the acute management of asthma in children - mdaap …mdaap.org/2014_mdaap_asthma_pathway.pdf ·...
TRANSCRIPT
Page 1 of 16
The Acute Management of Asthma in Children – Revision Draft Updated May 2014 The Members of the Maryland Chapter of the American Academy of Pediatrics MDAAP Committee on Pediatric Emergency Medicine COPEM, have developed a clinical pathway for the management of children presenting to the emergency department with asthma exacerbations. This clinical pathway can serve as a clinical practice guideline and was developed using the latest in evidence-based medicine. It is in line with current asthma treatment protocols utilized in the major children’s hospitals in the Baltimore/Washington DC/ Philadelphia areas. This clinical practice guideline is not intended as the only source of guidance in the management of acute asthma exacerbations. Instead, it can be used to assist clinicians by providing a framework for clinical decision-making. It does not replace clinical judgment or establish a protocol for all children with this condition and these recommendations may not provide the only appropriate approach to the acute management of asthma exacerbations in children. We hope that you will find this revision useful. We would appreciate your feedback, comments and suggestions. Please submit comments/ corrections to: Lesley Stephens Hanes, MD MSc, FAAP [email protected]

2
Background: Asthma is the most common chronic disease in childhood in the United States representing about 5% to 10% of ED visits annually 1 . Hospitalization rates have increased steadily over the years, especially in children less than 4 years of age, despite advances in the knowledge of the pathophysiology of asthma and in the availability of new treatment modalities for acute and preventive care. One of the many reasons the prevalence, morbidity and mortality from asthma seem to be on the rise is under diagnosis and inappropriate or under treatment especially in infants and small children 2 . The diagnosis of asthma in this age group is particularly challenging because of the inherent difficulties in obtaining objective measurements of lung function and airway inflammation. Some physicians therefore try to avoid labeling these children as “asthmatics” and instead diagnose them with “reactive airway disease” or “wheezy bronchitis”. The most recent National Asthma Education and Prevention Program (NAEPP) expert panel report recommends that the diagnosis of asthma should be considered in “infants and young children who have had more than 3 episodes of wheezing in the past year that lasted more than 1 day and affected sleep AND who have risk factors for the development of asthma” 2, 3, 4 (see Table 1). These criteria are mainly based on the asthma predictive index proposed in a landmark study from the Tucson Respiratory Study Group 4 . Table 1: Risk Factors for Development of Asthma
Parental history of asthma Physician-diagnosed atopic dermatitis 2 of the following:
Physician-diagnosed allergic rhinitis Wheezing apart from colds Peripheral blood eosinophilia
______________________________________________________________________________
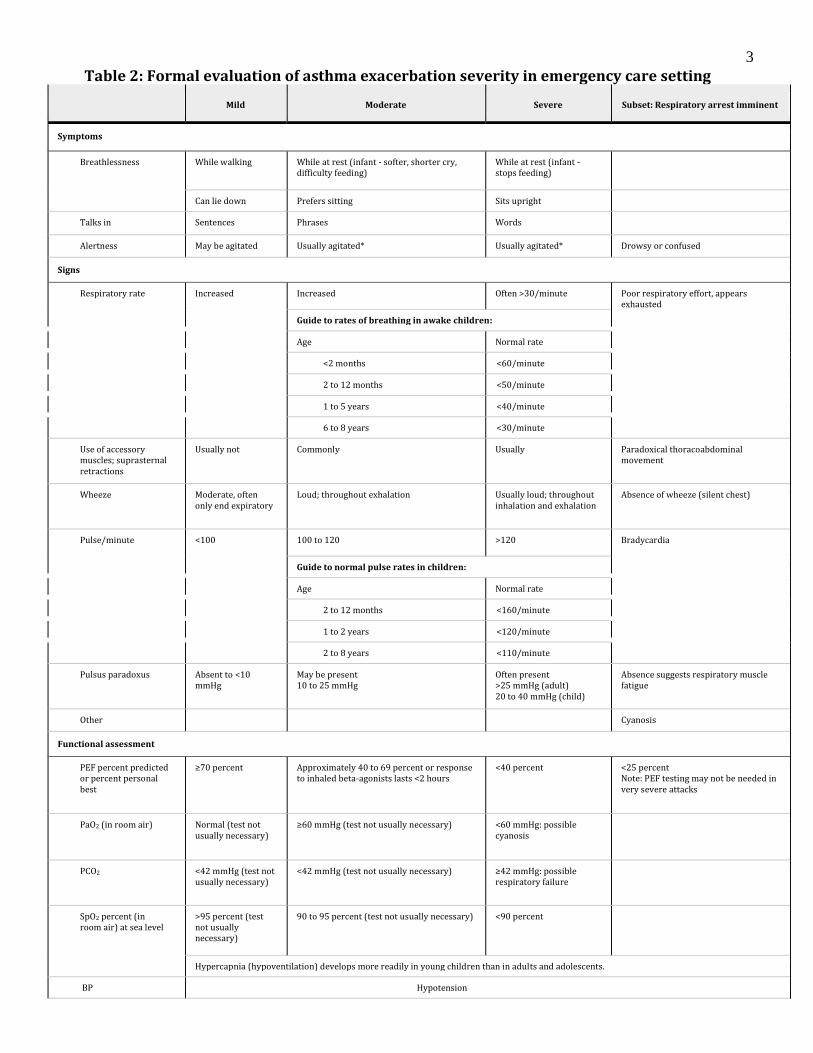
The expert panel also classifies acute asthma exacerbations as mild, moderate and severe based
on clinical symptoms and signs 2 (see Table 2). Because peak expiratory flow rates (PEFR) are
difficult to obtain in young children, several asthma severity scores have been published to
