soft lenses are made of hydrophilic(water-absorbing) plastic materials called “hydro-gels.” The basic hydrogel plastic is hydroxyethyl-methacrylate (HEMA), although new hydrogelmaterials and other soft-lens plastics have recentlybeen developed. These plastics absorb water (asmuch as 85 to 90 percent by weight) and becomesoft and flexible in proportion to their absorbency.In 1960, Wichterle and Lim, Czechoslovakianchemists working with Dreifus, an ophthalmolo-gist, researched hydrogels, and with Dreifus beganto formulate hydrophilic contact lenses.
Although hydrogels have become the main typeof contact lenses currently on the market, theywere not a practical alternative to hard lenses for
a decade or more after their invention. Being softand permeable, they were comfortable on the eye,but their water content made them difficult tohandle, of poor optical quality, and raised ques-tions about the absorption of infectious bacteria.However, within several years, improved mate-rials and lens designs were formulated. After afew years of experimentation and improvement,Wichterle granted to National Patent Develop-ment Corp. (NPD), a U.S. firm, exclusive West-ern Hemisphere rights to the new hydrogel ma-terials and to a novel molding process, now called“spin casting, “ for the fabrication of hydrogel con-tact lenses. NPD, in turn, licensed Bausch &Lomb Inc. to use these product and process pat-ents. In 1971, after considerable improvementand careful testing, Bausch & Lomb obtained ap-proval from the U.S. Food and Drug Adminis-tration to sell hydrogel lenses in the United States.After several years, other firms began to obtainsimilar approvals for their hydrogel lenses, andmany firms are now in the market.
Today, there are more than 30 manufacturersof soft lenses (31,48). For any given use, differentbrands of lenses may differ slightly in design andhydrophilic capacity, some higher for greatercomfort and permeability, others lower for greaterdurability and visual acuity. Soft lenses are nowavailable for a wide variety of vision problemsand for extended wear.
The decade of the 1970S thus marked the in-troduction, acceptance, and ultimate dominanceof soft lenses over the older PMMA hard lenses,but as the decade ended a new type of lens, per-haps a third generation, was introduced. This lensis a gas-permeable hard lens, made of eithercellulose acetate butyrate (CAB), PMMA-siliconecombinations, or pure silicone. These lenses allowoxygen to reach the cornea through the lens assoft lenses do, while also offering the opticalclarity and ease of handling of hard lenses. In1979, the first gas-permeable hard lenses were ap-proved for use in the United States, and recently,others have followed. Currently, in addition tothe wide range of soft lenses available or beingtested, experimentation with newer gas-permeablehard lenses, including extended wear lenses, isactive.

12 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
The history of the development of contactlenses is considerably more detailed and complexthan is suggested by a discussion of its significantdevelopments or a chronological listing of itshighlights. Today’s wide range of precision-made,carefully fitted, and extensively used contactlenses represents the contributions of a large num-ber of scientific areas and industrial sectors whichplayed key roles. These include: physics, biology,and chemistry and their continually expandingtheoretical and empirical foundations; precisionglassmaking, which made possible early lenses of
thin optical glass; the plastics industry, which hasdeveloped an expanded inventory of sophisticatedpolymer plastics that are the foundation of today’scontact lenses; the precision machine tool indus-try, which has provided ultra-fine grinding,lathing, and molding machines for lens finishing;the optical instruments industry, for its provisionof precise ophthalmic measurement and exami-nation technology and eye-care practitioners andtechnical personnel, who have utilized the newtechnologies and encouraged their continuedevolution.

3 ■
Types of Contact Lenses andTheir Characteristics1
The basic categories of contact lenses currentlyin use are the original hard (polymethylmethacry-late [PMMA]) lenses, soft hydrogels (hydro-xymethylmethacrylate [HEMA] and other mate-rials), and gas-permeable hard lenses (cellulose
HARD PMMA LENSES
As discussed in the previous chapter, hardPMMA lenses were the first lenses introducedonto the market, and corneal PMMA lenses simi-lar to those currently in use have been availablesince the early 1950s. Compared to later types oflenses, PMMA lenses can be difficult to adapt to,and perhaps as many as half of the people fitteddo not become long-term wearers. Since PMMAis not water- or gas-permeable, wearers must relyon the “tear pump” action of the eye to provideoxygen to the covered portion of the cornea. Asthe wearer blinks, tear interchange occurs fromoutside the lens to beneath it, providing the nec-essary oxygen. Although hard lenses are verysmall and cover only a portion of the cornea,many persons may not be able to provide enoughtears for comfortable wear. Others may “get by”for 8 to 12 hours but beyond that time, they suf-fer from dryness, swelling, and discomfort of theeye. Thus, hard lenses are, at best, “daily” wearlenses, but for many people they are very com-fortable for that duration.
The positive characteristics of PMMA lenses arenumerous. PMMA is made by annealing, a proc-ess of successive heating and cooling, which leavesit free of toxic chemicals. It thus is an inert mate-
‘This discussion of lens types and characteristics is drawn from:Aquavella and Gullapali, 1980 (3); Check, 1982 (8); ConsumerReports, 1980 (9); Dixon, 1982 (13); Feldman, 1981 (14); Kersley,1980 (19); and Morrison, 1976 (27).
acetate butyrate [CAB], PMMA-silicone, andsilicone). There are variations within each group,but their respective properties are similar enoughto consider them as essentially the same type oflenses.
rial and safe for use in the eye. It can be moldedor lathed into lenses with a high degree of preci-sion. Once made, PMMA lenses can be reworkedand modified to customize them to an individual’srequirements. The result is a safe lens of excellentvisual properties which very closely conforms topatient requirements. PMMA lenses require min-imal use of cleaning, soaking, and wetting solu-tions. They may be tinted to reduce excessive lightsensitivity, to make them easier to find whendropped, or for appearance reasons. They aredurable, can be renewed by polishing away mi-nor surface scratches, and often last 5 to 7 yearsor more. Last, they tend to be cheaper than otherlens types, because they are an older product withmany small suppliers and little difference amongdifferent brands.
Despite attempts to improve their permeabilityby drilling small holes in the lenses (“fenestra-tion”), adding hydrogel to the PMMA, or othermodifications, impermeability remains the majorshortcoming of rigid PMMA lenses. Because ofthis impermeability, they cannot cover much ofthe cornea and therefore must be small. They mustbe light and thin to adhere to the eye, which pre-cludes their use for correcting corneal astigmatismbeyond a moderately severe degree.
In summation, then, hard lenses are effectivefor daily wear for those persons who have nor-mal or better tearing action and who have mainlysingle vision refractive problems, such as near-
15

16 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
sightedness (myopia) and farsightedness (hyper-metropia). They are not suitable for those withpoor tearing action, high corneal oxygen need,
SOFT LENSES
Soft lenses differ from PMMA lenses in manyways. Their basic soft quality comes from theirwater absorbency. They are usually gas-perme-able, allowing oxygen transport to the cornea.This softness and permeability make them con-siderably more comfortable than hard lenses, andmany wearers can adapt to them almost at once.These qualities can be of great advantage towearers, but they come at the expense of somevisual clarity. Soft lenses, which may containanywhere from 30 to 90 percent water, can bevery flexible, but what is called their “bag ofwater” nature has an effect on refraction, yieldingless clear images than provided by hard lenses.Additionally, high water content lenses are usu-ally fragile and easily torn. Reducing the watercontent in order to increase acuity and durability,however, sacrifices comfort. Reducing the plasticcontent to increase acuity by making a thinnerlens usually increases fragility. These tradeoffs arethe major problem with soft lenses. Further, theselenses cannot be easily modified. The extensive,but limited, inventories of ready-made lenses andthe lack of post-prescription customizing cannotpossibly meet the exact needs of all wearers. Still,lenses are readily available for the most commonrefractory corrections and may be available forless common corrections. For most wearers theoriginal fit is close enough, and the flexibility ofthe lens provides an additional, built-in elementof modification.
The comfort and permeability of soft lensesallow for uses beyond the correction of near-sightedness and farsightedness. Some brands havebeen approved by FDA for 15-day and even 30-day extended wear. Extended-wear lenses offerparticular benefits to those who find lens inser-tion and removal difficult, such as persons withextremely poor eyesight or troubled by arthritisor unsteadiness of the hand. Extended-wear softlenses, therefore, are often used by persons with
difficult multifocal correction requirements, orwho are unable to follow a daily regimen of care,insertion, and removal.
aphakia (i.e., those who have undergone lensremoval, usually due to cataracts) who may notsee well enough without contact lenses to insertthem properly, and are of particular value to olderpersons.
The larger size of soft lenses offers anotheradvantage. They can overlap comfortably ontothe scleral portion of the eye and under the lid,which stabilizes the lenses. This allows a softbifocal or multifocal lens to be tried in those casesof presbyopia (loss of flexibility in adjusting fromfar to near vision, usually associated with age)where hard PMMA bifocals have not proven suc-cessful. Multifocal soft lens are still problemati-cal for most users, particularly as other alterna-tives exist, such as bifocal eyeglasses; single visionlens-eyeglass combinations; and an unmatchedpair of monovision contact lenses, one correct-ing for nearsightedness, the other for farsighted-ness. The stability of soft lenses has also led tothe recent introduction of soft toric lenses, whichare used to correct for uneven focusing of the eye(so-called “corneal astigmatism”).
Special problems associated with soft lensesrelate to their hydrogel construction, fluid con-tent, and extended-wear functions. The potentialexists for the accumulation of both surface depos-its and bacteria, and the latter, particularly, wasthought to be a serious problem. As a result,special cleaning methods are used, and disinfec-tion techniques are also necessary. First, “hot”methods of disinfection (e.g., boiling), and then“cold” methods (chemical solutions) were devel-oped and appear to be equally effective in pre-venting serious problems that might otherwise de-velop in wearing waterlogged lenses for longperiods of time. However, these cleaning anddisinfection methods are costly, raising the ex-pense of maintaining soft lenses to upwards of$100 a year or more and stimulating the growthof a sizable lens care products industry (31).

Ch. 3—Types of Contact Lenses and Their Characteristics ● 17
GAS= PERMEABLE LENSES
Gas-permeable lenses are the newest type to ap- care. Their rigidity helps to correct astigmatism,pear and are made of either CAB, a PMMA- they are small but easy to handle, and they havesilicone combination, or pure silicone. They are recently become available in tints. Of the threerigid lenses, with the optical properties of PMMA types of gas-permeable lenses, the PMMA-siliconelenses, but approach soft lenses in comfort because combination is the most preferred at present, butof their permeability. They take more getting used the pure silicone lens has proved popular sinceto than soft lenses do but require considerably less its introduction.
PRESENT USAGE AND FUTURE TRENDS
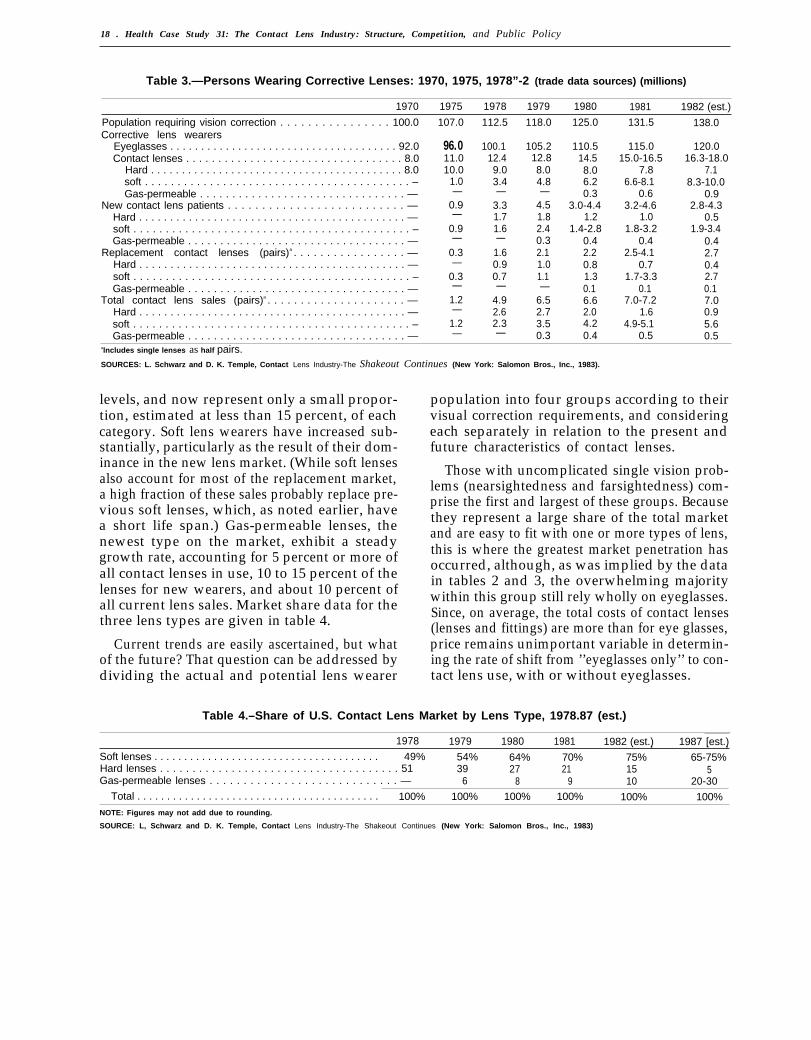
Both governmental and trade sources providedata on current levels and trends in contact lensuse, but they are in some disagreement. Com-parisons of the data in table 2, which contains esti-mates from the National Health Survey on cor-rective lens usage in 1966, 1971, and 1977, andthat of table 3, which contains estimates from in-dustry sources for the period 1970-82, show that,where the two sets overlap, the governmental sta-tistics are considerably more conservative. For ex-ample, the National Health Survey estimates oftotal lens wearers in 1971 and 1977 are 2.4 mil-lion and 7.0 million persons, respectively; thetrade data for 1970 and 1975 suggest that therewere 8.0 million and 11.0 million lens wearers inthose years. The wide gap between these two setsof estimates is explainable if the National HealthSurvey data relate to those who wear contactlenses, and the industry data, to those who havepurchased them. In any case, caution is called forin making definitive statements about rates ofsales and levels of usage of contact lenses. Thesubsequent analysis of trends and levels of con-tact lens wear derives mainly from the data intable 3, which are more detailed and current, ifhigher, than the data in table 2.
The numbers of eyeglass and contact lenswearers appear to have grown at fairly steadyrates since 1979, with eyeglass wearers increas-ing by about 5 million per year and contact lenswearers by about 1.5 million per year. Since thenumber of new contact lens patients per year iswell above 1.5 million, it appears that substan-tial attrition or failure rates do occur. The stablegrowth rate among lens wearers, however, may
Table 2.—Persons Wearing Corrective Lenses:1966, 1971, and 1977
1966 1971 1977
In millionsPopulation 3 years and over . . . . . . . . 178.9 191.6 202.9
Wearing corrective lenses. . . . . . . . 86.0 94.3 103.3Eyeglasses only . . . . . . . . . . . . . . 84.2 90.3 96.3Contact lenses, with
or without eyeglasses . . . . . . . 1.8 2.4 7.0
PercentagesPercent of population wearing lenses 48.1 49.2 50.9
Eyeglasses only . . . . . . . . . . . . . . 47.1 47.1 47.5Contact lenses, with
or without eyeglasses . . . . . . . 1.0 1.3 3.5SOURCES: 1966: U.S. Department of Health, Education, and Welfare, Character-
istics of Persons With Corrective Lenses, United States: July 1965-June 1966, Vital and Health Statistics, series 10, No. 53, prepared byM. M. Hannaford, DHEW publication No. (PHS) 1000 (Washington, DC:U.S. Government Printing Office, June 1969). 1971 and 1977: U.S. De-partment of Commerce, Bureau of the Census, Statistical Abstractof the United States, 1982-83 (103 cd.), Washington, DC, 1983.
be only a temporary phenomenon. Since new (asopposed to replacement) contact lenses are expen-sive and usually represent an alternative to eye-glasses for cosmetic reasons, it is likely that therecession of the early 1980s had a significant neg-ative effect on lens purchases. Additionally, thesales data probably do not yet reflect the ultimateacceptance levels of recent contact lens inno-vations.
Perhaps the more meaningful implications ofthe data relate to patterns among contact lenstypes rather than to aggregated totals. Here, thedata tell a less ambiguous story. The older hardlenses are declining in total usage, having droppedfrom 10 million to 7.1 million wearers between1975 and 1982. Each year they have accountedfor a declining share of both new and replacement
18 . Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
Table 3.—Persons Wearing Corrective Lenses: 1970, 1975, 1978”-2 (trade data sources) (millions)
1970 1975 1978 1979 1980 1981 1982 (est.)
Population requiring vision correction . . . . . . . . . . . . . . . . 100.0Corrective lens wearers
Eyeglasses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92.0Contact lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8.0
Hard . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8.0soft . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . –Gas-permeable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . —
New contact lens patients . . . . . . . . . . . . . . . . . . . . . . . . . . —Hard . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . —soft . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . –Gas-permeable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . —
Replacement contact lenses (pairs)a . . . . . . . . . . . . . . . . . —Hard . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . —soft . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . –Gas-permeable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . —
Total contact lens sales (pairs)a . . . . . . . . . . . . . . . . . . . . . —Hard . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . —soft . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . –Gas-permeable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . —
107.0
96.011.010.0
1.0—
0.9—
0.9—
0.3—
0.3—
1.2—
1.2—
112.5
100.112.49.03.4—
3.31.71.6—
1.60.90.7—
4.92.62.3—
118.0
105.212.88.04.8—
4.51.82.40.32.11.01.1—
6.52.73.50.3
125.0
110.514.58.06.20.3
3.0-4.41.2
1.4-2.80.42.20.81.30.16.62.04.20.4
131.5
115.015.0-16.5
7.86.6-8.1
0.63.2-4.6
1.01.8-3.2
0.42.5-4.1
0.71.7-3.3
0.17.0-7.2
1.64.9-5.1
0.5
138.0
120.016.3-18.0
7.18.3-10.0
0.92.8-4.3
0.51.9-3.4
0.42.70.42.70.17.00.95.60.5
alncludes single lenses as half pairs.SOURCES: L. Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros., Inc., 1983).
levels, and now represent only a small propor-tion, estimated at less than 15 percent, of eachcategory. Soft lens wearers have increased sub-stantially, particularly as the result of their dom-inance in the new lens market. (While soft lensesalso account for most of the replacement market,a high fraction of these sales probably replace pre-vious soft lenses, which, as noted earlier, havea short life span.) Gas-permeable lenses, thenewest type on the market, exhibit a steadygrowth rate, accounting for 5 percent or more ofall contact lenses in use, 10 to 15 percent of thelenses for new wearers, and about 10 percent ofall current lens sales. Market share data for thethree lens types are given in table 4.
Current trends are easily ascertained, but whatof the future? That question can be addressed bydividing the actual and potential lens wearer
population into four groups according to theirvisual correction requirements, and consideringeach separately in relation to the present andfuture characteristics of contact lenses.
Those with uncomplicated single vision prob-lems (nearsightedness and farsightedness) com-prise the first and largest of these groups. Becausethey represent a large share of the total marketand are easy to fit with one or more types of lens,this is where the greatest market penetration hasoccurred, although, as was implied by the datain tables 2 and 3, the overwhelming majoritywithin this group still rely wholly on eyeglasses.Since, on average, the total costs of contact lenses(lenses and fittings) are more than for eye glasses,price remains unimportant variable in determin-ing the rate of shift from ’’eyeglasses only’’ to con-tact lens use, with or without eyeglasses.
Table 4.–Share of U.S. Contact Lens Market by Lens Type, 1978.87 (est.)
1978 1979 1980 1981 1982 (est.) 1987 [est.)Soft lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. , . ,49% 54% 64% 70% 75% 65-75%
Hard lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51 39 27 21 15 5Gas-permeable lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . — 6 8 9 10 20-30
Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100% 100% 100% 100% 100% 100%NOTE: Figures may not add due to rounding.
SOURCE: L, Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros., Inc., 1983)

