acute 2/ acute exacerbation of copd asthma 3 ... - · pdf file1/ acute asthma 2/ acute...
TRANSCRIPT

1/ Acute asthma
2/ Acute exacerbation of COPD
3/ Pneumonia
4/ Pneumothorax
Pascal Van BleyenberghDepartment of Pulmonology, UZ Leuven
AcuteAsthma
Pascal Van BleyenberghDepartment of Pulmonology, UZ KULeuven
allergensexercisecold airSO2 ,…
symptoms
hyperreactivityairflow
limitation
inflammationallergens
?
Asthma is a chronic inflammatory disorder of the airways
GINA 2015; www.ginasthma.org
Asthma in ER is not a frequent problem
prevalence of atopy 17–44%prevalence of asthma 5-6%<20% of asthmatics have been seen/admitted for an acute asthma exacerbation acute severe asthma ≤5% of all ER visits
ER & hospitalization >50% of total asthma costs
30% 4-7%

Asthma mortality rate is decreasing
mortality rate of 5,2/100.000 (US data)
rate decreasing: -8%status asthmaticus: 0-21% in hospital mortalityafter near-fatal attack: 26% 6-year mortality
Belgium<20pts/year
USA5.000/year
worldwide150.000/year
post-discharge management !!
Correct management- exposition- anti-inflammatorytreatment
- education
Risk factors of death from asthma attack - 1
60% female 45% age <25 years(chronic) Severe asthma
asthma history ≥15 years, ≥3 types of asthma medicationprevous use of systemic corticosteroids>2 canisters of SA β2-agonists / monthhigh degree of bronchial hyperresponsivenessprevious ER visits or ICU/hospital admissionsprior intubation for asthma
Smoking - illicit drug use - environmental factors
Co-morbidityobesity, cardiovascular, pulmonary, GERD,….
Alvarez GG et al. Can Respir J 2005; 12:265-270
Risk factors of death from asthma attack - 2
Medication: aspirin - β-blokker – NSAID - …Psychosocial problems
Low socioeconomical status Adherence and compliance with therapy inhaled steroids!
Blunted perception of airway obstruction
poor perception of dyspnea “underperceivers”
Genetic factors IgE, steroid responsiveness, TNFα in airways,
β-agonist responsivenes, …
Alvarez GG et al. Can Respir J 2005; 12:265-270
Phenotypes of acute asthma attack
Restrepo RD, Peters J. Curr Opin Pulm Med 2008; 14:13-23

Assessment of acute asthma
History/clinical examinationnonspecific – absence does not excude severe attack
O2sat, ABGtitration of O2therapy (94-98%)SpO2 >92%: hypercapnia rarehypercapnia severity of attack!
Laboratory datahypokalemia, leukocytosis (eos.), lactate,…
Chest radiographECGPulmonary function test
serial PEFR, FEV1 (bedside)
Assessment of acute asthma
GIN
A 20
15; w
ww.
gina
sthm
a.or
g
Assessment of acute asthmaseverity
BTS guidelines 2009; www.brit-thoracic.org.uk
Conditions mimicking an acute asthma attack
upper airway obstruction(VCD, tumor, stricture or foreign body)

Conditions mimicking an acute asthma attack
upper airway obstruction(VCD, tumor, stricture or foreign body)
AECOPD
patient characteristics
history of disease
Assessment of acute asthmadifferentiation with AECOPD…
ASTHMA
young age, sudden onset
atopy, familial history
episodic symptoms
reversible airway obstruction
serum IgE, airway inflammation (eosinophils, mastcells,
Th2 lymphocytes)
bronchial hyperresponsivenessidentifiable triggers
COPD
>40-60 years
smoking history
progressively worsening symptoms
not fully reversible airway obstruction
airway inflammation(macrophages, neutrophils)
chronic sputum expectoration, emphysema (parenchymal destruction)
Conditions mimicking an acute asthma attack
upper airway obstruction(VCD, tumor, stricture or foreign body)
AECOPDcongestive heart failurepulmonary embolismbronchopneumoniabronchiectasis vasculitis (Churg Strauss, ..)carcinoid syndromehyperventilation syndrome…
Management of acute asthma treatment
standard therapyoxygenbronchodilatorscorticosteroids (PO-IV-SC-inhalation)
additional therapy?MgSO4
-agonists SC or IVmethylxanthines...
(non)invasive ventilationprevention of future asthma attacks
Lazarus SC. New Engl J Med 2010; 363:755-764Papiris SA et al. Drugs 2009; 69(17):2363-2391
ALL PATIENTS!
Management of acute asthma:1/ oxygen
Hypoxemia= important cause of acute asthma-related death
supplemental oxygenO2 saturation ≥90-93%no RCT: "common sense" based medicineFiO2 28-32% is sufficient most of the timeshumidification recommended
hypoxemia may persist upon resolution of asthma attacknebulisation with oxygen! (10-12L/min)
Management of acute asthma:2/ inhaled 2-agonists
mechanism of action:bronchodilatation (+ other effects…)fast onset of action (5 min)
clinical benefit:acute symptoms of asthmamild, moderate & severe asthma attack
to be given immediately, on presentation!short-acting 2-agonists
salbutamol (= albuterol)formoterol(terbutaline), (fenoterol), R-enantiomer of albuterol (levalbuterol): improved bronchodilatation?adrenaline, isoprenaline: less selective!
Management of acute asthma:2/ inhaled 2-agonists
administration:nebulized salbutamol
dosing: 2,5–5mg q 15-20min for 1h2,5–5mg salbutamol q 1 h for 4-5 h2,5–5mg salbutamol q 4 h or on demand(2,5mg 10 dr Ventolin®)
continuous better than repetitive? (FEV1<30%)MDI with spacer
as effective as nebulization !dosing: 400-600 µg salbutamol ( 4-6 puffs Ventolin®)
q 10min for 1 hq 1h for 4 h q 4h or on demand
patient coordination and supervision required!!
side effects: tremor, tachycardia, hypokalemia
Management of acute asthma:2/ 2-agonists SC - IV
2-agonists SC or IV (or PO)
conflicting evidence: no clear advantage of IV or SC administration over inhaled routeindications
inability to administer inhaled medicationinadequate response to inhaled therapy(severe refractory asthma?)
administrationIV salbutamol 0,5-30µg/kg/minSC epinephrine 0,3mg q20 min for 1h
more side effects !

Management of acute asthma:2/ inhaled anticholinergics
mechanism of action:bronchodilatation, less potent than 2-agonistsslower onset of actionadditive to 2-agonists (other mechanism!)
clinical benefit:improvement of FEV1 and PEFRreduction in admission rate
indication:adjunct to 2-agonists & steroidsmore severe disease (FEV1 <35%)
administration:nebulization
0,5 mg ipratropium bromide ( 20 dr or 1 MD Atrovent®)q 20 min for 1 h, continue q 4 h if improvement
MDI with spacer 80-160 µg ipratropium bromide ( 4-8 puffs Atrovent®) q 10-20 min for 1 h, continue q 4 h if improvement
no benefit of nebulized atropine
Rodrigo GJ et al.Thorax 2005; 60:740-746
Management of acute asthma:3/ corticosteroids - systemic
mechanism of action:anti-inflammatory effectimprovement of 2-induced bronchodilatationslow onset of action: improvement 6-12 h after first dose
clinical benefit:'common practice'more rapid improvement of lung function, fewer hospitalizations & lower rate of relapse (although only small RCT…)
indications:ALL moderate to severe attackspoor response to 2- agonistspts already on steroids (or need of steroid use in prior attacks)
administration:prednisone 50-100mg q 24 h or methylprednisolone 40-80mg q 24 horal therapy equivalent to IVcontinue steroids >5-10d (0,5-1mg/kg/d po, stop without tapering)
side effects: hyperglc, mood alteration, hypertension, …
Sherman MS et al. Clin Pulm Med 2006;13:315-320Krishnan JA et al. Am J Med 2009;122:977-991
Management of acute asthma:3/ corticosteroids - inhaled
rationaletopical anti-inflammatory effectquicker onset of action (<3h)
clinical benefitunequivocal study resultssmall benefit: slight improvement of FEV1 and reduction of admission rate (3 meta-analyses)
indications:treatment of chronic asthmaexacerbation & mild asthma attacksevere asthma attack ?post discharge
administration: high dose (250-500 µg fluticasone or 400 mg budesonide q10min for 3h)no severe side effects
NO SUBSTITUTE FOR SYSTEMIC STEROIDS !!
Management of acute asthma:4/ additional therapy
magnesium sulphatemechanism of action:
bronchodilationeffect on inflammation
resultssmall improvement of FEV1 for <4h reduction in admission rate
pts with severe asthma or FEV1<30%pred 2g MgSO4 IV over 20 minsingle or q30min? (max 12g/12h)nebulized MgSO4 (135-1152mg) : less evidence!
Rowe BH et al. Curr Opin Pulm Med 2008; 14:70-76