objectively determine the severity of an acute exacerbation (Insert) 5. The Pulmonary Index Score
(PIS) (Table 3) is used widely to determine the initial severity of the exacerbation and level of
treatment needed (ie, mild, moderate, or severe)
Insert: Predicted Average Peak Expiratory Flow Rates by Height
Courtesy: Dr. Suggs (Franklin Square Medical Center)
3
Table 2: Formal evaluation of asthma exacerbation severity in emergency care setting
Mild Moderate Severe Subset: Respiratory arrest imminent
Symptoms
Breathlessness While walking While at rest (infant - softer, shorter cry, difficulty feeding)
While at rest (infant - stops feeding)
Can lie down Prefers sitting Sits upright
Talks in Sentences Phrases Words
Alertness May be agitated Usually agitated* Usually agitated* Drowsy or confused
Signs
Respiratory rate Increased Increased Often >30/minute Poor respiratory effort, appears exhausted
Guide to rates of breathing in awake children:
Age Normal rate
<2 months <60/minute
2 to 12 months <50/minute
1 to 5 years <40/minute
6 to 8 years <30/minute
Use of accessory muscles; suprasternal retractions
Usually not Commonly Usually Paradoxical thoracoabdominal movement
Wheeze Moderate, often only end expiratory
Loud; throughout exhalation Usually loud; throughout inhalation and exhalation
Absence of wheeze (silent chest)
Pulse/minute <100 100 to 120 >120 Bradycardia
Guide to normal pulse rates in children:
Age Normal rate
2 to 12 months <160/minute
1 to 2 years <120/minute
2 to 8 years <110/minute
Pulsus paradoxus Absent to <10 mmHg
May be present 10 to 25 mmHg
Often present >25 mmHg (adult) 20 to 40 mmHg (child)
Absence suggests respiratory muscle fatigue
Other Cyanosis
Functional assessment
PEF percent predicted or percent personal best
≥70 percent Approximately 40 to 69 percent or response to inhaled beta-agonists lasts <2 hours
<40 percent <25 percent Note: PEF testing may not be needed in very severe attacks
PaO2 (in room air) Normal (test not usually necessary)
≥60 mmHg (test not usually necessary) <60 mmHg: possible cyanosis
PCO2 <42 mmHg (test not usually necessary)
<42 mmHg (test not usually necessary) ≥42 mmHg: possible respiratory failure
SpO2 percent (in room air) at sea level
>95 percent (test not usually necessary)
90 to 95 percent (test not usually necessary) <90 percent
Hypercapnia (hypoventilation) develops more readily in young children than in adults and adolescents.
BP Hypotension

4
Notes:
- The presence of several parameters, but not necessarily all, indicates the general classification of the exacerbation.
- Many of these parameters have not been systematically studied, especially as they correlate with each other. Thus, they
serve only as general guides (Cham et al 2002; Chey et al 1999; Gorelick et al 2004b; Karras et al 2000; Kelly et al. 2002b
and 2004; Keogh et al 2001; McCarren et al 2000; Rodrigo and Rodrigo 1998b; Rodrigo et al 2004; Smith et al 2002).
- The emotional impact of asthma symptoms on the patient and family is variable, but must be recognized and addressed
and can affect approaches to treatment and follow-up (Ritz et al 2000; Strunk and Mrazek 1986; von Leupoldt and Dahme
2005).
PaO2: arterial oxygen pressure; PCO2: partial pressure of carbon dioxide; PEF: peak expiratory flow; SpO2: oxygen saturation; BP:
blood pressure.
* Some children with an acute severe asthma exacerbation do not appear agitated.
