the abcs of acg - university of waterloo | university of ... · to compare peripheral anterior...
TRANSCRIPT

The ABCs of ACGCOPE Course ID: 61470-GL
Sarah MacIver, OD, FAAODerek MacDonald, OD, FAAO
WOVS CE 2019June 14 2019
UW School of Optometry and Vision Science
Financial DisclosuresHonoraria: Alcon (DM)
Allergan (DM)Carl Zeiss Meditec (DM)Eye Recommend (DM)
The content and format of this course is presented without commercial bias and does not claim superiority of anycommercial product or service

Epidemiology
Glaucoma is the second leading cause of blindness worldwide
• estimated to affect 80 million people by 20201
Primary angle-closure glaucoma (PACG):
• represents ~25% of all cases of glaucoma2
• nearly 20 million will be affected by 2020
• is responsible for a disproportionate amount of severe
vision loss
• nearly 50% of the cases of glaucoma-related blindness3
• risk of blindness is 4x greater in ACG than in OAG4
1. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 2006;90:262-7.
2. He M, et al. Laser peripheral iridotomy for the prevention of angle closure. Lancet 2019;doi.org/10.1016/S0140-6736(18)32607-2.
3. Quigley HA. The number of people with glaucoma worldwide. Br J Ophthalmol 1996;80:389-93.
4. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.
Risk factors
Advancing age
• nearly 50x more common for ages ≥70 versus <501
• lens thickens, chamber depth decreases, angle narrows
• PACG at an age <40 tend to be plateau iris2
1. Day AC, et al. The prevalence of primary angle closure glaucoma in European derived population: a systematic review. Br J Ophthalmol 2012;96:1162-7.2. Ritch R, et al. Angle closure in younger patients. Ophthalmology 2003;110:1880-9.3. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 2006;90:262-7.4. Foster PJ, Johnson GJ. Glaucoma in China: how big is the problem? Br J Ophthalmol 2001;85:1277-85.5. Arkell SM, et al. The prevalence of glaucoma among Eskimos of northwest Alaska. Arch Ophthalmol 1987;105:482-5.
Female sex
• 3 to 5x more common in women than men3
• smaller eyes, narrower angles, longer lifespans
Asian ethnicity
• nearly 50% of people with PACG are found in China4
• ~90% of glaucoma-related blindness in Asia is due to PACG
• PACG prevalence is highest in the Inuit population5
• up to 50x more common in Inuit than in Europeans

Risk factors
Ocular biometry• hyperopia: short axial length, shallow anterior chamber
depth, small cornea, thicker and more anterior lens2
1. Amerasinghe N, et al. The heritability and sibling risk of angle closure in Asians. Ophthalmology 2011;118:480-5.2. Lee DA, et al. Anterior chamber dimensions in patients with narrow angles and angle-closure glaucoma. Arch Ophthalmol 1984;102:46-50.3. Tarongoy P, et al. Angle-closure glaucoma: the role of the lens in the pathogenesis, prevention, and treatment. Surv Ophthalmol 2009;54:211-25.4. Salmon JF. Predisposing factors for chronic angle-closure glaucoma. Prog Ret Eye Res 1998;18:121-32.5. Wright C, et al. Primary angle-closure glaucoma: an update. Acta Ophthalmol 2016;94:217-25.
Crystalline lens size, shape, and position• all ages: thicker and/or more anteriorly positioned3
• advancing age: thickening exacerbates angle crowding4
Family history• up to 7x more common in siblings of Asians with PACG1
Exfoliation• lax zonules: anterior lens shift and angle crowding5

Diagnosis
1. Thomas R, Walland MJ. Management algorithms for primary angle closure disease. Clin Experiment Ophthalmol 2013;41:282-92.2. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.
“The current gold standard for the detection of [primary angle closure] is still gonioscopy, and the importance of routine gonioscopy in a clinical situation cannot be overstated.”1
Gonioscopy:• differentiates open angle from angle closure glaucoma• differentiates primary from secondary glaucoma
In angle closure glaucoma, gonioscopy:• detects iridotrabecular contact (ITC, the hallmark of PACG)2
• compression/indentation gonioscopy:• differentiates appositional from synechial closure• helps detect plateau iris
For an excellent reference, visit

diagnosis
Despite being essential, gonioscopy is very underutilized
by both optometrists and ophthalmologists
1. Coleman AL, et al. Use of gonioscopy in Medicare beneficiaries before glaucoma surgery. J Glaucoma 2006;15:486-93.2. Varma DK, et al. Proportion of undetected narrow angles or angle closure in cataract surgery referrals. Can J Ophthalmol 2017;52:366072.3. Varma DK, et al. Undetected angle closure in patients with a diagnosis of open-angle glaucoma. Can J Ophthalmol 2017;52:373-8.4. American Academy of Ophthalmology Glaucoma Panel. Preferred Practice Pattern Guidelines. Primary Angle Closure. San Francisco: AAO; 2015.
Gonioscopy is performed less than half the time
in the 5 years preceding glaucoma surgery1
As many as one in eight patients referred for CE
(by both ODs and OMDs) have undocumented narrow angles2
75% of referrals by OMDs for tertiary glaucoma care did not
include angle status …
… and one in ten patients referred for POAG had PACG3
4

For 50 years, Van Herick angle assessment (VHA) has been used to compare peripheral anterior chamber depth to peripheral corneal thickness in the screening of non-glaucomatous patients1
• an angle is felt to be “open” when peripheral chamber depth is >1/4 peripheral corneal thickness
1. Van Herick W, et al. Estimation of width of angle of anterior chamber: incidence and significance of the narrow angle. Am J Ophthalmol 1969;68:626-9.2. Johnson TV, et al. Low sensitivity of the Van Herick method for detecting gonioscopic angle closure independent of observer expertise. Am J Ophthalmol
2018;195:63-71.
However:• VHA cannot detect synechiae or secondary mechanisms• inter-examiner sensitivity and specificity vary widely• VHA fails to detect as many as 40% of angles judged to be
narrow by gonioscopy2
“… clinical assessment of anterior chamber angleconfiguration is best accomplished with gonioscopy …”
diagnosis