Management of acute asthma:4/ additional therapy
anti-leukotriene antagonist po - ivmechanism of action
anti-inflammatorybronchodilatation
clinical benefitweak but significant improvement of FEV1 -dyspneano reduction of admission rate (?)additive to 2-agonists & steroidsrapid onset of action (IV>>PO; <1-2hrs)
montelukast, zafirlukastno side effects
not recommended for routine useCamargo CA et al. J Allergy Clin Immunol 2010; 125:374-380
Management of acute asthma:4/ additional therapy
methylxanthinesbronchodilatation, anti-inflammmatoryinsufficient evidence of benefit
inferior to 2-agonists small effect on FEV1 & exacerbation rate?
side effects!!only for very severe refractory asthma?0,4 mg/kg/h IV (serum level 8-15µg/ml)
not recommended for routine use!
Parameswaran K et al. Cochrane Database Syst Rev 2000; 4:CD002742
Management of acute asthma:4/ additional therapy
helium-oxygen mixtures70-80% He & 20-30% O2 (density one third of air)mechanism of action
decrease airway resistance & hyperinflationimprove deposition of aerosolized bronchodilators
evidence of benefit in severe refractory attacks
experimental options: no routine useinhaled anesthetics: halothane, enflurane (case reports)nebulized lidocaïne(inhaled furosemide)
antibiotics: not routinely indicated!!contra-indicated
inhaled mucolyticssedation
Rodrigo G et al. Cochrane Database Syst Rev 2006; 4:CD002884
Management of acute asthma: treatment summary
Triage patient immediately- history of risk factors- vital signs and suymptoms
Oxygen(sat ≥90-94%)
Short-acting ß2-agonist +/- anticholinergic* nebulizer q20’ for 1h
*nebulizer q1hr or continuously
Oral/IV corticosteroids40mg methylprednisolone q12hrs
Continue treatmentfor 1-3 hrs
Discharge oradmission?
Consider magnesium sulfate2g IV once
Consider heliox
Consider NIPPVIntubation & ventilation
(bedside decision!!!)

Management of acute asthma: discharge or admission
discharge home
admit to hospital
admit to ICU
asthma action planmedical follow-up
• continue other treatment options
• possible intubation and ventilation
continue treatment
improvement no improvement
good responsePEF ≥70% for >1h
incompleteresponse
PEF 40-69%
poor responsePEF <40%
deteriorationpCO2 ≥42 mmHg
severe symptoms
Complications of asthma
mucous plugging and atelectasispneumonia (VAP!!)electrolyte disturbances (hypokalemia in 17%)hyperglycemialactic acidosisbarotrauma (≥4%): pneumothorax, pneumomediastinum, pneumopericardium, SC emphysemamyopathy (10-30%)myocardial infarct, arrhythmia,CV collapseanoxic brain injuryin hospital mortality 0-21%
Management of acute asthmapost ICU/ED care
(observe on ICU for >24h after extubation)course of oral steroids at dischargeadequate inhaled treatment:
= inh. steroids + long-acting 2-agonists + rescue therapy
check inhaler techniqueuse PEF meterformulate 'exacerbation action plan' with patient (cave ‘underperceivers’!)identification and avoidance of triggersregular follow-up care
COPDexacerbations
Pascal Van BleyenberghDepartment of Pneumology, UZ KULeuven
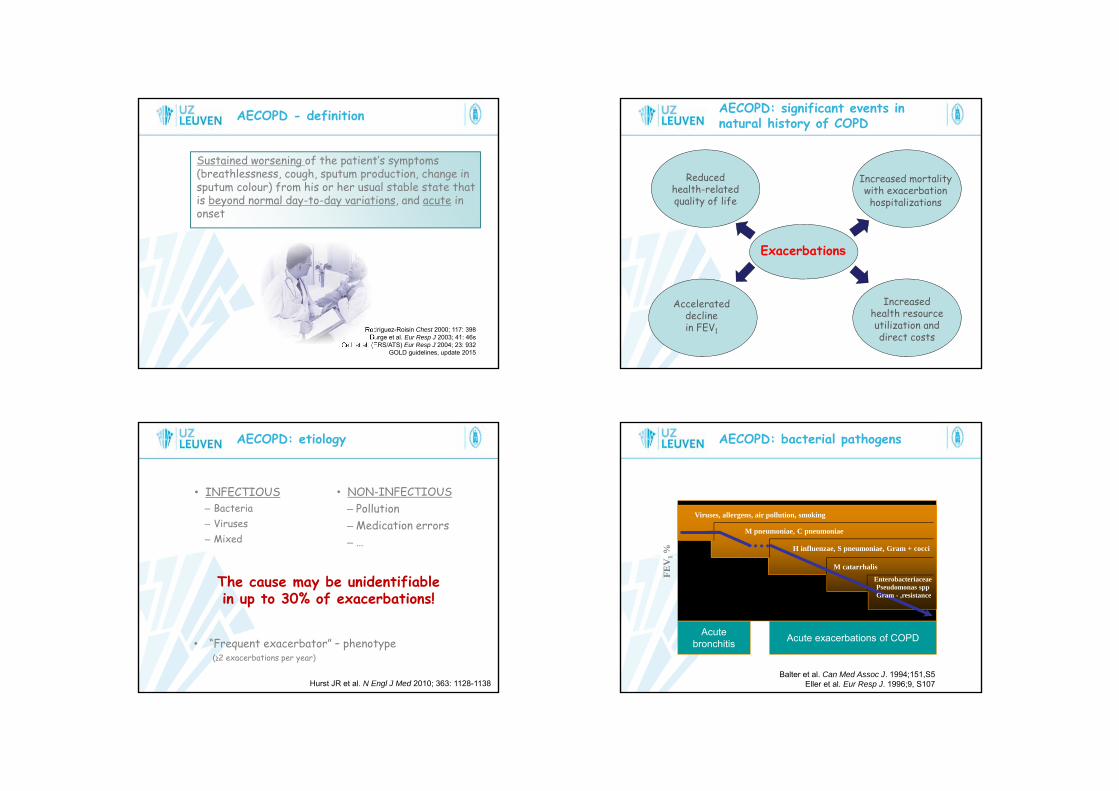
Sustained worsening of the patient’s symptoms (breathlessness, cough, sputum production, change in sputum colour) from his or her usual stable state that is beyond normal day-to-day variations, and acute in onset
AECOPD - definition
Rodriguez-Roisin Chest 2000; 117: 398 Burge et al. Eur Resp J 2003; 41: 46s
Celli et al. (ERS/ATS) Eur Resp J 2004; 23: 932GOLD guidelines, update 2015
AECOPD: significant events in natural history of COPD
Increased mortalitywith exacerbationhospitalizations
Accelerateddeclinein FEV1
Reducedhealth-relatedquality of life
Exacerbations
Increasedhealth resource utilization anddirect costs
• INFECTIOUS– Bacteria– Viruses– Mixed
AECOPD: etiology
35
• NON-INFECTIOUS– Pollution– Medication errors– …
The cause may be unidentifiablein up to 30% of exacerbations!
• “Frequent exacerbator” – phenotype(≥2 exacerbations per year)
Hurst JR et al. N Engl J Med 2010; 363: 1128-1138
AECOPD: bacterial pathogens
Balter et al. Can Med Assoc J. 1994;151,S5Eller et al. Eur Resp J. 1996;9, S107
Acutebronchitis
FEV
1 %
Acute exacerbations of COPD
Viruses, allergens, air pollution, smoking
M catarrhalisEnterobacteriaceae Pseudomonas sppGram - ,resistance
H influenzae, S pneumoniae, Gram + cocci
M pneumoniae, C pneumoniae