Reproduced from: National Heart, Blood, and Lung Institute Expert Panel Report 3 (EPR 3): Guidelines for the Diagnosis and
Management of Asthma. NIH Publication no. 08-4051, 2007. Graphic 76344 Version 5.0
Table 3: Pulmonary index score
Score Respiratory
rate* Wheezing•
Inspiratory/expiratory
ratio
Accessory
muscle use
Oxygen
saturation
0 ≤30 None 2:1 None 99 to 100
1 31 to 45 End expiration 1:1 + 96 to 98
2 46 to 60 Entire expiration 1:2 ++ 93 to 95
3 >60 Inspiration and
expiration
1:3 +++ <93
* For patients ≥age 6: through 20, score 0; 21 to 35, score 1; 36 to 50, score 2; >50, score 3. The total score ranges from 0 to 15. In
general, a score of less than 7 indicates a mild attack, a score of 7 to 11 indicates a moderately severe attack, and a score of 12 or
greater indicates a severe attack. However, the Pulmonary Index Score may underestimate the degree of illness in an older child.
• If no wheezing due to minimal air entry, score 3.
Courtesy of Richard Scarfone, MD, FAAP.
Relapse rates for children with asthma seen and released from the emergency department can be as high as 30% 1 . Emergency physicians who care for children with asthma should therefore be skilled in the assessment, treatment and proper disposition of these patients.

5
Acute Asthma Management: Mild exacerbation (Peak Flow > 70% predicted; PIS <7) to Moderate exacerbation (Peak Flow 40-69% predicted; PIS 7 to 11) The following Pediatric Asthma Clinical Pathway is for the pediatric patient who presents to the emergency department with a mild-moderate exacerbation of asthma. It is based on a timeline with 3 phases: triage phase, acute management phase and disposition phase. Special emphasis is given to these areas (Pathway 1):
1. Triage Phase - Immediate treatment with inhaled beta-agonists and steroids in the triage phase cannot be overemphasized. The early administration of steroids has been shown in several studies to significantly decrease hospitalization rates. Steroids can be deferred or used in a stepwise manner after starting albuterol in the acute setting if asthma symptoms are mild and patient is not currently using a beta agonist.
2. Management Phase – Continuous or back-to-back nebulizer therapy with beta
agonists/albuterol for patients with continuing wheeze, tachypnea or increased work of breathing (WOB) is important. The first hour of nebulization should include anticholinergics (ipratropium bromide/ atrovent). Patients who remain symptomatic after the first hour of treatment should continue to receive albuterol alone without atrovent, until they are either clear for discharge or admitted for further treatment. Patients may require 1-3 hours of treatment in the ED before a disposition can be made. Children with increased WOB should receive continuous hourly nebulizations. Single nebs q 1 hour should be reserved for the mildest cases. All patients require, at a minimum, hourly reassessments to determine if the treatments are working. Patients who do not improve are admitted or transferred to an appropriate facility for ongoing care. Those who respond to treatment should be observed and monitored closely for 30- 60 minutes off the nebulized treatments, and may be safely discharged if doing well 1 hour after the last treatment.
3. Disposition Phase – Patients who meet the following criteria may be safely discharged home:
a. PEFR has returned to > 70% predicted. b. If unable to do peak flow, exacerbation symptoms are minimal or absent
(respiratory rate normal for age, adequate air movement, absent or minimal wheeze, no retractions, nasal flaring or agitation).
c. Oxygen saturation on room air > or equal to 94%. d. The patient has been observed for at least 30- 60 minutes after last treatment. e. Patient on home regimin of medications and likely able to space to every 4 -6 hour
albuterol treatments f. There is access to medical care within 24-48 hrs.
Typical discharge medications include the following:
g. Children are discharged on beta agonist nebulizer therapy, 1 unit dose/2.5mg every 4 hours for 7 days, gradually increasing the intervals between doses to 6-8 hours as the child improves. If a nebulizer is not available, most children over 6 months of age can be discharged on an albuterol metered dose inhaler (MDI) with a

6
valve holding chamber (aerochamber) 7. The dosage is 2 - 4 puffs every 4 hours for 24 hours then gradually increasing intervals between doses over the next 7 days.
h. MDI teaching should be done prior to discharge. Infants and preschool children usually take the albuterol during tidal breathing with 5—6 normal breaths between puffs. School-aged children should do a deep inhalation technique with each puff. Additional metered dose inhalers with spacers should be prescribed for use in daycare and/or in school.