DiagnosisPerforming indirect gonioscopy with a 4-mirror corneal lens1. Instil anesthetic in both eyes2. Place the lens on the cornea• the patient may initially look up, then straight ahead
3. Use low ambient lighting and a short narrow beam• avoid pupil constriction, which can deepen the angle
4. Begin with the superior mirror and proceed clockwise• inferior angle tends to be deepest and most pigmented,
making angle structures easier to identify5. Use mid- to high magnification to identify angle details6. Tilt the lens toward the angle to “look over” a steep iris• tilt toward any bubbles to eliminate them
7. Indent to differentiate appositional from synechial closure
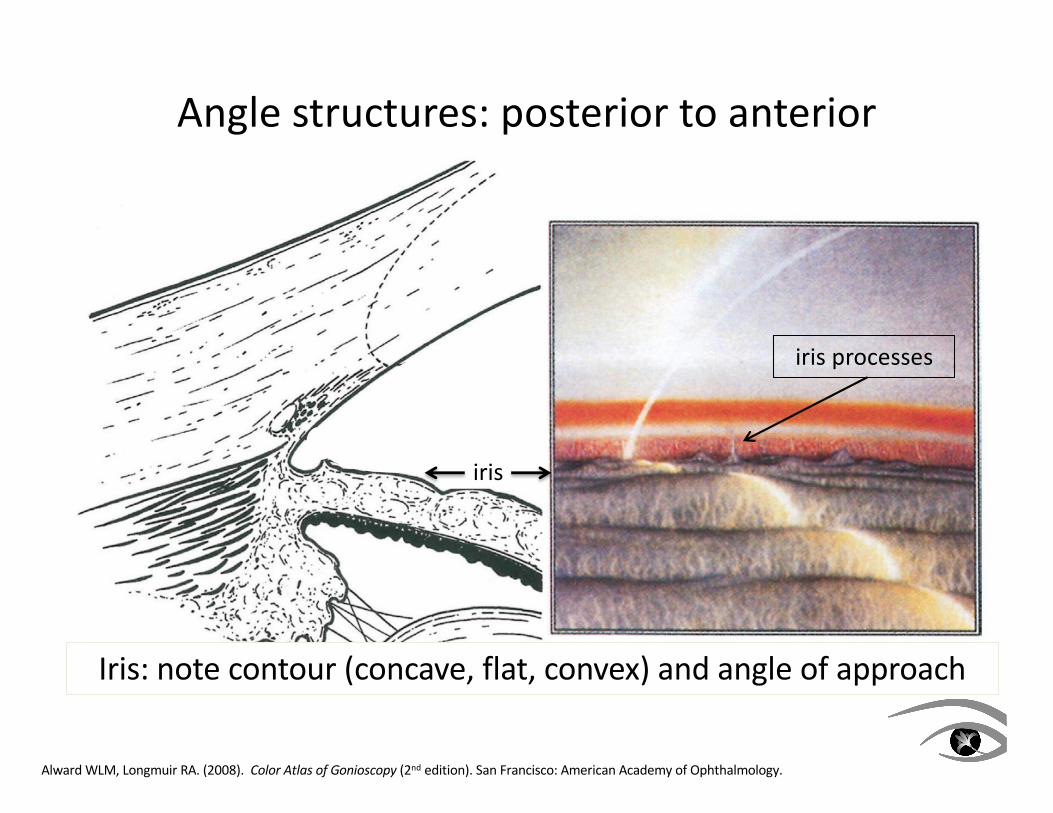
Angle structures: posterior to anterior
iris
Alward WLM, Longmuir RA. (2008). Color Atlas of Gonioscopy (2nd edition). San Francisco: American Academy of Ophthalmology.
iris processes
Iris: note contour (concave, flat, convex) and angle of approach

CB
Alward WLM, Longmuir RA. (2008). Color Atlas of Gonioscopy (2nd edition). San Francisco: American Academy of Ophthalmology.
Ciliary body (CB): pink/brown/grey band at iris root
Angle structures: posterior to anterior

SS
Alward WLM, Longmuir RA. (2008). Color Atlas of Gonioscopy (2nd edition). San Francisco: American Academy of Ophthalmology.
Scleral spur (SS; insertion of ciliary muscle): white band between CB and TM (obscured by benign iris processes or pathologic PAS)
Angle structures: posterior to anterior

PTM
Alward WLM, Longmuir RA. (2008). Color Atlas of Gonioscopy (2nd edition). San Francisco: American Academy of Ophthalmology.
Posterior (pigmented) trabecular meshwork (PTM): functional two-thirds of TM; visibility suggests angle open in that quadrant
Angle structures: posterior to anterior

ATM
Alward WLM, Longmuir RA. (2008). Color Atlas of Gonioscopy (2nd edition). San Francisco: American Academy of Ophthalmology.
Anterior trabecular meshwork (ATM): non- or lightly pigmented
(and non-functional) anterior one-third of TM
Angle structures: posterior to anterior

SL
Alward WLM, Longmuir RA. (2008). Color Atlas of Gonioscopy (2nd edition). San Francisco: American Academy of Ophthalmology.
corneal wedge
Schwalbe line (SL; termination of Descemet membrane): fine line; variable pigmentation (Sampaolesi line); suggests narrow angle
Angle structures: posterior to anterior

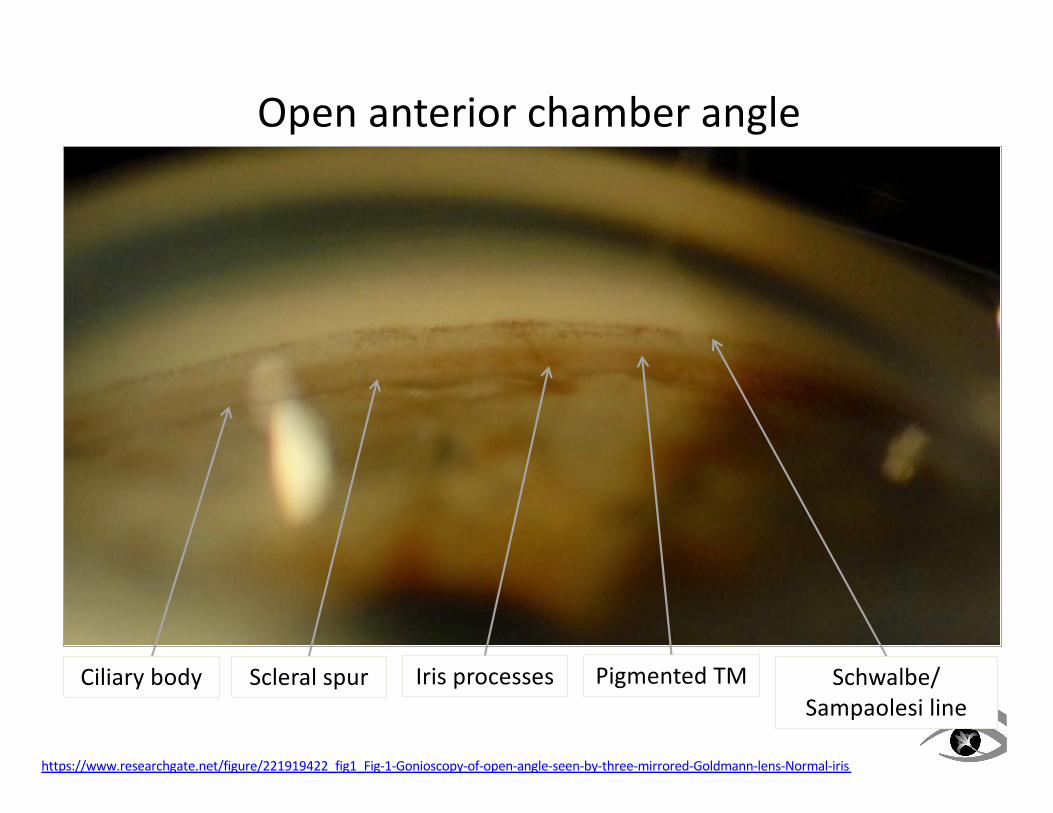
Open anterior chamber angle
Ciliary body Iris processes Scleral spur Pigmented TM
https://www.researchgate.net/figure/221919422_fig1_Fig-1-Gonioscopy-of-open-angle-seen-by-three-mirrored-Goldmann-lens-Normal-iris
Schwalbe line