Ch. 3–Types of Contact Lenses and Their Characteristics “ 19
The second and third components of the totalmarket also are large, but the difficulties in de-veloping wearable lenses have left most of thismarket untapped. These two groups are, respec-tively, the moderate-to-severe astigmatic, andthose with presbyopia, for which bifocal or multi-focal corrective lenses are usually employed.
By and large, the use of contact lenses in thesethree groups can be considered “cosmetic,” since,with some exceptions, eyeglasses readily affordsatisfactory levels of correction. For the fourthmarket segment, however, contact lenses can beconsidered therapeutic, since, using the same cri-terion, eyeglasses have limited capability for cor-rection. In this group are those who suffer fromcorneal abnormalities such as keratoconus andother pathological conditions such as trachoma,corneal ulcers, and scarred corneas (20).
Projections for contact lens use for the short-run future can be made by extrapolating currentmarket trends; for the medium-run future by esti-mating the effects of changes currently underwayor impending but which have not yet materializedas strong market factors; and for the long-runfuture by predicting the effects of changes thattoday may be only hypotheses, concepts, or ideas.
In the short run, current trends are likely to con-tinue. Contact lens wearers will increase steadily,if slowly, as a percentage of the total vision-corrected population. Soft and gas-permeable lenswearers will grow and hard lens wearers will de-cline as percentages of the total contact lens-wearing population. Sales of soft lenses will growas the currently strong competition in innovationand improvement creates increasingly satisfactoryproducts for those who have not yet adoptedlenses or have failed with hard lenses. The uniquequalities of soft lenses will make them increasinglyattractive to those persons with visual problemsnot resolvable with hard or the earlier soft lenses.Accordingly, growth in the use of soft lenses islikely, perhaps at a rate of 10 to 15 percent peryear as their uses for single vision problems,astigmatism, presbyopia, and therapeutic applica-tions expand. Further, as the majority of lenswearers shifts to soft lenses, their fairly short aver-age duration (9 to 18 months) will generate a verysizable replacement lens market.
The use of gas-permeable lenses will also growrapidly as users of hard lenses switch over, non-users adopt them, and those who might otherwiseselect soft lenses are attracted by the lower long-term costs (from less frequent replacement andsimpler care procedures), and excellent vision cor-rection of the gas-permeables. An additional at-traction is that these lenses, unlike the soft ones,can be readily custom-fitted. Thus, over the next5 years gas-permeable contact lenses will contrib-ute substantially to the decline of hard lenses andmay also take part of the market that wouldotherwise be won by soft lenses. Their percent-age growth rate will be especially impressive,given the present small base against which thatrate will be calculated.
Beyond the extension of present trends into theshort-run, certain projections for the medium-runfuture can be made if one looks at forces of changecurrently in their incipiency. At present, softlenses are fragile and not reworkable. However,promising advances in plastics and in lens manu-facturing technology will result in more durableand more precisely fit soft lenses. Combined withtheir comfort and extended-wear capabilities,these improvements will enable soft lenses to pro-tect their market position relative to gas-perme-able lenses. As long as they remain distinguish-able lens types, both soft and gas-permeable lenseswill grow steadily in use. Together, they will ren-der hard lenses obsolete, and each will find itsrespective market position. Soft lenses will be theproduct of choice for those with single visionproblems who place a high premium on comfortand extended wear, and they will be especiallyuseful for presbyopia and for conditions not cor-rectable with eyeglasses. On the other hand,gas-permeable lenses will be attractive to the singlevision problem wearer who finds them sufficientlycomfortable and prefers their overall economy,ease of application, and current availability intints.
The recent introduction of extended-wear gas-permeable lenses, however, provides a strong hintthat the eventual merging of the two main typesof lenses has begun and that the future will bringa new, hybrid type of lens combining the bestfeatures of both. But in the long run, many other

20 . Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
changes which today may only be in their basicresearch stages will play prominent roles, and allpredictions are very uncertain. However, basedon what is on the horizon today, the long-runfutures of both soft and gas-permeable lenses lookpromising, possibly more so for soft lenses, if thedistinction continues. New soft lens develop-ments, such as optically superior, nontoxic ma-terials requiring minimal care even in extendeduse, and lens-making methods that allow moreexact fitting and duplication, can be expected.And as new manufacturing methods—e.g., im-provements of today’s low-cost spin-castingmethod—reduce costs, the popularity of softlenses should increase. Accordingly, the lens ofthe future may well be a low-cost, easy-to-wear,visually near-perfect, extended-wear, disposablelens.
A hybrid lens that provides the best qualitiesof both soft and gas-permeable lenses is a distinctpossibility, as mentioned. If it develops, then the
terms soft and (hard) gas-permeable will be ob-solete. An additional quality of the lens of thefuture will be durability, which may make lensesstill more affordable by reducing replacementcosts, and may increase their attractiveness tousers by making them more interchangeable witheyeglasses, since they will be able to be handledmore often without damage.
Finally, in the past, many of the important de-velopments in contact lenses originated from awide range of scientific and industrial sources.This lesson of the long-term past is particularlyapplicable to the long-term future. The technol-ogies of electronics, imaging, optics, and all ofthe other sciences are expanding exponentially.In the long run, then, contact lenses will makesubstantial gains as a form of corrective eyewear.Given their potential development, it is at leastconceivable to project their displacement of eye-glasses as the dominant method of vision correc-tion in the not-too-distant future.

4.Wearers, Prices, and Sources of Payment
WEARERS OF CONTACT LENSES
“Disorders of refraction and accommodation, ”according to the U.S. Public Health Service,ranked 14th among the 20 most common reasonsfor visiting a physician but accounted for only 1.4percent of all visits to non-Federal, office-basedphysicians in 1981 (52). Unlike other diagnosticcategories, however, refractive examinations andcorrective-lens prescribing and fitting can be ob-tained from eye-care professionals other than phy-sicians (i. e., optometrists and, in some States, op-ticians). In fact, optometrists represent abouttwo-thirds of those professionals legally permittedto examine eyes and prescribe corrective lenses,and they prescribe approximately three-fourthsof all corrective lenses and 60 percent of all con-tact lenses (5,12). If all such eye care were pro-vided by ophthalmologists, refractive disorderswould rank among the top three reasons forvisiting a physician, either closely followinghypertension and normal pregnancy or leadingthem, depending on the adjustment factor cho-sen. Accordingly, it is not surprising that over halfof the population 3 years old and above wear cor-rective lenses and that about 15 million personswear contact lenses.
In table 5, data from three National HealthSurvey studies of corrective lens wearers arepresented. These data, for 1965-66, 1971, and1979-80, show some interesting patterns andtrends among users. In each of the study periods,contact lens wearing was at least twice as preva-lent among females, overall, as among males. Fur-ther, lens wearing is most common among youngadults, tapering to low levels at middle age andbeyond. This pattern is almost totally the oppositeof the age-related frequency of use of eyeglasses.(However, in 1979-80, lens wearing in the 65 andover group, both males and females, rose sharply. )Third, over the covered period, lens wearing in-creased at every age level for both males andfemales. Thus, the general view of contact lensesas primarily a “younger female” product has sub-
Table 5.—Contact Lens Wearers, Percentof Population, by Sex and Age,
1965-66, 1971, and 1979.80
Percent of population 3years and over wearing
contact lenses
Sex and age group 1965-66 1971 1979-80
Both sexes:All ages, 3 and over. . . . . . . . .3-16 . . . . . . . . . . . . . . . . . . . . . . .17-24 . . . . . . . . . . . . . . . . . . . . . .25-44 . . . . . . . . . . . . . . . . . . . . . .45-54 . . . . . . . . . . . . . . . . . . . . . .55-64 . . . . . . . . . . . . . . . . . . . . . .65 and over . . . . . . . . . . . . . . . .
Male:All ages, 3 and over. , . . . . . . .3-16 . . . . . . . . . . . . . . . . . . . . . . .17-24 . . . . . . . . . . . . . . . . . . . . . .25-44 . . . . . . . . . . . . . . . . . . . . . .45-54 . . . . . . . . . . . . . . . . . . . . . .55-64 . . . . . . . . . . . . . . . . . . . . . .65 and over . . . . . . . . . . . . . . . .
Female:All ages, 3 and over. . . . . . . . .3-16 . . . . . . . . . . . . . . . . . . . . . . .17-24 . . . . . . . . . . . . . . . . . . . . . .25-44 . . . . . . . . . . . . . . . . . . . . . .45-54 . . . . . . . . . . . . . . . . . . . . . .55-64 . . . . . . . . . . . . . . . . . . . . . .65 and over . . . . . . . . . . . . . . . .
1.00.33.71.30.40.3—
0.6—2.00.90.3
1.30.45.21.70.5——
2.10.66.63.00.70.70.7
1.20.33.41.80.50.70.7
2.90.99.54.20.90.60.7
4.51.09.47.72.11.64.3
2.80.65.34.41.41.44.6
6.21.5
13.310.72.71.94.0
SOURCES: 1965-66: U.S. Department of Health, Education, and Welfare,Characteristics of Persons With Corrective Lenses, United StatesJuly 1965-June 1966, Vital and Health Statistics, series 10, No. 53,prepared by M. M. Hannaford, DHEW publication No. (PHS) 1000(Washington, DC: US. Government Printing Office, June 1969) 1971:U.S. Department of Health, Education, and Welfare, Characteristicsof Persons With Corrective Lenses, United States: 1971, Vital andHealth Statistics, series 10, No. 93, prepared by M. H. Wilder, DHEWpublication no. (HRA) 75-1520, Washington, DC, 1974. 1979-60: R. Hol-Iander, U.S. Department of Health and Human Services, Public HealthService, Rockville, MD, personal communication, June 30, 1983.
stantial validity, but the pattern presently ischanging in substantial ways and will be con-siderably different in the future. The currentchanges, particularly the increasing use of con-tact lenses by older persons, are attributable toyounger lens wearers’ moving through the agespectrum; the development of newer types ofbifocal and toric lenses, which relate especiallyto the vision problems of older persons; and the
23
25-339 0 - 84 - 5 : QI, 3

—
24 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
growth in soft and extended-wear lenses, whichparticularly help older persons, whose eyes areless accommodating to contact lenses than arethose of younger persons. Further, differences inthe rates of lens usage by women and men are nar-rowing, and in new fits the differences will soonbe eliminated. Accordingly, the lens market willno longer be dominated by the young adult femalewearer; the traditional patient base will expandwidely; and all groups except perhaps children willbecome important users.
Although as large a part of the population withvision correction suffers from presbyopia as fromsingle-vision problems, lens wearing is much moreprevalent among the latter group. As lenses forall users improve, the greatest relative growth willbe for presbyopes and astigmatic, but contactlenses will continue to be prescribed most fre-quently for single-vision problems. Within thesingle-vision category, about 60 percent havemyopia, 40 percent hyperopia. In addition, therelative use of contact lenses for those with myopiaruns somewhat higher than among those withhyperopia. Therefore, at least through the 1980s,the largest absolute volume of sales will continueto be for the correction of myopia, followed byhyperopia, with presbyopic use gaining quicklyand perhaps passing hyperopia before the 1980shave ended.
Additional data from the National Health Ex-penditures Survey (51) show contact lens use tobe relatively more common in suburban than ru-ral or inner-city areas, among whites than non-whites (particularly blacks and Hispanics), andalso to be positively associated with the educa-tional level of the family head. All of these cor-relations are explainable in terms of the higher in-come levels among suburban residents, whites,and the more educated. (Other features in the pat-tern of contact lens use show that lenses are moreoften worn by white-collar and service workersthan by blue-collar or farm workers. These dif-ferences may also be explainable in part by in-come differentials, but probably more so by thegreater proportion of women employed in thewhite-collar and service sectors, and perhaps alsoby the actual physical conditions of each type ofwork. ) In other words, contact lenses are a “nor-mal” economic good, with purchases expanding
as income expands, or in economists’ parlance,with a positive income elasticity of demand.
Data from the National Center for Health Serv-ices Research’s National Health ExpendituresStudy (table 6) shed a bit more light on the in-come elasticity of demand for contact lenses. (Theincome elasticity of demand measures the relation-ship between changes in income and the resultingchanges in the number of units purchased. ) If wewere to assume average incomes within the threeclasses to be $6,000, $18,000, and $30,000 respec-tively, with all other characteristics showing simi-lar patterns among income classes, then the in-come elasticity would be approximately 0.13 to0.27, which is a plausible range of estimation. (Anincome elasticity of demand of 0.13 means thata l-percent increase [decrease] in income causesa 0.13 of l-percent increase [decrease] in units[pairs of contact lenses] purchased.)
Although no measurement or estimation ismade here of the price elasticity or cross elasticityof demand (defined as the effects on lens purchasesof changes in the price of lenses and of changesin the price of other goods, particularly eyeglasses,respectively) for contact lenses, certain relation-ships may be suggested on the basis of recent ex-perience. First, the demand for lenses seems to beat least somewhat sensitive to changes in the rela-tive price of lenses in that wearers of eyeglassesfrequently specify cost as one of their reasons fornot switching to lenses. (Theoretically, if the de-mand for a product is sensitive to changes in in-come levels, it also is sensitive to price changesof that product. The connection between thetwo is the so-called “income effect” of the pricechange. )
Table 6.—Purchase or Repair of Contact Lensesper 1,000 Population at Different Family
income Levels, 1977
Persons with purchase or repairFamily income of contact lenses
Less than $12,000 . . . . . . 0.9$12,000 to $19,999 . . . . . 1.1$20,000 or more. . . . . . . . 1.4SOURCE: U.S. Department of Health and Human Services, Public Health Service,
National Center for Health Statistics, 1981 Summary: National Ambu-latory Medical Care Survey, NCHS Advance data, prepared by L. Law-rence and T. McLemore, No. 66, Hyattsville, MD, Mar. 16 1963.

Ch. 4—Wearers, Prices, and Sources of Payment ● 25
Second, through time, new developments inboth contact lenses and eyeglasses may have nar-rowed the qualitative differences between the twotypes of corrective lenses, leaving the remainingdifferences, including price, as relatively more im-portant bases of choice than previously was thecase. For example, lenses may be bought becausewearers “look better” than if they were wearingeyeglasses. However, the emphasis on “fashioneyewear” has made the wearing of eyeglasses, par-ticularly among males, considerably more accept-able. Other qualitative advantages of contactlenses may have been offset by improvements ineyeglasses: the lightness of contact lenses havebeen offset somewhat by the popularity of light,plastic lenses for eyeglasses; tinted contact lensesare matched by “prescription sunglasses” andphoto-chromic spectacle lenses; both contact andeyeglass lenses are available in bifocal and multi-focal modes; new sports goggles have eliminated
PRICES
In 1980, consumers spent an estimated $700 mil-lion on contact lenses, lens-care products, andprofessional services (23). In view of the signifi-cant growth in contact lens usage, this dollar fig-ure would have been much higher had it not beenfor the notable price declines of the late 1970s,which have continued into the 1980s.
These declines are exemplified by the data intable 7, which show soft-lens list prices to thepractitioner and total fitting prices, includinglenses, for selected years from 1971 to 1982. Soft-lens prices fell by over 50 percent during this
the safety advantage of contact lenses in activi-ties where spectacle frames and lenses have poseda problem; new eyeglass lenses of plastic on theinside, for safety, and glass on the outside, fordurability, have just been introduced.
Thus, although the price level of correctiveeyewear as a whole determines the affordabilityof obtaining vision correction, the price structureof corrective eyewear (the magnitude of the dif-ferential between the price of contact lenses andthat of eyeglasses) appears to be influential in thechoice between the two alternatives. Here again,recent events seem favorable for long-term growthin contact lens usage, because prices for lens fit-ting have dropped significantly and are likely tocontinue to compare favorably with eyeglassprices. (Causes of these price declines will be iden-tified in the next section of this chapter. )
period. Total fitting prices have also fallen, re-flecting in part the effects of the fall in the priceof the lens component of the total price. Despitethe high rates of general and medical price infla-tion during this period, which would have morethan offset lens price declines, there were alsostrong competitive forces at work within and be-tween the various categories of fitters which kepttotal prices stable or declining. Thus, contact lensand total fitting prices have experienced large re-ductions despite high inflation. Although pricetrends for gas-permeable lenses are still too earlyto trace, two forces running counter to each other
Table 7.—Average Soft Contact Lens List and Totai Fitting Prices, per Pair,1971-82, Seiected Years
1971-74 1975 1980 1981 1982
List pricea . . . . . . . . . . . . . . . . . . . . $65.00 $68.70 $50.00 $40.00 $30.00Total fitting price:a
Ophthalmologist . . . . . . . . . . . . . $500-600 $250-325 $250-300 $250-300 $250-300Optometrist . . . . . . . . . . . . . . . . . 300-350 400 250 225 225Optical outlet . . . . . . . . . . . . . . . — — 170 150-170 125
Large chain . . . . . . . . . . . . . . . 120 100Independent. . . . . . . . . . . . . . . 178 160
aPrices are higher for extended-wear soft Contact lenses.
SOURCES: L. Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros., Inc.,1983); and M. Carr, Health Products Research, Inc., Somerville, NJ, personal communication, July 7, 1983,