i. Oral prednisolone or prednisone 1-2 mg/kg (maximum 60mg – 80mg) divided Q day or BID for an additional 4 days should be started. If oral steroids have been given during the past 2-3 weeks, consider tapering over 7-10 days. Inhaled corticosteroids as well as other controller medications should be continued during administration of oral glucocorticoids. Some institutions are using one or two doses of dexamethasone instead of 5 days of prednisolone or prednisone. The references for dosing dexamethasone are included in the bibliography. 11,12

7
Pathway 1: Mild - Moderate Asthma Exacerbations
Inclusion Criteria: 1. Pediatric patients aged 6mos-18yrs 2. History of prior wheezing episodes or diagnosis of asthma 3. Mild to moderate asthma NOTE: Increased risk of severe disease in patients with: Extreme prematurity History of prior intubation for asthma Pre-existing pulmonary or cardiac disease
Exclusion Criteria: 1. Severe respiratory distress 2. Co morbidity- heart disease, cystic fibrosis or other chronic lung disease
NOTE: Patients on pathway with worsening respiratory distress or symptoms should be evaluated for transfer to a Pediatric Intensive Care Unit PICU
I. Triage Phase 1. Obtain vital signs RR, HR, Temp, Pulse Ox, Weight and (Height if >5yrs old) 2. Obtain peak flow PF PF > 5 yrs or pulmonary/asthma score for < 5 yrs old 3. Give neb solution/ MDI Albuterol 2.5mg to 5mg or MDI 2 to 4 puffs with space r 4. Give steroid Prednisone/prednisolone 2mg/kg PO maximum 60 mg – 80mg If vomits give solumedrol 2mg/kg IM/IV maximum 125mg 5. O2 To maintain O2 sats >93%
Time II. Management Phase
1st hour Reassess vitals Continuing wheeze/tachypnea/↑WOB No Yes Continuous 1 hour or back to back nebs 2nd hour Reassess vitals Continuing wheeze/tachypnea/↑WOB* No Yes Continuous 1 hour or back to back nebs 3rd hour Reassess vitals Continuing wheeze/tachypnea/↑WOB* No Yes Continuous 1 hour or back to back nebs
III. Disposition Phase Reassess vitals Continuing wheeze/tachypnea/↑WOB No Yes Discharge Home Admit to Floor or Observation Unit or PICU Albuterol MDI/spacer 2-4 puffs or Albuterol continuous nebs or single nebs 2.5-5mg q 1-3 hrs Albuterol neb 2.5mg q 4-6 hr weaning to q 4hr when able And And Prednisone/Prednisolone Prednisone/Prednisolone 2mg/kg/day Max 60 mg/day or 1-2mg/kg/day Max 60 mg/day Solumedrol IV/IM 2mg/kg/day divided q6hr Max 125mg/dose

8
Medications (Table 4a and 4b):
1. Beta agonists are the standard first line therapy for the management of acute asthma because it effectively and rapidly relieves bronchospasm and airflow obstruction by relaxing airway smooth muscles. Its onset of action is within 5 minutes, peak effect in 15 minutes and duration of bronchodilation is 4-6 hours 8. It has been shown to improve mucociliary clearance as well by enhancing water output from bronchial mucus glands. Conventional albuterol still remains the preferred choice over levalbuterol (Xopenex). Side effects of conventional albuterol are usually mild and well tolerated and include tachycardia, muscle tremors, hyperactivity, and hypokalemia. Arrhythmias are very rare. The dose of albuterol is 2.5 mg as a single neb or 7.5 mg as a continuous neb for children< 35 kg. For children > 35kg, the dose for a single neb is 2.5-5mg and 7.5-15 mg as a continuous neb over 1 hour.
2. Ipratropium bromide (Atrovent) is an anticholinergic that effectively blocks
acetylcholine-mediated bronchoconstriction with essentially no effect on heart rate even at high doses. Several studies have demonstrated that ipratropium bromide seems to be an effective adjunct therapy in acute childhood asthma when given in 2 to 3 doses during acute exacerbations.8 Atrovent can be administered simultaneously with albuterol via nebulization with a maximum total dose of 750 mcg (<35 kg) or 1500 mcg (>35 kg) over 1 hour during the first hour of treatment only. It is unclear if subsequent doses are effective in reducing hospitalization rates. Peanut allergy is not a contraindication to nebulized Ipratropium Bromide. Sporadic cases of anaphylaxis have been reported in the literature regarding the use of the aerosol inhaler version of Ipratropium Bromide only, not the nebulized medication, in patients with peanut allergy. 10
3. Systemic steroids are indicated for most patients in the emergency department who
present with an acute asthma exacerbation and don’t clear completely with one inhaled beta-agonist treatment. Steroids should also be given to patients who are already on beta agonists at home and who present to the ED with persistant asthma symptoms, even if those symptoms are mild. Steroids should be given in the triage phase with albuterol because they have been shown to speed the resolution of airflow obstruction, potentiate the effects of beta-agonist therapy, and decrease hospitalization rates. 8 Several studies have shown that the effects of IV versus PO administered steroids are equivalent. The PO route is preferred in children because it is inexpensive and less painful. The initial dose of oral prednisolone or prednisone is 2mg/kg, (maximum of 60 mg-80mg). IV or IM steroids are reserved for those who cannot tolerate the PO preparation or who are too ill to receive oral medications. For patients who vomit their oral dose or are too ill to receive the oral preparation, Solumedrol is given at an initial dose of 2mg/kg IV or IM (maximum of 125 mg). Subsequent doses of IV Solumedrol may be given every 6 hrs. Subsequent doses of prednisolone or prednisone may be given every 12-24 hrs. Some institutions are using one or two doses of oral dexamethasone instead of a 5 day course of prednisolone or prednisone. The references for dosing dexamethasone are included in the bibliography. 11,12

9
Table 4a: Recommended doses of medications to treat children with an acute asthma
exacerbation
Inhaled short-acting bronchodilators (beta2-agonists)
Albuterol (salbutamol) by
nebulizer
0.15 mg/kg per dose (minimum 2.5 mg, maximum 5 mg/dose) every 20 to 30 minutes for
three doses, then 0.15 to 0.3 mg/kg (maximum 10 mg) every 30 minutes to four hours as
needed or switch to continuous therapy.