Open anterior chamber angle
Ciliary body Scleral spur Pigmented TM
https://www.researchgate.net/figure/221919422_fig1_Fig-1-Gonioscopy-of-open-angle-seen-by-three-mirrored-Goldmann-lens-Normal-iris
Schwalbe line
Open anterior chamber angle
Ciliary body Scleral spur Iris processes Pigmented TM
https://www.researchgate.net/figure/221919422_fig1_Fig-1-Gonioscopy-of-open-angle-seen-by-three-mirrored-Goldmann-lens-Normal-iris
Schwalbe/Sampaolesi line

DiagnosisIndentation gonioscopy
If the posterior TM is not visible, the angle is narrow or closed• ITC may be appositional or synechial1
• indentation will not open an angle closed by PAS• appositional closure (+/- iris processes) will open
A pigmented appositionally-closed angle opens with indentation
1. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.

Asia-Pacific Glaucoma Society, 2016
Posterior TM (more conservative)
Interpretation of gonioscopy

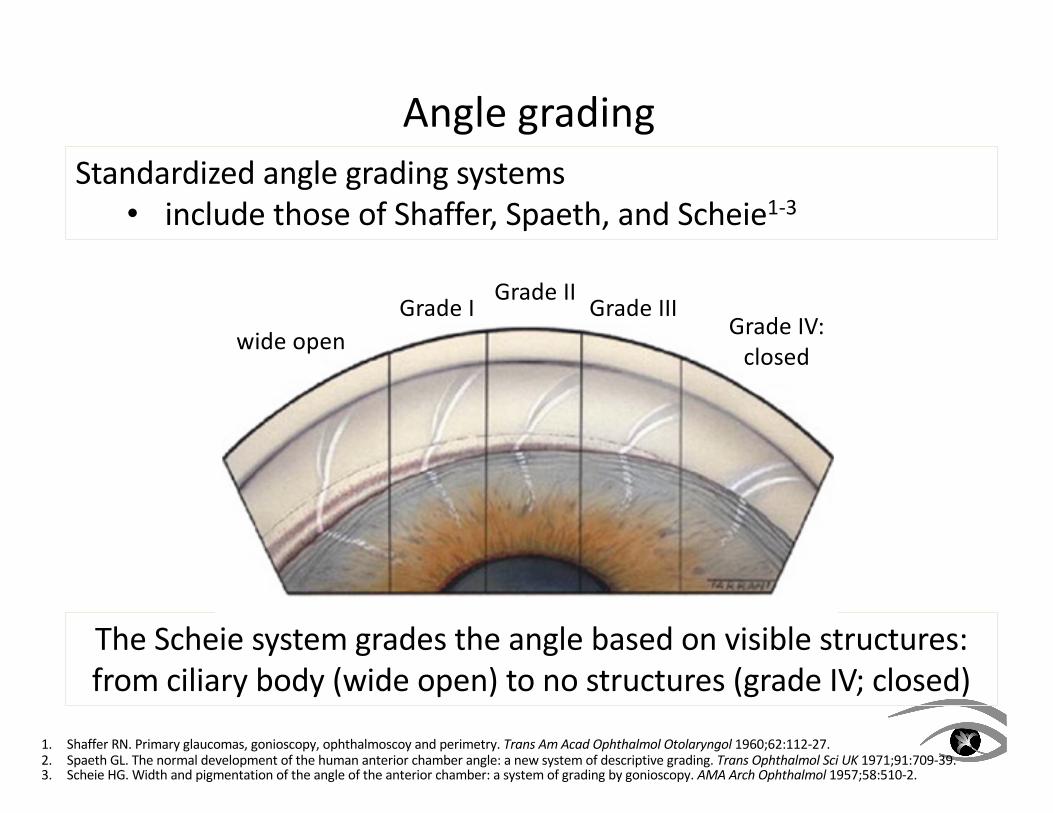
Angle gradingStandardized angle grading systems• include those of Shaffer, Spaeth, and Scheie1-3
1. Shaffer RN. Primary glaucomas, gonioscopy, ophthalmoscoy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 1960;62:112-27.2. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Sci UK 1971;91:709-39.3. Scheie HG. Width and pigmentation of the angle of the anterior chamber: a system of grading by gonioscopy. AMA Arch Ophthalmol 1957;58:510-2.
The Shaffer system is based on the angle between iris and cornea:closure is unlikely at >20°, possible at <20°, and likely at <10°

Angle gradingStandardized angle grading systems• include those of Shaffer, Spaeth, and Scheie1-3
1. Shaffer RN. Primary glaucomas, gonioscopy, ophthalmoscoy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 1960;62:112-27.2. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Sci UK 1971;91:709-39.3. Scheie HG. Width and pigmentation of the angle of the anterior chamber: a system of grading by gonioscopy. AMA Arch Ophthalmol 1957;58:510-2.
The Spaeth system is a complex extension of the Shaffer system:also describes iris contour (top right) and insertion (bottom)

Angle grading
1. Shaffer RN. Primary glaucomas, gonioscopy, ophthalmoscoy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 1960;62:112-27.2. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Sci UK 1971;91:709-39.3. Scheie HG. Width and pigmentation of the angle of the anterior chamber: a system of grading by gonioscopy. AMA Arch Ophthalmol 1957;58:510-2.
Standardized angle grading systems• include those of Shaffer, Spaeth, and Scheie1-3
The Scheie system grades the angle based on visible structures: from ciliary body (wide open) to no structures (grade IV; closed)

