the challenge of knowledge management - ahrq national
TRANSCRIPT

Sustainable Clinical Decision Support: The Challenge of Knowledge Management
Robert A. Jenders, MD, MS, FACP, FACMI
Staff Scientist, National Library of Medicine US National Institutes of Health
Attending Staff Physician Georgetown University Hospital
AHRQ CDS TEP 6 December 2011

Disclosure
“This material is presented from my own perspective and should not be taken as representing the viewpoint of DHHS, NIH or NLM.” (NIH Policy 1184, 10 March 2008)

Knowledge Management
• “Traditional” CDS: Still work to be done – KR for sharing = transfer + reuse – Data aggregation
• Evolving CDS: Knowledge access + quality – Access standards: Infobutton, DSS – Measuring quality: HQMF + more – “Intermediate” KR: eRecommendations
• KM: Practical advice/tools re process
CDS: The National Roadmap
Osheroff JA, Teich JM, Middleton B et al. A roadmap for national action on clinical decision support. J Am Med Inform Assoc. 2007 Mar-Apr;14(2):141-5.

CDS National Roadmap: Three Pillars
Jenders RA, Morgan M, Barnett GO. Use of open standards to implement health
maintenance guidelines in a clinical workstation. Comput Biol Med 1994;24:385-390.
CDS National Roadmap: Strategic Objectives
• Knowledge in standard format
• Collect, organize knowledge for importation
• Address policy & legal barriers to CDS
• Disseminate best practices for CDS implementation
• Collect, refine and disseminate CDS results
• Use EHR data to improve clinical knowledge

CDS = Data + Knowledge

Getting More (Structured) Data: Standards
• Work is not yet done
• Ongoing efforts – UCUM – Genetics: MFHP (+ associated HL7), NBS – Research studies: “CDEs” (+ associated LOINC) – Personalized medicine: PHRs (CCR, CCD)
• Challenge: Getting standards (and the systems in
which they are embedded) used




Standard KR: Arden Syntax
• ASTM v1 1992, HL7 v2 1999, v2.1 (ANSI) 2002, v2.5 2005, v2.6 2007, v2.7 2008, v 2.8 2011
• Formalism for procedural medical knowledge
• Unit of representation = Medical Logic Module (MLM) – Enough logic + data to make a single decision – Generate alerts/reminders
• Adopted by several major vendors
– Active use, e.g., CDC meeting re structured format for vaccination knowledge
Jenders RA, Dasgupta B. Challenges in implementing a knowledge editor for the Arden Syntax: knowledge base maintenance and standardization of database linkages. Proc AMIA Symp 2002;:355-359.

Challenge with “Traditional” CDS: Use
• Adoption – Even some basic areas (lab observations, units)
remain a challenge
• Interoperability – Mapping to local data (“curly braces problem”)
• Evolving mission of CDS
– QI

Access to Knowledge: Infobuttons
• Infobutton: Application that mediates queries of knowledge sources by clinical applications (EHRs, etc)
• Process – Clinical information system invokes infobutton
manager (IM) with patient/user data – IM creates 1+ infobuttons, each = different kind of
query – User chooses infobutton to execute query against a
knowledge source, which displays response
Cimino JJ, Li J, Bakken S, Patel VL. Theoretical, empirical and practical approaches to resolving the unmet information needs of clinical information system users. Proc AMIA Symp 2002;:170-174.