• Pneumonia• Pneumothorax• Pulmonary embolus• Lung cancer• Upper airway obstruction• Pleural effusion• Recurrent aspiration
• Left ventricular failure• Cardiac ischemia/myocardial infarction
• …
AECOPD: differential diagnosis
37
• Use of respiratory muscles• Paradoxical chest wall movement• Worsening or new central cyanosis• Development of peripheral edema• Hemodynamic instability• Deteriorated mental status
AECOPD: assessmentClinical signs of severity
38
• Inadequate respons to initial emergency therapy• Changes in mental status (confusion, lethargy, coma)• Persistent or worsening hypoxemia or respiratory
acidosis (pH <7,25mmHg)• Need for invasive mechanical ventilation• Hemodynamic instability - Need for vasopressors
• Full blood count & biochemistry (electrolytes, glycemia,…)
• Theophylline level (in pts on theophylline therapy)
• Arterial blood gases+ record inspired oxygen concentration!!
• Sputum for microscopy and culture (if purulent)
• Blood cultures (if pt is pyrexial)
• ECG• Chest X-ray
• Lung function tests not for routine use
AECOPD: assessmentUsefull diagnostic tests
39
A = Antibiotics
AECOPD: the A-B-C approach
40

AECOPD: antibiotics or not?
Saint et al. JAMA 1995; 273: 957
–1.0 1.0–0.5 1.50 0.5
Elmes et al. 1957Berry et al. 1960
Fear and Edwards. 1962Elmes et al. 1965
Petersen et al. 1967Pines et al. 1972
Nicotra et al. 1982Anthonisen et al. 1987Jorgensen et al. 1992
Overall
Pro placebo Pro antibiotica
Effect size
1. Anthonisen criteria Ann Intern Med 1987; 106: 196-204
a) dyspnea Bach Ann Intern Med 2001; 134: 600
b) increase in sputum productionc) increase in sputum purulence
2. Severity of underlying COPD Soler et al. Thorax 2007; 62: 29
FEV1 <50% antibiotics
3. Respiratory failure Nouira et al. Lancet 2001; 358: 2020
AECOPD: when antibiotics?
Difficult differential diagnosis 1/ infectious >< non-infectious
2/ bacterial >< viral
AECOPD: indications for antibiotics
FEV1 >80% FEV1 50-80% FEV1 <50%
Anthonisen 3/3 NO YES YES
Anthonisen 2/3(incl. sputum purulence)
NO YES YES
Anthonisen 1/3 NO NO YES
Acute respiratory failure YES YES YES
IDAB guidelines 2010Sanford guide, Belgian edition, 2013-2014
AECOPD: antibiotics
* Antibiotics almost always necessary in hospital
* Oral route is preferred
* Sequential therapy if intravenously started! (day 3)
1. Mild to moderate COPD (FEV1 <50%)
2. Severe to very severe COPD (FEV1 <50%),without risk-factors for P. aeruginosa
3. Severe to very severe COPD (FEV1 <50%),with risk-factors for P. aeruginosa
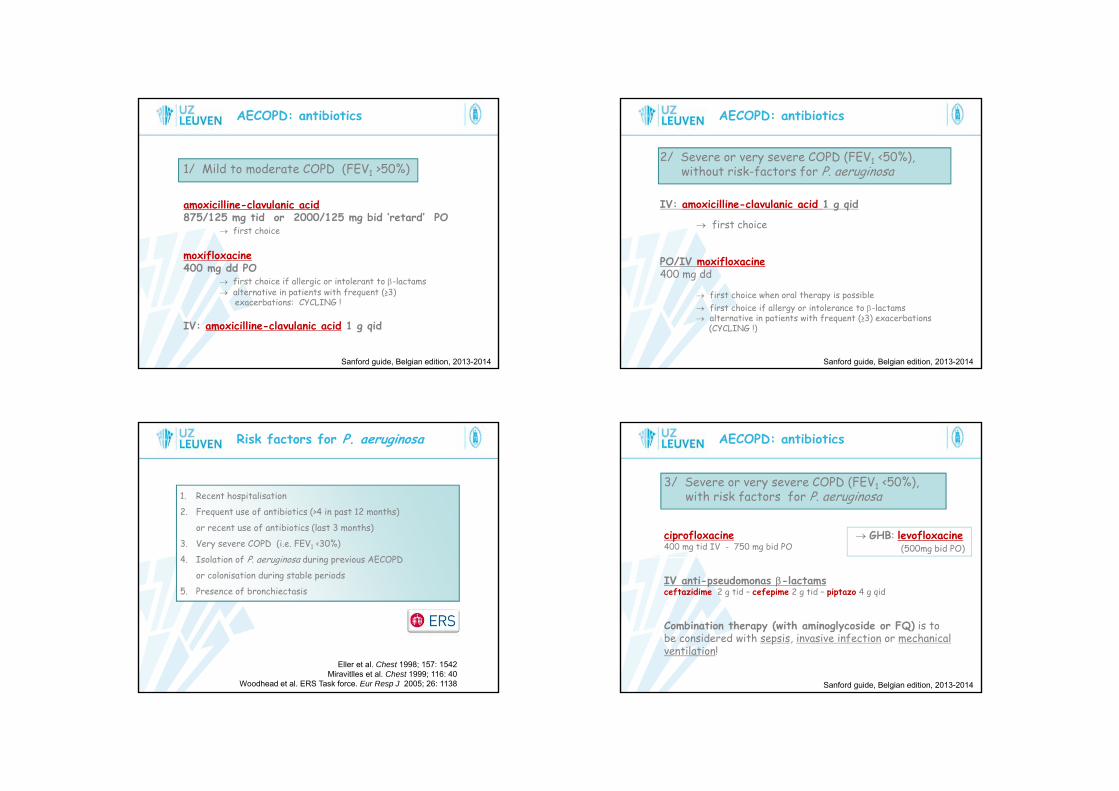
AECOPD: antibiotics
1/ Mild to moderate COPD (FEV1 >50%)
amoxicilline-clavulanic acid875/125 mg tid or 2000/125 mg bid ‘retard’ PO
first choice
moxifloxacine400 mg dd PO
first choice if allergic or intolerant to -lactams alternative in patients with frequent (≥3)
exacerbations: CYCLING !
IV: amoxicilline-clavulanic acid 1 g qid
Sanford guide, Belgian edition, 2013-2014
AECOPD: antibiotics
2/ Severe or very severe COPD (FEV1 <50%),without risk-factors for P. aeruginosa
IV: amoxicilline-clavulanic acid 1 g qid
first choice
PO/IV moxifloxacine400 mg dd
first choice when oral therapy is possible first choice if allergy or intolerance to -lactams alternative in patients with frequent (≥3) exacerbations
(CYCLING !)
Sanford guide, Belgian edition, 2013-2014
Risk factors for P. aeruginosa
1. Recent hospitalisation
2. Frequent use of antibiotics (>4 in past 12 months)
or recent use of antibiotics (last 3 months)
3. Very severe COPD (i.e. FEV1 <30%)
4. Isolation of P. aeruginosa during previous AECOPD
or colonisation during stable periods
5. Presence of bronchiectasis
Eller et al. Chest 1998; 157: 1542Miravitlles et al. Chest 1999; 116: 40
Woodhead et al. ERS Task force. Eur Resp J 2005; 26: 1138
AECOPD: antibiotics
3/ Severe or very severe COPD (FEV1 <50%),with risk factors for P. aeruginosa
ciprofloxacine400 mg tid IV - 750 mg bid PO
IV anti-pseudomonas -lactamsceftazidime 2 g tid – cefepime 2 g tid – piptazo 4 g qid
Combination therapy (with aminoglycoside or FQ) is to be considered with sepsis, invasive infection or mechanical ventilation!
GHB: levofloxacine(500mg bid PO)
Sanford guide, Belgian edition, 2013-2014