Angle grading
1. Shaffer RN. Primary glaucomas, gonioscopy, ophthalmoscoy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 1960;62:112-27.2. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Sci UK 1971;91:709-39.3. Scheie HG. Width and pigmentation of the angle of the anterior chamber: a system of grading by gonioscopy. AMA Arch Ophthalmol 1957;58:510-2.
Standardized angle grading systems• include those of Shaffer, Spaeth, and Scheie1-3
The Scheie system grades the angle based on visible structures: from ciliary body (wide open) to no structures (grade IV; closed)

Angle grading
1. Shaffer RN. Primary glaucomas, gonioscopy, ophthalmoscoy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 1960;62:112-27.2. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Sci UK 1971;91:709-39.3. Scheie HG. Width and pigmentation of the angle of the anterior chamber: a system of grading by gonioscopy. AMA Arch Ophthalmol 1957;58:510-2.
Standardized angle grading systems• include those of Shaffer, Spaeth, and Scheie1-3
The Scheie system grades the angle based on visible structures: from ciliary body (wide open) to no structures (grade IV; closed)
Angle grading
1. Shaffer RN. Primary glaucomas, gonioscopy, ophthalmoscoy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 1960;62:112-27.2. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Sci UK 1971;91:709-39.3. Scheie HG. Width and pigmentation of the angle of the anterior chamber: a system of grading by gonioscopy. AMA Arch Ophthalmol 1957;58:510-2.
Standardized angle grading systems• include those of Shaffer, Spaeth, and Scheie1-3
The Scheie system grades the angle based on visible structures: from ciliary body (wide open) to no structures (grade IV; closed)
wide openGrade I
Grade IIGrade III
Grade IV:closed

Angle gradingStandardized angle grading systems• include those of Shaffer, Spaeth, and Scheie1-3
• a modified Scheie system may be most clinically useful:• in each quadrant, specify the most posterior visible
angle structure, and a qualitative description of iris approach and any abnormalities (PAS, pigment, etc.)
1. Shaffer RN. Primary glaucomas, gonioscopy, ophthalmoscoy and perimetry. Trans Am Acad Ophthalmol Otolaryngol 1960;62:112-27.2. Spaeth GL. The normal development of the human anterior chamber angle: a new system of descriptive grading. Trans Ophthalmol Sci UK 1971;91:709-39.3. Scheie HG. Width and pigmentation of the angle of the anterior chamber: a system of grading by gonioscopy. AMA Arch Ophthalmol 1957;58:510-2.
ATMflat
trace TM pig
CBflat
sig TM pigiris processes
PTMflat
mod TM pig
PTMflat
mod TM pig
no SLflat
SLflat
SLflat
ATMflat
single PAS

Ancillary diagnostic procedures
1. American Academy of Ophthalmology Glaucoma Panel. Preferred Practice Pattern Guidelines. Primary Angle Closure. San Francisco: AAO; 2015.2. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.3. Nongpiur ME, et al. Angle closure glaucoma: a mechanistic review. Curr Opin Ophthalmol 2011;22:96-101.
Anterior segment optical coherence tomography
• most common technique in current clinical practice1
• helpful if gonioscopy is difficult/inconclusive2
• helpful in the detection of plateau iris
• poor visualization of structures posterior to iris
• quantification of AC width, area, volume (all less in ACG)
• quantification of lens vault (predisposes to pupillary block)3

PreventionGiven that the pathophysiology of PACG is solely IOP elevation
secondary to mechanical obstruction of the TM,PACG is a preventable disease
if the angle closure can be halted in the early stages1
1. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.
Identifying those patients at risk is of paramount importance given the risk of significant vision loss
ClassificationPrimary angle closure suspect (PACS):• at least 180° of iridotrabecular contact (ITC) on gonioscopy• posterior (pigmented) TM not visible ≥180°
• normal IOP and no glaucomatous optic neuropathy (GON)1
Progression of PACS is variable:• 5 to 25% progress to PAC (develop IOP elevation and/or
peripheral anterior synechiae) within 5 to 6 years2,3
• exacerbated by (topical/systemic) pupil dilation4
of both angle and IOP is indicated• routine prophylactic laser peripheral iridotomy (LPI) is
indicated, but may be considered in patients at higher-risk (ITC ≥270°) or requiring routine pupil dilation5,6
1. Foster PJ, et al. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol 2002;86:238-42.2. Thomas R, et al. Five year risk of progression of primary angle closure suspects to primary angle closure: a population based study. Br J Ophthalmol 2003;87:450-4.3. He M, et al. Laser peripheral iridotomy for the prevention of angle closure. Lancet 2019;doi.org/10.1016/S0140-6736(18)32607-2.4. American Academy of Ophthalmology Glaucoma Panel. Preferred Practice Pattern Guidelines. Primary Angle Closure. San Francisco: AAO; 2015.5. Thomas R, Walland MJ. Management algorithms for primary angle closure disease. Clin Experiment Ophthalmol 2013;41:282-92.6. Weinreb RN, Moghimi S. Prophylactic laser iridotomy in primary angle-closure suspects. Lancet 2019;doi.org/10.1016/S0140-6736(18)33059-9.
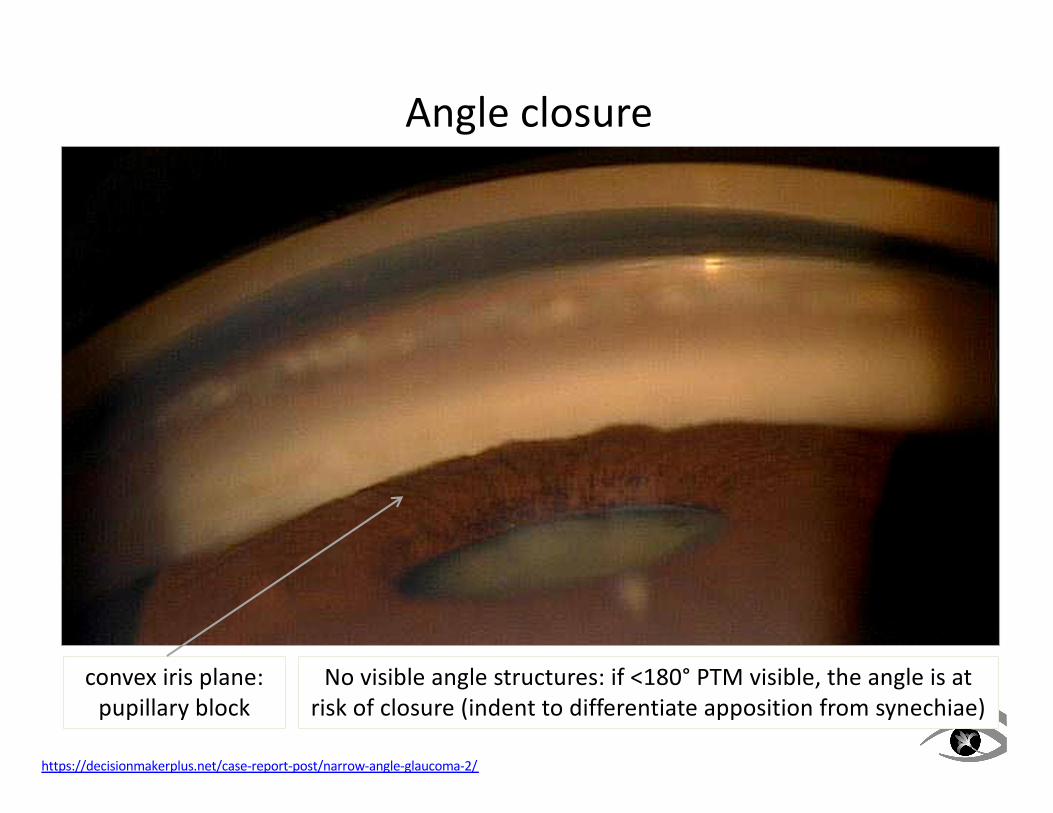
Angle closure
convex iris plane:
pupillary block
https://decisionmakerplus.net/case-report-post/narrow-angle-glaucoma-2/
No visible angle structures: if <180° PTM visible, the angle is at
risk of closure (indent to differentiate apposition from synechiae)