Continuous albuterol
(salbutamol) by nebulizer
0.5 mg/kg per hour (maximum 20 mg per hour) by large volume nebulizer. Dose may
also be determined based upon body weight as follows:
5 to 10 kg - 7.5 mg per hour
10 to 20 kg - 11.25 mg per hour
>20 kg - 15 mg per hour
Albuterol by MDI with spacer
(VHC)
(90 micrograms/puff)
One-fourth to one-third puff/kg or four to eight puffs every 20 to 30 minutes for three
doses, then every one to four hours as needed (minimum two puffs/dose, maximum eight
puffs/dose). Use VHC spacer; add mask in children less than four years.
Levalbuterol (levosalbutamol) One-half the recommended dose for racemic albuterol.
Inhaled bronchodilator (anticholinergic)
Ipratropium bromide nebulizer
solution (250 micrograms/mL)
<20 kg - 250 mcg/dose
≥20 kg - 500 mcg/dose
Every 20 minutes for three doses, then as needed. May combine with albuterol for
intermittent or continuous nebulizer treatment.
Ipratropium bromide MDI with
spacer (18 micrograms/puff)
Four to eight puffs every 20 minutes as needed for up to three hours. Use VHC spacer;
add mask in children less than four years. May give as combined MDI (18 micrograms
ipratropium with 90 micrograms albuterol per puff).
Systemic glucocorticoids
Prednisone or prednisolone* 1 to 2 mg/kg (maximum 60 mg/day) by mouth for the first dose, and then 0.5 to 1 mg/kg
twice daily for subsequent doses starting the following day; a 3 to 10 day course is
generally given.
Methylprednisolone 1 to 2 mg/kg (maximum 125 mg/day) IV
Dexamethasone 0.6 mg/kg (maximum 16 mg/day) by mouth, IM or IV
Systemic beta2-agonists•
Epinephrine 1 mg/mL (also
labeled 1:1000)
0.01 mg/kg IM or SC if no evidence of anaphylaxis (maximum 0.4 mg/dose = 0.4 mL of 1
mg/mL solution). May be repeated every 10 to 20 minutes for three doses.