26 ● Health Case Study 31: The Contact Lens Industry: Structurer Competition, and Public Policy
will determine that trend. First, the early domi-nance of Syntex in the PMMA-silicone lens fieldhas given it an established position much like thatof Bausch & Lomb in the first years of soft lenses.Without serious competition in PMMA-siliconelenses, Syntex has avoided direct price competi-tive moves by close rivals. (However, althoughBausch & Lomb was the only seller of soft lensesfor 3 or 4 years, Syntex must take heed, at leastto some extent, of the prior presence of threecellulose acetate butyrate (CAB) lenses in the gas-permeable market. ) On the other hand, gas-per-meable lenses represent replacements for hardPMMA lenses and alternatives to soft lenses. Bothof these other types of lenses have experiencedsharp price reductions as the number of sellers hasgrown, excess production capacity has emerged,and cost-reducing production methods have beendeveloped. In fact, wholesale hard lens prices ranless than $10 a pair in 1982 (10), and total fittingcosts were, on average, 30 percent lower than forother lens types.
The prospects are strong that future price de-clines will be a common event in the markets, if
SOURCES OF PAYMENT
Consideration of how the yearly $700 millionexpenditure for contact lenses, lens-care products,and fitting services is paid for raises two questions:first, what are the sources of payment funds, andsecond, does the payment pattern, specifically theshare from Federal program sources, exert a feed-back influence on the quantity of demand for thecovered goods and services.
The three main sources of funds for health careexpenditures are family out-of-pocket payment,private insurance, and government. These threesources can also be separated by the distinctionbetween “private” and “public” sources, withfamily out-of-pocket and private insurance groupedtogether as private and government classified aspublic; and also by the distinction between out-of-pocket and “third-party,” which includes bothprivate insurance and government.
For all personal health care expenditures as awhole, 33 percent is paid out-of-pocket, almost
economic forces are free to manifest themselves.While empirical verification is lacking, it may wellbe the case that there are no substantial economiesof scale in research or manufacturing, since smallerfirms show impressive records in product andprocess discoveries, improvements, and imple-mentation. The economic barriers to entry arelow, with capital requirements relatively modest,the necessary inputs widely available, and withfew important patent barriers. And an informedgroup of buyers (practitioners) serve to mitigate,at least somewhat, the effects of excessive or flam-boyant promotional rivalry. Accordingly, manyrivals, of small but efficient size, with abundantresearch and production capacity, seem ready topromote technological progress, efficient produc-tion, and competitive pricing. However, there areseveral threats to this competitive state of affairs,particularly the regulatory barrier to entry, in theform of a costly and sometimes long approvalprocess before widespread marketing of a lens ispermitted by the Food and Drug Administration(FDA). (The matter of FDA approval is examinedin ch. 7.)
27 percent by private insurers, and 40 percent bygovernment. Thus, the payment mix is 60 percentprivate/40 percent public and 33 percent out-of-pocket/67 percent third-party in origin (57).
Among the different components of personalhealth care the proportions vary considerably. Forexample, in 1981 the range, using the private/pub-lic distinction, went from 44 percent private/56percent public for nursing home care to 96 per-cent private/4 percent public for dentists’ serv-ices. For the out-of-pocket v. third-party distinc-tion, the range went from 11 percent out-of-pocket/89 percent third-party for hospital care to82 percent out-of-pocket/18 percent third-partyfor eyeglasses and other medical appliances. Thus,contact lenses are in a group of products with thelowest proportion of payment by third-partysources. In terms of private v. public sources, theyare close to dentists’ services for the lowest pro-portion of payments by government, with 10 per-cent (57) 0

Ch. 4—Wearers, Prices, and Sources of Payment “ 27
If third parties as a whole and government inparticular play relatively small roles in financing“eyeglass and appliance” purchases, those rolesare even smaller in the case of contact lenses. Interms of private insurance, for example, one largesurvey of employer-provided health-care planscovering 21.8 million workers showed that only3.6 million were covered for vision-care, includingexaminations, refractions, and eyeglass lenses andframes. When there is vision-care insurance, thestudy found, contact lenses may be included.Thus, private insurance for vision-care expensesapplied to only 16.5 percent of the workers in thisstudy, and coverage for contact lenses was nar-rower and shallower, geared mainly to the costof eyeglasses (57).
Government programs that pay for personalhealth care are numerous, and include Medicareand Medicaid; the Civilian Hospital and Ambu-latory Medical Program of the Uniformed Serv-ices (CHAMPUS); the Civilian Hospital andAmbulatory Medical Program of the VeteransAdministration (CHAMPVA); the Veterans Ad-ministration; the military; the Indian Health Serv-ice; and other Federal, State, county, and citypayers (51). All these sources together represent,as indicated, 10 percent of the payment for eye-glasses and appliances, and about 8 percent of theannual expenditures for purchases and repairs of“vision aids” (51). Little, if any, authorization ex-ists for the provision of funds for contact lenses.Medicare, the main Federal health financing pro-gram for elderly or disabled people, pays only forlenses for therapeutic use, and most of these lensesare connected with cataract removal (4), for whichintraocular lenses are increasingly being used.
Considerably less is known about the 55 sepa-rate Medicaid programs, which are jointly fundedby the Federal Government and the States or ter-ritories. A review of the overall Medicaid enabl-ing legislation makes no mention of contact lenses.
Therefore, public sector outlays, while coveringmany millions of eligible recipients, are apparentlynot available for a very large majority of all con-tact lens purchases (4,49,54).
The result of the limited applicability of bothprivate and public third-party arrangements isthat an estimated 84 percent of all vision-aid costsare funded out-of-pocket. Of the 16 percent thatis covered, more of it appears to be provided byprivate sources than government. Therefore, ifthird-party payments increase health care utili-zation over that occurring in a market where allpayment is out-of-pocket, such effects are likelyto be relatively small for contact lenses. The roleof government in inducing greater demand issmaller still, since government plays a lesser rolethan private insurers, and that role, such as it is,is limited to a small part of the current patientpopulation.
Further, if resources are not drawn into the de-velopment and manufacture of contact lens dueto expanded utilization levels, then resourceallocation to this industry has suffered relative toother medical technologies, which are more broadlycovered by insurance. It is, of course, possible thatdevelopments in contact lenses would have beeneven more pronounced with insurance coveragecomparable to that which has been available topay for other medical technologies. Yet the per-formance level of the contact lens industry seemsnot to have been affected adversely; its record ofinnovation, quality improvement, and price re-duction is impressive when compared to mostother medical goods and services. Perhaps the ex-planation for this apparent paradox is to be foundin the fact that, unlike other medical technologies,contact lenses are a consumer-oriented product,sold in a market setting where the buyer-sellerrelationships emphasize rivalry in three importantdimensions: innovation, quality, and price.

5 .Producers of Contact Lenses
A large number of firms make contact lenses,but the overall industry is rather highly concen-trated and the largest half-dozen manufacturershold most of the market. For example, soft lensescurrently make up 75 percent of total lens pro-duction, and the four largest soft lens producersaccount for over two-thirds of that sector, equiva-lent to about 55 percent of the total contact lensmarket (table 8). Gas-permeable lenses representabout 15 percent of the total market, but one type,PMMA-silicone lenses (which outsell the othertype, CAB lenses, by four pairs to one), are almostentirely provided by one firm (table 9). Only forhard lenses, which have a small and decliningshare of the market, are there many sellers, noone or few of which are dominant.
Sales concentration in the predominant soft-lenssector would rank high by most economic stand-
ards. The largest firm, Bausch & Lomb, accountsfor at least 40 percent of the market. The fourlargest (adding American Hydron, Barnes Hind/Hydrocurve, and CooperVision1) account forabout 70 percent; and the seven largest (includingUCO Optics, Wesley-Jessen, and American Op-tical) account for over 80 percent of the market(31). (UCO has since been acquired by Cooper-Vision, doubling the latter’s market share to ap-proximately 15 percent and increasing the four-and eight-firm concentration levels somewhat(41). ) The data on firm shares in this market seg-ment for 1978 to 1982 are presented in table 8,which shows four- and eight-firm concentrationlevels to be high in each of the 5 years. However,both, especially four-firm concentration levels,
‘CooperVision was recently sold to Nestle.
Table 8.—Market Shares and Concentration Ratios, Soft Lenses,1978-82 (est.) (percentages)
Firm 1978 1979 1980 1981 1982 est.
Bausch & Lomb. . . .61 48 53 48 40+American Optical . . . . 16 19 13 11 4Barnes-Hind/Hydrocurve . . . . 12 14 11 10 13Wesley-Jessen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 4 3 2 5UCO Optics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 8 7 8 7Channel/Lombart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . — 3 4 3 2American Hydron . . . . . . . . . . . . . . . . . . . . . . . . . . . . — 3 5 7 8CooperVision . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . — — 2 3 8Vistakon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 2 2Other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . — — 1 7 9
Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100 100 100 100 100Four largest firms total . . 95 89 84 77 69Eight largest firms total . . . . . . . . . . . . . . . . . . . . . . . 100 100 98 91 89SOURCE: L. Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros., Inc., 1963).
Table 9.—Market Shares and Concentration Ratios, Gas-Permeabie Lenses,1979-82 (est.) (percentages)
Firm Trade name Lens type 1979 1980 1981 1982 (est.)
Syntex . . . . . . . . . . . . . . . . . . Polycon PM MA-silicone 30 67 64 80Barnes-Hind/Hydrocurve . . . CAB Curve CAB – – 15 6Danker Laboratories. . . . . . . Meso CAB 40 20 11 6Rynco Scientific . . . . . . . . . . RX56 CAB 30 13 9 5Dow Corning . . . . . . . . . . . . . Silcon silicone — — 1 3
Four largest firms total. . . . . . . . . . . . . . . . . . . . . . . . . . . . I00a 100 a 99 97aThree firms accounted for the total market.SOURCE: L. Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros., Inc., 1983).
31

32 ● Health Case Study 31: The Contact Lenss Industry: Structure, Competition, and Public Policy
have declined steadily. Although the shares of theleading firms are far from being equalized, com-petitors capable of eroding the share of the one-time monopolist in soft-lens manufacture, Bausch& Lomb, are well established in the market.
For gas-permeable lenses, there are fewer firms,and the dominance of the leader is greater thanin the case of soft lenses. Here, as indicated earlier,the preferred PMMA-silicone lenses have 80 per-cent of gas-permeable lens sales. One firm, Syntex,accounts for about the entire output of PMMA-silicone lenses. (Several others were marketing thistype of lens to a limited extent in 1983, but theirproducts had not yet been approved by the Foodand Drug Administration (FDA). They have beenmarketing their lenses under “Investigational De-vice Exemptions” issued by FDA and thereforemust operate within certain restrictions. ) Fourfirms produce the CAB-type, and one (Dow Cor-ning) markets an all-silicone gas-permeable lens.Thus, the gas-permeable lens’ general market isalso highly concentrated, with one dominant firm,five others with small shares, and a fringe of sev-eral brands under clinical investigation or ap-proved for a specific use only. Market share datafor this sector are presented in table 9.
However, the dominance of Syntex and thealmost 100 percent four-firm concentration level,while implying a potentially noncompetitive sit-uation, must be viewed in historical perspective.The soft lens market was dominated for the firstseveral years by the initial entrant, Bausch &Lomb, but subsequent entry, after 4 to 5 years,led to the erosion of Bausch & Lomb’s share anda decreasing four-firm concentration ratio. Thevigorous competition in this market has been dem-onstrated by the sizable price declines describedin the previous chapter. Therefore, the situationin gas-permeable lenses represents, at least thusfar, a replication of the development of soft lenses.If substantial entry occurs, Syntex’s large sharewill be reduced and strong price competition willoccur. But even if entry occurs only gradually,firms that may dominate in this sector of the in-dustry must still take into account the substitut-ability among lens types and thus adopt pricesthat practitioners and patients will accept relativeto those of hard and soft lenses.
For the older, hard PMMA lenses, the case isquite different. This market sector has been char-acterized as a “cottage industry,” where small lab-oratories prevail. They generally operate withina small geographic area, manufacturing lensesfrom plastic “buttons” purchased from bulkplastics manufacturers, and providing customservices to prescribing dispensers. There are manysuch small manufacturers and so-called “opticallaboratories” that can compete effectively withlarger manufacturers. While the case is not con-clusive, there is at present no evidence of econ-omies of large-scale production in lens manu-facturing of any type. However, many smallmanufacturers have gone out of business or suf-fered sales declines during the past decade becauseof the shrinkage of the market for hard lenses,and the small firms’ inability to meet the require-ments for FDA approval of the newer lens types(22). Nonetheless, this segment of the market re-mains especially price competitive.
In summation then, the three sectors of the con-tact lens industry display different degrees of com-petition, yet the differences are explainable interms of the different stage in the “life cycle” ofeach. The mature hard lens sector has few, if any,dominant firms, and has been highly price com-petitive for many years. The soft-lens sector ismoving out of its youth phase and now displaysincreasing entry, an equalizing of market poweramong a group of large firms, and strong com-petition in price and innovation. The newest prod-uct sector, gas-permeable lenses, thus far hasretraced the steps of the soft-lens sector, and theeconomic forces at work promise to maintain thatsimilarity, conditional on the magnitude of thebarriers to entry such as those posed by premarketregulatory requirements.
With regards to the individual firms who com-prise the industry, table 10 provides data on 17major competitors, ranging from Bausch & Lomb,with 1982 worldwide lens sales of $150 millionand profits of $52 million (including lens solu-tions), to Rynco and Alcon Optic, each with only$2 million in sales. Of these 17 firms, only Bausch& Lomb can be called a broad line optical goodsproducer; the others are primarily contact lensproducers, although many have broad contact

Ch. 5—The Producers of Contact Lenses ● 33
Table 10.—Worldwide Sales, Profit, and R&D Data of the 17 Major Firmsin the Contact Lens Industry, 1982 (millions of dollars)
Contact lens Lens solutions OperatingFirm (and parent company) sales sales profit
Bausch & Lomb . . . . . . . . . . . . . . . . . . . . . . . . . 150.0 57.0 52Barnes-Hind/Hydrocurve (Revlon). . . . . . . . . . . 38.0 48.0 8.5CooperVision (Cooper Laboratories) . . . . . . . . 36.0 15.0 17.2Syntex Ophthalmic (Syntex Corp.) . . . . . . . . . 26.7 — 0.7American Hydron (National marginally
Patent Development Corp.) . . . . . . . . . . . . . . 30.0 — profitableUCO Optics (CooperVision) . . . . . . . . . . . . . . . 19.0 — 2.8Wesley-Jessen (Schering-Plough, Inc.) . . . . . . 15.0 — marginally
profitableAmerican Optical . . . . . . . . . . . . . . . . . . . . . . . . 13.0 — lossAmerican Medical Optics (American
Hospital Supply) . . . . . . . . . . . . . . . . . . . . . . . 2.5 — —Ciba Vision Care (Ciba-Geigy) . . . . . . . . . . . . . 9.0 — lossVistakon (Johnson & Johnson). . . . . . . . . . . . . 8.0 — lossDanker Laboratories . . . . . . . . . . . . . . . . . . . . . . 5.0 — lossDow Corning Ophthalmic (Dow Corning Corp.) 5.0 — lossChannel-Lombart (Channel Industries) . . . . . . 8.0 — lossRynco Scientific . . . . . . . . . . . . . . . . . . . . . . . . . 2.0 — lossAlcon Optic (Nestle). . . . . . . . . . . . . . . . . . . . . . 2.0 26.0 NAAllergan (Smith Kline-Beckman) . . . . . . . . . . . . — 69.0 NANA indicates data not available.
SOURCES: L. Schwarz and D K Temple, Contact Lens Industry-The Shakeout Continues (New York Salomon Bros., Inc.,1983), and Moody’s Industrial Manual, 1982, vols. 1 and 2 (New York: Moody’s Investor Service, 1982).
lens product lines or are owned by parent com-panies that range across the health care and per-sonal products fields or even into heavy indus-try and broadly based conglomerate activities. Infact, 13 of the 17 largest firms are parts of largercorporate organizations as a result of mergers andacquisitions, and the acquisition of one or morecontact lens firms is usually only part of a largeracquisition pattern by the parent company (seeapp. A).
Small firms historically have been among theindustry’s most successful innovators, and entryvia small-firm acquisition often provides the largeracquirer with a position in the industry more ad-vanced than it could obtain with a “de novo” en-try. (For example, Syntex, which had a bifocalsoft lens only “in development, ” recently acquiredSalvatori Laboratories, a long-established, smallerfirm which had moved very to close to obtainingFDA approval for a bifocal soft lens. ) This ad-vanced position, combined with the parent com-pany’s financial resources, marketing strength,and in one case a captive chain of dispensing op-tician outlets, provides a strong potential for even-tual large-scale commercial success. Thus, on theone hand, the “deep pocket” of the acquirer, to-
gether with the innovational momentum of theacquired firm, provides an effective challenger tothe market position of dominant firms, whichenhances competition. On the other hand, con-tinuous acquisitions of smaller by larger firms nar-row the base of product innovation. A largernumber of small, dynamic firms becomes reducedto a smaller number of larger firms, and there isas yet little, if any, evidence to indicate that theircombined research productivity will exceed thatof the smaller firms.
As a result of both mergers and internal expan-sion, almost all of the major firms produce sev-eral lines of contact lenses (see table 11). The twofirms included in table 10 but not in table 11 areAlcon Optic and Allergan, each of whose primaryactivity is the sales of lens solutions. Most havediversified their product lines to cover all or mostof the soft lenses’ individual submarkets as wellas gas-permeable lenses.
Thus, while the number of major competitorsis growing, their full-line strategies are making itmore difficult for the small, specialized firm tooccupy more than a toehold position. For exam-ple, a list of FDA-approved spherical (single-
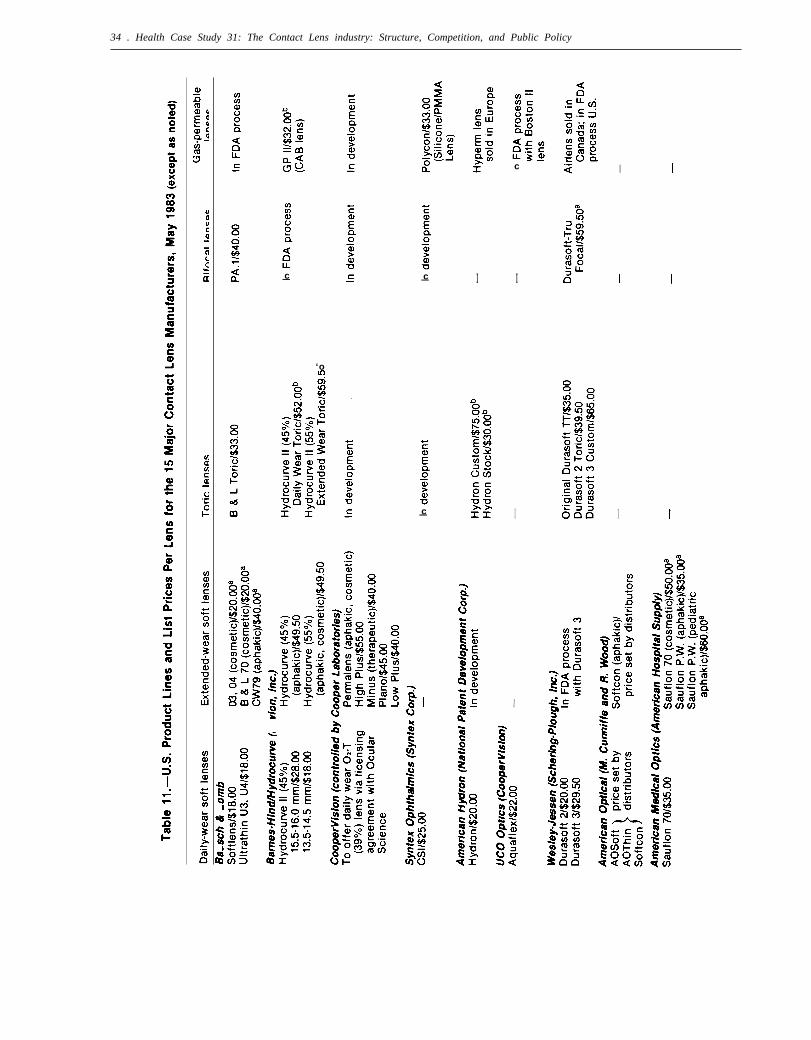
34 . Health Case Study 31: The Contact Lens industry: Structure, Competition, and Public Policy
c I I
I I Ic— c— I
‘om
c— I I
I
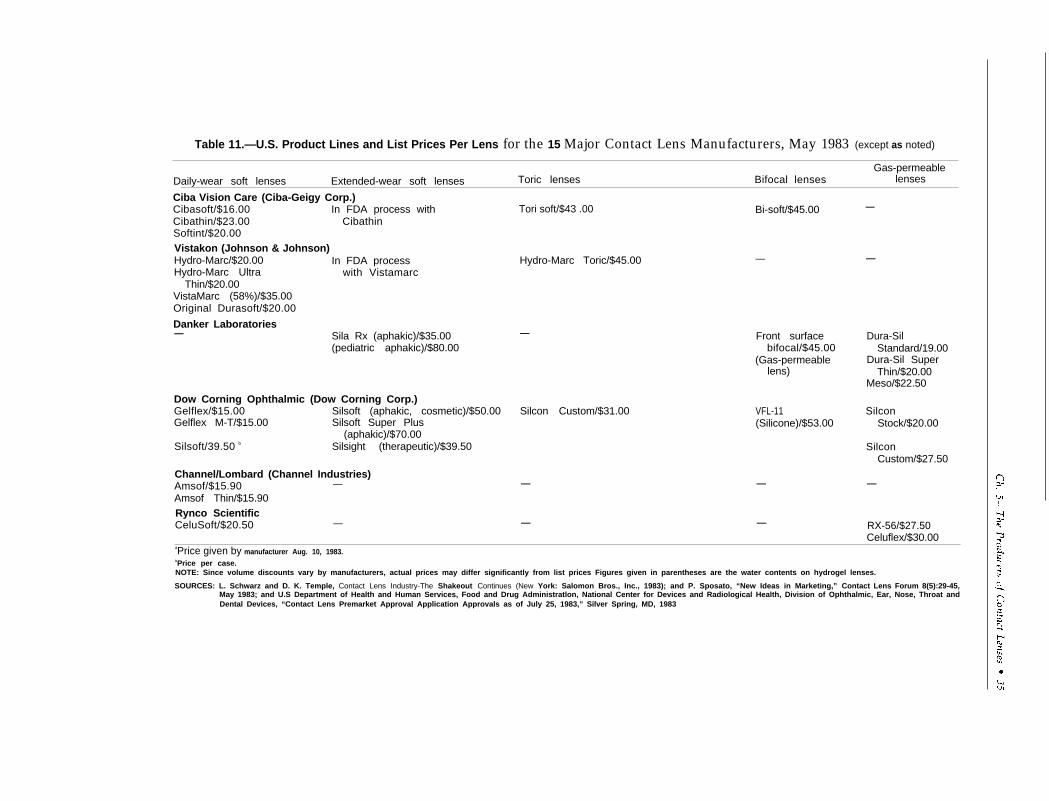
Table 11.—U.S. Product Lines and List Prices Per Lens for the 15 Major Contact Lens Manufacturers, May 1983 (except as noted)
Gas-permeableDaily-wear soft lenses Extended-wear soft lenses Toric lenses Bifocal lenses lenses
Ciba Vision Care (Ciba-Geigy Corp.)Cibasoft/$16.00 In FDA process withCibathin/$23.00 CibathinSoftint/$20.00Vistakon (Johnson & Johnson)Hydro-Marc/$20.00 In FDA processHydro-Marc Ultra with Vistamarc
Thin/$20.00VistaMarc (58%)/$35.00Original Durasoft/$20.00
Danker Laboratories— Sila Rx (aphakic)/$35.00
(pediatric aphakic)/$80.00
Dow Corning Ophthalmic (Dow Corning Corp.)Gelflex/$15.00 Silsoft (aphakic, cosmetic)/$50.00Gelflex M-T/$15.00 Silsoft Super Plus
(aphakic)/$70.00Silsoft/39.50 b Silsight (therapeutic)/$39.50
Channel/Lombard (Channel Industries)Amsof/$15.90 —Amsof Thin/$15.90Rynco ScientificCeluSoft/$20.50 —
Tori soft/$43 .00 Bi-soft/$45.00
Hydro-Marc Toric/$45.00 —
— Front surfacebifocal/$45.00
(Gas-permeablelens)
Silcon Custom/$31.00 VFL-11(Silicone)/$53.00
— —
— —
—
—
Dura-SilStandard/19.00
Dura-Sil SuperThin/$20.00
Meso/$22.50
SilconStock/$20.00
SilconCustom/$27.50
—
RX-56/$27.50Celuflex/$30.00
aPrice given by manufacturer Aug. 10, 1983.bPrice per case.NOTE: Since volume discounts vary by manufacturers, actual prices may differ significantly from list prices Figures given in parentheses are the water contents on hydrogel lenses.
SOURCES: L. Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros., Inc., 1983); and P. Sposato, “New Ideas in Marketing,” Contact Lens Forum 8(5):29-45,May 1983; and U.S Department of Health and Human Services, Food and Drug Administratlon, National Center for Devices and Radiological Health, Division of Ophthalmic, Ear, Nose, Throat andDental Devices, “Contact Lens Premarket Approval Application Approvals as of July 25, 1983,” Silver Spring, MD, 1983