ClassificationPrimary angle closure (PAC):• an “intermediate stage” with at least 180° of ITC, elevated
IOP (≥21mmHg) and/or PAS, but no GON1
• asymptomatic, but evidence of TM dysfunction2
• not secondary to any other cause or concurrent disease
is recommended• may require adjunctive medical (similar to OAG) and/or
surgical treatment to adequately control IOP4
• a visually significant cataract should be removed
PAC can progress:• ~30% of PAC progressed to PACG over 5 years3
1. Foster PJ, et al. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol 2002;86:238-42.2. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.3. Thomas R, et al. Five year risk of progression of primary angle closure to primary angle closure glaucoma: a population based study. Acta Ophthalmol Scand
2003;81:480-5.4. Emanuel ME, et al. Evidence-based management of primary angle closure glaucoma. Curr Opin Ophthalmol 2014;25:89-92.

Peripheral anterior synechiae
https://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/Peripheral-anterior-synechiae.htm
Following prolonged appositional closure, peripheral anterior synechiae (PAS; broad adhesions between the iris and angle structures, often anterior to TM) can form

Iris processes versus PAS
Normal iris processes: fine strands of peripheral iris that do not cross the TM
Indentation gonioscopy
https://www.slideshare.net/suneelnarahari/gonioscopynew
Pathologic PAS: broad areas of adhesion of iris to/anterior to TM, often superiorly
ClassificationPrimary angle closure glaucoma (PACG):• PAC becomes PACG with evidence of GON1
• angle closure is more commonly chronic (slow insidious closure) or intermittent, rather than acute• chronic PACG is usually asymptomatic (much like OAG)2
• in the absence of gonioscopy, misdiagnosed as OAG
1. Foster PJ, et al. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol 2002;86:238-42.2. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.3. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.
Because of its relatively slow and insidious clinical course, the optic neuropathy of PACG can also be similar to that of POAG:• NRR loss violating ISNT Rule; vessel baring; βPPA• however, PACG may have more severe central visual
field loss and more inter-eye asymmetry3

Classificationof PACG recommended:
• augmented by medical treatment similar to OAG1
• pilocarpine (and to a lesser extent, brimonidine) cause pupillary miosis, reopening the angle
2,3
1. Emanuel ME, et al. Evidence-based management of primary angle closure glaucoma. Curr Opin Ophthalmol 2014;25:89-92.2. Thomas R, Walland MJ. Management algorithms for primary angle closure disease. Clin Experiment Ophthalmol 2013;41:282-92.3. Zarnowski T, Harasymowycz P. Management algorithms for primary angle closure disease: response. Clin Experiment Ophthalmol 2013;41:400-1.

Classification
• leads to a sudden and dramatic elevation in IOP• often ≥70mmHg• signs/symptoms: pain, headache, corneal edema, blur,
haloes, redness, nausea/vomiting, mid-dilated pupil• significant and permanent vision loss can occur rapidly1
Following an AACC attack, patients may be left with:• pigmented anterior chamber precipitates• irregular iris atrophy• glaukomflecken (anterior lens opacities)
Some patients present with mild (incomplete) angle closure attacks, characterized by similar but less serious symptoms:
these may be considered “warning signs” of impending AACC2
1. Emanuel ME, et al. Evidence-based management of primary angle closure glaucoma. Curr Opin Ophthalmol 2014;25:89-92.2. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.

Acute angle closure crisis
https://www.nejm.org/doi/full/10.1056/NEJMicm1712742
Classic signs of AACC, including:• vascular congestion, mid-dilated pupil, and corneal edema
with symptoms of pain, nausea/vomiting, and blur/haloes
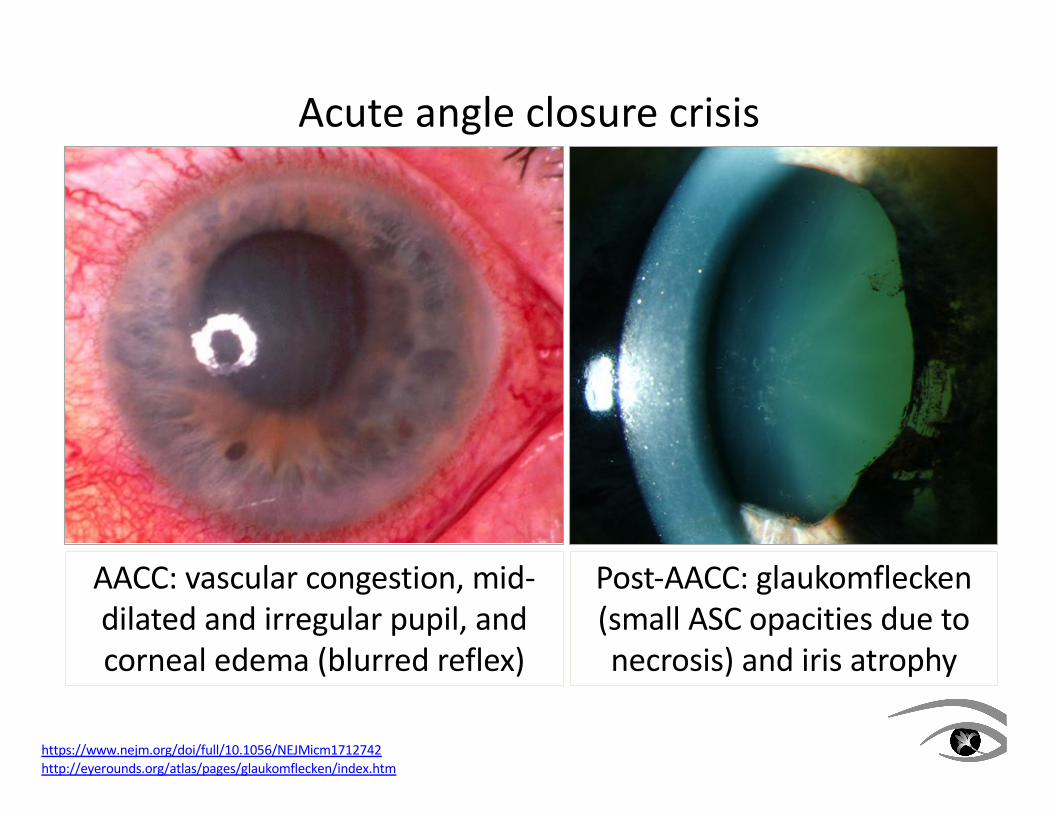
Acute angle closure crisis
https://www.nejm.org/doi/full/10.1056/NEJMicm1712742http://eyerounds.org/atlas/pages/glaukomflecken/index.htm
AACC: vascular congestion, mid-dilated and irregular pupil, and corneal edema (blurred reflex)
Post-AACC: glaukomflecken(small ASC opacities due to necrosis) and iris atrophy