B = Bronchodilators– Improve symptoms and FEV1
– MDI = nebuliser use (but…)– Nebuliser driven by compressed air, not oxygen– Increasing dose and/or frequency of short-acting BD– Combine β2-agonists and anticholinergics– Theophyllines only to be used as second-line therapy (significant
side effects, only modest and inconsistent beneficial effects)
AECOPD: the ABC approach
49
Celli BR et al. Eur Respir J 2004; 23: 932-946NICE Guidelines, 2010
GOLD Guidelines, 2015
Salbutamol 2,5mg + Ipratropium 0,5mg, qid (Combivent®)Fenoterol 1,25mg + Ipratropium 0,5mg, qid (Duovent®)
C = Corticosteroids– Improve symptoms, FEV1 and PaO2 in moderate/severe
AECOPD– Reduce treatment failure, relapse and LOS– Oral route is preferred– Induce possible side effects (hypoglycemia, …)
AECOPD: the ABC approach
50
Niewoehner DE et al. N Engl J Med 1999; 340: 1941-1947Aaron SD et al. N Engl J Med 2003; 348: 2618-2625
De Jong YP et al. Chest 2007; 132: 1741-1747Walters JA et al. Cochrane Database Syst Rev 2011; 10: CD006897
GOLD Guidelines, 2015
30-40mg prednisolonefor 5(-10) days
= 32mg methylprednisolone
Oxygen– Key component of therapy – CAVE hypercapnia!!– Titrated to target saturation of 88-92% ( 1-2 L/minute)– Check ABG after 30-60 minutes!
AECOPD: beyond ABC…
51
Austin MA ete al. BMJ 2010; 341: 5462
Noninvasive mechanical ventilation– Success rate of 80-85%– Improves respiratory acidosis– Decreases respiratory rate, work of breathing, severity of
breathlessness, complications of IPPV, LOS– Reduces mortality and intubation rates
Brochard L et al. N Engl J Med 1995; 333: 817-822Kramer N et al. Am J Respir Crit Care Med 1995; 151: 1799-1806
Plant PK et al. Lancet 2000; 355: 1931-1935
• Respiratory acidosis (pH ≤7,35 and/or PaCO2 ≥45mmHg)
• Severe dyspnea with clinical signs suggestive of respiratory muscle fatigue, increased work of breathing, or both(use of respiratory accesory muscles, paradoxical motion of the abdomen, retraction of intercostal spaces,…)
AECOPD: indications for NIPPV
52
Consensus report. Chest 1999; 116: 521-534Int Consensus Conference in Intens Care Med. Am J Respir Crit Care Med 2001; 163: 283-291
Lightowler JV et al. BMJ 2003; 326: 185GOLD Guidelines, 2015
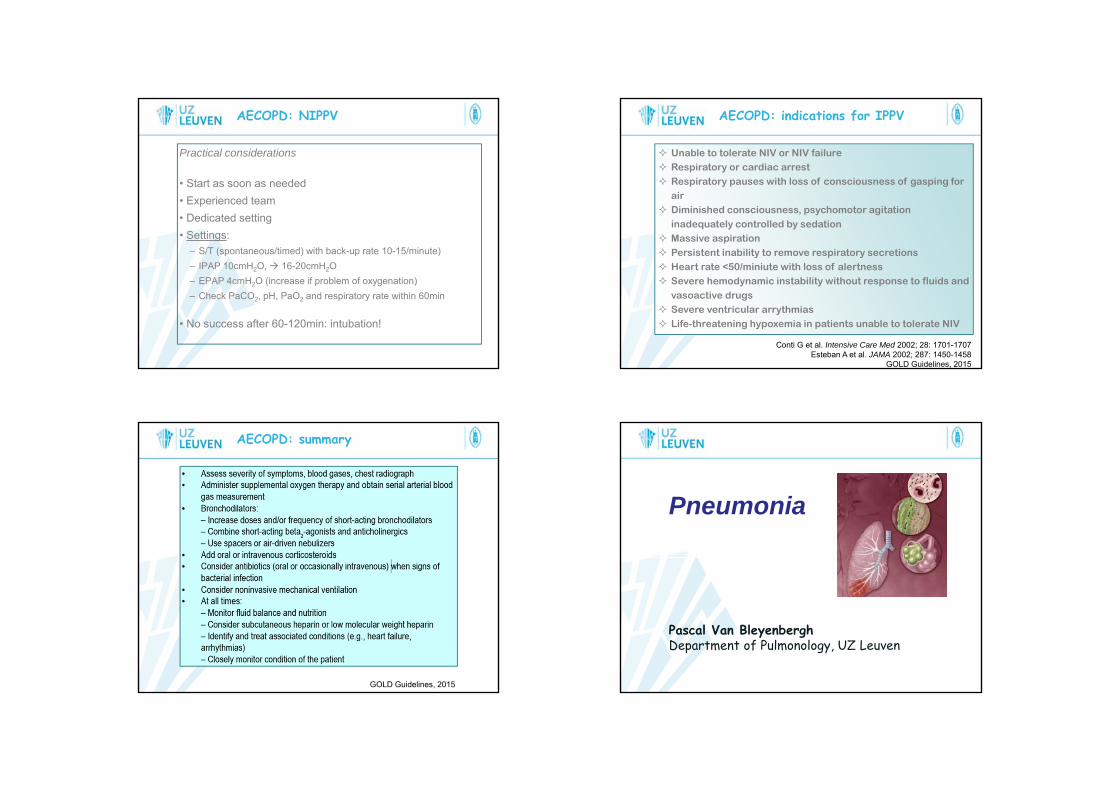
Practical considerations
• Start as soon as needed• Experienced team• Dedicated setting• Settings:
– S/T (spontaneous/timed) with back-up rate 10-15/minute)– IPAP 10cmH2O, 16-20cmH2O– EPAP 4cmH2O (increase if problem of oxygenation)– Check PaCO2, pH, PaO2 and respiratory rate within 60min
• No success after 60-120min: intubation!
AECOPD: NIPPV
53
AECOPD: indications for IPPV
54
Conti G et al. Intensive Care Med 2002; 28: 1701-1707Esteban A et al. JAMA 2002; 287: 1450-1458
GOLD Guidelines, 2015
Unable to tolerate NIV or NIV failure Respiratory or cardiac arrest Respiratory pauses with loss of consciousness of gasping for
air Diminished consciousness, psychomotor agitation
inadequately controlled by sedation Massive aspiration Persistent inability to remove respiratory secretions Heart rate <50/miniute with loss of alertness Severe hemodynamic instability without response to fluids and
vasoactive drugs Severe ventricular arrythmias Life-threatening hypoxemia in patients unable to tolerate NIV
AECOPD: summary
55GOLD Guidelines, 2015
Pneumonia
Pascal Van BleyenberghDepartment of Pulmonology, UZ Leuven