36 . Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
vision correction) soft lenses (see app. A) includesthose of 17 firms not included in table 11, but theircombined market share is not more than 1 or 2percent. None of the firms outside of the 15 intable 11 had an FDA approval at the end of 1983for the sale of extended-wear, cosmetic-use softlenses, and only two firms not on the list had anapproved bifocal soft lens (31,48).
Last in this survey of the activities and relativesizes of the various lens manufacturing firms is
a brief profile of each, emphasizing its method ofentry into the industry and the acquisitions andlicensing arrangements that have contributed toits growth. This material is presented in appen-dix B. These descriptions show that acquisitions,joint ventures, and licensing agreements haveplayed important roles in firm growth and rela-tive market shares in the contact lens industry.The public policy aspects of these growth mech-anisms are discussed in chapter 7.
6
Contact Lens Prescribers andDispensers

6 ■
Contact Lens Prescribers and Dispensers
Contact lenses are prescribed and fitted by threetypes of eye-care practitioners: ophthalmologists,optometrists, and, to a limited extent, opticians.Ophthalmologists are doctors of medicine, spe-cializing in problems of the eye. As such, theymay perform a wide variety of examination pro-cedures and medical and surgical treatments, testfor refraction errors, and prescribe and fit all typesof corrective lenses. Optometrists are also spe-cialists in eye care, but their functions, althoughexpanding, are narrower than those of ophthal-mologists. Optometrists generally measure refrac-tion, prescribe and fit corrective lenses, and detectand diagnose vision problems and the conditionof the eye for referral to ophthalmologists andother appropriate practitioners. In some States,
OPHTHALMOLOGISTS
There are about 12,500 ophthalmologists in theUnited States today, of whom perhaps 11,000 areinvolved in regular patient care as hospital- oroffice-based physicians. (The remainder are oph-thalmology residents or engaged in teaching andresearch. ) Half or more of these 11,000 offerdispensing services in addition to prescribing cor-rective eyewear, sometimes in conjunction withopticians. They account for 30 percent of the totalretail corrective lens market and about 20 percentof the contact lens market, operating from 6,000locations with $1.35 billion in revenues (5).
optometrists may use drugs for diagnostic pur-poses, and in a few, use for therapeutic purposesalso. Fewer generalizations can be made about therole of opticians, since the State laws defining theirpermissible scope of activities vary, but opticiansare usually limited to the roles of “dispensing op-ticians, ” who make and fit corrective lensesprescribed by ophthalmologists and optometrists,either under their supervision or independently,or “optical technicians, ” who grind the lenses forothers to fit to patients. In some States, however,opticians may also examine, prescribe, and fit pa-tients with contact lenses, if an ophthalmologistor optometrist has already determined that the pa-tient needs some form of corrective lenses (5,55).
Of all dispensing ophthalmologists, at presentmore fit soft lenses (73 percent) than hard (71 per-cent) or gas-permeables (51 percent). This situa-tion is reflected in the relative amounts of the threetypes of lenses ophthalmologists prescribe in theaggregate, as shown by the data on prescribingpractices by ophthalmologists in table 12.
Other significant data on ophthalmologists’contact lens practices relate to prices and wereshown in table 7. Those data indicate that the costof being fitted with contact lenses by an ophthal-
Table 12.—Contact Lens Fitting by Ophthalmologists, 1982
Lens type
soft Hard Gas-permeable All
Percent of ophthalmologists fitting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73 71 51Percent of all contact lenses fitted by ophthalmologists . . . . . . . . . . . . . . . . . . . . . . 68 23
—9
Contact lenses fitted by ophthalmologists as a percent—
of total fittings by all practitioners . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20a 26a NA 15-20NA indicates data not available,a1979.
SOURCES: M. Carr, Health Products Research, Inc., Somerville, NJ, personal communication, July 7, 1983; S. Davidson,Ophthalmic, Norfolk, VA, 1983; D. P. Hayes,
“Market Data Book,” unpublished, Dow Corning“Results From the Vision Care Survey Relative to the Profile of Contact Lens Fitters, ” Contact and Intraocular
Lens Medical Journal 7(1):9-10, January-March 1981; and L. Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: SalomonBros., Inc., 1983).
39
25-339 0 - 84 - 4 : QL 3
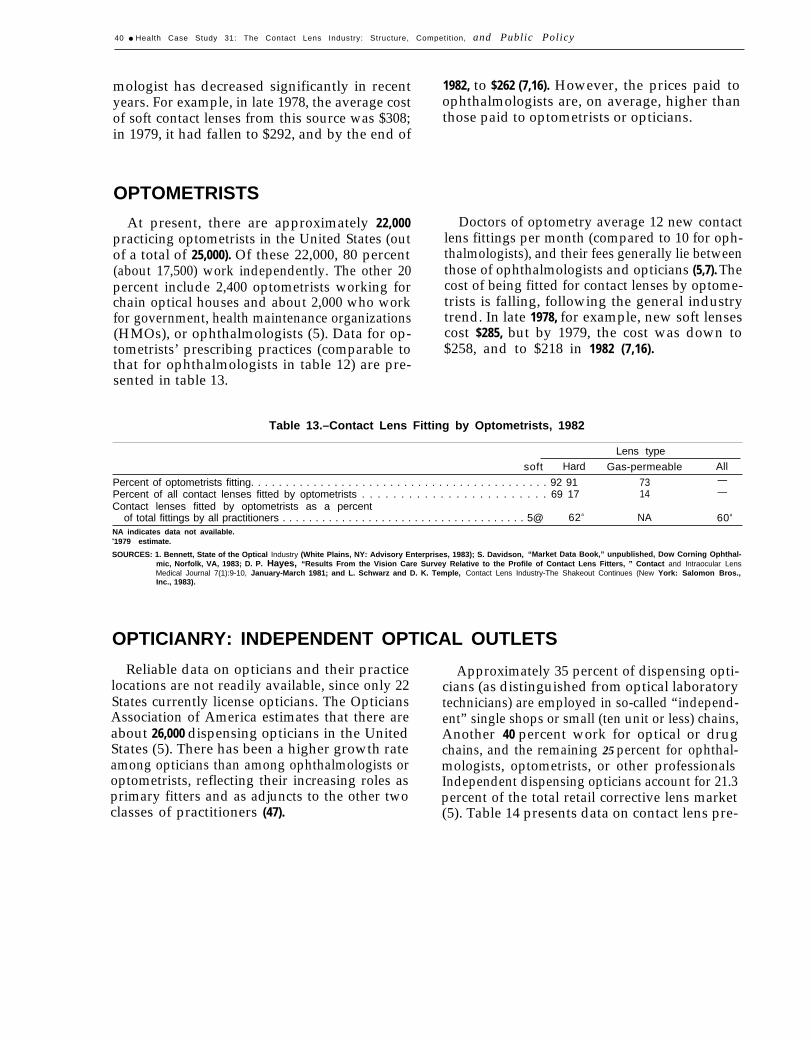
40 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
mologist has decreased significantly in recent 1982, to $262 (7,16). However, the prices paid toyears. For example, in late 1978, the average cost ophthalmologists are, on average, higher thanof soft contact lenses from this source was $308; those paid to optometrists or opticians.in 1979, it had fallen to $292, and by the end of
OPTOMETRISTS
At present, there are approximately 22,000practicing optometrists in the United States (outof a total of 25,000). Of these 22,000, 80 percent(about 17,500) work independently. The other 20percent include 2,400 optometrists working forchain optical houses and about 2,000 who workfor government, health maintenance organizations(HMOs), or ophthalmologists (5). Data for op-tometrists’ prescribing practices (comparable tothat for ophthalmologists in table 12) are pre-sented in table 13.
Doctors of optometry average 12 new contactlens fittings per month (compared to 10 for oph-thalmologists), and their fees generally lie betweenthose of ophthalmologists and opticians (5,7). Thecost of being fitted for contact lenses by optome-trists is falling, following the general industrytrend. In late 1978, for example, new soft lensescost $285, but by 1979, the cost was down to$258, and to $218 in 1982 (7,16).
Table 13.–Contact Lens Fitting by Optometrists, 1982
Lens type
soft Hard Gas-permeable All
Percent of optometrists fitting. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92 91 73Percent of all contact lenses fitted by optometrists . . . . . . . . . . . . . . . . . . . . . . . . 69 17
—14
Contact lenses fitted by optometrists as a percent—
of total fittings by all practitioners . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5@ 62a NA 60a
NA indicates data not available.a1979 estimate.
SOURCES: 1. Bennett, State of the Optical Industry (White Plains, NY: Advisory Enterprises, 1983); S. Davidson, “Market Data Book,” unpublished, Dow Corning Ophthal-mic, Norfolk, VA, 1983; D. P. Hayes, “Results From the Vision Care Survey Relative to the Profile of Contact Lens Fitters, ” Contact and Intraocular LensMedical Journal 7(1):9-10, January-March 1981; and L. Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros.,Inc., 1983).
OPTICIANRY: INDEPENDENT OPTICAL OUTLETS
Reliable data on opticians and their practicelocations are not readily available, since only 22States currently license opticians. The OpticiansAssociation of America estimates that there areabout 26,000 dispensing opticians in the UnitedStates (5). There has been a higher growth rateamong opticians than among ophthalmologists oroptometrists, reflecting their increasing roles asprimary fitters and as adjuncts to the other twoclasses of practitioners (47).
Approximately 35 percent of dispensing opti-cians (as distinguished from optical laboratorytechnicians) are employed in so-called “independ-ent” single shops or small (ten unit or less) chains,Another 40 percent work for optical or drugchains, and the remaining 25 percent for ophthal-mologists, optometrists, or other professionalsIndependent dispensing opticians account for 21.3percent of the total retail corrective lens market(5). Table 14 presents data on contact lens pre-
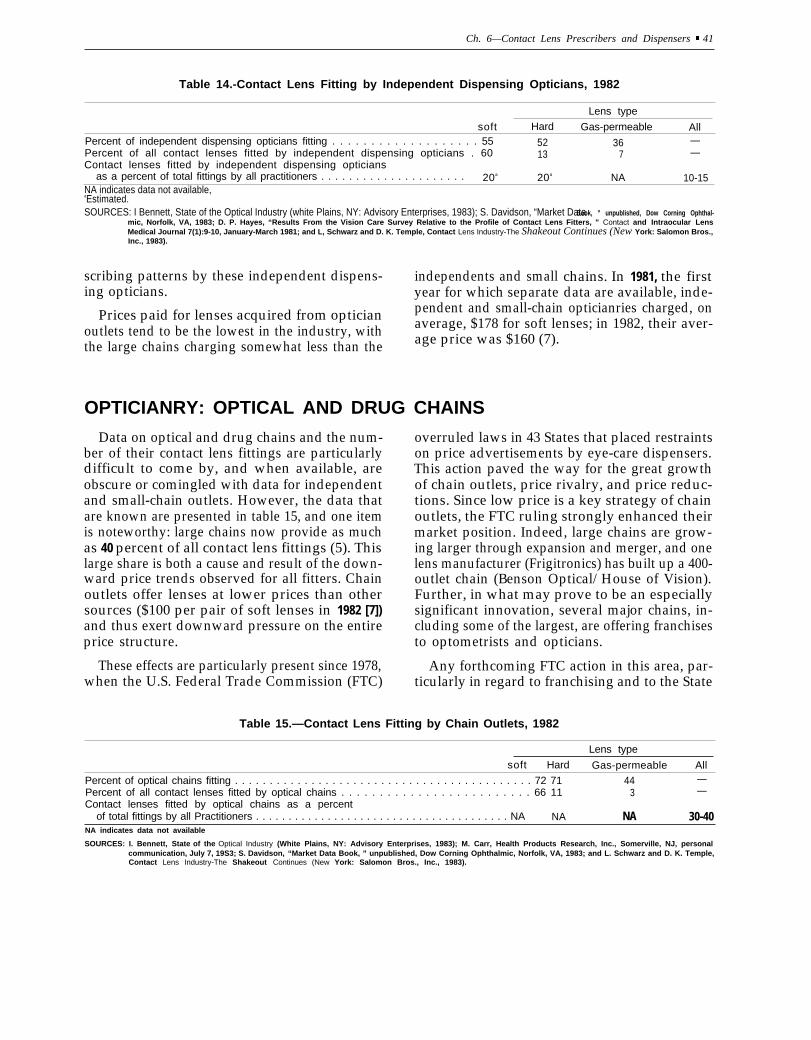
Ch. 6—Contact Lens Prescribers and Dispensers “ 41
Table 14.-Contact Lens Fitting by Independent Dispensing Opticians, 1982
Lens type
soft Hard Gas-permeable AllPercent of independent dispensing opticians fitting . . . . . . . . . . . . . . . . . . . 55 52 36Percent of all contact lenses fitted by independent dispensing opticians . 60
—13 7
Contact lenses fitted by independent dispensing opticians—
as a percent of total fittings by all practitioners . . . . . . . . . . . . . . . . . . . . . 20a 20a NA 10-15NA indicates data not available,aEstimated.SOURCES: I Bennett, State of the Optical Industry (white Plains, NY: Advisory Enterprises, 1983); S. Davidson, “Market Data Book, ” unpublished, Dow Corning Ophthal-
mic, Norfolk, VA, 1983; D. P. Hayes, “Results From the Vision Care Survey Relative to the Profile of Contact Lens Fitters, ” Contact and Intraocular LensMedical Journal 7(1):9-10, January-March 1981; and L, Schwarz and D. K. Temple, Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros.,Inc., 1983).
scribing patterns by these independent dispens- independents and smalling opticians. year for which separate
chains. In 1981, the firstdata are available, inde-
Prices paid for lenses acquired from optician pendent and small-chain opticianries charged, on
outlets tend to be the lowest in the industry, with average, $178 for soft lenses; in 1982, their aver-
the large chains charging somewhat less than the age price was $160 (7).
OPTICIANRY: OPTICAL AND DRUG CHAINS
Data on optical and drug chains and the num-ber of their contact lens fittings are particularlydifficult to come by, and when available, areobscure or comingled with data for independentand small-chain outlets. However, the data thatare known are presented in table 15, and one itemis noteworthy: large chains now provide as muchas 40 percent of all contact lens fittings (5). Thislarge share is both a cause and result of the down-ward price trends observed for all fitters. Chainoutlets offer lenses at lower prices than othersources ($100 per pair of soft lenses in 1982 [7])and thus exert downward pressure on the entireprice structure.
overruled laws in 43 States that placed restraintson price advertisements by eye-care dispensers.This action paved the way for the great growthof chain outlets, price rivalry, and price reduc-tions. Since low price is a key strategy of chainoutlets, the FTC ruling strongly enhanced theirmarket position. Indeed, large chains are grow-ing larger through expansion and merger, and onelens manufacturer (Frigitronics) has built up a 400-outlet chain (Benson Optical/House of Vision).Further, in what may prove to be an especiallysignificant innovation, several major chains, in-cluding some of the largest, are offering franchisesto optometrists and opticians.
These effects are particularly present since 1978, Any forthcoming FTC action in this area, par-when the U.S. Federal Trade Commission (FTC) ticularly in regard to franchising and to the State
Table 15.—Contact Lens Fitting by Chain Outlets, 1982
Lens type
soft Hard Gas-permeable All
Percent of optical chains fitting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 71 44Percent of all contact lenses fitted by optical chains . . . . . . . . . . . . . . . . . . . . . . . . . 66 11
—3
Contact lenses fitted by optical chains as a percent—
of total fittings by all Practitioners . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . NA NA NA 30-40NA indicates data not available
SOURCES: I. Bennett, State of the Optical Industry (White Plains, NY: Advisory Enterprises, 1983); M. Carr, Health Products Research, Inc., Somerville, NJ, personalcommunication, July 7, 19S3; S. Davidson, “Market Data Book, ” unpublished, Dow Corning Ophthalmic, Norfolk, VA, 1983; and L. Schwarz and D. K. Temple,Contact Lens Industry-The Shakeout Continues (New York: Salomon Bros., Inc., 1983).