Classificationof AACC essential:
1
The optic neuropathy following acute angle closure may resemble that of anterior ischemic optic neuropathy more than POAG:• pale disc with relatively shallow cupping2
PACG, whether chronic or acute, is a bilateral disease:• treatment of the fellow eye (prophylactic LPI) is critical• untreated, 50% will develop AACC within 25 years3
1. Emanuel ME, et al. Evidence-based management of primary angle closure glaucoma. Curr Opin Ophthalmol 2014;25:89-92.2. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.3. Lowe RF. Primary angle-closure glaucoma: prevention and early treatment. Isr J Med Sci 1972;8:1362-5.

Emergency treatment of AACC
1. American Academy of Ophthalmology Glaucoma Panel. Preferred Practice Pattern Guidelines. Primary Angle Closure. San Francisco: AAO; 2015.2. Lam DS, et al. Randomized trial of early phacoemulsification versus peripheral iridotomy to prevent intraocular pressure rise after acute primary angle closure.
Ophthalmology 2008;115:1134-40.3. Thomas R, Walland MJ. Management algorithms for primary angle closure disease. Clin Experiment Ophthalmol 2013;41:282-92.
1. Immediate IOP lowering with medications1
i. begin with (no more than 2gtt)ii. add or (2gtt 30 min apart)iii. add (acetazolamide 2 x 250mg PO) and/or
hyperosmotics2. Topical (q15min) to treat inflammation3. Once IOP <40mmHg and iris perfusion has improved,
to pull the iris away from the angle• indentation gonioscopy may help break pupillary block
4. Once corneal edema has decreased, therapeutic LPI• prophylactic LPI is necessary for the fellow eye
• CE may be an alternative to, or addition to LPI2
• extensive PAS or uncontrolled IOP: trabeculectomy3
5. Recheck IOP after 30 to 60 minutes if still in-office
In-office AACC toolkit:
1. topical beta-blocker
2. topical CAI or alpha agonist (ideally fast-acting Iopidine)
3. oral CAI (2 x 250mg acetazolamide, sustained release)
4. topical pilocarpine

MechanismAppositional closure1. Pupillary block• the primary mechanism for angle closure1
• irido-lenticular contact at pupil inhibits aqueous flow2
• increasing IOP in posterior chamber causes anterior iris bowing and appositional angle closure• more common with:• shallow anterior chamber• thicker (more pigmented) iris• thicker and/or more anterior lens• advancing age, cataract, exfoliation
1. American Academy of Ophthalmology Glaucoma Panel. Preferred Practice Pattern Guidelines. Primary Angle Closure. San Francisco: AAO; 2015.2. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.

MechanismAppositional closure2. a. Plateau iris configuration (PIC; pre-surgical diagnosis):
• angle crowding due to iris compression between a large anteriorly positioned CB and the TM1
• more common in younger hyperopic women2
• flat central iris (deep central chamber) turns sharply posteriorly before inserting into CB (narrow angle)• “double-hump” sign on compression gonioscopy• iris curves over peripheral CB and central lens
• may lead to widespread PAS and increased IOP• in PIC, there is still an element of pupillary block
1. Pavlin CJ, et al. Ultrasound biomicroscopy in plateau iris syndrome. Am J Ophthalmol 1992;113:390-5.2. Ritch R, et al. Angle closure in younger patients. Ophthalmology 2003;110:1880-9.3. Tarongoy P, et al. Angle-closure glaucoma: the role of the lens in the pathogenesis, prevention, and treatment. Surv Ophthalmol 2009;54:211-25.
2. b. Plateau iris syndrome (PIS; post-surgical diagnosis):• persistent ITC despite a patent LPI3

Plateau iris
http://webeye.ophth.uiowa.edu/eyeforum/cases/143-plateau-iris.htmPrata TS, et al. Indentation slitlamp-adapted optical coherence tomography technique for anterior chamber angle assessment. Arch Ophthalmol 2010;128:646-7.
Indentation gonioscopy causing a “double hump” in plateau iris: the peripheral hump is over the CB, the central is over the anterior lens (inset: as seen by AS-OCT)

Mechanism
UBM image of pupillary block: irido-lenticular contact causing
anterior bowing of the peripheral iris and appositional
angle closure
UBM image of plateau iris: anterior rotation of the ciliary
body creating appositional angle closure (note flat central iris and deep central chamber)
1. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.2. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.

MechanismAppositional closure3. Angle crowding• anterior segment imaging has suggested that a bulkier or
thicker peripheral iris may narrow the angle• may occur in the absence of, or in combination with
pupillary block or plateau iris1
• may be more common in, and help explain the higher prevalence of ACG in Asian eyes
• iris thickness is greatest in AACC and least in PACS
Most cases of PACG are due to more than one mechanism, although an element pupillary block is essentially universal2
1. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.2. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.