10
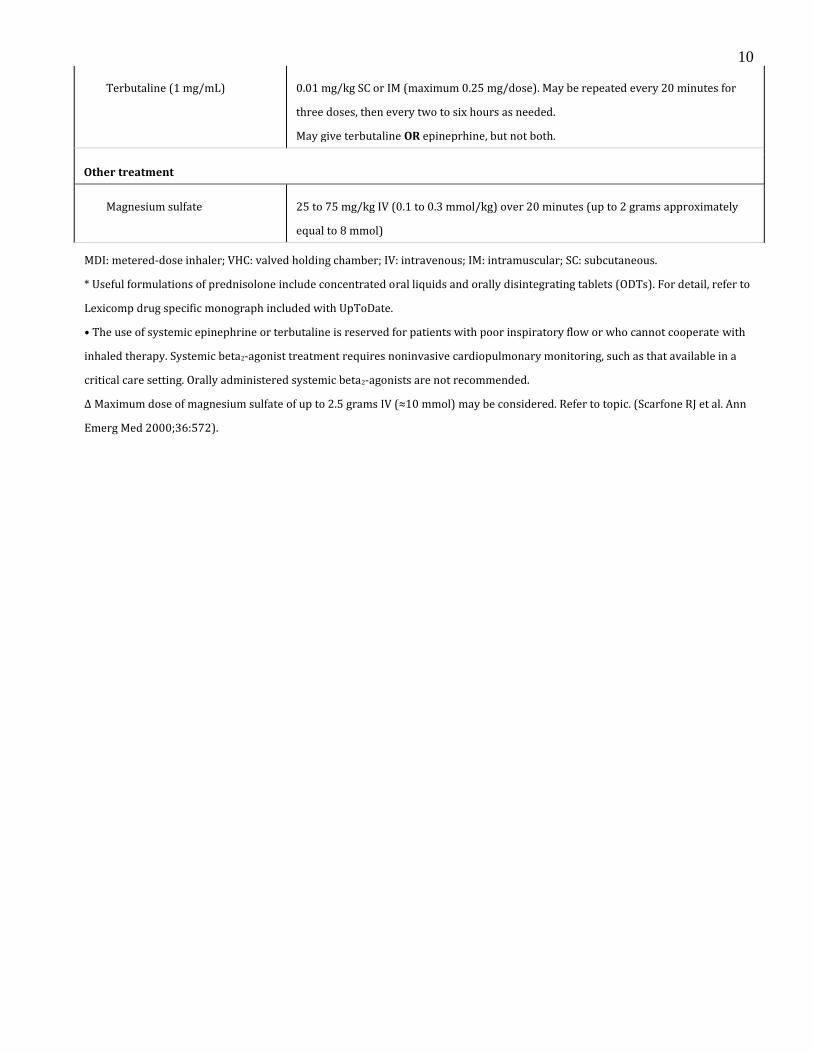
Terbutaline (1 mg/mL) 0.01 mg/kg SC or IM (maximum 0.25 mg/dose). May be repeated every 20 minutes for
three doses, then every two to six hours as needed.
May give terbutaline OR epineprhine, but not both.
Other treatment
Magnesium sulfate 25 to 75 mg/kg IV (0.1 to 0.3 mmol/kg) over 20 minutes (up to 2 grams approximately
equal to 8 mmol)
MDI: metered-dose inhaler; VHC: valved holding chamber; IV: intravenous; IM: intramuscular; SC: subcutaneous.
* Useful formulations of prednisolone include concentrated oral liquids and orally disintegrating tablets (ODTs). For detail, refer to
Lexicomp drug specific monograph included with UpToDate.
• The use of systemic epinephrine or terbutaline is reserved for patients with poor inspiratory flow or who cannot cooperate with
inhaled therapy. Systemic beta2-agonist treatment requires noninvasive cardiopulmonary monitoring, such as that available in a
critical care setting. Orally administered systemic beta2-agonists are not recommended.
Δ Maximum dose of magnesium sulfate of up to 2.5 grams IV (≈10 mmol) may be considered. Refer to topic. (Scarfone RJ et al. Ann
Emerg Med 2000;36:572).

11
Table 4b
Albuterol Weight-based Dosing
Kg Unit Dose (0.5%) MDI Puffs
Continuous
5-10 2.5 mg (0.5 mL) 4 7.5 mg/hr
>10-20 3.75 mg (0.75mL) 6 11.25 mg/hr
>20 5 mg (1.0 mL) 8 15 mg/hr
Ipratropium Weight-based Dosing
5-10 500 mcg over 1 hr in unineb or 250 mcg q20 min x 2
>10 1000 mcg over 1 hr in unineb or 500 mcg q20 min x 2
Prednisone/Methylprednisolone
2 mg/kg p.o./IV, MAX 60 mg
Magnesium Sulfate
50 mg/kg, MAX 2 g
Terbutaline
Subcutaneous: 0.01 mg(mL)/kg MAX 0.25 mg (0.25 mL)
Bolus 10 mcg/kg (Range 2-10 mcg/kg) MAX 750 mcg
Infusion (consider intermittent boluses as alternative) Starting dose 0.4 mcg/kg/min (Range 0.4 mcg/kg-3 mcg/kg/min) Titrate to Max 3 mcg/kg/min
Posted: October 2005
Revised: November 2011, September 2013
Authors: J. Zorc MD, R. Scarfone MD, AM Reardon CRNP, N. Stroebel CRNP, W. Frankenberger RN, L. Tyler RT, D. Simpkins RT
Laboratory and Xray: Chest xrays, CBC and basic metabolic panel (BMP) are not routinely obtained during an acute asthma exacerbation. These tests are reserved for those patients in whom a complication is suspected (eg pneumonia or pneumothorax) or for those who do not improve as expected with therapy. ABGs are only needed in the very sick child with severe respiratory distress or impending respiratory failure.