42 ● Health Case Study 31: The Contact Lens ]ndustry: Structure, Competition, and Public Policy
laws that define the permissible limits of opticiansin the fitting of contact lenses, will exert great in-fluences on the extent and forms of competitionamong all classes of practitioners, with strong im-plications for future price structures and trends.Whatever happens, the large optical chain has be-come an important part of the contact lens dis-tribution mechanism and promises to play a largerrole in future years. In table 16, eight of the largestchains are identified, along with their presentnumber of outlets.
In conclusion, the three classes of practitionershave become more competitive with each other,particularly since 1978, when some of the limita-tions on price competition and on the role of op-ticians as independent dispensers were reduced.As a result of these changes, the total supply ofpractitioner/dispensers has expanded, and thehighlighting of price as a basis of choice has servedas one common denominator among all types ofdispensers. Increasingly, price differentials amongdispensers have come to reflect their qualitativedifferences as perceived by consumers, regardlessof whether these perceptions are borne out in factby either actual market experience or “objective”measures of dispenser “quality. ” These perceivedqualitative differentials seem to have narrowedover time, perhaps because soft lenses, which pre-dominate in the market, usually have well-knowncompany labels, and because customizing of softlenses is not widely done. With the tangible partof the combined lens/fitting rendered more homo-geneous among different types of practitioners,the remaining differences, including price, havebecome more important in the choice among prac-titioners. And with the growing influence of price,the lower prices of high-volume chain opticianries
have attracted more and more consumers andpulled down the entire contact lens price struc-ture, as described in chapter 4.
Those closest in character to the larger chains—namely, the smaller chains and independent op-ticianries—have been affected the most, with op-tometrists the next most affected, and ophthal-mologists the least but still feeling the impact. Ifboth large and small opticianries are consideredtogether, then their emphasis on price competi-tion most seriously affects optometrists. This ex-pectation is supported by the decline optometristshave experienced in their soft lens market sharefrom 60 percent in 1979 to 40 percent in 1980 (5).
Over the next several years and into the middle-run future, price competition can be expected tocontinue. The entire price structure for conven-tional contact lenses will continue to ease down-ward, at least relative to the structure of all prices.Within the contact lens retail price structure, posi-tions are not likely to change, with the chaindispensers at the bottom of the structure initiat-ing price reductions and compelling the otherdispensers, mainly small opticianries and individ-ual optometrists but even ophthalmologists, tofollow. Furthermore, these competitive pressuresin the retail market can be expected to spill overinto the manufacturers’ sector as all dispensers,led by the large chains and their expanding outletsand franchises, exert buyer pressure for lowerprices in the wholesale market. Accordingly, theentire industry, wholesale and retail, promises tobe characterized by a high degree of price com-petition along with strong rivalry in lens innova-tion in the years ahead.
Table 16.—Major Optical Chains and Number of Outlets, 1982
Chain name(s), if differentChain owner from owner Number of outletsSearle . . . . . . . . . . . . . . . . . . . . . . Pearle Vision Centers and Texas
State OpticalCole National. . . . . . . . . . . . . . . . Sears; Montgomery Ward 465Frigitronics. . . . . . . . . . . . . . . . . . Benson’s; House of Vision 400Sterling . . . . . . . . . . . . . . . . . . . . . 110Lee Optical. . . . . . . . . . . . . . . . . . 100D.O.C. . . . . . . . . . . . . . . . . . . . . . . 85Western State Optical . . . . . . . . 64American Vision Centers. . . . . . 40SOURCE: 1. Bennett, State of fhe Optical Industry (White Plains, NY: Advisory Enterprises, 1983).

Ch. 6—Contact Lens Prescribers and Dispensers ● 43
THE MARKETING OF CONTACT LENSES TO DISPENSERS
Manufacturers distribute their contact lenses tothe three groups of dispensers, who in turn makethem available to patients. Thus, manufacturers’promotional efforts are mainly directed to theseprofessionals, although some consumer-oriented,brand-name advertising takes place.
Manufacturers offer a wide and sometimes con-fusing array of marketing plans, and any givenfirm may have several programs in effect. Fur-ther, the programs are usually in a state of change,reflecting new attempts to induce dispensers torely more heavily on one brand or to fend off theaggressive programs of rivals. (Because of therange and diversity of marketing techniques, thisdiscussion will focus on those of the larger firms2
engaged in nationwide distribution, since thesmaller labs depend more on reputation and word-of-mouth promotion in their local areas to pro-mote sales. )
The larger firms often distribute lenses on a con-signment basis. Some require the dispenser to paya one-time fee per lens, others require no fee, andstill others charge prescribers an annual per-lensfee on the original lens consignment. Dispensersare generally required to keep their inventoriesat the original consignment levels and to pay forlenses as they are ordered to restock to the speci-fied level.
A common promotional practice is volume dis-counting, Manufacturers offer dispensers pricecuts if they order a certain volume of lenses, andthe discounts are often graduated and cumulative,linking dispensers increasingly closer to producersas their usage volume expands. At least one ma-jor manufacturer has offered prizes such as Mercedesautomobiles and gold bullion to practitioners forordering its lenses in large quantities.
Most manufacturers offer limited warrantiesand exchanges on their lenses. The warranties usu-
‘This discussion is drawn from Contact Lenses, 1982 (10); andvarious articles from the Contact Lens Forum, 1979-1983, providedby Patty Sposato, Associate Editor (2,18,26,32,33,35,36,37,38,39).
‘The firms discussed include: American Hydron, American Med-ical Optics, American Optical, Barnes-Hind/Hydrocurve, Bausch& Lomb, Channel/Lombart, Ciba Vision Care, Dow Coming, Paris,Syntex Ophthalmic, Vistakon, Wesley-Jessen, Salvatori Oph-thalmics.
ally apply only to material and workmanshipdefects and exclude tearing and other damagefrom use and handling. The dispensers usuallyhave 30 to 60 days to return defective lenses. Theyalso can return those lenses not suitable for a pa-tient; some firms give full credit, others partialcredit, for such returns. Many firms now also of-fer lenses with no warranty, which lowers pricesand reduces paperwork for dispensers. There isalso a general movement in the industry to sim-plify and expedite warranty procedures.
Price competition and simplified billing routinesare heavily used to promote sales. Prices havebeen dropping steadily in the industry over thepast 5 years, as described in previous chapters,and between May 1982 and May 1983 only onedaily wear lens was increased in price. Many man-ufacturers now give practitioners a choice of pric-ing methods: per lens or per fitting (“per case”),which allows for lens return. Both types of priceshave been part of the downward price trend.
Along with rivalry in price formats and pricelevels, contact lens producers are also moving into“full line” marketing strategies. The goal of thesestrategies is to entrench a brand name across thedifferent specialty markets, offering the dispenser“one-stop” shopping, so to speak. The competi-tive implications for smaller firms have not yetbecome clear. Full-line strategies are pursued incontact lens accessories as well as in the lensesthemselves as the markets for lens solutions andpractitioner aids have grown large.
To introduce prescribers and dispensers to abrand of lens, its producer may offer diagnosticlens sets free of charge or at a great discount. Thistechnique is reported to have met considerablesuccess with new practitioners.
Once a prescriber-dispenser begins to use a par-ticular type of lens, firms usually emphasize serv-ice to continue the affiliation. The larger firmsmaintain full-time customer service and sales staffsto deal with problems. They also try to anticipatepractitioners’ needs and frequently use computer-generated inventory plans for individual offices.Some firms further strengthen their relationshipswith dispensers by training the dispensers’ staffs.

44 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
Beyond thescribed abovemanufacturer
general marketing techniques de- On a more conventional scale, some smallare more unusual programs. One PMMA hard lens makers are becoming distribu-(Channel/Lombart) has offered a tors for the soft lenses made by larger firms,
one-time lens exchange program in which a prac-titioner could exchange 100 used soft or hardlenses for 100 new soft lenses at about $6 off theregular per lens price. Other firms seek goodwillthrough funding educational grants for studentor graduate practitioners, one of a variety of waysto establish the names of firms and their prod-ucts in the minds of those making selection deci-sions among competing products.
allowing the small firms to have at least some de-gree of participation in this much greater marketand allowing the larger manufacturer to expandits distributional and promotional mechanism.Wholesale-only houses are also appearing in someregions, and at least one consortium (Product De-velopment Consortium) of small firms has beenorganized to manufacture and market soft lenses.
7
The Role of Federal Policy

The Role of Federal Policy
GENERAL OVERVIEW
Federal policies affect the development, man-ufacture, distribution, and use of contact lensesthrough various paths and in varying degrees,ranging from minor to large.
Direct Federal in-house activities and externalfunding for vision-care research play only a slightrole in the operation of the contact lens industry,one of whose main benefits to consumers lies inthe cosmetic qualities of contact lenses. Similarly,tax policy may have an important effect on theindustry but not in any way that is distinct fromother industries. Features of the tax laws, particu-larly provisions for accelerated depreciation, in-vestment credits, favorable treatment for retainedcorporate earnings, and restrictions on corporatedivestitures favor larger corporations relative tosmaller ones, but the inherent features of the con-tact lens industry are compatible with small firms,and their position is not seriously threatened byany advantages provided their larger rivals throughthese tax provisions.
Foreign trade policy does not appear to ad-versely affect the contact lens industry. The tar-iff on imported contact lenses is low, 8.5 percentof value (5.6 percent for those coming from coun-tries with preferential treatment), much less than
PATENTS
For the most part, patents neither pose prob-ems nor exert special influence on the contact lensindustry. They seem to offer an acceptable bal-ance between the sometimes conflicting goals ofstimulating innovation and keeping market com-petition viable. On the one hand, they provideincentives and rewards for new product and proc-ess developments; on the other hand, they do notappear to create formidable barriers to entry. Therecord of innovation is a good one, covering a
for almost all other components of the tariff cat-egory “optical goods, ” yet imports account foronly a small share (7 percent in 1980) of total do-mestic purchases (56). (Many of the imported con-tact lenses, of course, may come from the foreign-owned enterprises of U.S. producers. )
Direct government procurement, an influentialeconomic force in many other industries, is min-imal for contact lenses, and Federal third-partypayment mechanisms, mainly Medicare and Med-icaid, pay for contact lenses only as a therapeu-tic item for aphakia and a few other ophthalmicconditions. This adds to the use of lenses for theseconditions, and probably spurs some research anddevelopment along related lines, but has little ef-fect on the much larger general market.
However, not all Federal policies are so easilydiscounted as factors influencing the contact lensindustry. Three, in particular, warrant closer ex-amination. In ascending order of impact, they are:1) patent policy; 2) policies toward the enforce-ment and maintenance of competition within mar-kets; and 3) regulatory policies that require gov-ernment approval prior to the general marketingand use of products such as drugs and medicaldevices, including contact lenses.
wide range of lens materials, many lens designsfor similar applications, and a variety of manu-facturing processes. Further, the majority of thesedevelopments are accessible to any lens producer.Other evidence shows that entry barriers frompatents are not high: upwards of three dozen firmsproduce soft lenses and over 50 make hard lenses.Although relatively few firms manufacture andsell gas-permeable lenses, the market barrier inthis case (and in some others) is not the unavail-
47
48 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
ability of materials or techniques because ofpatents, but premarket approval by the Food andDrug Administration (FDA), which will be exam-ined later in this chapter.
Patents may still be important in the contactlens industry, however, because they can reservesuperior materials, designs, and processes for oneor a few firms to the disadvantage of others.
Among the more important patents are thosederiving from Wichterle’s original work on softlenses in Czechoslovakia, for which the NationalPatent Development Corp. (NPD) obtained cer-tain rights, which were then sublicensed to Bausch& Lomb. The headstart provided by the NPDpatents on hydrogel material and the spin-castingmethod for making soft contact lenses enabledBausch & Lomb to enter the market first (1971)and remain as the sole seller of soft lenses until1975. The subsequent development of otherhydrophilic polymer plastics allowed many rivalsto get around the NPD-Wichterle product patent,and vigorous price competition has been one of
the results. However, the economical spin-castingmanufacturing process has continued to work tothe advantage of Bausch & Lomb, enabling it tooperate profitably in the face of large price de-clines.
However, neither of the original patents suc-cessfully blocked entry by others; the productpatent was quite easy to invent around and theprocess patent, although very advantageous anddurable, covers but one of several manufactur-ing methods. The resulting entry of other firmshas brought lens prices down by a considerableamount since 1975, as shown in table 7 (soft lenswholesale prices were $68.70 in 1975, but only$30 in 1982). Accordingly, patents seem to be arather noncontroversial element in the contact lensindustry. However, to remain so, they shouldcontinue to be carefully defined, affording onlythe reasonable minimum degree of exclusivitywarranted by the particular discovery or in-vention.
THE MAINTENANCE OF MARKET COMPETITION
Policies to protect competition in the marketsof the U.S. economy are administered at the Fed-eral level by the Department of Justice and theFederal Trade Commission (FTC). The two agen-cies enforce the Federal antimonopoly laws andin other ways also seek to maintain, restore, orcreate competition in society’s interest.
Two facets of the contact lens industry’sities relate to these laws and enforcement
activ-agen-
cies. The first of these is the considerable mergeractivity that has occurred up to the present time,including the acquisition of smaller firms by largerones within the industry, and of larger firms byexternal industrial corporations. Under the Clay-ton Act, mergers that may substantially lessencompetition are prohibited, and thus an exami-nation of these mergers in the context of theClayton Act is instructive.
The second link between the contact lens in-dustry and the antitrust enforcement agencies isfound in the distributional mechanism by which
lenses reach the consumer, particularly the pres-ence or absence of competition, and the forms ittakes, among dispensers. In recent years the FTChas addressed two restraints on distributioncompetition: State limitations on the competitiveopportunities for opticians, and State approvalof professional prohibitions on price competitionby lens prescribers and fitters.
Mergers
Many of the numerous mergers that have oc-curred in the contact lens industry are identifiedin appendix B. Since none of these involved theacquisition of one major producer by another(generally illegal under the Clayton Act), the ob-served degrees of market concentration, if somewhat higher than had these mergers not occurredare mostly explainable in other terms, mainly theearly phases of the typical industry life cycle.
But concentration levels are not the only basisfor judging the effect of mergers. The absorption

Ch. 7—The Role of Federal Policy “ 49
of smaller firms by larger ones threatens a majorsource of innovation. The history of the indus-try is replete with the achievements of individualscientists and small firms. For example, key con-tributions in the development of the soft lens sec-tor include those of the then-small NPD in theorigination of the product, and the later researchcontributions of such smaller firms as Milton-Roy(since acquired by Bausch& Lomb), Calcon Lab-oratories, Polymer Optics, Salvatori Ophthalmic(these last two recently have been acquired bySyntex), Rynco Scientific, Danker Laboratories,and others, none of which rank among the ma-jor firms.
State Commercial Practice Restraints
Regulation of the commercial practices of eye-care professionals occurs at the State level and hasan especially strong impact on the prices con-sumers ultimately pay for their contact lenses.
The acquisition cost of contact lenses includes,in addition to the lenses, a refraction test and lensprescription, post-refraction corneal measure-ment, trial lens fitting, and followup examinationsand care. Competition among lens manufacturershas brought the price of lenses down substantially,but lens prices are not the major component ofthe total cost of obtaining contact lenses, at leastfrom ophthalmologists and optometrists. The pre-dominant component is the professional servicesrequired to examine the eye and to choose andfit the lenses with satisfactory results. Thus thepotential gains from competition, including price,in these services considerably outweigh those fromcompetition among lens manufacturers. In fact,competition in the service component of contactlens acquisition costs has been the main contrib-utor to the price declines observed for all majorlens types.
State laws covering eye-care professionals varyfrom one class of practitioner to another, and varysharply from State to State for optometrists andopticians. Ophthalmologists, as medical special-ists, are governed by medical practices acts, whichare essentially uniform from State to State. Op-tometrists and opticians, however, are subject toother specific regulations such as those issued byState optometry boards. Generally, the regula-
tions on these two classes of practitioners coverprofessional qualifications for licensure; restric-tions on employment activities and optometricand optician outlet locations, including branching;and limitations on doing business under a tradename. Optometrists are usually more restrictedthan ophthalmologists and less restricted than op-ticians in their provision of eye-care services (55).
The greatest State-to-State variation in per-missible activities is in the case of opticians. Thesevariations, shown as they relate to the provisionof contact lenses, are given in table 17. In no Statecan opticians prescribe corrective lenses. In thefive States comprising group I, they are “expressly
Table 17.-Contact Lens Fitting by Opticians: Surveyof State Limitations (including District of Columbia)
1. States where opticians are expressly permitted to fit con-tact lenses:
Arizona North CarolinaConnecticut OhioMassachusetts
Il. States where opticians are expressly forbidden to fit con-
III
IV
tact lenses:Kansas New MexicoMissouri VermontNew Jersey
States where opticians may fit contact lenses on thedirection of or under the supervision of an ophthalmol-ogist or optometrist:
Alaska MississippiCalifornia NevadaColorado New YorkDelaware OregonFlorida South CarolinaHawaii TennesseeIllinois TexasKentucky Virginia
States where opticians may dispense contact lenses ona fully written “prescription: “
Alabama FloridaDistrict of Columbia Wyoming
V. States where law on the question is ambiguous or non-existent:
Arkansas NebraskaGeorgia New HampshireIdaho North DakotaIndiana OklahomaIowa PennsylvaniaLouisiana Rhode IslandMaine South DakotaMaryland UtahMichigan WashingtonMinnesota West VirginiaMontana Wisconsin
SOURCE: U.S. Federal Trade Commission, Bureau of Consumer Protection, StateRestrictions on Vision Care Providers: The Effects on Consumers(“Eyeglasses II”), Washington, DC, 1980.