MechanismSynechial closure• with prolonged appositional closure (more common in
chronic ACG), broad PAS form1
• IOP increase can be significant, and difficult to control• permanent trabecular damage is possible2
• PAS usually require more treatment than LPI alone:• argon laser peripheral iridoplasty• lens extraction
• more extensive PAS (≥180°) may necessitate:• goniosynechialysis (+/- CE)• trabeculectomy3
1. Tian T, et al. The effect of phacoemulsification plus goniosynechialysis in acute and chronic angle closure patients with extensive goniosynechiae. BMC Ophthalmol 2019;19:65.
2. Sihota R, et al. The trabecular meshwork in acute and chronic angle closure glaucoma. Indian J Ophthalmol 2001;49:255-9.3. Radhakrishnan S, Chen L. Diagnosis and monitoring of primary angle closure. Curr Ophthalmol Rep 2015;3:51-7.

Peripheral anterior synechiae
https://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/Peripheral-anterior-synechiae.htm
Following prolonged appositional closure, peripheral anterior synechiae (PAS; broad adhesions between the iris and angle structures, often anterior to TM) can form

Medical treatment of chronic PACG
1. Emanuel ME, et al. Evidence-based management of primary angle closure glaucoma. Curr Opin Ophthalmol 2014;25:89-92.2. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.3. Wright C, et al. Primary angle-closure glaucoma: an update. Acta Ophthalmol 2016;94:217-25.4. Pavlin CJ, et al. Ultrasound biomicroscopy in plateau iris syndrome. Am J Ophthalmol 1992;113:390-5.
Aqueous suppressants:• beta-blockers, alpha agonists, and carbonic anhydrase
inhibitors can be effective in initial IOP control1• brimonidine may also cause helpful pupillary miosis2
Prostaglandin analogs (PGA):• effective in PACG even in the presence of extensive PAS3
Parasympathomimetics (miotics):• first used in the late 1800s• ciliary muscle contraction mechanically opens the TM• pupil constriction pulls the iris away from the TM• particularly helpful in preventing AACC in plateau iris4

Laser treatment
Laser peripheral iridotomy (LPI):
• has been first-line treatment for ACG for nearly 50 years1
• reduces pupillary block by reducing IOP differential
between anterior and posterior chambers2
• iris flattens and CB moves posteriorly, opening angle
• can reduce the progression from PACS to PAC to PACG
• more effective in early disease3
• less effective in the presence of extensive PAS
• relatively good safety profile4
• with a thick and darkly pigmented iris, LPI can induce
significant inflammation and pigment release, leading
to a post-treatment pressure spike5
1. Robin AL, Pollack IP. Argon laser peripheral iridotomies in the treatment of primary angle closure glaucoma. Arch Ophthalmol 1982;100:919-23.
2. He M, et al. Laser peripheral iridotomy in eyes with narrow drainage angles: ultrasound biomicroscopy outcomes. Ophthalmology 2007;114:1513-9.
3. Peng PH, et al. Long-term outcomes of laser iridotomy in Vietnamese patients with primary angle closure. Br J Ophthalmol 2011;95:1207-11.
4. Quigley HA. Long-term follow-up of laser iridotomy. Ophthalmology 1981;88:218-24.
5. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.

Laser treatment
Although most angles widen post-LPI:
• up to 25% will show persistent angle closure
• angle width significantly narrows 6 to 18 months post-LPI1
• angle closure can recur following initially successful LPI2
• nearly 60% of PAC eyes with ≥180° persistent
appositional closure go on to develop PACG3
1. Jiang Y, et al. Longitudinal changes of angle configuration in primary angle-closure suspects. Ophthalmology 2014;121:1699-1705.
2. Ng WT, Morgan W. Mechanisms and treatment of primary angle closure: a review. Clin Exp Ophthalmol 2012;40:e218-e228.
3. Qiu L, et al. Appositional angle closure and conversion of primary angle closure into glaucoma after laser peripheral iridotomy. Br J Ophthalmol 2019; doi:
10.1136/bjophthalmol-2018-312956
Laser treatmentArgon laser peripheral iridoplasty (ALPI):• superficial thermal burns pull peripheral iris away from TM,
widening angle• more effective in combination with LPI1
• effective in plateau iris to reduce ITC post-LPI2
• can be used post-pilocarpine administration in AACC3
• immediate effect• may help prevent subsequent PAS formation4
• possible adverse effect: Urrets-Zavalia syndrome (prolonged pupil dilation following ALPI)5
1. Sun X, et al. Laser peripheral iridotomy with and without iridoplasty for primary angle-closure glaucoma. Am J Ophthalmol 2010;150:68-73.2. Ritch R, et al. Long-term success of argon peripheral laser iridoplasty in the management of plateau iris syndrome. Ophthalmology 2004;111:104-8.3. Tham CC, et al. Immediate argon laser peripheral iridoplasty for acute attack of PACG. Ophthalmology 1999;106:1042-3.4. Tarongoy P, et al. Angle-closure glaucoma: the role of the lens in the pathogenesis, prevention, and treatment. Surv Ophthalmol 2009;54:211-25.5. Espana EM, et al. Urrets-Zavalia syndrome as a complication of argon laser peripheral iridoplasty. Br J Ophthalmol 2007;91:427-9.