Pneumonie
1. Community-acquired (CAP)
2. Health-care associated (HCAP)
3. Hospital-acquired (HAP)
* Ventilator associated (VAP)
CAP: definitie= pneumonie, ontstaan buiten het ziekenhuis (‘thuis ’) of 72uur
na ontslag uit ziekenhuis
frequente en ernstige ziekte, ondanksbeschikbaarheid van krachtige antibiotica en effectieve vaccins !
- zesde doodsoorzaak ter wereld- meest lethale infectie
alle leeftijden 5-15/1000/jaar>65 jaar 20/1000/jaar>75 jaar 34/1000/jaar
21%-44% hospitalisatie
opname op ICU 5%-10%
CAP: epidemiologie
1900 1950 2000
Mortaliteit:- outpatients 1%- 5%- inpatients
- CAP III 6%-14%- CAP IV 36%-60%
- 18-44 jaar <1%- >65 jaar 12,5%
Gilbert K, Fine MJ. Semin Respir Infect 1994Marston et al, Arch Intern Med 1997
Gegevens van de ziekenhuizen in de VSPatiënten ≥12 jaar met bacteriële pneumonie
Gegevens van de ziekenhuizen in de VSPatiënten ≥12 jaar met bacteriële pneumonie
Meta-analyse
Gehospitaliseerde, ambulante en ICU, CAP
patiënten >18 jaar
Meta-analyse
Gehospitaliseerde, ambulante en ICU, CAP
patiënten >18 jaar
Gegevens van ziekenhuizen in de VS
CAP patiënten<2 jaar -> 65 jaar
Gegevens van ziekenhuizen in de VS
CAP patiënten<2 jaar -> 65 jaar
Gegevens van ziekenhuizen in de VS
CAP-patiënten >18 jaar
Gegevens van ziekenhuizen in de VS
CAP-patiënten >18 jaar
12.3%MORTALITEIT
(N=4432)
12%MORTALITEIT
(N=5837)
~12%MORTALITEIT
(N=730)
12.2%MORTALITEIT
(N=1130)
1966 -1995
1995 -1997
1999 -2001
1952 -1962
Austrian R et al. Ann Intern Med 1964; 60: 759Fine MJ et al. JAMA 1996; 274: 134
Feikin DR et al. Am J Pub Health 2000; 90: 223Restrepo MI et al. Chest 2008; 133: 610
Mortaliteit CAP over tijd…

CAP: oorzaken
Welte T et al. Thorax 2012; 67: 71
Typische vs. atypische pneumonie
Mycoplasma pneumoniaeChlamydophila pneumoniaeLegionella species
Virussen
Streptococcus pneumoniaeHaemophilus influenzaeMoraxella catarrhalis
Enterobacteriaceae
Legionella species
…
β-lactam antibiotica macrolidenfluoroquinolones
Atypisch Typisch
Anamnese jonge patiënten oudere patiëntengeen co-morbiditeit productieve hoestdroge hoest hoge koorts, rillingenviraal syndroom dyspneegeen pleurale pijn pleurale pijninsidieus begin plots begin
Kliniek niet altijd crepitaties crepitatiesmineure klachten consolidatie
Labo lage leucocytose hoge leucocytose geen neutrofilie neutrofilie
Radiologie wazige infiltraten alveolair vullingsbeeldinterstitiële pneumonie lobair - multilobair
Atypisch Typisch
Anamnese jonge patiënten oudere patiëntengeen co-morbiditeit productieve hoestdroge hoest hoge koorts, rillingenviraal syndroom dyspneegeen pleurale pijn pleurale pijninsidieus begin plots begin
Kliniek niet altijd crepitaties crepitatiesmineure klachten consolidatie
Labo lage leucocytose hoge leucocytose geen neutrofilie neutrofilie
Radiologie wazige infiltraten alveolair vullingsbeeldinterstitiële pneumonie lobair - multilobair
Pneumonie: kliniek vaak atypisch!
koorts + dyspnee + hoesten: 30-50%
* koorts: 30%-60%* verwardheid en bewustzijnsstoornissen: 40%* vallen: 16%* achteruitgang van ADL-functies: 10%* incontinentie: 7%* hoest vaak minder productief (dehydratatie, spierzwakte, …)* anorexie, braken, tachypnee, thoracale pijn, hypotensie,
tachycardie…
vnl. bij oudere patiënten, co-morbiditeit,…
CAP: aanbevolen onderzoeken
* Anamnese en klinisch onderzoek
* Routine laboratorium(perifeer bloedbeeld, serum electrolyten, lever- en nierfunctie)
inschatten van ernst
* Bepaling van oxygenatie (oximetrie/arteriële bloedgassen)
* RX thorax- zekerheidsdiagnose van pneumonie (caveats!)- inschatten van ernst- onderliggende aandoeningen of complicaties- geen correlatie met etiologische kiem !!
* Sputum: kleuring en cultuur= controversieel (kolonisatie / contaminatie !!)
CAP: aanbevolen onderzoeken
* Hemoculturen alle gehospitaliseerde patiënten met CAP (11% positief)
(S. pneumoniae, H. influenzae, S. aureus, K. pneumoniae)
* Serologische testen (Influenza, Para-influenza, Adeno, RSV, Mycoplasma, Chlamydia,…)
- patiënten met ernstige pneumonie- onvoldoende of geen respons op empirische therapie- specifieke epidemiologische omstandigheden
legionella antigeendetectie in urine patiënten met ernstige pneumonie alle patiënten met pneumonie bij epidemie
Scoresystemen/criteria voor beoordeling ernst CAP
BTS: CURB (1996) CURB-65 (2003)Fine: PSI (Pneumonia Severity Index) (1997)ATS: criteria for ‘severe pneumonia’Sepsis, severe sepsis, septic shockIDAB richtlijnen

Aangepaste BTS criteria“CURB-65”
Neill AM et al. Thorax 1996; 51(10):1010-6Lim WS et al. Thorax 2003;58:377-382
ConfusionUrea >7mmol/l (42 mg/dL)Respiratory rate ≥30/minBlood pressure: Psyst <90mmHg
Pdias ≤60mmHg
Age ≥65years
BTS Guidelines. Lim WS et al.Thorax 2009; 64(3); iii1-55
Resistentie in België
J. Verhaegen, referentie-laboratorium Leuven, 2014
Invasieve isolaten CAP: behandeling1. Ambulante patiënten zonder cardiopulmonaire ziekte en/of
andere risicofactoren
2. Ambulante patiënten met cardiopulmonaire ziekte en/of andere risicofactoren
3. Gehospitaliseerde patiënten, opgenomen op ‘gewone’ zaal
4. Gehospitaliseerde patiënten, opgenomen op eenheid voor Intensieve Zorgen
5. Gehospitaliseerde patiënten, opgenomen op eenheid voor Intensieve Zorgen mét risicofactoren voor infectie met P. aeruginosa
Sanford Guide to Antimicrobial Therapy 2013-2014Antibioticagids UZ Leuven 2014: www.uzleuven.be/antibioticagids