50 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
permitted” to do post-prescription corneal meas-urements, select appropriate lenses, and completethe fitting procedure. In the five States in groupII, they are expressly forbidden to perform anyof these procedures. In the 16 States in group III,they may perform the post-prescription proce-dures “on the direction or under the supervision”of a prescribing ophthalmologist or optometrist.The four jurisdictions in group IV permit opticiansto select and fit lenses for a patient with a “fullywritten” prescription (containing both refractiontest information and post-refractive eye measure-ments) from an optometrist or ophthalmologist,and in the 22 States in group V the law is “am-biguous or nonexistent.”
An analysis of restrictions on opticians’ activi-ties raises the question of the extent to which theyare warranted as consumer protections and theextent to which they are intended to constrain thecompetition posed by opticians against ophthal-mologists and optometrists. The FTC has exam-ined these questions and has come to view manyof the restraints to be both unnecessary in termsof protecting the consumer and undesirable froma competitive point of view. (These conclusionshave been strongly challenged by both ophthal-mologic and optometric professional groups. ) Ac-cordingly, in the proposed “Eyeglasses II rule, ”the FTC staff recommended making contact lensfitting by opticians more accessible to consumers.The FTC staff did not suggest that a broad Fed-eral law supplant the individual State laws (al-though Federal law can do so) so the effects ofthe proposed rule would occur only in Stateswhere opticians can fit or dispense contact lenses.The ruling would require the initial examiner(ophthalmologist or optometrist), initial fitter(ophthalmologist, optometrist, or optician) andany subsequent fitter to provide patients withcomplete and fillable copies of their contact lensprescriptions so they could have the original orsubsequent lenses fit by opticians, if they sochoose and where the State law allows. At theend of 1983, this proposal was “on hold, ” awaiting
the FTC’s decision whether or not to take action.It may not be adopted, it may be adopted as is,or it may be adopted in expanded form (29).
Although not suggested by FTC staff, the FTCruling could supersede all State laws, widelybroadening the rules on opticians’ practices tomake them fully competitive with optometristsand more so with ophthalmologists. This type ofaction could increase competition in the market-place while allowing for due assurance of quality.The less sweeping Eyeglass II rule would achievethese results in lesser degree.
Last, the FTC has been a participant in a suc-cessful attempt to expand competition—specif-ically, price competition —in the fitting of contactlenses. State laws directly or indirectly prohibitingprice advertising by professionals have beenseverely narrowed on two grounds. First, limita-tions and sanctions imposed by professionalgroups against price advertisers invite challengeunder the antitrust laws as price-fixing agree-ments. Second, this type of restriction on ad-vertising and direct statutory prohibitions is ofdoubtful enforceability because of their apparentconflict with the rights of free speech granted bythe first amendment to the Constitution. The Su-preme Court has ruled that truthful advertisingfalls within these rights (3a, 39). Accordingly,price advertising by optical outlets has becomecommon and has generated an increased aware-ness of prices by consumers. As a result, opticaloutlets have priced their services at the lower endof the price range and have pulled down pricescharged by other contact lens providers. Amongoutlets, the large optical chain has been an espe-cially vigorous price competitor, providing softlens fittings for an average price close to $100.Thus, Federal policy, through the FTC, has con-tributed to price competition among lens care pro-viders and has the potential, through the presently
shelved Eyeglasses II rule, to create more marketalternatives and further price competition, pos-sibly in every State.

Ch. 7–The Role of Federal Policy ● 51
FDA REGULATORY POLICY
Of all the aspects of Federal policy that bearon the operation of the contact lens industry, noneis more controversial or perhaps as influential asthe requirement that soft and gas-permeable lensesbe approved by the FDA for safety and efficacyprior to general marketing. Such a requirementgenerates both benefits and costs for society. Thebenefits stem from the greater knowledge and ex-perience acquired in the proapproval laboratoryand clinical studies, which may lead to more ef-fective and safe products and their wiser use. Thecosts are broader in variety, including the re-sources expended in any proapproval studies thatotherwise might not be conducted, the impactson consumers from delayed or denied approvalof new contact lenses, and any anticompetitive im-pacts of the regulatory barrier. Ideally, premar-keting approval would impose only those coststhat are outweighed by the resulting benefits, butfor soft and gas-permeable lenses this may not bethe case. Controversy exists because the regula-tory process places* a high benefit on problemsaverted by cautious premarket testing. Producers,on the other hand, since they bear much of thecosts directly, are especially sensitive to this sideof the equation relative to the benefits. Accord-ingly, it may be inevitable that regulators and theregulated, with different perceptions of the weightsto give benefits and costs, are in conflict over theappropriate extent of regulation. In the case ofcontact lenses, FDA’s policies have remained un-changed, due largely to the complexity of the lawin effecting a lower level of regulation, and, toa lesser extent, the opposition of some firms thathave gained marketing approval for their prod-ucts under the current high standards.
The Origins, Development, and Scope ofFDA Authority Over Contact Lenses
An understanding of the economic effects andcurrent issues in the regulation of contact lensesrequires an understanding of the law itself, in-cluding a look at its origins and present features.
Prior to 1968, when only hard contact lenseswere available, there was little, if any, regulation.However, in 1968, formal regulation of contact
lenses began as a result of two factors. These werethe development of hydrophilic soft lens material,and two court cases (1,42) that established FDA’sauthority to regulate contact lenses, nylon sutures,and several other “devices” as drugs, and to sub-ject them to premarket approval requirementscomparable to those for new drugs. A medical de-vices group was set up to handle this responsi-bility, and some guidelines for contact lenses wereestablished in 1969. (The first approval underthese guidelines for soft lenses was granted toBausch & Lomb in 1971. ) In the 1976 Medical De-vices Amendments to the Federal Food, Drug, andCosmetic Act, contact lenses were specificallydefined as medical devices.
The 1976 law established three classes for allmedical devices according to the degrees of riskassociated with their uses. Class I devices are notused for sustaining human life and do not posesignificant risks to human health. Devices soclassified must be made in accordance with goodmanufacturing practices (GMPs), which includekeeping a device master file that contains designspecifications, production and quality assurancedata, control numbers and dates of manufacture,distribution information, and complaint records.
Devices placed in Class II are (somewhatunclearly) defined as those for which the “gen-eral controls” of Class I offer insufficient assuranceof safety and effectiveness, and information ex-ists for establishing “performance standards. ”Class II devices must meet the Class I standardof good manufacturing practices, as well as theClass II performance standards; but no Class IIperformance standards have been formulated, soClass II devices are, in effect, treated as Class Idevices.
Class III was established for those devices forwhich Class I controls offer inadequate protec-tion, Class II performance standards do not existdue to the absence of sufficient information, andthe device “supports life, prevents health impair-ment, or presents a potentially unreasonable riskof illness or injury.” All medical devices producedafter 1976 that are not “substantially equivalent”in intended use, safety, and effectiveness to de-

52 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
vices marketed prior to 1976 are automaticallyplaced in Class III and require FDA “premarketapproval” prior to their general distribution anduse, unless they are reclassified to a lower class.They must also meet the general controls require-ments for Class I and Class II devices.
Contact lenses were originally placed in Class111, except for hard (PMMA) lenses, which wereplaced in Class II. At the end of 1983, all lenseswith 95 percent or more PMMA were in Class II(6), and the FDA was engaged in a lengthy pro-cedure to reclassify daily-wear spherical soft lensesand rigid gas-permeable lenses to Class I (or per-haps Class II). The reclassification of rigid gas-permeable lenses was denied by FDA in Decem-ber 1983 because of inadequate, publicly avail-able data on safety and effectiveness (43).
The route for obtaining premarket approval fornew Class III devices is the Investigational DeviceExemption (IDE) process, which allows a producerto market a device on a limited scale, under con-trolled conditions, to obtain the information nec-essary for FDA evaluation. IDE guidelines areestablished by the FDA, and the study protocolsset forth by manufacturer must conform to theseguidelines.
Typically, only the large contact lens manufac-turers have performed full IDE studies from testingthe effects of the polymer on corneal tissue all theway through the actual clinical trials of the fin-ished lenses (28). Studies of this scope usually cost$1 million or more (40). Smaller makers of con-tact lenses, who usually purchase the polymer“buttons” from another source, leave tissue testingand other related studies to the polymer manu-facturer and just sponsor the clinical trials. Thesetrials usually take from 6 to 12 months and costbetween $250,000 and $350,000 (28,40).
The Effects of the Present Systemof Regulation
Regulation has had several effects on the struc-tures of contact lens markets, and the higherclassification for soft and gas-permeable lenses hascreated larger effects on them than on hard lenses.The negligible regulation of hard lens market en-try before 1969 and the modest regulation since
then have kept the barriers to entry low, explain-ing in large part why this industry sector is char-acterized by many firms, mostly small, competingin price, innovation, and service, usually on alocal basis.
In contrast, Class III status for other lens typesposes a formidable financial barrier for the smallfirm; as a result, few of them have gained a posi-tion in these markets, although a small numberhave managed to come into specialized sectors.Thus, the soft and gas-permeable lens markets arealmost wholly accounted for by large firms, manyin the case of soft lenses, only a few in the caseof gas-permeable lenses. As both sectors growrelative to hard lenses, the smaller firm may be-come less prominent in this industry. The num-ber of small producers has declined sharply, andmost of the survivors have had to steadily reducetheir output and employment levels (22,28).
Paradoxically, regulation also offers a tem-porary method of survival, which many havegrasped. Since their survival depends on beingable to market the newer, more popular lenstypes, but premarket approval is costly, manysmaller firms have capitalized on the letter, if notthe spirit, of the IDE. They have begun to pro-duce and distribute lenses for supposed “clinicalinvestigation” purposes, but really to gain atoehold in these otherwise foreclosed markets.Since IDEs initially required that clinical investiga-tions contain a minimum level of case studies butspecified no ceiling, they provided much morethan a modest level of opportunity. But even largesales under an IDE may not be profitable if fullcase files and reporting systems are maintained,thus creating an incentive, even the necessity, forsuch costly work to be foregone. The hope ofmany of these firms seems to have been to mar-ket their lenses as investigatory products exten-sively and indefinitely, with little accountabilityto the FDA as to results, or that reclassificationof soft and gas-permeable lenses would render thewhole IDE procedure moot before the time of ac-countability arrived.
Recent action by the FDA, however, may wellclose this marketing of lenses. Open-ended in-vestigational periods and data collection can nowbe halted by mandatory FDA cutoff dates for