Surgical treatment
Goniosynechialysis (GSL):• strips PAS and allows aqueous to access the TM3
• effective early: prolonged PAS irreversibly damage TM• usually used in combination with LPI, ALPI, and/or CE4
There is little consensus, and some controversy, on the best approach to surgically manage angle closure disease1
Anterior chamber paracentesis• leads to a rapid short-term decrease in IOP in AACC2
• can be technically difficult in a crowded inflamed eye
1. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.2. Lam DS, et al. Efficacy and safety of immediate anterior chamber paracentesis in the treatment of acute primary angle-closure glaucoma. Ophthalmology
2002;109:64-70.3. Wright C, et al. Primary angle-closure glaucoma: an update. Acta Ophthalmol 2016;94:217-25.4. Tanihara H, et al. Surgical results and complications of goniosynechialysis. Graefes Arch Clin Exp Ophthalmol 1992;230:309-13.
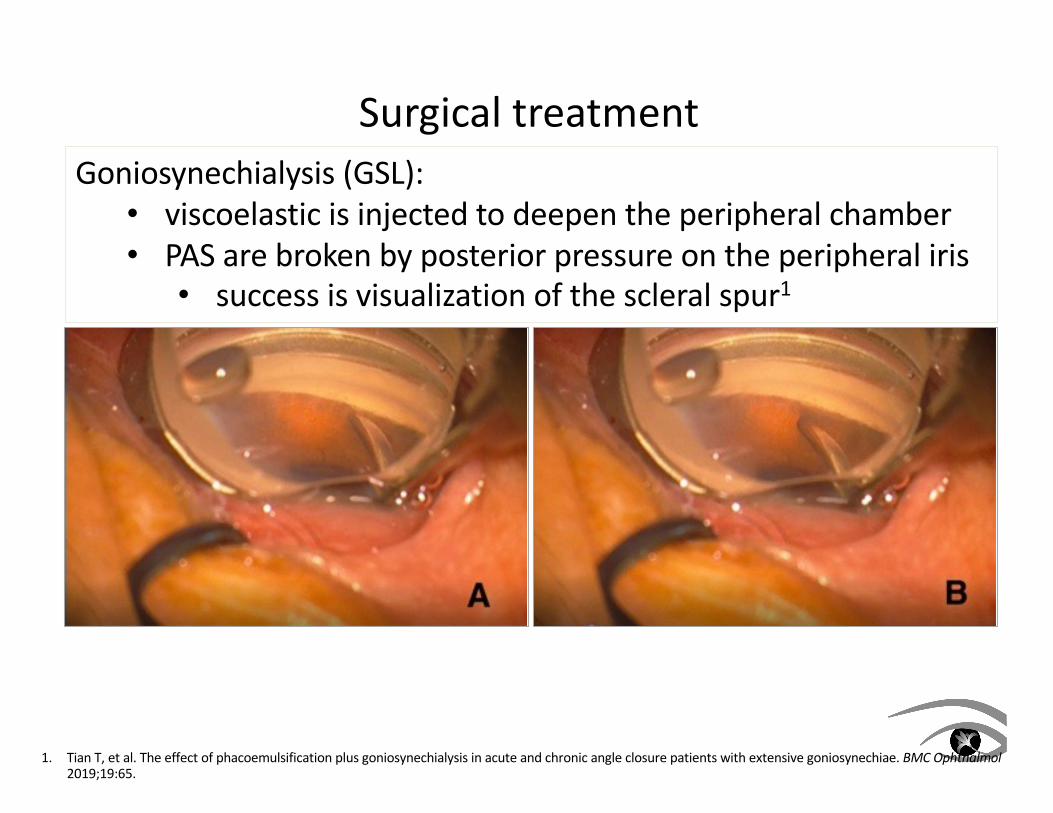
Surgical treatmentGoniosynechialysis (GSL):• viscoelastic is injected to deepen the peripheral chamber• PAS are broken by posterior pressure on the peripheral iris• success is visualization of the scleral spur1
1. Tian T, et al. The effect of phacoemulsification plus goniosynechialysis in acute and chronic angle closure patients with extensive goniosynechiae. BMC Ophthalmol2019;19:65.

Surgical treatmentTrabeculectomy:• with permanent TM dysfunction, the surgical treatment of
PACG becomes similar to that of POAG• adequate IOP control in nearly 70% of cases1
• however, technically challenging in a narrow angle• risk of complications is greater in PACG than POAG2
• most commonly, shallow or flat anterior chamber3
• high IOP: malignant (ciliary block) glaucoma• post-operative inflammatory CB swelling4
• increased pressure in the vitreous causing anterior movement of CB, iris, and lens5
• hypotony: choroidal effusion
1. Salmon JF. The role of trabeculectomy in the treatment of advanced chronic angle-closure glaucoma. J Glaucoma 1993;2:285-90.2. Bevin TH, et al. Otago Glaucoma Surgical Outcome Study: long-term results of 841 trabeculectomies. Clin Experiment Ophthalmol 2008;36:731-7.3. Sun X, et al. Primary angle closure glaucoma: what we know and what we don’t know. Prog Ret Eye Res 2017;58:26-45.4. Tian T, et al. The effect of phacoemulsification plus goniosynechialysis in acute and chronic angle closure patients with extensive goniosynechiae. BMC Ophthalmol
2019;19:65.5. Ng WT, Morgan W. Mechanisms and treatment of primary angle closure: a review. Clin Exp Ophthalmol 2012;40:e218-e228.

Surgical treatment
Cataract or clear lens extraction (CE)
• many studies have suggested that CE is effective in PACG1
• all anterior segment parameters improve significantly
following CE (more so than following LPI)2-4
• effectively eliminates pupillary block
• increased chamber depth and angle width
• no residual angle closure (vs. ~25% post-LPI)
• lower IOP and fewer post-treatment medications
• improved BCVA post-CE
• can be used in combination with GSL and trabeculectomy
CE can be technically difficult in ACG: shallow chamber, thick lens
• plateau iris configuration may persist post-CE5
1. Tham CC, et al. Phacoemulsification versus combined phacotrabeculectomy in medically uncontrolled chronic angle closure glaucoma with cataracts. Ophthalmology2009;116:725-31.
2. Yan C, et al. Effects of lens extraction versus laser peripheral iridotomy an anterio segment morphology in primary angle closure suspect. Graefe’s Arch Clin ExpOphthalmol 2019;doi: 10.1007/s00417-019-04353-8.
3. Hayashi K, et al. Changes in anterior chamber angle width and depth after intraocular lens implantation in eyes with glaucoma. Ophthalmology 2000;107:698-703.
4. Tarongoy P, et al. Angle-closure glaucoma: the role of the lens in the pathogenesis, prevention, and treatment. Surv Ophthalmol 2009;54:211-25.
5. Chan PP, Tham CC. Commentary on effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE). Ann Eye Sci 2017;2:21.

Surgical treatmentEAGLE Study• Effectiveness in Angle-closure Glaucoma of Lens Extraction• 419 patients ≥50 years old with PAC (IOP ≥30mmHg) or
PACG randomized to LPI or CE1
At 36 months, resulted in:• significantly better quality of life scores• significantly lower IOP• significantly fewer post-treatment medications• further surgical treatment (CE and trabeculectomy) was
3x more common post-LPI2
1. Azuara-Blanco A, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomized controlled trial. Lancet2016;388:1389-97.
2. Chan PP, Tham CC. Commentary on effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE). Ann Eye Sci 2017;2:21.

Surgical treatmentEAGLE Study:
“… initial treatment [with CE] was superior to [LPI] plus topical medical treatment for participants with [PAC and PACG] …”1
“The potential importance of this definitive procedureto correct persistent pupillary-block and angle crowdingafter LPI in both the treatment and prevention of acute
and chronic angle closure glaucoma cannot be overstated.”2
1. Azuara-Blanco A, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomized controlled trial. Lancet2016;388:1389-97.
2. Chan PP, Tham CC. Commentary on effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE). Ann Eye Sci 2017;2:21.

Primary angle closure is very under-diagnosed, andresponsible for a disproportionate amount of severe vision lossAs such, the identification of patients at risk of progressing toprimary angle closure glaucoma is of paramount importance
While imaging techniques are useful adjuncts,gonioscopy remains the gold standard of angle assessment
When primary angle closure or primary angle closure glaucoma is identified, surgical intervention is indicated to reduce the risk of ongoing appositional or synechial angle closure and permanent trabecular damage• laser peripheral iridotomy, often in conjunction with (and
perhaps soon to be replaced by) cataract surgery