Ambulant, geen risicofactoren
Eerste keuze: amoxycilline 1 g 3x/d PO
Alternatieven:
* IgE-gemedieerde overgevoeligheid/ernstige intolerantie moxifloxacine 400 mg 1x/d PO
* Ongunstig klinisch verloop swith naar resp. FQ
of associeer neo-macrolide/azalide
Ambulant, met risicofactoren
Eerste keuze: amoxycilline-clavulaanzuur 2 g 2x/d POEerste keuze: amoxycilline-clavulaanzuur 2 g 2x/d POEerste keuze: amoxycilline-clavulaanzuur 2 g 2x/d PO
Alternatieven:
* IgE-gemedieerde overgevoeligheid/ernstige intolerantie moxifloxacine 400 mg 1x/d PO
* Ongunstig klinisch verloop swith naar resp. FQ
of associeer neo-macrolide/azalide
Opgenomen patiënten, ‘gewone zaal’
Orale behandeling mogelijk: moxifloxacine 400 mg 1x/d
Parenterale behandeling: amoxyclavulaanzuur 1 g 4x/d
IgE-gemedieerde overgevoeligheid/ernstige intolerantie moxifloxacine 400 mg 1x/d PO/IV
Ongunstig klinisch verloop switch naar resp. FQ IV
of associeer neo-macrolide IV
Opgenomen patiënten, ‘intensieve’
amoxyclavulaanzuur 1 g 4x/d IV
cefotaxime 2 g 3x/d IVceftriaxone 2 g 1x/d IV
plus
clarithromycin 500 mg 2x/d IV
moxifloxacine 400 mg 1x/d IV
ofof
clarithromycin 500 mg 2x/d IV
moxifloxacine 400 mg 1x/d IV
of

Opgenomen patiënten, P. aeruginosa
IV Antipseudomonas -lactam(cefepime, meropenem, pipera/tazobactam, ceftazidime)
IV Antipseudomonas fluoroquinolone plusplus
IV Antipseudomonas -lactam(cefepime, meropenem, pipera/tazobactam, ceftazidime)
IV Antipseudomonas fluoroquinolone plus
of
IV Antipseudomonas -lactam(cefepime, carbapenem, pipera/tazobactam, ceftazidime)
Aminoglycoside
IV clarithromycine of IV fluoroquinolone
plusplus
plusplus
IV Antipseudomonas -lactam(cefepime, carbapenem, pipera/tazobactam, ceftazidime)
Aminoglycoside
IV clarithromycine of IV fluoroquinolone
plus
plus
IV PO switch:criteria voor ‘klinische stabiliteit’
• Temperatuur ≤37,8°C• Hartritme ≤100/minuut• Bloeddruk systolisch ≥90mmHg• Ademhaling ≤24/minuut• PaO2 ≥60mmHg of SaO2 ≥90%• Normale mentale status• Orale route mogelijk
Halm EA, Fine MJ, Marrie TJ, et al. JAMA 1998; 279; 1452-1457
-lactam -lactamfluoroquinolone fluoroquinolone
cefalosporine fluoroquinolone
IV PO switch:Bio-equivalente antibiotica
Levofloxacine Tavanic®
Moxifloxacine Avelox®
Clarithromycine Biclar®
Clindamycine Dalacin®
Linezolide Zyvoxid®
Metronidazole Flagyl®
Ornidazole Tiberal®
Fluconazole Diflucan®
SMX/TMP Bactrim®, Eusaprim®
Duur van therapie met antibiotica Geen robuste data!
“tot 3 dagen koortsvrij”
Li JZ et al. Am J Med 1997; 120: 783-790BTS Guidelines. Lim WS et al. Thorax 2009; 64(3); iii1-55
5-7 dagen S. pneumoniae7-14 dagen Enterobacteriaceae
Pseudomonas aeruginosa14 dagen Staphylococci14-21 dagen Mycoplasma spp.
Chlamydophila spp.Legionella spp.

Hospital-acquired pneumonia (HAP)
= pneumonia die ontstaat ≥48u na hospitalisatie- geen incubatie op moment van opname- gewone afdeling/intensieve zorgen
Ventilator-associated pneumonia (VAP)= pneumonia die ontstaat ≥48-72u na
endotracheale intubatie
Niederman MS. Curr Opin Pulm Med 1996; 2:161-165
HAP: hoge morbiditeit en mortaliteit!
• 2de meest frequente oorzaak van nosocomiale infectie
• 5-10/1.000 hospitalisaties• 6-21voudige stijging bij geventileerde patiënten• 25% van alle ICU infecties
Chastre J. AJRCCM 2002; 163: 867-903Rello et al. Chest 2002; 122: 2121-2132
• VAP = 90% van alle HAP• incidentie stijgt met duur van ventilatie• risico is hoogst vroegtijdig in verloop van ventilatie• minder frequent bij niet-invasieve ventilatie
HAP: hoge morbiditeit en mortaliteit!
• ‘Globale’ mortaliteit voor HAP 30% - 70%
EN
‘specifieke’ mortaliteit = 33% - 50%- bacteriëmie (P. aeruginosa, Acinetobacter sp.)- medische eerder dan chirurgische pathologie- ernst van de onderliggende aandoening(en)- ‘inappropriate’ antibiotica-therapie
Heylandt et al. AJRCCM 1999; 159: 1249-1256Bregeon et al. Anesthesiology 2001; 94: 554-560
Papazian et al. AJRCCM 1996; 154: 91-97
CAP/HAP: microbiologie