Ch. 7–The Role of Federal Policy “ 53
these IDEs and other new criteria that firms mustfollow. In the absence of reclassification, this cut-off policy may render the small firm a minimalfactor in the new product markets.
The complex question of reclassification raisestwo important points. First, standard, provenmaterials, such as the HEMA polymer used forsoft lenses, might be reclassified to Class II or I,while newer materials could remain in Class III.In other words, reclassification could be ongoingand determined more by actual risk and less bypossible risk, as time passes, than is presently thecase. Reclassification could rely heavily on gen-eral experience-in-use of lens materials and typesas they become more commonly adopted andthereby become stronger candidates for reclas-
fsiication.
Second, the professional literature and report-ing of problems from lens use is also a contribu-tor to the diminishing role of small firms. Unlikehe case of drugs, for which a large body of inde-pendent clinical literature is generated by profes-sional sources and can be called on to supportpremarket approval applications by small mar-ket entrants, almost all clinical studies of contactroses are made by the larger manufacturers and,hus, are proprietary information not to be usedby other producers in support of their applica-tions without permission. In addition to theredundancy of effort caused by the absence of acommon base of available clinical documentation,this “ground zero” approach rewards early entryand creates for those who clear the premarket ap-proval hurdle a vested interest in keeping the bar-er high for other would-be entrants. Accord-ingly, independent professional clinical studies ofnew lens materials, designs, and uses could be en-couraged. (Although funding these studies posespractical problem, it is not an insurmountableone. One possibility is an excise tax on lenses, ear-marked specifically for clinical research purposes. )
The likely structural effects of the Class IIIpremarket approval requirement in the contactns field are fewer firms entering at a slower rate.Any entrant will be delayed; many, particularlysmall firms, may not be able to enter at all. Inrn, any effects on structure are likely to be
translated into changes in market behavior. Com-petition among fewer firms often differs from thatamong many, and competition among large firmstakes different forms than that among smallerfirms. Consequently, although price competitionmay be seen in the market for soft and gas-per-meable lenses, it may well be less than would oc-cur if smaller firms were also in these markets.The emphasis in rivalry threatens to shift increas-ingly to promotion and away from price. Verticalties between manufacturers, prescribers, andoutlets are more likely to emerge, narrowing prod-uct choice to consumers.
Smaller firms may continue to find ways to sur-vive and to create some market competition, al-though in narrower roles than the protection ofmaximum competition calls for. Operating aslicensees of other firms, especially those rankingbelow the leaders in market share, smaller firmscan increase the challenge against the dominantfirms. By acting in consortia, small firms mayeven generate a research effort. But neither theirprice nor research roles are likely to approach themagnitudes that small firms have achieved in thehard lens market and in certain specialty areas ofthe soft lens market (28,34).
Thus, the likely economic effects of FDA reg-ulatory policy toward contact lenses are not theelimination of competition or serious threats ofits large-scale curtailment, but a degree of limita-tion. What is at stake is the rigor of market com-petition. Consumers of contact lenses maybe lesswell off if small firms, which history shows to beespecially vigorous competitors in contact lens de-velopment and pricing, are constrained, becauseof limited economic resources, from entering themarket as effective rivals,
In conclusion, the study of regulatory and otherFederal policies toward contact lenses, their man-ufacturers, dispensers, and users, is instructiveboth for what it tells us about the effects of thesepolicies on the economic performance of the con-tact lens industry, and for the broader implica-tions offered about regulation in general. Eitherway, the objective is wiser and more effective Fed-eral policy determination and administration.
Appendixes
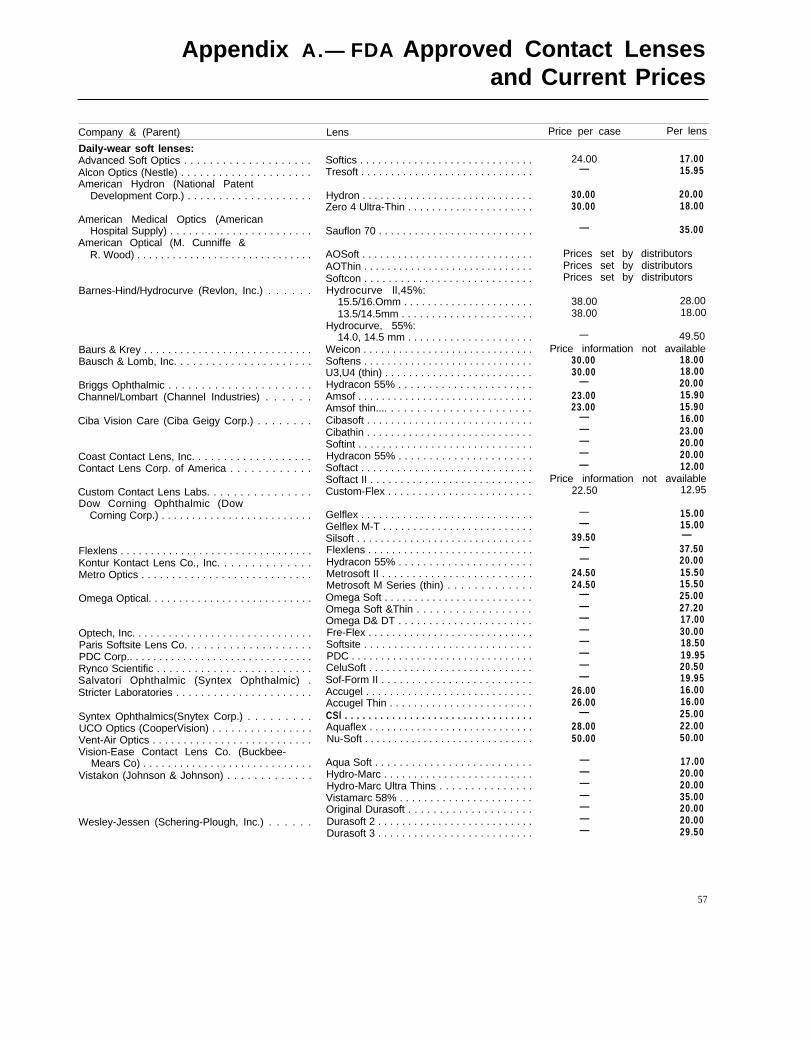
Appendix A.— FDA Approved Contact Lensesand Current Prices
Company & (Parent) Lens Price per case Per lens
Daily-wear soft lenses:Advanced Soft Optics . . . . . . . . . . . . . . . . . . . .Alcon Optics (Nestle) . . . . . . . . . . . . . . . . . . . . .American Hydron (National Patent
Development Corp.) . . . . . . . . . . . . . . . . . . . .
American Medical Optics (AmericanHospital Supply) . . . . . . . . . . . . . . . . . . . . . . .
American Optical (M. Cunniffe &R. Wood) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Barnes-Hind/Hydrocurve (Revlon, Inc.) . . . . . .
Baurs & Krey . . . . . . . . . . . . . . . . . . . . . . . . . . . .Bausch & Lomb, Inc. . . . . . . . . . . . . . . . . . . . . .
Briggs Ophthalmic . . . . . . . . . . . . . . . . . . . . . .Channel/Lombart (Channel Industries) . . . . . .
Ciba Vision Care (Ciba Geigy Corp.) . . . . . . . .
Coast Contact Lens, Inc. . . . . . . . . . . . . . . . . . .Contact Lens Corp. of America . . . . . . . . . . . .
Custom Contact Lens Labs. . . . . . . . . . . . . . . .Dow Corning Ophthalmic (Dow
Corning Corp.) . . . . . . . . . . . . . . . . . . . . . . . . .
Flexlens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Kontur Kontact Lens Co., Inc. . . . . . . . . . . . . .Metro Optics . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Omega Optical. . . . . . . . . . . . . . . . . . . . . . . . . . .
Optech, Inc. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Paris Softsite Lens Co. . . . . . . . . . . . . . . . . . . .PDC Corp.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Rynco Scientific . . . . . . . . . . . . . . . . . . . . . . . . .Salvatori Ophthalmic (Syntex Ophthalmic) .Stricter Laboratories . . . . . . . . . . . . . . . . . . . . . .
Syntex Ophthalmics(Snytex Corp.) . . . . . . . . .UCO Optics (CooperVision) . . . . . . . . . . . . . . . .Vent-Air Optics . . . . . . . . . . . . . . . . . . . . . . . . . .Vision-Ease Contact Lens Co. (Buckbee-
Mears Co) . . . . . . . . . . . . . . . . . . . . . . . . . . . .Vistakon (Johnson & Johnson) . . . . . . . . . . . . .
Wesley-Jessen (Schering-Plough, Inc.) . . . . . .
Softics . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tresoft . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Hydron . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Zero 4 Ultra-Thin . . . . . . . . . . . . . . . . . . . . .
Sauflon 70 . . . . . . . . . . . . . . . . . . . . . . . . . .
AOSoft . . . . . . . . . . . . . . . . . . . . . . . . . . . . .AOThin . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Softcon . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hydrocurve ll,45%:
15.5/16.Omm . . . . . . . . . . . . . . . . . . . . . .13.5/14.5mm . . . . . . . . . . . . . . . . . . . . . .
Hydrocurve, 55%:14.0, 14.5 mm . . . . . . . . . . . . . . . . . . . . .
Weicon . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Softens . . . . . . . . . . . . . . . . . . . . . . . . . . . . .U3,U4 (thin) . . . . . . . . . . . . . . . . . . . . . . . . .Hydracon 55% . . . . . . . . . . . . . . . . . . . . . .Amsof . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Amsof thin.... . . . . . . . . . . . . . . . . . . . . . .Cibasoft . . . . . . . . . . . . . . . . . . . . . . . . . . . .Cibathin . . . . . . . . . . . . . . . . . . . . . . . . . . . .Softint . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hydracon 55% . . . . . . . . . . . . . . . . . . . . . .Softact . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Softact II . . . . . . . . . . . . . . . . . . . . . . . . . . .Custom-Flex . . . . . . . . . . . . . . . . . . . . . . . .
Gelflex . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Gelflex M-T . . . . . . . . . . . . . . . . . . . . . . . . .Silsoft . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Flexlens . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hydracon 55% . . . . . . . . . . . . . . . . . . . . . .Metrosoft II . . . . . . . . . . . . . . . . . . . . . . . . .Metrosoft M Series (thin) . . . . . . . . . . . . .Omega Soft . . . . . . . . . . . . . . . . . . . . . . . . .Omega Soft &Thin . . . . . . . . . . . . . . . . . .Omega D& DT . . . . . . . . . . . . . . . . . . . . . .Fre-Flex . . . . . . . . . . . . . . . . . . . . . . . . . . . .Softsite . . . . . . . . . . . . . . . . . . . . . . . . . . . .PDC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CeluSoft . . . . . . . . . . . . . . . . . . . . . . . . . . . .Sof-Form II . . . . . . . . . . . . . . . . . . . . . . . . .Accugel . . . . . . . . . . . . . . . . . . . . . . . . . . . .Accugel Thin . . . . . . . . . . . . . . . . . . . . . . . .CSl . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Aquaflex . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nu-Soft . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aqua Soft . . . . . . . . . . . . . . . . . . . . . . . . . .Hydro-Marc . . . . . . . . . . . . . . . . . . . . . . . . .Hydro-Marc Ultra Thins . . . . . . . . . . . . . . .Vistamarc 58% . . . . . . . . . . . . . . . . . . . . . .Original Durasoft . . . . . . . . . . . . . . . . . . . .Durasoft 2 . . . . . . . . . . . . . . . . . . . . . . . . . .Durasoft 3 . . . . . . . . . . . . . . . . . . . . . . . . . .
24.00 17.00— 15.95
30.00 20.0030.00 18.00
— 35.00
Prices set by distributorsPrices set by distributorsPrices set by distributors
38.00 28.0038.00 18.00
— 49.50Price information not available
30.00 18.0030.00 18.00
— 20.0023.00 15.9023.00 15.90
— 16.00— 23.00— 20.00— 20.00— 12.00
Price information not available22.50 12.95
— 15.00— 15.00
39.50 —— 37.50— 20.00
24.50 15.5024.50 15.50
— 25.00— 27.20— 17.00— 30.00— 18.50— 19.95— 20.50— 19.95
26.00 16.0026.00 16.00
— 25.0028.00 22.0050.00 50.00
— 17.00— 20.00— 20.00— 35.00— 20.00— 20.00— 29.50
57
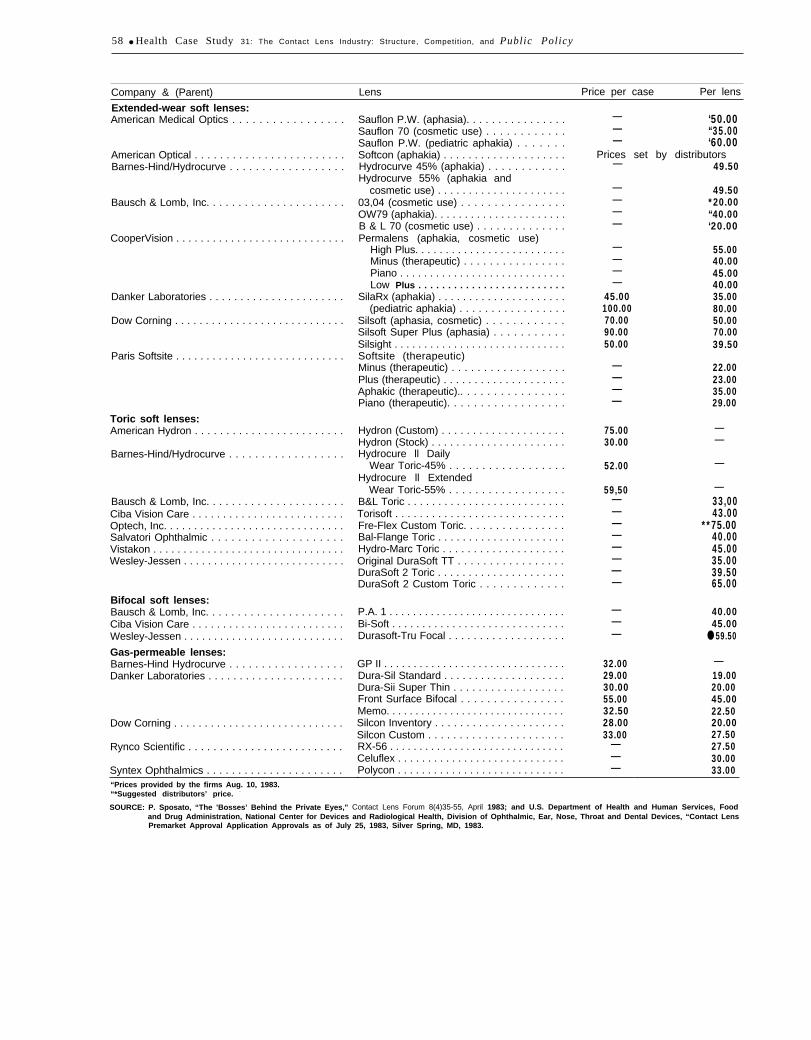
58 ● Health Case Study 31: The Contact Lens Industry: Structure, Competit ion, and Public Policy
Company & (Parent) Lens Price per case Per lens
Extended-wear soft lenses:American Medical Optics . . . . . . . . . . . . . . . . .
American Optical . . . . . . . . . . . . . . . . . . . . . . . .Barnes-Hind/Hydrocurve . . . . . . . . . . . . . . . . . .
Bausch & Lomb, Inc. . . . . . . . . . . . . . . . . . . . . .
CooperVision . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Danker Laboratories . . . . . . . . . . . . . . . . . . . . . .
Dow Corning . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Paris Softsite . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Toric soft lenses:American Hydron . . . . . . . . . . . . . . . . . . . . . . . .
Barnes-Hind/Hydrocurve . . . . . . . . . . . . . . . . . .
Bausch & Lomb, Inc. . . . . . . . . . . . . . . . . . . . . .Ciba Vision Care . . . . . . . . . . . . . . . . . . . . . . . . .Optech, Inc. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Salvatori Ophthalmic . . . . . . . . . . . . . . . . . . . .Vistakon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Wesley-Jessen . . . . . . . . . . . . . . . . . . . . . . . . . . .
Bifocal soft lenses:Bausch & Lomb, Inc. . . . . . . . . . . . . . . . . . . . . .Ciba Vision Care . . . . . . . . . . . . . . . . . . . . . . . . .Wesley-Jessen . . . . . . . . . . . . . . . . . . . . . . . . . . .
Gas-permeable lenses:Barnes-Hind Hydrocurve . . . . . . . . . . . . . . . . . .Danker Laboratories . . . . . . . . . . . . . . . . . . . . . .
Dow Corning . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Rynco Scientific . . . . . . . . . . . . . . . . . . . . . . . . .
Syntex Ophthalmics . . . . . . . . . . . . . . . . . . . . . .
Sauflon P.W. (aphasia). . . . . . . . . . . . . . . .Sauflon 70 (cosmetic use) . . . . . . . . . . . .Sauflon P.W. (pediatric aphakia) . . . . . . .Softcon (aphakia) . . . . . . . . . . . . . . . . . . . .Hydrocurve 45% (aphakia) . . . . . . . . . . . .Hydrocurve 55% (aphakia and
cosmetic use) . . . . . . . . . . . . . . . . . . . . .03,04 (cosmetic use) . . . . . . . . . . . . . . . .OW79 (aphakia). . . . . . . . . . . . . . . . . . . . . .B & L 70 (cosmetic use) . . . . . . . . . . . . . .Permalens (aphakia, cosmetic use)
High Plus. . . . . . . . . . . . . . . . . . . . . . . . .Minus (therapeutic) . . . . . . . . . . . . . . . .Piano . . . . . . . . . . . . . . . . . . . . . . . . . . . .Low Plus . . . . . . . . . . . . . . . . . . . . . . . . .
SilaRx (aphakia) . . . . . . . . . . . . . . . . . . . . .(pediatric aphakia) . . . . . . . . . . . . . . . . .
Silsoft (aphasia, cosmetic) . . . . . . . . . . . .Silsoft Super Plus (aphasia) . . . . . . . . . . .Silsight . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Softsite (therapeutic)Minus (therapeutic) . . . . . . . . . . . . . . . . . .Plus (therapeutic) . . . . . . . . . . . . . . . . . . . .Aphakic (therapeutic).. . . . . . . . . . . . . . . .Piano (therapeutic). . . . . . . . . . . . . . . . . .
Hydron (Custom) . . . . . . . . . . . . . . . . . . . .Hydron (Stock) . . . . . . . . . . . . . . . . . . . . . .Hydrocure ll Daily
Wear Toric-45% . . . . . . . . . . . . . . . . . .Hydrocure ll Extended
Wear Toric-55% . . . . . . . . . . . . . . . . . .B&L Toric . . . . . . . . . . . . . . . . . . . . . . . . . .Torisoft . . . . . . . . . . . . . . . . . . . . . . . . . . . .Fre-Flex Custom Toric. . . . . . . . . . . . . . . .Bal-Flange Toric . . . . . . . . . . . . . . . . . . . . .Hydro-Marc Toric . . . . . . . . . . . . . . . . . . . .Original DuraSoft TT . . . . . . . . . . . . . . . . .DuraSoft 2 Toric . . . . . . . . . . . . . . . . . . . . .DuraSoft 2 Custom Toric . . . . . . . . . . . . .
P.A. 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Bi-Soft . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Durasoft-Tru Focal . . . . . . . . . . . . . . . . . . .
GP II . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dura-Sil Standard . . . . . . . . . . . . . . . . . . . .Dura-Sii Super Thin . . . . . . . . . . . . . . . . . .Front Surface Bifocal . . . . . . . . . . . . . . . .Memo. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Silcon Inventory . . . . . . . . . . . . . . . . . . . . .Silcon Custom . . . . . . . . . . . . . . . . . . . . . .RX-56 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Celuflex . . . . . . . . . . . . . . . . . . . . . . . . . . . .
— ‘50.00— “35.00— ‘60.00
Prices set by distributors—
————
————
45.00100.0070.0090.0050.00
————
75.0030.00
52.00
59,50————————
———
32.0029.0030.0055.0032.5028.0033.00
———Polycon . . . . . . . . . . . . . . . . . . . . . . . . . . . .
“Prices provided by the firms Aug. 10, 1983.
49.50
49.50*20.00“40.00‘20.00
55.0040.0045.0040.0035.0080.0050.0070.0039.50
22.0023.0035.0029.00
——
—
—33,0043.00
**75.0040.0045.0035.0039.5065.00
40.0045.00
● 59.50
—19.0020.0045.0022.5020.0027.5027.5030.0033.00
“*Suggested distributors’ price. -
SOURCE: P. Sposato, “The ’Bosses’ Behind the Private Eyes," Contact Lens Forum 8(4)35-55, April 1983; and U.S. Department of Health and Human Services, Foodand Drug Administration, National Center for Devices and Radiological Health, Division of Ophthalmic, Ear, Nose, Throat and Dental Devices, “Contact LensPremarket Approval Application Approvals as of July 25, 1983, Silver Spring, MD, 1983.

Appendix B.— Major Contact Lens Manufacturers,Methods of Entry, and Acquisitions
and License Agreements
Bausch & Lomb
Method of entry: Entered de novo in daily-wear softlenses in 1971, using exclusive licenses obtained fromNational Patent Development Corp. (NPD) in 1966 toproduce and sell soft lenses made of basic hydrophilicpolymer developed in Czechoslovakia and to use spin-casting production method also developed in Czech-oslovakia.
Acquisitions: Bausch & Lomb acquired design fortoric soft lenses from Milton Roy Co. when that firmwent out of business in 1979 and sold its manufactur-ing facilities to Bausch & Lomb. Recently acquiredworldwide rights to two soft lens tinting processesfrom Leroy Meshel, M. D., of California. In October1983 Bausch & Lomb acquired Polymer TechnologyCorp., a maker of gas-permeable lens material and lenscare solutions.
Revlon (Barnes= Hind/Hydrocurve)
Method of entry: Acquired number three firm incontact lens industry, Continuous Curve, in August1980.
Other acquisitions: Acquired Coburn Optical Indus-tries (1975), maker of plastic and glass eyeglass lensesand interocular lenses. In 1976 acquired Barnes-HindPharmaceutical, major producer of lens care prod-ucts. Continuous Curve and Barnes-Hind operationscombined to form Barnes-Hind/ Hydrocurve. Revlonhas been licensed by National Patent DevelopmentCorp. (NPD) to manufacture and sell soft lenses, afterNPD’s successful suit for patent infringement in 1982.
CooperVision(controlled by Cooper Laboratories)
Method of entry: Entered de novo. Created fromformerly wholly owned subsidiary of Cooper Labs in1980.
Acquisitions: In June 1983, acquired UCO Opticsfrom Union Corp., giving CooperVision 15 percent ofoverall soft lens market and number two position inindustry. Before acquisition CooperVision had 8 per-cent of market and was tied for number four positionwith American Hydron; UCO Optics had 7 percentand was ranked number five. In 1980, acquired Smith,Miller & Patch and Flow Pharmaceuticals from Cooper
1 Parent company is listed first and acquired companies are in italics.
Labs; also acquired Global Vision, a soft lens maker,from Cooper Labs. In 1981, bought C.V. Labs Ltd.,a British lens manufacturer, and International LensCorp., which holds patents on cast molding lens man-ufacturing process.
Syntex Corp. (Syntex Ophthalmic)
Method of entry: Acquired Polymer Optics, makerof the polycon gas-permeable lens, in 1977.
Acquisitions: In November 1978 acquired CornealSciences, Inc., maker of soft lenses. In May 1983 ac-quired Salvatori Ophthalmics, maker of soft lenses,obtaining a daily wear lens, and extended wear andbifocal lenses then in FDA approval process. Prior tothis acquisition, Syntex had daily wear and gas-permeable lenses only, and was developing toric andbifocal lenses.
National Patent Development Corp.(American Hydron)
Method of entry: Entered de novo. Companyformed by NPD in 1978.
Acquisitions: Acquired original patents for soft lenshydrophilic polymer and spin-casting productionmethod from Czechoslovakian Academy of Science in1964. Sublicensed Bausch& Lomb to manufacture softlenses by spin-cast method. Has reacquired some rightsto make soft lenses via spin-casting, and some rightsto the cast molding process through partial acquisi-tion of international Lens Corp. stock in 1973. Inter-national Lens subsequently bought by CooperVision.American Hydron has entered joint ventures withFrench, Japanese, Canadian, and English firms to mar-ket products in those countries. As a result of suc-cessful infringement suits, NPD receives an 8 percentroyalty on lens sales from Revlon, Johnson & Johnson(Vistakon), Ciba-Geigy, Nestle (Alcon), Channel-Lombart, Schering-Plough (Wesley-Jessen), and Amer-ican Optical. Also has a joint venture (1983) withAmerican Hospital Supply (American Medical Optics)to develop extended-wear soft lens.
Schering-Plough (Wesley-Jessen)
Method of entry: Acquired Wesley-lessen in 1980,number seven in industry at that time.
Other acquisitions: None.
59

60 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Publ ic Po l icy
American Hospital Supply(American Medical Optics)
Method of entry: Acquired Heyer-Schulte in 1974,Created American Medical Optics around contact lenstechnology acquired from Heyer-Schulte.
Other acquisitions: Sauflon International in 1978.Joint venture with NPD in 1983 to develop extendedwear lens. Majority of current sales are to Bausch &Lomb, which markets American Medical Optics’extended-wear lens for aphakic and cosmetic use.
Ciba-Geigy Corp. (Ciba Vision Care)
Method of entry: Formed joint venture with Titmus-Eurocon (West Germany), Europe’s largest maker ofcontact lenses, to sell Titmus-Eurocon products in theUnited States (1980). In 1983, Ciba-Geigy Corp. pur-chased Titmus-Eurocon.
Other acquisitions: None.
Johnson & Johnson (Vistakon)
Method of entry: Acquired Frontier Contact Lenses(now Vistakon) in 1981. Frontier Contact Lensesranked ninth in soft lenses market at time of acqui-sition.
Other acquisitions: Purchased Iolab Corp., a makerof interocular lenses.
Danker Laboratories
Method of entry: Entered de novo (1958). Companymakes hard and gas-permeable lenses only.
Acquisitions: Purchased hard lens and solutionsbusiness from Milton Roy in 1979. May have acquiredsome technology in gas-permeable lenses through thisacquisition.
Dow Corning(Dow Corning Ophthalmic)
Method of entry: Purchase of lens technology fromBreger in 1972. Dow Corning itself is a joint ventureof Dow Chemical Corp. and Corning Glass; createdDow Corning Ophthalmic to market silicone contactlenses.
Acquisitions: Calcon Labs (1978); thereby obtain-ing Gelflex, the material used in daily-wear lensesmade by Dow Corning. (Currently suing Danker Lab-oratories for patent infringement as a result of latter’sintroduction of 100 percent silicone lenses. )
Channel- Lombart
Method of entry: Acquired Lombart Lenses, largestmaker of hard lenses, from American Sterilizer Corp.in 1982.
Other acquisitions: None.
Rynco Scientific
Method of entry: Entered de novo in 1962. Producemostly gas-permeable lenses; may also make hardlenses.
Acquisitions: Three, perhaps four small lens man-ufacturers. CAB (cellulose acetate butyrate) gas-permeable technology may have come from these ac-quisitions.
Maurice Cunniffe and Rudolf Wood(American Optical Co.)
Method of entry: Acquired American Optical Co.in 1982 from Warner-Lambert Corp.
Other acquisitions: American Optical and then-parent Warner-Lambert were licensed for 17 years, be-ginning in 1973, to make and sell soft contact lensesof material developed by Frigitronics, Inc. Warner-Lambert paid royalties to Frigitronics. When Ameri-can Optical was sold to Cunniffe and Wood, Frigi-tronics would not allow Warner-Lambert to automat-ically transfer licenses to new owners. Until this disputeis settled, American Optical will act as a contractorto Warner-Lambert, who will continue to be respon-sible to Frigitronics for royalties. Warner-Lambert alsois paying 8 percent royalties to NPD.
Frigitronics
Method of entry: Hard lenses—acquisition of Pre-cision-Cosmet Co. in 1969; soft lenses—acquisition ofGriffin Labs (now Frigi-Griffen labs) in 1971. Frigi-tronics markets both hard and soft lenses throughPrecision-Cosmet Co.
Other acquisitions: In 1980 acquired Custom Con-tact Lens Lab, maker of hard contact lenses. Someother firms also acquired, possible makers of contactlenses. Also acquired Bensons (1969) and House of Vi-sion (1982), two optical chains, with a combined totalof 400 outlets.
Nestle (Alcon)
Method of entry: Acquired Alcon in 1977.Other acquisitions: Burton Parsons & Co., a maker

App. B—Major Contact Lens Manufacturers, Methods of Entry, and Acquisitions and License Agreements ● 61
of lens care products (1979) and Scanlens, a Swedish Manns, A., Bausch& Lomb, Inc., Rochester, NY, let-contact lens maker (1982). ter and data packet, July 15 and Nov. 23, 1983.
Moody’s Industrial Manual, 1982, vols. 1 and 2 (NewSources York: Moody’s Investor Service, 1982).
Schwarz, L., and Temple, D. K., Contact Lens In-Contact Lenses, Vision Press International, Sylmar, dustry-Shakeout Continues (New York: Salo-
CA, May 1982. mon Bros., Inc., 1983).Davidson, S., “Market Data Book,” unpublished, Dow
Corning Ophthalmic, Norfolk, VA, 1983.