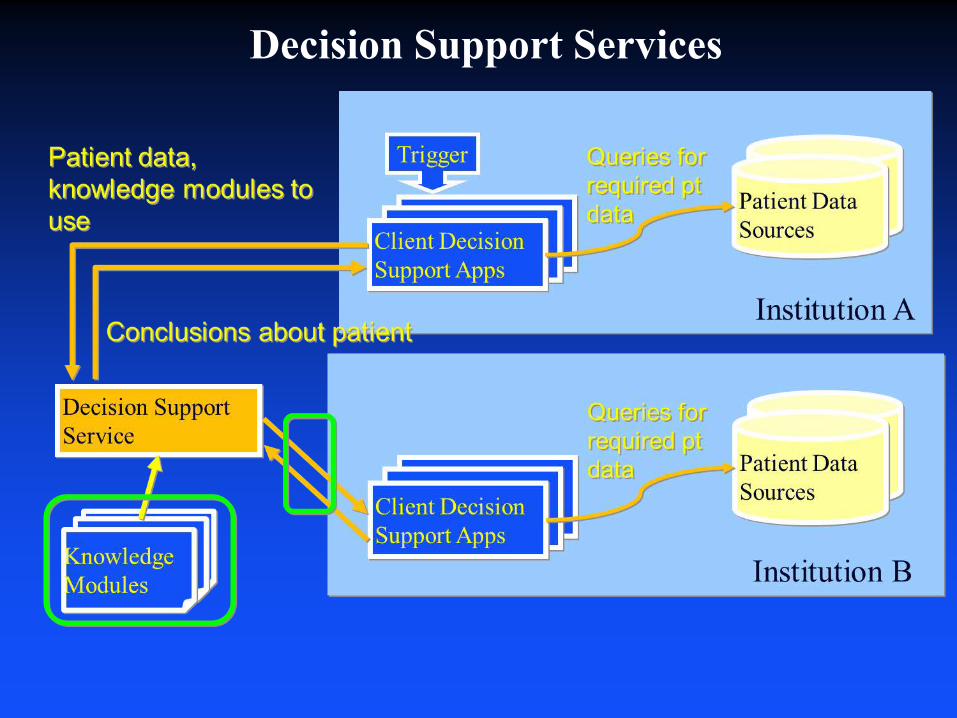
Decision Support Services

Representation of Quality Indicators
• Subset of guideline challenge: Measures + decision support across a population
• Infrastructure: Data + Knowledge representation – Data: QRDA = Specification of HL7 CDA to
represent data needed by quality measures – KR: Many possibilities, active work
• Example: Arden Syntax and ACOVE – N = 39 measures applicable to EHR/administrative
data – Arden can represent logic of all – 38% limited by lack of data in a typical EHR Jenders RA. Suitability of the Arden Syntax for representation of
quality indicators. AMIA Annu Symp Proc 2008:991.

Healthcare Quality Measure Format (HQMF) DSTU
• Increasing mandates for clinical performance measurement – Pay for performance – CMS: No payment for hospital-acquired conditions – Competitive measurement: hospitalcompare.gov
• Implementation of quality indicators (QIs) can be
costly – Need to translate published QI to computable form – Need to collect digital data in structured format – Otherwise, paper-based collection is time- and
resource-intensive

HQMF

Intermediate KR: AHRQ eRecommendations
• SCRCDS – Highly structured and implementable but not
necessarily computable – Analogy: GLIF levels (conceptual, implementable,
computable) • Format
– Header: Management of the eRecommendation – Data and Logic Specification
• Data: Code sets and standards • Logic: Boolean, temporal, math operators
(Arden, HQMF) – Implementation Considerations
• Information useful for local implementation

Category Data Elements Relevant Notes Eligibility/Inclusion-related data
Demographic • Target gender: F • Target age low limit: 50 • Target age high limit: 74 Condition • [not relevant to mammography example] Risk • [not relevant to mammography example]
For PQRI 112 to which this logic statement is related, age high limit = 69
Exclusion criteria-related data
High risk patients <Value set: History of chest radiation > • Quality data type: Procedure Result • Code set: (CPT 4, ICD9, SNOMED) • Code list: {list of relevant codes relating to
Hx of chest radiation}. <Value set: Known genetic mutation, BRCA1, BRCA2, [possibly others]> • Quality data type: Laboratory test result • Code set: (LOINC, SNOMED) • Code list: {list of relevant codes for genetic
tests} <Value set: mammogram results documented within 2 years > • Quality data type: Diagnostic study result • Code set: (CPT,LOINC, SNOMED) • Code list: {list of relevant codes}
High risk patients may require a different screening protocol. The USPSTF recommendation states that a known genetic mutation or a history of chest radiation puts a woman at an increased risk for breast cancer and excludes this group from the screening recommendation. The recommendation implies that a different screening/treatment recommendation/protocol applies to this high risk group, although it does not make explicit such a recommendation/protocol.


Improving Outcomes with Clinical Decision Support: An Implementer’s Guide
• First edition (2005) = Product of HIMSS Patient Safety Task Force
• Second edition (2012): Sponsored by AHRQ
• Goal: Provide practical advice to health care organizations – Choosing decision support goals – Choosing technology to advance those goals – Developing a deployment strategy
http://www.himss.org/cdsworkbook
Jenders RA, Osheroff JA, Sittig DF, Pifer EA, Teich JM. Lessons in clinical
decision support deployment: synthesis of a roundtable of medical directors of information systems. AMIA Annu Symp Proc. 2007 Oct 11:359-63.
Implementer’s Guide: KM
• A comprehensive process for acquiring, adapting and monitoring information for use in clinical decision support that keeps it up-to-date with current clinical evidence, expert consensus and local conditions including pertinent health information system implementation(s).

KM: Key Lessons
• A systematic, cyclic process for managing your CDS knowledge assets is essential and includes people, procedures and information systems.
• KM = an important subcomponent of your CDS program activities, and leverage decision making and management approaches and tools from those broader activities.
• A knowledge management infrastructure should be established before beginning any CDS implementation.
• External support for knowledge management activities may be available from vendor personnel or consultants and should be used to supplement internal staff efforts as needed.

KM: Key Elements • Knowledge sources = diverse
– Vendor-supplied; locally-developed; sharing repositories (“pay to play”)
– Repository/tools to track content (even nonlocal), local decisions and status
• Governance structure with clear accountability – Cycles systematically to acquire, review and update
knowledge – Incorporates regulation, clinical goals, business
needs, financial incentives (e.g., MU) – People + systems
• Emphasis on standards: Data + knowledge (and tracking these)

Conclusions: KM for Sustainable CDS
• Conventional CDS: Data standards, KR for knowledge transfer
• Evolving knowledge standards: Remote access (DSS, Infobuttons), QI (HQMF), “intermediate” KR (eRec)
• Process + tools to support the process: Knowledge repositories, tracking software, toolkits for local organizations