HAP: microbiologie
Chastre J, Fagon JY. AJRCCM 2002; 165(7): 867–903
HAP: belang van tijdstip van ontstaan
• ‘Early-onset’ HAP/VAP= ontstaan binnen de eerste 7 dagen
na hospitalisatie/ventilatie
• ‘Late-onset’ HAP/VAP= ontstaan na 7 dagen na
hospitalisatie of ventilatie
≈ ‘early-onset’ HAP/VAP met voorafantibiotica/hospitalisatie (90d.)
HAP: belang van tijdstip van ontstaan HAP: diagnostische strategieHAP/VAP or HCAP suspectedHAP/VAP or HCAP suspected
Lower respiratory tract sample for culture and microscopyLower respiratory tract sample for culture and microscopy
Unless there is both a low clinical suspicion for pneumonia & negative microscopy of LRT sample, start empiric antimicrobial therapy
Unless there is both a low clinical suspicion for pneumonia & negative microscopy of LRT sample, start empiric antimicrobial therapy
Days 2-3: Check cultures & assess clinical response:(Temp., WBC, Chest X-ray, Oxygenation, Purulent sputum, Hemodynamic changes and Organ
function)
Days 2-3: Check cultures & assess clinical response:(Temp., WBC, Chest X-ray, Oxygenation, Purulent sputum, Hemodynamic changes and Organ
function)
Clincal improvement at 48-72 hoursClincal improvement at 48-72 hours
NONO
Adjust AB therapy, Search for other pathogens, Complications, Other diagnosies or Other sites of
infection
Adjust AB therapy, Search for other pathogens, Complications, Other diagnosies or Other sites of
infection
YESYES
Cultures -Cultures -
Stop ABStop AB
Cultures +Cultures +
De-escalalate AB if possible.
Treat selected pts for 7-8d.
De-escalalate AB if possible.
Treat selected pts for 7-8d.
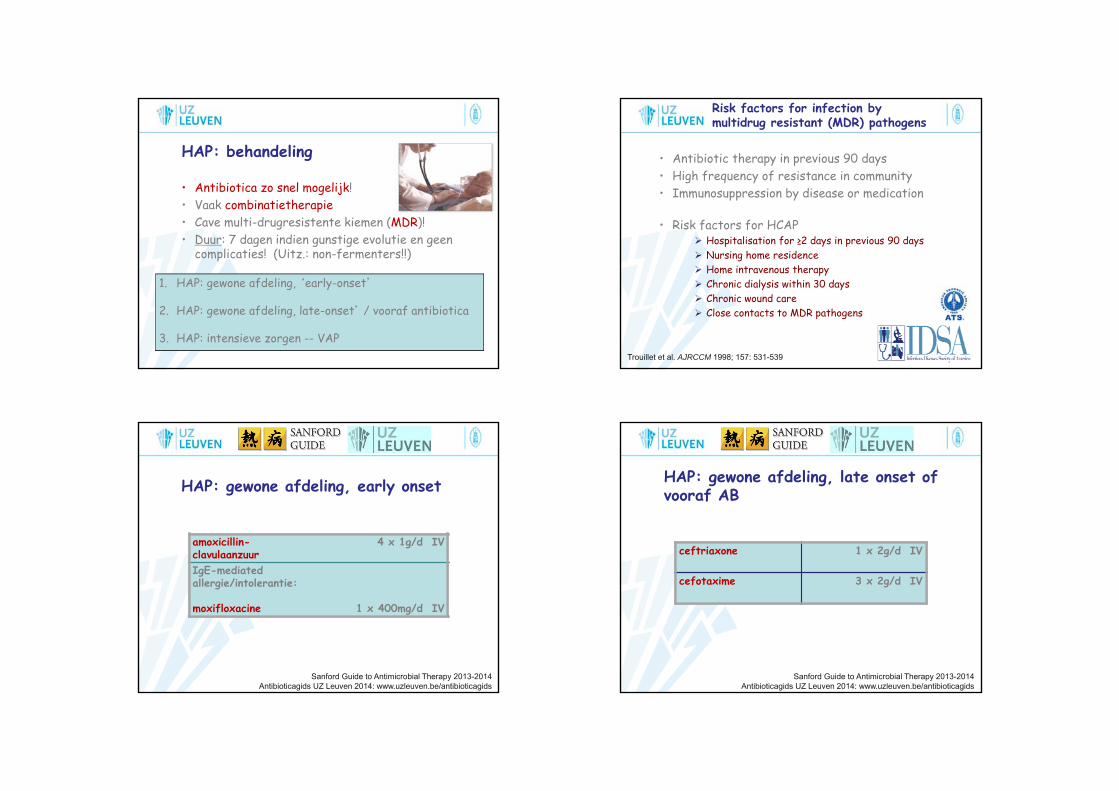
HAP: behandeling
• Antibiotica zo snel mogelijk!• Vaak combinatietherapie• Cave multi-drugresistente kiemen (MDR)!• Duur: 7 dagen indien gunstige evolutie en geen
complicaties! (Uitz.: non-fermenters!!)
1. HAP: gewone afdeling, ‘early-onset’
2. HAP: gewone afdeling, late-onset’ / vooraf antibiotica
3. HAP: intensieve zorgen -- VAP
Risk factors for infection by multidrug resistant (MDR) pathogens
• Antibiotic therapy in previous 90 days• High frequency of resistance in community• Immunosuppression by disease or medication
• Risk factors for HCAP Hospitalisation for ≥2 days in previous 90 days Nursing home residence Home intravenous therapy Chronic dialysis within 30 days Chronic wound care Close contacts to MDR pathogens
Trouillet et al. AJRCCM 1998; 157: 531-539
HAP: gewone afdeling, early onset
amoxicillin-clavulaanzuur
4 x 1g/d IV
IgE-mediatedallergie/intolerantie:
moxifloxacine 1 x 400mg/d IV
Sanford Guide to Antimicrobial Therapy 2013-2014Antibioticagids UZ Leuven 2014: www.uzleuven.be/antibioticagids
HAP: gewone afdeling, late onset of vooraf AB
ceftriaxone 1 x 2g/d IV
cefotaxime 3 x 2g/d IV
Sanford Guide to Antimicrobial Therapy 2013-2014Antibioticagids UZ Leuven 2014: www.uzleuven.be/antibioticagids

HAP: intensieve zorgen -- VAP
cefepime 3 x 2g/d IV
meropenem 3 x 1g/d IV
piperacillin/tazobactam 4 x 4g/d IV
ceftazidim 3 x 2g/d IV
PLUS (MIN)
amikacine(of anti-Ps. fluoroquinolone)
1 x 1g/d IV
PLUS vancomycine (indien hoge prevalentie van MRSA)
Sanford Guide to Antimicrobial Therapy 2013-2014Antibioticagids UZ Leuven 2014: www.uzleuven.be/antibioticagids
Complicaties van pneumonie
• Pneumonie met abnormaal verloop- klinisch- radiologisch
• Ernstige pneumonie, leidend tot orgaanfalen
• Infectieuse complicaties van pneumonie
• Niet-infectieuse complicaties van pneumonie
Pneumonie met abnormaal verloop
Geen éénduidige definitie !! klinische evolutie
- koorts – CRP - Wbc 2- 4 dagen- respiratoire klachten 4- 9 dagen- auscultatoire tekens 3-14 dagen- radiologische afwijkingen 2- 4 weken
radiologische evolutie= meest gebruikte parameter in literatuur
‘slow’/’non-resolving’ pneumonia<50% of geen verbetering na één maand
Abnormaal verloop: oorzaken...
1. Niet-bacteriële etiologie- mycobacteriën (m. tuberculosis, NTM)- schimmels (Aspergillus spp., …)- nocardia/actinomyces- viraal, …
2. Resistente kiemen- S. pneumoniae (DRSP)- MRSA, P. aeruginosa, aërobe Gram- bacillen,…
3. Infectieuze complicaties- gecompliceerde parapneumonische effusie, empyeem- abcedatie- metastatische infecties, …

Abnormaal verloop: oorzaken...
4. Gastheerfactoren- structurele longaandoeningen (bronchiëctasieën, tumor,…)- immuunsuppressie, …
5. Niet-infectieuze etiologie (20%)- maligniteit- collageen-vasculaire ziekten- BOOP- hypersensitiviteitspneumonitis- medicamenteus of toxisch longlijden- longembolie, longinfarct, longbloeding- longoedeem- radiatie-pneumonitis- ARDS
Abnormaal verloop: diagnostiek
* grondige heranamnese en klinisch onderzoek
* aanvullende biochemische testen inflammatoire parameters, auto-immuunserologie,…
* beeldvorming RX thorax – (HR)CT thorax – Echo thorax
* bronchoscopie washing, broncho-alveolaire lavage, biopsies
* pleurapunctie
* longbiopsie
* V/Q-scan, arteriografie, zweettest, …
Ernstige pneumonie orgaanfalen
Opname op intensieve zorgen
* kunstmatige ventilatie 50%-88%
* septische shock 10%-42%
* acuut nierfalen 30%-42%
* andere mentale verwardheid metastatische infectie acuut hartfalen ...
Pleuravocht punctie!
Stages Macroscopicappearance
Pleural fluidcharacteristics
Comments
Simpleparapneumonic
Clear fluid pH>7.2LDH<1000Glucose>30
Antibiotics(Drain if requiredon symptomatic
grounds)
Complicatedparapneumonic(fibrinopurulent)
Clear fluid
Cloudy/turbid
pH<7.2LDH>1000Glucose<30
Gram/cult. +/-
Chest tube drainage (+ …)
Empyema Frank pus Gram/cult. +/-
No other tests required
Chest tube drainage (+ …)
Surgery
Davies CWH. Thorax 2003