12
Acute Asthma Management: Severe exacerbations (Peak Flow <40% predicted; PIS >12)
Acute severe asthma exacerbation may be defined by a Pulmonary Index Score of ≥12 or peak flow rate <40 percent of the predicted value for age, sex, and height or personal best.
Children with acute severe asthma exacerbation who fail to improve with initial treatment (initial 1-2 hourse) in the emergency department should be admitted to the pediatric intensive care unit (ICU).
ICU management of children with acute severe asthma entails aggressive pharmacotherapy (Pathway 2 and Insert 2):
o Subcutaneous administration of epinephrine or terbutaline o Magnesium sulfate o Terbutaline IV given as a bolus then followed by continuous infusion o Heliox therapy o High Flow Nasal Canula o Bipap or endotracheal intubation for imminent respiratory failure. o Consider: Ketamine; Aggressive hydration in infants and children
Pathway 2: Management of severe asthma in children
IM: intramuscular; SC: subcutaneous; IV: intravenous.
Courtesy of Richard Scarfone, MD, FAAP.

13
Insert 2: Additional Therapeutic Interventions
Courtesy: Dr. Suggs (Franklin Square Medical Center)
In select patients, noninvasive positive pressure ventilation (NPPV) may avoid the need for intubation. Provided that the child is alert, cooperative, and without increased airway secretions, and the ICU personnel are experienced in the administration of NPPV, we suggest a trial of NPPV in the following situations.
The child remains hypoxemic despite high flow oxygen and/or has documented hypercarbia
To ease the child's work of breathing while awaiting maximal therapeutic effects of corticosteroids and bronchodilators
The child is progressing toward respiratory muscle fatigue
The decision to intubate a patient with status asthmaticus is made clinically based upon clinical findings and physiologic changes. Care must be taken to control the airway before the patient suffers a respiratory arrest or a hypoxic insult. The clinician most experienced with airway management should perform the intubation.
Successful mechanical ventilation in patients with asthma depends upon limiting the risk of hyperinflation and barotrauma. This requires acceptance of PaCO2 that is higher, and a pH that is lower than normal, a strategy called "permissive hypercapnia" or "controlled hypoventilation."
Ventilator settings should be adjusted as necessary to maintain adequate ventilation, assessed by chest auscultation and measurement of arterial blood gases, and to prevent complications (table 5).

14
Complications of mechanical ventilation in patients with asthma include hyperinflation, barotrauma, pneumothorax, myopathy, nosocomial infection, gastrointestinal bleeding, and subglottic stenosis.
Supportive measures that help to prevent tachypnea, breath stacking, and ventilator dyssynchrony include analgesia, sedation, and paralysis. To minimize the risk of myopathy, neuromuscular blocking agents should be discontinued as soon as is feasible.
Adjunctive therapies, such as general anesthesia or extracorporeal life support, may be warranted for patients who do not respond to aggressive pharmacologic therapy and mechanical ventilation.
The mortality rate for ventilated asthmatic children is 2 to 3 percent.
Table 5: Initial ventilator settings in children with status asthmaticus
Parameter Recommended initial setting Maximum recommended setting
Tidal volume 8-10 ml/kg 12 ml/kg
Respiratory rate 8-12 breaths/min 16 breaths/min
Inspiratory time 0.75- 1 second 1.5 seconds
I: E ratio 1:3 - 1:5 >1:3
Inspiratory flow 4-10 liters/kg/min 4-10 liters/kg/min
Minute ventilation <115 ml/kg/min <115 ml/kg/min

15 References: 1. Baren JM, Zorc JJ. Contemporary approach to the emergency department management of pediatric
asthma. Emerg Clin North Am 2002 Feb; 20(1): 115-38. 2. National Asthma Education and Prevention Program Expert Panel Report Guidelines for the
diagnosis and treatment of asthma. NIH Publication No. 97-4051. July 1997. Bethesda, MD. 3. Emond SD, Camargo CA Jr, Nowak RM. 1997 NAEPP guidelines: a practical summary for emergency
physicians. Ann Emerg Med 1998 May; 31(5): 579-89. 4. Covar RA, Spahn JD. Treating the wheezing infant. Pediatr Clin North Am 2003 Jun; 50(3): 631-54. 5. Smith SR, Strunk RC. Acute asthma in the pediatric emergency department. Pediatr Clin North Am
1999 Dec; 46(6): 1145-65. 6. Fleisher GR, Ludwig S. (eds): Textbook of Pediatric Emergency Medicine 3rd ed. Baltimore, Williams
and Wilkins, 1993, pp. 860-61. 7. Rubin BK, Fink JB. The delivery of inhaled medication to the young child. Pediatr Clin North Am
2003 Jun; 50(3): 717-31. 8. Stempel DA. The pharmacologic management of childhood asthma. Pediatr Clin North Am 2003 Jun;
50(3): 609-29. 9. Gunn VL, Nechyba C. The Harriet Lane Handbook 16th ed. The Johns Hopkins Hospital, Mosby, 2002. 10. Robertson J, Shilkorski N. The Harriet Lane Handbook 17th ed. The Johns Hopkins Hospital, Mosby
2005 11. Altamimi S, et al. Single-Dose oral dexamethasone in the emergency management of children with
exacerbations of mild to moderate asthma. Pediatric Emergency Care 2006 Dec; 22(12): 786-93. 12. Qureshi F, Zaritsky A, Poirier M. Comparative efficacy of oral dexamethasone versus oral
prednisone in acute pediatric asthma. J Pediatri 2001;139:20-6. Additional Reading: 13. Ducharme FM, et al. Safety Profile of Frequent Short Courses of Oral Glucocorticoids in Acute
Pediatric Asthma: Impact on Bone Metabolism, Bone Density, and Adrenal Function. Pediatrics 2003 Feb; 111(2):376-382
14. Goggin N, et al. Randomized Trial of the Addition of Ipratropium Bromide to Albuterol and Corticosteroid Therapy in Children Hospitalized Because of an Acute Asthma Exacerbation. Arch Pediatri Adolesc Med 2001 Dec;155:1329-34.