Appendix C.— Glossary of Terms and Acronyms
Glossary of Terms
Aphakia: The absence of the crystalline lens of the eye,commonly due to the surgical removal of lenscataracts. Aphakia is usually an age-related condi-tion in which the lens transparency is lost. Theresulting opaque quality of the lens may diminishvision to light perception only, necessitating surgicalintervention.
Astigmatism: A defect of vision usually caused by ir-regular conformation of the cornea of the eye,because of which light rays fail to meet at a singlefocal point, resulting in a lack of sharpness or even-ness of focus.
Bifocal lenses: Eyeglass or contact lenses divided intotwo separate focal lengths for near and far vision.
Contact lens: A ground or molded lens of glass orplastic that fits over the corneal portion or moreof the scleral surface of the eye, for the purpose ofcorrecting vision problems or for protection.
Cornea: A clear, central portion of the sclera, whichserves as the first element in the light focusingsystem of the eye.
Corneal ulcers: Pits, perforations, or other lesions ofthe cornea.
Gas-permeable lenses: Contact lenses made of mate-rials through which gases can penetrate so that ox-ygen can reach the underlying cornea.
Extended-wear lenses: Contact lenses that can be wornfor an extended period (e.g., 1 month) because ofbeing made of gas-permeable materials or otherwiseconstructed so that oxygen can reach the underly-ing cornea.
Hard lenses: Contact lenses made of rigid, non-gas-permeable plastic materials.
Hydrogel (hydrophilic material): Highly water-absorb-ent, plastic material from which most soft lenses aremade. The most commonly used of these materialsis hydroxyethylmethacrylate (HEMA).
Hypermetropia: Same as hyperopia.Hyperopia: Farsightedness; a condition in which visual
images come to a focus behind the retina, resultingespecially in defective vision of near objects.
Intraocular lens: A lens implanted in the eye to replacethe natural lens removed during cataract surgery.
Keratoconus: A pathological condition of the eye inwhich the cornea becomes distended into a conicalor nipple shape.
Monovision: A sight difficulty in one eye only.Myopia: Nearsightedness; a condition in which the
visual images come to a focus in front of the retina,resulting especially in defective vision of distantobjects.
Photo-chromatic lenses: Eyeglass lenses that brighten
62
or darken in response to changes in the availablesurrounding light.
Polymer: A large molecule consisting of a chain ofsmall molecules. Most contact lenses are made frompolymer plastics.
Presbyopia: Inelasticity of the lens, which causes dif-ficulty in the viewing of near objects. The condi-tion usually is age related, beginning normallyaround 45 and continuing until about 70, when itlevels off.
Refractive disorders: Conditions of the eye in whichthe light-bending properties do not provide for clearfocusing. Most common among these conditions aremyopia (nearsightedness), hypermetropia (farsighted-ness), and astigmatism.
Retina: A thin tissue consisting of several layers ofcells, which contains the light-receptor cells thatallow the sense of sight.
Sclera: The elastic coating of connective tissues thatcovers the eye, including the “white” of the eye.
Single-vision disorder: Hypermetropia, myopia, andother disorders that involve only one type of visiondifficulty, rather than presbyopia, which involvesdifficulties with both near and far vision.
Soft lenses: Contact lenses made of water-absorbingmaterials. They are more comfortable to wearbecause of flexibility and gas-permeability, butrelatively more difficult to handle and of poorer op-tical quality than hard lenses.
Spin-casting: A technique for manufacturing contactlenses, in which the lens material, in soft form, isplaced in a cup-like mold, and the desired lens cur-vatures are achieved by spinning the mold at an ap-propriate speed.
Toric lenses: Contact lenses used to correct for unevenfocusing of the eye due to corneal abnormalities.
Trachoma: A chronic, contagious conjunctivitis char-acterized by the presence of inflammatory granula-tions on the conjunctival surfaces (the mucousmembrane covering the inner surface of the eyelid).These granulations eventually are replaced by scartissue.
Glossary of Acronyms
CAB —cellulose acetate butyrateFDA —Food and Drug Administration, U.S. De-
partment of Health and Human ServicesFTC —Federal Trade CommissionHEMA —hydroxyethylmethacrylateIDE —investigational device exemption by FDANPD —National Patent Development Corp.PMMA —polymethylmethacrylate

Appendix D. —Acknowledgments andHealth Program Advisory Committee
This case study has benefited from the advice and review of several people in addition to the advisory panel.The staff would like to express its appreciation to the following people for their valuable guidance:
Constance W. Atwell Daniel J. ManelliNational Institutes of Health Thompson & MitchellDepartment of Health and Human Services Washington, DCBethesda, MD
Neal J. BaileyContact Lens ForumColumbus, OH
James W. Clark, Jr.American Optometric AssociationWashington, DC
J. Richard CroutBoehringer-Mannheim Corp.Rockville, MD
Oliver H. Dabezies, Jr.Contact Lens Association of Ophthalmologists,
Inc.New Orleans, LA
Scott C. DavidsonDow Corning OphthalmicNorfolk, VA
Margaret J. GianniniVeterans AdministrationWashington, DC
Melinda HattonAmerican Academy of OphthalmologyWashington, DC
George K. MeszarosCapitol Contact Lenses, Inc.Kensington, MD
Peter O. SafirContact Lens InstituteWashington, DC
Lorraine SchwarzSalomon Brothers, Inc.New York, NY
Patty SposatoContact Lens ForumColumbiana, OH
Norman E. WallisInternational Association of Boards of Examiners
in Optometry, Inc.Washington, DC
Ann M. WittOffice of General CounselFood and Drug AdministrationDepartment of Health and Human ServicesRockville, MD
Thomas O. HenteleffContact Lens InstituteWashington, DC
63
64 ● Health Case Study 31: The Contact Lens Industry: structure, Competition, and Public Policy
HEALTH PROGRAM ADVISORY COMMITTEE
Sidney S. Lee, Committee ChairPresident, Milbank Memorial Fund
New York, NY
Stuart H. Altman*DeanFlorence Heller SchoolBrandeis UniversityWaltham, MAH. David BantaDeputy DirectorPan American Health OrganizationWashington, DCCarroll L. Estes**ChairDepartment of Social and Behavioral SciencesSchool of NursingUniversity of California, San FranciscoSan Francisco, CARashi FeinProfessorDepartment of Social Medicine and Health PolicyHarvard Medical SchoolBoston, MAHarvey V. FinebergDeanSchool of Public HealthHarvard UniversityBoston, MAMelvin A. Glasser***DirectorHealth Security Action CouncilCommittee for National Health InsuranceWashington, DCPatricia KingProfessorGeorgetown Law CenterWashington, DCJoyce C. LashofDeanSchool of Public HealthUniversity of California, BerkeleyBerkeley, CA
Alexander LeafProfessor of MedicineHarvard Medical SchoolMassachusetts General HospitalBoston, MAMargaret Mahoney****PresidentThe Commonwealth FundNew York, NYFrederick MostellerProfessor and ChairDepartment of Health Policy and ManagementSchool of Public HealthHarvard UniversityBoston, MANorton NelsonProfessorDepartment of Environmental MedicineNew York University Medical SchoolNew York, NYRobert OseasohnAssociate DeanUniversity of Texas, San AntonioSan Antonio, TXNora PioreSenior AdvisorThe Commonwealth FundNew York, NYMitchell Rabkin*PresidentBeth Israel HospitalBoston, MADorothy P. RiceRegents LecturerDepartment of Social and Behavioral SciencesSchool of NursingUniversity of California, San FranciscoSan Francisco, CA
*Until April 1983. **Until March 1984.***until October 1983.****Until August 1983.
App. D—Acknowledgments and Health Program Advisory Committee “ 65
Richard K. RiegelmanAssociate ProfessorGeorge Washington UniversitySchool of MedicineWashington, DCWalter L. RobbVice President and General ManagerMedical Systems OperationsGeneral Electric Co.Milwaukee, WI
Frederick C. RobbinsPresidentInstitute of MedicineWashington, DCRosemary StevensProfessorDepartment of History and Sociology of ScienceUniversity Of PennsylvaniaPhiladelphia, PA
———.
References
1.
2.
3.
3a.4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
.4.
5.
6.
7.
8.
AMP, Inc. v. Gardner, 389 F. 2d 825(1968); cert.denied 393 U.S. 825 (1968).“A Battle With the Chains for Contact Lens Pa-tients, ” Contact Lens Forum 7(10):45-51, October1982.Aquavella, J. V. and Gulapali, N. R., “WhichLens: Contact Lenses Currently Available for Ex-tended Wear in Aphakia,” Ophthalmology 87(2):151-54, February 1980.Bates v. State Bar of Arizona, 1979.Beatty, K., Health Care Financing Administra-tion, Baltimore, MD, personal communication,July 6, 1983.Bennett, I., State of the Optical Industry (WhitePlains, NY: Advisory Enterprises, 1983).Brown, D., U.S. Department of Health andHuman Services, Food and Drug Administration,Division of Ophthalmic, Ear, Nose, Throat andDental Devices, Silver Spring, MD, personalcommunication, Aug. 3, 1983.Carr, M., Health Products Research, Inc., Somer-ville, NJ, personal communication, July 7, 1983.Check, W. A., “Contact!” Health 14(9):20-22,September 1982.“Contact Lenses, ’f Consumer Reports 45(5):288-292, May 1980.Contact Lenses, Vision Press International, Sylmar,CA, May 1982.Davidson, S., Dow Corning Ophthalmic, Nor-folk, VA, personal communication, July 15, 1983.Davidson, S., “Market Data Book,” unpublished,Dow Corning Ophthalmic, Norfolk, VA, 1983.Dixon, J. M., “Twenty Years and Twenty Thou-sand Contact Lens Patients, ” Transactions of theAmerican Ophthalmological Society 79:65-72,1982.Feldman, G. L., “Contact Lens Materials, ” Com-plications of Contact Lenses, D. Miller and P. F.White (eds. ) (Boston, MA: Little, Brown, 1981).Graham, R., “Historical Development, ” ContactLens Practice, 3d cd., R. B. Mandell (cd.) (Spring-field, IL: Charles C. Thomas, 1981).Hayes, D. P., “Results From the Vision CareSurvey Relative to the Profile of Contact Lens Fit-ters," Contact and Intraocular Lens Medical Jour-nal 7(1):9-10, January-March 1981.Hollander, R., U.S. Department of Health andHuman Services, Public Health Service, Rock-ville, MD, personal communication, June 30,1983.“Keeping Posted, ” Contact Lens Forum 8(4):7,April 1983.
19.
20.
21.
22.
23,
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
Kersley, H. J., “Contact Lenses—Is There Prog-ress?” Practitioner 224 (1344):614-20, June 1980.Krezanoski, J. Z., “A New Look at Soft Lensesand Their Solutions, ” Amer. Pharmacy NS21(5):12-19, May 1981.Lowther, G. E., Contact Lenses: Procedures andTechniques (Boston, MA: Butterworths, 1982).Manelli, D., Contact Lens Manufacturers Asso-ciation, Washington, DC, personal communica-tion, June 7, 1983.Manns, A., Bausch& Lomb, Inc., Rochester, NY,letter and data packet, July 15, 1983.Manns, A., Bausch& Lomb, Inc., Rochester, NY,letter, Nov. 23, 1983.Moody’s Industrial Manual, 1982, vols. 1 and 2(New York: Moody’s Investor Service, 1982).“More About Contacts on Consignment, ” Con-tact Lens Forum 4(8):27-39, August 1979.Morrison, R. J., “Contact Lens Materials—AnOverview,” J. Amer. Optometric Assoc. 47(3):298, March 1976.Platt, W., President, Platt Contact Lens Service,Mt. Vernon, OH, personal communication, Aug.3, 1983.Pollard, M., U.S. Federal Trade Commission,Washington, DC, personal communications, June16 and July 27, 1983.Ruben, M., Contact Lens Practice (Baltimore,MD: The Williams & Wilkens Co., 1976).Schwarz, L., and Temple, D. K., Contact LensIndustry—The Shakeout Continues (New York:Salomon Bros., Inc., 1983).Sposato, P., “1982 Marketing Spiral,” ContactLens Forum 7(5):16-21, May 1982.Sposato, P., “Contact Lenses: The ChangingMarketplace Revisited, ” Contact Lens Forum4(9):73-81, September 1979.Sposato, P., “Life Preservers for Small PMMAFirms,” Contact Lens Forum 5(12):33-37, Decem-ber 1980,Sposato, P., “Marketing in Motion, ” ContactLens Forum 6(5):17-25, May 1981.Sposato, P., “Marketing Spiral, Part 2,” ContactLens Forum 7(6):61-67, June 1982.Sposato, P., “Marketing Update, Part 2: QualityCounts, ” Contact Lens Forum 6(6):25-41, June1981.Sposato, P., “New Ideas in Marketing, ” ContactLens Forum 8(5):29-45, May 1983.Sposato, P., ‘Taming the Marketplace,” ContactLens Forum 5(4):51-61, April 1980.Sposato, P., “The ‘Bosses’ Behind the Private
69
70 ● Health Case Study 31: The Contact Lens Industry: Structure, Competition, and Public Policy
41.
42.
43.
44.
45.
46.
47,
48.
49,
Eyes,” Contact Lens Forum 8(4):35-55, April1983.“Union Corp. Says It Sold Contact Lens Businessto CooperVision Unit, ” Wall Street Journal, July6:14 (col.2), 1983.United States v. An Article of Drug . . . Bacto-unidisk, 394 U.S. 784 (1969).U. S., Federal Register 48:56,778-56,798, Dec. 23,1983.U.S. Department of Commerce, Bureau of theCensus, Statistical Abstract of the United States,1982-83 (103d cd.), Washington, DC, 1983.U.S. Department of Health, Education, and Wel-fare, Characteristics of Persons With CorrectiveLenses, United States: July 1965-June 1966, Vitaland Health Statistics, series 10, No. 53, preparedby M. M. Hannaford, DHEW publication No.(PHS) 1000 (Washington, DC: GovernmentPrinting Office, June 1969).U.S. Department of Health, Education, and Wel-fare, Characteristics of Persons With CorrectiveLenses, United States: 1971, Vital and Health Sta-tistics, series 10, No. 93, prepared by M. H.Wilder, DHEW publication No. (HRA) 75-1520,Washington, DC, 1974.U.S. Department of Health, Education, and Wel-fare, National Center for Health Statistics, Of-fice of Health Research Statistics and Technology,Public Health Service, Health Manpower andHealth Facilities, 1976-77 cd., DHEW publicationNo. (PHS) 79-1509, Hyattsville, MD, 1977.U.S. Department of Health and Human Services,Food and Drug Administration, National Cen-ter for Devices and Radiological Health, Divisionof Ophthalmic, Ear, Nose, Throat and Dental De-vices, “Contact Lens Premarket Approval Ap-plication Approvals as of July 25, 1983,” SilverSpring, MD, 1983.U.S. Department of Health and Human Services,Health Care Financing Administration, TheMedicare and Medicaid Data Book, 1981, HCFApublication No. 03128 (Baltimore, MD: HCFA,April 1982).
50.
51.
52.
53.
54.
55 .
56.
57.
U.S. Department of Health and Human Services,Health Resources Administration, Division ofHealth Professions Analysis, Bureau of HealthProfessions, Supply and Characteristics of Se-lected Health Personnel, Washington, DC, 1981.U.S. Department of Health and Human Services,National Center for Health Services Research,Eyeglasses and Contact Lenses: Purchases, Ex-penditures, and Sources of Payment, NCHSRNational Health Care Expenditures Study, DataPreview 11, prepared by D. C. Walden, DHHSpublication No. (PHS) 82-3322 (Hyattsville, MD:DHHS, October 1982).U.S. Department of Health and Human Services,Public Health Service, National Center for HealthStatistics, 1981 Summary: National AmbulatoryMedical Care Survey, NCHS Advance data, pre-pared by L. Lawrence and T. McLemore, No. 88,Hyattsville, MD, Mar. 16, 1983.U.S. Department of Health and Human Services,Public Health Service, Office of Health Research,Statistics, and Technology, Health United States,1982, Hyattsville, MD, 1981.U.S. Department of Health and Human Services,Social Security Administration, Office of FamilyAssistance, Characteristics of State Plans for Aidto Families With Dependent Children Under theSocial Security Act Title IV-A, 1981 cd., SSApublication No. 80-21235, Washington, DC,1981.U.S. Federal Trade Commission, Bureau of Con-sumer Protection, State Restrictions on VisionCare Providers: The Effects on Consumers (“Eye-glasses II”), Washington, DC, 1980.U.S. International Trade Commission, Summaryof Trade and Tariff Information: UnmountedOphthalmic Lenses, TSUS Item 708.01, USITOpublication No. 841, Washington, DC, October1978.Waldo, D. R., and Gibson, R. M., “NationalHealth Expenditures 1981, ” Health Care Financeing Rev. 4(1):1-35, September 1982.
0