Pleuravocht/empyeem: behandeling
• Antibiotica- intraveneus / empyeem: langere duur (cf. longabces)
• Thoraxdrainage etter pH < 7,2 aanwezigheid van micro-organismen
bij etter best brede drain (Ch.28-32), in suctie spoeling noodzakelijk bij dunne drains
• GEEN NUT: seriële puncties, fibrinolytica (tenzij…!!!)
• Chirurgie zo onvoldoende effect na 3(-5) dagen!
Pulmonaryembolism
Pascal Van BleyenberghDepartment of Pulmonology, UZ Leuven
103
Asymptomatic
Epidemiology difficult to determine
104
Sudden death
• Increased risk if >40years (risk x2 with each decade)
• Deaths 34% sudden fatal PE 59% PE undiagnosed during life
• Provoked >< unprovoked
• Risk factors - patient-related- setting-related
Cohen AT et al. Thromb Haemost 2007; 98: 756-764
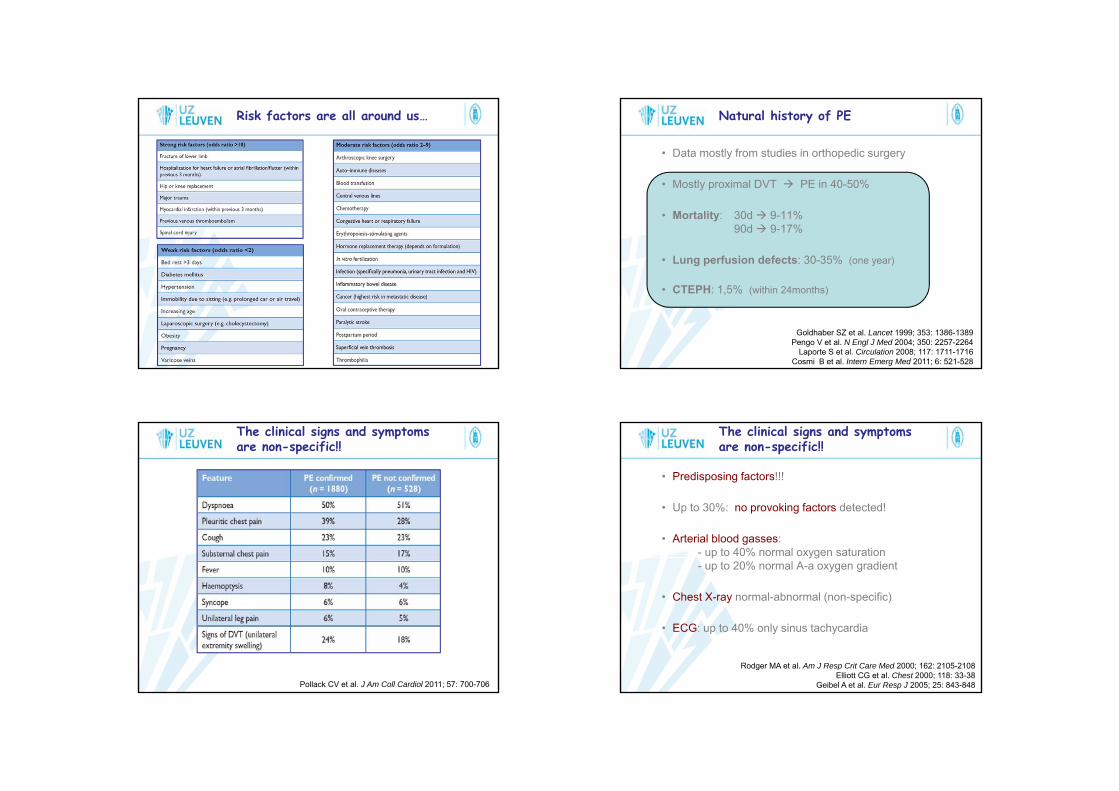
Risk factors are all around us…
105
• Data mostly from studies in orthopedic surgery
• Mostly proximal DVT PE in 40-50%
• Mortality: 30d 9-11%90d 9-17%
• Lung perfusion defects: 30-35% (one year)
• CTEPH: 1,5% (within 24months)
Natural history of PE
106
Goldhaber SZ et al. Lancet 1999; 353: 1386-1389Pengo V et al. N Engl J Med 2004; 350: 2257-2264
Laporte S et al. Circulation 2008; 117: 1711-1716Cosmi B et al. Intern Emerg Med 2011; 6: 521-528
The clinical signs and symptomsare non-specific!!
107Pollack CV et al. J Am Coll Cardiol 2011; 57: 700-706
• Predisposing factors!!!
• Up to 30%: no provoking factors detected!
• Arterial blood gasses:- up to 40% normal oxygen saturation- up to 20% normal A-a oxygen gradient
• Chest X-ray normal-abnormal (non-specific)
• ECG: up to 40% only sinus tachycardia
The clinical signs and symptomsare non-specific!!
108
Rodger MA et al. Am J Resp Crit Care Med 2000; 162: 2105-2108Elliott CG et al. Chest 2000; 118: 33-38
Geibel A et al. Eur Resp J 2005; 25: 843-848

Initial assessment: early mortality?
109
Key step in all diagnostic algorithms
Clinical or pre-test probability
110
Clinical judgement
Clinical prediction rules1. WELLS2. GENEVA
Clinical prediction rule: WELLS
111Wells PS et al. Thromb Haemost 2000; 83: 416-420
Gibson NS et al. Thromb Haemost 2008; 99: 229-234
Clinical prediction rule: GENEVA
112Le Gal G et al. Ann Intern Med 2006; 144: 135-171
Klok FA et al. Ann Intern Med 2008; 168: 2131-2136

Diagnostic algorithm “high-risk”
113
Diagnostic algorithm “low-risk”
114
Prognostic assessment: PESI score
115
Aujesky D et al. Am J Resp Crit Care Med 2005; 172: 1041-1046
Jimenez D et al. Arch Intern Med2010; 170: 1383-1389
Classification of pts with acute PE based on early mortality risk
116
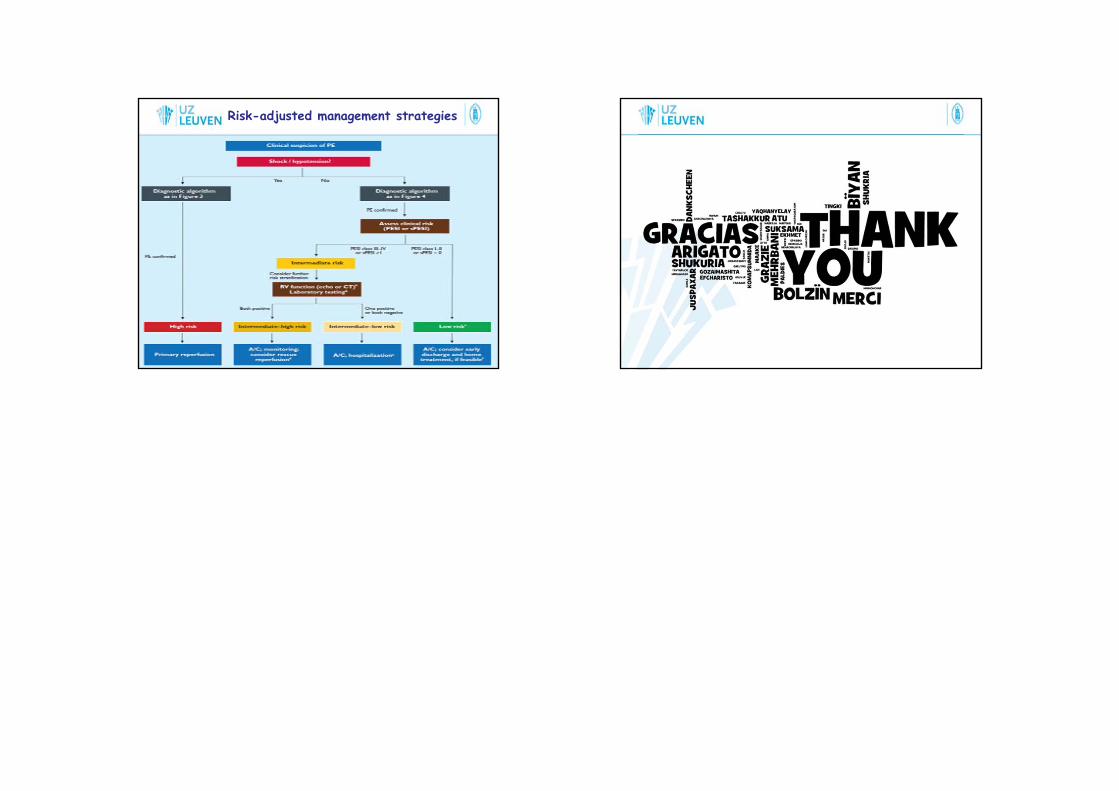
Risk-adjusted management strategies
117 118