15. Mace SE. Asthma Therapy in the Observation Unit. Emerg Med Clin North Am. 2001 Feb; 19(1):169-80.
16. Mandlberg A, et al. Is Nebulized Aerosol Treatment Necessary in the Pediatric Emergency Department? Comparison with a Metal Spacer Device for Metered-Dose Inhaler. Chest 2000 May; 117(5):1309-13.
17. Newman KB, et al. A Comparison of Albuterol Administered by Metered-Dose Inhaler and Spacer With Albuterol by Nebulizer in Adults Presenting to an Urban Emergency Department with Acute Asthma. Chest 2002; 121:1036-41
18. Scarfone RJ, Friedlaender E. Corticosteroids in Acute Asthma: Past, Present, and Future. Pediatri Emerg Care 2003 Oct; 19(5):355-61.
19. Scarfone RJ, Friedlaender EY. Beta 2 Agonists in acute asthma: The evolving state of the art. Pediatr Emerg Care 2002 Dec;18(6): 442-47.
20. Zorc JJ, et al. Scheduled Follow-up After a Pediatric Emergency Department Visit for Asthma: A Randomized Trial. Pediatrics 2003 March;111(3):495-502.
21. Zorc JJ, et al. Ipratropium Bromide Added to Asthma Treatment in the Pediatric Emergency Department. Pediatrics 1999 Apr;103(4):748-52.

16 Links to Evidence http://www.chop.edu/pathways/emergency-department/asthma/ M-PACT:
Sampayo E.M., Chew, A, Zorc J. Make an M-PACT on Asthma: Rapid Identification of Persistent Asthma
Symptoms in
a Pediatric Emergency Department. Pediatric Emergency Care January 2010 ,Vol 26 (1) pp 1-5.
Overview of Asthma Therapy:
National Asthma Education and Prevention Program. Expert panel report 3:Guidelines for the Diagnosis and
Management
of Asthma. 2007
http://www.nhlbi.nih.gov/nhlbi/lung/asthma
Inhaled ß2-agonists:
Cates CJ, Bara A, Crilly JA, Rowe BH. Holding chambers versus nebulisers for beta-agonist treatment of acute
asthma.
Cochrane Database of Systematic Reviews, 2006.
http://www2.cochrane.org/reviews/en/ab000052.html
Anticholinergics:
Qureshi F, Zaritsky A, Lakkis H. Effect of nebulized ipratropium on the hospitalization rates of children with
asthma. N
Engl J Med 1998;339:1030-1035.
http://content.nejm.org/cgi/content/full/339/15/1030
Zorc JJ, Pusic MV, Ogborn CJ et al. Ipratropium bromide added to asthma treatment in the pediatric emergency
department. Pediatrics 1999:103:748-752.
http://pediatrics.aappublications.org/cgi/content/abstract/103/4/748
Corticosteroids:
Scarfone RJ, Fuchs SM, Nager AL, Shane SA. Controlled trial of oral prednisone in the emergency department
treatment
of children with acute asthma. Pediatrics 1988;82(4):513-518.
http://pediatrics.aappublications.org/cgi/content/abstract/92/4/513
Magnesium Sulfate:
Ciarallo L, Brousseau D, Reinert S. Higher-dose intravenous magnesium therapy for children with moderate to
severe
acute asthma. Arch Pediatr Adolesc Med 2000;154:979-983.
http://archpedi.ama-assn.org/cgi/content/abstract/154/10/979